Embed Size (px)
Citation preview
Headaches
Donald L. Gilbert MD MSProfessor of Pediatrics and Neurology
DisclosuresI have the following financial relationships with the manufacturers of commercial products and/or providers of commercial services:
Ecopipam Pharmaceuticals, EryDel Pharmaceuticals, and Neurocrine Pharmaceuticals - Research Grant
(Please note: Clinical trial site investigator); Elsevier – Royalties for books
I do not intend to discuss an unapproved/investigative use of a commercial products (drugs, devices) related to these relationships.
Objectives
1) List key strategies for managing migraines and chronic daily headache in children, including lifestyle counseling and evidence based pharmacological treatments for aborting and preventing migraines
2) Identify “red flags” on history and physical examination that a headache may be secondary to an intracranial process.
As a result of attending this lecture at the 2017 Practical Pediatrics CME course, I encourage you to make the following change in your practice• Use current diagnostic criteria for headaches• Treat patients with frequent migraines aggressively with a combined
approach that includes lifestyle and psychological interventions• Remain vigilant for secondary headaches and evaluate appropriately

BACKGROUND
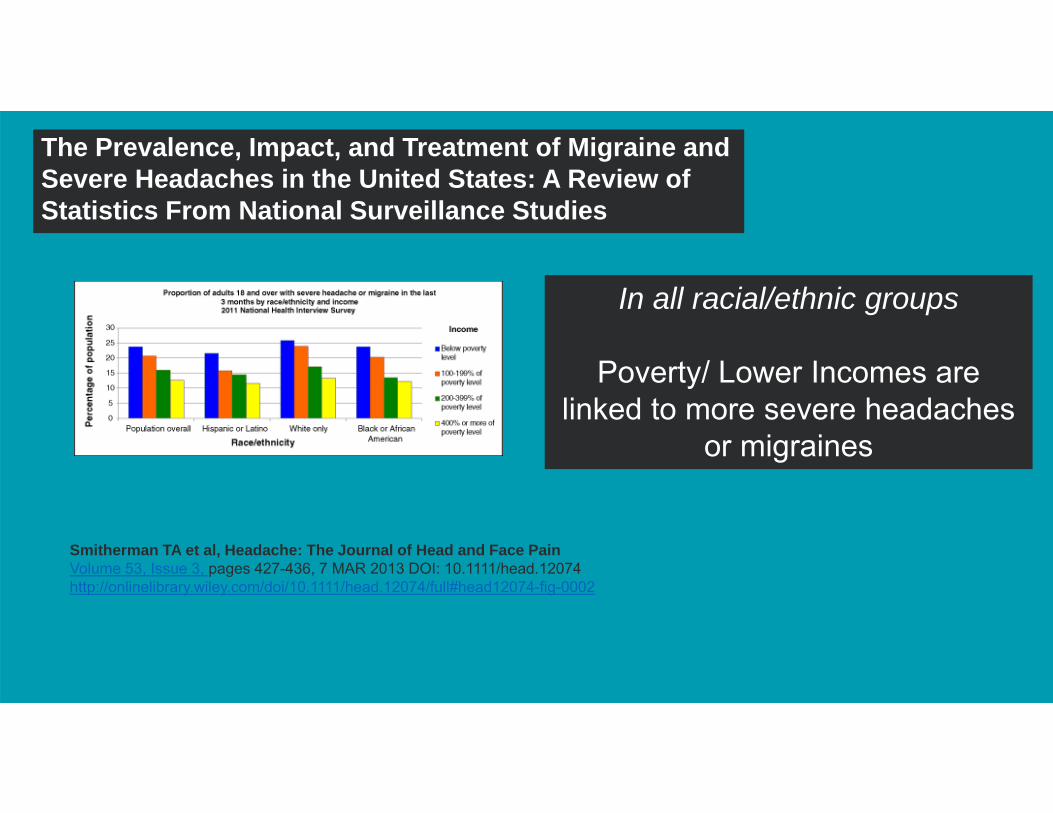
The Prevalence, Impact, and Treatment of Migraine and Severe Headaches in the United States: A Review of Statistics From National Surveillance Studies
Smitherman TA et al, Headache: The Journal of Head and Face PainVolume 53, Issue 3, pages 427-436, 7 MAR 2013 DOI: 10.1111/head.12074http://onlinelibrary.wiley.com/doi/10.1111/head.12074/full#head12074-fig-0002
In all racial/ethnic groups
Poverty/ Lower Incomes are linked to more severe headaches
or migraines
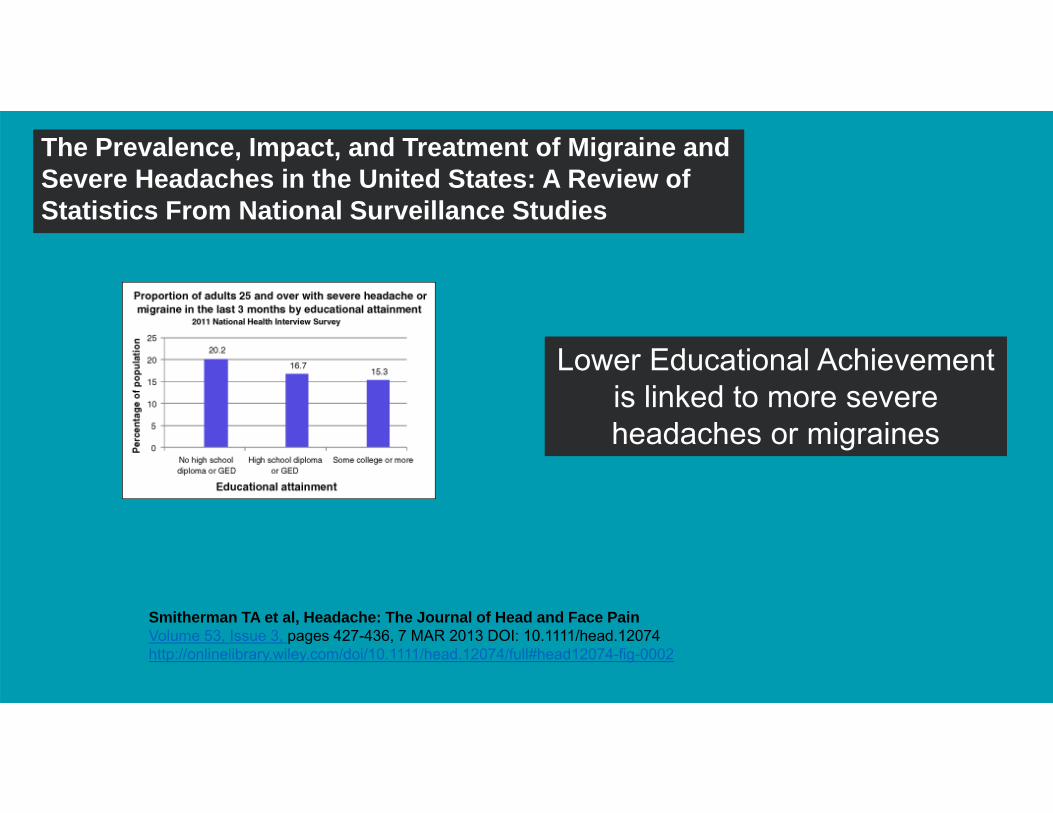
Lower Educational Achievement is linked to more severe headaches or migraines
Smitherman TA et al, Headache: The Journal of Head and Face PainVolume 53, Issue 3, pages 427-436, 7 MAR 2013 DOI: 10.1111/head.12074http://onlinelibrary.wiley.com/doi/10.1111/head.12074/full#head12074-fig-0002
The Prevalence, Impact, and Treatment of Migraine and Severe Headaches in the United States: A Review of Statistics From National Surveillance Studies
Prevalence in Childhood
• Headache 54% (95% CI 43-66%)• Migraine 9% (95% CI 7-11%)
– Estimated from 64 studies, 32 countries, totaling >200,000 subjects
• Wober-Bingo C, Current Pain and Headache Reports 2013
Classification – ICHD-3 beta
• https://www.ichd-3.org
• This is a useful website with helpful information for you and nice slide-sets as well
International Headache SocietyClassification of HeadacheDisorders
“Good Headache”
Chronic, nonprogressive headache disorders; “primary headaches”
“Bad Headache”
Headaches caused by intracranial pathological processes; “secondary headaches”
Workup – diagnostic approach
There are algorithms to help balance between excessive expensive low yield workups of “good headaches” and missing subtle presentations of “bad headaches” but ultimately this is not easy. Experience helps. When you’re not sure, refer.
Case
• A 14 year old, healthy female in the ninth grade presents for evaluation for headache.

DIAGNOSIS?
NEUROLOGY REQUIRES A SYSTEMATIC APPROACH
History – key points
• Think about secondary headaches first• Ask key questions• Look for key signs on exam

Secondary Headaches
18
Increased Intracranial Pressure (ICP)
• Before the sutures and fontanelles are closed, the skull can grow to accommodate space-occupying pathology
• After sutures are closed, space occupying pathologies raise intracranial pressure– Extra fluid (hydrocephalus)– Extra blood (vascular problems))– “Extra brain” (tumors)– Pseudotumor
19
Elements of History Concerning for increased ICP
• Increased pain at night – headaches awaken from sleep• Headaches increase with valsalva• Vomiting• Double vision that goes away when covering one eye
– Or vision loss/ enlarged blindspot etc
20
Examination Signs Concerning for increased ICP
• Ocular malalignment (new) (note: usually non-localizing 6th nerve palsy – one or both eyes can’t abduct/go-out)
• Fundoscopic examination papilledema– Always check fundi
• Meningismus, Babinski (toes up), clonus, gait problems, limb ataxia, focal weakness
• Hyper-reflexia concerning but less specific if this is the only finding
What should you do if you suspect a headache is caused by increased
intracranial pressure?
Refer to Emergency Department
• Call the ED and let them know you are referring child in and are worried about a brain tumor or idiopathic intracranial hypertension which could cause vision loss
• Ask for confirmation of your papilledema finding• Ask them to please call you back with imaging findings and the
opening pressure from the Lumbar Puncture• Urgent imaging (usually CT) should be obtained and LP performed if
symptoms and signs of raised ICP without CT findings. If CSF pressure high, MRI brain with MRV, further workup indicated
**What medications are linked to pseudotumorcerebri?**1. Antibiotics: tetracycline, minocycline, doxycycline,
nitrofurantoin, sulphonamides, nalidixic acid2. Hormonals: tyroxine, growth hormone, tamoxifen3. Vitamin A: excess A, retinoids like isotretrinoin (for acne)4. Other: steroids, lithium, cyclosporine
**Post concussive headaches**
• Persistent headache often occurs after mild concussion• In children, this is strongly linked to family history of
migraine• Treatment with interventions similar to primary headache
disorders is probably similarly effective
Primary headache diagnoses per ICHD-3 beta
Migraine
A. At least 5 attacksB. Duration 2 to 72 hoursC. With ≥ 2 features:
1. Unilateral2. Pulsating quality3. Moderate to severe intensity pain4. Aggravated by or causing avoidance of routine physical activity
D. Accompanied by ≥ 1 other symptoms1. Nausea and/or vomiting2. Photophobia and phonophobia
Tension Type Headache
A. At least 10 attacksB. Duration 30 minutes to 7 daysC. With ≥ 2 features:
1. Bilateral2. Pressing/tightening, non-pulsating3. Mild or moderate4. Not aggravated by routine physical activity
D. Both of these:1. No nausea or vomiting2. No more than one of photo- or phonophobia
Chronic Migraine (chronic daily headache)
A. Headache (tension type and/or migraine-like) on ≥ 5 days per month for ≥ 3 months
B. Headache has migrainous features >7 days per monthC. At clinical presentation, may also meet criteria for
Medication-overuse headache.

Case
Case 1
• A 14 year old, healthy female in the ninth grade presents for evaluation for headache. She has had similar headaches for at least 3 years, but this fall they are occurring 2-3x per week.
Case 1
• Headaches are bifrontal, throbbing, sometimes severe enough that she misses school. They last 2 or more hours but are relieved by sleep and/or ibuprofen. She wants to lie down in a dark room. She has nausea, pallor, photophobia, phonophobia.
Case 1• Headaches are bifrontal,
throbbing, sometimes severe enough that she misses school. They last 2 or more hours but are relieved by sleep and/or ibuprofen. She wants to lie down in a dark room. She has nausea, pallor, photophobia, phonophobia.
A. At least 5 attacksB. Duration 2 to 72 hoursC. With ≥ 2 features:
1. Unilateral2. Pulsating quality3. Moderate to severe intensity
pain4. Aggravated by or causing
avoidance of routine physical activity
D. Accompanied by ≥ 1 other symptoms
1. Nausea and/or vomiting2. Photophobia and phonophobia
1/17/2017 33
Migraine Treatment - infrequent
• Reduce any identifiable triggers – lifestyle, healthy habits
• Abortive treatment with NSAIDS• Triptans statistically no better, but some patients may
respond better to triptans and nasal dosing may be helpful for headaches with nausea/vomiting
Migraines – frequent but not daily, non-medical interventions
• Lifestyle, lifestyle, lifestyle• Weight loss, exercise, sleep, caffeine• Hydrate – 8 8 oz glasses of water per day• Coping training?
Severe Migraine in the ED
• IV fluids 20 mg/kg NS bolus, max 1 L
• Prochlorperazine (Compazine) 0.15 mg/kg IV (max 10 mg) plus Ketorolac (Toradol) 0.5 mg/kg IV (max 30 mg)
Migraines – frequent but not daily: what preventive treatment is evidence based?
Migraines – frequent but not daily: what preventive treatment is evidence based?
• Ciproheptadine 2 to 4 mg QD or BID for kids < 7y• Amitryptiline up to 1 mg/kg/day good first line choice • Topiramate escalate slowly to avoid SE’s, e.g. 25 mg
daily, increase by 25 mg/week for 4 weeks• Other RX: propranolol, verapamil, etc
Clinical Trial Evidence
8-17 year olds, mean 11 migraine
headaches per month pre treatment
8-17 year olds, mean 11 migraine headaches per
month pre treatment
If you did nothing, how likely would these kids be to improve significantly
in the next 6 months?
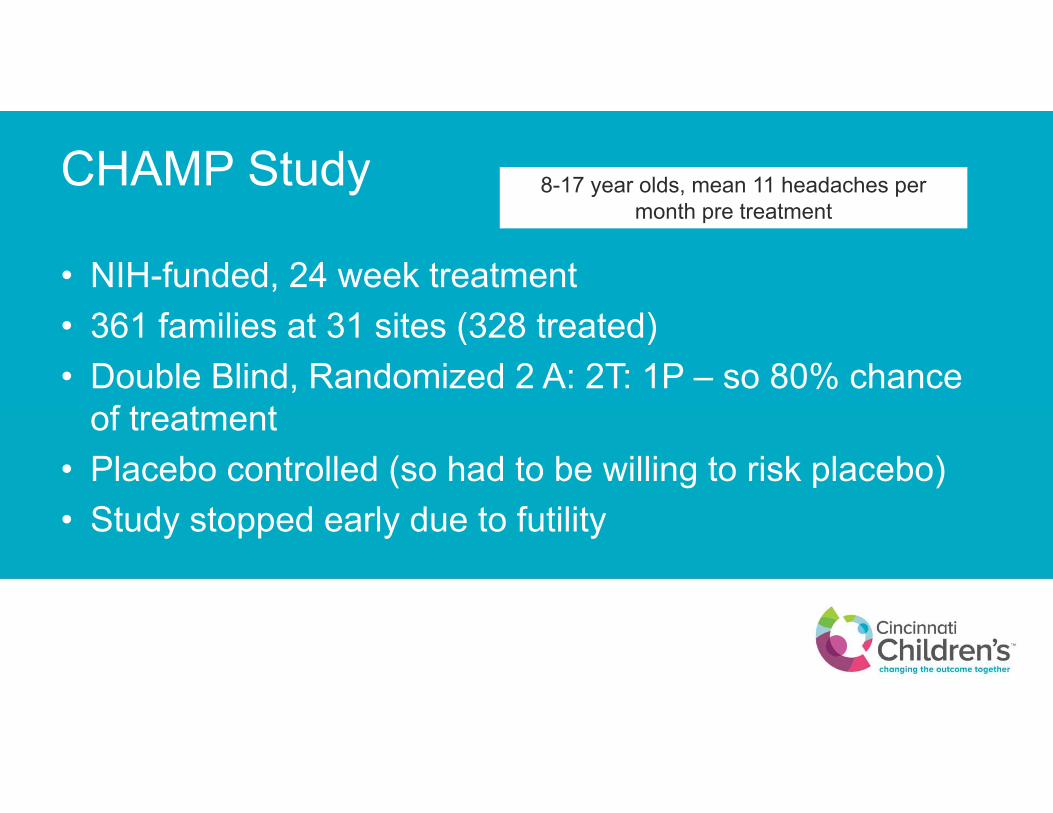
CHAMP Study
• NIH-funded, 24 week treatment• 361 families at 31 sites (328 treated)• Double Blind, Randomized 2 A: 2T: 1P – so 80% chance
of treatment• Placebo controlled (so had to be willing to risk placebo)• Study stopped early due to futility
8-17 year olds, mean 11 headaches per month pre treatment
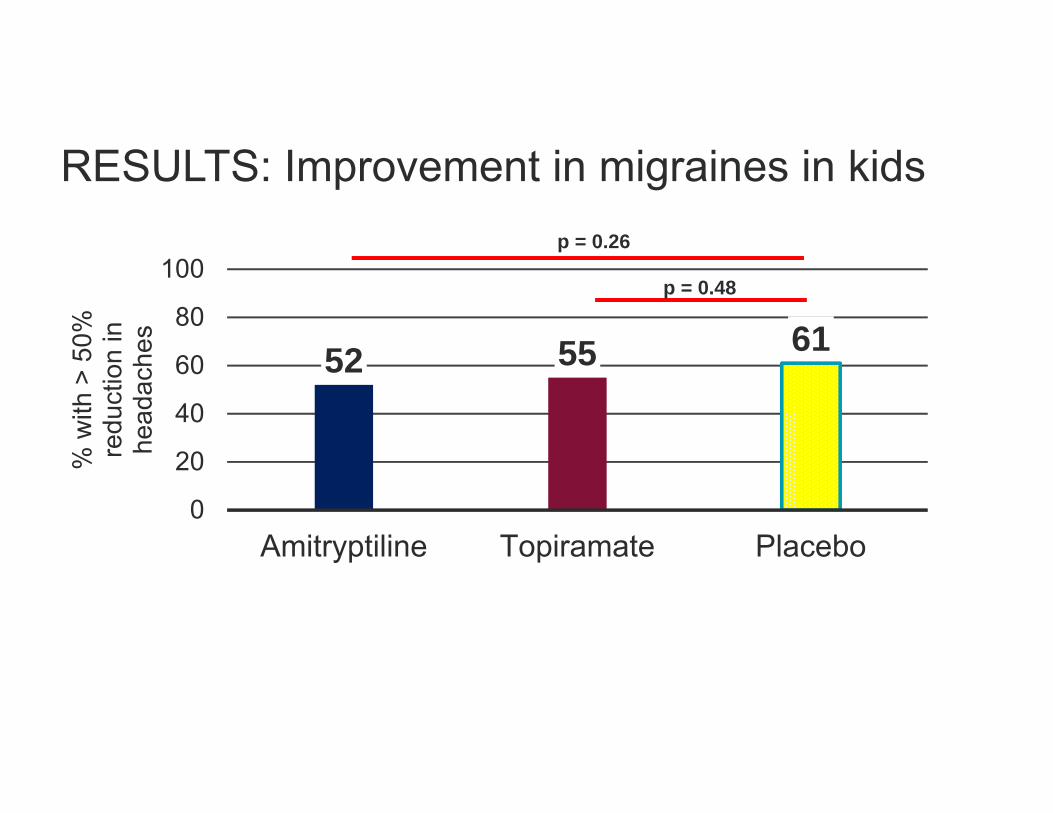
RESULTS: Improvement in migraines in kids
52 55 61
0
20
40
60
80
100
Amitryptiline Topiramate Placebo
% w
ith >
50%
re
duct
ion
in
head
ache
s
p = 0.26
p = 0.48
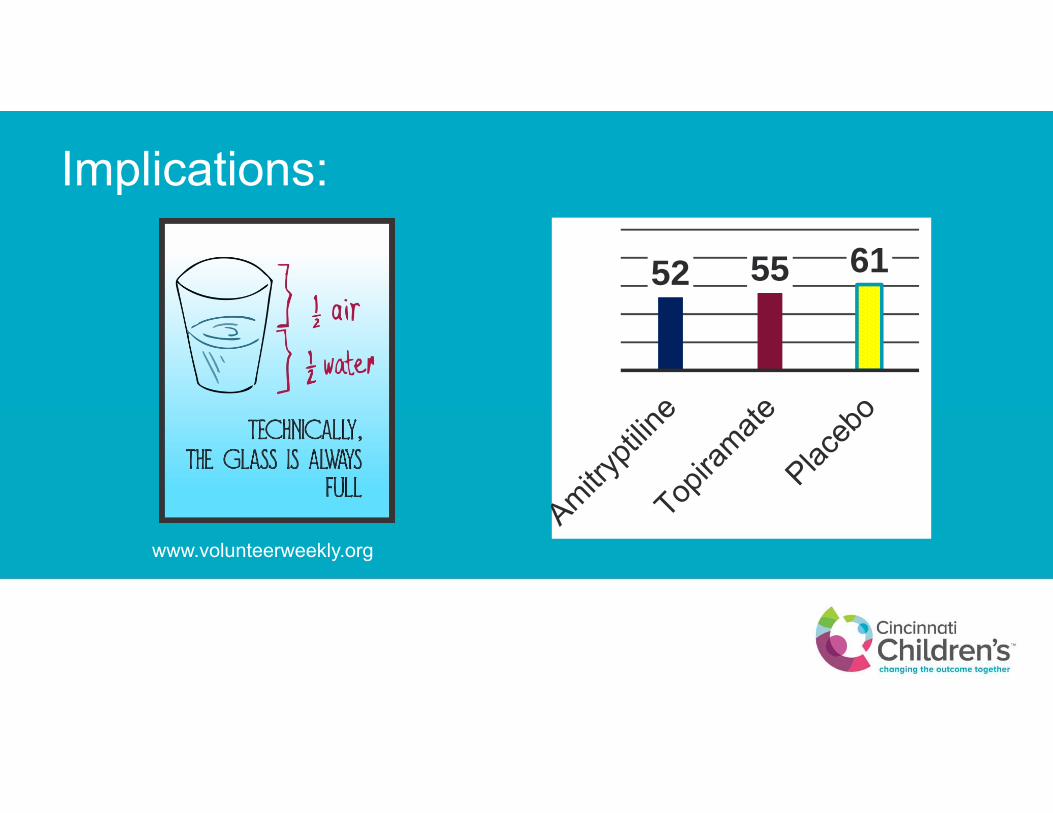
Implications:
52 55 61
www.volunteerweekly.org
Spending time with the patients validating their concerns, working on lifestyle and psychological issues is a winning strategy
It is still OK to prescribe preventive treatments favored by headache experts: amitryptiline and topiramate

One more
Migraine – daily/ chronic daily headache
• Controversy as to whether this is conversion from inadequately treated/severe episodic migraines, or has psychosomatic origin. Probably both are involved.
• High stress/ high psychological needs population• Lots of somatization and school avoidance behaviors. May be
enabled by the parents• Referral to psychology for behavioral therapies is indicated.
As a result of attending this lecture at the 2017 Practical Pediatrics CME course, I encourage you to make the following change in your practice• Use current diagnostic criteria for headaches• Treat patients with frequent migraines aggressively with a combined
approach that includes lifestyle and psychological interventions• Remain vigilant for secondary headaches and evaluate appropriately
References1. Smitherman TA, Burch R, Sheikh H, Loder E. The prevalence, impact, and
treatment of migraine and severe headaches in the United States: a review of statistics from national surveillance studies. Headache. 2013;53(3):427-436.
2. Ravishankar K. "WHICH Headache to Investigate, WHEN, and HOW?". Headache. 2016;56(10):1685-1697.
3. Powers SW, Coffey CS, Chamberlin LA, et al. Trial of Amitriptyline, Topiramate, and Placebo for Pediatric Migraine. N Engl J Med. 2016.
4. Kroner JW, Hershey AD, Kashikar-Zuck SM, et al. Cognitive Behavioral Therapy plus Amitriptyline for Children and Adolescents with Chronic Migraine Reduces Headache Days to </=4 Per Month. Headache. 2016;56(4):711-716.
5. O'Brien HL, Kabbouche MA, Kacperski J, Hershey AD. Treatment of pediatric migraine. Curr Treat Options Neurol. 2015;17(1):326.

References6. Markey KA, Mollan SP, Jensen RH, Sinclair AJ. Understanding idiopathic
intracranial hypertension: mechanisms, management, and future directions. Lancet Neurol. 2016;15(1):78-91.
7. Kuczynski A, Crawford S, Bodell L, Dewey D, Barlow KM. Characteristics of post-traumatic headaches in children following mild traumatic brain injury and their response to treatment: a prospective cohort. Dev Med Child Neurol. 2013;55(7):636-641.
8. Green A, Kabbouche M, Kacperski J, Hershey A, O'Brien H. Managing Migraine Headaches in Children and Adolescents. Expert Rev ClinPharmacol. 2016;9(3):477-482.
9. Alfonzo M, Chen L. Acute Migraine Management in Children. Pediatr EmergCare. 2015;31(10):722-727; quiz 728-730.
Thank you for your attention