Embed Size (px)
Citation preview
СЪДЪРЖАНИЕ
172
183
189
194
201
208
211
216
CONTENTS
B U L G A R I A N F O R U M
G L A U C O M AEdition of the ãNational Academy GlaucomaÓ Foundation, Sofia, Bulgaria
SURGICAL TREATMENT1. Clinical cases of surgical revision with OlogenTM im -plantation in eyes with glaucoma and Еx-PRESS¨ im-plant
B. Anguelov
GLAUCOMA - PATHOGENESIS
2. Blood pressure, ocular perfusion pressure and glau-coma
A. Martinez
DIAGNOSTICS3. Practical guidance for application of standard auto-mated perimetry in glau coma diagnostics
M. Benova, B. Anguelov
MEDICAL THЕRAPY4. Mechanism of action of prostaglandin F
2α-ana lo-gues in the eye in the treatment of glaucoma
B. Anguelov, B. Mihaylova, N. Dakov
CASE REPORT
5. Myopia as a risk factor for glaucoma.
Case report
B. Samsonova
6. Case of a child with congenital glaucoma asso-ciated with malformative syndrome
А. Popova, R. Tinchevа
GLAUCOMA - TYPES7. Corticosteroid induced ocular hypertension and glau-coma
K. Petrova, B. Anguelov
8. Management of post-traumatic glaucoma
B. Anguelov, B. Gagova
ХИРУРГИЧНО ЛЕЧЕНИЕ1. Clinical cases of surgical revision with OlogenTM im -plantation in eyes with glaucoma and Еx-PRESS¨ im-plant
B. Anguelov
ГЛАУКОМА - ПАТОГЕНЕЗА
2. Blood pressure, ocular perfusion pressure and glau -coma
A. Martinez
ДИАГНОСТИКА3. Практически насоки за приложението на стан-дартна автоматична периметрия в диагнос ти-ката на глаукомата
М. Бенова, Б. Ангелов
МЕДИКАМЕНТОЗНА ТЕРАПИЯ4. Механизъм на действие на простагландинови-те F
2α-аналози в окото при лечението на глау-кома
Б. Ангелов, Б. Михайлова, Н. Даков
КЛИНИЧEН СЛУЧАЙ
5. Миопията като рисков фактор за развитието на глаукома. Клиничен случай
Б. Самсонова
6. Случай на дете с вродена глаукома асоциирана с малформативен синдром
А. Попова, Р. Тинчева
ГЛАУКОМА - ВИДОВЕ7. Кортикостероид индуцирана очна хипер тен-зия и глаукома
К. Петрова, Б. Ангелов
8. Терапевтичен подход при посттравматична глаукома
Б. Ангелов, Б. Гагова
ГЛАВЕН РЕДАКТОР:
Доц. д-р Ботьо Ангелов, д.м. Катедра по офталмология, МУ
УМБАЛ ãАлександровскаÓ, София, България
Assoc. Prof. Botio Anguelov, MD, PhD Department of Ophthalmology, Medical University
ãAlexandrovskaÓ Hospital, Sofia, Bulgaria
EDITOR-IN-CHIEF:
РЕДАКЦИОННА КОЛЕГИЯ: EDITORIAL BOARD:
Проф. д-р Силвия Чернинкова, д.м., д.м.н. Катедра по неврология, МУ
УМБАЛ ãАлександровскаÓ, София, България
Проф. д-р Габор Хoло, д.м., д.м.н.Катедра по офталмология
Университетска болница ãСемелвейсÓБудапеща, Унгария
Проф. д-р Милко ИлиевКатедра по офталмология
Университетска болница, Берн, Швейцария
Доц. д-р Барбара Цвенкел, д.м.Очна клиника, Университетски медицински център Любляна
Любляна, Словения
Проф. д-р Фотис Топузис, д.м.Университет ãАристотелÓ, Болница AХEПА
Катедра по ОфталмологияСолун, Гърция
Проф. д-р Александър Куроедов, д.м., д.м.н.2-ра Централна военна болница ãМандрикаÓ
Катедра по офталмологияДържавен медицински университет, Москва, Русия
Доц. д-р Пол Чю, д.м.Катедра по офталмология
Национална университетска болницаСингапур
Д-р Терек ШарауиГлаукомен сектор
Катедра по клинични невронаукиЖеневски университет
Швейцария
Проф. д-р Антонио Мартинес, д.м.Катедра по офталмология
Университет ãСантяго де КомпостелаÓЛа Коруня, Испания
Проф. д-р Робърт Уейнреб Очен център ãШилейÓ
Глаукомен център ãХамилтънÓКалифорнийски университет, Сан Диего, Калифорния, САЩ
Проф. д-р Тануж Дада Център по очни науки ãД-р Раджендра ПрасадÓ
Институт по медицински наукиНю Делхи, Индия
Д-р Антон ХомерГлаукомен сектор, Болница ãХераÓ
Виена, Австрия
Проф. д-р Шломо Меламед, д.м.Глаукомен център ãСам РотбергÓМедицински център ãШебаÓТел Хашомер, Израел
Д-р Радуил Цеков, д.м.Институт ãРоскампÓ, Сарасота, Флорида
Очен Институт, Университет на Южна Флорида, Тампа, Флорида, САЩ
Д-р Боряна Цветкова Страсбург, Франция
Д-р Николай Даков Катедра по офталмология, МУ
УМБАЛ ãАлександровскаÓ, София, България
Prof. Sylvia Cherninkova, MD, PhD, DSci Department of Neurology, Medical University
ãAlexandrovskaÓ Hospital, Sofia, Bulgaria
Prof. Gabor Hollo, MD, PhD, DSciDepartment of Ophthalmology
Semmelweis UniversityBudapest, Hungary
Prof. Milko Iliev, MDDepartment of Ophthalmology
University of Bern, Inselspital, Bern, Switzerland
Assoc. Prof. Barbara Cvenkel, MD, PhDEye Clinic, University Medical Centre Ljubljana
Ljubljana, Slovenia
Prof. Fotis Topouzis, MD, PhDAristotle University, AHEPA Hospital
Department of OphthalmologyThessaloniki, Greece
Prof. Alexander Kuroyedov, MD, PhD, DSciMandryka 2nd Central Clinical Hospital
Department of OphthalmologyRussian State Medical University, Moscow, Russia
Assoc. Prof. Paul Chew, MD, PhDDepartment of Ophthalmology
National University HospitalSingapore
Tarek Shaarawy, MDGlaucoma sector
Department of Clinical NeurosciencesUniversity of Geneva
Switzerland
Prof. Antonio Martlnez, MD, PhDDepartment of Ophthalmology
University of Santiago de CompostelaLa Coruna, Spain
Prof. Robert Weinreb, MDShiley Eye Center
Hamilton Glaucoma CenterUniversity of California, San Diego, California, USA
Prof. Tanuj Dada, MDDr Rajendra Prasad Centre for Ophthalmic Sciences
All India Institute of Medical SciencesNew Delhi, India
Anton Hommer, MDGlaucoma Unit, Hera Hospital
Vienna, Austria
Prof. Shlomo Melamed, MD, PhDThe Sam Rothberg Glaucoma Center
Sheba Medical CenterTel Hashomer, Israel
Radouil Tzekov, MD, PhDThe Roskamp Institute, Sarasota, FloridaUSF Eye Institute, Tampa, Florida, USA
Boriana Tzvetkova, MD Strasbourg, France
Nikolai Dakov, MD Department of Ophthalmology, Medical University
ãAlexandrovskaÓ Hospital, Sofia, Bulgaria
~
Õ
Contact information: e-mail: [email protected]
Õ Õ
172 2013, ТОМ 3, Брой 4
ХИРУРГИЧНО ЛЕЧЕНИЕ / SURGICAL TREATMENT
IntroductionIn the fi eld of antiglaucoma surgery well established
operative techniques are being improved or entirely new interventions and implants are being developed and introduced in the clinical practice. Improving the long term hypotensive effect and reducing the complications (intraoperative, early and late postoperative) is the key goal.
One of the leading causes for failure of antiglaucoma fi ltration surgery is the fi brotic changes in the bleb area [13]. Episcleral fi brosis, fi brosis and bleb encapsulation, dysmorphic fi ltering bleb can compromise to a varying degree the outcome of the performed surgical intervention. Restriction of the aqueous humor outfl ow trough the newly created pathway leads to IOP elevation above the target values.
There was a huge progress with the introduction and wide use of antifi brotic agents that undoubtedly led to the improvement and optimization of the results after antiglaucoma surgery. Despite that, the application of antifi brotic agents considerably increases the risk of developing some complications and the
most serious of them are the the hypotony maculopathy and endophthalmitis [14, 15, 24].
OlogenTM (Aeon Astron Corp., Netherlands) is a biodegradable collagen matrix implant comprised of 90% atelocollagen type I and 10% glycosaminoglycans. It has a porous structure with pore size ranges between 10~300 μm. According to different data, it degrades for a period of 90 to 180 days [7, 10, 38]. The Ologen is available in different forms and sizes and apart from glaucoma surgery it is used in the operative management of strabismus and pterigium. The basic idea in the development and application of the Ologen in glaucoma surgery is the reduction and postponement of the fi brous processes in the fi ltering bleb area. As a result the IOP lowering effect of the operation is being improved and stabilized and the complications due to usage of antimetabolites are being reduced [3, 28, 33].
When dysfunction of the bleb occurs along with restriction of aqueous humor outfl ow and IOP elevation, there are some options at the surgeon‘s disposal which frequently may need to
Clinical cases of surgical revision with OlogenTM implantation in eyes with glaucoma and Еx-PRESS¨
implant
B. AnguelovDepartment of Ophthalmology, Medical University „Alexandrovska” Hospital, Sofi a
AbstractPurpose: To perform a surgical revision with OlogenTM implantation in eyes with glaucoma and Еx-PRESS® implant and to follow up the postoperative results.Material and methods: Three patients (3 eyes) are presented: 61-year-old primary open angle glaucoma patient, a 33-year-old patient with glaucoma associated with Sturge-Weber syndrome and a 59-year-old primary open angle glaucoma patient. All patients were previously operated for glaucoma with Еx-PRESS® implantation. Postoperatively, after different period of time, a bleb encapsulation was observed in two of the eyes and excessive fi brosis in the fi ltration area in one eye. In the eyes with bleb encapsulation we performed bleb needling several times, but with unsatisfactory outcome. Due to the permanent IOP elevation in all 3 eyes we performed a surgical revision using OlogenTM biodegradable implant which was placed in the bleb area under tenon and conjunctiva. Results: During the follow up period (from 3 months to 11 months for the different patients) IOP drop to the target values was achieved in all operated eyes. Discontinuing of the drug therapy was achieved in all operated eyes. During the follow up period, neither additional IOP lowering interventions were performed nor antiglaucoma drops were installed on the operated eyes. No complications were observed.Conclusion: All the described patients are diffi cult for management cases of advanced glaucoma, medically treated for long period of time. What is more, prior the our intervention, one or more glaucoma surgery procedures were performed in all eyes, which defi nitely have a negative impact on the post-op results. In two of the eyes bleb needling was performed several times. Despite that, postoperative results are really promising and show that the surgical revision with OlogenTM implantation in eyes with glaucoma and Еx-PRESS® implant leads to IOP reduction. Following up more patients for a longer period of time is needed.We were unable to fi nd publications or other articles in the open literature, describing a surgical procedure and patients’ follow up after an intervention similar to the one we’ve performed - surgical revision with OlogenTM implantation in eyes with glaucoma and Еx-PRESS® implant.Key words: glaucoma, surgical revision, glaucoma implants, Еx-PRESS®, OlogenTM.

1732013, Vol. 3, Issue 4
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
be used simultaneously:- Drug treatment – topical therapy with IOP lowering drugs.
Topical steroids application may also limit the severe fi brosis- Manual ocular massage- Laser suture lysis- Bleb needling (with or without antifi brotic agents)- Surgical revision (with or without antifi brotic agents)- Performing entirely new antiglaucoma surgery at a new
side or using antiglaucoma implants (with or without antifi brotic agents).
Even after perfectly performed surgery, sooner or later, additional procedures or interventions are necessary to improve the outcome or to cope with any complications. Such procedures are the manual ocular massage, bleb needling, additional application of antifi brotic agents, surgical revision, entirely new antiglaucoma surgery etc. In many cases surgical revision is the surgeon‘s most adequate choice.
PurposeTo perform a surgical revision with OlogenTM implantation,
due to a permanent IOP elevation, in eyes with glaucoma and Еx-PRESS® implant. To follow up the postoperative results.
Material and MethodsThree cases of patients with different glaucoma types
are presented - 61-year-old primary open angle glaucoma patient, a 33-year-old patient with glaucoma associated with Sturge-Weber syndrome and a 59-year-old primary open angle glaucoma patient.
Patients underwent routine ophthalmological examination, as well as ultrasound pachymetry (Ocuscan RxP, Alcon), optical coherence tomography (RTVue-100, Optovue), Heidelberg retinal tomography (HRT II, Soft. ver. 3.1.2., Heidelberg Engineering GmbH), standard automated computer perimetry performed with Humphrey Field Analyzer (HFA II; Carl Zeiss, Meditec, Dublin, CA, USA). All IOP measurements were made with a Goldmann tonometer.
One eye of each patient was previously operated for glaucoma with Ex-PRESS® Glaucoma Filtration Device implantation. After a different period of time, a bleb encapsulation was observed in two of the eyes and excessive fi brosis in the fi ltration area in one eye. There was a permanent IOP elevation (above the target IOP) in all eyes operated with Ex-PRESS®. In the eyes with bleb encapsulation we perform bleb needling several times, but with an unsatisfactory outcome.
Due to the permanent IOP elevation (above the target IOP) in all three eyes we performed a surgical revision with OlogenTM implantation under tenon and conjunctiva in the area of the scleral fl ap.
All surgical revision were carried out in a operating room from one surgeon. The OlogenTM used in each eye was 12.0 mm in diameter and 1.0 mm in height. All the patients signed an Informed consent form. Retrobulbar anesthesia was used. A
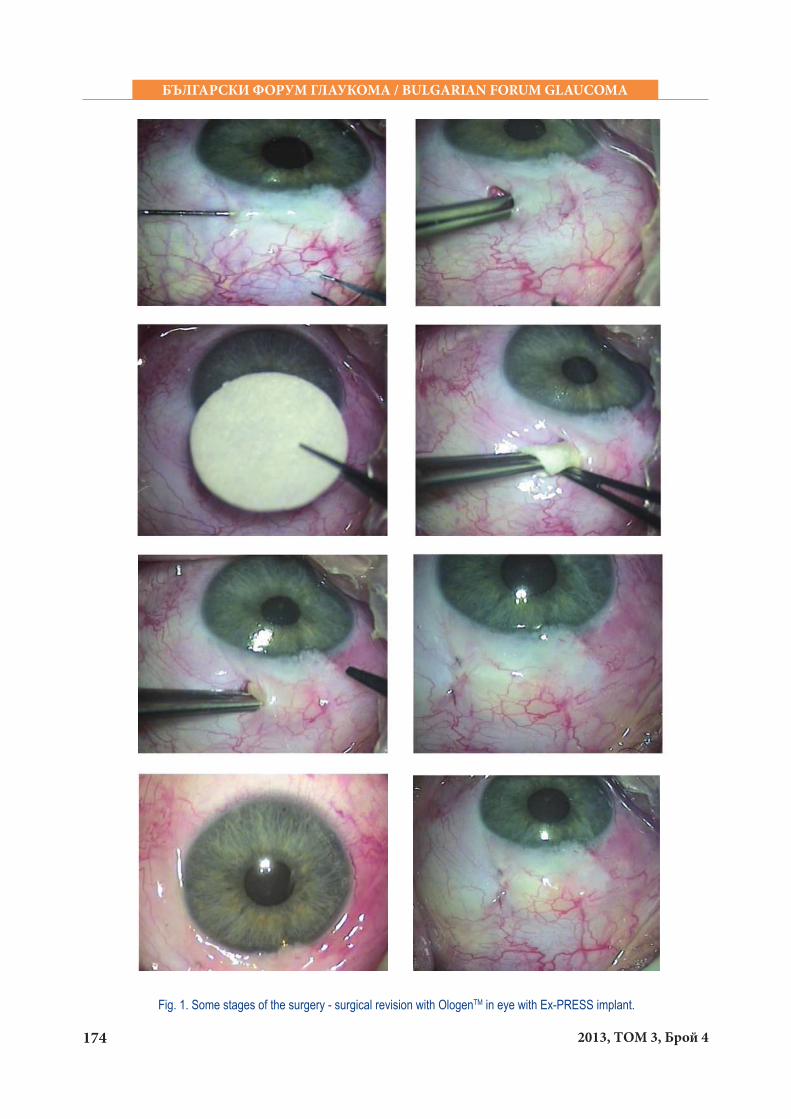
conjunctival and tenon incision was made. We perform a revision of the bleb with a needle before the OlogenTM implantation in the eyes with bleb encapsulation. Cauterization was not used. The OlogenTM was folded and placed under the tenon and conjunctiva in area of the scleral fl ap. Conjunctiva and tenon were sutured with 10-0. The main stages of the surgery are demonstrated on Figure 1.
Case - IA 33-year-old female patient diagnosed with glaucoma
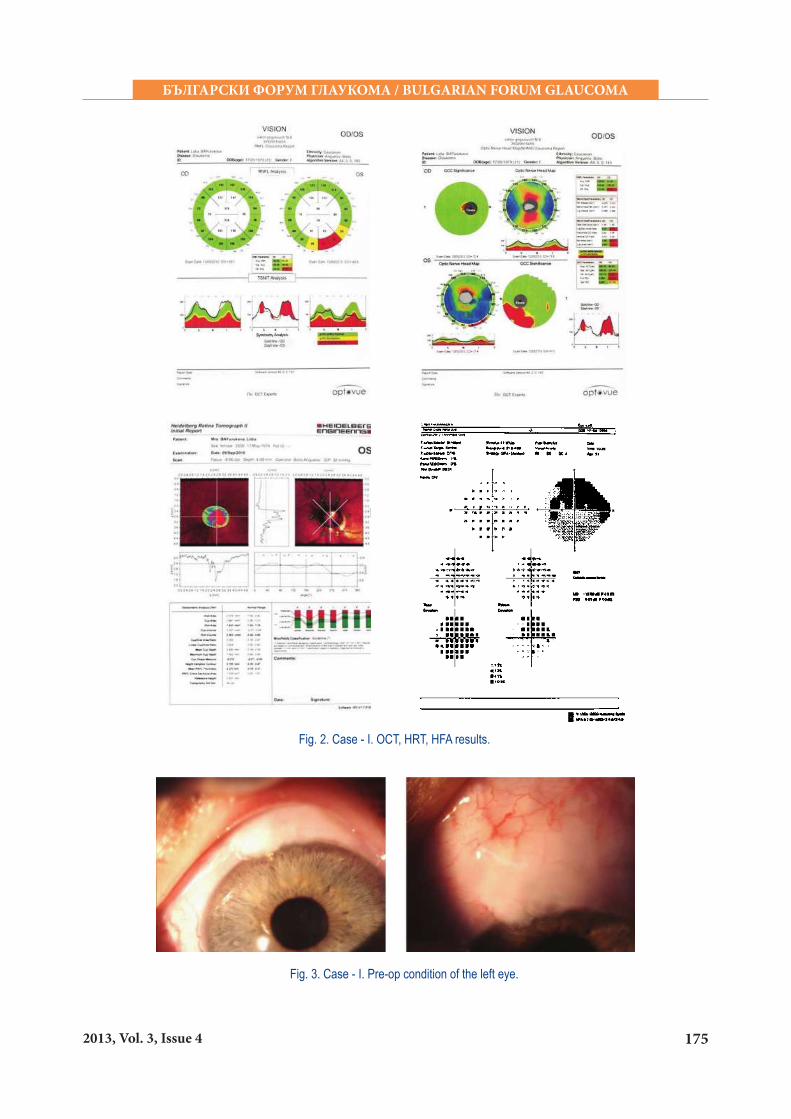
associated with Sturge-Weber syndrome. At the time she came to our glaucoma unit, she was installing 3 hypotensive medications on the left eye. The IOP of the left eye measured by Goldmann tonometer was 29 mmHg. Central corneal thickness of the left eye measured by ultrasound pachymeter was 551 μm (0). Best corrected visual acuity of the left eye was 20/40. Ophthalmoscopy showed asymmetry between the optic nerve heads of the eyes. Cup to disc ratio of the right eye was 0.5 with centered blood vessels, while the cup to disc ratio of the left eye was 0.8 with nasal displacement of the blood vessels and parapappilary atrophy. Gonioscopy proved open anterior chamber angle - Shaffer III degree.
OCT, HRT and HFA revealed glaucomatous structural and functional changes on the left eye (Fig. 2).
Taking into account the results of our ophthalmological examination, the glaucomatous changes revealed by OCT, HRT and HFA and the unsatisfactory results of the drug therapy, we perform an anti-glaucoma surgery on the left eye – an Ex-PRESS® implantation under a scleral fl ap.
Postoperative outcome was really good. For almost a year the IOPs of the operated left eye were between 11 and 16 mmHg without any IOP lowering medications. Unfortunately, a tendency for bleb encapsulation and IOP increase was observed. Bleb needling was performed several times but with short term effect.
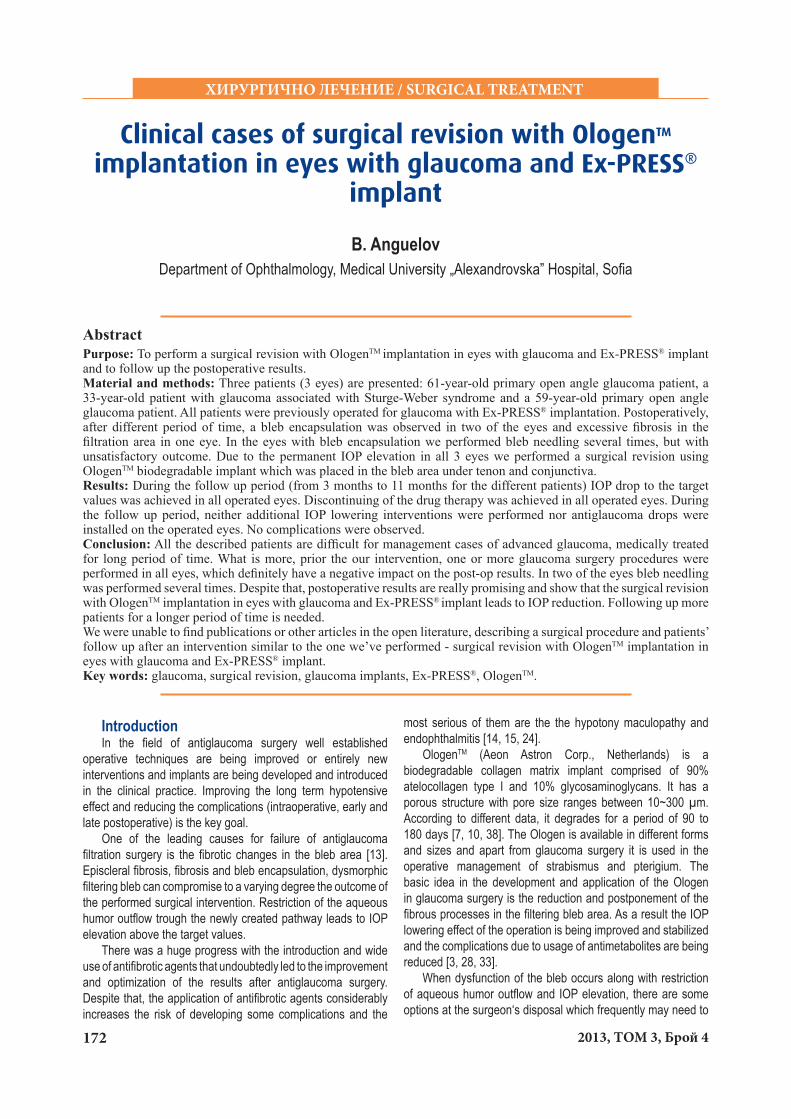
We decided that a surgical revision was needed. Pre-op the IOP of the left eye was 25 mmHg. A surgical revision on the left eye was performed with OlogenTM implantation in the bleb area, under tenon and conjunctiva. Figure 3 demonstrates the preoperative condition of the left eye. During the surgery and early post-op period no complications were observed.
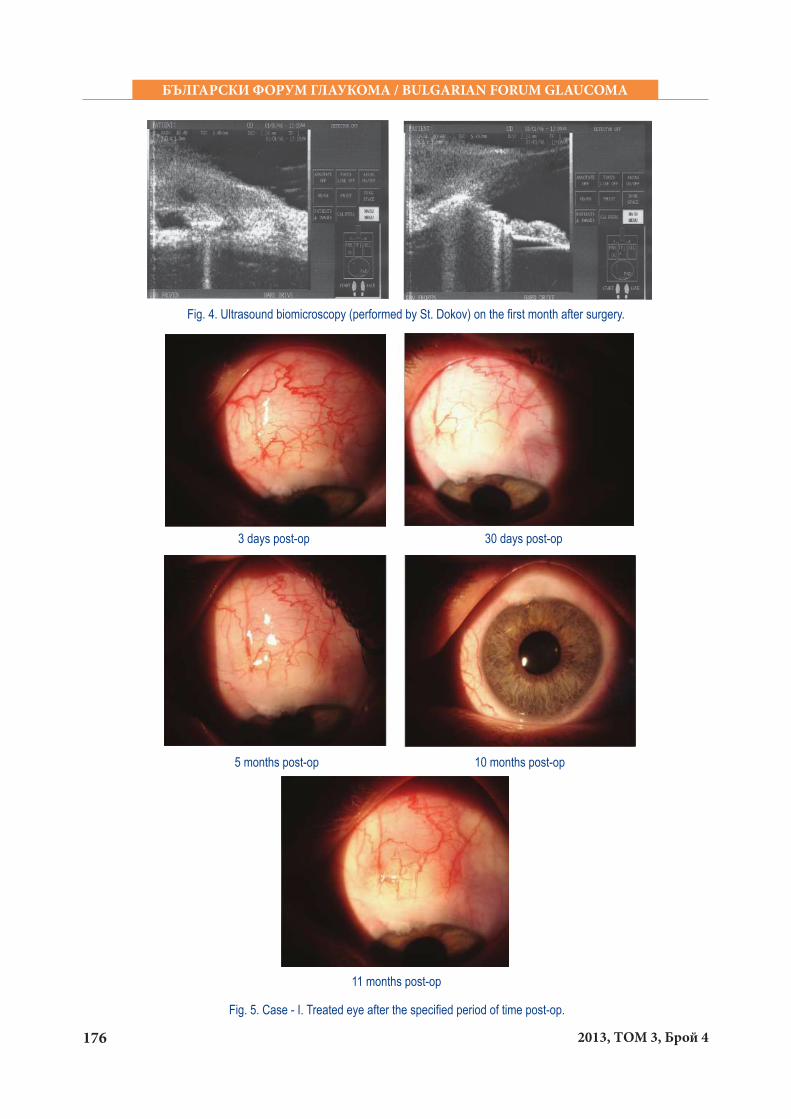
One day post-op the IOP of the treated eye was 13 mmHg. Thirty days post-op the IOP of the treated eye was 12 mmHg. Ultrasound biomicroscopy was performed and the two implants as well as the fi ltering bleb were visualized (Fig. 4).
Anterior segment photos of the treated eye after the specifi ed period of time post-op, are demonstrated on Figure 5. Eleven months post-op the IOP of the treated eye was 12 mmHg. On Table 1 the IOPs measured at the follow up visits are presented.
During the 11 months follow up period, neither additional IOP lowering interventions were performed nor antiglaucoma drops were installed on the operated eye.
174 2013, ТОМ 3, Брой 4
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
Fig. 1. Some stages of the surgery - surgical revision with OlogenTM in eye with Ex-PRESS implant.
1752013, Vol. 3, Issue 4
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
Fig. 2. Case - I. OCT, HRT, HFA results.
Fig. 3. Case - I. Pre-op condition of the left eye.
176 2013, ТОМ 3, Брой 4
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
Fig. 4. Ultrasound biomicroscopy (performed by St. Dokov) on the fi rst month after surgery.
10 months post-op
Fig. 5. Case - I. Treated eye after the specifi ed period of time post-op.
3 days post-op 30 days post-op
5 months post-op
11 months post-op
1772013, Vol. 3, Issue 4
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
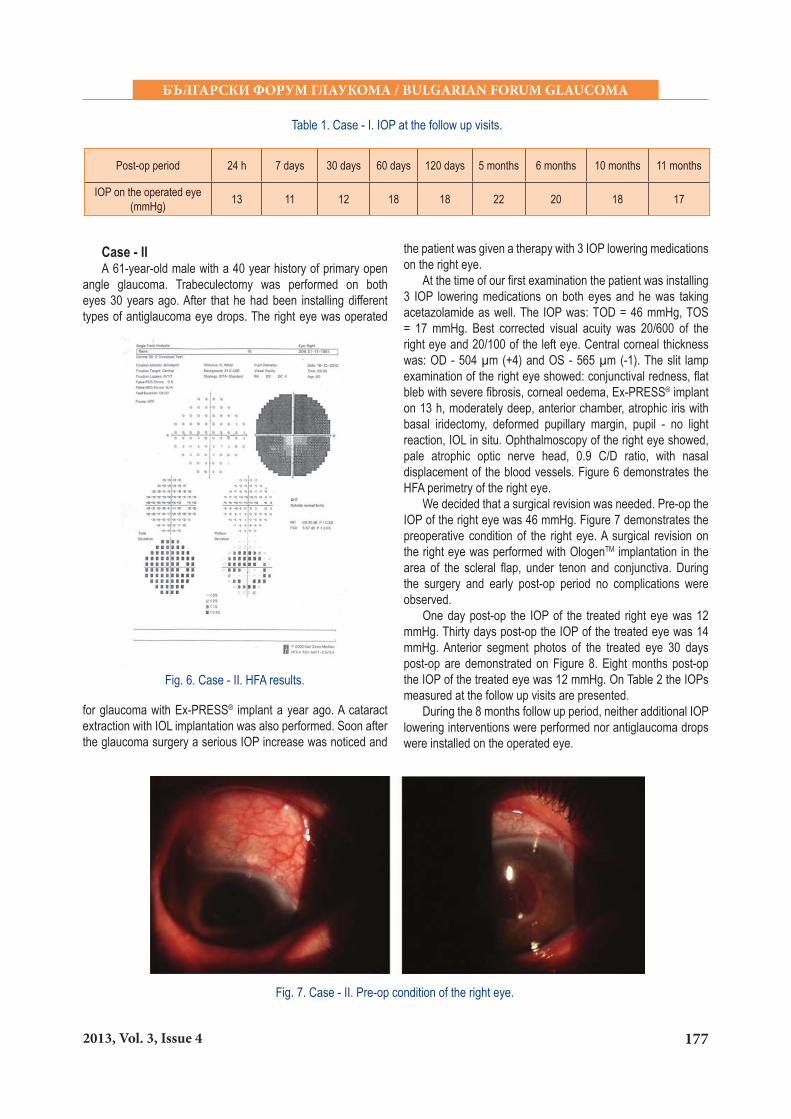
Case - IIА 61-year-old male with a 40 year history of primary open
angle glaucoma. Trabeculectomy was performed on both eyes 30 years ago. After that he had been installing different types of antiglaucoma eye drops. The right eye was operated
Fig. 6. Case - II. HFA results.
Fig. 7. Case - II. Pre-op condition of the right eye.
the patient was given a therapy with 3 IOP lowering medications on the right eye.
At the time of our fi rst examination the patient was installing 3 IOP lowering medications on both eyes and he was taking acetazolamide as well. The IOP was: TОD = 46 mmHg, TOS = 17 mmHg. Best corrected visual acuity was 20/600 of the right eye and 20/100 of the left eye. Central corneal thickness was: OD - 504 μm (+4) and OS - 565 μm (-1). The slit lamp examination of the right eye showed: conjunctival redness, fl at bleb with severe fi brosis, corneal oedema, Ex-PRESS® implant on 13 h, moderately deep, anterior chamber, аtrophic iris with basal iridectomy, deformed pupillary margin, pupil - no light reaction, IOL in situ. Ophthalmoscopy of the right eye showed, pale atrophic optic nerve head, 0.9 C/D ratio, with nasal displacement of the blood vessels. Figure 6 demonstrates the HFA perimetry of the right eye.
We decided that a surgical revision was needed. Pre-op the IOP of the right eye was 46 mmHg. Figure 7 demonstrates the preoperative condition of the right eye. A surgical revision on the right eye was performed with OlogenTM implantation in the area of the scleral fl ap, under tenon and conjunctiva. During the surgery and early post-op period no complications were observed.
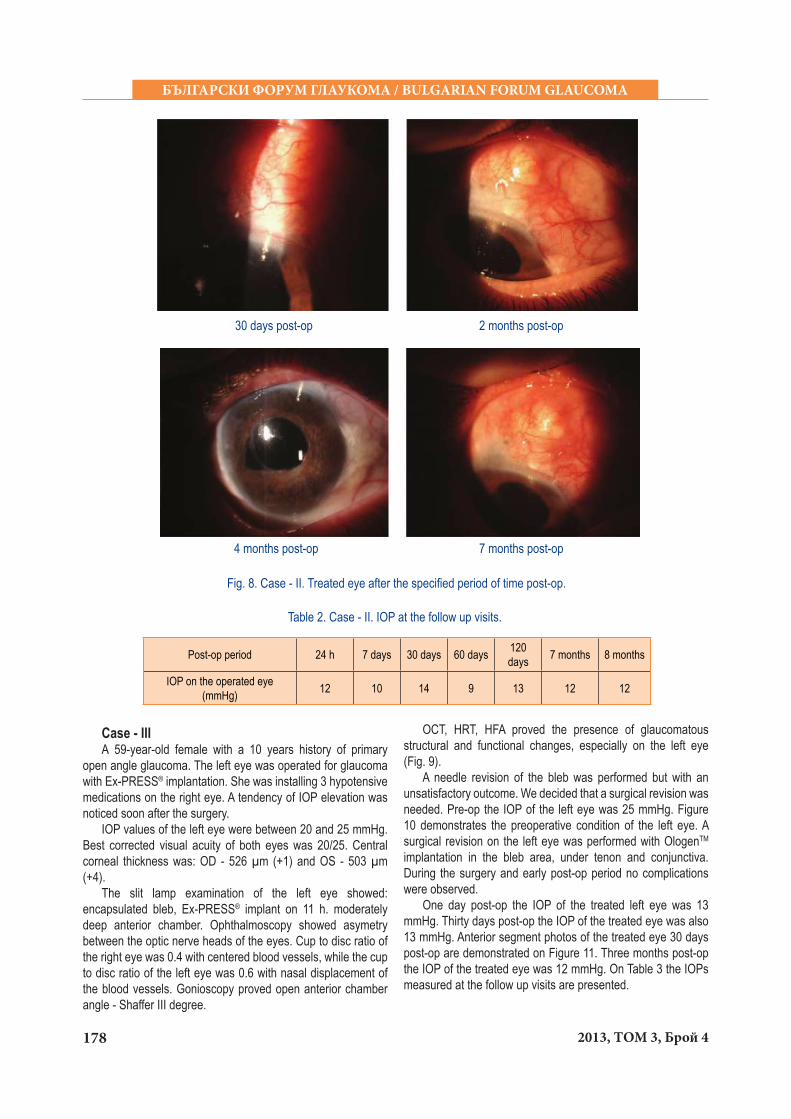
One day post-op the IOP of the treated right eye was 12 mmHg. Thirty days post-op the IOP of the treated eye was 14 mmHg. Anterior segment photos of the treated eye 30 days post-op are demonstrated on Figure 8. Eight months post-op the IOP of the treated eye was 12 mmHg. On Table 2 the IOPs measured at the follow up visits are presented.
During the 8 months follow up period, neither additional IOP lowering interventions were performed nor antiglaucoma drops were installed on the operated eye.
Post-op period 24 h 7 days 30 days 60 days 120 days 5 months 6 months 10 months 11 months
IOP on the operated eye (mmHg) 13 11 12 18 18 22 20 18 17
Table 1. Case - I. IOP at the follow up visits.
for glaucoma with Ex-PRESS® implant a year ago. A cataract extraction with IOL implantation was also performed. Soon after the glaucoma surgery a serious IOP increase was noticed and
178 2013, ТОМ 3, Брой 4
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
Case - IIIА 59-year-old female with a 10 years history of primary
open angle glaucoma. The left eye was operated for glaucoma with Ex-PRESS® implantation. She was installing 3 hypotensive medications on the right eye. A tendency of IOP elevation was noticed soon after the surgery.
IOP values of the left eye were between 20 and 25 mmHg. Best corrected visual acuity of both eyes was 20/25. Central corneal thickness was: OD - 526 μm (+1) and OS - 503 μm (+4).
The slit lamp examination of the left eye showed: encapsulated bleb, Ex-PRESS® implant on 11 h. moderately deep anterior chamber. Ophthalmoscopy showed asymetry between the optic nerve heads of the eyes. Cup to disc ratio of the right eye was 0.4 with centered blood vessels, while the cup to disc ratio of the left eye was 0.6 with nasal displacement of the blood vessels. Gonioscopy proved open anterior chamber angle - Shaffer III degree.
Fig. 8. Case - II. Treated eye after the specifi ed period of time post-op.
2 months post-op
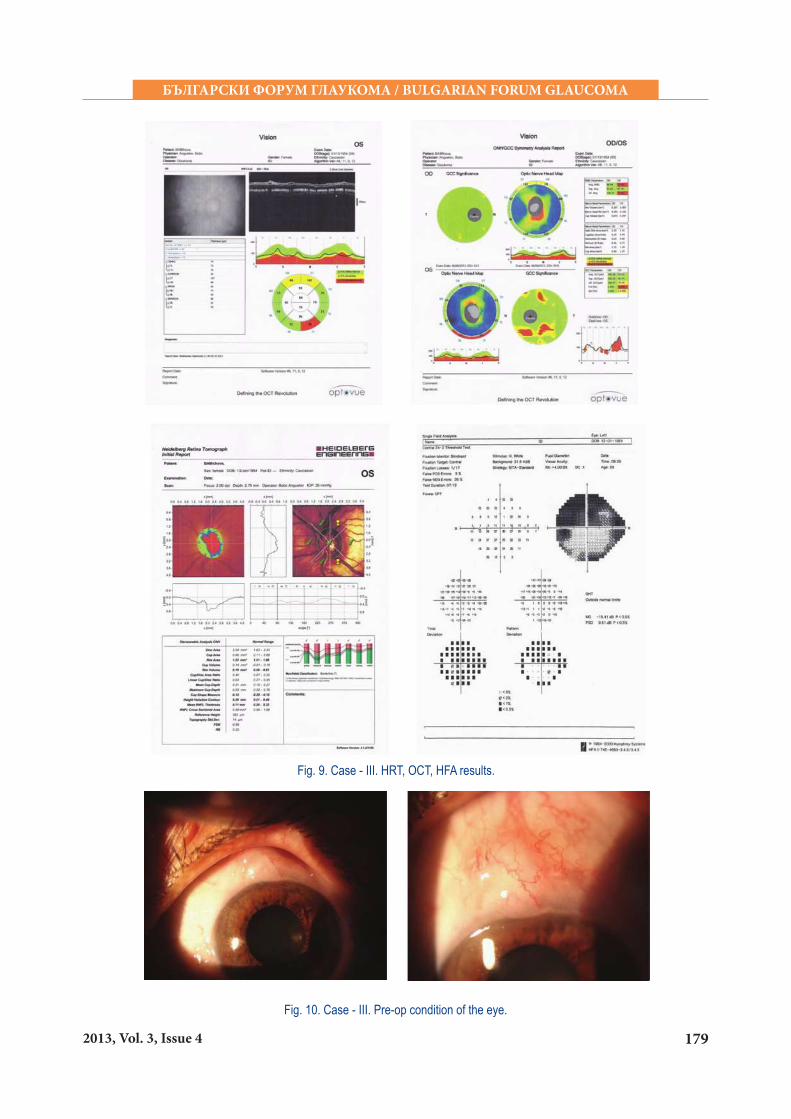
OCT, HRT, HFA proved the presence of glaucomatous structural and functional changes, especially on the left eye (Fig. 9).
A needle revision of the bleb was performed but with an unsatisfactory outcome. We decided that a surgical revision was needed. Pre-op the IOP of the left eye was 25 mmHg. Figure 10 demonstrates the preoperative condition of the left eye. A surgical revision on the left eye was performed with OlogenTM implantation in the bleb area, under tenon and conjunctiva. During the surgery and early post-op period no complications were observed.
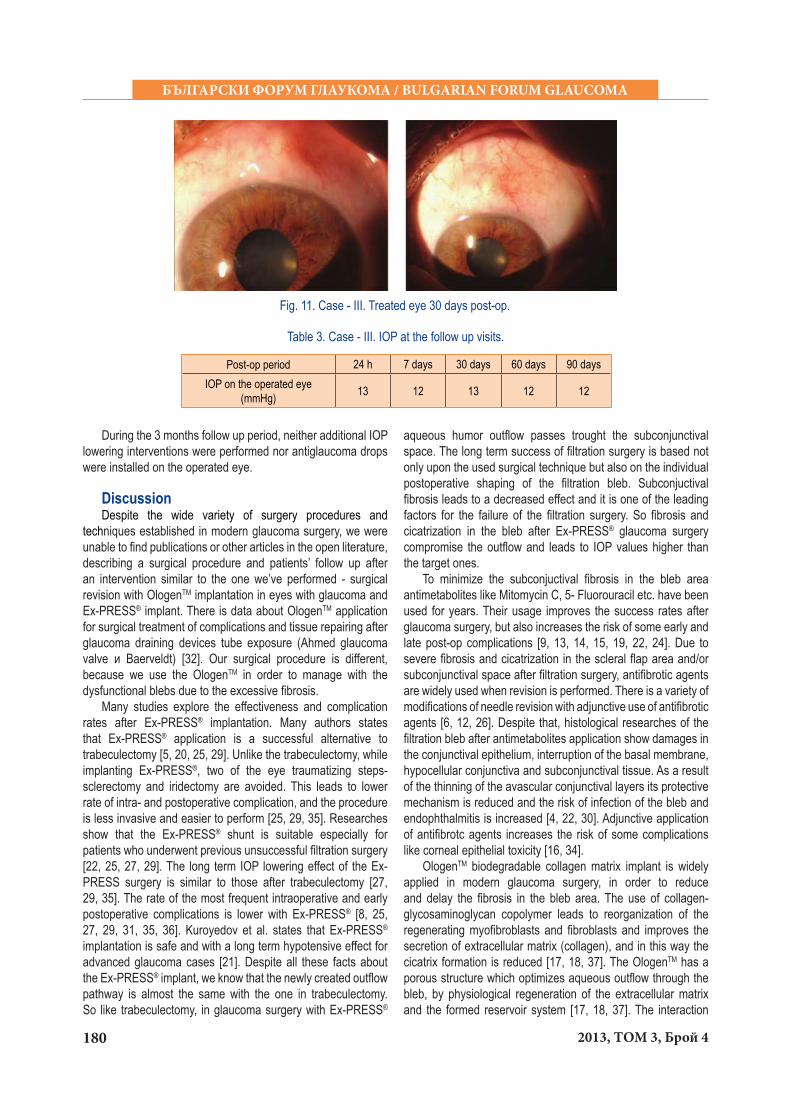
One day post-op the IOP of the treated left eye was 13 mmHg. Thirty days post-op the IOP of the treated eye was also 13 mmHg. Anterior segment photos of the treated eye 30 days post-op are demonstrated on Figure 11. Three months post-op the IOP of the treated eye was 12 mmHg. On Table 3 the IOPs measured at the follow up visits are presented.
Post-op period 24 h 7 days 30 days 60 days 120 days 7 months 8 months
IOP on the operated eye (mmHg) 12 10 14 9 13 12 12
Table 2. Case - II. IOP at the follow up visits.
30 days post-op
4 months post-op 7 months post-op
1792013, Vol. 3, Issue 4
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
Fig. 9. Case - III. HRT, OCT, HFA results.
Fig. 10. Case - III. Pre-op condition of the eye.
180 2013, ТОМ 3, Брой 4
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
Fig. 11. Case - III. Treated eye 30 days post-op.
During the 3 months follow up period, neither additional IOP lowering interventions were performed nor antiglaucoma drops were installed on the operated eye.
Discussion Despite the wide variety of surgery procedures and
techniques established in modern glaucoma surgery, we were unable to fi nd publications or other articles in the open literature, describing a surgical procedure and patients’ follow up after an intervention similar to the one we’ve performed - surgical revision with OlogenTM implantation in eyes with glaucoma and Еx-PRESS® implant. There is data about OlogenTM application for surgical treatment of complications and tissue repairing after glaucoma draining devices tube exposure (Аhmed glaucoma valve и Baerveldt) [32]. Our surgical procedure is different, because we use the OlogenTM in order to manage with the dysfunctional blebs due to the excessive fi brosis.
Many studies explore the effectiveness and complication rates after Ex-PRESS® implantation. Many authors states that Ex-PRESS® application is a successful alternative to trabeculectomy [5, 20, 25, 29]. Unlike the trabeculectomy, while implanting Ex-PRESS®, two of the eye traumatizing steps-sclerectomy and iridectomy are avoided. This leads to lower rate of intra- and postoperative complication, and the procedure is less invasive and easier to perform [25, 29, 35]. Researches show that the Ex-PRESS® shunt is suitable especially for patients who underwent previous unsuccessful fi ltration surgery [22, 25, 27, 29]. The long term IOP lowering effect of the Ex-PRESS surgery is similar to those after trabeculectomy [27, 29, 35]. The rate of the most frequent intraoperative and early postoperative complications is lower with Ex-PRESS® [8, 25, 27, 29, 31, 35, 36]. Kuroyedov et al. states that Ex-PRESS® implantation is safe and with a long term hypotensive effect for advanced glaucoma cases [21]. Despite all these facts about the Ex-PRESS® implant, we know that the newly created outfl ow pathway is almost the same with the one in trabeculectomy. So like trabeculectomy, in glaucoma surgery with Ex-PRESS®
aqueous humor outfl ow passes trought the subconjunctival space. The long term success of fi ltration surgery is based not only upon the used surgical technique but also on the individual postoperative shaping of the fi ltration bleb. Subconjuctival fi brosis leads to a decreased effect and it is one of the leading factors for the failure of the fi ltration surgery. So fi brosis and cicatrization in the bleb after Ex-PRESS® glaucoma surgery compromise the outfl ow and leads to IOP values higher than the target ones.
To minimize the subconjuctival fi brosis in the bleb area antimetabolites like Mitomycin C, 5- Fluorouracil etc. have been used for years. Their usage improves the success rates after glaucoma surgery, but also increases the risk of some early and late post-op complications [9, 13, 14, 15, 19, 22, 24]. Due to severe fi brosis and cicatrization in the scleral fl ap area and/or subconjunctival space after fi ltration surgery, antifi brotic agents are widely used when revision is performed. There is a variety of modifi cations of needle revision with adjunctive use of antifi brotic agents [6, 12, 26]. Despite that, histological researches of the fi ltration bleb after antimetabolites application show damages in the conjunctival epithelium, interruption of the basal membrane, hypocellular conjunctiva and subconjunctival tissue. As a result of the thinning of the avascular conjunctival layers its protective mechanism is reduced and the risk of infection of the bleb and endophthalmitis is increased [4, 22, 30]. Adjunctive application of antifi brotc agents increases the risk of some complications like corneal epithelial toxicity [16, 34].
OlogenTM biodegradable collagen matrix implant is widely applied in modern glaucoma surgery, in order to reduce and delay the fi brosis in the bleb area. The use of collagen-glycosaminoglycan copolymer leads to reorganization of the regenerating myofi broblasts and fi broblasts and improves the secretion of extracellular matrix (collagen), and in this way the cicatrix formation is reduced [17, 18, 37]. The OlogenTM has a porous structure which optimizes aqueous outfl ow through the bleb, by physiological regeneration of the extracellular matrix and the formed reservoir system [17, 18, 37]. The interaction
Table 3. Case - III. IOP at the follow up visits.
Post-op period 24 h 7 days 30 days 60 days 90 daysIOP on the operated eye
(mmHg) 13 12 13 12 12

1812013, Vol. 3, Issue 4
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
between the tissue and the collagenous matrix leads to a formation of a stable bleb structure.
Research results show that, OlogenTM is applied successfully in patients with different glaucoma types, including refractory ones [4]. Trabeculectomy with OlogenTM leads to a similar hypotensive effect. There are less post-op complications, and it is an effective and safer adequate alternative to trabeculectomy with MMC [11, 33]. OlogenTM is also used for phacotrabeculectomy in patients with cataract and primary open angle glaucoma [2]. It is also applied for surgical treatment of complications and tissue repairing after glaucoma draining devices tube exposure (Аhmed glaucoma valve и Baerveldt) [32].
Our experience shows that glaucoma surgery with Ex- PRESS® as well as with OlogenTM leads to improvement of postoperative outcome even in refractory glaucomas. The vast majority of our patients with Ex- PRESS® show permanent IOP lowering without additional interventions (needle revision, surgery revision etc.) or hypotensive drugs. However, in some cases, after a different period of time, severe fi brosis in the bleb area occurs, which inevitably leads to restriction of aqueous humor outfl ow and compromises the hypotensive effect of the intervention. In such cases we perform needling of the encapsulated bleb. When necessary, more than one needle revision is done. Some patients need only needle revision in order to achieve better outfl ow trough the fi ltration area. However the effect is often transitory. There is no doubt that frequent needle revision is risky. In some advanced glaucoma cases we perform single step implantation of both Ex-PRESS® and OlogenTM with a very good outcome Postoperative results are really promising with constant IOP lowering effect without additional interventions (needle revision, surgery revision etc.) or hypotensive drugs [1].
By performing surgical revision with OlogenTM implantation on patients with Ex- PRESS® we achieve some major goals:
- Disrupting of the scar tissue in the bleb area;- By Ologen application we modulate the wound healing
response and lower the risk of future excessive cicatrization; - Avoid the application of antimetabolites and so the
complications of their usage;- Improvement of aqueous outfl ow through the Ex- PRESS®
shunt and the bleb; - IOP lowering and discontinuing the antiglaucoma
medications.What is more, as a result of our procedure, in every eye
there are two different antiglaucoma implants with different mode of action. When discussing the postoperative results, we must have in mind that all the described patients are diffi cult for management cases of advanced glaucoma, medically treated for long period of time. What is more, prior to our intervention, one or more glaucoma surgery procedures were performed in all eyes, which defi nitely have negative impact on the post-op results.
ConclusionPostoperative results show that the surgical revision with
OlogenTM implantation in eyes with glaucoma and Еx-PRESS®
implant leads to IOP drop and discontinuing of the IOP lowering medications. The surgical approach we suggest could be a successful alternative to the other possible revision procedures after fi ltration surgery, especially to these where antimetabolites are applied. Following up more patients for a longer period of time is needed.
References:1. Anguelov B. Surgical treatment of some types of advanced glaucoma
with a single step implantation of two different implants - Ex-PRESS and Ologen. Bul F Glaucoma 2012; 2(4):4-17.
2. Anguelov B. Phacotrabeculectomy with absorbable suture of the scleral fl ap and subconjunctival biodegradable collagen matrix implant (OlogenTM) in eyes with a cataract and primary open angle glaucoma. Ref Bul Ophthalmol 2009; 6:17-26.
3. Anguelov B. Trabeculectomy with absorbable suture of the scleral fl ap and subconjunctival biodegradable collagen matrix implant (OlogenTM) in primary open angle glaucoma Ref Bul Ophthalmol 2010; 1:21-8.
4. Anguelov B. Trabeculectomy with absorbable suture of the scleral fl ap and subconjunctival biodegradable collagen matrix implant (OlogenTM) in refractory glaucoma. Ref Bul Ophthalmol 2009; 5:23-30.
5. Ahmed K. Ex-PRESS Mini glaucoma shunt: techniques and pearls. Clinical & surgical ophthalmology 2008; 26(9):306-10.
6. Anand N, Khan A. Long-term outcomes of needle revision of trabeculectomy blebs with mitomycin C and 5-fl uorouracil: a comparative safety and effi cacy report. J Glaucoma 2009 Sep; 18(7):513-20.
7. Aptel F, Dumas S, Denis P. Ultrasound biomicroscopy and optical coherence tomography imaging of fi ltering blebs after deep sclerectomy with new collagen implant. Eur J Ophthalmol 2009; 19:223-30.
8. Beltran-Agullo L, Trope GE, Jin Y, Wagschal LD, Jinapriya D, Buys YM. Comparison of visual recovery following ex-press versus trabeculectomy: Results of a Prospective Randomized Controlled Trial. J Glaucoma 2013 Jun 25. [Epub ahead of print]
9. Bindlish R, Condon GP, Schlosser JD, D‘Antonio J, Lauer KB, Lehrer R. Effi cacy and safety of mitomycin-C in primary trabeculectomy: fi ve-year follow-up. Ophthalmology 2002 Jul; 109(7):1336-41.
10. Boey PY, Narayanaswamy A, Zheng C, Perera SA, Htoon HM, Tun TA, Seah SK, Wong TT, Aung T. Imaging of blebs after phacotrabeculectomy with Ologen collagen matrix implants. Br J Ophthalmol 2011 Mar; 95(3):340-4.
11. Cillino S, Di Pace F, Cillino G, Casuccio A. Biodegradable collagen matrix implant vs mitomycin-C as an adjuvant in trabeculectomy: a 24-month, randomized clinical trial. Eye (Lond) 2011 Dec; 25(12):1598-606.
12. Dalvi R, Orzech N, Kranemann C, Birt CM. Five-year results of 5-fl uorouracil augmented needling revision of failing blebs. Ophthalmic Surg Lasers Imaging. 2012 Jan-Feb; 43(1):32-8.
13. DeBry PW, Perkins TW, Heatley G, Kaufman P, Brumback LC. Incidence of late-onset bleb-related complications following trabeculectomy with mitomycin. Arch Ophthalmol 2002; 120:297-300.
14. Gedde SJ, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, Schiffman JC. Surgical complications in the Tube Versus Trabeculectomy Study during the fi rst year of follow-up. Am J Ophthalmol 2007; 143:23-31.
15. Greenfi eld DS, Suñer IJ, Miller MP, Kangas TA, Palmberg PF, Flynn HW Jr. Endophthalmitis after fi ltering surgery with mitomycin. Arch Ophthalmol 1996; 114:943-9.
16. Hodge W, Saheb N, Balazsi G, Kasner O. Treatment of encapsulated blebs with 30-gauge needling and injection of low-dose 5-fl uorouracil. Can J Ophthalmol 1992; 27:233-6.
17. Hsu W-C, Ritch R, Krupin T, Chen HS-L. Tissue bioengineering for surgical bleb defects: an animal study. Graefes Arch Clin Exp Ophthalmol 2008; 246:709-17.
18. Hsu WC, Spilker MH, Yannas IV, Rubin PA. Inhibition of conjunctival scarring and contraction by a porous collagen-glycosaminoglycan implant. Invest Ophthalmol Vis Sci 2000 Aug; 41(9):2404-11.
19. Hu CY, Matsuo H, Tomita G, Suzuki Y, Araie M, Shirato S, Tanaka S. Clinical characteristics and leakage of functioning blebs after

182 2013, ТОМ 3, Брой 4
БЪЛГАРСКИ ФОРУМ ГЛАУКОМА / BULGARIAN FORUM GLAUCOMA
trabeculectomy with mitomycin-C in primary glaucoma patients. Ophthalmology. 2003 Feb; 110(2):345-52.
20. Jong L, Lafuma A, Aguadé AS, Berdeaux G. Five-year extension of a clinical trial comparing the EX-PRESS glaucoma fi ltration device and trabeculectomy in primary open-angle glaucoma. Clin Ophthalmol 2011; 5:527-33.
21. Kuroyedov A, Ogorodnikova V. A long-term period of observation of patients with advanced glaucoma after implantation of Ex-PRESS glaucoma fi ltration device. Bul F Glaucoma 2012; 2(2):15-21.
22. Lama PJ, Fechtner RD. Antifi brotics and wound healing in glaucoma surgery. Surv Ophthalmol 2003 May-Jun; 48(3):314-46.
23. Lankaranian D, Razeghinejad MR, Prasad A, Fakhraie G, Freitas DJ, Ichhpujani P, Moster MR. Intermediate-term results of the Ex-PRESS® miniature glaucoma implant under a scleral fl ap in previously operated eyes. Clin Experiment Ophthalmol 2011 Jul; 39(5):421-8.
24. Law SK, Nguyen AM, Coleman AL, Caprioli J. Severe loss of central vision in patients with advanced glaucoma undergoing trabeculectomy. Arch Ophthalmol 2007; 125:1044-55.
25. Long LA. The Ex-PRESS glaucoma shunt versus trabeculectomy in open-angle glaucoma: a prospective randomized study. Adv Ther March 2009; 26(3):336-45.
26. Maestrini HA, Cronemberger S, Matoso HD, Reis JR, Mérula RV, Filho AD, Sakurai E, Ferreira GA. Late needling of fl at fi ltering blebs with adjunctive mitomycin C: effi cacy and safety for the corneal endothelium. Ophthalmology 2011 Apr;118(4):755-62.
27. Maris PJ, Smith ME, Netland PA. Clinical outcomes with the Ex-PRESS miniature glaucoma implant. Invest Ophthalmol Vis Sci 2005; 46.
28. Papaconstantinou D, Georgalas I, Karmiris E, Diagourtas A, Koutsandrea C, Ladas I, Apostolopoulos M, Georgopoulos G. Trabeculectomy with ologen versus trabeculectomy for the treatment
of glaucoma: a pilot study. Acta Ophthalmol 2010; 88:80-5.29. Peter J, Maris G, Ishida K, Netland A. Comparison of trabeculectomy
with Ex-PRESS miniature glaucoma device implanted under scleral fl ap. J Glaucoma 2007; 16:14-9.
30. Poulsen EJ, Allingham RR. Characteristics and risk factors of infections after glaucoma fi ltering surgery. J Glaucoma 2000 Dec; 9(6):438-43.
31. Reinthal EK, Rohrbach JM, Grisanti S. Glaucoma drainage implants. Klin Monbl Augenheilkd Jan 2010; 227(1):49-55.
32. Rosentreter A, Schild AM, Dinslage S, Dietlein TS. Biodegradable implant for tissue repair after glaucoma drainage device surgery. J Glaucoma 2012 Feb; 21(2):76-8.
33. Rosentreter A, Schild AM, Jordan JF, Krieglstein GK, Dietlein TS. A prospective randomised trial of trabeculectomy using mitomycin C vs an ologen implant in open angle glaucoma. Eye 2010; 24:1449-57.
34. Shin DH, Kim YY, Ginde SY, Kim PH, Eliassi-Rad B, Khatana AK, et al. Risk factors for failure of 5-fl uorouracil needling revision for failed conjunctival fi ltration blebs. Am J Ophthalmol 2001; 132:875-80.
35. Wamsley S, Moster MR, Rai S, Alvim HS, Fontanarosa J. Results of the use of the Ex-PRESS miniature glaucoma implant in technically challenging, advanced glaucoma cases: a clinical pilot study. Am J Ophthalmol Dec 2004; 138(6):1049-51.
36. Wang W, Zhou M, Huang W, Zhang X. Ex-PRESS implantation versus trabeculectomy in uncontrolled glaucoma: a meta-analysis. PLoS One 2013 May 31; 8(5):e63591.
37. Young MJ, Borrás T, Walter M, Ritch R. Tissue bioengineering: potential applications to glaucoma. Arch Ophthalmol 2005 Dec; 123(12):1725-31.
38. Zelefsky JR, Hsu WC, Ritch R. Biodegradable collagen matrix implant for trabeculectomy. Expert Rev Ophthalmol 2008; 3:613-7.

























![Effect of Preoperative Intravitreal Bevacizumab on the ... · without loss of light perception (LP), and with or without the use of antiglaucoma medication [12]. Surgical failure](https://img.pdfslide.net/doc/110x75/608df9a17225244145645e0a/effect-of-preoperative-intravitreal-bevacizumab-on-the-without-loss-of-light.jpg)



