Embed Size (px)
Citation preview

1
Public Health, Innovation and Intellectual Property
Global Platform on Innovation and Access
Request for Proposals (RFP)
WHO Bid Reference: GPIA 2013

2
TABLE OF CONTENTS
TABLE OF CONTENTS ............................................................................................................................... 2
1. INTRODUCTION ................................................................................................................................ 4 1.1 Objective of the RFP ......................................................................................................... 4 1.2 About WHO ........................................................................................................................ 4
1.2.1 WHO Mission Statement .................................................................................... 4 1.2.2 Structure of WHO ............................................................................................... 4 1.2.3 Description of Cluster/Service/Unit ..................................................................... 5
1.3 Definitions, Acronyms and Abbreviations ..................................................................... 5
2. DESCRIPTION OF PROJECT ........................................................................................................... 6 2.1 Overview ............................................................................................................................ 6 2.2 Objectives of the project .................................................................................................. 6 2.3 Existing resources ............................................................................................................ 7
3. REQUIREMENTS ............................................................................................................................... 8 3.1 Characteristics of the provider ....................................................................................... 8
3.1.1 Status ................................................................................................................. 8 3.1.2 Previous experience ........................................................................................... 8 3.1.3 Logistical and staffing capacity ........................................................................... 8
3.2 Work to be performed ...................................................................................................... 8 3.2.1 General requirements ......................................................................................... 8 3.2.2 Technical requirements .................................................................................... 11 3.2.3 Reporting requirements .................................................................................... 13 3.2.4 Performance monitoring ................................................................................... 13 3.2.5 Further Capacities ............................................................................................ 13
4. DELIVERABLES, TIME FRAME AND BUDGET ............................................................................ 14 4.1 Deliverables ..................................................................................................................... 14 4.2 Timeline* .......................................................................................................................... 15 4.3 Budget 15
5. INSTRUCTIONS TO BIDDERS ....................................................................................................... 16 5.1 Language of the Proposal and other Documents ....................................................... 16 5.2 Cost of Proposal ............................................................................................................. 16 5.3 Communications during the Call Period ...................................................................... 16 5.4 Period of Validity of Proposals ..................................................................................... 16 5.5 Closing Date for Submission of Proposals .................................................................. 16 5.6 Amendment of the Call ................................................................................................... 17 5.7 Clarification of Proposals .............................................................................................. 17
6. AWARD OF CONTRACT ................................................................................................................. 18 6.1 Award Criteria, Award of Contract ................................................................................ 18 6.2 WHO's Right to modify Scope or Requirements during the Evaluation/Selection Process 18 6.3 WHO's Right to Extend/Revise Scope or Requirements at Time of Award .............. 18 6.4 WHO's Right to enter into Negotiations ....................................................................... 18 6.5 Signing of the Contract .................................................................................................. 18
7. GENERAL AND CONTRACTUAL CONDITIONS ........................................................................... 20 7.1 Conditions of Contract ................................................................................................... 20 7.2 Responsibility ................................................................................................................. 20 7.3 Source of Instructions .................................................................................................... 21 7.4 Warranties ....................................................................................................................... 21 7.5 Legal Status .................................................................................................................... 21 7.6 Relation Between the Parties ........................................................................................ 22 7.7 No Waiver ........................................................................................................................ 22 7.8 Liability ............................................................................................................................ 22
3
7.9 Assignment ..................................................................................................................... 22 7.10 Officials not to Benefit ................................................................................................... 22 7.11 Indemnification ............................................................................................................... 22 7.12 Contractor's Responsibility for Employees ................................................................. 23 7.13 Subcontracting ............................................................................................................... 23 7.14 Place of Performance ..................................................................................................... 23 7.15 Language ......................................................................................................................... 23 7.16 Confidentiality ................................................................................................................. 23 7.17 Title Rights ...................................................................................................................... 24 7.18 Termination and Cancellation ....................................................................................... 24 7.19 Force Majeure ................................................................................................................. 24 7.20 Surviving Provisions ...................................................................................................... 25 7.21 Use of WHO name and emblem .................................................................................... 25 7.22 Successors and Assignees ........................................................................................... 25 7.23 Payment ........................................................................................................................... 25 7.24 Title to Equipment .......................................................................................................... 25 7.25 Insurance and Liabilities to Third Parties .................................................................... 26 7.26 Settlement of Disputes ................................................................................................... 26 7.27 Observance of Laws ....................................................................................................... 26 7.28 Authority to Modify ......................................................................................................... 26 7.29 Privileges and Immunities ............................................................................................. 26 7.30 No Terrorism or Corruption ........................................................................................... 27
8. PERSONNEL ................................................................................................................................... 27 8.1 Approval of Contractor Personnel ................................................................................ 27 8.2 Project Managers ............................................................................................................ 28 8.3 Foreign Nationals ........................................................................................................... 28 8.4 Compliance with WHO’s Policies .................................................................................. 28 8.5 Ethical Behaviour ........................................................................................................... 28 8.6 Engagement of Third Parties and use of In-house Resources .................................. 28
9. ANNEX 1: NATIONAL ASSESSMENT TOOL FOR GSPA-PHI ..................................................... 30
10. ANNEX 2: NATIONAL ASSESSMENT TOOL DIVIDED INTO SECTIONS AND SUB-SECTIONS WITH INDICATORS AND MATCH WITH PCP .................................................................................................... 37
11. ANNEX 3: APPROVED PROGRESS INDICATORS....................................................................... 50
12. ANNEX 4: SECTIONS AND SUB-SECTIONS OF INDICATORS LISTED IN ANNEX 2 ............... 52
ANNEX 5: EXAMPLES OF HIGH LEVEL REQUIREMENTS ................................................................... 53
4
1. INTRODUCTION
1.1 Objective of the RFP The purpose of this Request for Proposals (RFP) is to enter into a contractual agreement with a successful bidder and select a suitable contractor to carry out the following work: Building the Global Platform on Innovation and Access, an on-line portal that helps to monitor the progress of the implementation of the Global Strategy and Plan of Action on Public Health, Innovation and Intellectual Property (GSPA-PHI) by Member States and other stakeholders, collecting information on innovation and access to medical products and technologies. This document aims to:
Establish scope of the project;
Identify the general and technical requirements of the Global Platform;
Establish timeframe for the implementation of the project;
Establish expectation on deliverables, duration and on-going support services. The World Health Organization (WHO) is an organization that is dependent on the budgetary and extra-budgetary contributions it receives for the implementation of its activities. Bidders are therefore requested to propose the best and most cost-effective solution to meet WHO requirements, while ensuring a high level of service.
1.2 About WHO
1.2.1 WHO Mission Statement
The WHO was established in 1948 as a specialized agency of the United Nations. The objective of WHO (www.who.int) is the attainment by all peoples of the highest possible level of health. Health, as defined in the WHO Constitution, is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. WHO's main function is to act as the directing and coordinating authority on international health work.
1.2.2 Structure of WHO
The World Health Assembly (WHA) is the main governing body of WHO. It generally meets in Geneva in May of each year and is composed of delegations representing all 194 Member States. Its main function is to determine the policies of the Organization. In addition to its public health functions, the Health Assembly appoints the Director-General, supervises the financial policies of the Organization, and reviews and approves the proposed programme budget. It also considers reports of the WHO Executive Board, which it instructs with regard to matters upon which further action, study, investigation or report may be required. The Executive Board is composed of 34 members elected for three-year terms. The main functions of the Board are to give effect to the decisions and policies of the WHA, to advise it and generally to facilitate its work. The Board normally meets twice a year; one meeting is usually in January, and the second is in May, following the World Health Assembly. The WHO Secretariat consists of some 8,300 health and other officers at the Organization's headquarters in Geneva, in the six regional offices and in countries. The Secretariat is headed by the Director-General, who is appointed by the WHA on the nomination of the Executive Board. The current Director-General is Dr Margaret Chan. The head of each regional office is a Regional Director. Regional directors are appointed by the Executive Board in agreement with the relevant regional committees.

5
1.2.3 Description of Cluster/Service/Unit WHO’s Health Systems and Innovation Cluster (HIS) has the mission to provide information, evidence and guidance to Member States and other stakeholders to support evidence-informed decision-making to strengthen health systems for better health outcomes. Within the HIS cluster, the Department of Public Health, Innovation and Intellectual Property (PHI) is responsible for the interface between public health, innovation, research, transfer of technology and intellectual property. PHI is also the knowledge centre for health-related intellectual property and trade issues.
1.3 Definitions, Acronyms and Abbreviations
Acronym
GSPA-PHI Global Strategy and Plan of Action on Public Health, Innovation and Intellectual Property
RFP Request for Proposal
HIS Health Systems and Innovation Cluster
PHI Department of Public Health, Innovation and Intellectual Property
WHA World Health Assembly
PAHO Pan American Health Organization
PCP Pharmaceutical Country Profiles
EMP Department of Essential Medicines and Pharmaceutical Policies
6
2. DESCRIPTION OF PROJECT
2.1 Overview One of the main tasks of PHI is to coordinate the implementation of the GSPA-PHI. The GSPA-PHI was initially adopted by the 61st World Health Assembly (WHA61.21) and finalized by the 62nd World Health Assembly (WHA62.16)1,2. GSPA-PHI is a medium term plan (2008-2015) that aims to promote innovation, improve access, build capacity, and mobilize resources. The eight elements of the GSPA-PHI are:
1. Prioritizing research and development needs 2. Promoting research and development 3. Building and improving innovative capacity 4. Transfer technology 5. Application and management of intellectual property to contribute to innovation and promote public
health 6. Improving delivery and access 7. Promoting sustainable financing mechanisms 8. Establishing monitoring and reporting systems
WHA Resolution 61.21 requires WHO to establish monitoring and reporting systems in order to track the implementation of GSPA-PHI and report back to WHO governing bodies on the progress made. The Global Platform on Innovation and Access is to respond to this request. It aims to provide governments and other stakeholders with a user-friendly and reliable platform to manage and share information on national health innovation systems, access to health products and technologies, and activities to implement GSPA-PHI on an on-going basis. Additional objectives of the platform include:
1. Facilitate interaction between stakeholders within the innovation and access domains; 2. Create effective linkages between an array of interdependent processes and amongst various
stakeholders; 3. Offer a series of virtual tools that promote and support innovation, access, and governance in the
area of medical products and technologies. In 2012, the Pan American Health Organization (PAHO) launched the Regional Platform for Access and Innovation on Health Technologies 3 (referred to as the “PAHO Regional Platform” in this document). This PAHO Regional Platform will serve as a template for the Global Platform. The Global Platform will be developed on the foundation of some features and functionalities of the PAHO Regional Platform. This will be achieved by linking the two platforms for an automatic exchange of compatible data and information, making measurement indicators available to both platform users.
2.2 Objectives of the project The platform will help to monitor the progress of the GSPA-PHI’s implementation by Member States and other stakeholders against the eight elements mentioned in section 2.1. The Global Platform aims to:
1. Provide a tool to upload, store, report on and visualize the relevant information on implementation activities undertaken by national institutions and organizations, giving the possibility to Member States to share progress in implementation and difficulties faced;
2. Ensure consistency and avoid duplication in reporting mechanisms from Member States to the WHO;
1 WHA61.21 and Annex, WHA61/2008/REC/1. < http://apps.who.int/gb/e/e_wha61.html>
2 WHA62.16 and WHA62/2009/REC/1. <http://apps.who.int/gb/e/e_wha62.html>
3 Regional Platform for Access and Innovation on Health Technologies. <http://prais.paho.org/rscpaho/ >
7
3. Be a global reference point for relevant legislation, policies, and other documentation on innovation and access in medical products and technologies;
4. Provide updates on the activities implemented by the WHO in the area of innovation and access to medical products and technologies;
5. Provide a resource section on technology transfer and local production including reports, links and documents;
6. Allow for discussion between users through a forum and a pool of practices and web tools on issues relevant to innovation and access to health products for diseases disproportionally affecting developing countries.
2.3 Existing resources Data sources The main data source for the Global Platform will be the data derived from the National Assessment Tool for GSPA-PHI (Annex 1). The selected vendor will develop a data upload interface that follows the indicators of the National Assessment Tool. Before asking Member States to fill out every question asked by the assessment tool, available data sources at the WHO will be utilized to pre-fill the questionnaire. The most relevant data source from the WHO is the Pharmaceutical Country Profiles (PCP) conducted by the Department of Essential Medicines and Pharmaceutical Policies (EMP). Currently, the PCP database is in the form of a Microsoft Excel spread sheet, part of which will be uploaded to the Platform. The parts of the PCP that match the indicators of the assessment tool are indicated in Annex 2 as well as the input format required in the database. For most indicators, a single record will need to be stored for each year and historical data should be maintained to allow for temporal visualizations, for instance seeing the evolution of the number of countries with a policy on health research and development over time year by year. An audit trail should also be maintained, and certain fields may be defined to have more than one data point per year. Additionally, certain fields, such as the list of collaborating centres in a country, will need to be linked to existing internal WHO databases, perhaps by XML and updating at a consistent interval. The PAHO Regional Platform The PAHO Regional Platform launched in 2012, serves as a template for the Global Platform. PAHO has agreed to share its data sources and structure so that the Global Platform can build on the features and functionalities of the PAHO Regional Platform. A direct data interchange needs to be established between the Regional and the Global Platform so that the two platforms are synchronized. In Annex 2, the matched data fields can be found in the column “Match with PAHO”. Whenever there is an update on one platform, the changes should be reflected on the other one automatically.
8
3. REQUIREMENTS
3.1 Characteristics of the provider
3.1.1 Status
The service provider shall be a for-profit or not-for-profit institution operating in the field of technological innovation, with proven expertise in the design and development of software/IT solutions for strategic management of information and knowledge.
3.1.2 Previous experience
Previous work with WHO, PAHO, other international organizations, and/or major institutions in the field of information sharing, data management, and platform design is desirable.
3.1.3 Logistical and staffing capacity
The service provider should have adequate logistical and staffing capacity to deliver the agreed deliverables within the timeframe requested.
3.2 Work to be performed
3.2.1 General requirements
The Global Platform will be a system that brings multiple tools together such as the National Assessment Tool, the PCP and the PAHO Regional Platform. Thus, its design and functionality should allow for adding and supporting these tools. Furthermore, the technology should be agile enough to add new data and tools, if required. It is a mechanism to:
Develop a knowledge base;
Share relevant resources and information;
Facilitate technical cooperation between different stakeholders including WHO Member States and relevant departments in the WHO;
Link the results of the work of several parts of the WHO that are engaged in the area of access to medical products and technologies under the same framework;
Be a central resource section on technology transfer and local production including reports, links and documents
Raise awareness on key issues and priorities regarding innovation and access. The long-term vision of the Global Platform is to help monitor progress in the implementation of the GSPA-PHI by Member States and other stakeholders. It will be built by the integration of three main components:
1. Information hub 2. Knowledge repository (Basic text search, text interpretation desired but not required) 3. Virtual forum on innovation
Key components of the Information Hub include:
1. The interface of the Global Platform (the “empty box”), set up in order to accommodate
expansions at later stages
9
2. The data/information uploading tool based on the assessment tool/questionnaire (and upload of
the assessment results that have already been conducted)
3. Data linkages to existing internal WHO databases for certain fields such as list of collaborating
centres in a country (indicated in Annex 2)
4. The linkage to the PAHO Regional Platform to automatically synchronize and share data between
the 2 platforms
More details are provided below.
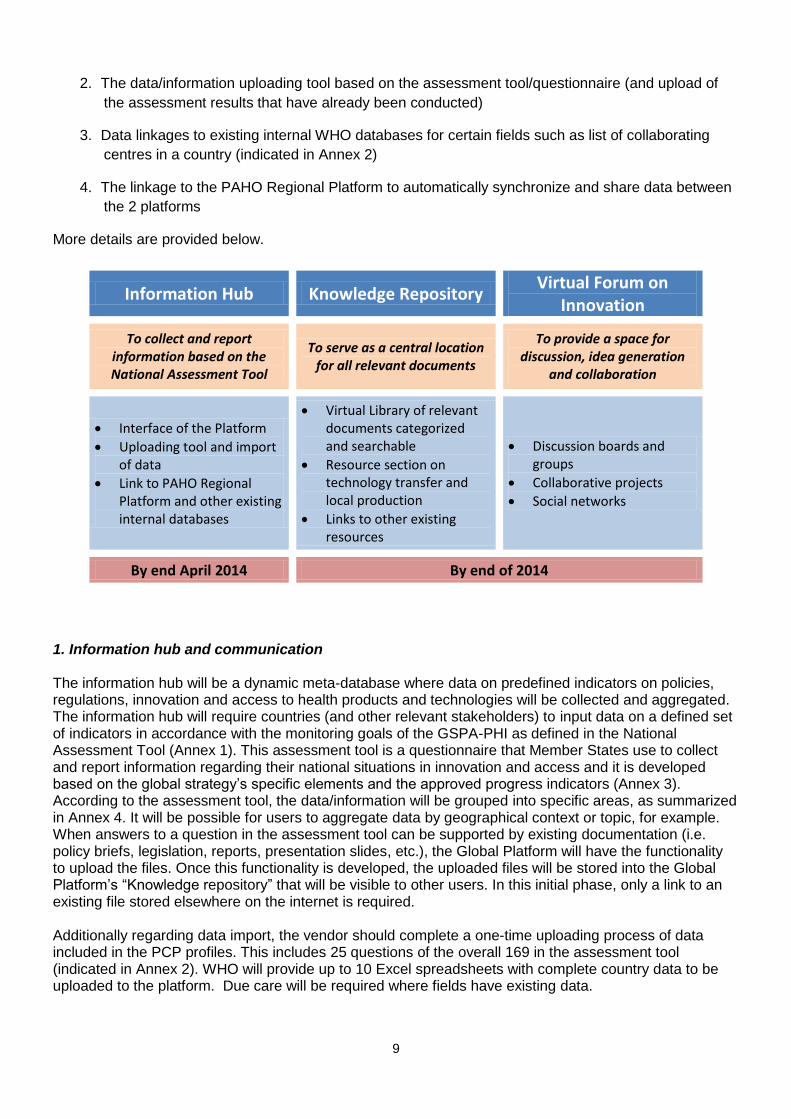
Information Hub Knowledge Repository Virtual Forum on
Innovation
To collect and report information based on the National Assessment Tool
To serve as a central location for all relevant documents
To provide a space for discussion, idea generation
and collaboration
Interface of the Platform
Uploading tool and import of data
Link to PAHO Regional Platform and other existing internal databases
Virtual Library of relevant documents categorized and searchable
Resource section on technology transfer and local production
Links to other existing resources
Discussion boards and groups
Collaborative projects
Social networks
By end April 2014 By end of 2014
1. Information hub and communication The information hub will be a dynamic meta-database where data on predefined indicators on policies, regulations, innovation and access to health products and technologies will be collected and aggregated. The information hub will require countries (and other relevant stakeholders) to input data on a defined set of indicators in accordance with the monitoring goals of the GSPA-PHI as defined in the National Assessment Tool (Annex 1). This assessment tool is a questionnaire that Member States use to collect and report information regarding their national situations in innovation and access and it is developed based on the global strategy’s specific elements and the approved progress indicators (Annex 3). According to the assessment tool, the data/information will be grouped into specific areas, as summarized in Annex 4. It will be possible for users to aggregate data by geographical context or topic, for example. When answers to a question in the assessment tool can be supported by existing documentation (i.e. policy briefs, legislation, reports, presentation slides, etc.), the Global Platform will have the functionality to upload the files. Once this functionality is developed, the uploaded files will be stored into the Global Platform’s “Knowledge repository” that will be visible to other users. In this initial phase, only a link to an existing file stored elsewhere on the internet is required. Additionally regarding data import, the vendor should complete a one-time uploading process of data included in the PCP profiles. This includes 25 questions of the overall 169 in the assessment tool (indicated in Annex 2). WHO will provide up to 10 Excel spreadsheets with complete country data to be uploaded to the platform. Due care will be required where fields have existing data.

10
A linkage also needs to be established between the Global Platform and the PAHO Regional Platform. There are 31 questions of the assessment tool that are also part of the PAHO Regional Platform (indicated in Annex 2). Data on these 31 out of 169 questions need to be directly linked to the Global Platform. Hence, if there is any change or addition in the Regional Platform, the data should be automatically updated in the Global Platform and vice versa. This database will then allow WHO and all other users to analyze data and build reports to identify trends and monitor progress and challenges in GSPA-PHI implementation. As mentioned earlier, these indicators are updated at most once per year and historical data should be maintained to allow for temporal visualizations, for instance seeing the evolution of the number of countries with a policy on health research and development over time year by year. Certain visualizations and mapping will be required. For visualizations, WHO prefers that the vendor use software for which the Organization or vendor already possess the necessary rights. For instance, a WHO in-house mapping module is available that meets the WHO guidelines on country names, territories, and boundaries. An example can be seen on the Global Database on the Implementation of Nutrition Action (GINA).4 This existing mapping module allows a selection/display of 11 themes, 5 indicators, and 3 layers – policy, action, and action location. Other modules can be proposed by the vendor. A similar look and feel of the PAHO Regional Platform could be beneficial for the user experience in cooperation with PAHO partners. WHO staff members responsible for the Global Platform will need to be able to maintain the homepage and news sections highlighting various data from the hub. They will need the ability and interface to do so. There should be capacity to change the actual content of the questionnaire (and therefore of the information collected through it) to respond to new information needs in the future. Finally, communication with the various user groups defined later in this RFP will be important. Administrators and users should have the ability to create groups/communities/circles to facilitate discussion on various topics. 2. Knowledge repository The “Knowledge repository” component of the Global Platform will give users access to information on areas such as access to medicines, intellectual property, research and development, innovation for health, and innovation policies and regulations. It will provide a “one-stop shop” for information on access and innovation, linking a series of useful web-based sources and storing relevant documents from countries and all stakeholders. It will be searchable by criteria such as country, date, subject, and keywords. In addition to the data collected based on the GSPA-PHI indicators, the “Knowledge repository” will integrate new and existing resources that facilitate access to information. These resources that are relevant to the scope of the Platform will include:
Directories from a virtual library;
Links to existing scientific and evidence libraries;
Links to existing portals and thematic websites (Re:Search, HRWeb, African Network for Drugs and Diagnostics Innovation (ANDi), etc.)
Full integration with the PAHO Regional Platform Knowledge repository is desirable.
4 https://extranet.who.int/nutrition/gina/
11
3. Virtual forum on innovation The “Virtual forum on innovation” will be a space where different stakeholders can engage with the research community to stimulate discussion around innovation and access to specific medical products and technologies. Through the networks that stem from this interactive space, it will be possible to promote multi-center projects by breaking down the R&D processes among experts in different geographical locations. These communities will have a dedicated space (protected environment) within the Platform to work, as well as share ideas and information. They will take advantage of collaborative instruments (i.e. Wikis, virtual libraries, etc.), connect with partners regardless of their geographical locations, and ultimately construct a participatory knowledge base to solve global problems in a more efficient and sustainable manner. Furthermore, in certain areas such as technological innovation, these virtual communities will be instrumental for the development of an open innovation model. It will allow the flow of ideas beyond institutional and national boundaries, and expand partnerships that cooperate in the development of medicines and technologies to combat priority diseases. A social network will be established and users will be able to create their own profiles that showcase their experiences and areas of expertise. Also, this social network will facilitate the identification of experts and individuals (expert locator) working on a particular area or with a particular interest.
3.2.2 Technical requirements
Integration Integration with the PAHO Regional Platform is of key importance and should be considered mandatory. An interface to this platform would most probably be accomplished by web service using WSDL/SOAP. The PAHO Regional Platform is built on Java with the database running on Postgre SQL. The vendor can propose the appropriate solution. Offline functionality Due to the limited internet access at many developing countries, the Global Platform should be accessible even with low bandwidth internet. Also, there should be built-in offline functionality. Users should be able to download the assessment tool as a file and fill in offline. When access to Internet is available, users can then upload the file into the Global Platform to input their data. This file should be stored in the platform for verification purposes. Data input To input data, an uploading tool based on the National Assessment Tool will be developed. The assessment results on Tanzania, Kenya, Jordan, and Bangladesh will be imported via a one-time upload. The National Assessment Tool is divided into the following eight sections: 1. Health research and development 2. Building and improving innovative capacity 3. Manufacturing of pharmaceuticals 4. Application and management of intellectual property 5. Improving delivery and access 6. Promoting sustainable financing mechanisms 7. Traditional medicine 8. Monitoring and reporting A summary of all eight sections and their sub-sections is included in Annex 4. In total, there are 169 questions/fields to be included in the uploading tool. When inputting data through the uploading tool, the user (prior registration/permission will be required) should be able to select their country, year of reference, and category. This will allow them to access the relevant sections of the questionnaire. Then, they will be able to view the question list, validate pre-filled field data, input further answers, provide links to supporting documents (eventually having the ability to upload attachments), and receive a confirmation
12
message informing them of the completion of their data entry. These attachments will eventually be stored in the appropriate section of the “Knowledge repository,” which will be visible to other permitted users. When users search for information on indicators for a particular country, they should be able to access and/or download the supporting documents at the same time. For monitoring and evaluation purposes, users should be able to view indicators and responses after selecting the specific country and year of reference. There should also be capacity to facilitate the analysis of each indicator for each country through the reporting system. For example, users should be able to generate pie charts, bar graphs, time trends, etc. to display the collected information. In terms of visualization tools, WHO prefers tools with no or low license fees. Proprietary tools are acceptable where suitable. Users and administrators Different types of user rights need to be defined and incorporated in the login and profile construction processes. The authorized personnel to import, update, and verify data should be selected personnel from the Member States’ Ministries of Health or identified/nominated governmental agencies. After users create their profiles, they should be able to customize the visibility of their profiles (Listed in order of increasing visibility):
Visible to users only (private)
Visible to WHO secretariat
Visible to other member states
Visible to other member states and WHO secretariat
Visible to the public Additionally, institutional profiles are required that link the users to that institution. Examples of high level requirements can be found in Annex 5. User login WHO uses two systems for user authentication. A requirement is that WHO staff members login to the system using their normal username and password (called a “WIMS” account). This uses the OpenID standard. A connection should be made to profiles maintained in the Global Platform. Existing WHO user authentication modules for potential adaptation Modules available include but are not limited to those indicated below. Where possible, we encourage the vendor to make use of existing resources from WHO/PAHO. For external users, a separate WHO authentication system exists. It is called an “ADS” account. Use of this is optional and the vendor can decide whether to include this in the proposal or another option. ADS accounts also use OpenID. User login modules can be adapted directly from existing WHO databases such as the Global Database on the Implementation of Nutrition Action (GINA) 5. This allows users to log in and log out. Users benefit from being able to sign in because this associates content they create with their account. However, this in-house user authentication module does not support different user roles, this would be required in the platform. Data sources to integrate with The Global Platform should link to the PAHO Regional Platform to retrieve the data stored there. If there are automatic updates on the PAHO Regional Platform, the Global Platform should be updated automatically, and vice versa. Matching of data/indicators between the assessment tool and the
5 https://extranet.who.int/nutrition/gina/
13
questionnaire used by PAHO is provided in Annex 2. Out of the 169 indicators of the assessment tool, there are 31 that are also found in the PAHO Regional Platform questionnaire. The Global Platform should also have the capacity to allow uploading of other data sources such as the PCP. For the initial stage of building the database, there will be a one-time upload of PCP data. Platform vulnerability and security tests The Global Platform will be required to pass a standard batch of vulnerability and security tests done by the WHO ITT Department.
3.2.3 Reporting requirements
Throughout the project, several key reports are expected from the vendor: 1. Requirement analysis 2. Mock-up design (front-end) 3. Functional prototype design (back-end) 4. Administrator and user manuals
These reports need to be submitted to WHO by the key dates indicated in Section 4.2. Once feedback is received, and required modification completed, they should be integrated into the requirement analysis and platform design.
3.2.4 Performance monitoring
The vendor should provide plans and deliverables to address the following two aspects of performance monitoring:
1. Implementation of the project 2. Performance of the platform itself after launch
3.2.5 Further Capacities
The vendor should provide training to WHO staff after the execution of the project. The training should cover both the user and maintenance aspects. WHO staff from PHI and IT should be well versed with the functionalities and maintenance of the platform so that they can provide support to other users. There should also be capacity for future customization. Some possible future customization/development includes:
Adjustment to the uploading tool
Integration of other in-house WHO data sources
Knowledge repository
Virtual forum on innovation including the social network functionality
Integration of other external data sources

14
4. DELIVERABLES, TIME FRAME AND BUDGET
4.1 Deliverables
Phase Deliverable output
1. Initiation
The initiation phase will define and confirm the objectives, scope, timeframe and deliverables to be produced from the project.
Answer to the call for proposal with proposed: o Scope o Timeframes o Resources
2. Requirements analysis
The “Requirements analysis” identifies a detailed list of what must be delivered in line with the agreed project scope.
Finalized functional requirements analysis document o A map of “work breakdown structure” o A list of detailed functional requirements, based
on both general and technical requirements requested in the RFP
o User case scenario documentation o Business rule description o Test case scenarios
3. Platform mock-up (front-end)
This mock-up is the prototype of the front-end of the platform.
Mock-up o Design of the mock-up that gives the client a
clear representation of the front-end user interface.
4. Functional prototype (back-end)
The functional prototype will provide the back-end of the data structure.
Functional prototype o Design of the back-end data structure that
allows data input, data linkage to the PAHO regional platform, and data output.
Mapping of navigation system
5. Data linkage/transfer
Importation of existing data sources.
Establish an active link with the PAHO regional platform so that the two platforms are synchronized.
Import data from PCP, NAT and other relevant sources
6. Visualization elements
Provide the visualization elements for key reports and maps.
Interactive maps based on the mapping module provided.
o One color-coded map that indicates the countries that have answered the assessment tool.
o Maps that allow users to pick and choose indicators and themes
7. Go-live
Launch the platform. Platform goes live after client’s approval. The contractor should notify client of the intended go-live date.
8. Post-project support
Technical support in the initiate usage stage of the platform.
The contractor should provide technical/service support in case there are any further questions from the client.
There should be capacity to allow addition of other elements to the platform such as up-loading of additional datasets.
Full hand-over to WHO including user and administrator manual/training guide.
15
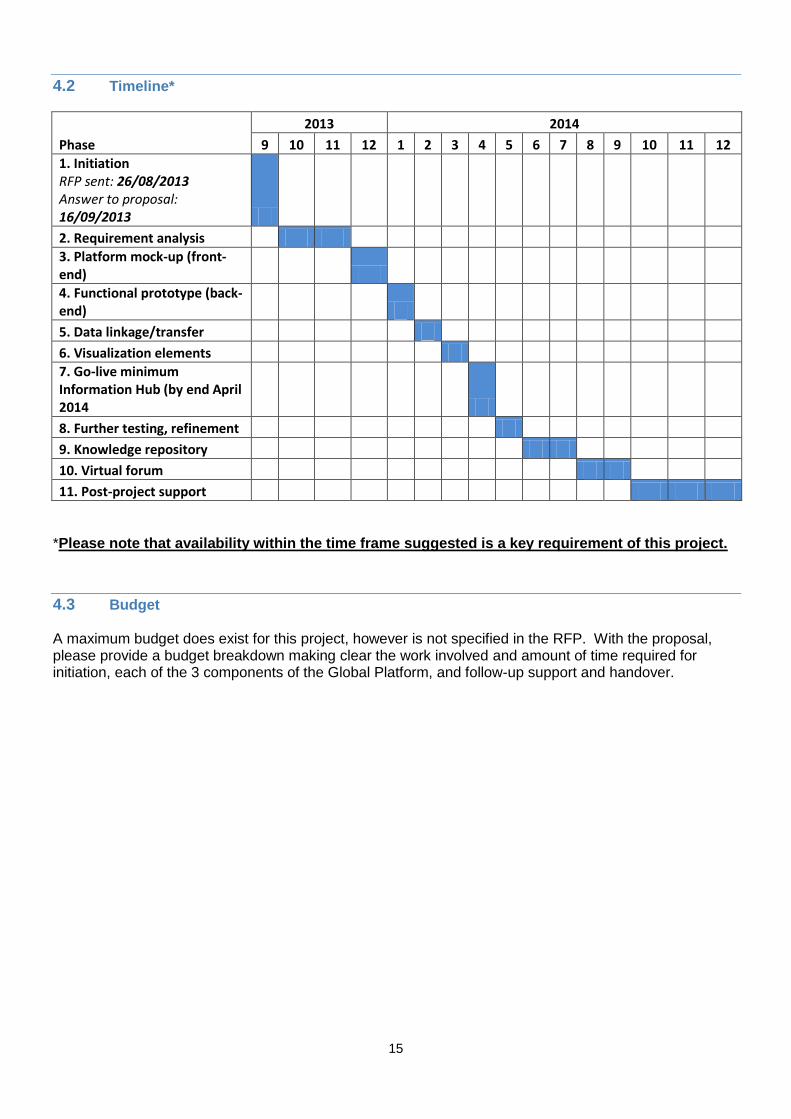
4.2 Timeline*
Phase
2013 2014
9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12
1. Initiation RFP sent: 26/08/2013 Answer to proposal: 16/09/2013
2. Requirement analysis
3. Platform mock-up (front-end)
4. Functional prototype (back-end)
5. Data linkage/transfer
6. Visualization elements
7. Go-live minimum Information Hub (by end April 2014
8. Further testing, refinement
9. Knowledge repository
10. Virtual forum
11. Post-project support
*Please note that availability within the time frame suggested is a key requirement of this project.
4.3 Budget A maximum budget does exist for this project, however is not specified in the RFP. With the proposal, please provide a budget breakdown making clear the work involved and amount of time required for initiation, each of the 3 components of the Global Platform, and follow-up support and handover.
16
5. INSTRUCTIONS TO BIDDERS Bidders should follow the instructions set forth below in the submission of their proposal to WHO.
5.1 Language of the Proposal and other Documents The proposal prepared by the bidder, and all correspondence and documents relating to the proposal exchanged by the bidder and WHO shall be written in the English language.
5.2 Cost of Proposal The bidder shall bear all costs associated with the preparation and submission of the proposal, including but not limited to the possible cost of discussing the proposal with WHO, making a presentation, negotiating a contract and any related travel. WHO will in no case be responsible or liable for those costs, regardless of the conduct or outcome of the selection process.
5.3 Communications during the Call Period
A prospective bidder requiring any clarification on technical, contractual or commercial matters may notify WHO via email at the following address no later than 3 working days prior to the closing date for the submission of offers. Email for submissions of all queries: [email protected] (use subject: WHO Bid Reference: GPIA 2013) The PHI department at WHO will respond in writing (via email only) to any request for clarification of the call that it receives by the deadline indicated above. Questions are to be submitted by e-mail to the above address. There shall be no individual presentation by or meeting with bidders until after the closing date. From the date of issue of this call to the final selection, contact with WHO officials concerning the call process shall not be permitted, other than through the submission of queries and/or through a possible presentation or meeting called for by WHO, in accordance with the terms of this call.
5.4 Period of Validity of Proposals
The offer outlined in the proposal must be valid for a minimum period of 120 calendar days after the closing date. A proposal valid for a shorter period may be rejected by WHO. In exceptional circumstances, WHO may solicit the bidder’s consent to an extension of the period of validity. The request and the responses thereto shall be made in writing. Any bidder granting such an extension will not, however, be permitted to otherwise modify its proposal.
5.5 Closing Date for Submission of Proposals
Proposals must be received at WHO at the e-mail address [email protected] no later than 16 September 2013, 17:00 hours, Geneva time. WHO may, at its own discretion, extend this closing date for the submission of proposals by notifying all bidders thereof in writing.
17
Any proposal received by WHO after the closing date for submission of proposals may be rejected.
5.6 Amendment of the Call
WHO may, at any time before the closing date, for any reason, whether on its own initiative or in response to a clarification requested by a (prospective) bidder, modify the call by written amendment. Amendments could, inter alia, include modification of the project scope or requirements, the project timeline expectations and/or extension of the closing date for submission. All prospective bidders that have submitted a proposal with regard to the call will be notified in writing of all amendments to the call and will, where applicable, be invited to amend their proposal accordingly.
5.7 Clarification of Proposals
WHO may, at its discretion, ask any bidder for clarification of any part of its proposal. The request for clarification and the response shall be in writing. No change in price or substance of the proposal shall be sought, offered or permitted during this exchange.
18
6. AWARD OF CONTRACT
6.1 Award Criteria, Award of Contract
WHO reserves the right to:
Award the contract to a bidder of its choice, even if its bid is not the lowest;
Award separate contracts for parts of the work, components or items, to one or more bidders of its choice, even if their bids are not the lowest;
Accept or reject any proposal, and to annul the solicitation process and reject all proposals at any time prior to award of contract, without thereby incurring any liability to the affected bidder or bidders and without any obligation to inform the affected bidder or bidders of the grounds for WHO's action;
Award the contract on the basis of the Organization’s particular objectives to a bidder whose proposal is considered to be the most responsive to the needs of the Organization and the activity concerned;
Not award any contract at all.
WHO has the right to eliminate bids for technical or other reasons throughout the evaluation/selection process. WHO shall not in any way be obligated to reveal, or discuss with any bidder, how a proposal was assessed, or to provide any other information relative to the evaluation/selection process or to state the reasons for elimination to any bidder. NOTE: WHO is acting in good faith by issuing this RFP. However, this document does not obligate WHO to contract for the performance of any work, nor for the supply of any products or services.
6.2 WHO's Right to modify Scope or Requirements during the Evaluation/Selection Process At any time during the evaluation/selection process, WHO reserves the right to modify the scope of the work, services and/or goods called for under this RFP. WHO shall notify the change to only those bidders who have not been officially eliminated due to technical reasons at that point in time.
6.3 WHO's Right to Extend/Revise Scope or Requirements at Time of Award WHO reserves the right at the time of award of contract to extend, reduce or otherwise revise the scope of the work, services and/or goods called for under this RFP without any change in the base price or other terms and conditions offered by the selected bidder.
6.4 WHO's Right to enter into Negotiations WHO also reserves the right to enter into negotiations with one or more bidders of its choice, including but not limited to negotiation of the terms of the proposal(s), the price quoted in such proposal(s) and/or the deletion of certain parts of the work, components or items called for under this RFP.
6.5 Signing of the Contract Within 30 days of receipt of the contract, the successful bidder shall sign and date the contract and return it to WHO according to the instructions provided at that time. If the bidder does not

19
accept the contract terms without changes, then WHO has the right not to proceed with the selected bidder and instead contract with another bidder of its choice.
20
7. GENERAL AND CONTRACTUAL CONDITIONS
The contract between WHO and the selected bidder ("the Contract") will, unless otherwise explicitly agreed in writing, include the provisions as set forth in this section, and will otherwise inter alia address the following issues:
responsibilities of the selected bidder(s) ("the Contractor(s)") and WHO;
clear deliverables, timelines and acceptance procedures;
payment terms tied to the satisfactory performance and completion of the work;
notices. The prices payable by WHO for the work to be performed under the Contract shall be fixed for the duration of the Contract and shall be in a UN convertible currency (preferably US Dollars), based on the UN exchange rate of the date of invoice. The total amount payable by WHO under the Contract may be either a lump sum or a maximum amount. If the option for payment of a lump sum applies, that lump sum is payable in the manner provided, subject to satisfactory performance of the work. If the option for payment of a maximum amount applies:
The Contract shall include a detailed budget;
The Contractor shall be held to submit a financial statement together with each invoice;
Any advance payments by WHO shall be used by the Contractor exclusively for the work in accordance with the budget and any unspent balance shall be refunded to WHO;
Payment by WHO shall be subject to satisfactory performance and the acceptance of the Contractor's financial statements; and
All financial reports shall be subject to audit by or on behalf of WHO, including examination of supporting documentation and relevant accounting entries in the Contractor's books. In order to facilitate financial reporting and audit, the Contractor shall keep systematic and accurate accounts and records in respect of the work.
Unless otherwise specified in the Contract, WHO shall have no obligation to purchase any minimum quantities of goods or services from the Contractor, and WHO shall have no limitation on its right to obtain goods or services of the same kind, quality and quantity as described in the Contract, from any other sources at any time.
7.1 Conditions of Contract Any and all of the Contractor's (general and/or special) conditions of contract are hereby explicitly excluded from the Contract, i.e., regardless of whether such conditions are included in the Contractor's offer, or printed or referred to on the Contractor's letterhead, invoices and/or other material, documentation or communications.
7.2 Responsibility The Contractor will be responsible to ensure that the work performed under the Contract meets the agreed specifications and is completed within the time prescribed. The Contractor shall facilitate the operational audit related to the execution of the work and the compliance with the obligations set forth in the Contract, by persons so designated by WHO. In this regard, the Contractor shall make all relevant operational information, without restriction, available to persons so designated by WHO and provide satisfactory explanations to all queries arising in connection therewith.
21
7.3 Source of Instructions The Contractor shall neither seek nor accept instructions from any authority external to WHO in connection with the performance of the work under the Contract. The Contractor shall refrain from any action which may adversely affect WHO and shall fulfil its commitments with the fullest regard to the interests of WHO.
7.4 Warranties The Contractor warrants and represents to WHO as follows:
1) The deliverables shall meet the specifications called for in the Contract and shall be fully adequate to meet their intended purpose. The Contractor furthermore warrants that the deliverables shall be error-free. The Contractor shall correct any errors in the deliverables, free of charge, within fifteen days after their notification to the Contractor, during a period of at least one year after completion of the work. It is agreed, however, that errors and other defects which have been caused by modifications to the deliverables made by WHO without agreement of the Contractor are not covered by this paragraph.
2) The deliverables shall, to the extent they are not original, only be derived from, or incorporate, material over which the Contractor has the full legal right and authority to use it for the proper implementation of the Contract. The Contractor shall obtain all the necessary licenses for all non-original material incorporated in the deliverables (including, but not limited to, licenses for WHO to use any underlying software, application, and operating deliverables included in the deliverables or on which it is based so as to permit WHO to fully exercise its rights in the deliverables without any obligation on WHO’s part to make any additional payments whatsoever to any party.
3) The deliverables shall not violate any copyright, patent right, or other proprietary right of any third party and shall be delivered to WHO free and clear of any and all liens, claims, charges, security interests and any other encumbrances of any nature whatsoever.
4) The Contractor, its employees and any other persons and entities used by the Contractor shall not violate any intellectual property rights, confidentiality, right of privacy or other right of any person or entity whomsoever.
5) Except as otherwise explicitly provided in the Contract, the Contractor shall at all times provide all the necessary on-site and off-site resources to meet its obligations hereunder. The Contractor shall only use highly qualified staff, acceptable to WHO, to perform its obligations hereunder.
6) The Contractor shall take full and sole responsibility for the payment of all wages, benefits and monies due to all persons and entities used by it in connection with the implementation and execution of the Contract, including, but not limited to, the Contractor’s employees, permitted subcontractors and suppliers.
Contractor furthermore warrants and represent that the information provided by it to WHO in response to the RFP and during the bid evaluation process is accurate and complete. Contractor understands that in the event Contractor has failed to disclose any relevant information which may have impacted WHO's decision to award the Contract to Contractor, or has provided false information, WHO will be entitled to rescind the contract with immediate effect, in addition to any other remedies which WHO may have by contract or by law.
7.5 Legal Status The Contractor shall be considered as having the legal status of an independent contractor vis-à-vis WHO, and nothing contained in or relating to the Contract shall be construed as establishing or creating an employer/employee relationship between WHO, on the one hand, and the
22
Contractor or any person used by the Contractor in the performance of the work, on the other hand. Thus the Contractor shall be solely responsible for the manner in which the work is carried out. WHO shall not be responsible for any loss, accident, damage or injury suffered by the Contractor or persons or entities claiming under the Contractor, arising during or as a result of the implementation or execution of the Contract, including travel, whether sustained on WHO premises or not. The Contractor shall obtain adequate insurance to cover such loss, accident, injury and damage, before commencing work on the Contract. The Contractor shall be solely responsible in this regard and shall handle any claims for such loss, accident, damage or injury.
7.6 Relation Between the Parties Nothing in the Contract shall be deemed to constitute a partnership between the Parties or to constitute either Party as the agent of the other.
7.7 No Waiver
The waiver by either Party of any provision or breach of the Contract shall not prevent subsequent enforcement of such provision or excuse further breaches.
7.8 Liability The Contractor hereby indemnifies and holds WHO harmless from and against the full amount of any and all claims and liabilities, including legal fees and costs, which are or may be made, filed or assessed against WHO at any time and based on, or arising out of, breach by the Contractor of any of its representations or warranties under the Contract, regardless of whether such representations and warranties are explicitly incorporated here in or are referred to in any attached Appendices.
7.9 Assignment The Contractor shall not assign, transfer, pledge or make any other disposition of the Contract or any part thereof, or any of the Contractor's rights, claims or obligations under the Contract except with the prior written consent of WHO.
7.10 Officials not to Benefit The Contractor warrants that no official of WHO has received or will be offered by the Contractor any direct or indirect benefit arising from the Contract or the award thereof. The Contractor agrees that breach of this provision is a breach of an essential term of the Contract.
7.11 Indemnification
The Contractor shall indemnify and hold WHO harmless, from and against the full amount of any and all claims and liabilities, including legal fees and costs, which are or may be made, filed or assessed against WHO at any time and based on, or arising out of, the acts or omissions of the Contractor, or the Contractor's employees, officers, agents, partners or sub-contractors, in the performance of the Contract. This provision shall extend, inter alia, to claims and liabilities in the
23
nature of workmen's compensation, product liability and liability arising out of the use of patented inventions or devices, copyrighted material or other intellectual property by the Contractor, its employees, officers, agents, servants, partners or sub-contractors.
7.12 Contractor's Responsibility for Employees The Contractor shall be responsible for the professional and technical competence of its employees and will select, for work under the Contract, reliable individuals who will perform effectively in the implementation of the Contract, respect the local laws and customs, and conform to a high standard of moral and ethical conduct.
7.13 Subcontracting Any intention to subcontract aspects of the Contract must be specified in detail in the proposal submitted. Information concerning the subcontractor, including the qualifications of the staff proposed for use must be covered with same degree of thoroughness as for the prime contractor. No subcontracting will be permitted under the Contract unless it is proposed in the initial submission or formally agreed to by WHO at a later time. In any event, the total responsibility for the Contract remains with the Contractor. The Contractor shall be responsible for ensuring that any and all subcontracts shall be fully consistent with the Contract, and shall not in any way prejudice the implementation of any of its provisions.
7.14 Place of Performance The place of performance of the work under the Contract shall be at the contractor’s site.
7.15 Language All communications relating to the Contract and/or the performance of the work thereunder shall be in English.
7.16 Confidentiality
1) Except as explicitly provided in the Contract, the Contractor shall keep confidential all information which comes to its knowledge during, or as a result of, the implementation and execution of the Contract. Accordingly, the Contractor shall not use or disclose such information for any purpose other than the performance of its obligations under the Contract. The Contractor shall ensure that each of its employees and/or other persons and entities having access to such information shall be made aware of, and be bound by, the obligations of the Contractor under this paragraph. However, there shall be no obligation of confidentiality or restriction on use, where: (i) the information is publicly available, or becomes publicly available, otherwise than by any action or omission of the Contractor, or (ii) the information was already known to the Contractor (as evidenced by its written records) prior to becoming known to the Contractor in the implementation and execution of the Contract; or (iii) the information was received by the Contractor from a third party not in breach of an obligation of confidentiality.
2) The Contractor, its employees and any other persons and entities used by the Contractor shall furthermore not copy and/or otherwise infringe on copyright of any document (whether machine-readable or not) to which the Contractor, its employees and any other persons and entities used by the Contractor have access in the performance of the Contract.
24
3) The Contractor may not communicate at any time to any other person, Government or authority external to WHO, any information known to it by reason of its association with WHO which has not been made public except with the authorization of WHO; nor shall the Contractor at any time use such information to private advantage.
7.17 Title Rights
1. All rights pertaining to any and all deliverables under the Contract and the original work product leading thereto, as well as the rights in any non-original material incorporated therein as referred to in section 7.4.2 above, shall be exclusively vested in WHO.
2. WHO reserves the right to revise the work, to use the work in a different way from that originally envisaged or to not use the work at all.
3. At WHO's request, the Contractor shall take all necessary steps, execute all necessary documents and generally assist WHO in securing such rights in compliance with the requirements of applicable law.
7.18 Termination and Cancellation WHO shall have the right to cancel the Contract (in addition to other rights, such as the right to claim damages):
1. In the event the Contractor fails to begin work on the date agreed, or to implement the work in accordance with the terms of the Contract; or
2. In the event the progress of work is such that it becomes obvious that the obligations undertaken by the Contractor and, in particular, the time for fulfilment of such obligations, will not be respected.
In addition, WHO shall be entitled to terminate the Contract (or part thereof), in writing:
1. At will with the provision of thirty (30) days prior notice in writing; and
2. With immediate effect (in addition to other rights, such as the right to claim damages), if, other than as provided above, the Contractor is:
a. In breach of any of its material obligations under the Contract and fails to correct such breach within a period of thirty (30) days after having received a written notification to that effect from WHO; or
b. Adjudicated bankrupt or formally seeks relief of its financial obligations.
7.19 Force Majeure No party to the Contract shall be responsible for a delay caused by force majeure, that is, a delay caused by reasons outside such party's reasonable control it being agreed, however, that WHO shall be entitled to terminate the Contract (or any part of the Contract) forthwith if the implementation of the work is delayed or prevented by any such reason for an aggregate of thirty (30) days. Such termination shall be subject to payment of an equitable part of the Contract sum and/or other reasonable charges. In the event of such termination, the Contractor shall, in accordance with the ownership rights referred to in section 7.17 Title rights, deliver to WHO all work products and other materials so far produced. In the event of and as soon as possible after the occurrence of any cause constituting force majeure, the Contractor shall give notice and full particulars in writing to WHO, of such occurrence or change if the Contractor is thereby rendered unable, wholly or in part, to perform its obligations and meet its responsibilities under the Contract. The Contractor shall also notify WHO of any other changes in conditions or the occurrence of any event which interferes or threatens to interfere with its performance of the Contract. The notice shall include steps proposed by the
25
Contractor to be taken including any reasonable alternative means for performance that is not prevented by force majeure. On receipt of the notice required under this section, WHO shall take such action as it, in its sole discretion, considers to be appropriate or necessary in the circumstances, including the granting to the Contractor of a reasonable extension of time in which to perform its obligations under the Contract.
7.20 Surviving Provisions
Those rights and obligations of the Parties as set forth in sections 7 and 8 that are intended by their nature to survive the expiration or earlier termination of the Contract shall survive indefinitely. This includes, but is expressly not limited to, any provisions relating to WHO's right to financial and operational audit, conditions of contract, warranties, legal status and relationship between the parties, breach, liability, indemnification, subcontracting, confidentiality, title rights, use of the WHO name and emblem, successors and assignees, insurance and liabilities to third parties, settlement of disputes, observance of laws, privileges and immunities, no terrorism or corruption, foreign nationals and compliance with WHO policies.
7.21 Use of WHO name and emblem Without WHO’s prior written approval, the Contractor shall not, in any statement of an advertising or promotional nature, refer to the Contract or its relationship with WHO. In no case shall the Contractor use the name or emblem of the World Health Organization, or any abbreviation thereof, in relation to its business or otherwise.
7.22 Successors and Assignees The Contract shall be binding upon the successors and assignees of the Contractor and the Contract shall be deemed to include the Contractor’s successors and assignees, provided, however, that nothing in the Contract shall permit any assignment without the prior written approval of WHO.
7.23 Payment Payment will be made against presentation of an invoice in a UN convertible currency (preferably US Dollars) in accordance with the payment schedule contained in the Contract, subject to satisfactory performance of the work. The price shall reflect any tax exemption to which WHO may be entitled by reason of the immunity it enjoys. WHO is, as a general rule, exempt from all direct taxes, custom duties and the like, and the Contractor will consult with WHO so as to avoid the imposition of such charges with respect to this contract and the goods supplied and/or services rendered hereunder. As regards excise duties and other taxes imposed on the sale of goods or services (e.g. VAT), the Contractor agrees to verify in consultation with WHO whether in the country where the VAT would be payable, WHO is exempt from such VAT at the source, or entitled to claim reimbursement thereof. If WHO is exempt from VAT, this shall be indicated on the invoice, whereas if WHO can claim reimbursement thereof, the Contractor agrees to list such charges on its invoices as a separate item and, to the extent required, cooperate with WHO to enable reimbursement thereof.
7.24 Title to Equipment Title to any equipment and supplies that may be furnished by WHO shall remain with WHO and any such equipment shall be returned to WHO at the conclusion of the Contract or when no longer needed by the Contractor. Such equipment, when returned to WHO, shall be in the same condition as when delivered to the Contractor, subject to normal wear and tear. The Contractor

26
shall be liable to compensate WHO for equipment determined to be damaged or degraded beyond normal wear and tear.
7.25 Insurance and Liabilities to Third Parties The Contractor shall provide and thereafter maintain: (i) insurance against all risks in respect of its property and any equipment used for the execution of the Contract; (ii) all appropriate workmen's compensation insurance, or its equivalent, with respect to its employees to cover claims for personal injury or death in connection with the Contract; and (iii) liability insurance in an adequate amount to cover third party claims for death or bodily injury, or loss of or damage to property, arising from or in connection with the performance of the work under the Contract or the operation of any vehicles, boats, airplanes or other equipment owned or leased by the Contractor or its agents, servants, employees, partners or sub-contractors performing work in connection with the Contract. Except for the workmen's compensation insurance, the insurance policies under this section shall:
a) Name WHO as additional insured;
b) Include a waiver of subrogation to the insurance carrier of the Contractor's rights against WHO;
c) Provide that WHO shall receive written notice from the Contractor's insurance carrier not less than thirty (30) days prior to any cancellation or material change of coverage.
The Contractor shall, upon request, provide WHO with satisfactory evidence of the insurance required under this section.
7.26 Settlement of Disputes Any dispute relating to the interpretation or application of the Contract shall, unless amicably resolved, be subject to conciliation. In the event of failure of the latter, the dispute shall be settled by arbitration. The arbitration shall be conducted in accordance with the modalities to be agreed upon by the parties or, in the absences of agreement, with the rules of arbitration of the International Chamber of Commerce. The parties shall accept the arbitral award as final.
7.27 Observance of Laws The Contractor shall comply with all laws, ordinances, rules, and regulations bearing upon the performance of its obligations under the terms of the Contract.
7.28 Authority to Modify No modification or change of the Contract, no waiver of any of its provisions or any additional contractual relationship of any kind shall be valid and enforceable unless signed by a duly authorized representative of both parties.
7.29 Privileges and Immunities Nothing in or relating to the Contract shall:

27
- be deemed a waiver of any of the privileges and immunities of WHO in conformity with the Convention on the Privileges and Immunities of the Specialized Agencies approved by the General Assembly of the United Nations on November 21, 1947 or otherwise under any national or international law, convention or agreement; and/or - be construed as submitting WHO to any national court jurisdiction.
7.30 No Terrorism or Corruption The Contractor warrants that:
(i) it is not and will not be involved in, or associated with, any person or entity involved in terrorism, that it will not make any payment to any such person or entity and that it will not enter into any employment or subcontracting relationship with any such person or entity; and (ii) it shall not engage in any illegal, corrupt, fraudulent, collusive or coercive practices in connection with execution of the Contract. The Contractor agrees that breach of this provision is a breach of an essential term of the Contract. Any payments used by the Contractor for the promotion of any terrorist activity or any illegal, corrupt, fraudulent, collusive or coercive practice shall be repaid to WHO without delay.
8. PERSONNEL
8.1 Approval of Contractor Personnel WHO reserves the right to approve any employee, subcontractor or agent furnished by the Contractor and Contractor's consortium partners for the performance of the work under the Contract (hereinafter jointly referred to as "Contractor Personnel"). All Contractor Personnel must have appropriate qualifications, skills, and levels of experience and otherwise be adequately trained to perform the work. WHO reserves the right to undertake an interview process as part of the approval of Contractor Personnel.
The Contractor acknowledges that the qualifications, skills and experience of the Contractor Personnel proposed to be assigned to the project are material elements in WHO’s engaging the Contractor for the project. Therefore, in order to ensure timely and cohesive completion of the project, both parties intend that Personnel initially assigned to the project continue through to project completion. Once an individual has been approved and assigned to the project, such individual will not, in principle, thereafter be taken off the project by the Contractor, or reassigned by the Contractor to other duties. Circumstances may arise, however, which necessitate that Personnel be substituted in the course of the work, e.g. in the event of promotions, termination of employment, sickness, vacation or other similar circumstances, at which time a replacement with comparable qualifications, skills and experience may be assigned to the project, subject to approval of WHO. WHO may refuse access to or require replacement of any Contractor Personnel if such individual renders, in the sole judgment of WHO, inadequate or unacceptable performance, or if for any other reason WHO finds that such individual does not meet his/her security or responsibility requirements. The Contractor shall replace such an individual within fifteen (15) business days of receipt of written notice from WHO. The replacement will have the required qualifications, skills and experience and will be billed at a rate that is equal to or less than the rate of the individual being replaced.
28
8.2 Project Managers Each party shall appoint a qualified project manager (“Project Manager”) who shall serve as such party’s primary liaison throughout the course of the project. The Project Manager shall be authorized by the respective party to answer all questions posed by the other party and convey all decisions made by such party during the course of the project and the other party shall be entitled to rely on such information as conveyed by the Project Manager. The Project Managers shall meet on a monthly basis in order to review the status of the project and provide WHO with reports. Such reports shall include detailed time distribution information in the form requested by WHO and shall cover problems, meetings, progress and status against the implementation timetable.
8.3 Foreign Nationals The Contractor shall verify that all Contractor Personnel is legally entitled to work in the country or countries where the work is to be carried out. WHO reserves the right to request the Contractor to provide WHO with adequate documentary evidence attesting this for each Contractor Personnel. Each party hereby represents that it does not discriminate against individuals on the basis of race, gender, creed, national origin, citizenship.
8.4 Compliance with WHO’s Policies The Contractor shall at all times comply with and ensure that the Contractor and each of its partners, subcontractors and their employees and agents comply with any applicable laws and regulations and with all WHO policies and reasonable written directions and procedures relating to: (i) occupational health and safety, (ii) security and administrative requirements, including, but not limited to computer network security procedures, (iii) sexual harassment, (iv) privacy, (v) general business conduct and disclosure, (vi) conflicts of interest and (vii) business working hours and official holidays. In the event that the Contractor becomes aware of any violation or potential violation by the Contractor, its partners, subcontractors or any of their employees or agents, of any laws, regulations, WHO policies or other reasonable written directions and procedures, the Contractor shall immediately notify WHO of such violation or potential violation. WHO, in it sole discretion, shall determine the course of action to remedy such violation or prevent such potential violation, in addition to any other remedy available to WHO under the Contract or otherwise.
8.5 Ethical Behaviour WHO, the Contractor and each of the Contractor’s partners, subcontractors and their employees and agents shall adhere to the highest ethical standards in the performance of the Contract. In this regard, the Contractor shall also ensure that neither Contractor nor its partners, subcontractors, agents or employees will engage in activities involving child labour, trafficking in arms, promotion of tobacco or other unhealthy behaviour, or sexual exploitation.
8.6 Engagement of Third Parties and use of In-house Resources The Contractor acknowledges that WHO may elect to engage third parties to participate in or oversee certain aspects of the project and that WHO may elect to use its in-house resources for the performance of certain aspects of the project. The Contractor shall at all times cooperate with

29
and ensure that the Contractor and each of its partners, subcontractors and their employees and agents cooperate, in good faith, with such third parties and with any WHO in-house resources.
30
9. ANNEX 1: NATIONAL ASSESSMENT TOOL FOR GSPA-PHI
HEALTH RESEARCH AND DEVELOPMENT Health R&D policies and infrastructure 1. National strategy(ies): Does your country have a national health research policy or strategy? If yes, please
comment on its goals, structure, and mechanisms for intra-ministerial coordination. Provide links to sources of information.
2. Domestic support and leadership: Does your country have a national health research council or equivalent
domestic funding body/agency? Please provide links to sources of information. (Element 2.5.a)
3. Research institutions, capacity and accreditation: What are the key publicly-funded R&D centres/institutes in your country? (Element 3.1.b) What is the balance of publicly-funded research taking place in universities, government research institutions, hospitals, field sites and non-governmental organizations? Does your country have systems to accredit universities, courses and other training, including research training? Please list WHO collaborating centres in your country [POSSIBLE SOURCE: WHO/KMS]
4. Priority setting: Has your country established needs-based priorities for health R&D? What was the process for their definition (e.g., did it include relevant stakeholders)? How often are these priorities reassessed? (Element 1.2.a) Has your country included health systems research in the national health research policy/strategy or in any other equivalent document? (Element 1.2.c)
5. Research networks: Do researchers and/or research institutions in your country participate in national,
regional and/or global health research networks or groups?6 (Element 3.1b) Please, provide links to sources of
information. Funding for health R&D 6. Public spending: What is the national health budget?
7 What is the public budget for health R&D? How much
does the private sector spend on health R&D? (Element 1.2e). If possible, provide trends in such funding over the past 5-10 years. (Element 1.2e) [POSSIBLE SOURCE: National Health Accounts
8]
7. External support: Provide information related to donor funding for public sector health research programs
including health-related innovation. (Element 2.1.b,c) 8. Tracking and transparency: Does your country have publicly accessible information on sources of financing
for health R&D? If yes, please provide details. Discovery science and clinical research 9. Research exemption: Does legislation in your country provide a research exemption to ensure that research
involving patented inventions is not considered infringement? (Element 2.4.e)
10. Clinical trials capacity: Are there any public and/or private efforts in your country to build capacity to conduct clinical trials? Does your country maintain a publically available clinical trials registry? Please provide a brief
6 e.g., (i) permanent/semi- permanent network such as academic societies/associations or ad hoc/time-limited joint venture for a
specific research project; (ii) network/group to be composed only of public sector institutes, only private sector institutes, or both public and private sector institutes. etc.
7 Total government health expenditure, total health expenditures as % of nominal GDP, government health expenditure as % of
total government expenditure 8 http://www.who.int/nha/en/index.html

31
description of clinical trials capacity in your country, both public and private (e.g., contract research organizations).
11. Ethical review: Is there a national ethical review policy for clinical trials? Does it cover the composition and
functions of institutional ethical review committees? Where have such committees been established, and are they linked to other similar committees through national, regional and/or global networks? (Elements 2.2.f, 3.3.b, 3.3.c)
12. International collaboration: Does your country participate in international efforts to build capacity and
improve information in this area, e.g., International Clinical Trials Registry Platform (ICTRP) or European and Developing Countries Clinical Trials Partnership (EDCTP)? (Elements 2.2.f, 3.3.b, 3.3.c, 6.2.f)
Access to knowledge 13. Scientific literature: Do health professionals and researchers in your country have ready access to global
public health literature? Are relevant publications available in national academic and government research institutions? (Element 2.4.a)
14. Compound libraries: Does your country maintain compound libraries?
9 If yes, please provide a list,
description, and note whether your country provides open access to these. (Element 2.2.a,b) Do researchers in your country have access to compound libraries established abroad? Please provide details and reasons. (Element 2.2.a,b)
15. Relevance to product development: If such open-access is available (as explained above), has it led to any new medical products? (Element 2.2.a)
BUILDING AND IMPROVING INNOVATIVE CAPACITY Human resource needs 16. National policy: Does your country have a national policy or strategy focusing on human resources for
health? If yes, does this policy include health researchers? Does it include incentives to retain health professionals including researchers? Please, provide details (Element 3.2.b,c)
17. Public investment: How much does your country invest in education and training of researchers and public
health workers? (Element 3.1.a)
18. Future workforce, general: What disciplines are taught at university level related to public health, health research and health innovation?
10 How many doctoral students per discipline
11 does your country have? What
has been the trend over the last 5-10 years? (Element 3.1a) [POSSIBLE SOURCE: UNESCO]
19. Local production: Do universities in your country provide education in industrial pharmacy, technology
assessment, technology management, business management and entrepreneurship, project management and accounting? Do they have basic and applied tertiary science education and research training relevant to drug manufacture (e.g., medicinal chemistry, pharmacology, biostatistics, target identification, etc.) and vaccine manufacture (e.g., antigen development, vaccine formulation and industrial engineering education covering biologics manufacturing)?
20. IP management: Has there been any assessment of education and training needs for IP management,
drafting and negotiating licenses, drafting patent applications, patent management, claims interpretation, how to manage IP "creatively" to promote both innovation and access, how to use TRIPS flexibilities and how to draft IP-related legislation that is sensitive to public health needs? (Element 5.1.a,e)
9 Definition of compound libraries from Nature.com: A structurally diverse collection of chemical molecules, typically containing
several hundred thousand entities, that is used to identify new lead candidates. http://www.nature.com/nrg/journal/v5/n4/glossary/nrg1317_glossary.html
10 Medicine, pharmaceutical science, health economics, traditional medicine, nursing schools etc
11 Life sciences, pharmaceutical sciences, chemistry, biology, traditional medicine, biotechnology, genomics etc. Please, refer to
doctorate candidates with the nationality of your country that graduate from local universities.

32
21. Dialogue with industry: Do educational institutions and the education ministry in your country have
mechanisms for continuing dialogue with representatives from industry to match curricula with industry needs? If yes, please provide details.
Incentives for health innovation 22. “Putting fuel in the tank” (rewarding academics): Is there a policy or mechanism in your country to
encourage health researchers to contribute to technological innovation (e.g., career advancement linked to patenting and/or industry collaboration)?
12 (Element 3.5b)
23. “Engaging the gears” (local public-private R&D partnerships): Does your country have national policies to
encourage R&D partnerships between publicly funded research institutions and local industry (e.g., Bayh-Dole-like legislation)? Please list examples of such partnerships, if any, and describe outcomes. Do academic and government research institutions in your country have Technology Transfer Offices (TTOs) to facilitate such partnerships to translate publicly funded research knowledge into products? If so, have they developed institutional policies to encourage access to inventions that arise from public investments?
13
24. “Driving innovation” (with push and pull incentives): What incentives exist in your country to encourage
and reward local entrepreneurs and manufacturers in order to strengthen local innovation and production of health products (Element 3.5.a)? Examples may include R&D grants, tax breaks for R&D, business incubators, recognition and/or monetary prizes, soft-loans, preferential pricing for procurement from local manufacturers, restrictions on importation, grants to local public-private R&D partnerships and for Small Business Innovation Research (SBIR) to help local industry attract private capital and encourage the creation of spin-off companies from academic and government research institutions. Please distinguish between domestic incentives and those (if any) from external development partners. Please provide sources and examples.
25. “Steering” innovation toward affordability and access: Are any such incentives specifically designed to
promote affordability and access for medicines that are a high priority to the national health system? Please provide sources and examples.
26. Understanding national health information system: Provide details about national health surveillance and
information systems (Element 3.1c). Are there any assessment reports on the national health information system of your country?
North-south and south-south cooperation for building innovation capacity 27. Partnering: Are there any North–South and/or South–South partnerships and programs for capacity building
in the area of health innovation? (Elements 3.3.b, 2.2.f, 4.2.a)
MANUFACTURING OF PHARMACEUTICALS International transfer of technology 28. National strategy: Is there a national strategy or policy to encourage and assist local manufacturers to
acquire technologies from other countries for local production of health care products (“North-South technology transfer)? Please provide a link to sources of information.
12
In public or private academic institutions or government laboratories. 13
For example, have they signed the AUTM Statement of Principles and Strategies for the Equitable Dissemination of Medical Technologies?
NOTE: Questions 26-30 are drawn primarily from GSPA-PHI Element 4. Questions 31-50 are based on legislative and industry sections of "Strengthening Pharmaceutical Innovation in Africa,
1" a project of
the New Partnership for Africa’s Development (NEPAD) and the Council on Health Research for Development (COHRED).
33
29. Technology assessment: Is there a capacity for technology assessment in your country? Is there any recent assessment of technologies needed for health R&D and for local production of health products? (Element 4.3.b) Please provide links to sources of information. (See Q: 20, 43)
30. Tracking collaboration and outcomes: Does your country have a system for recording initiatives to facilitate technology transfer for local production of health products including: national, South-South and North-South cooperation? (Element 4.2.b) Does your country measure the contribution of local production to access to health products? If yes, please provide links to sources of information.
31. Case studies: Does your country have examples of success stories or failures in North–South and South–South technology transfer for local production of health products?
14 If yes, please provide details and sources.
(Elements 4.2.a, 3.3.b, 2.2.f)
32. External private investment: What is the level of foreign private investment (FDI and other financial flows) in pharmaceutical and other essential health technologies in your country? Please provide links to sources of information.
Local production: policies, capacity and legislation 33. National policies: Does your country have a national trade and investment policy? Does that policy cover
active pharmaceutical ingredients (APIs) and biologics? Does your country have a national industrial policy? Does it cover the biotechnology and pharmaceuticals sectors? Does your country have a national science and technology (or innovation) policy or strategy? Does it include the health sector, and how does it balance economic aspirations with improvements in well-being including public health. What mechanisms are in place for intra-ministerial coordination of the S&T/innovation) policy? Provide links to sources of information.
34. Publicly funded research institution capacities: Are academic and government research institutions in your
country able to act as sponsors for clinical trials? Do they have facilities (e.g., animal facilities) and the technical capacity to meet international licensure standards (Good Laboratory Practice) for drug discovery and for preclinical studies including preclinical vaccine studies (e.g., toxicity)? Do they have access to vaccine delivery systems and adjuvants?
35. Biosafety: What level of biosafety facilities exists in your country? 36. Border controls: Does your country minimize tariffs and duties on imported APIs? Describe. Can customs
controls distinguish genuine from counterfeit API imports and exports? Does your country have anti-dumping policies (e.g., punitive tariffs)?
15
Industry capacity for local production of existing products 37. Good Manufacturing Practice: Are pharmaceutical firms able to comply with Good Manufacturing Practice
(GMP) in the manufacture of health products? Please provide links to sources of information. 38. Importing Active Pharmaceutical Ingredients (APIs): Are pharmaceutical firms able to identify API certified
suppliers and test identity, quality and safety of procured APIs? Are they able to specify and test API requirements, e.g., formulation design, which can affect stability and bioavailability of finished drugs? Are they able to conduct bioequivalence studies of generic formulations? Please provide links to sources of information.
39. Manufacturing and distributing generic drugs: Are pharmaceutical firms able to undertake formulation,
process and scale-up of generic drugs? Are they able to produce APIs to GMP standards and pharmacopoeia requirements? Are they able to undertake small to large-scale manufacturing, commercialize appropriately for local markets and link to local distribution networks? Please provide links to sources of information.
40. Meeting regulatory requirements: Are pharmaceutical firms able to prepare drug master files for registration with the National Regulatory Authority? Are they able to prepare regulatory dossiers for generic drug
14
This covers medicines, diagnostics, vaccines medical equipment and other medical devises… 15
"Dumping" happens when a manufacturer offers its product(s) at a price or quantity that cannot be explained through normal market competition. This may force other manufacturers out of a market, or completely out of business, leaving the "dumper" with a monopoly position. (http://en.wikipedia.org/wiki/Dumping_(pricing_policy)
34
registration, using both data from their own studies and referencing quality, safety and efficacy data from original drug regulatory files?
41. Vaccine production: Do firms have facilities specifically tailored to undertake large scale GMP-standard vaccine production (e.g., sealed fermentation, aseptic production and purification, and large-scale harvesting)?
42. Vaccine quality control and assurance: Are vaccine producers able to maintain and demonstrate a
completely controlled production process (i.e., carry out stability and potency studies; maintain potency and yield during sterile filtration of particle-containing solutions; carry out full tracking of manufacturing batches and lot-by-lot release of vaccines)? Do firms have dedicated in-house quality control laboratories for assay development and processing?
Industry capacity to develop new products 43. Improving known products: Are public and/or private sector manufacturers able to access rights to original
drugs and registration data for further development (e.g., combination therapies and new formulations)?
44. Preclinical testing: Are public and/or private sector manufacturers able to conduct drug and/or vaccine discovery and preclinical studies, bioequivalence studies and complex drug and vaccine clinical trials to international licensure standards? Are they able to access compound libraries and screening facilities? Are they able to access adjuvants and vaccine delivery technologies, and to conduct feasibility studies for large scale vaccine manufacturing?
45. Meeting regulatory requirements: Are public and/or private sector manufacturers able to prepare regulatory dossiers for clinical trial authorization and drug and biologics (vaccine) registration using data from their own clinical studies and referencing quality, safety and efficacy data from original drug regulatory files?
46. Clinical trails: Are public and/or private sector manufacturers able to design and implement clinical development plans for drugs and biologics (vaccines), and to sponsor drug and vaccine trials?
APPLICATION AND MANAGEMENT OF INTELLECTUAL PROPERTY Trade agreements and intellectual property (IP) 47. WTO and TRIPS: Is your country a member of the World Trade Organization (WTO)? Has it entered into
bilateral or regional trade agreements which have resulted in IP protection going beyond what is required by the TRIPS agreement? Has there been any public health impact assessment of such commitments? (Element 5.2.b) Do health representatives in your country participate in bilateral and multilateral trade and IP negotiations? (Element 5.1.g)
48. National legislation: Does national patent legislation incorporate flexibilities available under TRIPS and the
Doha Declaration on TRIPS and Public Health? Has there been any assessment of national IP legislation with regard to public health? (Elements 5.2.a,c,d, 6.3.a) If your country is a least-developed country, has it used transitional periods offered by TRIPS for pharmaceutical processes? (Element 6.1.b)
49. Intra-ministerial coordination: What mechanism does your country use to coordinate policies on public
health, intellectual property and trade? (Element 5.1.h) Patents and clinical trial data exclusivity 50. National patent office: Does your country have a national patent office? Is it a member of a relevant regional
organization? Please, provide details. Does your country maintain a national database on patent applications and patents' legal status (patent registry)? Is this information available electronically and accessible online?
51. Protection of data disclosed to regulatory authorities: Does your country provide for protection of clinical
test data submitted to the national regulatory authority (as required by TRIPS to prevent unfair commercial use)? If yes, how?
35
IMPROVING DELIVERY AND ACCESS Access to quality medicines 52. Policies: Is there a national poverty reduction strategy in your country, and does it address the health sector?
(Element 6.1.f, 6.3.b) Is there a national medicines policy in the country, and a national essential medicines list? Does the national medicines policy include improving access to affordable medicines as one of its objectives? (Element 6.3.b, 6.1.f)
53. Product quality: Are any of the following standards/guidelines available in your country: Good Manufacturing
Practices (Element 6.2.c); Good Clinical Practice (Elements 2.2.f, 3.3.b, 3.3.c, 6.2.f); and Good Laboratory Practice. Is there a national quality control laboratory in your country? Are any medical products from your country prequalified by the WHO? (Element 6.2.d) If yes, please list them.
Delivery infrastructure and incentives 54. Procurement mechanisms: What is the per-capita expenditure on medicines by government in your country,
and what have been the trends over the past 5-10 years? (Element 6.1.a) Is your country part of any pooled procurement program for health products? (Element 6.1.g) If yes, please list them.
55. Delivery infrastructure: What are the strengths and weaknesses in the health delivery infrastructure in your
country? Has there been any formal assessment of this infrastructure?16
(Element 6.1.a) 56. Local incentives for delivery innovation: What mechanisms are in place to create incentives for local
delivery innovation, and for the adoption and adaptation of cost-effective health product and service delivery approaches from other countries or other sociocultural contexts?
Regulation of safety and efficacy 57. Capacity and practice: What are the staff numbers, budget and other capacity measures for the national
regulatory authority (NRA) of your country. Is there any formal assessment report available on the NRA? Does the NRA regulate clinical trials? If so, does it require that all clinical trial data must be obtained from ethically approved trials? (Elements 3.2.a, 6.2.a)
58. Harmonization or creation of regional authorities: Is your country’s NRA part of any regional or sub-regional regulatory harmonization program? (Element 6.2.e) Is your country involved in negotiations that could lead to the creation of a regional regulatory authority to improve economies of scale, transparency and governance?
Affordability of medical products 59. Promoting generics: Are users, doctors and pharmacies in your country encouraged to use generic
medicines. (Element 6.3.g) Please provide details. Does the national patent law in your country have a regulatory exception (“Bolar” type provision) by which generic versions can be introduced immediately after the expiration of a patent? (Element 6.3.a, 5.2.a,c,d)
60. Understanding costs: Has there been any medicine price survey in your country? Is there a price monitoring mechanism? (Element 6.3.e) Has any study been conducted to understand different price components (e.g., tariffs, whole-sale and retail-sale margins, etc.)? Does the government impose import duties on essential medicines and health technologies? (Element 6.3.c)
PROMOTING SUSTAINABLE FINANCING MECHANISMS Public-private R&D partnerships (PDPs)
16
Refer to WHO assessments
36
61. Global PDPs: Is your country involved in partnerships with any global public-private product development partnership (PDP; e.g., International AIDS Vaccine Initiative, Medicines for Malaria Venture, Global Alliance for TB Drug Development, DNDi)? (Element 7.2a) If yes, please provide details on the partnership(s).
62. Domestic support for global PDPs: Does your country give either financial or in-kind support to global
PDPs? Please, provide details. (Element 7.2c) Does your country periodically assess the performance of local collaboration with global PDPs? If yes, please provide methodology. (Element 7.2b)
New sources of funding 63. Revenue generation: Has your country considered any of the options reviewed by the WHO Expert Working
Group on R&D Financing,17
or its successor the WHO Consultative Expert Working Group on R&D Financing, for revenue generation to support domestic health innovation?
TRADITIONAL MEDICINE Health, health research and health innovation policies 64. National policies: Does your country have a national policy on traditional medicine? If yes, does it cover
issues related to innovation in the field of traditional medicine? (Element 3.4 a,b,c) Has your country included traditional medicine in its national health R&D strategy, and are there any R&D priorities identified in traditional medicine? (Element 1.3.a)
Production, regulation and protection 65. Production and development: Is there any local production of traditional medicines in your country? If yes,
do publicly funded research institutions and/or private manufacturers have an ability to systematically evaluate and screen traditional medicines for successful compounds to be identified, developed and marketed?
66. Regulation: What is the status of regulation of traditional medicine in the country? Are there any national standards for quality production and R&D for tradition medicine? (Element 3.4.c)
67. Protection of traditional knowledge: What mechanism does your country use to prevent the misappropriation of traditional (medicinal) knowledge? Are there digital libraries for traditional medical knowledge, and do patent examiners have access to such information when examining patent applications? (Element 5.1.f.e)
MONITORING AND REPORTING 68. Health metrics: How are health and health system-related data and information collected in your country?
18
In what form are such data and information available? Are there any on-going or planned national surveys on health-related issues in your country? If yes, please list them. Does your country participate in international initiatives to monitor progress in achieving the Millennium Development Goals? If yes, please list them.
69. Domestic M&E profession: Does your country have professional associations or organizations of experts in monitoring and evaluation (M&E) in the social sector? If yes, please provide a list.
17
Research and Development - Coordination and Financing: Report of the World Health Organization Expert Working Group on Research and Development Financing, January 2010 (http://www.who.int/phi/documents/ewg_report/en/index.html)
18 i.e.: clinical trials, epidemiology data (burden of diseases), medical records, healthcare facility and hospital management
data, human resources for health

37
10. ANNEX 2: NATIONAL ASSESSMENT TOOL DIVIDED INTO SECTIONS AND SUB-SECTIONS WITH INDICATORS AND MATCH WITH PCP
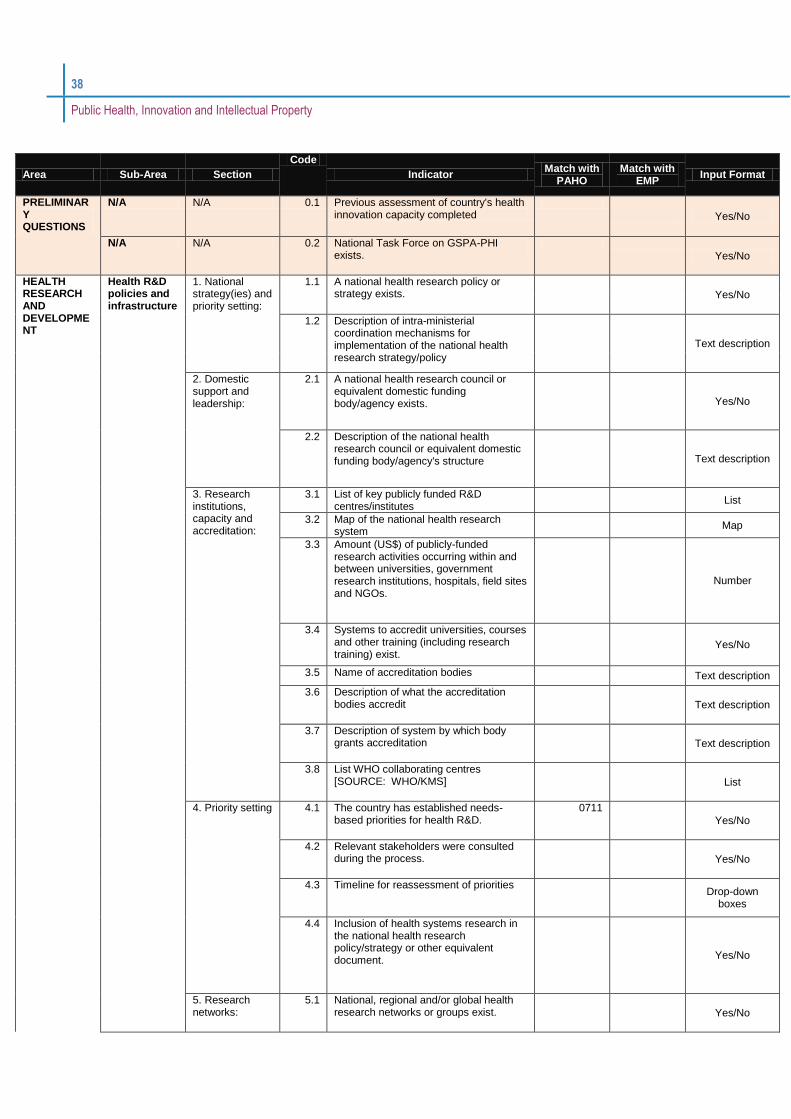
38
Public Health, Innovation and Intellectual Property
Area Sub-Area Section
Code
Indicator Match with
PAHO Match with
EMP Input Format
PRELIMINARY QUESTIONS
N/A N/A 0.1 Previous assessment of country's health innovation capacity completed
Yes/No
N/A N/A 0.2 National Task Force on GSPA-PHI exists.
Yes/No
HEALTH RESEARCH AND DEVELOPMENT
Health R&D policies and infrastructure
1. National strategy(ies) and priority setting:
1.1 A national health research policy or strategy exists.
Yes/No
1.2 Description of intra-ministerial coordination mechanisms for implementation of the national health research strategy/policy
Text description
2. Domestic support and leadership:
2.1 A national health research council or equivalent domestic funding body/agency exists.
Yes/No
2.2 Description of the national health research council or equivalent domestic funding body/agency's structure
Text description
3. Research institutions, capacity and accreditation:
3.1 List of key publicly funded R&D centres/institutes
List
3.2 Map of the national health research system
Map
3.3 Amount (US$) of publicly-funded research activities occurring within and between universities, government research institutions, hospitals, field sites and NGOs.
Number
3.4 Systems to accredit universities, courses and other training (including research training) exist.
Yes/No
3.5 Name of accreditation bodies Text description
3.6 Description of what the accreditation bodies accredit
Text description
3.7 Description of system by which body grants accreditation
Text description
3.8 List WHO collaborating centres [SOURCE: WHO/KMS]
List
4. Priority setting 4.1 The country has established needs-based priorities for health R&D.
0711
Yes/No
4.2 Relevant stakeholders were consulted during the process.
Yes/No
4.3 Timeline for reassessment of priorities
Drop-down
boxes
4.4 Inclusion of health systems research in the national health research policy/strategy or other equivalent document.
Yes/No
5. Research networks:
5.1 National, regional and/or global health research networks or groups exist.
Yes/No
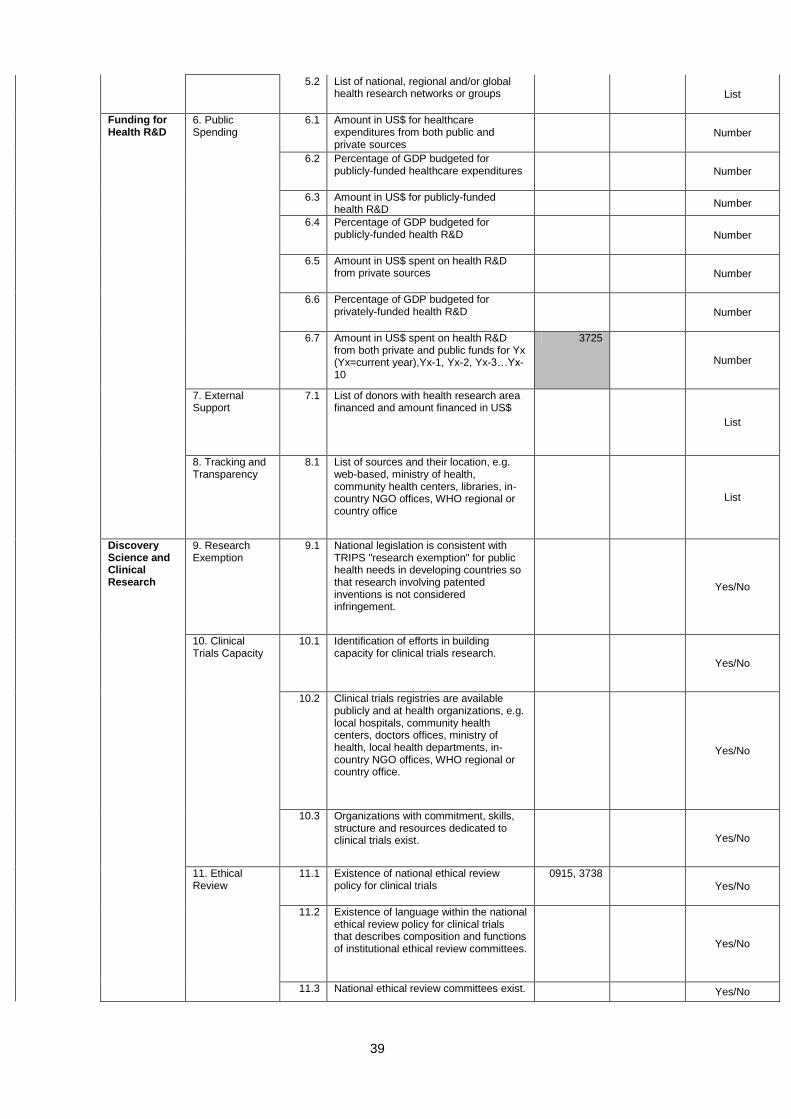
39
5.2 List of national, regional and/or global health research networks or groups
List
Funding for Health R&D
6. Public Spending
6.1 Amount in US$ for healthcare expenditures from both public and private sources
Number
6.2 Percentage of GDP budgeted for publicly-funded healthcare expenditures
Number
6.3 Amount in US$ for publicly-funded health R&D
Number
6.4 Percentage of GDP budgeted for publicly-funded health R&D
Number
6.5 Amount in US$ spent on health R&D from private sources
Number
6.6 Percentage of GDP budgeted for privately-funded health R&D
Number
6.7 Amount in US$ spent on health R&D from both private and public funds for Yx (Yx=current year),Yx-1, Yx-2, Yx-3…Yx-10
3725
Number
7. External Support
7.1 List of donors with health research area financed and amount financed in US$
List
8. Tracking and Transparency
8.1 List of sources and their location, e.g. web-based, ministry of health, community health centers, libraries, in-country NGO offices, WHO regional or country office
List
Discovery Science and Clinical Research
9. Research Exemption
9.1 National legislation is consistent with TRIPS "research exemption" for public health needs in developing countries so that research involving patented inventions is not considered infringement.
Yes/No
10. Clinical Trials Capacity
10.1 Identification of efforts in building capacity for clinical trials research.
Yes/No
10.2 Clinical trials registries are available publicly and at health organizations, e.g. local hospitals, community health centers, doctors offices, ministry of health, local health departments, in-country NGO offices, WHO regional or country office.
Yes/No
10.3 Organizations with commitment, skills, structure and resources dedicated to clinical trials exist.
Yes/No
11. Ethical Review
11.1 Existence of national ethical review policy for clinical trials
0915, 3738
Yes/No
11.2 Existence of language within the national ethical review policy for clinical trials that describes composition and functions of institutional ethical review committees.
Yes/No
11.3 National ethical review committees exist. Yes/No
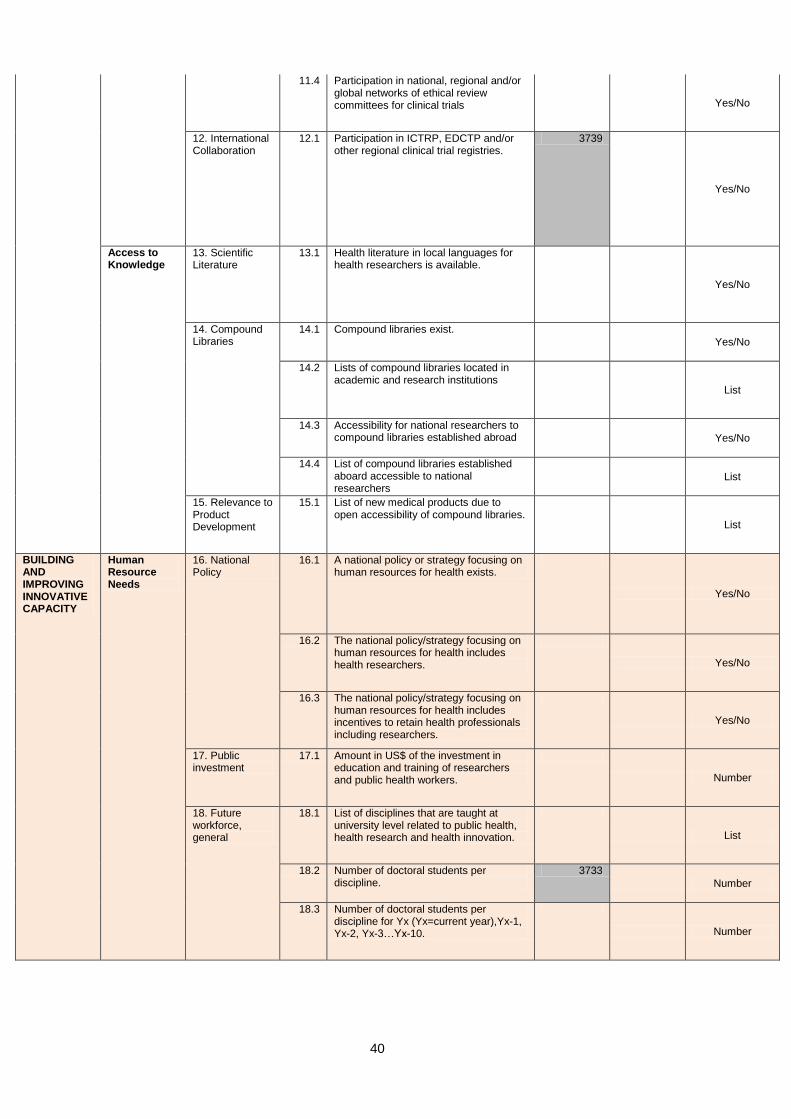
40
11.4 Participation in national, regional and/or global networks of ethical review committees for clinical trials
Yes/No
12. International Collaboration
12.1 Participation in ICTRP, EDCTP and/or other regional clinical trial registries.
3739
Yes/No
Access to Knowledge
13. Scientific Literature
13.1 Health literature in local languages for health researchers is available.
Yes/No
14. Compound Libraries
14.1 Compound libraries exist.
Yes/No
14.2 Lists of compound libraries located in academic and research institutions
List
14.3 Accessibility for national researchers to compound libraries established abroad
Yes/No
14.4 List of compound libraries established aboard accessible to national researchers
List
15. Relevance to Product Development
15.1 List of new medical products due to open accessibility of compound libraries.
List
BUILDING AND IMPROVING INNOVATIVE CAPACITY
Human Resource Needs
16. National Policy
16.1 A national policy or strategy focusing on human resources for health exists.
Yes/No
16.2 The national policy/strategy focusing on human resources for health includes health researchers.
Yes/No
16.3 The national policy/strategy focusing on human resources for health includes incentives to retain health professionals including researchers.
Yes/No
17. Public investment
17.1 Amount in US$ of the investment in education and training of researchers and public health workers.
Number
18. Future workforce, general
18.1 List of disciplines that are taught at university level related to public health, health research and health innovation.
List
18.2 Number of doctoral students per discipline.
3733
Number
18.3 Number of doctoral students per discipline for Yx (Yx=current year),Yx-1, Yx-2, Yx-3…Yx-10.
Number

41
19. Local production
19.1 Provision of education in industrial pharmacy, technology assessment, technology management, business management and entrepreneurship, project management and accounting.
Yes/No
19.2 Provision of basic and applied tertiary science education and research training relevant to drug manufacture (e.g., medicinal chemistry, pharmacology, biostatistics, target identification, etc.) and vaccine manufacture (e.g., antigen development, vaccine formulation and industrial engineering education covering biologics manufacturing).
Yes/No
20. IP management
20.1 Previous assessment of country's education and training needs for IP management, drafting and negotiating licenses, drafting patent applications, patent management, claims interpretation, how to manage IP "creatively" to promote both innovation and access, how to use TRIPS flexibilities and how to draft IP-related legislation that is sensitive to public health needs completed.
Yes/No
21. Dialogue with industry
21.1 Educational institutions and the education ministry have mechanisms for continuing dialogue with representatives from industry to match curricula with industry needs.
Yes/No
Incentives for health innovation
22. “Putting fuel in the tank” (rewarding academics):
22.1 Policies and mechanisms to encourage health researchers to contribute to technological innovation (e.g., career advancement linked to patenting and/or industry collaboration) exist.
3702
Yes/No
23. “Engaging the gears” (local public-private R&D partnerships):
23.1 There are national policies to encourage R&D partnerships between publicly funded research institutions and local industry (e.g., Bayh-Dole-like legislation).
3717
Yes/No
23.2 List of examples of such partnerships and outcomes.
List
23.3 Academic and government research institutions have Technology Transfer Offices (TTOs) to facilitate such partnerships to translate publicly funded research knowledge into products.
Yes/No
23.4 Institutional policies have been developed to encourage access to inventions that arise from public investments.
Yes/No

42
24. “Driving innovation” (with push and pull incentives):
24.1 List of incentives to encourage and reward local entrepreneurs and manufacturers in order to strengthen local innovation and production of health products.
3708
List
25. “Steering” innovation toward affordability and access:
25.1 The incentives are specifically designed to promote affordability and access for medicines that are a high priority to the national health system.
Yes/No
26. Understanding national health information system:
26.1 A national health surveillance and information system exist.
Yes/No
26.2 Previous assessment reports on the national health information system have been completed.
Yes/No
North-south and south-south cooperation for building innovation capacity
27. Partnering: 27.1 North–South and/or South–South partnerships and programs for capacity building in the area of health innovation exist.
Yes/No
MANUFACTURING OF PHARMACEUTICALS
International transfer of technology
28. National strategy:
28.1 There is a national strategy or policy to encourage and assist local manufacturers to acquire technologies from other countries for local production of health care products (“North-South technology transfer).
Yes/No
29. Technology assessment:
29.1 There is capacity for technology assessment.
Yes/No
29.2 Recent assessment of technologies needed for health R&D and for local production of health products has been completed.
Yes/No
30. Tracking collaboration and outcomes:
30.1 There is a system for recording initiatives to facilitate technology transfer for local production of health products including: national, South-South and North-South cooperation.
Yes/No
30.2 The contribution of local production to access to health products is measured.
Yes/No
31. Case studies:
31.1 List examples of success stories or failures in North–South and South–South technology transfer for local production of health products.
List
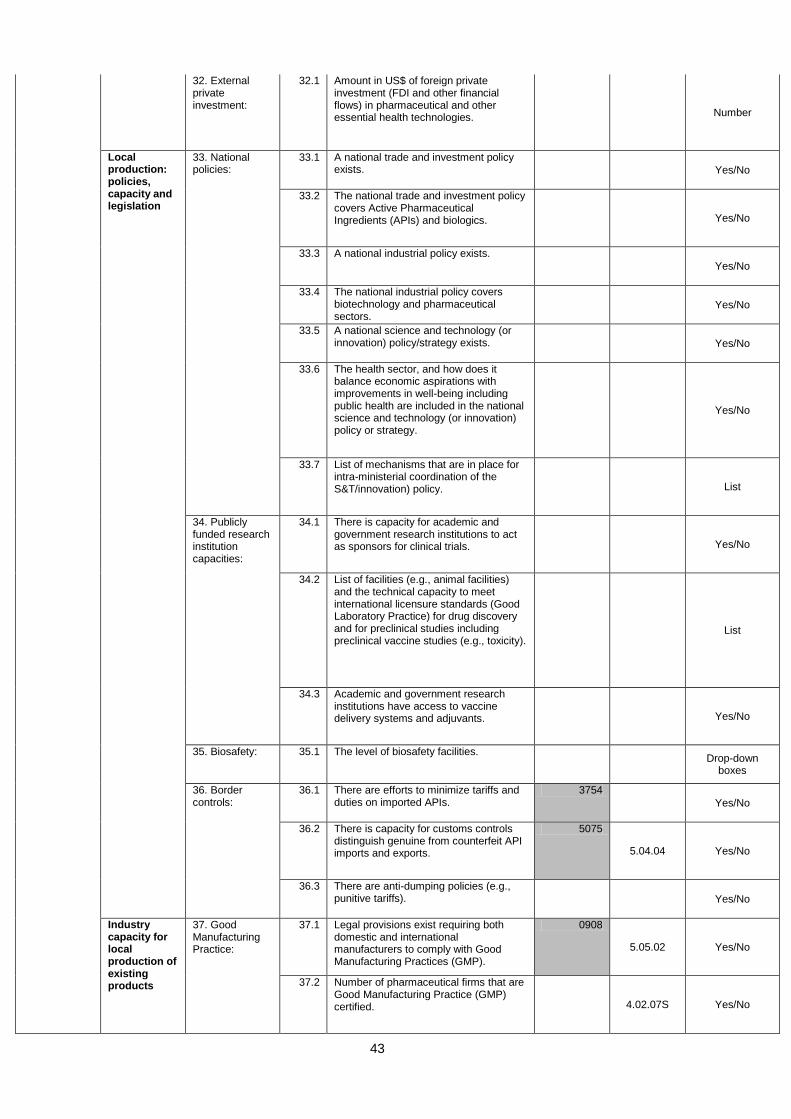
43
32. External private investment:
32.1 Amount in US$ of foreign private investment (FDI and other financial flows) in pharmaceutical and other essential health technologies.
Number
Local production: policies, capacity and legislation
33. National policies:
33.1 A national trade and investment policy exists.
Yes/No
33.2 The national trade and investment policy covers Active Pharmaceutical Ingredients (APIs) and biologics.
Yes/No
33.3 A national industrial policy exists.
Yes/No
33.4 The national industrial policy covers biotechnology and pharmaceutical sectors.
Yes/No
33.5 A national science and technology (or innovation) policy/strategy exists.
Yes/No
33.6 The health sector, and how does it balance economic aspirations with improvements in well-being including public health are included in the national science and technology (or innovation) policy or strategy.
Yes/No
33.7 List of mechanisms that are in place for intra-ministerial coordination of the S&T/innovation) policy.
List
34. Publicly funded research institution capacities:
34.1 There is capacity for academic and government research institutions to act as sponsors for clinical trials.
Yes/No
34.2 List of facilities (e.g., animal facilities) and the technical capacity to meet international licensure standards (Good Laboratory Practice) for drug discovery and for preclinical studies including preclinical vaccine studies (e.g., toxicity).
List
34.3 Academic and government research institutions have access to vaccine delivery systems and adjuvants.
Yes/No
35. Biosafety: 35.1 The level of biosafety facilities.
Drop-down
boxes
36. Border controls:
36.1 There are efforts to minimize tariffs and duties on imported APIs.
3754
Yes/No
36.2 There is capacity for customs controls distinguish genuine from counterfeit API imports and exports.
5075
5.04.04 Yes/No
36.3 There are anti-dumping policies (e.g., punitive tariffs).
Yes/No
Industry capacity for local production of existing products
37. Good Manufacturing Practice:
37.1 Legal provisions exist requiring both domestic and international manufacturers to comply with Good Manufacturing Practices (GMP).
0908
5.05.02 Yes/No
37.2 Number of pharmaceutical firms that are Good Manufacturing Practice (GMP) certified.
4.02.07S Yes/No
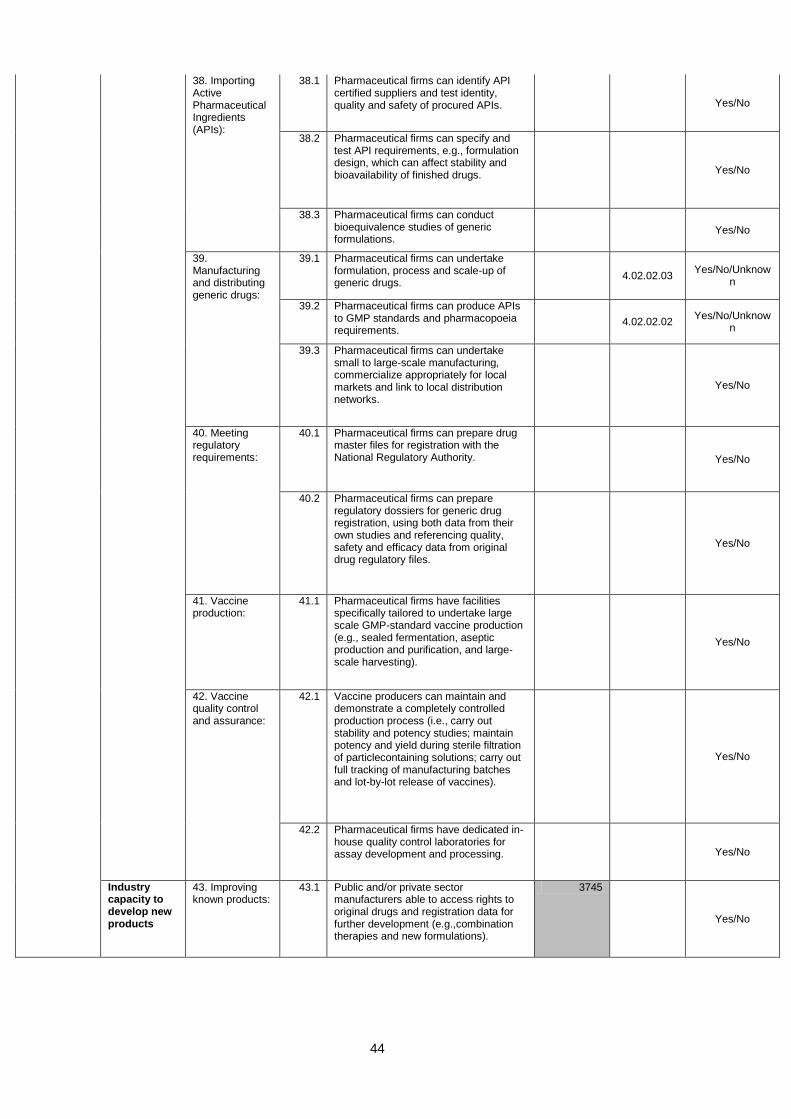
44
38. Importing Active Pharmaceutical Ingredients (APIs):
38.1 Pharmaceutical firms can identify API certified suppliers and test identity, quality and safety of procured APIs.
Yes/No
38.2 Pharmaceutical firms can specify and test API requirements, e.g., formulation design, which can affect stability and bioavailability of finished drugs.
Yes/No
38.3 Pharmaceutical firms can conduct bioequivalence studies of generic formulations.
Yes/No
39. Manufacturing and distributing generic drugs:
39.1 Pharmaceutical firms can undertake formulation, process and scale-up of generic drugs.
4.02.02.03 Yes/No/Unknow
n
39.2 Pharmaceutical firms can produce APIs to GMP standards and pharmacopoeia requirements.
4.02.02.02 Yes/No/Unknow
n
39.3 Pharmaceutical firms can undertake small to large-scale manufacturing, commercialize appropriately for local markets and link to local distribution networks.
Yes/No
40. Meeting regulatory requirements:
40.1 Pharmaceutical firms can prepare drug master files for registration with the National Regulatory Authority.
Yes/No
40.2 Pharmaceutical firms can prepare regulatory dossiers for generic drug registration, using both data from their own studies and referencing quality, safety and efficacy data from original drug regulatory files.
Yes/No
41. Vaccine production:
41.1 Pharmaceutical firms have facilities specifically tailored to undertake large scale GMP-standard vaccine production (e.g., sealed fermentation, aseptic production and purification, and large-scale harvesting).
Yes/No
42. Vaccine quality control and assurance:
42.1 Vaccine producers can maintain and demonstrate a completely controlled production process (i.e., carry out stability and potency studies; maintain potency and yield during sterile filtration of particlecontaining solutions; carry out full tracking of manufacturing batches and lot-by-lot release of vaccines).
Yes/No
42.2 Pharmaceutical firms have dedicated in-house quality control laboratories for assay development and processing.
Yes/No
Industry capacity to develop new products
43. Improving known products:
43.1 Public and/or private sector manufacturers able to access rights to original drugs and registration data for further development (e.g.,combination therapies and new formulations).
3745
Yes/No
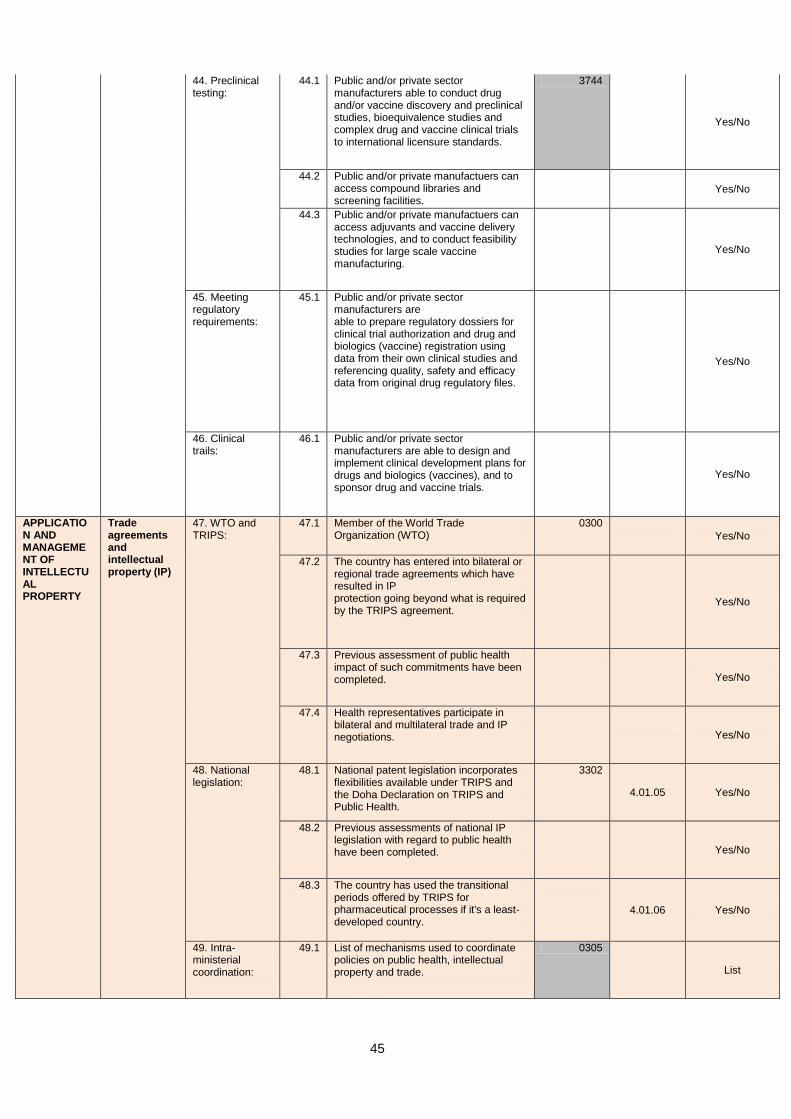
45
44. Preclinical testing:
44.1 Public and/or private sector manufacturers able to conduct drug and/or vaccine discovery and preclinical studies, bioequivalence studies and complex drug and vaccine clinical trials to international licensure standards.
3744
Yes/No
44.2 Public and/or private manufactuers can access compound libraries and screening facilities.
Yes/No
44.3 Public and/or private manufactuers can access adjuvants and vaccine delivery technologies, and to conduct feasibility studies for large scale vaccine manufacturing.
Yes/No
45. Meeting regulatory requirements:
45.1 Public and/or private sector manufacturers are able to prepare regulatory dossiers for clinical trial authorization and drug and biologics (vaccine) registration using data from their own clinical studies and referencing quality, safety and efficacy data from original drug regulatory files.
Yes/No
46. Clinical trails:
46.1 Public and/or private sector manufacturers are able to design and implement clinical development plans for drugs and biologics (vaccines), and to sponsor drug and vaccine trials.
Yes/No
APPLICATION AND MANAGEMENT OF INTELLECTUAL PROPERTY
Trade agreements and intellectual property (IP)
47. WTO and TRIPS:
47.1 Member of the World Trade Organization (WTO)
0300
Yes/No
47.2 The country has entered into bilateral or regional trade agreements which have resulted in IP protection going beyond what is required by the TRIPS agreement.
Yes/No
47.3 Previous assessment of public health impact of such commitments have been completed.
Yes/No
47.4 Health representatives participate in bilateral and multilateral trade and IP negotiations.
Yes/No
48. National legislation:
48.1 National patent legislation incorporates flexibilities available under TRIPS and the Doha Declaration on TRIPS and Public Health.
3302
4.01.05 Yes/No
48.2 Previous assessments of national IP legislation with regard to public health have been completed.
Yes/No
48.3 The country has used the transitional periods offered by TRIPS for pharmaceutical processes if it's a least-developed country.
4.01.06 Yes/No
49. Intra-ministerial coordination:
49.1 List of mechanisms used to coordinate policies on public health, intellectual property and trade.
0305
List
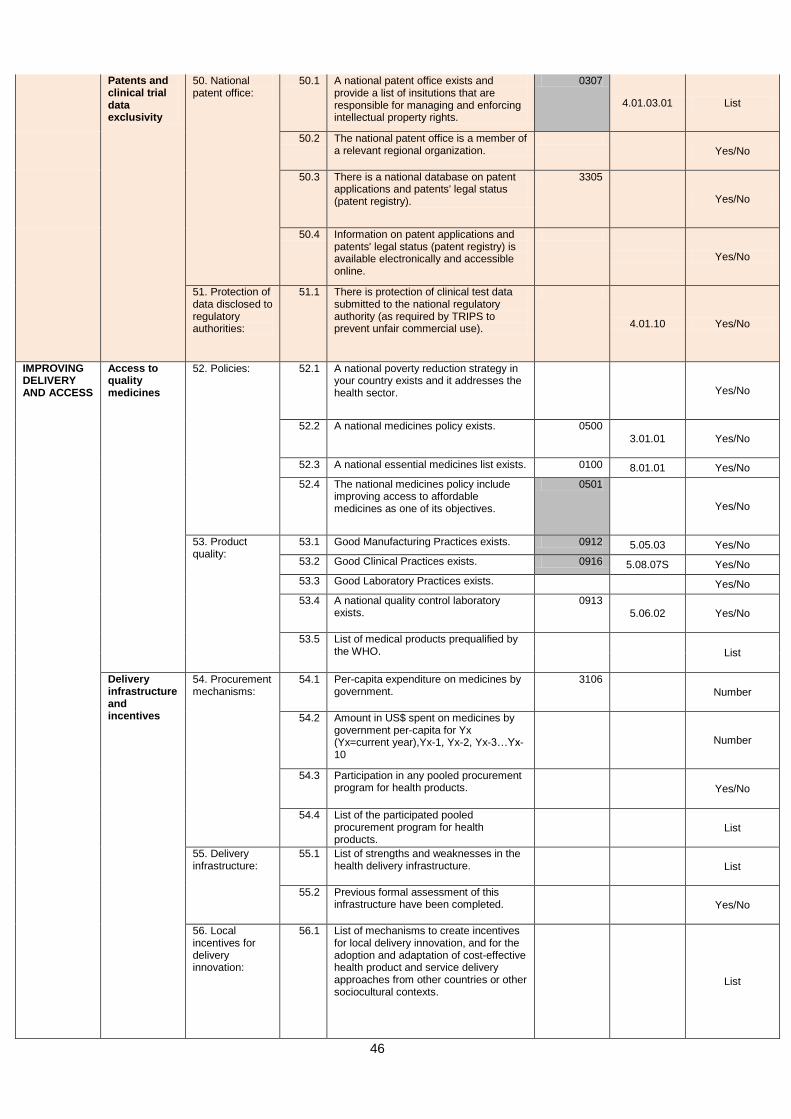
46
Patents and clinical trial data exclusivity
50. National patent office:
50.1 A national patent office exists and provide a list of insitutions that are responsible for managing and enforcing intellectual property rights.
0307
4.01.03.01 List
50.2 The national patent office is a member of a relevant regional organization.
Yes/No
50.3 There is a national database on patent applications and patents' legal status (patent registry).
3305
Yes/No
50.4 Information on patent applications and patents' legal status (patent registry) is available electronically and accessible online.
Yes/No
51. Protection of data disclosed to regulatory authorities:
51.1 There is protection of clinical test data submitted to the national regulatory authority (as required by TRIPS to prevent unfair commercial use).
4.01.10 Yes/No
IMPROVING DELIVERY AND ACCESS
Access to quality medicines
52. Policies: 52.1 A national poverty reduction strategy in your country exists and it addresses the health sector.
Yes/No
52.2 A national medicines policy exists. 0500
3.01.01 Yes/No
52.3 A national essential medicines list exists. 0100 8.01.01 Yes/No
52.4 The national medicines policy include improving access to affordable medicines as one of its objectives.
0501
Yes/No
53. Product quality:
53.1 Good Manufacturing Practices exists. 0912 5.05.03 Yes/No
53.2 Good Clinical Practices exists. 0916 5.08.07S Yes/No
53.3 Good Laboratory Practices exists. Yes/No
53.4 A national quality control laboratory exists.
0913
5.06.02 Yes/No
53.5 List of medical products prequalified by the WHO.
List
Delivery infrastructure and incentives
54. Procurement mechanisms:
54.1 Per-capita expenditure on medicines by government.
3106
Number
54.2 Amount in US$ spent on medicines by government per-capita for Yx (Yx=current year),Yx-1, Yx-2, Yx-3…Yx-10
Number
54.3 Participation in any pooled procurement program for health products.
Yes/No
54.4 List of the participated pooled procurement program for health products.
List
55. Delivery infrastructure:
55.1 List of strengths and weaknesses in the health delivery infrastructure.
List
55.2 Previous formal assessment of this infrastructure have been completed.
Yes/No
56. Local incentives for delivery innovation:
56.1 List of mechanisms to create incentives for local delivery innovation, and for the adoption and adaptation of cost-effective health product and service delivery approaches from other countries or other sociocultural contexts.
List
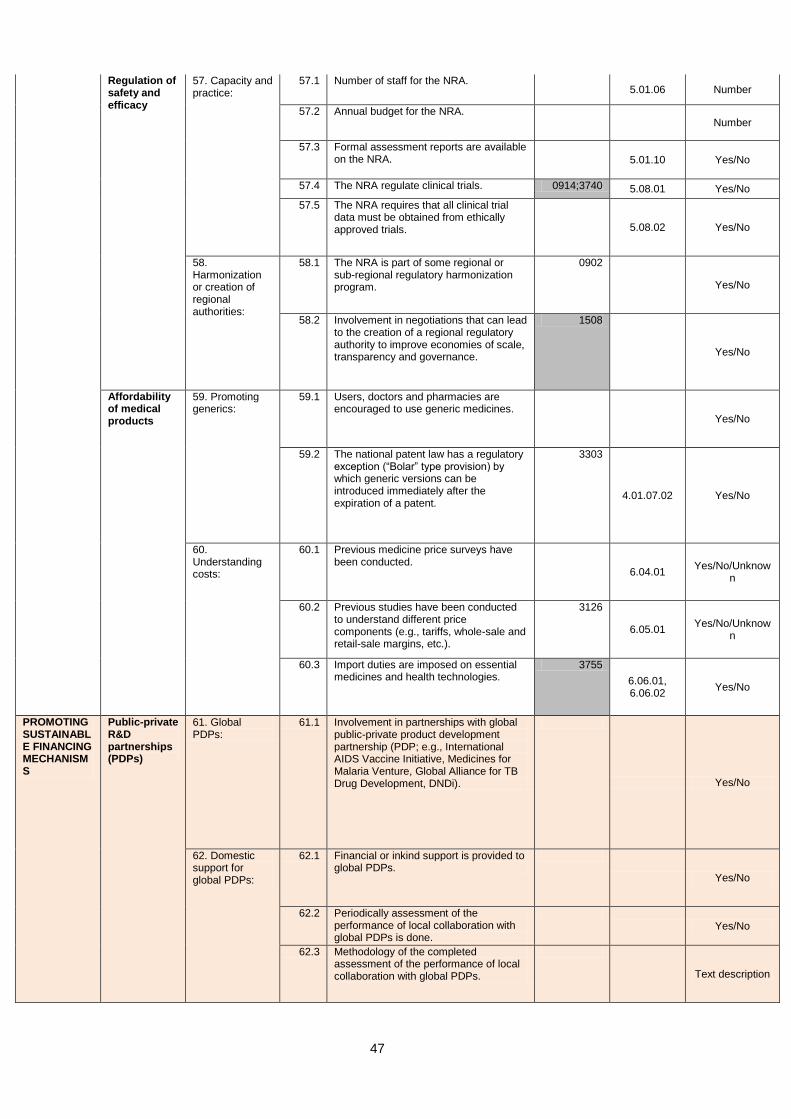
47
Regulation of safety and efficacy
57. Capacity and practice:
57.1 Number of staff for the NRA. 5.01.06 Number
57.2 Annual budget for the NRA. Number
57.3 Formal assessment reports are available on the NRA.
5.01.10 Yes/No
57.4 The NRA regulate clinical trials. 0914;3740 5.08.01 Yes/No
57.5 The NRA requires that all clinical trial data must be obtained from ethically approved trials.
5.08.02 Yes/No
58. Harmonization or creation of regional authorities:
58.1 The NRA is part of some regional or sub-regional regulatory harmonization program.
0902
Yes/No
58.2 Involvement in negotiations that can lead to the creation of a regional regulatory authority to improve economies of scale, transparency and governance.
1508
Yes/No
Affordability of medical products
59. Promoting generics:
59.1 Users, doctors and pharmacies are encouraged to use generic medicines.
Yes/No
59.2 The national patent law has a regulatory exception (“Bolar” type provision) by which generic versions can be introduced immediately after the expiration of a patent.
3303
4.01.07.02 Yes/No
60. Understanding costs:
60.1 Previous medicine price surveys have been conducted.
6.04.01 Yes/No/Unknow
n
60.2 Previous studies have been conducted to understand different price components (e.g., tariffs, whole-sale and retail-sale margins, etc.).
3126
6.05.01 Yes/No/Unknow
n
60.3 Import duties are imposed on essential medicines and health technologies.
3755
6.06.01, 6.06.02
Yes/No
PROMOTING SUSTAINABLE FINANCING MECHANISMS
Public-private R&D partnerships (PDPs)
61. Global PDPs:
61.1 Involvement in partnerships with global public-private product development partnership (PDP; e.g., International AIDS Vaccine Initiative, Medicines for Malaria Venture, Global Alliance for TB Drug Development, DNDi).
Yes/No
62. Domestic support for global PDPs:
62.1 Financial or inkind support is provided to global PDPs.
Yes/No
62.2 Periodically assessment of the performance of local collaboration with global PDPs is done.
Yes/No
62.3 Methodology of the completed assessment of the performance of local collaboration with global PDPs.
Text description
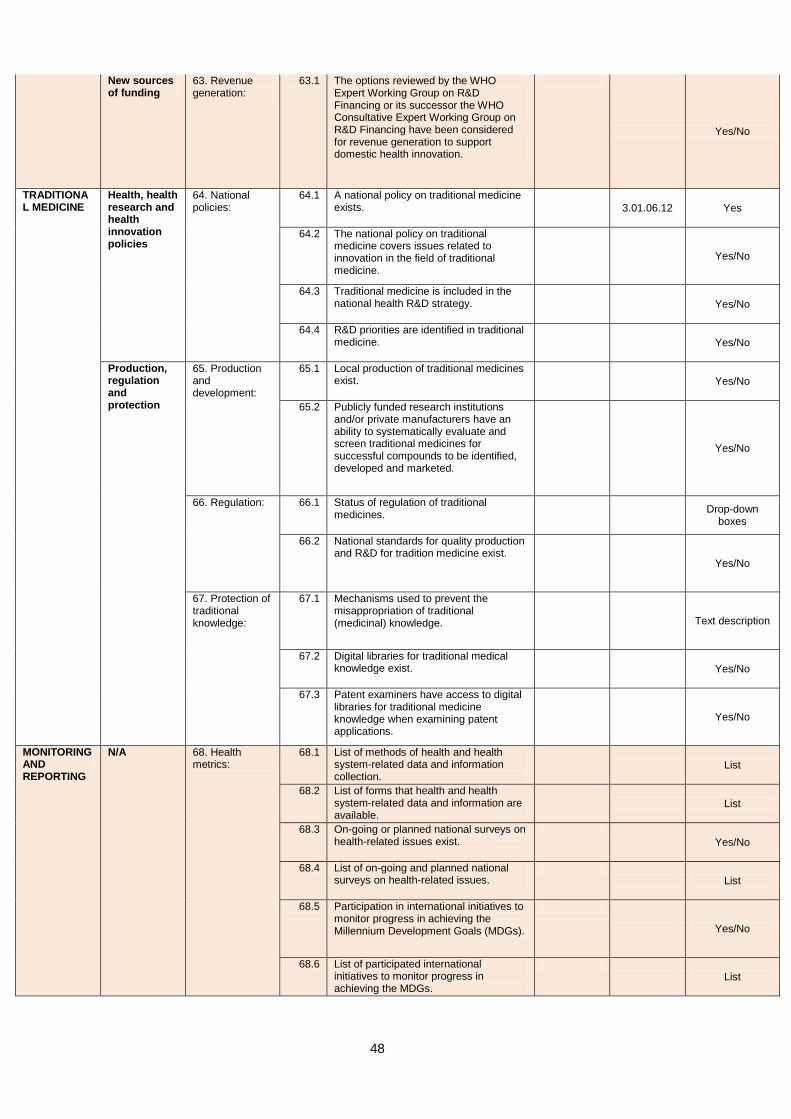
48
New sources of funding
63. Revenue generation:
63.1 The options reviewed by the WHO Expert Working Group on R&D Financing or its successor the WHO Consultative Expert Working Group on R&D Financing have been considered for revenue generation to support domestic health innovation.
Yes/No
TRADITIONAL MEDICINE
Health, health research and health innovation policies
64. National policies:
64.1 A national policy on traditional medicine exists.
3.01.06.12 Yes
64.2 The national policy on traditional medicine covers issues related to innovation in the field of traditional medicine.
Yes/No
64.3 Traditional medicine is included in the national health R&D strategy.
Yes/No
64.4 R&D priorities are identified in traditional medicine.
Yes/No
Production, regulation and protection
65. Production and development:
65.1 Local production of traditional medicines exist.
Yes/No
65.2 Publicly funded research institutions and/or private manufacturers have an ability to systematically evaluate and screen traditional medicines for successful compounds to be identified, developed and marketed.
Yes/No
66. Regulation: 66.1 Status of regulation of traditional medicines.
Drop-down
boxes
66.2 National standards for quality production and R&D for tradition medicine exist.
Yes/No
67. Protection of traditional knowledge:
67.1 Mechanisms used to prevent the misappropriation of traditional (medicinal) knowledge.
Text description
67.2 Digital libraries for traditional medical knowledge exist.
Yes/No
67.3 Patent examiners have access to digital libraries for traditional medicine knowledge when examining patent applications.
Yes/No
MONITORING AND REPORTING
N/A 68. Health metrics:
68.1 List of methods of health and health system-related data and information collection.
List
68.2 List of forms that health and health system-related data and information are available.
List
68.3 On-going or planned national surveys on health-related issues exist.
Yes/No
68.4 List of on-going and planned national surveys on health-related issues.
List
68.5 Participation in international initiatives to monitor progress in achieving the Millennium Development Goals (MDGs).
Yes/No
68.6 List of participated international initiatives to monitor progress in achieving the MDGs.
List
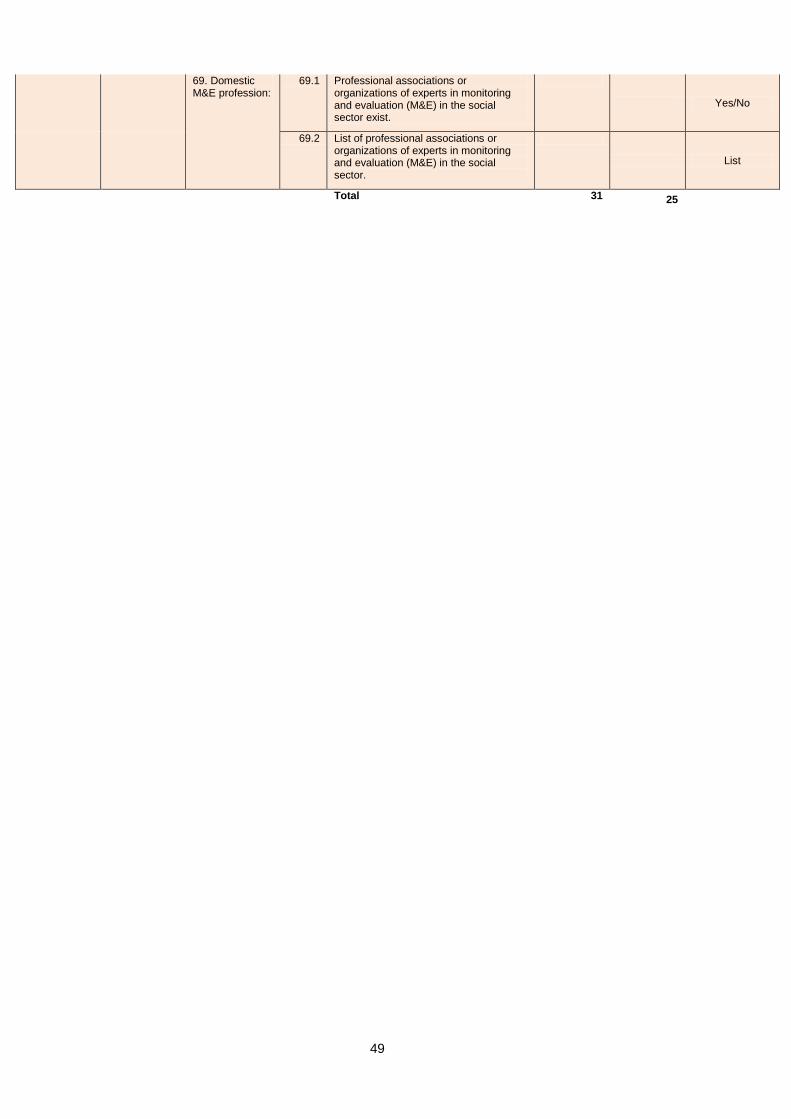
49
69. Domestic M&E profession:
69.1 Professional associations or organizations of experts in monitoring and evaluation (M&E) in the social sector exist.
Yes/No
69.2 List of professional associations or organizations of experts in monitoring and evaluation (M&E) in the social sector.
List
Total 31 25
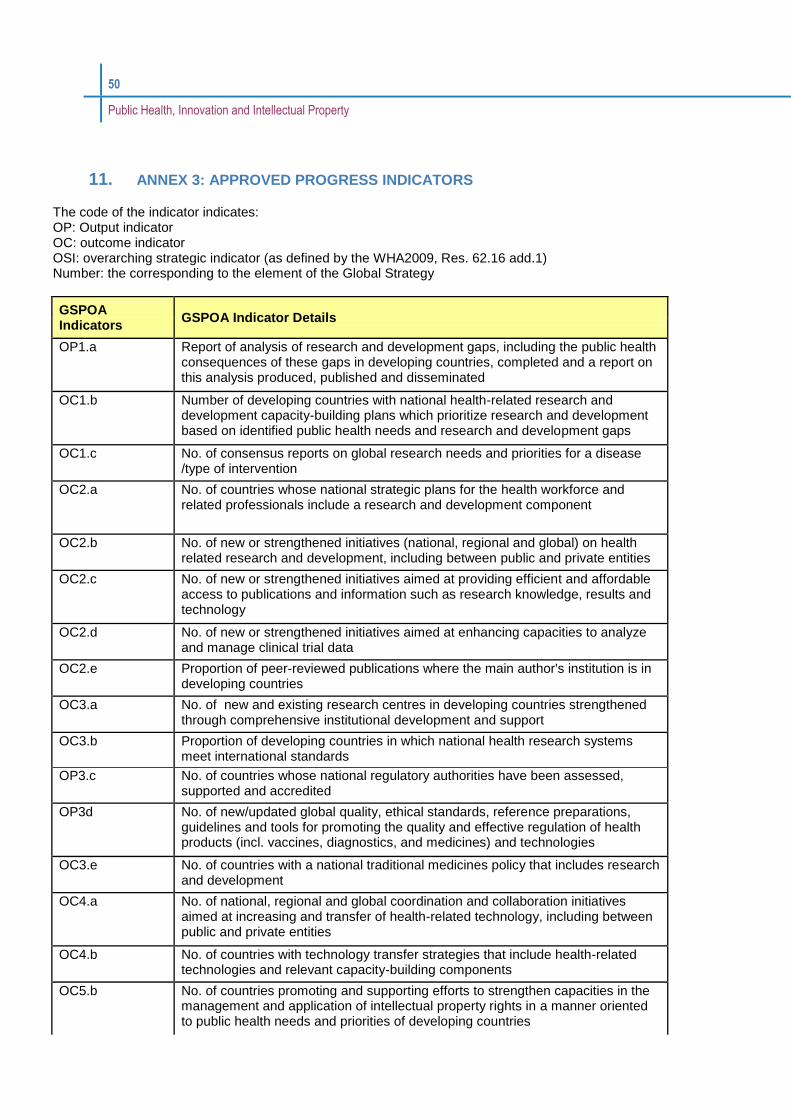
50
Public Health, Innovation and Intellectual Property
11. ANNEX 3: APPROVED PROGRESS INDICATORS
The code of the indicator indicates: OP: Output indicator OC: outcome indicator OSI: overarching strategic indicator (as defined by the WHA2009, Res. 62.16 add.1) Number: the corresponding to the element of the Global Strategy
GSPOA Indicators
GSPOA Indicator Details
OP1.a Report of analysis of research and development gaps, including the public health consequences of these gaps in developing countries, completed and a report on this analysis produced, published and disseminated
OC1.b Number of developing countries with national health-related research and development capacity-building plans which prioritize research and development based on identified public health needs and research and development gaps
OC1.c No. of consensus reports on global research needs and priorities for a disease /type of intervention
OC2.a No. of countries whose national strategic plans for the health workforce and related professionals include a research and development component
OC2.b No. of new or strengthened initiatives (national, regional and global) on health related research and development, including between public and private entities
OC2.c No. of new or strengthened initiatives aimed at providing efficient and affordable access to publications and information such as research knowledge, results and technology
OC2.d No. of new or strengthened initiatives aimed at enhancing capacities to analyze and manage clinical trial data
OC2.e Proportion of peer-reviewed publications where the main author's institution is in developing countries
OC3.a No. of new and existing research centres in developing countries strengthened through comprehensive institutional development and support
OC3.b Proportion of developing countries in which national health research systems meet international standards
OP3.c No. of countries whose national regulatory authorities have been assessed, supported and accredited
OP3d No. of new/updated global quality, ethical standards, reference preparations, guidelines and tools for promoting the quality and effective regulation of health products (incl. vaccines, diagnostics, and medicines) and technologies
OC3.e No. of countries with a national traditional medicines policy that includes research and development
OC4.a No. of national, regional and global coordination and collaboration initiatives aimed at increasing and transfer of health-related technology, including between public and private entities
OC4.b No. of countries with technology transfer strategies that include health-related technologies and relevant capacity-building components
OC5.b No. of countries promoting and supporting efforts to strengthen capacities in the management and application of intellectual property rights in a manner oriented to public health needs and priorities of developing countries
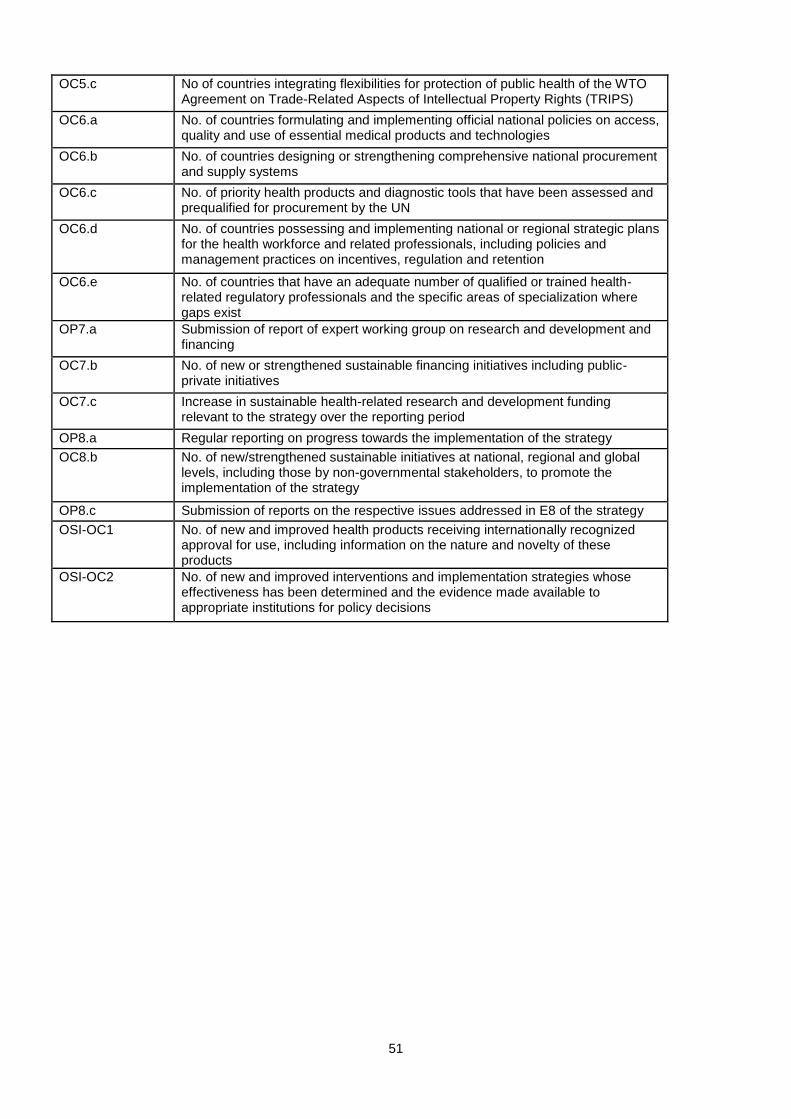
51
OC5.c No of countries integrating flexibilities for protection of public health of the WTO Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS)
OC6.a No. of countries formulating and implementing official national policies on access, quality and use of essential medical products and technologies
OC6.b No. of countries designing or strengthening comprehensive national procurement and supply systems
OC6.c No. of priority health products and diagnostic tools that have been assessed and prequalified for procurement by the UN
OC6.d No. of countries possessing and implementing national or regional strategic plans for the health workforce and related professionals, including policies and management practices on incentives, regulation and retention
OC6.e No. of countries that have an adequate number of qualified or trained health-related regulatory professionals and the specific areas of specialization where gaps exist
OP7.a Submission of report of expert working group on research and development and financing
OC7.b No. of new or strengthened sustainable financing initiatives including public-private initiatives
OC7.c Increase in sustainable health-related research and development funding relevant to the strategy over the reporting period
OP8.a Regular reporting on progress towards the implementation of the strategy
OC8.b No. of new/strengthened sustainable initiatives at national, regional and global levels, including those by non-governmental stakeholders, to promote the implementation of the strategy
OP8.c Submission of reports on the respective issues addressed in E8 of the strategy
OSI-OC1 No. of new and improved health products receiving internationally recognized approval for use, including information on the nature and novelty of these products
OSI-OC2 No. of new and improved interventions and implementation strategies whose effectiveness has been determined and the evidence made available to appropriate institutions for policy decisions

52
12. ANNEX 4: SECTIONS AND SUB-SECTIONS OF INDICATORS LISTED IN ANNEX 2
HEALTH RESEARCH AND DEVELOPMENT
Health R&D policies and infrastructure Funding for health R&D Discovery science and clinical research Access to knowledge
BUILDING AND IMPROVING INNOVATIVE CAPACITY Human resource needs Incentives for health innovation North-south and south-south cooperation for building innovation capacity
MANUFACTURING OF PHARMACEUTICALS International transfer of technology Local production: policies, capacity and legislation Industry capacity for local production of existing products Industry capacity to develop new products
APPLICATION AND MANAGEMENT OF INTELLECTUAL PROPERTY Trade agreements and intellectual property (IP) Patents and clinical trial data exclusivity
IMPROVING DELIVERY AND ACCESS Access to quality medicines Delivery infrastructure and incentives Regulation of safety and efficacy Affordability of medical products
PROMOTING SUSTAINABLE FINANCING MECHANISMS Public-private R&D partnerships (PDPs) New sources of funding
TRADITIONAL MEDICINE Health, health research and health innovation policies Production, regulation and protection
MONITORING AND REPORTING

53
ANNEX 5: EXAMPLES OF HIGH LEVEL REQUIREMENTS
Manage user: The system should allow the admin to manage users.
Manage administrators: The system should allow the admin to manage users.
Add administrators: The system should allow the admin to add other administrators.
Add Permission Access to reach Basic Indicators: The system should allow the users to reach basic indicators.
Add Permission Access to reach Restricted Indicators: The system should allow the admin to add permission access to reach restricted indicators.
Access the information hub page: The system should allow the user the access the information hub page
Information Hub – Add a profile: The system should allow the user add a profile
Information Hub – view indicators results: The system should allow the user to view the indicators results
Repository – Remove a document: The system should allow the users to remove a document
Repository – Edit a document: The system should allow the users to edit a document.
Repository – Add a document: The system should allow the users to add a document
Manage public repository: The system should allow the admin to manage the repository.
Communities – manage: The system should allow the admin manage communities.
Communities – reported: The system should allow the admin manage communities.
Communities – blocked: The system should allow the admin manage communities.
Comments sent – evaluate: The system should allow the admin manage comments sent.
Edit institutional profile: The system should allow the users to edit institutional profile.
Edit institutional profile – Edit institutional representative: The system should allow the users to edit the representative within institutional profile.





























