Embed Size (px)
Citation preview

WHO/CDS/CPE/CEE/2002.28Original: English
W H O
C D S
C P E
C E E
AnnualReporton LymphaticFilariasis2 0 0 1
World Health Organization
global programme to eliminate lymphatic filariasis

© World Health Organization, 2002
This document is not a formal publication of the World Health Organization (WHO), and all rights are reservedby the Organization. The document may, however, be freely reviewed, abstracted, reproduced or translated,in part or in whole, but not for sale or for use in conjunction with commercial purposes.
The designations employed and the presentation of the material in this publication do not imply theexpression of any opinion whatsoever on the part of the World Health Organization concerning the legalstatus of any country, territory, city or area or of its authorities, or concerning the delimitation of itsfrontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may notyet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they areendorsed or recommended by the World Health Organization in preference to others of a similar naturethat are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguishedby initial capital letters.
The World Health Organization does not warrant that the information contained in this publication is completeand correct and shall not be liable for any damages incurred as a result of its use.

World Health OrganizationGeneva, 2002
AnnualReport onLymphaticFilariasis
global programme to eliminate lymphatic filariasis
WHO/CDS/CPE/CEE/2002.28Original: English
W H O
C D S
C P E
C E E

■ Project Manager: Dr Francesco Rio
■ Writer: Ms Angela Haden
■ Additional WritingContributions: Dr Mary Alleman
Dr Brian BagnallDr Claudio BeltramelloDr Gautam BiswasDr Ole ChristensenDr Paul DerstineDr John EhrenbergDr Kazuyo IchimoriDr Mary Ellen KitlerDr Vasanthapuram KumaraswamiMr Kevin LyonnetteMr Chris MaddockProfessor David MolyneuxDr Maria NeiraDr Nikolai NeuouimineDr Kevin PalmerDr Eric OttesenDr Chusak PrasittisukDr Frank RichardsDr Francesco RioDr Jean-Baptiste RoungouDr Anders SeimDr Nana Twum-DansoDr Sergio YactayoMr Andy WrightDr Nevio Zagaria
■ EditorialContributions: Ms Rosemary Besana
Ms Barbara CampaniniMs Sandra DoyleMs Tabinda FaiziDr Ali Hussein
■ Designers: Helena Zanelli Creation
■ Photographs: World Health Organization
Additional copies of this publication are available at no charge from:
CDS Information Resource CentreWorld Health Organization1211 Geneva 27, SwitzerlandFax: +41 22 791 42 85E-mail: [email protected]
www.who.int/infectious-disease-news
This publication can be viewed and downloaded from the website of theGlobal Alliance to Eliminate Lymphatic Filariasis at: http://www.filariasis.org
CONTRIBUTORS

CONTENTS
Programme Highlights . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Chapter 1. Understanding the problem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
The disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Transmission of lymphatic filariasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Clinical forms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Global burden . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
WHO’s global strategy to eliminate lymphatic filariasis . . . . . . . . . . . . . . . . . . . . . . 9
Finding the answers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Chapter 2. Supporting the Global Initiative . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
The start of the global initiative . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
The Global Alliance to Eliminate Lymphatic Filariasis . . . . . . . . . . . . . . . . . . . . . . . 11
The regionalization process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
1. African Programme Review Group . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
2. American Programme Review Group . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
3. Eastern Mediterranean Programme Review Group . . . . . . . . . . . . . . . . . . . . . . 17
4. Mekong-Plus Programme Review Group . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
5. Indian Subcontinent Programme Review Group . . . . . . . . . . . . . . . . . . . . . . . . 18
6. PacELF Coordination and Review Group . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Chapter 3. Implementing the programme . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Initial assessment and mapping of LF distribution . . . . . . . . . . . . . . . . . . . . . . . . . 19
Mass drug administration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Social mobilization and advocacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Preventing and limiting disability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Training . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Monitoring PELF and information system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Activities in regions and countries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
1. African Programme Review Group . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
2. American Programme Review Group . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
3. Eastern Mediterranean Programme Review Group . . . . . . . . . . . . . . . . . . . . . . 40
4. Mekong-Plus Programme Review Group . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
5. Indian Subcontinent Programme Review Group . . . . . . . . . . . . . . . . . . . . . . . . 43
6. PacELF Coordination and Review Group . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
WHO/CDS/CPE/CEE/2002.28

Chapter 4. Facing future challenges................................................................................. 47
Fighting diseases of poverty ................................................................................... 47
Comprehensive health planning ............................................................................ 47
Collaboration with other programmes.................................................................... 48
Targets for 2002 and beyond ................................................................................. 49
Financial resources ................................................................................................. 52
Ways and means to achieve the targets ................................................................. 52
Annexes1. Reports of major international supporters and partners . . . . . . . . . . . . . . . . . . . 53
2. List of lymphatic filariasis-endemic countries and territories by RPRGs . . . . . . . . 59
3. Reporting SAEs associated with DEC + albendazole regimens . . . . . . . . . . . . . . 61
4. Reporting SAEs associated with the ivermectin + albendazole regimens . . . . . . 67
5. Glossary of acronyms and PELF definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73

1
2001 – The Programmegains momentum
In the countries
� A total of 26 million people in 22 countrieswere administered a 2-drug, once-yearlytreatment in the second year of mass drugadministration (MDA) in 2001, almosta ten-fold increase from the year 2000.
� Eleven countries, whose national plansand requests for donated drugs werereviewed and approved, will implementtheir national programmes in 2002.
� A total of 44 million albendazole tabletswere shipped by GlaxoSmithKline to 26countries for either the first or a subsequentround of mass drug administration.
� A total of 22 million ivermectin tablets(Mectizan®) were shipped by Merck & Co.,Inc. to 8 countries covered by the Africanand Eastern Mediterranean ProgrammeReview Groups; 15.5 million were for MDAin areas with only lymphatic filariasis (LF)while 6.5 million were for areas wherelymphatic filariasis and onchocerciasis areco-endemic.
� Surveys continued in all the regionsto map implementation units withLF transmission.
Global Programmeto Eliminate Lymphatic Filariasis (GPELF)P R O G R A M M E H I G H L I G H T S

2
In the regions
� Four of the six regional programme reviewgroups met for the first time in 2001, andtwo had their first meeting in January 2002.In these meetings, roles and effectiveworking mechanisms were discussed andnew plans and re-applications for drugswere reviewed.
� Four workshops on mapping were conducted— three in Africa and one for the countriesof the Mekong-Plus programme review group.
� Ten participants from India and 12 fromother countries in the South-East AsianRegion were trained on disability preventionand alleviation in Pondicherry, India.
� Twenty-two programme managers weretrained in an interregional workshopfor countries in the South-East Asian andWestern Pacific Regions in programmeplanning, implementation, managementand monitoring held, in Kuala Lumpur,Malaysia.
� The 3rd PacELF Annual Meeting took placein Nadi, Fiji on 24-29 September 2001 withtwenty-eight participants from 17 countries.
At the global level
� The Technical Advisory Group (TAG) metfor the second time to discuss the issuesof monitoring the safety of mass drugco-administration regimens, verifyingthe absence of infection and interruptionof transmission, preventing and alleviatingdisability caused by lymphatic filariasis,and the supply and dosage formsof diethylcarbamazine citrate (DEC).On the recommendation of the TAG, theChairman continued working in closecollaboration with the Programme fromthe second half of 2001. In associationwith the Secretariat, the current prioritieswere examined and the topics for discussionby the next TAG identified.
� The process of regionalization of theProgramme Review Group was completed.Six regional programme review groupswere created, where necessary, based onepidemiological requirements rather thanthe WHO regional organization.
� As a follow-up to the recommendationof the TAG, the data accumulated fromthe active surveillance were reviewed withthe pharmacovigilance specialist ofthe TAG. The results indicated that theco-administered regimens were safe forwide-scale use. The reactions werequalitatively and quantitatively similarto those reported previously and appearedto be related to the therapeutic effectsof the co-administered drugs.
� Training modules for drug distributorson disability prevention and control werepublished.
P R O G R A M M E H I G H L I G H T S

3
This report highlights the progress made during the year 2001 in
activities aimed at the elimination of lymphatic filariasis (LF) worldwide.
There are more than a billion people who are at risk of lymphatic
filariasis, which is not a killer disease. The infection is caused by thread-
like worms (filariae) which lodge in the lymphatic system, producing
millions of minute larvae (microfilariae) that circulate in the blood.
Although infection often occurs in childhood, the symptoms are
commonly delayed until adulthood.
Over 120 million people are currently living with the disease, including
about 40 million who are incapacitated and disfigured by it. Of all
diseases, lymphatic filariasis is the second leading cause of permanent
and long-term disability.
Until recently, the diagnosis of lymphatic filariasis depended on night
blood examinations to detect microfilariae. Now, there is an antigen-
detection test that can be taken at any time of the day, making it
feasible to map the disease geographically. Drugs, which are available
free or at low cost, kill the microfilariae in the blood. Simple methods
of hygiene and self-care can reduce the effects of the disease. With
such effective tools to hand, the Fiftieth World Health Assembly, in
1997, resolved to eliminate lymphatic filariasis as a public health
problem. This report discusses the progress so far.
Introduction

� Chapter 1 outlines the causes and effectsof the disease, showing how anunderstanding of the transmissionmechanisms led to a consensus on themost effective strategy to pursue. Thisstrategy has two goals:first, to interrupt transmission of infectionso as to protect future generations;and second, to prevent or alleviate thesuffering of those who already have thedisease.
� Chapter 2 describes the creation anddevelopment of the WHO Programmeto Eliminate Lymphatic Filariasis (PELF).One of the dynamic outcomes of thisProgramme is the launching of a globalalliance, comprising ministers of healthof endemic countries, the private sector,international development agencies,nongovernmental organizations,international organization and academicinstitutions.
� Chapter 3 looks at the activities in theregions and countries, showing how theglobal strategy is being implemented inpractice and how the programme is findinginnovative ways to overcome the specificchallenges that countries and communitiesface. In this respect, advocacy and awareness-building are vital components of theprogramme, as the whole population atrisk must be convinced of the importanceof taking anti-filarial drugs.
� Chapter 4 views the Programme to EliminateLymphatic Filariasis from a health systemsperspective. Obviously, the Programmedoes not exist in a vacuum. It relies onthe health systems in endemic countriesto deliver the necessary drugs and promoteproper care for those affected by the disease.Moreover, it strengthens health systems byproviding training and expertise in diseasemapping, drug delivery strategies, andsocial mobilization. Efforts to eliminatelymphatic filariasis also provide a welcomebonus in terms of reducing the problemsrelated to soil-transmitted helminths.Finally, this chapter identifies future challengesand sets out the targets to be met in orderto reach the goal of eliminating lymphaticfilariasis.
4

The disease
Lymphatic filariasis, also known aselephantiasis, is caused by the threadlikeparasitic worms Wuchereria bancrofti,Brugia malayi and Brugia timori. Theseworms lodge in the lymphatic system, whichis a network of lymph nodes and vesselsmaintaining the fluid balance between thetissues and the blood, and an essentialcomponent of the body’s immune defencesystem. The worms live for 4–6 years,producing millions of minute larvae(microfilariae) which circulate in the blood.
Transmissionof lymphatic filariasis
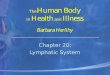
The disease is transmitted by mosquitoes, butthe reservoir of infection is 90% human.The mosquito bites an infected personand picks up the microfilariae which developinside the mosquito into the infective stage,in a process that usually takes 7–21 days.The larvae then migrate to the biting mouth-parts of the mosquito, and enter the puncturedskin of the person who is next bitten by themosquito. The life-cycle of lymphatic filariasisis illustrated schematically in Figure 1.1.
Chapter 1Understanding the problem
Figure 1.1. Lymphatic filariasis life cycle
Larvae developinto adult wormsin lymphatic vessels
Mosquito takes blood meal,infecting a personwith L3 larvae
Blood microfilariaeingested by mosquito duringa blood meal
Adult female wormsproduce microfilariaewhich migrate to peripheral blood
5

Clinical forms
Although the majority of people infectedwith the parasites that cause lymphaticfilariasis have no outward symptoms,virtually all of them suffer subclinicallymphatic damage. Some 40% of thoseinfected suffer renal damage, resultingin blood in the urine (haematuria) andan excess of serum proteins in the urine(proteinuria).
Infection can lead to a variety of clinicalmanifestations, including lymphoedema andelephantiasis of the limbs, as well as genitaldiseases, especially hydrocoele, chylocoele,and elephantiasis of the scrotum and penis.Infection can also lead to acute, recurrentsecondary bacterial infections, known as“acute attacks”.
The most significant factor in producinglymphoedema and elephantiasis, whichcompounds the damage caused by filarialparasites, is bacterial and fungal ‘super-infection’ of the skin. These infections causesevere, febrile syndromes in patients, whilefurther destroying the delicate lymphaticvessels and exacerbating both progressionof the disease and frequency of clinicalsymptoms.
The most obvious manifestations of lymphaticfilariasis are enlargement of the entire legor arm, the genitals, vulva or breasts.In endemic communities, 10–50% of menand up to 10% of women can be affected.
6

7
� Chapter 1 Understanding the problem
Global burden
Lymphatic filariasis is primarily a disease ofthe poor because of its prevalence in remoterural areas and in disfavoured peri-urbanand urban areas. In recent years, lymphaticfilariasis has steadily increased because ofthe expansion of slum areas and poverty,especially in Africa and the Indian subcontinent.Some 120 million people are infectedworldwide, and the disease is endemic
in more than 80 countries and territories
(Map 1.1). Globally, lymphatic filariasis is
thought to be the second leading cause
of permanent and long-term disability.
An estimated 118 million people have one
form or other of the clinical disease.
Of these, 74 million who are microfilaraemicbut asymptomatic have hidden lymphaticand renal pathology. Another 27 millionmen in endemic areas are believed to havehydrocoele due to filariasis. In addition,approximately 16 million people havelymphoedema or elephantiasis alongwith the accompanying recurrent episodesof acute adenolymphangitis. Lastly, a millionindividuals have cryptic infections resultingin conditions such as tropical pulmonaryeosinophilia (TPE).
The designations employed and the presentation of material on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers
or boundaries. Dashed lines represent approximate border lines for which there may not yet be full agreement.
Map 1.1 Lymphatic filariasis-endemic-countries and territories, 2001
Endemic countries
Source:LF eliminationprogramme

Most infections are acquired inchildhood, with a long period ofsubclinical disease before thecharacteristic, overt clinicalmanifestations appear in adults.The re-evaluation of previousunderestimated figures of lymphaticfilariasis in children may well lead tothe disease being identified as theleading cause of permanent andlong-term disability worldwide.Recognition of this fact means thatchildren will be the principalbeneficiaries of any programme forthe elimination of lymphaticfilariasis, and they represent aparticularly important targetpopulation for the programme toachieve its twin goals of interruptingtransmission and preventing disease.
Among tropical diseases, onlymalaria causes a greater burden, asmeasured in disability-adjusted life-years (DALYs). Lymphatic filariasisreduces peoples ability to work,resulting in loss of family income.Furthermore, sufferers often wastemoney on costly but ineffectivetreatments. In India alone, theeconomic losses resulting fromdecreased productivity and lostworkdays are estimated to be of theorder of US$ 1 billion annually.
Box 1.1
FIFTIETH WORLD HEALTH ASSEMBLY WHA50.29
Agenda item 20 13 May 1997
Elimination of lymphatic filariasisas a public health problem
The Fiftieth World Health Assembly,
Deeply concerned at the widening spread and increased distribution of lymphatic filariasis throughout the world in both urban and rural areas and concerned that itaffects all ages and both sexes;
Appreciating with grave concern the human suffering, social stigma and costs tosociety associated with lymphatic filariasis morbidity;
Recognizing that there is a general lack of awareness concerning this disease and itsimpact on health status, and that there are insufficient data on its prevalence anddistribution;
Welcoming the recent studies which have defined new, simplified, highly effectivestrategies;
Acknowledging that an international task force on disease eradication has recentlyidentified lymphatic filariasis as one of only six “potentially eradicable” infectiousdiseases,
1. URGES Member States:
(1) to take advantage of recent advances in the understanding of lymphatic filariasisand the new opportunities for its elimination by developing national plans leading to its elimination, as well as for the monitoring and evaluation of programmeactivities;
(2) to strengthen local programmes and their integration with the control of otherdiseases, particularly at the community level. in order to implement simple,affordable, acceptable and sustainable activities based on community-wide treatment strategies, but supplemented where feasible by vector control and improved sanitation;
(3) to strengthen training, research, diagnostic laboratory, disease and datamanagement capabilities in order to improve clinical, epidemiological and operational activities directed toward eliminating lymphatic filariasis as a publichealth problem..
(4) to mobilize support of all relevant sectors, affected communities and non-governmental organizations for the elimination of the disease.
2. INVITES other specialized agencies of the United Nations system, bilateraldevelopment agencies, nongovernmental organizations and other groups concerned.to increase cooperation in the elimination of lymphatic filariasis through support ofnational and international programmes relevant to the prevention and elimination oflymphatic filariasis;
3. REQUESTS the Director-General:
(1) to bring to the attention of the other specialized agencies and organizations of theUnited Nations system, bilateral development agencies, nongovernmentalorganizations and other groups concerned the need for closer collaboration in theelimination of lymphatic filariasis as a public health problem;
(2) to mobilize support for global and national elimination activities;
(3) to keep the Executive Board and Health Assembly informed as necessary ofprogress in the implementation of this resolution.
Ninth plenary meeting, 13 May 1997A50/VR/9
8

9
WHO’s global strategyto eliminate lymphaticfilariasis
In 1997, the World Health Assembly decidedthat lymphatic filariasis should be eliminatedas a public health problem, and outlineda strategy to achieve that goal (Box 1.1).
Elimination of lymphatic filariasis means areduction of the disease incidence close tozero as a result of deliberate efforts requiringcontinued and coordinated activities. WHO’sstrategy comprises two components —interruption of transmission, and care forthose who already have the disease.
To interrupt the transmission of infection, theentire population at risk must be covered bymass drug administration (MDA) for a periodlong enough to ensure that the level ofmicrofilariae in the blood remains below thatwhich is necessary to sustain transmission.The following drug regimens are recommended,which must be administered once a year forat least 5 years or until the transmission hasbeen interrupted:
■ 6 mg/kg diethylcarbamazine(DEC) + 400 mg albendazole; or
■ 150 µg/kg ivermectin+ 400 mg albendazole.
A third option is to follow a treatment regimenusing DEC-fortified cooking salt daily for aperiod of 6–12 months.
Although vector control is not advocated asan operational component, the programmeencourages its application as part of otherongoing integrated vector control activities.This approach is primarily intended tochannel the available resources in nationalprogrammes towards achieving a high levelof drug coverage. During the last quarter of
2001, preparations were made to conduct aninformal consultation (in Geneva, Switzerlandon 29–31 January 2002) to define the role ofvector control and xenomonitoring in theGlobal Programme to Eliminate LymphaticFilariasis.
The elimination of lymphatic filariasis ispossible but it is important to act quickly.Both the combined drug regimens and theenriched salt regimen are effective. However,the combination with a second drug increasesthe microfilaricidal effect and sustains it forlonger periods. The use of two drugs, inprinciple, also reduces the risk of developmentof resistance to either drug. Because of thehuman reservoir of infection for Wuchereriabancrofti (accounting for more than 90% ofpersons with lymphatic filariasis) and bearingin mind the difficulty associated with vectorcontrol, the most effective strategy toeliminate lymphatic filariasis is to treat theentire population at risk in definedgeographical areas. This is possible becausean easy-to-use diagnostic test enablesendemic areas to be mapped rapidly, andbecause the drugs required for masscampaigns are available free of charge. Thus,all members of the population who are eligibleshould be covered by MDA, therebyeliminating the need to assess (laboriouslyand with recognized inaccuracy) the presenceof infection in each individual. In the case ofBrugia malayi and B. timori, however, a numberof other animals (particularly felines andmonkeys) may also harbour the infection.This is an important issue that must beaddressed as the elimination effort goesforward.
While the drug regimens outlined above caninterrupt transmission of the disease in thefuture, they will not cure people who arealready affected by it, although the drugs doreduce some of the symptoms. Thus, in addition
� Chapter 1 Understanding the problem

to aiming at interrupting transmission, theelimination strategy has a second objective:to prevent the occurrence of any disability or deformity that is not already present, toprevent the worsening of existing disabilitiesand deformities, and to alleviate the socialburden due to the disease.
Impairment and disability in lymphaticfilariasis are due to either lymphoedema andthe associated repeated attacks of adeno-lymphangitis, or urogenital manifestations of the disease such as hydrocoele. TheProgramme emphasizes care and support forthe patients who are affected by the chronicconsequences of lymphatic filariasis, such aslymphoedema and the urogenitalmanifestations like hydrocoele. It utilizesscientific knowledge that identifies secondarybacterial infection as a key factor for theprogression of the disease in patients withlymphoedema. Simple methods of self-careand hygiene can rid patients of their bacterialinfection, and the patients (especially withhelp from the community) can easily carryout these tasks themselves.
Preventing bacterial super-infection removessome of the factors responsible for diseaseprogression, and thus makes it possible tostop the disease. Such prevention can beeffected through regular washing (Figure 1.2)and skin care. Other simple practices, such asexercise, elevating the affected limb andwearing appropriate footwear, will alsorelieve symptoms due to lymphoedema.
During the year 2001, the Programmeattempted to identify the elements and
the process of defining a strategy for theprevention and alleviation of disabilityassociated with lymphatic filariasis. Meetingswere organized with groups that haveexperience in similar activities (e.g. HandicapInternational, International Foundation forDermatology, and International Skin CareNursing Group) and with national programmemanagers to help evolve the principles of theglobal strategy. The conceptual framework of this strategy is to be presented at the 3rd meeting of the TAG in 2002.
Finding the answers
The World Health Assembly has providedguidance on how the problem of lymphaticfilariasis, as outlined above, should be solved.Translating that guidance into practicalapplication is no small task and will requirethe active participation of the endemiccommunities, ministries of health,international organizations and the privatesector. The WHO Programme to EliminateLymphatic Filariasis pursues the scientificapproach of framing questions and trying tofind answers to questions such as:
■ What is the population at risk? ■ What is needed in the way of management,
financing and logistics? ■ How can surveillance and follow-up be
ensured?
The chapters that follow describe the progressmade so far in these matters, focusing on theactivities carried out in the year 2001.
Figure 1.2: Simple hygiene toalleviate and prevent disability.From “Lymphatic Filariasis”, acomic book for primary andsecondary schoolchildren.
10

The startof the global initiative
The WHO Programme for the Elimination ofLymphatic Filariasis (PELF) enjoys the backingof the international health community —represented by the World Health Assembly —which meets every year and brings togetherhealth ministers from 199 countries to discussmatters of public health importance and todirect the work of WHO. As mentionedabove, the World Health Assembly in 1997,considered the problem of lymphatic filariasisand decided that WHO should work towardsits elimination. That decision is embodied inresolution WHA50.29 (see Box 1.1 above).
It was clear from the outset that such a hugeprogramme would require a dynamic andflexible structure to ensure that the resourcesand the activities were well managed. Therelationship between the partners involvedin the global programme are illustrated inFigure 2.1. The activities of the variouscomponents of the global programme arediscussed below, as well as aspects offinancing, in-kind support, and logistics.
The Global Allianceto Eliminate LymphaticFilariasis
While preparing the technical basis for themassive public health undertaking to eliminatelymphatic filariasis, WHO endeavoured to bringtogether a broad coalition of partners to sharein this global effort.
A global coalition was forged between manyorganizations, each with a different mandatebut all having a common goal: to tackle thewide-ranging and complex process of scienceand practice that will result in the eliminationfrom the world of lymphatic filariasis as apublic health problem.
Early support in the task of eliminatinglymphatic filariasis came from the ministriesof health of the endemic countries and anumber of international organizations,including the Arab Fund for Economic andSocial Development (AFESD), the UnitedStates Centers for Disease Control andPrevention (CDC), and the Department forInternational Development in the UnitedKingdom (DFID).
In 1998, the coalition was given a powerfulboost when GlaxoSmithKline (formelySmithKline Beecham) announced its commitmentto collaborate with WHO in a unique partnership
Coordination/Communications/Technical Advice
CCC : GSK/WHO Collaborating Coordination Committee
EMEC : Expanded Mectizan® Expert Committee
Figure 2.1 Global Alliance to EliminateLymphatic Filariasis
80 endemic countries& more than 30 partners
working together
National Programmes to EliminateLymphatic Filariasis
WHO acts as Secretariat of the Global Alliance
Endemic communities
RegionalProgramme
Review Groups
TechnicalAdvisoryGroup
CCCEMEC
Chapter 2Supporting the Global Initiative
11

between the private sector and the publicsector to support the Global Programme toEliminate Lymphatic filariasis, by donatingalbendazole (one of the drugs used againstlymphatic filariasis) free of charge for as longas necessary. The two parties pledged to worktogether closely to undertake this massiveinternational public health effort.Subsequently, Merck & Co., Inc. pledgedto expand its ongoing Mectizan® DonationProgram for onchocerciasis (river blindness)to cover treatment of lymphatic filariasis withivermectin in all African countries where thetwo diseases occur together. The donationswill enable countries which are in need, butwhich are without the necessary resources, toacquire the drugs and to pursue their nationalelimination programmes.
These drug donations triggered a process thathas evolved continuously since its inception.To date, GlaxoSmithKline has provided morethan 58 million tablets of albendazole to WHOfor use in LF-endemic countries, and Merck &Co., Inc. has provided more than 17 milliontablets of ivermectin directly to the Africanlymphatic filariasis programmes, in additionto its donation for those areas wherePELF is being implemented in onchocerciasisco-endemic areas. The Mectizan® DonationProgram and its Expert Committee areresponsible for the approval of ivermectindonation in African countries whereonchocerciasis is co-endemic with lymphaticfilariasis.
In 2000, the Bill and Melinda Gates Foundationdonated US$ 20 million to support lymphaticfilariasis activities from 2000 to 2004. Thegrant proposal to the Bill and MelindaGates Foundation was developed byrepresentatives of most of the principalpartners in the Global Alliance and wasfinalized at a meeting of more than 20individuals representing these partnersin Atlanta, GA, USA, during the first weekof September 2000. The structure of theproposal was such that there were to befour ‘nodes’ of activity receiving funds: thatof WHO; a group based in Atlanta, USA(primarily comprising Rollins School ofPublic Health, the Centers for DiseaseControl and Prevention, and the CarterCenter); a group of nongovernmentaldevelopment organizations; and theLiverpool LF Support Centre (together with other academic partners).
WHO uses the grant to finance theimplementation of activities in the followingfields: 1) field interventions; 2) training,communication and information; and3) technical meetings, coordination andmonitoring. In addition to the endemiccountries, the Alliance has broadened toinclude more than 30 organizations fromvarious sectors of society, including thepublic and private sectors, academia,government bodies, and nongovernmentaldevelopment organizations (Box 2.1).
12

13
National Ministries of Health
� Ministries of Health of the 80 endemiccountries
International Organizations
� The World Bank � United Nations Children's Fund - UNICEF � World Health Organization - WHO
Private Sector
� Binax, Inc., USA � Merck & Co., Inc., USA� GlaxoSmithKline, UK
International Development Agenciesand Foundations
� Arab Fund for Economic and SocialDevelopment (AFESD), Kuwait
� Bill and Melinda Gates Foundation, USA� Centers for Disease Control and
Prevention (CDC), Atlanta, USA � Department for International
Development (DFID), UK � Directorate General for Development
Cooperation (DGCS), Italy � Japan International Cooperation Agency
(JICA), Japan � Ministry of Health and Welfare, Japan � Ministère fédéral des Affaires sociales,
de la Santé publique et del'Environnment, Belgium
� Ministerio de Sanidad y Consumo, Spain � Ministry of Health, Welfare and Sport,
The Netherlands
Nongovernmental DevelopmentOrganizations
� Amaury Couthino, Brazil � Global 2000 of the Task Force for Child
Survival, USA� Handicap International, France � Health and Development International
(HDI), Norway � International Foundation for
Dermatology, UK� International Skin Care Nursing Group, UK� Interchurch Medical Assistance (IMA), USA� International Volunteers in Urology, USA� The Carter Center, Atlanta, USA� The Centres for Partnerships in Health,
Australia � The Mectizan® Donation Program, USA� World Alliance for Community Health,
Canada
Academia and Research Institutions
� Ain Shams University, Egypt � Bernhard Nocht Institute for Tropical
Medicine, Germany � Chinese Academy of Preventive Medicine,
China � Danish Bilharziasis Laboratory (DBL),
Denmark � Emory University, Atlanta, USA� Institute for Medical Research (IMR),
Malaysia � James Cook University, Australia � Lymphatic Filariasis Support Centre
Liverpool School of Tropical Medicine, UK � Michigan State University, USA� Notre Dame University, USA� Universidade Federal de Pernambuco,
Brazil � Vector Control Research Centre (VCRC),
Indian Council of Medical Research, India� Washington University in St. Louis -
Barnes-Jewish Hospital, USA
Box 2.1 List of the partners of the Global Alliance to Eliminate Lymphatic Filariasis
� Chapter 2 Supporting the Global Initiative

The Global Alliance was formed duringa meeting at Santiago de Compostela, Spain,in May 2000. During this first meeting thediscussions focused on support (includingfunding) for effective country action,communication and information needs,the role of non- governmental developmentorganizations in national programmes toeliminate lymphatic filariasis, critical elementsfor successful programmes, and onmaximizing regional cooperation.
The second meeting of the Global Alliance(to be held in New Delhi, India, in May2002) will focus on empowering countriesand their people to manage public healthdevelopment and pursue poverty alleviationthrough the elimination of lymphaticfilariasis. Representatives of the GlobalAlliance will discuss national ownership ofelimination programmes, poverty alleviationand sustainable development related tolymphatic filariasis elimination, and thecommitment to global partnership as wellas national-level partnerships.
The Global Alliance to Eliminate LymphaticFilariasis can now envisage the eliminationof the disease as the focus of a widelybeneficial public health intervention,organized through existing or strengthenednational health systems. Individually, noneof these partners can eliminate lymphaticfilariasis; but by working together, andworking through the ministries of health inthe endemic countries, the goal can beachieved. Not all partners will work in everycountry, but together they will cover all theaffected countries and will have a positiveimpact on many millions of lives. Annex 1contains the reports of major internationalsupporters and partners.
14

15
� Chapter 2 Supporting the Global Initiative
The Technical Advisory Group (TAG)The TAG advises WHO on key issues (policy,strategy and operations) relevant toimplementation, monitoring of the progressand success of the elimination effort. It alsoidentifies research questions that need to beaddressed to enhance the acceptability andthe sustainability of the Programme.
During its first meeting, which was heldparallel to the meeting of the Global Alliancein Spain in 2000, the TAG examined thefollowing issues:a) indicators for monitoring programmes toeliminate lymphatic filariasis;b) disability prevention and control strategies;c) lymphatic filariasis as a childhood disease;and d) ensuring supplies of quality DEC.
The second meeting of the TAG, held inGeneva in March 2001, considered issuesrelated to: a) disability alleviation andprevention; b) verifying the absenceof infection or interruption of transmission;c) DEC supply; and d) safety monitoringof drug combinations. Following therecommendations of the TAG, WHOorganized a consultative meeting inDecember 2001 to examine the safety datathat had been collected by the Programme.A review of the accumulated data furtherreaffirmed that the co-administered drugswere safe and there was very little concernabout the safety of their wide-scale use.The side-effects observed were conventionalreactions, consistent with past experiencewith the drug combinations.
The TAG recommended that PELF shouldcritically evaluate the role of vector controlin the Programme and defined its need inspecial epidemiological situations.Accordingly, an informal consultation on
the role of vector control in PELF wasplanned for January 2002. On therecommendation of the TAG, a socialscientist has been included as a TAG member.The Chairman of the TAG collaborated closelyon all the activities of the Programme duringthe second half of 2001. In association withthe WHO Secretariat he conducted an analysisof the current priorities of the PELF. Basedon this analysis and the current needs ofthe Programme, the topics for discussionat the next TAG meeting were identified.
The regionalizationprocess
The Global and Regional ProgrammeReview Groups (GPRG and RPRG)A GPRG was set up under the drug donationMemorandum of Understanding withGlaxoSmithKline, with the task of reviewingapplications for donated drugs receivedfrom national ministries of health forlymphatic filariasis programmes. With therapid increase in programme activities, itbecame clear that programmes could bereviewed more efficiently at regional level.
The seventh meeting of the GPRG, which tookplace at WHO headquarters, Geneva,Switzerland, on 26–27 February 2001, agreedon the terms of reference of the RegionalProgramme Review Groups (RPRGs) and sixRPRGs were proposed. In the case of theSouth-East Asian and Western Pacific regions,interregional and subregional groupsof countries were created, rather than on thebasis of WHO’s regions. These groups werebased on the epidemiological distribution oflymphatic filariasis in the two regions. Box 2.2presents the terms of reference of the RPRGs.

■ Review and provide guidance to countriesin the development of their national plansof action for the elimination of lymphaticfilariasis, which are consistent with nationalpublic health policies and global andregional strategies for the eliminationof disease, and which take into considerationthe specific conditions of the region, so thatthe countries will build on their existingcapacities rather than create vertical structures.
■ Review the applications and re-applicationsfor drug donations of albendazole (andivermectin in the onchocerciasis co-endemiccountries of the regions concerned), wheresuch drugs form part of the national plansconsistent with safe and rational use andthe approved prescribing informationin all areas where lymphatic filariasis isendemic; in countries where onchocerciasisis co-endemic, the request will be forwardedto the Expanded Mectizan® ExpertCommittee (EMEC) for final authorization.
■ Review the implementation and progressof national programmes and ensureconsistency with the regional and globalstrategies and targets, and make
Box 2.2 Terms of reference of the RPRGs
recommendations to the WHO RegionalDirectors on future requests foralbendazole and ivermectin, and onscaling up the programmes in the comingyears.
■ Provide technical guidance on theimplementation of the recommendationsof the Technical Advisory Group that arerelevant to the countries of the region.
■ Identify operational research issues arisingfrom the implementation of programmesin the region, and refer them to therelevant research institutions of theregion, the Technical Advisory Group, therelevant WHO Regional Office, and theWHO Task Force on Filarial InterventionResearch.
■ Advise WHO on matters relating to theconfirmation of interruption or absence oflymphatic filariasis in the countries of theregion.
■ Advocate and support WHO MemberStates in seeking political commitmentsfrom governments and ministries of healthfor the elimination of lymphatic filariasis.
16

17
It is clear that a crucial role is going to beplayed by the Regional Programme ReviewGroups (RPRGs) in monitoring, assessing,and facilitating the progress of countryactivities.
A meeting between the chairperson of theGPRG and the chairpersons of the six RPRGswill take place in New Delhi, India, followingthe second meeting of the Global Alliance.During this meeting the modalities of howto best maintain regular communicationamong these groups will be discussed.
1. African Programme Review GroupThe first meeting of the African PRG on29–31 October 2001 in Cotonou, Benin,provided an opportunity to bring to themembers of the group the results of theoperations of the global programme toeliminate lymphatic filariasis andinformation on the activities of theTechnical Advisory Group. Members of theregional group took note of the follow-upactions taken and still outstanding inresponse to the recommendations of theGlobal Programme Review Group.
The African PRG reviewed the nationalplans for Benin, Burkina Faso, Ghana,Kenya, Nigeria, Togo, Uganda, and theUnited Republic of Tanzania. Some of theseplans had already been reviewed by theGlobal Programme Review Group for thepurpose of approving drug applications.The regional group considered its workingmethods and identified areas of operationalresearch that would be likely to result inimproving programme implementation inthe countries of the region.
2. American Programme ReviewGroup
The first meeting of the American PRG tookplace in Georgetown, Guyana, on 23 August2001. The meeting set in motion theregionalization of the albendazole applicationprocess, and identified the technical andnon-technical aspects of national plans thatcould benefit from feedback from theAmerican PRG and the TAG. The meetingreviewed the national plans for Brazil, CostaRica, Guyana, Haiti, Suriname, and Trinidadand Tobago. None of these plans had beenreviewed previously by the Global ProgrammeReview Group. Other issues highlightedduring the meeting were: the importanceof emphasizing the role of the WHORepresentatives in countries in identifyingfunding; the designation of subcommitteesto follow up on funding strategies at countrylevel; and the importance of using the WHOprocurement process as the most cost-effective mechanism for obtaining drugsand other essential tools.
3. Eastern MediterraneanProgramme Review Group
The WHO Regional Office for the EasternMediterranean (EMRO) organized the firstmeeting of the Eastern Mediterranean PRGfrom 23 to 24 December 2001 in Cairo,Egypt. The agenda of the meeting includeda review of the plans of action for the year2002; review of current global activities onthe elimination of lymphatic filariasis;review of progress in elimination activitiesin Egypt and Yemen; approval of the re-application request from Egypt and Yemenfor drug donation; and discussion on theorganization of mapping activities in Sudan.
4.
� Chapter 2 Supporting the Global Initiative

4. Mekong-Plus Programme ReviewGroup
The first meeting of the Mekong-Plus PRG,which was originally scheduled forDecember 2001, took place on 8–9 January2002 in Kuala Lumpur, Malaysia. Thisinterregional group was established to dealwith the problem of lymphatic filariasisspreading across the borders of thecountries of the WHO South-East Asia andWestern Pacific regions. Because of thecross-border migration of people, efforts toeliminate lymphatic filariasis will require thecoordinated efforts of countries from bothWHO regions. In the light of theseepidemiological concerns, an interregionalprogramme review group was establishedfor the countries of the Mekong and thesurrounding region, known as the Mekong-Plus PRG. This group consists of Cambodia,China, Lao People’s Democratic Republic,Malaysia, Philippines and Vietnam from theWHO Western Pacific Region, and Indonesia,Myanmar and Thailand from the WHOSouth-East Asian Region.
5. Indian Subcontinent ProgrammeReview Group
The Indian subcontinent PRG is composedof the countries of the WHO South-EastAsian Region that are not covered by theMekong-Plus PRG, along with Bangladesh,India, Maldives, Nepal and Sri Lanka. Thefirst meeting of the Indian SubcontinentPRG, originally scheduled for December2001, took place on 14–15 January 2002 inNew Delhi, India. This Group will play a key role in the GlobalProgramme as the major burden of filariasisis borne by countries in this region.
The Group extensively reviewed the progressbeing made by these countries and approvedthe request for albendazole for the secondround of mass drug administration (MDA)in Bangladesh and Sri Lanka, and for thefirst round of MDA in Nepal. The needfor rapid scaling-up of operations in thesecountries was emphasized.
6. PacELF Coordination and ReviewGroup (PacCARE)
The 22 Pacific island countries andterritories in the Western Pacific Region(American Samoa, Cook Islands, FederalStates of Micronesia, Fiji, French Polynesia,Guam, Kiribati, Marshall Islands, Nauru,New Caledonia and Dependencies, Niue,Northern Mariana Islands, Palau, PapuaNew Guinea, Pitcairn Islands, Samoa,Solomon Islands, Tokelau, Tonga, Tuvalu,Vanuatu, and Wallis & Futuna Islands) had,already established a lymphatic filariasiselimination programme in 1999 incoordination with the Secretariat for thePacific Community. This programme is calledthe Pacific Initiative for the Elimination ofLymphatic Filariasis (PacELF). These Pacificisland countries constituted the PacELFCoordination and Review Group (PacCARE)to review the national plans of the Pacificisland endemic countries and requests foralbendazole. The first meeting of thePacCARE was held in October 2001, and thesecond in February 2002. The PacELFheadquarters is located in Suva, Fiji, andacts as the central warehouse for supplyingalbendazole to the island countriesparticipating in PacELF.
18

19
time of the day, and gives a result within afew minutes. Annex 2 contains a list ofcountries and territories which arelymphatic filariasis-endemic. The surveyresults are plotted on the map of thecountry and, based on the results, theuncertain IUs are categorizedas endemic or non-endemic.
In January 2001, a workshop was held inBangkok in collaboration with SEAMEOTropmed, the Liverpool LF Support Centre,and WHO for the Mekong-Plus countries.Eight countries (Cambodia, Laos, Indonesia,Malaysia, Myanmar, Philippines, Thailandand Vietnam) reviewed the distribution oflymphatic filariasis in the country on thebasis of published reports and surveysundertaken by the national programmes.Implementation units, as defined by eachcountry, were categorized on the basis ofsuch information as endemic, non-endemicor uncertain (Map 3.1). A plan for furthersurveys in the uncertain areas was preparedby each country. Technical and financialassistance is being provided to the countriesin the surveys, as well as in mapping whichis currently in progress.
The first cluster of West African countries(Benin, Burkina Faso, Ghana, and Togo),which had completed the antigenaemiasurveys in 2000 were brought together in afinal data analysis workshop inOuagadougou in March 2001. The datawere cleaned, validated and entered inHealthMapper by the participants. Trainingon the spatial analysis of the data wasorganized by WHO/TDR to create thecontour maps of varying levels ofendemicity. The second phase of theworkshop included categorization of theimplementation units into those withtransmission and those without, on thebasis of the sampled villages byimplementation units and the spatial
Chapter 3Implementing the Programme
This chapter looks first at some of the major areas of activity of theProgramme to Eliminate LymphaticFilariasis (PELF), and then givesexamples of how those activities arebeing carried out within countries.
Initial assessmentand mappingof LF distribution
Objective for 2001: To strengthen thecapacities of endemic countries to assessand map the distribution of lymphaticfilariasis in preparation for mass drugadministration.
The initial assessment and mapping of thedistribution of lymphatic filariasis withinendemic countries continued to be one ofthe priorities in 2001. The principal strategyfor interrupting transmission of infection isto treat the entire ‘at risk’ population eitherwith a single administration of two drugs,given together once yearly for 4–6 years,or with DEC-fortified salt intake. Beforemass drug administration can be plannedand implemented in LF-endemic countries,implementation units (IU) need to bedefined and units where transmissionoccurs have to be identified. Based onrecently available information on theprevalence of lymphatic filariasis, IUs arecategorized as (a) endemic or with transmission,(b) non-endemic, or (c) uncertain. Furthersurveys to verify the LF status are carriedout in the “uncertain” units, preferably bydetection of antigenaemia with ICT cards inareas where W. bancrofti is endemic or bynight blood surveys in brugian filariasisendemic areas. The ICT test can be performedon a fingerprick blood droplet taken at any

analysis (Map 3.2). In the third phase of theworkshop, draft plans for implementingand monitoring PELF in those units whichwere identified as having LF transmissionwere drawn up by the participants. Theworkshop was also supported by funds fromTDR and the Liverpool LF Support Centre.
To strengthen the capacities of endemiccountries in mapping the distribution oflymphatic filariasis in preparation for massdrug administration, two workshops wereheld, one in Dakar primarily for the WestAfrican French-speaking countries(Cameroon, Central African Republic,Guinea, Mali, Niger, Senegal, and theRepublic of the Gambia), and the secondin Nairobi for the anglophone countriesmostly in East Africa (Kenya, Liberia, UnitedRepublic of Tanzania, Uganda, Zimbabweand Zambia) (Map 3.3). More specifically,these workshops aimed to present theparticipants with the standardizedmethodology for LF mapping, facilitatedthe compilation of existing information onLF prevalence, assisted the participants indeveloping a plan for LF mapping in theirrespective countries, and trained them inthe use of the HealthMapper as a tool formapping, monitoring and evaluating theimplementation of mass drug administration.
Map 3.1 Status of implementation unitsin the Mekong-Plus countries
Map 3.2 Status of implementation unitsin Benin, Burkina Faso, Ghana and Togo
Map 3.3 Status of implementation unitsin Kenya, Malawi, Uganda, UR Tanzania,Zambia and Zimbabwe
Endemic
Non-endemic
Uncertain
Endemic
Non-endemic
Uncertain
Endemic
Non-endemic
Uncertain
20

21
Progress in mapping in individual countriesis summarized in Table 3.1.
The HealthMapper, an integrated databasemanagement and mapping tool developedby WHO, is a software package which helpsusers through the following steps: choosingthe implementation units; drawing thepreliminary map of disease distributionbased on existing data; selecting samplevillages for survey, data entry and analysisof survey results; overlaying prevalencecontour maps or other relevant layers;classifying the implementation units intodifferent LF status; preparing a plan ofaction; monitoring the coverage by massdrug administration; and monitoring theimpact indicators.
Mass drug administration
Objective for 2001: To cover 25 millionpeople with MDA.
The drugs needed to interrupt transmissionof lymphatic filariasis already exist. They arealbendazole, diethylcarbamazine (DEC), andivermectin. Mass treatment calls for thedistribution of huge numbers of tablets,and hence for innovative logistics. Anexample from a small island country isdescribed in Box 3.1.
Box 3.1 Distribution of albendazoleand DEC in French Polynesia
Since joining the Pacific Programme toEliminate Lymphatic Filariasis (PacELF) as afounder member in 1999, French Polynesiahas carried out two rounds of mass drugadministration, in 2000 and 2001, achievingcoverage rates of 92% and 95% respectively.During Filariasis Week, the public healthservice and the education service jointlydistribute tablets in all schools, as well asthrough distribution points in all theislands. On Filariasis Day, which is the Fridayin filariasis week, tablets are distributed inthe streets to all adults. Distributioncontinues through public health offices andprivate chemists during the following week,and is maintained throughout the year. The DEC tablets are produced in differentcolours to denote the dosage (100 mg, 400 mg and 600 mg), and are packed inplastic bags for the major centres.Before, during and after Filariasis Week, a mass advertising campaign via the mediaprovides a constant flow of information inboth French and Tahitian.
In the African countriesCompleted In progress Planned� Benin � Kenya � Cameroon� Burkina Faso � Nigeria � Central African � Côte d’Ivoire � Tanzania, United Republic of Republic� Ghana � Gambia, the � Togo
� UgandaRepublic of the
� Guinea � Liberia� Madagascar� Malawi� Mali� Niger� Senegal� Zambia
In the American Completed In progress� Guyana � Dominican Republic� Haiti � Costa Rica� Suriname � Trinidad & Tobago
In the Eastern Mediterranean countries� Egypt � Yemen
In the Mekong PlusCompleted In progress� Thailand � Indonesia
� Myanmar� Cambodia� Laos� Philippines
In the Indian sub-continent countriesCompleted In progress� Maldives � Bangladesh
� Nepal� Sri Lanka
Table 3.1 Progress in initialassessment of LF distribution
� Chapter 3 Implementing the Programme

India
Nigeria
Myanmar
Bangladesh
Philippines
Burkina Faso
Sri Lanka
Ghana
Haiti
Tanzania
Egypt
Togo
Comoros
Pac-ELF (9 countries)
Within the Programme to EliminateLymphatic Filariasis, a total of 22 countrieshave already started mass drugadministration, as shown in Figure 3.1. Thetotal population at risk of the 22 countries is679.8 million which represents 61.8% of thetotal at-risk population in all 80 endemiccountries. The increase in the numbers ofpeople covered by MDA overall and bycountry, between 2000 and 2001, is evidentfrom Figure 3.2. and Table 3.2., respectively.The percentage of the target population(that is, the population at risk in endemiccountries) that had been targeted by MDAby the end of 2001 is shown in Figure 3.3.
Table 3.2 Population covered by MDA in 2000and 2001
PRG Region Country Population covered by MDA2000 2001
AFRICAN � Burkina Faso 431 399� Comoros 53 308� Ghana 114 947 393 677� Nigeria 159 698 675 701� Togo 51 722 342 398� United Republic of Tanzania 37 240 316 494
(excluding Zanzibar)� Zanzibar, part of UR of Tanzania 638 909
AMERICAN � Haiti 105 750
EASTERNMEDITERRANEAN � Egypt 1 759 553 2 325 724
MEKONG PLUS � Philippines 331 526 2 236 110� Myanmar 1 803 306
INDIAN � Bangladesh 808 697SUB-CONTINENT � India 13 433 322
� Sri Lanka 1 666 389
PacELF � American Samoa 11 081 29 991� Cook Islands 13 344 11 562� French Polynesia 205 000 214 149� Kiribati 46 047� Niue 1 802 1 706� Samoa 91 613 119 100� Tonga 79 969� Tuvalu 6 742� Vanuatu 154 739 155 517
Grand Total 2 932 265 25 895 967
45480
46.5
34
23.5
12
9.5
6.7
Population (millions)
No countries
mill
ion
s co
vere
d
No
of
cou
ntr
ies
0
0 0
25 50 75 100
6
2.6
2.4
1.1
0.6
0.9
Figure 3.1 Population at risk in the22 endemic countries that implementedPELF IN 2001
Egypt
Pac-ELF (9)
Togo
Sri Lanka
Tanzania
Comoros
Philippines
Ghana
Burkina Faso
Myanmar
India
Haiti
Bangladesh
Nigeria
100
79.3
41.7
24.1
16.5
10.3
9.5
8.8
0 25 50 75 100
4.5
4.2
3.4
2.5
2.5
0.8
Figure 3.3 Percentage of at-riskpopulation targeted for MDA in 2001
Figure 3.2 Progress in mass drugadministration in 2000 and 2001
5
10
15
20
25
30
5
10
15
20
25
26
2000 2001
No. Administered
3
�
22

23
33.89
44.89
3.3
22 22.2
148.98
The strategy of mass drug administration iscentral to one of the objectives of the GlobalProgramme for the Elimination of LymphaticFilariasis. This strategy not only requiresawareness-raising efforts, but also presentsa logistic challenge Figure 3.4.
Albendazole is a widely-used antiparasitic drugthat cures intestinal worm infections in children.When co-administered as a single treatmentwith either of the older anti-filarial drugs, DECor ivermectin, it enhances the ability of thesedrugs to stop the spread of filarial infection.Albendazole is donated to the programmefree of charge by GlaxoSmithKline.
DEC was developed over 50 years ago, andis inexpensive, safe and effective. A singleannual dose can reduce microfilariae forat least one year. If DEC is given in combinationwith albendazole or ivermectin, its effectivenessis enhanced and transmission can beinterrupted. Unfortunately, DEC cannot beused to treat lymphatic filariasis in most ofAfrica because of severe side-reactionswhen other parasitic infections, such asonchocerciasis, are also present. DEC costsless than US$ 0.01 per person per year.
Common edible salt can be fortified easilyand cheaply with DEC. The drug is verystable, survives cooking, and is tasteless.Small amounts taken over a period ofmonths to years can eliminate microfilariaeand interrupt stransmission completely.
A WHO audit team, in collaborationwith the National and State RegulatoryAuthorities, carried out on-site audit visitsto the manufacturers of DEC tablets andDEC starting material, to evaluate GoodManufacturing Practices (GMPs) and Good(Quality Control) Laboratory Practices, andcoordinated the validation of an HPLC assayfor DEC starting material and DEC tablets.The new HPLC assay for DEC and for evaluationof dissolution is now in USP25 (2002).Future audit visits to the manufacturers ofDEC starting material and DEC tablets havebeen planned and will be carried out in 2002.WHO procured DEC for some of theLF-endemic countries, on request.Ivermectin is a drug that is safe and easy
Figure 3.4: Advocacy for mass drugadministration. From “LymphaticFilariasis”, a comic book for primaryand secondary schoolchildren.
Figure 3.5 Shipments of drugs toLF-endemic countries in 2000 and 2001
tab
lets
(m
illio
ns)
0
20
40
60
80
100
120
140
160
Albendazole Ivermectin DEC
� Chapter 3 Implementing the Programme

Table 3.3 Shipment of drugs to endemic countries in 2000 and 2001
Region Albendazole Ivermectin DEC Albendazole Ivermectin DEC
Africa 2 318 600 3 300 000 6 847 321 21 875 000 3 150 000
Americas 475 000 470 000 1 512 500
Eastern Mediterranean 2 900 000 10 000 000 1 887 000 125 000 11 022 000
Mekong-plus 4 021 000 11 300 000 5 609 450 107 800 000
Indian subcontinent 23 100 000 28 267 523 25 500 000
PacELF countries 1 065 000 920 000 1 767 750
TOTAL 33 879 600 3 300 000 22 220 000 44 849 044 22 000 000 148 984 500
Year 2000 Year 2001
to use. A single dose quickly kills immatureforms of the filarial worms (microfilariae)within the human body. When ivermectinis used with albendazole or DEC,the transmission of lymphatic filariasisis reduced dramatically for one year.Millions of people in Africa and theAmericas are already receiving ivermectinannually for the treatment of onchocerciasis(river blindness). Merck & Co., Inc. isdonating ivermectin free of charge to theAfrican countries that are endemic for bothlymphatic filariasis and onchocerciasis, andwhere DEC should therefore not be used.The numbers of drugs shipped to endemic
countries by the Programme in 2000 and2001 are shown in Table 3.3. The massiveincrease in the number of drugs shippedbetween those two years is shown inFigure 3.5.
As can be seen from Figure 3.6, the majorpart of the Programme’s activities in massdrug administration in 2001 was concentratedin South-East Asia. This focus reflects thevast population at risk in that area. Thenext chapter describes how the Programmeassesses the population at risk and howactivities to eliminate lymphatic filariasisare implemented.
Figure 3.6 Proportion of poulation coveredby MDA in different PRG regions in 2001
Indian subcontinent
62.34%
Africa
11.18%
Americas
0.41%
EasternMediterranean
9.11%
Mekong-Plus
14.69%
PacELF
2.27%
24

25
Social mobilizationand advocacy
Objective for 2001:To provide technical assistance to countriesin order to achieve high coverage duringmass drug administration.
The high coverage rates required to reachthe goal of elimination can be achievedonly if the target populations are motivatedto receive and take the drugs that aresupplied to them.
High coverage rates need to be sustainedfor at least 4–6 years. The lower the coverageis the longer the period necessary to achieveinterruption of transmission will be. Suchsustained high coverage requires intensesocial mobilization through advocacy andeffective communication. Strong politicaland administrative commitment will engagethe population to participate actively.People need such information so that theycan act in their own interests and those oftheir children. Yet communication throughinterpersonal or group contacts, or via themass media, is still needed to motivatepeople to take the decision to accept healthinterventions.
Social mobilization is a planned processwhich enlists the support of any or all sectorsof society that can play a role in achievingan agreed social objective. To be sustainable,the process has to be rooted in the community.Planning for social mobilization begins witha situation analysis and identification of thebehavioural change required to achieve thehealth goal. The analysis identifies potentialallies and points of resistance, ways to improvethe knowledge and motivation of thebeneficiaries, effective media channels, andthe potential for community participation. An example of successful social mobilizationis described in Box 3.2.
Box 3.2 Communication forbehavioural impact: the experienceof ZanzibarIn October 2001, a first round of mass drugadministration took place in Zanzibar,United Republic of Tanzania. Zanzibarcomprises two main islands, Unguja andPemba, with a population of 941 546.Filariasis is highly endemic in both islands,with microfilaraemia ranging from 5% to30% of the adult population. A surveycarried out one week after the drugdistribution showed an overall drugcoverage rate of 76%. A key factor in achieving this high coveragerate was an active social mobilizationcampaign which started about threemonths before the mass drugadministration day (promoted as FilariaDay) and which continued until Filaria Day.The campaign focused on the behaviouralresult expected: the ready acceptance oftaking the tablet on Filaria Day. A variety ofmeans of communication were used,including:� The use of drug distributors as social
mobilizers, through two preparatory visitsto households.
� The intensive use of mass media, postersand banners.
� The active involvement of religious andpolitical leaders.
� Chapter 3 Implementing the Programme

In India, the State of Orissa recognized theneed to ensure adequate social mobilizationbefore implementing the mass administrationof albendazole and DEC. A WHOcommunications adviser visited Orissa and,following preliminary observations in villagesand discussions with officials at district andstate levels, drafted a plan forcommunication for behavioural impact(COMBI). The plan was later discussed at aworkshop in Hyderabad in May 2001(Photograph 3.2). The workshop wasattended by national and state-levelprogramme managers and communicationsexperts from different endemic states, as wellas by social scientists from research institutesand universities and media experts. Using aparticipatory approach, the workshop drafteda document highlighting the principles ofCOMBI, as well as model plans for Orissa,Tamil Nadu and Kerala. The WHOcommunications adviser subsequentlycollaborated with state programme managersand local research institutions in Orissa andTamil Nadu to draw up detailed operationalplans for model social mobilization projectsto be carried out in those two states. Withfunding from the Gates Foundation, theseprojects are scheduled to be implemented inJanuary and February 2002.
Materials for advocacy purposesPamphlets for advocacy purposes have beenproduced in collaboration with countryofficers and have been adapted to localsituations. In particular, in order to raiseawareness of the importance of ongoinglymphatic filariasis mass drug administrationcampaigns and to convey basic messages ondisability prevention and control, it wasdecided to produce a comic book, targetingschoolchildren and their families in sub-SaharanAfrican countries.A similar comic book, developed incollaboration with schoolteachers, was fieldtested in primary and secondary schools inEgypt as part of a KAP (knowledge,attitude, practice) survey. The results wereboth positive and encouraging towards theuse of this kind of material in schools, andthe book will be widely distributed. Indianofficials have seen the Egyptian comic bookand are interested in having a similar bookdeveloped for India.
The production of a package of advocacyfilms has started. Filming of mass drugdistribution, education and socialmobilization activities has already takenplace in India and the Philippines, andfilming in Africa will provide a global overviewof the programme. The end product will bea package of three films (of approximately2, 5 and 15 minutes’ duration), which canbe used in the promotion of activities toeliminate lymphatic filariasis.
Photograph 3.2 Participantsof the Social Mobilisation andCommunications Workshop,Hyderabad, India
26

27
WebsiteFollowing the distribution of a questionnaireto all interested parties to gather informationon the objectives and the intended targetaudience (speed, page size, layout, appearance,overall usefulness, site structure), as well asnavigation and content of the EliminatingLymphatic Filariasis website, the site hasbeen completely redesigned to become thewebsite of the Global Alliance to EliminateLymphatic Filariasis.
The website contains documents on theLymphatic Filariasis Elimination Programme,covering strategy, policy, project management,operational and research issues comprised ofreference materials for national programmemanagers and other national officials involvedin the Elimination Programme, relevantscientific papers covering both the publichealth and clinical health aspects of thedisease, iconographic materials, and linksto relevant partners. A crucial part of the siteis the extranet that enables partners tocommunicate with one another and exchangedata. Figure 3.7 shows a screenshot of thehome page of the website.
Preventingand limiting disability
Objective for 2001:To develop a global strategy for disabilityprevention and control.
With a view to preventing and limitingdisability, the strategy of PELF is encouragespatients with lymphoedema to practise regularskin care and hygiene and to wear appropriatefootwear. Surgery is recommended forindividuals with hydrocoele. This requirestraining of health workers, as well as healtheducation and mass communication.The comic book produced for sub-SaharanAfrican countries places great emphasison simple methods of hygiene and lifestylehabits that can contribute enormously topreventing or decreasing clinicalmanifestations of the disease (Figure 3.8).
A training module for health workers ondisability prevention and control has beenproduced.
Figure 3.7 The GlobalAlliance website
� Chapter 3 Implementing the Programme

The focus of health education is on: � thorough washing and careful drying
of the affected part of the body;� wound care;� exercise, but not during acute attacks;� elevating the affected limb; and� wearing of comfortable footwear
(i.e. open sandals rather than constrictingshoes or bare feet).
Health staff need to understand the reasonswhy patients fail to follow advice on hygieneand care, and they must be educated to listento, observe, train and encourage the patients.Much can be done at the peripheral level,and much can be achieved in disabilityprevention and limitation at very littlefinancial cost per patient by using commonlyavailable items. Protective footwear is themost expensive item, but it is relativelydurable. It is therefore important to makethe best possible use of locally-availableresources, and to guide the patient to dolikewise.
Effective prevention and limitation ofdisability requires:� practice of simple hygiene measures using
soap and water;� early recognition and prompt treatment of
entry lesions;� referral of patients with lymphoedema who
do not respond to treatment at home; and � referral of patients with hydrocoele for
surgery.
Training of physicians and health workers onthe principles of alleviation and prevention ofdisability associated with lymphatic filariasiscommenced n Bangladesh, Haiti, India, Nigeria,Philippines, Sri Lanka, Togo, and the UnitedRepublic of Tanzania. In Sri Lanka, over2 500 patients with lymphoedema underwenttreatment at the regional centres while another6 500 were treated at village health centres.In addition, it was reported that 1 876hydrocoelectomies were performed in thecountry.
Figure 3.8 From “LymphaticFilariasis” a comic book forprimary and secondaryschoolchildren.
28

29
Training
Objective for 2001:To organize the first workshop to trainprogramme managers, to finalize a trainingmodule for drug distributors, to trainhealth personnel in disability preventionand control techniques, and to commencethe preparation of a training package ondisability prevention and control forcommunity health workers.
SEARO Workshop on the Treatment andPrevention of Lymphoedema in LymphaticFilariasis, Pondicherry, IndiaA training workshop was organized from29 January to 3 February 2001 by theJawaharlal Institute of PostgraduateMedical Education and Research (JIPMER),with technical support from the WorldHealth Organization and financial supportfrom the Ministry of Health and Welfare ofthe Government of Japan. The workshopwas intended to provide senior healthpersonnel (doctors and nurses) with thecompetence required for effectiveassessment and management oflymphoedema in lymphatic filariasis. Therewere 22 participants — 10 from India and12 from other countries in the South-EastAsia Region (Bangladesh, Indonesia,Maldives, Myanmar, Nepal and Thailand).The emphasis of the workshop was on thetheoretical, practical and programmaticaspects of disability prevention and controlin LF. The training followed a problem-solving approach and a substantial amountof time was spent on interaction with theparticipants.
SEARO-WPRO Training Workshop forProgramme Managers of LymphaticFilariasis Elimination Programme, KualaLumpur, Malaysia The workshop was organized from 22to 27 October 2001 by the Institute of Medical
Research (IMR), Kuala Lumpur, Malaysia,with technical support from the World HealthOrganization and financial support fromthe Bill and Melinda Gates Foundation,the Liverpool LF Support Centre, and SEAMEO-TROPMED (Southeast Asian Ministers ofEducation Organization - Tropical Medicineand Public Health Network). The aim ofthe workshop was to train programmemanagers and WHO country desk officersfrom the WHO South-East Asian andWestern Pacific Regions how to develop,conduct and evaluate filariasis eliminationprogrammes that respond to the needs oftheir countries. The training was interactiveand, wherever possible, the participantsworked with national data which they wereasked to bring with them to the workshop.The main topics covered included: situationanalysis, health mapping, plan for interruptionof transmission, plan for disability control,surveillance, social mobilization, trainingand capacity-building, and monitoring andsupervision (see Photograph 3.3).
To follow up this training of nationalprogramme managers, an average ofUS$ 5 000 per country was made availableto the Regions to enable nationalprogrammes to organize workshops atdistrict level in their respective countries.These funds were allocated to the WHOSouth-East Asia and Western PacificRegional Offices.
Training module for programmemanagersA two-part training module (Learner’s Guideand Tutor’s Guide) for national programmemanagers has been developed and will bepublished in June 2002. The module wastested in the SEARO-WPRO Training Workshopfor Programme Managers of LymphaticFilariasis Elimination Programme, in KualaLumpur; comments and suggestions weregathered from the participants and tutors,
� Chapter 3 Implementing the Programme

and these are being incorporated in therevised version. The Learner’s Guide containstechnical principles, exercises and suggestionson the best way to achieve the learningobjectives, and the Tutor’s Guide is designedto give support to the trainers, providingpractical guidance on the organization andpresentation of the training course,suggesting a step-by-step approach totraining, and listing the basic resourcesrequired for optimal running of the course.
Disability prevention and controltraining package for communityhealth workersSimple guidelines for lymphatic filariasis
patients, together with materials to train
trainers at community level are being
developed. The materials will be field-tested
in pilot training workshops during 2002,
following a series of surveys that will be
carried out in Burkina Faso, Togo, and the
United Republic of Tanzania (including
Zanzibar). Feedback from the pilot
workshops will be incorporated and the
training materials will then be used in other
countries. The preparation of these materials
will involve thorough examination of the
professional profile of health workers
involved at community level.
Training materials for drugdistributorsA training module for drug distributors
(Learner’s Guide and Tutor’s Guide) has been
completed. The module was extensively
field-tested during several mass drug
administration campaigns, and is ready
to be printed and distributed. It can be used
equally well for basic training and for
refresher training.
An information sheet for drug distributors
has been produced and will be made
available to health personnel involved in
mass drug administration campaigns.
Photograph 3.3 Participants of the SEAR-WPRO training Workshop for ProgrammeManagers of Lymphatic Filariasis Elimination programme, Kuala Lumpur, Malaysia
30

31
Research
The Programme to Eliminate LymphaticFilariasis, like any other public healthprogramme to control or eliminate adisease, needs to include a strongoperational research component in order tobe sustainable and successful. Strategies ortechniques can always be improved, andproblems will always develop that need tobe resolved. The programme, in associationwith TDR, has promoted research in keyareas that are relevant to the Programme’simplementation and monitoring.
The Programme has been concerned withthe problem of low coverage during theMDAs and has accorded high priority todeveloping cost-effective drug deliverystrategies for achieving high and sustainedtreatment coverage (based on studies inGhana, India, Kenya, Myanmar, and Vietnam)and also to examining the strategies foreffective drug delivery in urban areas (India).
Where onchocerciasis and lymphatic filariasisco-exist, there is need for the developmentof an integrated drug delivery strategy.Studies in Ghana and Mali are examiningthis issue. Since advocacy and communicationare vital elements for the eliminationprogramme, strategies to enhance drugdelivery are ongoing in India. Long-termtransmission studies to answer key questionsrelating to the impact of MDA in achievingelimination for the main vector-parasitecomplexes are being undertaken in Ghana,India, Kenya, Mali and Papua New Guinea.Methods for community-based managementof lymphoedema and related adenolymphangitisare being examined in Ghana, Kenya, Mali,Nigeria, and the United Republic of Tanzaniawith TDR support.
Strategies and tools for monitoring andevaluating filariasis elimination programmesare being developed in laboratories inGermany, Ghana, Indonesia, Malaysia,Netherlands, and Uganda. A rapidassessment method for identifying areaswhere there is a risk of loa-associatedencephalopathy after ivermectinadministration was developed after studieswere completed in Cameroon and Nigeria.
The efficacy and safety of the albendazole+ ivermectin co-administered regimen indecreasing microfilaraemia was the subjectof studies conducted in Ghana, Kenya andZanzibar. In addition, the pharmacokineticsof regimens using two drugs simultaneouslywere studied in Ghana and India.
Finally, in the area of basic and strategicresearch the Programme is supporting studieson filarial genomes and drug discovery,especially targeting filaria-specific amino-acylt-RNA transferases.
Monitoring PELFand information system
The monitoring of programme implementationis an important component which needs tobe carried out at all levels — national,regional and global. The ProgrammeManager's Guidelines* provide a frameworkof the country’s information needs, togetherwith formats for collection of the relevantdata. Countries are encouraged to modifythe formats, if required, to match localdata collection systems. However, to ensurestandardization across countries for compilationof information at regional or global levels,a standard annual reporting format was
* Preparing and Implementing a National Plan toEliminate LF: a Guideline for Programme Managers.
� Chapter 3 Implementing the Programme

developed in consultation with theProgramme Review Group and the TechnicalAdvisory Group. Countries were expected tosend the reports of each calendar year by28 February of the following year.A summary of the reports received fromcountries which initiated PELF in 2000 and2001 is given in Table 3.4.
Countries were advised to report on theprogress made in their respective programmesto eliminate lymphatic filariasis as a publichealth problem.
As the programme progresses, the formatwill undergo revision. National programmemanagers were advised and encouraged toclosely monitor the implementation of theiractivities (Table 3.5 and Figure 3.9).
Table 3.4 Reports from countries that initiated PELF in2000 and 2001
Implemented Submitted Implemented Submitted MDA in 2000 annual report MDA in 2001 report
PRG Region for 2001 for 2001
African 4 2 6 6
American 0 0 1 1
Eastern Mediterranean 1 1 1 1
Mekong-Plus 1 1 2 2
Indian subcontinent 0 0 3 3
PacELF 6 6 9 7
Total 12 10 22 20
Number of countr ies
Table 3.5 Analysis of reporting on PELF activities(21*annual reports received)
Reported on No. of reports %
Initial assessment 18 85.71%
Sentinel sites identified 17 80.95%
Baseline mf only 10 47.62%
Baseline CFA only 2 9.52%
Baseline mf and CFA (both) 4 19.05%
Baseline hydrocoele 7 33.33%
Baseline elephantiasis 10 47.62%
Total population of IUs 19 90.48%
Number covered as reported by IUs 18 85.71%
Coverage cross-checked 7 33.33%
* United Republic of Tanzania submitted two annual reports:one for the mainland and one for Zanzibar
Figure 3.9 Reported and observeddrug coverage*
Bangladesh
Zanzibar (TZ)
Myanmar
Haiti
India
Population (millions)� Reported� Observed
0 20 40 60 80 100
* Drug coverage calculated as percentage of peopleadministered the drugs over total population in IUs
32

33
Information flowTo help countries in compiling andpresenting programme-related andepidemiological data, especially throughmaps and charts, the HealthMapper(software developed by WHO/CSR) wasmodified to include a module for PELF. Asmost national programme managers haveaccess to computer systems, theHealthMapper will be a simple and usefultool for programme managers to assessprogramme implementation (See “InitialAssessment and Mapping of LF Distribution”,page 19).
Systems for adverse eventmonitoringThe programme has put in place two systemsfor monitoring the safety of the co-administered drugs. The first is an activesurveillance system which requires countriesinitiating mass drug administrationprogrammes to document the occurrence ofany side-effects (usually resulting from killingof microfilariae by the drug and subsequenthost response to dying parasites) in the first2000 to 3000 individuals receiving the drug.A standard questionnaire to record the possibleadverse drug reactions (ADR) is provided tocountries and data from this monitoring arebeing collected by the PELF at WHO. A reviewof the accumulated data showed that theco-administered drugs were safe and there wasvery little concern about their safety throughwide-scale use. The side-effects seen wereconventional reactions, consistent with pastexperience with these combinations. Inaddition, the reactions were qualitatively andquantitatively similar to those reportedpreviously and seem to be related to thetherapeutic effects of the co-administered drugs.
The second system, which is to be continuedfor the life of the programme, is “passive”reporting of any serious adverse experience(SAEs) in subjects following co-administereddrug treatment. SAE report forms have beendeveloped, in consultation with the two donorpharmaceutical companies (GlaxoSmithKlineand Merck & Co., Inc.), for reporting SAEsassociated with DEC + albendazole regimens(Annex 3) and for reporting SAEs associatedwith the ivermectin + albendazole regimens(Annex 4). SAE reports are required to beforwarded to the drug regulatory authoritieswithin 15 days. WHO receives these SAE reportsconcurrently with the concernedpharmaceutical companies and interacts closelywith them and the local health authorities.During the year 2001, no SAE was observed orreported in any country implementing MDA.
� Chapter 3 Implementing the Programme

Activities in regionsand countries
1. African Programme Review GroupOf the 46 countries in the African Region,39 are LF-endemic. In total, approximately420 million people are considered to beat risk. Filariasis and onchocerciasis areco-endemic in 28 countries.
In 2001, 6 of the 39 countries with LFinitiated mass drug administration.Over 3.3 million people were coveredby MDA using ivermectin + albendazolein Burkina Faso, Ghana, Nigeria, Togo andthe United Republic of Tanzania, and usingDEC + albendazole in the Islamic FederalRepublic of the Comoros.
Other countries, such as Benin, Kenya,Madagascar and Uganda initiated planningand training activities related to PELF.The plans and application for drugs havebeen approved for Benin, Kenya andUganda, and the drugs have been shippedto these countries.
BeninStudies carried out in 1983 and 1995 in thesub-prefecture of Comé indicated a diseaseand microfilariae prevalence of 24.6% and46.3%, respectively. In the year 2000 anationwide survey was completed in villagessampled in each sub-prefecture. Based onthe survey, the following departments wereidentified as endemic — Mono, Ouémé, Zouand Atacora. The total population in thesefour departments is 4.2 million, all of whomare at risk. A national plan for PELF wasdeveloped and has been approved bythe Programme Review Group and theMectizan® Donation Program. Drugs forthe first round of treatment have beenprovided to Benin. Financial support for theprogramme has been provided by theLiverpool LF Support Centre.
Burkina FasoInitial assessment of the distribution oflymphatic filariasis was completed inBurkina Faso in 2000. According to thesurvey findings, which were later confirmed,all 53 health districts (implementation units)in the country were endemic. The entirepopulation of the country, estimated at12 million, is considered to be at risk forlymphatic filariasis.
Following the initial assessment of theLF situation in the country, the Ministryof Health (MoH) launched a national planto eliminate lymphatic filariasis. A nationaltask force was set up and a dynamic andefficient coordinator for PELF was nominated.A plan for initiating and scaling up PELFactivities was submitted to WHO and theMectizan® Donation Program for review andsupply of drugs. The request was favourablyconsidered and drugs were made availableto Burkina Faso, targeting 558 552 peoplein four implementation units in the Gaouaregion in the south. WHO and the LiverpoolLF Support Centre provided financialassistance for the start-up operational costsin the first year. During the first round ofMDA from December 2001 to January 2002,a total of 431 399 people receivedivermectin + albendazole. The reporteddrug coverage was 77.2% (range: 71.6–80.6%)— see Map 3.4. The drug administrationwas carried out by community drugdistributors after two days of training. Thebase-line survey carried out in the sentinelsite in Gaoua had a prevalence of microfilariaeof 11.4% (N° of mf+/N° of slides read).Another sentinel site in Dano (village of Gora)had a prevalence of mf of 14.2%.The Ministry of Health is also collaboratingwith Handicap International in thealleviation and prevention of disability
34

35
caused by lymphatic filariasis. Knowledge,attitude and practice (KAP) studies areunderway for the formulation of thestrategy and inclusion in the national PELF.
WHO staff from HQ and AFRO providedtechnical assistance to the nationalprogramme in planning the activities and inestablishing, with the MoH team, thestrategies for good monitoring andevaluation of the PELF activities. Financialassistance for the first round of MDA wasprovided by WHO and the Liverpool LFSupport Centre.
The Islamic Federal Republic of theComorosWHO provided technical support to developthe national plan and to train healthprofessionals to undertake mass drugadministration. All the 600 000 inhabitantsin the Islamic Federal Republic of theComoros are considered to be at risk for LF,as shown in the mapping of LF which wascompleted in 2000. The entire population isdistributed among three islands: Moheli,Grand Comore and Anjouan. In July 2001, atotal of 53 308 people in two islands(Moheli and Grand Comore) were coveredby MDA using DEC + albendazole. Thecoverage for the two islands was reportedto be 85.7% (range: 81–92%) — see Map3.5. Financial assistance was provided by agrant from the Arab Fund for Economic andSocial Development.
� Chapter 3 Implementing the Programme
Map 3.4 Burkina Faso: LF endemicitystatus and MDA coverage 2001
Map 3.5 Comoros: LF endemicity statusand MDA coverage 2001
Endemic
Non-endemic
Uncertain
Below 65 %
65-80 %
Above 80 %
MDA coverage
Endemic
Non-endemic
Uncertain
Below 65 %
65-80 %
Above 80 %
MDA coverage

GhanaMapping for lymphatic filariasis was carriedout in 2001. The population at risk in Ghanawas estimated to be approximately 6.57million in 41 districts. The first round ofMDA was begun in August 2000 in AhantaWest district, covering 114 947 persons. InJanuary and February 2001, a further fourdistricts with 393 677 people were coveredby MDA using ivermectin + albendazole; thereported drug coverage ranged between63% and 75%, with an average of 68.5%for all five districts(Map 3.6). Baseline surveys carried out in 21sentinel sites indicated a microfilariaprevalence of between 11% and 41%, andcirculating filaria antigen (CFA) between30% and 49%.
In addition to the Ministry of Health, theCatholic Medical Missions Board (CMMB)supported part of the GhanaianProgramme. Additional resources wereprovided by Health and DevelopmentInternational (HDI), the Liverpool LFSupport Centre, WHO, and a grant from theGates Foundation (received through HDI).
KenyaSix of the coastal districts are currentlyknown to be LF-endemic, microfilariaprevalence ranging between 9% and 28%.The prevalence of hydrocoele ranges from10% to 40% and that of elephantiasis from6% to 10%. A plan for nationwide mappinghas been prepared and a list of villages forthe survey identified. The Ministry of Healthsubmitted a plan for initiating aprogramme to eliminate lymphatic filariasis,starting in one district (Kilifi) and expandingto cover other areas. The plan was reviewedand approved by the Programme ReviewGroup and drugs for MDA were shipped toKenya. Further assistance was provided byWHO for preparing a district-level actionplan. The first round of MDA is expected totake place in July 2002.
Map 3.6 Ghana: LF endemicity statusand MDA coverage 2001
Endemic
Non-endemic
Uncertain
Below 65 %
65-80 %
Above 80 %
MDA coverage
36

37
MadagascarMadagascar is one of the four most highlyLF-endemic countries in the African Region.In December 2001, at the request of theMinister of Health, WHO sent a team tosupport the Ministry in preparing a strategyto eliminate lymphatic filariasis in the country. The Ministry of Health came to the conclusionthat mass drug administration using DEC-fortified salt might be the most appropriatestrategy to reach the population at risk. Onlythe district of Tuleare in the west, whichproduces local salt, might have a problembecause the iodized salt programme is havingdifficulty. This district could be covered byadministering a single dose of DEC +albendazole once every year.
NigeriaNigeria ranks third in the world, after Indiaand Indonesia, in terms of population at risk,which is estimated at about 80 million,distributed in Local Government Areas (LGA).LF mapping was carried out in two statesand nationwide mapping was proposed.The first round of MDA in September 2000,using ivermectin + albendazole, covereda total of 159 948 people; the averageobserved coverage was 56.7% (with thetotal population in the implementationunits (IU) as denominator). In 2001, 675 701people received ivermectin + albendazole. Atotal of 22 sentinel sites have been selected.The pre-MDA baseline circulating filarialantigenaemia ranged from 5% to 64%.
A KAP study identified the misconceptionsand superstitions that attempted to explainthe disease etiology. A negative attitudetowards men with hydrocoele was observed.While patients with hydrocoele consult bothmodern and traditional medical practitioners,lymphoedema and elephantiasis patientsmostly consult traditional practitioners.The programme in two states is supportedby the Carter Center.
TogoNational mapping of the entire country wascompleted in 2000. The population at riskwas estimated to be 1.1 million, distributedin 7 prefectures. The first round of MDA inApril 2000 covered 51 722 persons (reportedcoverage 80.6%) in Binah prefecture. In thesecond round in April 2001, 342 398 peoplereceived ivermectin + albendazole in threeprefectures (Binah, Toné and Kpendjal); theaverage reported coverage rate was 74.7%(range: 65–80.6%) — see Map 3.7. The pre-MDA baseline survey carried out in threesentinel sites (one each in Binah, Toné andKpendjal) showed the prevalence ofmicrofilaraemia to be between 0.6% and10%, that of circulating filaria antigen (CFA)between 5% and 31.3%, hydrocoelebetween 0.2% and 1%, and elephantiasisbetween 0.2% and 2%. Training of healthpersonnel at provincial and district levelswas organized for mass drug administrationand for the prevention and alleviation ofdisability.
Map 3.7 Togo: LF endemicity status and MDA coverage 2001
Endemic
Non-endemic
Uncertain
Below 65 %
65-80 %
Above 80 %
MDA coverage
� Chapter 3 Implementing the Programme

UgandaSurveys undertaken by the Vector ControlDivision of the Ministry of Health hadidentified four endemic districts in Uganda.Mapping in the rest of the country is inoperation. The Ministry of Health prepareda plan for treatment in the identified LF-endemic districts, starting with two districts(Lira and Katakwi) in the first round.Since both districts were also endemic forsoil-transmitted helminths and Lira forschistosomiasis as well, the plan for thesedistricts included helminth control. Afterthe first round of ivermectin + albendazolecovering the entire population for LF,a second round with albendazole (after sixmonths) will be implemented for school-agechildren. The national plan has beenapproved by the Programme Review Groupand the Expanded Mectizan® ExpertCommittee. Ivermectin and albendazolehave been shipped to Uganda. At therequest of the Ministry of Health, WHOprovided technical assistance to developdistrict action plans and training.Sensitization of local political andadministrative personnel in the two districtswas carried out. The district teams havebeen trained and an action plan developedfor MDA in March 2002. Financial supportfor the programme has been provided bythe Liverpool LF Support Centre and WHO,with the Ministry of Health bearing the restof the cost.
United Republic of TanzaniaMainland. Mapping the distribution of LF isin progress in the mainland. Of the 101districts, 48 have been surveyed, of which43 are endemic. The surveys in 53 districtsare expected to be completed by 2002.The at-risk population is estimated to be2.6 million. In the first round of MDA inOctober 2000, a total of 32 240 personsreceived ivermectin + albendazole (reportedcoverage, 76%).
The second round in 2001 targeted 6 districts,and reports from four showed that 316 494individuals were covered (average coverage,59.6%; range, 55.2–64.4%) — see Map 3.8.Reports from the other two districts are stillawaited. Care was given to 150 patientswith lymphoedema, and 100 operations forhydrocoele were carried out in one district-level health facility.The United Republic of Tanzania (mainland)programme received financial assistancefrom the Gates Foundation through theNGO node.
Zanzibar. The entire population of 941 546is considered to be at risk of LF. The firstround of MDA was carried out in October2001 using ivermectin + albendazole in 12districts. The number of people covered was638 909 (reported coverage, 67.9%; range,62–77%) — see Map 3.8. An extensiveassessment of actual drug coverage wascarried out in 39 random sites andinterviews with 26 143 individuals indicateda coverage rate of 76%. Pre-MDA baselinesurveys in two sentinel sites indicated aprevalence of microfilaraemia from 7% to18%, that of hydrocoele from 1.4% to7.8%, and lymphoedema from 2.2% to 8%WHO provided technical assistance to theMinistry of Health in Zanzibar in planningthe social mobilization campaign andmonitoring the drug coverage. Financialassistance to the Zanzibar programme wasprovided through WHO by the GatesFoundation.
Map 3.8 United Republic of Tanzania:LF endemicity status and MDA coverage 2001
Endemic
Non-endemic
Uncertain
Below 65 %
65-80 %
Above 80 %
Unknown
MDA coverage
38

39
2. American Programme ReviewGroup
Seven countries in this region are consideredLF-endemic: Brazil, Costa Rica, DominicanRepublic, Haiti, Guyana, Suriname, andTrinidad and Tobago, with a total of 7.6 millionpeople at risk in the LF-endemic areas.
Dominican RepublicThe Dominican Republic is currently carryingout mapping of LF-endemic units in thecountry. At present, 10 out of 14 provincesare endemic and surveys are in progress infour. The country submitted a national planand a request for drugs. The programmewas reviewed and supplies of drugs have beenshipped for initiating an MDA programme. The programme involves partnership with alocal regional hospital in the south-west totreat lymphatic filariasis patients and to actas a reference unit for the region. A surgicaltraining course was organized in which11 urologists participated, including 4 fromHaiti. An Agreement for the Performanceof Work has been signed with the “InstitutoDermatologico y Cirugia de la Piel” for themanagement of lymphoedema.The Institute will act as a reference healthcentre as well as training centre for fieldpersonnel in lymphoedema management.The routine activities of field staff willinclude detection of lymphoedema patients.A field epidemiologist is carrying out acensus of patients with lymphoedema in thecommunity, identifying local organizations,and organizing groups for lymphoedemamanagement.
Financial assistance to the DominicanRepublic is provided through the Atlantanode by the Gates Foundation.
GuyanaMapping of LF distribution in Guyana hasbeen completed, following the lot qualityassurance sampling method. Antigenpositive persons were found in all 10regions; however antigen positive personsin the interior generally reported periods ofexposure in Georgetown or other locales onthe coast.
Financial assistance was provided for theGuyana mapping exercise through theLiverpool LF Support Centre, and CDC inAtlanta provided ICT cards and technicalassistance.
HaitiHaiti has completed the initial assessmentand mapping of endemic areas.The number of "communes" to be chosenas implementation units is probably around73. The population at risk for the wholecountry was estimated at 6 million.The first round of MDA in Leogane inOctober 2001 covered 105 750 people withDEC + albendazole (reported coverage,70.5%); the observed coverage in sentinelsites was 61.9% — Map 3.9. Evaluationof the microfilarial density in the areas coveredby MDA showed a reduction of 50%.A national plan for Haiti is being developed.
Map 3.9 Haiti: LF endemicity statusand MDA coverage 2001
Endemic
Non-endemic
Uncertain
Below 65 %
65-80 %
Above 80 %
MDA coverage
� Chapter 3 Implementing the Programme

3. Eastern MediterraneanProgramme Review Group
The endemic countries in this region areEgypt, Sudan and Yemen. Egypt is the onlycountry which has been implementing anational programme to eliminate lymphaticfilariasis since 2000. Yemen initiated LFdistribution mapping and planned to carryout MDA in two districts. Egypt and Yemenreceived financial assistance for programmeimplementation with a grant, through WHO,from the Arab Fund for Economic and SocialDevelopment.
EgyptAccording to surveys that were carried out,the population at risk is currently 2.41 million.The first round of MDA in September 2000targeted the entire population at risk andcovered 1 759 553 people (reported coverage,96.4%). The second round with DEC +albendazole in September 2001 covereda total population of 2 325 724 in all178 endemic villages in 25 districts (reportedcoverage, 96.4%) — see Map 3.10. Pre-MDAbaseline surveys were carried out in twosentinel sites and spot-check sites in eachdistrict. The baseline prevalence ofmicrofilaraemia ranged from 0.2% to 4.2%in the sentinel sites and the diseaseprevalence ranged from 1% to 11.5%.
YemenAt the request of the Yemeni Ministry ofHealth, technical assistance was provided bya WHO consultant to help in training andmapping the distribution of lymphaticfilariasis. Of the 284 districts, 11 areconsidered endemic and 5 are uncertainand need verification. The remaining 268units are considered non-endemic. In 2001,the Ministry of Health planned to startMDA in 2002 in two implementation units,with a total target population of 52 000.
Map 3.10 Egypt: LF endemicitystatus and MDA coverage 2001
Endemic
Non-endemic
Uncertain
Below 65 %
65-80 %
Above 80 %
MDA coverage
40

41
4. Mekong-Plus ProgrammeReview Group
In this region there are 11 endemic countries:Brunei Darusalaam, Cambodia, China,Indonesia, Korea, Lao People's DemocraticRepublic, Malaysia, Myanmar, Philippines,Republic of Thailand, and Vietnam.
IndonesiaIndonesia is home to all three strains offilariasis — W. bancrofti, B. malayi and B. timori.Recently a rapid assessment survey, oflymphoedema and hydrocoele, undertakenthrough a questionnaire indicated anestimated 150 million people at risk in20 out of 23 provinces. This puts Indonesiain second place, after India, in terms ofpopulation numbers at risk. While extensivedata on microfilarial prevalence are availablefrom past surveys, there are still gaps in areaswhere the LF status needs to be assessed.A further operational challenge for programmeimplementation is posed by the numerousislands that make up the country.
At the request of the Indonesian Ministry ofHealth, a WHO consultant and staffcollaborated with the national programmein identifying the implementation units anddrawing up a phased plan, starting with1 million population in 2002. The Ministryof Health finalized and submitted a planto WHO for review by the Mekong-Plus PRG.The plan and the request for drugs havebeen approved.
MyanmarMyanmar has an estimated 46 millionpopulation at risk. The mapping of LFdistribution is in progress; 153 townshipsout of a total of 324 are endemic,22 non-endemic, and 149 still uncertain andtargeted for surveys. In November 2001,MDA was started in ten townships (totalpopulation: 1 939 964), of whom 1 803 306were covered (average reported coverage,93%; range, 91–97%) — see Map 3.11. The coverage was cross-checked by teamsfrom the national level in 8 sites byinterviewing 14 995 individuals; the averageobserved coverage was 74.3% (range,75.8–92.9%, except for one site with 13.6%).Subsequently, the defaulters in this last area(13.6%) were covered. The treatment givenwas a combination of DEC + albendazole.The pre-MDA baseline surveys carried outin four sentinel sites showed a prevalenceof microfilaraemia between 1.1% and 7.1%;the microfilaria (mf) density ranged from115 mf/ml to 675 mf/ml.
Map 3.11 Myanmar: LF endemicitystatus and MDA coverage 2001
Endemic
Non-endemic
Uncertain
Below 65 %
65-80 %
Above 80 %
MDA coverage
� Chapter 3 Implementing the Programme

PhilippinesThe Philippines has designated municipalitiesas the implementation unit for MDA. Thereare 1566 municipalities in the country; 290are considered endemic and 545 non-endemic;surveys are in progress to assess the 731municipalities in the uncertain category.The population currently at risk is estimatedat 23.5 million. MDA was initiated in 2000and covered 331 526 persons in 26 implementationunits (average reported coverage, 83%).In 2001, a total of 2 236 110 received DEC +albendazole (average reported coverage, 73.2%)— see Map 3.12. Mass drug administrationwas mostly organized through Filaria HealthFairs, organized by the health services with
the full participation and ownership of thecommunities. The local government supportedthe Filaria Health Fair and approved theallocation of funds for a Filaria Day eachyear for the next four years. In some areas anational immunization- day-type of approachis adopted for mass drug administration.
Thirty health staff have been trained in theprevention and alleviation of disabilityassociated with filariasis at the provincial level.
Patients with lymphoedema are given adviceon disability control and patients withhydrocoele are referred to district/provincial/regional hospitals for surgery.
Map 3.12 Philippines: LF endemicitystatus and MDA coverage 2001
Endemic
Non-endemic
Uncertain
Below 65 %
65-80 %
Above 80 %
MDA coverage
42

43
5. Indian SubcontinentProgramme Review Group
Half the global population at risk for LF livein five countries in this group —Bangladesh, India, Maldives, Nepal and SriLanka. Three of these countries initiatedMDAs in 2001.
BangladeshThe population at risk of LF in Bangladesh iscurrently estimated at 34 million. Out of 64districts, 12 are known to be endemic.Additional data on the target populationwill come from the mapping of LF which isin progress and is expected to be completedby 2002. In November 2001, MDA wasinitiated in the Panchagarh district with apopulation of 846 880, of whom 808 697received DEC + albendazole (reportedcoverage, 95.5%) — see Map 3.13. TheMinistry of Health organized a cross-checkof the reported drug coverage, which foundthe coverage in sentinel sites to be 93%.The MDA was carried out by door-to-dooradministration in the presence of healthand family welfare field staff andvolunteers. Drugs were not left with familymembers for absentees or for later intake.To increase the coverage, the drugs werealso administered in schools, colleges,madrasas (Koranic schools), mosques,cinema halls, markets, shopping complexes,etc. by volunteers and scout leaders. Eachinvestigator covered 120 to 150 persons ina day. MDA was completed in ten days.To achieve high coverage, the communitieswere mobilized through an information,education and communication (IEC) campaignand the programme was launched by theSpeaker of the National Assembly and theDirector-General of Health Services.
Fifteen physicians from district andsubdistrict (upzila) levels of Panchagarhwere trained in 2001 on disabilitymanagement, e.g. washing of limbs and
exercise for lymphoedema, which they willpractise in district and subdistrict hospitalsfrom January 2002. It is planned to train75 field staff in disability management inJanuary 2002. Financial assistance for theprogramme was provided by WHO andfor social mobilization by Aus-AID and theLiverpool LF Support Centre.
IndiaWith an estimated population at risk of 454million in 261 districts and with 22.5 millionindividuals with filarial diseasemanifestations (14 million with hydrocoeleand 8.5 million with lymphoedema/elephantiasis), India is the most LF-endemiccountry in the world. In 1997 the Indianprogramme initiated a revised strategybased on annual single-dose administrationsof DEC, which targeted 40 million of thepopulation at risk in 13 districts. In 2000,the programme planned mass drugadministration with DEC + albendazole,which targeted a population of 20 millionat risk in nine districts (six in Tamil Nadu,two in Orissa, and one in Kerala), in
Map 3.13 Bangladesh: LF endemicitystatus and MDA coverage 2001
Endemic
Non-endemic
Uncertain
Below 65 %
65-80 %
Above 80 %
MDA coverage
� Chapter 3 Implementing the Programme

collaboration with the Indian Council ofMedical Research. In February 2001, a totalof 13 433 322 people received a combinationof DEC + albendazole in 6 districts of TamilNadu and 1 district of Kerala (average reportedcoverage, 88%); the observed coverage insentinel sites was 59.3% — see Map 3.14.The other districts were covered by MDAusing DEC alone.
In view of the big difference betweenreported and observed coverages, thenational programme, in collaboration withWHO, organized a workshop on socialmobilization in May 2001 (see “SocialMobilization and Advocacy” above).Technical support was provided by a WHOconsultant to plan for social mobilization inOrissa and Tamil Nadu for the next round ofMDA in 2002.
Sri LankaOut of a total population of 18.9 million,nine million are considered to be at risk forLF. Eight of the 25 districts are endemic andnine are non-endemic. Since 1999, all eight
endemic districts have been carrying outsingle-dose MDA with DEC alone at six-month intervals. Following the launch ofWHO’s global programme to eliminatelymphatic filariasis, Sri Lanka planned thephased implementation of annual single-doseadministrations of DEC + albendazole,starting in 2001 in the Colombo district(population, 2.1 million). In May 2001, thiswas carried out on 1.7 million people, witha reported coverage of 76.7%, — see Map 3.15.Seven other districts continued with onlyDEC administration. For the next round inJune 2002, it is planned to scale up the MDAin order to cover the entire populationof 9 million at risk using DEC + albendazole.
For the prevention and alleviation of disabilityassociated with filariasis, Sri Lanka trained50 health staff at a national-level workshop.In 2001, 2666 filarial patients were cared forat the central Anti-Filaria Headquarters andanother 6856 at 14 different health centres.A total of 1876 patients with hydrocoelewere operated as part of routine surgicalmanagement.
Map 3.15 Sri Lanka: LF endemicity statusand MDA coverage 2001
Endemic
Non-endemic
Uncertain
Below 65 %
65-80 %
Above 80 %
MDA coverage
Endemic
Non-endemic
Uncertain
Below 65 %
65-80 %
Above 80 %
MDA coverage
Map 3.14 India: LF endemicity statusand MDA coverage 2001
44

45
6. PacELF Coordinationand Review Group
The population at risk in this region is estimatedat 4.13 million, distributed in 16 endemiccountries (American Samoa, Cook Islands,Marshall Islands, Fiji, French Polynesia, Kiribati,Micronesia, New Caledonia, Niue, Palau, PapuaGuinea, Samoa, Tonga, Tuvalu, Vanuatu, andWallis & Futuna ). Papua New Guinea is thecountry with the highest estimated at-riskpopulation — around 2 million — i.e. 50%of the total population at risk in the region.In 2001, nine out of the 16 countries at riskin this region — designated as PacELF(Pacific Elimination of Lymphatic Filariasis) —implemented MDA and other PELF activities.By the end of 2001, at least 850 000 peoplewere covered by MDA.
American SamoaAmerican Samoa was one of the firstcountries that started the PELF. Theprevalence of LF was assessed to be 16.5% by ICT cards. At the beginning of 2000, 11 081 people out of a total population of 46 757 inhabitants accepted mass drugadministration with DEC + albendazole(reported coverage, 23.7%). In September2001, a total of 29 991 people were coveredby MDA, with a reported coverage of 52%.
Cook IslandsThe first MDA was started in 2000 for thewhole country. Out of a total of 18 034inhabitants, 13 344 were covered by MDA,with a reported coverage of 74%. In thesecond round in February 2001, 11 562 personsreceived DEC + albendazole, with a reportedcoverage of 64.7% of the total population.
French PolynesiaThis country, with a population of 230 000,is LF-endemic. In March 2000, some 205 000people were covered by MDA, with areported coverage of 93.2%. In March 2001,
214 149 people received DEC + albendazole,with a reported coverage of 95.1%.
KiribatiThe first MDA round in PELF was started inAugust 2001 with a population of 85 778 at risk. In 2001, 46 047 individual wereadminestered DEC and albendazole.
NiueNiue started the first MDA round in PELFin 2000 for the whole population of 1913inhabitants. The treatment offered wasDEC + albendazole in a single dose (reportedcoverage, 94%). The second round of MDAwas in February 2001, wherein 1 706 witha reported coverage of 89.2%.
SamoaIn 2000, a total of 91 613 people were coveredby MDA, with a reported coverage of 96.4%.In October 2001, a total of 119 100 peoplewere covered by MDA with a reportedcoverage of 68.4%.
TongaThe whole country is considered to beLF-endemic. The first MDA round (DEC +albendazole) in April 2001 covered a totalof 79 969 people (reported coverage, 81.6%).
TuvaluThe whole country is considered to beLF-endemic. In the first MDA in August 2001,an estimated 6 742 individuals in nine islandsreceived DEC + albendazole drug coverage 81.2%.
VanuatuThe country’s 186 678 inhabitants wereconsidered to be at risk of LF. The first MDA(DEC + albendazole) in June 2000 covered154 739 people. In the second round in June2001, a total of 155 517 individuals receivedthe drugs (reported coverage, 83.3%).
� Chapter 3 Implementing the Programme

Table 3.6 A comprehensive overview of MDA coverage in 2001
Africa Burkina Faso 558 552 431 399 77.2% 90.4%**
Comoros, IslamicFederal Republic of 62 239 53 308 85.7% nd
Ghana 574 834 393 677 68.5% nd
Nigeria nd 675 701 nd
Togo 458 337 342 398 74.7% nd
United Republic ofTanzania (mainland) 675 087 316 494 71.4% nd
United Republic ofTanzania (Zanzibar) 941 546 638 909 67.9% 76%
Americas Haiti 150 000 105 750 70.5% 61.9%
Eastern Mediterranean Egypt 2 412 170 2 325 724 96.4% nd
Mekong-Plus Philippines 3 054 445 2 236 110 73.2% nd
Myanmar 1 939 964 1 803 306 93.0% 74.3%
Indian Sub-continent Bangladesh 846 880 808 697 95.5% 93%
India 15 267 529 13 433 322 88.0% 59.3%
Sri Lanka 2 171 386 1 666 389 76.7% nd
PacELF American Samoa 57 291 29 991 52.3% nd
Cook Islands 18 034 11 562 64.1% nd
French Polynesia 225 300 214 149 95.1% nd
Kiribati 46 047 nd
Niue 1 913 1 706 89.2% 99%**
Samoa 174 140 119 100 68.4% nd
Tonga 98 036 79 969 81.8% nd
Tuvalu 8 307 6 742 81.2% nd
Vanuatu 186 678 155 517 83.3% nd
22 countries 29 882 668 25 895 967
* Drug coverage calculated as percentage of persons administered the drugs over total population in IUs
**: Observed coverage is for drug coverage among eligible population
nd: data not reported in annual report
Totalpopulationof all IUs
targeted forMDA in 2001
Populationreportedto haveingestedthe drugs
Asreported by
IUs
As observedin cross-check
sites
Drug coverage %*
Region PRG Country
46

Fighting diseasesof poverty
The pursuit of health as an ethical objectivefor individuals and societies is unquestionable.However, health is also a fundamentallynecessary component of development,which scholars like Amartya Sen have madeclear in their research (Development asFreedom, 1999). Poverty is not simply a lackof money or income: it is a lack of accessto choices, resources and opportunity.The WHO Commission on Macroeconomicsand Health (Investing in Health forEconomic Development, December 2001)places disease control and eliminationsquarely and centrally within the frameworkof “any comprehensive development strategy”.In this perspective, the Commission argues,the control or elimination of diseases suchas lymphatic filariasis becomes not simplya “good thing to do”, nor even a laudableobjective of health sector policy — it is acentrally important factor in the eliminationof barriers to overall development and topoverty alleviation. Such diseases are thecauses of both poverty and non-developmentand they compound the problems of povertyalleviation and development the longer theypersist. Actions such as those of the GlobalAlliance to Eliminate Lymphatic Filariasismust break that connection and bothstrengthen national health systems so thatthey can deliver sustainable public health,and improve very concretely the humandevelopment potential at individual, family,community and national levels.
On the individual and family level, accordingto extensive research, good health is theprimary desire of people since it providesthe basis on which they can gain a reasonablelivelihood and achieve a decent quality oflife. On the societal level, unless quality ofhealth is set as a priority goal, the potentialof society for socioeconomic growth and
profitable participation in the globaleconomy is subject to severe, long-lastinglimitations. The pursuit of health is anessential goal of development per se.
Eliminating lymphatic filariasis will freemillions of people in low-income countriesfrom the threat or the effects of adebilitating and potentially disfiguringdisease. Caring for those who are alreadyinfected will reduce untold suffering. But can this be done? The answer is anunequivocal yes. Earlier programmeseliminated filariasis in Japan, and fromlarge parts of China, Malaysia, the Republicof Korea, and certain islands in the Pacific.Lymphatic filariasis has also disappearedfrom endemic areas in south-east USA andnorth-east Australia. The fact that thesesuccesses were achieved even without thecurrently available, much improved tools forcontrolling and monitoring the infectionaugurs well for the future success of thefilariasis elimination efforts now beingundertaken.
Comprehensivehealth planning
The Global Programme to Eliminate LymphaticFilariasis is the focal point of a wide-rangingand beneficial public health intervention.Because progress towards the elimination oflymphatic filariasis requires approaches andimplementation techniques which are notpurely medical, it is essential to involvesectors other than health in implementingand managing a successful programme. Forexample, social mobilization is a vital factorand requires input from the media, schools,religious organizations and communityleaders. This calls for collaboration betweenthe ministry of health and a host of othergroups. However, from the point of view ofoverall vision, management and guidance,
Chapter 4Facing future challenges
47

the process of eliminating lymphatic filariasismust be embedded in the existing structureof national health systems.
Moreover, with a programme of which theduration will cover a period of years andwhich depends so strongly on localcommitment and persistence, it is necessarythat the national health systems shouldboth “own” and benefit from theprogrammes to eliminate lymphaticfilariasis. Similarly, unless the nationalauthorities are committed to the goal ofeliminating LF, it will not be given thepriority it merits in terms of nationaldevelopment goals per se.
Collaboration with other programmes
The drugs used to control lymphaticfilariasis have a broad anti-parasitic effect(Table 4.1). One collateral benefit of theprogramme will be to control or preventhookworm in teenage girls and women.Hookworm is linked not only to anaemia,but also to growth stunting and cognitivedeficiencies in children. Stunting, in turn, isa predisposing factor for low birth weightin the next generation of infants. As far as
children are concerned, most of thepathophysiology of worm infections isnutritional in nature. Protein-energymalnutrition, iron deficiency anaemia,vitamin A deficiency, and iodine deficiencydisorders affect hundreds of millions ofpeople, especially children, and girls andwomen of childbearing age.
Albendazole, one of the drugs used by theGlobal Programme to Eliminate LymphaticFilariasis, is also used by the Programme onSoil-Transmitted Helminth Infections, eitheras albendazole or as mebendazole, analmost identical molecule. The Programmeon Soil-Transmitted Helminths distributesalbendazole or mebendazole generally onceor twice a year to schoolchildren,depending on the worm load. Control ofsuch helminths will also greatly benefit thehealth and social welfare of women(especially their pregnancy outcomes), theirfamilies, and future generations. Potentialcollaboration between the two programmesis focused on the administration ofalbendazole. The lymphatic filariasisprogramme administers albendazole (plusDEC or ivermectin, depending on thegeographical area), and six months later theprogramme on soil-transmitted helminthinfections provides the drug to schoolchildren.
Ivermectin Albendazole
Ascaris 100% Ascaris 100%
Strongyloides 95% Strongyloides 45%
Enterobius 85% Enterobius 85%
Trichuris 10-50% Trichuris 40-60%
Hookworm 0-20% Hookworm 95%
Larva migrans 100% Larva migrans 80%
Onchocerciasis 95% Cysticercosis*/Hydatids*
Lice 100% Giardia* / Trichomonads*
Scabies 100% Micro- / Crypto-sporidia*
* Requires more than 1 dose of albendazole
Table 4.1 Broad anti-parasite effectiveness of drugs used to control LF
48

49
Challenges to collaboration include thedifferent target populations and the necessarysynchronization of activities, especially as inmost situations there are different focalpoints at the national level: the lymphaticfilariasis programme targets the totalpopulation (except very small children andpregnant women) and may be implementedin LF-endemic areas in the country, while thehelminth programme targets only school-agechildren. Another difference between theprogrammes concerns the felt needs of thecommunity. In the helminth programme,teachers act as drug distributors and healtheducators, and the children are the main“captive population”. In contrast, the lymphaticfilariasis programme has to rely on socialmobilization to convince apparently “healthy”people that they should take the drugs.
In the Onchocerciasis Programmes in Africa,the administration of ivermectin to thepopulations at risk in the hyper- andmeso-endemic areas takes place once a year.Lymphatic filariasis is more widespread thanonchocerciasis since the latter is endemiconly in the river basins whilst LF occurs inmany other places. Thus, where LF isconcerned, there is a need to cover the totalpopulation of the implementation unitstargeted for MDA. However, since theOnchocerciasis Programme has beenoperating for a number of years and hasestablished a system for community-directed ivermectin treatment, the LFElimination Programme can take advantageof this experience by synergizing the drugadministration activities in co-endemic areasat sub-national level and similarly, withother programmes. Collaborative effortsalong these lines are underway in Benin,Burkina Faso, Ghana, Nigeria and Togo.
Targets for 2002and beyondTo achieve the goal of eliminating lymphaticfilariasis as a public health problem by 2020,transmission needs to be reduced to a pointwhere the 5-year-cumulative incidence inchildren born after initiating MDA in thearea is below 1 per 1000 by the year 2015.The five-year period from 2015 to 2020 isreserved for surveillance in these last areas.
MappingMapping the distribution of lymphaticfilariasis within endemic countries is thefirst priority. Knowledge of endemiclymphatic filariasis through implementationunits and their geographical distributionwill lead to better and more accurateassessment of the population at risk and theburden of disease in a country. Thisinformation is essential to enable ministriesof health to carefully plan nationalprogrammes to eliminate lymphatic filariasisand estimate the resources required. Recentexperience in Burkina Faso and Togoconfirmed that estimates of populationsat risk could change substantially aftercompletion of mapping. The populationat risk in Burkina Faso almost doubledcompared with the pre-mapping estimates.It is planned to complete such mapping inmost countries by 2005. This would requireplanning for the surveys following thestandard operational guidelines andensuring the supply of quality antigendetection card tests. For areas wherebrugian filariasis is endemic, the surveys willhave to be undertaken using night bloodsurveys un til the recently-developedantibody detection test kits arestandardized for use in community surveysand are available on a commercial basis.
� Chapter 4 Facing future challenges

Interruption of transmissionThe Programme for the Elimination ofLymphatic Filariasis has made a good startand is on a firm footing. Yet the challengesfacing it are enormous (Fig. 4.1). Thenational programmes need to scale up tocover at least 350 million people at risk bythe end of 2005 (Fig 4.2). The major challengein such up-scaling will be respectively in theAfrican region, the Indian Subcontinent andthe Mekong-Plus area (Figs. 4.3 to 4.8). Thechallenge is to strike a careful balance betweenscaling up the programmes to cover entireat-risk populations within countries whichhave already initiated programmes to interrupttransmission, and extending support toendemic countries which have not yetinitiated an elimination programme. It maybe necessary to rapidly expand the programmesalready initiated so as to cover the entireat-risk population and to make a significantepidemiological impact in the shortest periodof time. The decision will depend on thepolitical will and capacity of those countriesto scale up and on the part of those who willinitiate new national programmes in the nearfuture. The key would be to implementprogrammes that achieve the highest drugcoverage possible which would requirecloser monitoring and impact assessmentthan that currently carried out.
Figure 4.1 Ratio between populationat risk covered in 2001 and remainingpopulation to be covered in the22 countries that implemented PELF
Figure 4.2 MDA up-scaling requiredin the next three years
Figure 4.3 MDA up-scaling required inthe next three years in the African region
Figure 4.4 MDA up-scaling requiredin the next three years in the Americas
India
Nigeria
Myanmar
Bangladesh
Philippines
Burkina Faso
Sri Lanka
Ghana
Haiti
Tanzania
Egypt
Togo
Comoros
Pac-ELF (9)
20012000 2002 2003 2004 20050 0
10
20
30
40
50
60
N°
of
cou
ntr
ies
N°
of
cou
ntr
ies
mill
ion
s co
vere
d/t
arg
eted
mill
ion
s co
vere
d/t
arg
eted
50
100
150
200
250
300
350
400
3 ■
▲
▲
▲
▲
■
26
74
141
229
350■ No. Countries
No. AdministeredNo. forecast
■ Covered by MDA ■ Remaining
20012000 2002 2003 2004 20050
10
0
2
4
6
8
10
12
14
16
18
0.36
▲
■
3.2
16.1
21.6
32
48.5
■ No. CountriesNo. AdministeredNo. forecast
■
20
30
40
50
60
▲
▲
▲
■
N°
of
cou
ntr
ies
mill
ion
s co
vere
d/t
arg
eted
20012000 2002 2003 2004 20050
1
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
0.105■
0.105
1.65
2.65
3
5.65■ No. CountriesNo. AdministeredNo. forecast
2
3
4
5
6
▲
▲
■
▲
▲
▲▲
▲
�
0 25 50 75 100
▲
■
▲
■
▲
50

51
Alleviation and prevention ofdisability associated with LFThe alleviation and prevention of temporaryand permanent disability associated withLF is an integral component of nationalprogrammes to eliminate lymphaticfilariasis. However, this component, whichtargets those persons with LF-associateddisabilities, has not progressed much inmost countries. Although the managementof patients has been defined and severalhealth personnel have been trained in theseprocedures, programmes to eliminatelymphatic filariasis need to provide all LFpatients with access to home-based long-term care and decentralized health servicesfor hydrocoelectomies. Further, there is a needto recognize and reduce the social, economic,cultural and psychological setbacks thatpatients with lymphatic filariasis suffer.Again, the key would be to integrate suchservices within the health system so thataccess to those services are available atcommunity level where they are required most.
Figure 4.5 MDA up-scaling requiredin the next three years in the EasternMediterranean region
Figure 4.7 MDA up-scaling required in thenext three years in Mekong-Plus region
Figure 4.8 MDA up-scaling required inthe next three years in Pac ELF region
N°
of
cou
ntr
ies
mill
ion
s co
vere
d/t
arg
eted
20012000 2002 2003 2004 20050
1
0
1
2
3
1.8■
2.3
3
3.9
4.4
5.5■ No. CountriesNo. AdministeredNo. forecast
2
3
4
5
6
▲
▲
■
▲
▲
▲
Figure 4.6 MDA up-scaling required inthe next three years in the Indian region
N°
of
cou
ntr
ies
mill
ion
s co
vere
d/t
arg
eted
20012000 2002 2003 2004 20050
50
0■
15.9
36
80
133.5
198.5
■ No. CountriesNo. AdministeredNo. forecast
100
150
200
250
0
1
2
3
4
5
6
▲
▲
■
▲
▲
▲
N°
of
cou
ntr
ies
mill
ion
s co
vere
d/t
arg
eted
20012000 2002 2003 2004 20050
100.33
■
3.7
16.27
31.17
52.17
87.17
■ No. CountriesNo. AdministeredNo. forecast
0
1
2
3
4
5
6
7
8
▲
▲
■
▲
▲
▲
20
30
40
50
60
70
80
90
100
N°
of
cou
ntr
ies
mill
ion
s co
vere
d/t
arg
eted
20012000 2002 2003 2004 20050
0.5 0.478■
0.64
0.85
1.7
4.1
3.5
■ No. CountriesNo. AdministeredNo. forecast
0
2
4
6
8
10
12
14
16
18
▲
▲
■
▲
▲
▲
1
1.5
2
2.5
3
3.5
4
4.5
■
▲
■
▲
■
▲
■
▲
� Chapter 4 Facing future challenges

Financial resourcesBased on projection and estimates fromnational control programmes, at leastUS$ 100 million will be needed to scale upLF elimination activities at country level tocover a population of 350 million at risk ofLF by 2005. These funds would cover areassuch as social mobilization, activities relatedto training, mass drug administration,monitoring and evaluation and supply of DEC.
Ways and means toachieve the targets� The Global Alliance must generate
political commitment at the national andsubnational levels and societal awarenessto support the efforts needed to cover thetotal population at risk in endemiccountries. The national and localauthorities in the endemic countries musthave real ownership of the programme.
� Fortunately, the programme benefits fromthe support of members of the GlobalAlliance. GlaxoSmithKline will continue todonate albendazole free of charge untilthe disease is eliminated. Merck & Co., Inc.will expand the Mectizan® DonationProgrammes for onchocerciasis to coverthe countries co-endemic with lymphaticfilariasis and targeted for mass drugadministration in all the countries in
Africa where both diseases occur. Partnersfrom the public sector (such as DFID-UK,the Arab Fund for Economic and SocialDevelopment, the Ministry of Health andSocial Welfare of Japan), from the privatesector (such as the Bill and Melinda GatesFoundation) and academia (such as theLymphatic Filariasis Support Centre, Liverpool)have provided assistance in cash to fundthe start of both the global and the countryprogrammes. Annex 1 contains the reportsof major international supporters andpartners which show the extent of theircommitment to the Global Programmeto Eliminate Lymphatic Filariasis.
� Global Alliance members will seek toobtain the additional funds needed frombilateral agencies and private sources —while making a special effort to identifyInternational Financial Institutions (IFI)/World Bank funds which are alreadyavailable and could quickly be appliedto activities in the Global Programmeto Eliminate Lymphatic Filariasis (GPELF).
The Global Alliance has achieved a greatdeal since it met in Santiago de Compostela,Spain, in 2000. The future should be devotedto moving ahead quickly and efficiently withthe actions needed to achieve the goal theGlobal Alliance has set itself – particularly interms of scaling up national programmes.
52

Arab Fund for Economic andSocial Development (AFESD)
The AFESD is an Arab regional financialinstitution, whose objectives are to assistmember countries* in eliminating developmentconstraints, increasing absorptive capacityand achieving higher rates of growth; andto foster economic integration and cooperationamong Member countries. Its function is toassist the economic and social developmentof Arab countries through:■ financing economic and social
development projects, giving preferenceto overall Arab development and to jointArab projects;
■ financing private sector projects in MemberStates by providing all forms of loans andguarantees to corporations and enterprisespossessing juridical personality andparticipating in their equity capital, aswell as providing other forms of financingand furnishing the requisite financial,technical and advisory services;
■ forming or participating in the equitycapital of corporations possessing juridicalpersonality for the implementation andfinancing of private sector projects inMember States;
■ establishing and administering special fundswhose purpose is compatible with that ofthe Arab Fund, and whose resources areprovided by the Fund or other sources;
■ encouraging the investment, directly orindirectly, of private and public capital ina manner conducive to the developmentof the Arab economy; and
■ providing expertise and technical assistancein the various spheres of economicdevelopment.
The AFESD supports country activities in theWHO Eastern Mediterranean Region includingdisease detection, mapping, disabilityprevention and control activities, andlogistical support.
Reports of major internationalsupporters and partners
An
nex 1
AtlantaIn 2001 the Atlanta Node was establishedwith funds from the Bill and Melinda GatesFoundation as a collaborative effort of theLymphatic Filariasis (LF) Support Center ofEmory University, the Centers for DiseaseControl and Prevention and the CarterCenter. During that year these collaboratingorganizations developed and coordinatedactivities that included both programmaticinitiatives ("model programmes" in threecountries) and thematic activities in threespheres of expertise (economics, monitoringand evaluation, and morbidity/disabilitymanagement).
Model programmesSince the twin goals of the LF EliminationProgramme (interrupting transmissionthrough mass drug administration [MDA]and alleviating disability) are so distinctlydifferent, melting these two activities intosingle national programmes where bothcomponents complement each other providesa formidable, but essential challenge.In 2001 the Atlanta Node's CDC and Emorystaff worked closely with the Ministriesof Health in the Dominican Republic andGuyana to develop ‘model programmes‘incorporating both components effectivelyand across the entire countries. In theDominican Republic disability alleviationactivities are being integrated with an MDAbased on the yearly single-dose, two-drugtreatment approach, while in Guyana, thedisability component is being integratedwith an MDA based on the alternativestrategy of using DEC-fortified table/cookingsalt throughout the country. In 2001, bothcountries completed their strategic plans,mapped the distribution of infection, initiatedtraining programmes for disability management,laid the groundwork for MDAs beginning in2002, and established regional intercountrylinkages facilitated through PAHO.
53

The model programme in Nigeria- supported by the Carter Center, the FederalMinistry of Health and the Ministries of Healthin Plateau and Nasawara States - has adifferent purpose. Since LF and onchocerciasisoverlap in endemicity, the principal purposeof this project is to demonstrate the feasibilityand cost-effectiveness of adding (i.e., piggy-backing / integrating) LF-eliminationprogramme elements to those already wellestablished and on-going in the AfricanProgramme for Onchocerciasis Control.In 2001, the Nigerian programme expandedits combined treatment efforts (withivermectin and albendazole) to reach a totalof 675,400 individuals in all 12 endemic localgovernment areas (LGAs) of these two States.In addition, more than 800 childrenparticipated in a survey that will be usedas baseline for monitoring the MDA impacton reducing LF transmission; concurrententomological studies, carried out withassistance from CDC, aimed to developtechniques to measure the MDA impact ontransmission entomologically; and a needsassessment was conducted to determinethe surgical requirements for repairingthe urogenital damage caused by LF in men.
EconomicsProgramme costing, cost-effectiveness andcost-benefit are essential for sustainingcountry and donor investment in the GlobalProgramme to Eliminate LF. In 2001, theAtlanta Node's Emory staff developed theresearch agenda for economic studies to beconducted in the Gates grant-funded activities.Because of the necessity to use consistenteconomic methods across countries, first-year activities focused on the developmentof standard protocols (for programmecosting and cost-effectiveness analysis),training programmes (in programme costing),and measures of effectiveness of LFprogrammes in terms of health status (i.e.,‘quality-of-life’ indicators). Studies were
completed in Haiti, and protocols weredeveloped for Dominican Republic, Guyana,Egypt, Nigeria and Papua New Guinea.
Monitoring and evaluationMonitoring and evaluation is an absolutelyessential element in national programmesto eliminate LF. Only by having strong M&Ecan these programmes document the successof their activities and, even more importantly,identify programme elements in need ofstrengthening. The goal of the AtlantaNode is to provide support to nationalLF programmes to ensure their ability tomonitor and evaluate activities in accordwith the recommendations of the Guide forProgramme Managers entitled “Preparingand Implementing a national Plan toEliminate Lymphatic Filariasis” (versionfor countries that are co-endemic withonchocerciasis and those that are notco-endemic – WHO/CDS/CPE/CEE/2000.15and 16). In 2001, the Node’s activities includedstreamlining the M&E component of theGuide, developing specific M&E guidelinesfor countries using the DEC-salt MDA strategy,drafting an assessment protocol and strategyto identify barriers or potential barriers toprogramme monitoring that could limit theabilities of countries to provide the essentialoutcome data needed at both national andGlobal Programme levels, creating an ‘e-group’to share in attending to the Programme'sM&E needs and activities, and working withscientist colleagues to refine and makeavailable effective monitoring tools fordetecting parasite antigen and DNA.
An
nex
154

55
Morbidity and disabilitymanagementClinical management of filarial disease isthe essential element around which theentire disability-alleviation pillar of nationalLF elimination programmes is built. TheAtlanta Node represents a particularlystrong focus of clinical expertise in lymphaticfilariasis and, indeed, has a long andunparalleled experience in the support,development, organization, and teachingof courses to train health workers at alllevels in both the clinical and public healthmanagement of lymphoedema andhydrocoele. In 2001 the Node’s CDC staffcompleted a definitive manual forlymphoedema management, as well asother video and printed training materials,and it supported the initiation of trainingactivities in Haiti, Guyana, DominicanRepublic, India and Brazil. The beginningsof a network to link the fledgling disabilitymanagement programmes of recent traineeswere also developed.
Department for InternationalDevelopment (DFID)of the United KingdomThe Department for International Development(DFID), a UK Government department,is responsible for promoting developmentand reduction of poverty, and its currentfocus is to contribute to the halving ofthe proportion of people living in extremepoverty by 2015. Associated targets includebasic health care provision and universalaccess to primary education by the same date.
DFID seeks to work in partnership withgovernments committed to these targets,with business, civil society and the researchcommunity. DFID also works with multilateralinstitutions such as the World Bank, UnitedNations agencies such as the World HealthOrganization, and the European Community.
Reports of major international supporters and partners
DFID is helping to ensure the process ofchange brings benefits to all people,particularly the poorest, and for this reasonis a strong supporter of lymphatic filariasiselimination.
Bill and Melinda GatesFoundationIn November 2000, the Foundation madea generous contribution of US$20 milliontowards the elimination of LF. Funds areheld pending disbursement in a Trust Fundin the World Bank.At a meeting in early 2001, the groupsparticipating in the use of the grant,comprising the Atlanta USA group(LF Support Center of Emory University,Centers for Disease Control and Preventionand Carter Center), the LF Support Centre,Liverpool, UK, WHO and the Non-GovernmentalDevelopment Organizations group (led byInterChurch Medical Assistance), agreed onthe following strategic outline for the useof the Gates grant:■ demonstration projects to show interruption
of LF transmission; to move towards nationallevel coverage; to develop, implement andevaluate Disability Prevention strategies;and to evaluate cost-effectiveness
■ to ensure national momentum by providingsupport to countries for mapping andcountry scale implementation of ELFprogrammes
■ to ensure global momentum through adevelopment strategy covering regionalization,increase in the number of partners,advocacy and leverage of additional funding
■ evaluation and monitoring of thedemonstration projects, the countryprogrammes and the partnershipdevelopment.
The implementation of the Gates grant isnow in its second year and the Foundationhas expressed its satisfaction with thecurrent level of progress.

An
nex
1
GlaxoSmithKline (GSK)Since 1998, GSK has been playing a majorrole in the Global Alliance to Eliminate LF.Working closely with WHO headquartersand Regional Offices, as well as the Ministriesof Health in countries, GSK is an active andinvolved partner. The company providestens of millions of albendazole treatmentsto communities, and more than $1 millionin cash grants to other Alliance partnerseach year. In addition, GSK has a dedicatedLF Team of five full-time staff who supportthe global effort. GSK believes that, in additionto donating drugs and funds, it has manyprivate-sector management skills that its staffcan contribute to the planning and deliverywork of the Alliance.
GSK is fully committed to the long-term LFelimination programme and realizes thatthe work is still in its early phase. By theyear 2010, if all goes according to plan,more than 600 million community preventiontreatments will be provided each year in over80 participating endemic countries. GSK hasset no time limits or special conditions on itsparticipation. The company does not makeany decisions about selecting countries orcommunities to be treated — it leaves thisto the WHO-appointed regionalProgramme Review Groups. GSK also worksclosely with the Mectizan® DonationProgramme in Atlanta, USA, in a collaborationthat provides a simple harmonized approachfor drug requests from the countries of sub-Saharan Africa where LF and onchocerciasisco-exist.
In 2001, GSK produced an LF advocacy videoentitled "LF - The Patients Perspective",which has been made widely available toAlliance partners.
Lymphatic FilariasisSupport Centre, Liverpool,United Kingdom The Centre, which is situated within theLiverpool School of Tropical Medicine,benefits from the School’s experience inriver blindness control programmes and hassubstantial links with LF endemic countries.The Centre also has an extensive researchportfolio and technical background on thefilarial parasites and their mosquito vectors.
The Centre’s role is to provide advice,funding, liaison and facilitation to eliminatelymphatic filariasis. It acts as a key interfacebetween science and operations byfacilitating activities on mapping in Africaand South-East Asia, supporting operationalresearch with NGDOs and co-founding, withthe WHO/World Bank/UNDP SpecialProgramme for Research and Training(TDR), priority research activities forevaluation and monitoring.
56

57
Mectizan® Donation ProgramDuring the past year there has been significantexpansion of activities in the LymphaticFilariasis Section of the Mectizan® DonationProgram (MDP). The position of AssociateDirector for Lymphatic Filariasis was filledin August 2001 by Dr Nana A.Y. Twum-Danso.Since joining the MDP, she has been activelyworking on streamlining the operations ofthe Lymphatic Filariasis Section andstrengthening the partnership withMerck & Co., Inc., GlaxoSmithKline, WHO,and the Ministry of Health personnel in LF-endemic countries. In the first year, theMectizan® Donation Program and WHOdeveloped an integrated application processto meet the needs of countries that areco-endemic with onchocerciasis and LF.In 2000, the provisionally establishedExpanded Mectizan® Expert Committee(EMEC) approved initial applications forivermectin and albendazole from theProgramme to Eliminate Lymphatic Filariasis(PELF) in Ghana, Togo, Nigeria, and theUnited Republic of Tanzania. Continuingapplications for these four countries wereapproved in 2001, as well as initial applicationsfrom Benin, Burkina Faso, Uganda, and Yemen.
Non-Governmental DevelopmentOrganizations (NGDOs)Two NGDOs, Health & Development Internationaland Interchurch Medical Assistance supportedmass drug distributions by National LFElimination Programmes in Ghana andTanzania during 2001 as a result of fundingreceived from the Gates Grant/ World BankTrust Fund project. The two NGDOs, alongwith support of other bilateral and NGDOpartners, were also able to help strengthenNational LF Coordination Offices, and providenew equipment, technical support andfunding for awareness-raising activities, insupport of both mass drug administration(MDA) and disability alleviation and prevention,for LF elimination in these countries.
Reports of major international supporters and partners
GhanaGhana reached approximately 394,000 peoplewith mass drug administration, in 5 of the35 endemic districts during 2001. The planis to reach approximately 1.9 million peoplein 14 districts during 2002, and 4 millionpeople in 20 or more districts during 2003.This rapid expansion is resulting from strongpolitical and local popular demand forthe LF Elimination Programme. Health &Development International (HDI), andCatholic Medical Mission Board (CMMB) arethe two main NGDOs currently supportingactivities in Ghana, with CMMB having takenon disability alleviation and mass drugadministration activities for the entire UpperWest Region. HDI supports the national LFelimination secretariat, as well as disabilityalleviation and prevention activities at thenational level.
TanzaniaTanzania’s Programme is being managed bythe National Institute for Medical Research ofTanzania. The Programme treated 635,000persons in six districts in 2001, with MDAtaking place in October. This was anachievement of approximately 75% of thetargeted population. The programme wasalso able, with the assistance of financialsupport of the Gates Foundation and WorldBank, through the NGDO Node and otherpartners, to complete the development ofprocedures and materials for supporting theNational Programme. The NGDO Nodesupport also enabled the Programme toconduct 12 training sessions for district-levelpolitical leaders and medical personnel,with 60 persons trained. Financial supportenabled Programme personnel to make25 field trips during the year for purposesof programme assessments, baseline datacollection and monitoring of programmeimplementation activities.Partners to the Programme include InterchurchMedical Assistance, The LF Support Centre

An
nex
1
of the Liverpool School of Tropical Medicine,DFID-UK, Michigan State University, TheWorld Health Organization, GlaxoSmithKlineand the Mectizan® Donation Program.
Support of other NGDOsEncouraging additional NGDOs to join theLF elimination effort is a key task for whichthe NGDO Node members have taken onparticular responsibility, stimulated by theGates Foundation funding for this purpose,although all Alliance members areencouraged to do the same. InternationalVolunteers in Urology (IVU) was (along withCMMB mentioned above), the first majorNGDO to join the original group of agencies,offering to help improve technical expertisein the management of the diseases urogenitalmanifestations, through efforts by its membersin many countries. To facilitate recruitmentof new NGDOs, GlaxoSmithKline (GSK)hosted an initial meeting of NGDOs, in theirPhiladelphia office during October 2001.
58

An
nex 2
African PRG Dominican RepublicAngola GuyanaBenin HaitiBurkina Faso SurinameBurundi Trinidad and TobagoCameroon Eastern Mediterranean PRGCape Verde EgyptCentral African Republic SudanChad YemenCongo Mekong-Plus PRGCôte d'Ivoire Brunei DarussalamDemocratic Republic of Congo CambodiaEquatorial Guinea ChinaEthiopia IndonesiaGabon Lao People's Democratic RepublicGhana MalaysiaGuinea MyanmarGuinea-Bissau PhilippinesComoros Republic of KoreaKenya VietnamLiberia ThailandMadagascar Indian subcontinent PRGMalawi BangladeshMali IndiaMauritius MaldivesMozambique NepalNiger Sri LankaNigeria PacELF PRGRéunion American Samoa Rwanda Cook IslandsSao Tomé and Principe FijiSenegal French PolynesiaSeychelles KiribatiSierra Leone Micronesia (Federated States of)The Gambia New CaledoniaTogo NiueUganda Papua New GuineaUnited Republic of Tanzania SamoaZambia Solomon IslandsZimbabwe TongaAmerican PRG TuvaluBrazil VanuatuCosta Rica Wallis and Futuna
List of lymphatic filariasis endemic-countries and territories by RegionalProgramme Review Groups
59

An
nex 3
SERIOUS ADVERSE EXPERIENCE REPORTfor the
Global Lymphatic Filariasis Treatment ProgramWhere the Combination of DEC and Albendazole is Used
A serious adverse experience (SAE) is defined as an adverse experience following
treatment with a drug that results in any of the following :
• death
• life-threatening adverse drug experience
• in-patient hospitalization or prolongation of an existing hospitalization
• persistent or significant disability/incapacity
• congenital anomaly or birth defect
• cancer
• overdose (accidental or intentional)
Important medical events that may not result in death, be life-threatening, or require
hospitalization may be considered a serious adverse drug experience when, based upon
appropriate medical judgment, they may jeopardize the patient or subject, and may
require medical or surgical intervention to prevent one of the outcomes listed in the
definition above: such events should also be reported.
COMPLETE THIS FORM ONLY IF THE ADVERSE EXPERIENCE MEETS THE ABOVE CRITERIA
and
send it promptly to:
Mrs Sue ReesGlaxoSmithKline
Global Clinical Safety & PharmacovigilanceNew Frontiers Science Park (South)
Third AvenueHarlow, Essex, CM19 5AW, U.K.
Telephone number:44-1279-644693Fax number: 44-1279-644260
COLLABORATIVE GLOBAL PROGRAMMETO ELIMINATE LYMPHATIC FILARIASIS
61

62
Country: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Date of Report: ___/___/_____
(day/month/year)
1. Patient Information
Name (First/Middle/Last) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Age (years) . . . . . . . . . . . . . . . . . . . . Sex ■■ M ■■ F
Village . . . . . . . . . . . . . . . . . . . . . . District . . . . . . . . . . . . . . Province . . . . . . . . . . . . . . . .State
2. Pre-existing Conditions
Health Status before treatment with DEC and albendazole:
■■ Good ■■ Poor ■■ Unknown If “Poor” give details: . . . . . . . . . . . . . . . . . . . . . . .
Parasitic Infections Confirmed Suspected Unknown Details
1. Lymphatic Filariasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2. Onchocerciasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3. Loiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Other parasitic infections, known or suspected (e.g. Malaria) . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Other medications being taken (currently or recently): . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Is patient pregnant? ■■ Yes ■■ No ■■ Unknown
An
nex
3

63
3. Information on Recent Albendazole & DEC Treatment
Were albendazole & DEC given together? ■■ Yes ■■ No ■■ Unknown
If No, explain: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Date of treatment ___/___/_____(day/month/year)
Source of treatment:Dose of Dose of Patient’s Patient’s
DEC albendazole height weight
■■ Community treatment program(no. of tablets) (no. of tablets) (cm) (kg)
■■ Clinic or physician treatment
■■ Other method
Was this a first treatment with DEC? ■■ Yes ■■ No ■■ Unknown
Was this a first treatment withalbendazole for mass treatment of LF? ■■ Yes ■■ No ■■ Unknown
If “No”, explain when and circumstances of past treatment(s): . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4. Description of the Serious Adverse Experience (SAE)
Date of onset ___/___/_____ hrs . . . . . . . . . . . .OR . . . . . . . days
(day/month/year) How long after drugs were taken?
Clinical signs and symptoms (please describe) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Were there signs of acute alcohol intoxication on initial examination? ■■ Yes ■■ No
Do you think this adverse experience is/was life-threatening? ■■ Yes ■■ No
Laboratory results (please provide name of test) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Date of tests ___/___/_____
(day/month/year)

An
nex
3
a) Hospitalization ■■ Yes ■■ No
If “Yes”, indicate: 1. Date of admission (day/month/year) ___/___/_____
2. Reason for admission: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3. Date of discharge (day/month/year) ___/___/_____
b) Drug treatments administered: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
c) Clinical course: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
(Attach any relevant reports)
5. Condition/Outcome at time of last observation
Full recovery: ■■ Yes ■■ No ■■ Unknown
Ongoing illness: ■■ Yes ■■ No ■■ Unknown
If yes describe current condition: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Persistent/Significant Disability/Incapacity: ■■ Yes ■■ No ■■ Unknown
If yes describe: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Death: ■■ Yes ■■ No
If “Yes”, indicate: 1. Date of death (day/month/year) ___/___/_____
2. Cause of death: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3.Circumstances at the time of death, in detail: . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Report any autopsy findings made including tissues taken for histopathology and any additional
studies done or requested (use additional pages necessary to complete your answers):
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
64

6. Conclusions (to be completed by the health care provider)
Presumptive Diagnosis: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Do you think the combined drug treatment with DEC & albendazole was a possible
causative factor in this Serious Adverse Experience? ■■ Yes ■■ No ■■ Not sure
If “Yes”, explain: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
If “No” or “Not sure”, what do you believe was the cause of the experience? . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7. Source (reporter(s) of the data in this form)
Name of person making the report . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Title . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Organization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Address . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Telephone number . . . . . . . . . . . . . . . . . . . . . . . . Fax number . . . . . . . . . . . . . . . . . . . . . .
E-mail . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
65

An
nex
3
Within one working day of receipt, the report will be distributed by
GlaxoSmithKline Clinical Safety Group to:
Dr Mark Bradley Telephone number: 44 208 047 5521Manager Scientific Support Fax number: 44 208 047 0684Global Community Partnerships E-mail: [email protected] House, 980 Great West RoadBrentford, Middlesex TW8 9GS, U.K.
Dr G. Biswas Phone number: 41-22-791-3850Lymphatic Filariasis Elimination Fax number: 41-22-791-4777World Health Organization E-mail: [email protected] Avenue Appia, CH-1211Geneva 27, SWITZERLAND
PRIMARY CONTACT INDIVIDUAL
Mrs. Sue Rees Telephone number: 44-1279-644693Head, Postmarketing Group Fax number: 44-1279-644260GlaxoSmithKline E-mail: [email protected] Clinical Safety & PharmacovigilanceNew Frontiers Science Park (South)Third AvenueHarlow, Essex, CM19 5AW, U.K.
66

An
nex 4
SERIOUS ADVERSE EXPERIENCE REPORTfor the
African Lymphatic Filariasis Treatment Program
A serious adverse experience (SAE) to a drug is defined as an adverse experience
following treatment with a drug that results in any of the following :
• death
• life-threatening adverse drug experience
• in-patient hospitalization or prolongation of an existing hospitalization
• persistent or significant disability/incapacity
• congenital anomaly or birth defect
• cancer
• overdose (accidental or intentional)
Important medical events that may not result in death, be life-threatening, or require
hospitalization may be considered a serious adverse drug experience when, based upon
appropriate medical judgment, they may jeopardize the patient or subject, and may
require medical or surgical intervention to prevent one of the outcomes listed in the
definition above should also be reported.
COMPLETE THIS FORM ONLY IF THE ADVERSE EXPERIENCE MEETS THE ABOVE CRITERIA
and
send it promptly to:
Mectizan Donation Program750 Commerce Drive, Suite 400
Decatur, GA 30030USA
COLLABORATIVE GLOBAL PROGRAMMETO ELIMINATE LYMPHATIC FILARIASIS
67

68
Country: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Date of Report: ___/___/_____
(day/month/year)
1. Patient Information
Name (First/Middle/Last) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Age (years) . . . . . . . . . . . . . . . . . . . . Sex ■■ M ■■ F
Village . . . . . . . . . . . . . . . . . . . . . . District . . . . . . . . . . . . . . Province . . . . . . . . . . . . . . . .State
2. Pre-existing Conditions
Health Status before treatment with Mectizan®‚ and albendazole (including any CNS disability):
■■ Good ■■ Poor ■■ Unknown If “Poor” give details: . . . . . . . . . . . . . . . . . . . . . . .
Parasitic Infections Confirmed Suspected Unknown Details
1. Onchocerciasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2. Lymphatic Filariasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3. Loiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
If Loiasis is confirmed mf/ml (blood): . . . . . . . . . . . . .mf/ml (CSF): . . . . . . . . . . . . . . . . . .
Other parasitic infections, known or suspected (e.g. Malaria) . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Other medications being taken (currently or recently): . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Is patient pregnant? ■■ Yes ■■ No ■■ Unknown
Alcohol intake within 24hrs of taking drugs? ■■ Yes ■■ No ■■ Unknown
An
nex
4

69
3. Information on Recent Albendazole & Mectizan®‚ Treatment
Were albendazole & Mectizan®‚ given together? ■■ Yes ■■ No ■■ Unknown
If No, explain: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Date of treatment ___/___/_____(day/month/year)
Source of treatment:Dose of Dose of Patient’s Patient’s
Mectizan® albendazole height weight
■■ Community treatment program(no. of tablets) (no. of tablets) (cm) (kg)
■■ Clinic or physician treatment
■■ Other method
Was this a first treatment with Mectizan®? ■■ Yes ■■ No ■■ Unknown
Was this a first treatment withalbendazole for mass treatment of LF? ■■ Yes ■■ No ■■ Unknown
If “No”, explain when and circumstances of past treatment(s): . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4. Description of the Serious Adverse Experience (SAE)
Date of onset ___/___/_____ hrs . . . . . . . . . . . .OR . . . . . . . days
(day/month/year) How long after drugs were taken?
Clinical signs and symptoms (please describe) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Were there signs of acute alcohol intoxication on initial examination? ■■ Yes ■■ No
Do you think this adverse experience is/was life-threatening? ■■ Yes ■■ No
Laboratory results (please provide name of test) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Date of tests ___/___/_____
(day/month/year)

An
nex
4
a) Hospitalization ■■ Yes ■■ No
If “Yes”, indicate: 1. Date of admission (day/month/year) ___/___/_____
2. Reason for admission: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3. Date of discharge (day/month/year) ___/___/_____
b) Drug treatments administered: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
c) Clinical course: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
(Attach any relevant reports)
5. Condition/Outcome at time of last observation
Full recovery: ■■ Yes ■■ No ■■ Unknown
Ongoing illness: ■■ Yes ■■ No ■■ Unknown
If yes describe current condition: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Persistent/Significant Disability/Incapacity: ■■ Yes ■■ No ■■ Unknown
If yes describe: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Death: ■■ Yes ■■ No
If “Yes”, indicate: 1. Date of death (day/month/year) ___/___/_____
2. Cause of death: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3.Circumstances at the time of death, in detail: . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Report any autopsy findings made including tissues taken for histopathology and any additional
studies done or requested (use additional pages necessary to complete your answers):
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
70

6. Conclusions (to be completed by the health care provider)
Presumptive Diagnosis: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Do you think the combined drug treatment with Mectizan®‚ & albendazole was a
possible causative factor in this Serious Adverse Experience?
■■ Yes ■■ No ■■ Not sure
If “Yes”, explain: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
If “No” or “Not sure”, what do you believe was the cause of the experience? . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7. Source (reporter(s) of the data in this form)
Name of person making the report . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Title . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Organization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Address . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Telephone number . . . . . . . . . . . . . . . . . . . . . . . . Fax number . . . . . . . . . . . . . . . . . . . . . .
E-mail . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
71

An
nex
4
Please send this report to the following:
Mectizan® Donation Program Telephone number: 404-371-1460750 Commerce Drive, Suite 400 Fax number: 404-371-1138Decatur, Georgia 30030 E-mail: [email protected].
Within one working day of receipt, the report will be distributedby the Mectizan® Donation Program to:
Dr. Philippe Gaxotte Telephone number: 33-1-30-82-10-37Laboratoires Merck Sharp & Dohme Interpharma Fax number: 33-1-30-82-10-90106, Avenue Jean Moulin E-mail: [email protected] La Celle Saint Cloud, FRANCE
Dr Mark Bradley Telephone number: 44-208-047-5521Manager Scientific Support Fax number: 44-208-047-0684Global Community Partnerships E-mail: [email protected] House, 980 Great West RoadBrentford, Middlesex TW8 9GS, U.K.
Linda S. Hostelley Telephone number: 1-610-397-2416Executive Director Fax number: 1-610-397-2451Adverse Experience Reporting Worldwide E-mail: [email protected] Product Safety & EpidemiologyMerck Research LaboratoriesP. O. Box 4, BLB-30West Point, PA 19486, U.S.A.
Dr G. Biswas Telephone number: 41-22-791-3850Lymphatic Filariasis Elimination Fax number: 41-22-791-4777World Health Organization E-mail: [email protected] Avenue Appia, CH-1211Geneva 27, SWITZERLAND
Ms. Sue Rees Telephone number: 44-1279-644693Head, Postmarketing Group Fax number: 44-1279-644260GlaxoSmithKline E-mail: [email protected] Clinical Safety & PharmacovigilanceNew Frontiers Science Park (South)Third AvenueHarlow, Essex, CM19 5AW, U.K.
72

73
Acronyms
ADL Adenolymphangitis
ADR Adverse Drug Reactions
AFRO African Regional Office (of the WHO)
AMRO American Regional Office (of the WHO)
APOC African Programme for Onchocerciasis Control
CDS Communicable Diseases Cluster of WHO
CEE Strategy Development and Monitoring for Elimination and Eradication Unit
CPE Department for Communicable Disease Control Prevention and Eradication
CHW Community Health Worker
CSR Department for Communicable Disease Surveillance and Response
DEC Diethylcarbamazine citrate
DOT Directly Observed Treatment
ELF Elimination of Lymphatic Filariasis
EMRO Eastern Mediterranean Regional Office (of the WHO)
GAELF Global Alliance to Eliminate Lymphatic Filariasis
GIS Geographic Information System
GSK GlaxoSmithKline
ICT Immuno-chromatographic test
IEC Information, Education and Communication
ITN Insecticide Treatment Nets
IU Implementation Unit
KAP Knowledge, Attitude and Practices
LF Lymphatic Filariasis
LQAS Lot Quality Assurance Sampling
MDA Mass Drug Administration
MDP Mectizan® Donation Program
MIES Management Information and Evaluation System
MoH Ministry of Health
MSD Merck & Co., Inc.
NFCP National Filaria Control Programme
NGDO Non-Governmental Developmental Organization
NGO Non-Governmental Organization
NPS National Pharmacovigilance System
NTF-ELF National Task Force to Eliminate Lymphatic Filariasis
PacELF Pacific Initiative for the Elimination of Lymphatic Filariasis
PAHO Pan American Health Organization
PELF Programme to Eliminate Lymphatic Filariasis
PHC Primary Health Centre
PRG Programme Review Group
Glossary of acronyms and Programme toEliminate Lymphatic Filariasis definitions
An
nex 5

An
nex
5
QA Quality Assurance
QC Quality Control
SAE Serious Adverse Experience
SB SmithKline Beecham
SEARO South East Asian Regional Office (of the WHO)
TAG Technical Advisory Group
TCC Technical Consultative Committee (of APOC)
TDR WHO/World Bank/UNDP Special Programme for Research and Training
UN United Nations
UNDP United Nations Development Programme
UNFPA United Nations
UNICEF United Nations Children’s Fund
WHO World Health Organization
WPRO Western Pacific Regional Office (of the WHO)
PELF Definitions
A Serious Adverse Experience (SAE): an event which is fatal, life threatening, disabling
or incapacitating or results in hospitalization, prolongs a hospital stay or is associated
with congenital abnormality, cancer or overdose (either accidental or intentional). In
addition, any experience which the investigator regards as serious or which would
suggest any significant hazard, contraindication, side effect or precaution that may be
associated with the use of the drug should be reported as a serious event
Case classificationLymphatic Filariasis case: an individual having current infection with Brugia malayi,
Brugia timori or Wuchereria bancrofti, whether or not microfilaraemic.
Clinical case: individual with any of the clinical findings of hydrocoele, chylocoele,
lymphoedema, chyluria, haematochyluria, haematuria, hyper-eosinophilia or tropical
pulmonary eosinophilia syndrome; for which other causes have been excluded in a
resident of, or long-term visitor to, an endemic area, plus specific antibody elevations in
visitors to endemic regions.
Probable case: a case that meets the clinical case definition.
Confirmed case: a case confirmed by laboratory or ultrasonography examinations.
Laboratory criteria for diagnosis of infection: presence of microfilariae, circulating
filarial antigen or detection of adult worm(s) by ultrasonography or biopsy.
74

75
EndemicityCountries are classified as:
Implementation Unit (IU) for MDA: the designated administrative unit in a country, for
which the decision to administer the entire population with recommended anti filarial
drugs if identified as having indigenous transmission or endemic.
Endemic IU: IU whose average or any of its population sub-unit (village or urban area)
has an LF infection rate of 1% or more among its native population.
Endemic country: country where any of its IU is known or has reported to be endemic
after 1980.
Never endemic: country with no history or evidence of endemic filariasis.
Post-endemic: country with known history of endemic filariasis before 1980, but with no
evidence of transmission or new infection since 1980.
Unknown: Countries with history of endemic filariasis before 1980 or where evidence of
infection in immigrants is present but clear evidence of indigenous transmission is absent.
Drug administration and monitoringDrug coverage for a designated [area]: The proportion of all individuals of the [area] who
ingested the drug(s) in the adequate dosage
Number of individuals who ingested adequate dosage recommended antifilarial drugs x 100
Total population of the [area]
[area] refers to any geographical area up-to the level of the designated IU, e.g. if the
designated implementation unit is the district which is sub-divided into counties/blocks,
villages or urban areas, area could refer to villages, urban areas, counties/blocks or to the
district.
For reporting coverage for administrative units above the level of the IU, drug coverage
to be calculated as:
Sum of all individuals in the targeted IUs ingested the recommended AF drugs x 100
Total population of all the targeted IU under the administrative unit
Reported coverage: The coverage based on reports received from reporting units.
Geographical coverage: Proportion of IUs targeted covered by MDA during the reporting year
Number of IU covered by MDA in the year x 100
Total number of endemic IU during the year
Proportion of villages/urban areas covered by MDA in the targeted IU during the
reporting year
Glossary of Acronyms and LF Definitions

An
nex
5
Number of villages/urban areas in the targeted IU covered by MDA x 100
Total number of villages/urban areas in the target IU
Observed drug coverage: the coverage based on actual verification by supervisory tier
(done on a sample population).
Proportion of all verified individuals who ingested the drug(s) in the adequate dosage
Number of verified individuals who ingested adequate dosage antifialrial drugs x 100
Number of individuals in the verified households
Population at risk (or at-risk population): Total population in the endemic Implementation
Unit(s)
Microfilaria prevalence (mf%): Proportion of blood slides (20µl) found positive for
microfilariae (Wb, Bm or Bt) species.
Number of individuals whose slides are positive for mf x 100
Total number of individuals examined for mf
Microfilaria density (mfd): Average number of microfilarae in slides positive for
microfilaria expressed as per ml of capillary blood
Total count of microfilariae in the slides found positive x 50 (presuming 20 µl per slide)
Number of slides found positive
Antigen prevalence: Proportion of individuals surveyed testing positive for CFA
Number of individuals testing positive x 100
Total number of individuals with a valid test result
Please note: When Lot Quality Assurance Sampling (LQAS) is undertaken as in initial assessment and mapping
and the survey stopped on finding a positive result, it is inappropriate to calculate prevalence. The result would
only indicate that the antigenaemia is above the cut off percent.
Grading of Lymphoedema
Grade I : mostly pitting oedema; spontaneously reversible on elevation
Grade II : mostly non-pitting oedema; not spontaneously reversible on elevation
Grade III : gross increase in volume in a Grade II lymphoedema with dermatosclerosis
and papillomatous lesions
76