Embed Size (px)
Citation preview

GLOBAL VALUE DOSSIER FOR LIGASURETM TECHNOLOGY
COLECTOMY
Global Value Dossier: LigaSureTM Technology 2
Prepared by: Jason Davis
Coreva Scientific
Kaiser-Joseph Str 198-200
79098 Freiburg, Germany
Phone: +49 76 176 999 422
E-mail: [email protected]
Version No. 4.0
Date: October 19, 2017

Global Value Dossier: LigaSureTM Technology 3
Contents
1. Disclaimer and scope ..........................................................................................................5
1.1. Products and aliases ...................................................................................................5
1.2. Data sources ...............................................................................................................5
1.3. Analysis .......................................................................................................................5
2. Introduction to LigaSureTM technology ..............................................................................6
3. Clinical evidence for LigaSureTM devices in colectomy ......................................................7
3.1. Overview .....................................................................................................................7
3.2. The surgical area .........................................................................................................7
3.3. Indications and anatomy .............................................................................................7
3.4. Surgical settings .........................................................................................................8
3.5. LigaSureTM technology compared to conventional hemostasis in colectomy..........9
3.5.1. Operative time ................................................................................................. 10
3.5.2. Blood loss.......................................................................................................... 11
3.5.3. Length of hospital stay ..................................................................................... 12
3.5.4. Procedure-related complications .................................................................... 13
3.6. LigaSureTM technology compared to other energy devices in colectomy ............. 14
3.6.1. Operative parameters ...................................................................................... 14
3.6.2. Surgical experience considerations ................................................................. 17
4. Economic impact of LigaSureTM technology ................................................................... 18
4.1. Overview .................................................................................................................. 18
4.2. Health economics of surgery ................................................................................... 18
4.3. Economics of colorectal procedures ....................................................................... 19
4.4. LigaSureTM technology impact on colectomy ......................................................... 19
5. Conclusions ...................................................................................................................... 22
6. Source data tables ............................................................................................................ 23
6.1. Data table summary: LigaSureTM technology colectomy surgical outcome data .. 23
6.2. Data table summary: LigaSureTM technology economic data ................................ 31
7. Structured literature search details ................................................................................. 33
7.1. Searches performed ................................................................................................ 33
7.2. Screening literature results ..................................................................................... 34
7.2.1. Screening general search (EMBASE) results .................................................... 34
7.2.2. Screening returned results for evidence (PubMed) ......................................... 35
8. Data references ................................................................................................................ 36
9. Geographical references .................................................................................................. 38

Global Value Dossier: LigaSureTM Technology 4
List of Tables
Table 3-1 Colectomy procedures ...........................................................................................8
Table 3-2 Reported LigaSureTM device use in colorectal procedures ....................................9
Table 6-1 Publication data reporting on LigaSureTM technology for clinical outcomes in colectomy .............................................................................................................................. 23
Table 6-2 Publication data reporting on economics related to LigaSureTM technology use ... .............................................................................................................................. 31
Table 7-1 Structured searched in PubMed to identify relevant LigaSureTM technology data . .............................................................................................................................. 33
Table 7-2 Structured search in EMBASE to identify use of LigaSureTM devices ................. 34
Table 7-3 Description of exclusion criteria .......................................................................... 35
List of Figures
Figure 3-1 Regions of human colon ......................................................................................8
Figure 3-2 Clinical use of LigaSureTM devices in colorectal surgeries ..................................9
Figure 3-3 Change in operative time with LigaSureTM devices compared to mechanical ligation for colectomy ............................................................................................................. 10
Figure 3-4 Change in blood loss with LigaSureTM devices compared to mechanical ligation for colectomy .......................................................................................................................... 11
Figure 3-5 Length of hospital stay with LigaSureTM devices compared to mechanical ligation after colectomy .......................................................................................................... 12
Figure 3-6 LigaSureTM device rates of general complications for colectomy .................. 13
Figure 3-7 LigaSureTM device rates of specific complications after colectomy ............... 14
Figure 3-8 Operative time with LigaSureTM technology compared to other energy devices for colectomy ............................................................................................................. 15
Figure 3-9 Intra-operative blood loss with LigaSureTM technology compared to other energy devices for colectomy................................................................................................. 16
Figure 3-10 Change in length of hospital stay with LigaSureTM technology compared to other energy devices for colectomy ....................................................................................... 16
Figure 3-11 Intraoperative carbon dioxide usage with LigaSureTM technology versus other energy devices for colectomy................................................................................................. 17
Figure 3-12 Surgeon satisfaction with LigaSureTM devices compared to other energy devices .......................................................................................................................... 17
Figure 4-1 Operating room costs per minute ................................................................... 19
Figure 4-2 Per procedure cost analysis results of LigaSureTM devices compared to conventional ligation in colectomy ......................................................................................... 20
Figure 4-3 Per procedure cost analysis results of LigaSureTM devices compared to other energy devices in colectomy .................................................................................................. 21

Global Value Dossier: LigaSureTM Technology 5
1. Disclaimer and scope
1.1.Products and aliases
This document refers to devices making use of LigaSureTM technology. This technology includes, for laparoscopic procedures, the LigaSureTM 5mm blunt tip (37 cm and 44 cm) device, the LigaSureTM Maryland jaw (37 cm and 44 cm) device, the LigaSure AdvanceTM
Pistol Grip device, the LigaSure AtlasTM device and the LigaSureTM dolphin tip device. For open surgeries, applicable devices include the LigaSure PreciseTM device, the LigaSure ImpactTM device, the LigaSureTM small jaw device, the LigaSureTM 5mm blunt tip (23 cm) device, the LigaSureTM Maryland jaw (23 cm) device, the LigaSure AtlasTM (20 cm) device, the LigaSureTM dolphin tip (20 cm) device, the LigaSureTM curved jaw device and other reusable LigaSureTM instruments. Indications, contraindications, warnings, precautions and procedure steps may vary between products and models, and availability may vary by jurisdiction. Please always refer to indication labelling for your jurisdiction and read all applicable instructions for use provided with the products.
1.2. Data sources
Data regarding preclinical and clinical application of LigaSureTM devices were derived from searches of published literature in PubMed (February 2017) and EMBASE (November 2016). General text searches for LigaSureTM device references were performed in EMBASE to include all published instances of the use of the technology without restriction of time of publication. These results provide an overview of extent of usage of the technology.
For clinical evidence data of LigaSureTM technology usage, structured searches were performed using PubMed for peer-reviewed literature applying consistent exclusion criteria across searches for specific surgical indications (see Section 7, Structured literature search details). Results were restricted to publications based on data obtained within the most recent 10 years of the search (2007 and onwards), and excluded editorials/commentaries, articles with no abstract, those that did not report relevant clinical data (such as animal or ex vivo studies), those that reported data on fewer than 20 patients, those which were not focused on outcomes related to the technology (that is, no mention of vessel sealing or hemostasis), and articles which did not reference LigaSureTM or generic LigaSureTM technology (electrosurgical or radiofrequency bipolar vessel sealing).
1.3. Analysis
Clinical results from individual studies are presented as reported (including indication of statistical significance where determined). Where data are amalgamated from multiple reports, please note that the individual studies will vary in terms of design, protocol, surgical technique and patient population, which may limit conclusions drawn from direct comparison and relevant analysis of statistical significance. The resulting figures, however, provide insight into clinical outcomes that have been achieved using LigaSureTM devices in vessel sealing during surgical procedures.

Global Value Dossier: LigaSureTM Technology 6
2. Introduction to LigaSureTM technology
In surgery, for the patient’s health as well as to ensure maintenance of adequate visualization, the operative field must stay free of excess blood and other fluids. This is accomplished by hemostatic techniques, such as use of LigaSureTM technology. LigaSureTM technology is used in surgical procedures to divide and seal vessels up to and including 7 mm in diameter. The devices are electrosurgical in nature, using current delivered to patient tissues to effect tissue sealing. The complete LigaSureTM vessel sealing system comprises the vessel sealing device (the LigaSureTM sealer/divider), and the energy platform (such as the ForceTriadTM energy platform, the ValleylabTM LS10 generator or the ValleylabTM FT10 energy platform). The vessel sealing device delivers a combination of pressure and electrical current to tissues, and the current is provided in a smart algorithm by the energy platform, using tissue-sensing technology (TissueFectTM,a a component of the LS10 generator and the ForceTriadTM and FT10 energy platforms) to control energy delivery. The technology is suitable for use wherever the division and ligation of vessels is desired during general open or minimally invasive surgical procedures.
An accompanying dossier (LigaSureTM Technology GVD) is available detailing pre-clinical data and worldwide usage of LigaSureTM technology in clinical applications.
a White paper, ValleylabTM FT10 Energy Platform TissueFectTM Technology. McHenry J, Dunning J and Wagle K (2015) 10/2015 US150755[REF#479324]

Global Value Dossier: LigaSureTM Technology 7
3. Clinical evidence for LigaSureTM devices in colectomy
3.1. Overview
Summary and key messages
Broad usage of LigaSureTM technology: Published literature describing the use of LigaSureTM technology in colorectal procedures spans a wide variety of settings around the world, covering 35 countries.G1–G35
Shorter surgical times with LigaSureTM devices: LigaSureTM technology has demonstrated significantly shorter operative times compared to conventional ligation1-4 and monopolar scissors.5,6 Compared to ultrasonic technology (Harmonic Ace) surgical times have been both significantly shorter7,8 and equivalent.5,9
Positive impact on intra-operative blood loss: Intra-operative blood loss with LigaSureTM devices has been shown to be significantly lower2,3 to equivalent1,3,6 for various types of colectomy versus conventional and ultrasonic7-9 ligation methods.
No increase in complication rates: While there is some variability among studies, compared to conventional ligation with sutures or clips, LigaSureTM devices in colectomy have achieved equivalent rates of overall,4,6 intraoperative1,2 and postoperative1,2 complications. Complication rates are equivalent to those with monopolar5,6 and ultrasonic energy devices.5,6,8,9
Highly rated surgeon satisfaction: LigaSureTM devices received higher surgeon ratings for bleeding control and safety compared to monopolar and ultrasonic devices,5 and a higher handling performance rating than a comparable ultrasonic device.5
3.2. The surgical area
Diseases of the lower human digestive tract vary in severity and accordingly, in appropriate medical treatment. The more serious morbidities, such as neoplasms, require surgical intervention to remove affected tissues. Even for conditions with lower mortality than cancer, surgical removal of benign tissue may be indicated. LigaSureTM technology has been applied to the range of surgeries along the length of the tract, and the impact and outcomes of the use of LigaSureTM devices in these surgeries will be described.
3.3. Indications and anatomy
Colon resections are most frequently performed because of malignant neoplasms (38%), followed by diverticula (23%), and benign neoplasms (11%).10 Among the non-cancerous indications, complications related to Crohn’s disease may also require segmental resection.11 A diagram of the region of interest is shown in Figure 3-1.

Global Value Dossier: LigaSureTM Technology 8
Figure 3-1 Regions of human colon
8
Ascending/right colon
Transverse colon
Descending/left colon
Sigmoid colon
Rectum
Splenic flexure
Hepatic flexure
Anus
Regions of the lower human digestive tract progressing from the ascending or right colon to the anus. Removal of any section would constitute a colectomy or hemicolectomy (such as a right hemicolectomy). Anterior resections may extend from the sigmoid colon to the rectum and/or the anus. Figure adapted from stock image used under license 123rf.
Any region of the lower digestive tract may be subject to removal (Table 3-1). Depending on the region affected, the restoration of digestive function may take the form of intestinal anastomosis, where the remaining ends of the colon or intestine are attached, or colostomy, where digestive flow is redirected for collection in a pouch or bag outside of the body.
Table 3-1 Colectomy procedures
Type Surgery Description
RC/RH Right colectomy (hemicolectomy)
Removal of sections of the right or ascending colon
Trans Transverse colectomy
Removal of sections of the transverse colon
LC/LH Left colectomy (hemicolectomy)
Removal of sections of the left or descending colon
Sig Sigmoidectomy Removal of the sigmoid colon
AR Anterior resection Removal of the anterior segment of the colon, which may include sections of the rectum or anus
Tot Total colectomy Removal of the entire colon Surgeries and abbreviations are ordered according to the progression of digestive flow.
3.4. Surgical settings
LigaSureTM devices have been designed for use in the various forms of colorectal surgery as described above, including resections along the entire length of the colon, and for the removal of grade III and IV hemorrhoids. The technology has published references in 35 different countries across the world (Figure 3-2): Australia,G1 Austria,G2 Canada,G3 China,G4 Croatia,G5 Egypt,G6 Finland,G7 France,G8 Germany,G9 Greece,G10 India,G12 Iran,G13 Ireland,G14 Israel,G15 Italy,G16 Japan,G17 Kuwait,G18 Mexico,G19 Netherlands,G20 Pakistan,G21 Poland,G22 Romania,G23 Russia,G24 Saudi Arabia,G25 Serbia,G26 Singapore,G27 Slovenia,G5 South Korea,G28 Spain,G29 Switzerland,G30 Taiwan (Province of China),G31 Thailand,G32 Turkey,G33 the United KingdomG34 and the United States.G35 The subsequent sections report on peer-reviewed, published studies (randomized controlled trials and meta-analyses) describing clinical outcomes for LigaSureTM

Global Value Dossier: LigaSureTM Technology 9
technology in comparison to conventional methods of hemostasis and other advanced energy options for treatment.
Figure 3-2 Clinical use of LigaSureTM devices in colorectal surgeries
28
Highlighted are countries of origin for publications demonstrating the successful use of LigaSureTM technology in clinical settings across all types of colorectal surgery.
3.5. LigaSureTM technology compared to conventional hemostasis in colectomy
Studies reporting LigaSureTM device performance relative to conventional hemostasis methods (clips and vascular staples for colorectal resection) have varied in separation of surgical procedures. In colectomy, reports have mostly combined results for various forms of colon resection. One study focused on left colectomy while others have combined results for different surgeries.1,3 In both cases, although multiple types of procedures were performed (Table 3-2) results were reported as an amalgamation across all surgery types. The successful completion of this array of surgeries, however, illustrates the applicability of LigaSureTM technology for resection surgeries across the extent of the colon.
Table 3-2 Reported LigaSureTM device use in colorectal procedures
Type Conventional (N) LigaSureTM (N)
Surgeries performed in Adamina et al., 20111
Right colectomy 19 22
Left colectomy 15 19
Total colectomy 6 9 Proctectomy 5 5
All surgeries total 45 55
Surgeries performed in Takiguchi et al, 20103
Right colectomy 5 11
Transverse 1 2
Left colectomy 2 2 Sigmoidectomy 4 9
High anterior 6 3
Low anterior 8 9 Abdominoperineal 4 6
Other 2 3
All surgeries total 32 45

Global Value Dossier: LigaSureTM Technology 10
Surgical outcomes for LigaSureTM devices in colectomy have been reported in both randomized controlled trials1,3 and meta-analysis,6 and have included duration of operation, intraoperative blood loss, length of hospital stay, and rates of complications during or after surgery.
3.5.1. Operative time
Compared to conventional ligation in colectomy with clips and sutures, the use of LigaSureTM devices has resulted in savings of operative time1,3,6 (Figure 3-3). Different types of colectomy require different lengths of surgery, as different centers may have different protocols and personnel performing procedures. When results are stratified for specific types of surgery (proctocolectomy,2 sigmoidectomy,4 or total colectomy1), or for a single center in a multicenter study,3 the time savings achieved with LigaSureTM devices has been reported to be statistically significant at the 95% confidence level.
Figure 3-3 Change in operative time with LigaSureTM devices compared to mechanical ligation for colectomy
0
50
100
150
200
250
300
350
400
450
Op
era
tiv
e t
ime
(min
)
6
ColectomyLS vs conventional
AllNS
All*All
NS
AllNS LC
NS
PCNS
PC*
RCNS
SIG***
TC*
LigaSureTM Technology
Clips + Stapler
Clips + Harmonic Shears
All, mixed types of colectomy procedures; LC, left hemicolectomy; PC, proctectomy/proctocolectomy; RC, right hemicolectomy; SIG, sigmoidectomy; TC, total colectomy. The use of LigaSureTM devices has resulted in non-significantly, and significantly decreased operative time to complete colectomy surgeries. The type of colectomy included in each analysis is indicated above the comparisons, along with indication of statistical significance (* = p ≤ 0.05, *** = p ≤ 0.001, NS = non-significant at the 95% confidence level). In the study by Takiguchi et al., 2010,3 results were presented averaged across all centers, and authors reported separately results for the single center (†) that performed the most colectomies revealing a center-specific statistically significant time savings. The study of Trilling et al., 20164 (‡) compared mechanical ligation with a mixed group of energy devices (100 patients) of which 95% were LigaSureTM devices, the remaining 5% ultrasonic technology. Results are thus primarily attributable to LigaSureTM technology. Bars represent estimated means, error bars are the standard deviations when reported.

Global Value Dossier: LigaSureTM Technology 11
3.5.2. Blood loss
Blood loss in colectomy surgeries with LigaSureTM technology compared to conventional ligation with clips and sutures has been performed in single1 and multicenter3 randomized controlled trials (Figure 3-4). Results have shown decreased blood loss with the use of LigaSureTM technology when different types of colectomy are considered together. As in the case of operative time savings (3.5.1), this decrease was found to be statistically significant in one center that performed the most colectomies of the multicenter trial,3 as well as in a study reporting specifically hand-assisted laparoscopic restorative proctocolectomy.2 Using LigaSureTM devices therefore does not increase risks to patient safety due to blood losses.
Figure 3-4 Change in blood loss with LigaSureTM devices compared to mechanical ligation for colectomy
0
100
200
300
400
500
600
700
800
900
Blo
od
loss
(m
l)
7
ColectomyLS vs conventional
LigaSureTM Technology
Clips + Stapler
Clips + Harmonic Shears
AllNS
AllNS
AllNS
All*
LCNS
PCNS
RCNS
PC*
TCNS
All, mixed types of colectomy procedures; LC, left hemicolectomy; PC, proctectomy/proctocolectomy; RC, right hemicolectomy; TC, total colectomy. The use of LigaSureTM devices has resulted in non-significantly, and significantly decreased intra-operative blood loss during colectomy surgeries. The type of colectomy included in each analysis is indicated above the comparisons, along with indication of statistical significance (* = p ≤ 0.05, NS = non-significant at the 95% confidence level). In the study by Takiguchi et al., 2010,3 results were presented averaged across all centers, and authors reported separately results for the single center (†) that performed the most colectomies revealing a center-specific statistically significant time savings. Bars represent estimated means; error bars are the standard deviations when reported.
Global Value Dossier: LigaSureTM Technology 12
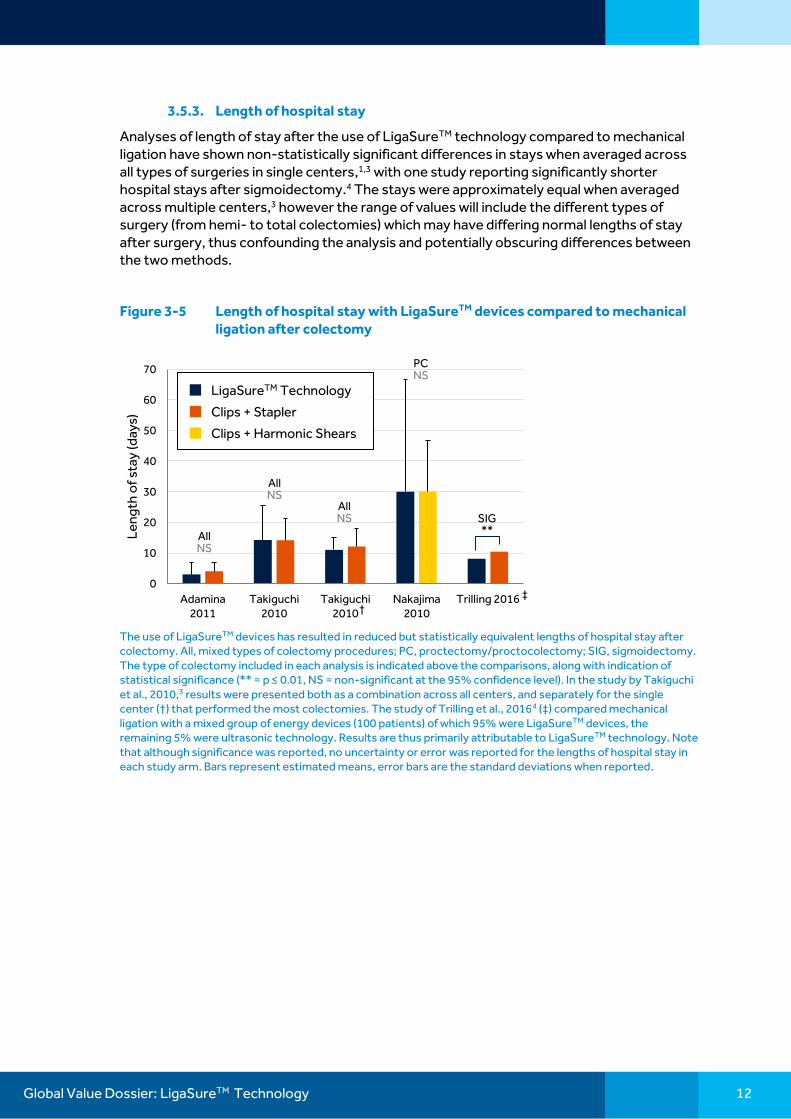
3.5.3. Length of hospital stay
Analyses of length of stay after the use of LigaSureTM technology compared to mechanical ligation have shown non-statistically significant differences in stays when averaged across all types of surgeries in single centers,1,3 with one study reporting significantly shorter hospital stays after sigmoidectomy.4 The stays were approximately equal when averaged across multiple centers,3 however the range of values will include the different types of surgery (from hemi- to total colectomies) which may have differing normal lengths of stay after surgery, thus confounding the analysis and potentially obscuring differences between the two methods.
Figure 3-5 Length of hospital stay with LigaSureTM devices compared to mechanical ligation after colectomy
0
10
20
30
40
50
60
70
Adamina2011
Takiguchi2010
Takiguchi2010
Nakajima2010
Trilling 2016
Le
ng
th o
f st
ay (d
ays)
9
ColectomyLS vs conventional
†
AllNS
AllNS
AllNS
PCNS
SIG**
‡
LigaSureTM Technology
Clips + Stapler
Clips + Harmonic Shears
The use of LigaSureTM devices has resulted in reduced but statistically equivalent lengths of hospital stay after colectomy. All, mixed types of colectomy procedures; PC, proctectomy/proctocolectomy; SIG, sigmoidectomy. The type of colectomy included in each analysis is indicated above the comparisons, along with indication of statistical significance (** = p ≤ 0.01, NS = non-significant at the 95% confidence level). In the study by Takiguchi et al., 2010,3 results were presented both as a combination across all centers, and separately for the single center (†) that performed the most colectomies. The study of Trilling et al., 20164 (‡) compared mechanical ligation with a mixed group of energy devices (100 patients) of which 95% were LigaSureTM devices, the remaining 5% were ultrasonic technology. Results are thus primarily attributable to LigaSureTM technology. Note that although significance was reported, no uncertainty or error was reported for the lengths of hospital stay in each study arm. Bars represent estimated means, error bars are the standard deviations when reported.

Global Value Dossier: LigaSureTM Technology 13
3.5.4. Procedure-related complications
Various colectomy-related complications have been reported for studies of LigaSureTM technology in comparison to mechanical ligation. These have been grouped generally into categories of overall,4,6 intra-operative1,2 and post-operative1,2,4 complications (Figure 3-6), and there have been comparisons of rates of specific complications (Figure 3-7) including fistula formation,4 infection rates1,2,4 and conversion from laparoscopic to open surgery.4 Across these studies, LigaSureTM devices have not increased the risk of general complications (including numerically lower, non-statistically significant reductions in complication rates).2,4 In the case of reported specific procedure-related complications, no statistically-significant differences have been shown between the use of LigaSureTM technology and conventional ligation for colectomy, demonstrating that LigaSureTM devices do not increase risks to patients during1,3,6 or after1,4 procedures.
Figure 3-6 LigaSureTM device rates of general complications for colectomy
0%
10%
20%
30%
40%
50%
60%
Ov
era
ll co
mp
lica
tio
n r
ate
(%
)
11
ColectomyLS vs conventional
AllNS
LigaSureTM Technology
Clips + Stapler
Clips + Harmonic ShearsSIGNS
AllNS
PCNS
PCNS
SIGNS
AllNS
Overall Intra PostMajor
Complication rates are shown, overall for the colectomy procedure (Overall), for intra-operative complications (Intra), post-operative complications (Post), and for complications classified as major events (level III-V on the Dindo classification scale).12 All, mixed types of colectomy procedures; PC, proctectomy/proctocolectomy; SIG, sigmoidectomy. The study of Trilling et al., 20164 (‡) compared mechanical ligation with a mixed group of energy devices (100 patients) of which 95% were LigaSureTM devices, the remaining 5% were ultrasonic technology. Results are thus primarily attributable to LigaSureTM technology. Bars represent percentages of patients with complications. NS = non-significant at the 95% confidence level. All studies were comparative, where in the above figure the absence of a bar indicates no events recorded in the corresponding study arm.

Global Value Dossier: LigaSureTM Technology 14
Figure 3-7 LigaSureTM device rates of specific complications after colectomy
0%
5%
10%
15%
20%
25%
30%
Trilling2016
Adamina2011
Nakajima2010
Trilling2016
Trilling2016
Sp
eci
fic
co
mp
lica
tio
n r
ate
(%
)
12
ColectomyLS vs conventional
LigaSureTM Technology
Clips + Stapler
Clips + Harmonic Shears
‡ ‡‡
SIGNS
SIGNS
SIGNS
AllNS
PCNS
Fistula Infections
Conversion to open
Complication rates are shown for specific reported complications of colectomy surgeries. The surgeries included in each analysis are shown above the comparisons. In most cases, LigaSureTM technology results in comparable complication rates (numerically lower, non-statistically-significant) in comparison to mechanical ligation. All, mixed types of colectomy procedures; PC, proctectomy/proctocolectomy; SIG, sigmoidectomy. The study of Trilling et al., 20164 (‡) compared mechanical ligation with a mixed group of energy devices (100 patients) of which 95% were LigaSureTM devices, the remaining 5% were ultrasonic technology. Results are thus primarily attributable to LigaSureTM technology. Bars represent percentages of patients with complications. NS = non-significant at the 95% confidence level.
3.6. LigaSureTM technology compared to other energy devices in colectomy
As for the comparison to conventional methods of hemostasis during surgery, the outcomes reported for comparisons to other energy devices must be subdivided according to type of surgery. Here, comparisons have been made between LigaSureTM technology and ultrasonic devices (Harmonic ScalpelTM*) and monopolar scissors.
The outcomes for LigaSureTM devices have been assessed in meta-analyses considering all colectomy surgeries together6 and specifying laparoscopic colorectal resection,13 and in a randomized controlled trial of left colectomy.5 The latter trial specified counts for different levels (rectosigmoid and low anterior), but outcomes were reported for entire treatment arms (monopolar scissors, LigaSureTM devices, ultrasonic coagulation shears) without specifying the level of left colectomy.5 Note that the meta-analysis of Tou et al, 20116 for comparisons with monopolar devices is derived from the results of Hubner et al., 2008.5 The Tou study reports means and standard deviations, obtained from communication with the original study authors, in contrast to the medians and ranges originally reported. Numerical data from the Tou data are thus used here for comparability with other studies, while study details (such as types of procedures) are cited from the original source.
3.6.1. Operative parameters
The main operative parameters reported for colon resection include operative time (Figure 3-8), blood loss (Figure 3-9), and length of hospital stay (Figure 3-10). LigaSureTM devices have been reported to achieve significant reductions in operative time compared to monopolar scissors,6 while compared to ultrasonic shears, operative times have been reported to be shorter8 and equivalent.5 These time differences have been assessed by meta-analysis for a mixture of all surgery types together,6 and individual randomized controlled trials separately for left7 and right7,8 hemicolectomies.

Global Value Dossier: LigaSureTM Technology 15
The amount of intra-operative blood lost during colectomy has been shown to be comparable among the energy technologies across all surgery types,5,9 but examples for specific surgeries of left7 and right7,8 hemicolectomy, and anterior resection7 have shown LigaSureTM device use to be associated with less intra-operative blood loss.
The final commonly reported parameter, the length of hospital stay after surgery, has been shown to be comparable among monopolar, ultrasonic and LigaSureTM technologies,5,7-9 demonstrating that LigaSureTM devices do not negatively impact on immediate patient outcomes after colectomy.
For these parameters, reductions have been seen (both statistically significant and non-significant at the 95% confidence level) when comparing LigaSureTM devices to other standard (monopolar scissors) and advanced (ultrasonic shears) energy technologies. Multiple studies thus demonstrate the superiority to non-inferiority of LigaSureTM devices to other available energy technologies.
Figure 3-8 Operative time with LigaSureTM technology compared to other energy devices for colectomy
0
50
100
150
200
250
Op
era
tiv
e t
ime
(min
)
15
ColectomyLS vs OAE
AllNS
LC***
RC**
RC*
††
LC***
LCNS LC
NS
†
LigaSureTM Technology
Monopolar Scissors
Ultrasonic technology
Study Surgery Comparator LS results LS err LS N OE res OE err OE N sig calc sig
Tou 2011 All MES 104.7 31.8 144.8 43.4 0.00078
Hübner 2008 LC MES 105 34.25 21 137 41.25 20 <0.001(K-W) 0.010617
Rimonda 2009 All UCS 116.3 44 70 114.8 47.6 70 0.89 0.846769
Tou 2011 All UCS 112.05 30.20 91 108.83 32.59 90 0.60
Campagnacci 2007 RC UCS 111 31.25 32 133 23.75 37 NS 0.001927
Guerreri 2008 RC UCS 98.4 23.75 45 122.7 45.75 44 <0.05 0.002599
Campagnacci 2007 LC UCS 140 12.5 50 176 36.25 47 NS 2.72E-08
Rimonda 2009 LC UCS 118.5 37.6 37 106 35.6 32 0.2 0.161177
Hübner 2008 LC UCS 105 34.25 21 90 33 20 <0.001(K-W) 0.161407
Rimonda 2009 AR UCS 152.14 28.6 18 158.5 57.2 22 0.72 0.651163
AllNS
ARNS
For studies comparing LigaSureTM devices to other energy devices, the types of surgeries included in each analysis are shown above the comparisons, along with indication of statistical significance (** = p ≤ 0.01, *** = p ≤ 0.001, NS = non-significant at the 95% confidence level). The dagger (†) indicates significance measures independently conducted. In the study of Campagnacci et al., 2007,7 all comparisons were reported as non-significant at the 95% confidence level, however independent testing (two-sided t-test) using provided data indicated significant reductions in operative time with the use of LigaSureTM devices compared to ultrasonic. Of the other two studies, Hübner et al.,5 did not perform direct comparisons between the technologies (only three-way analysis of variance) and the results of the study of Guerreri et al, 20088 were repeated, confirming the reported significant decrease in time with the LigaSureTM device compared to the ultrasonic technology. In the larger studies of Campagnacci7 and Rimonda,9 only surgery types with 20 or more patients were included for analysis. All, mixed types of colectomy procedures; AR, anterior resection; LC, left hemicolectomy; RC, right hemicolectomy. Bars indicate estimated means, error bars standard deviations.

Global Value Dossier: LigaSureTM Technology 16
Figure 3-9 Intra-operative blood loss with LigaSureTM technology compared to other energy devices for colectomy
0
100
200
300
400
500
600
Blo
od
loss
(m
l)
18
ColectomyLS vs OAE
LigaSureTM Technology
Monopolar Scissors
Ultrasonic technology
LCNS
AllNS
LC***
LCNS
LCNS
RC***
RC*
Authors Surgery Comp class LS res LS err LS N OE res OE err OE N sig
Tou 2011 All MES 108.6 139.1 138.5 115.1 0.45
Hübner 2008 LC MES 50 150 21 125 112.5 20 0.223(K-W)
Rimonda 2009 All UCS 111.2 51.5 70 107.9 42 70 0.72
Tou 2011 All UCS 111.109 49.9354 107.361 40.78187 0.63
Campagnacci 2007 RC UCS 115 32.5 32 370 132.5 37 <0.001
Guerreri 2008 RC UCS 115 67.5 45 220 62.5 44 <0.05
Campagnacci 2007 LC UCS 150 37.5 50 455 143.75 47 <0.001
Rimonda 2009 LC UCS 105.9 46 37 103 59.7 32 0.83
Hübner 2008 LC UCS 50 150 21 50 125 20 0.223(K-W)
Rimonda 2009 AR UCS 128 50.1 18 123.8 50.7 22 0.84
AllNS
ARNS
For studies comparing LigaSureTM devices to other energy devices, the types of surgeries included in each analysis are shown above the comparisons, along with indication of statistical significance (* = p ≤ 0.05, *** = p ≤ 0.001, NS = non-significant at the 95% confidence level). In the larger studies of Campagnacci7 and Rimonda,9 only surgery types with 20 or more patients were included for analysis. All, mixed types of colectomy procedures; AR, anterior resection; LC, left hemicolectomy; RC, right hemicolectomy. Bars indicate estimated means, error bars standard deviations.
Figure 3-10 Change in length of hospital stay with LigaSureTM technology compared to other energy devices for colectomy
0
2
4
6
8
10
12
14
16
18
Le
ng
th o
f st
ay (d
ays)
21
ColectomyLS vs OAE
LCNS
AllNS
ARNS
LCNS
LCNS
RCNS
LCNS
LigaSureTM Technology
Monopolar Scissors
Ultrasonic technology
AllNS
RCNS
Comparator ID SurgType Comparat
or
Outcomes LS res LS err OE res OE err sig
MES Tou 2011 All MES LoS (d) 9.2 6.70 9.7 5.8 0.8
MES Hübner 2008 LC MES LoS (d) 7 7.00 8.5 6 0.446 (K-W)
UCS (Harmonic Ace) Rimonda 2009 All UCS LoS (d) 6.9 3.30 7.4 2.2 0.37
UCS Tou 2011 All UCS LoS (d) 7.03 3.14 7.44 2.09 0.8
UCS Campagnacci 2007 RC UCS LoS (d) 5.2 0.50 6.1 0.25 NS
UCS (Harmonic Ace) Guerreri 2008 RC UCS LoS (d) 5.2 0.50 6.1 0.25 NS
UCS Campagnacci 2007 LC UCS LoS (d) 6.5 0.50 7.3 0.5 NS
UCS (Harmonic Ace) Rimonda 2009 LC UCS LoS (d) 7.2 1.90 7.4 2.3 0.85
UCS (Harmonic Ace) Hübner 2008 LC UCS LoS (d) 7 7.00 7 6.25 0.446(K-W)
UCS (Harmonic Ace) Rimonda 2009 AR UCS LoS (d) 6.7 1.00 8.2 5 0.35
Bars indicate estimated means, error bars standard deviations, and above the comparisons are the types of colectomy included in each study (All, mixed types of colectomy procedures; AR, anterior resection; LC, left hemicolectomy; RC, right hemicolectomy). In the larger studies of Campagnacci7 and Rimonda,9 only surgery types with 20 or more patients were included for analysis. None of the comparisons yielded statistically significant differences (NS, non-significant) at the 95% confidence level.

Global Value Dossier: LigaSureTM Technology 17
3.6.2. Surgical experience considerations
A single randomized controlled trial has reported an effort to measure the generation of smoke by the various energy devices in vivo, during surgery.5 The authors note that this parameter is difficult to quantify, and thus reported use of the consumption of CO2 to maintain a clear field as a proxy for smoke generated from each device (Figure 3-11). In this analysis, LigaSureTM devices generated the least smoke of the three devices used (with monopolar scissors and ultrasonic shears as comparators).
Figure 3-11 Intraoperative carbon dioxide usage with LigaSureTM technology versus other energy devices for colectomy
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
CO
2 u
sag
e (l
/min
)
20
ColectomyLS vs OAE
LigaSureTM MES UCS
LigaSureTM Technology
Monopolar Scissors
Ultrasonic technology
*
*
Authors used consumption of carbon dioxide as a proxy for smoke generated by each energy device during laparoscopic colorectal surgery.5 Bars indicate medians, error bars estimated standard deviations. The authors reported statistical testing on the three-way analysis of variance Kruskal-Wallis test. Subsequent independent testing using provided data indicated statistically significantly lower carbon dioxide use in direct comparisons with the monopolar scissors and ultrasonic shears (* = p ≤ 0.05, two-tailed t-test, Bonferroni multiple testing correction).
The same study also reported on surgeon satisfaction with features of LigaSureTM, monopolar, and ultrasonic devices5 (Figure 3-12). Results are from 12 different surgeons, and while overall, the devices demonstrate similar ratings (p = 0.425), in specific categories of safety profile, handling and bleeding control, significant differences were observed (p < 0.001). From the physicians’ perspective, within these comparisons, LigaSure™ devices demonstrated the best median ratings for safety and bleeding control, and significantly better handling than ultrasonic coagulating shears (p < 0.001).5
Figure 3-12 Surgeon satisfaction with LigaSureTM devices compared to other energy devices
0
1
2
3
4
5
6
7
8
9
10
Bleeding control Handling Safety Overall
Su
rge
on
ass
ess
me
nt
(VA
S)
21
Colectomy EconomicsLS vs OAE
*** LigaSureTM Technology
Monopolar Scissors
Ultrasonic technology
*** ***NS
Bars represent a visual analog score (VAS) on a scale from 0 to 10, where higher values indicate greater satisfaction with the device in the indicated categories of bleeding control, handling, safety, and an overall evaluation.5 Bars indicate medians, uncertainties/ranges were not reported (preventing independent post hoc pairwise testing) although significance from three-way analysis of variance (Kruskal-Wallis test; *** = p ≤ 0.001) from simultaneous comparison of all three technologies were given.

Global Value Dossier: LigaSureTM Technology 18
4. Economic impact of LigaSureTM technology
4.1. Overview
Summary and key messages
Shorter surgical times with LigaSureTM devices: LigaSureTM technology has demonstrated significantly shorter operative times compared to alternative methods of ligation in colorectal resection.1-8
Reduced operating room supply costs: In colectomy, direct analysis of costs revealed the single use LigaSureTM device to significantly reduce operating room supply costs by over 20% compared to reusable monopolar scissors.5
Equivalent costs and improved satisfaction compared to ultrasonic technology: Direct cost analysis of LigaSureTM devices for colectomy procedures found equivalence in operating room supply and overall procedure costs compared to ultrasonic technology,5 but the same study revealed significantly higher ratings in handling for the LigaSureTM device over the ultrasonic comparator.5
LigaSureTM devices reduce overall costs across a range of procedures: Analysis of different types of colorectal resection (including total colectomy, left hemicolectomy, and proctectomy), found savings with LigaSureTM device use of $100 to $400 per procedure (2016 USD).1,6
4.2. Health economics of surgery
As described earlier (Sections 3.3), the need for colorectal intervention ranges from life-saving interventions in the case of colonic neoplasms, to the severely debilitating pain of prolapsed hemorrhoids. Incidence of surgeries for the different procedures to address these morbidities will thus vary around the world. Wherever applicable, however, achieving efficiencies in the administration of surgical procedures has the potential to impact healthcare budgets and realize savings for payers.
As with any surgery, direct costs are incurred for consumables and hospital resources such as staffing and administration. The former contribute to variable costs, which will change with procedure volume while the latter may be fixed and thus not influenced by surgical parameters.14 Operating room costs vary widely by setting (Figure 4-1); estimates have ranged from USD 22 per minute (inflation adjusted to 2016 USD from 2009 USD)14 to a direct reporting of costs from a single Swiss center in a report on colectomy procedures5 of costs of USD 10 (inflation adjusted to 2016 USD from 2007 EUR). In seeking cost-saving strategies, the variable costs per procedure, which will include factors such as operative time and resource utilization, post-operative complications, and patient experience15 are one area more readily targeted than fixed costs such as building rental. Devices or changes to procedures that reduce components of the variable costs (operating room time or complications for example) per procedure have the potential to increase savings.

Global Value Dossier: LigaSureTM Technology 19
Figure 4-1 Operating room costs per minute
$0 $5 $10 $15 $20 $25 $30
Scotland 2016
Wales 2012
United States 2009
Switzerland 2007
2016 US Dollars
31
Colectomy EconomicsOR costs
Operating room costs per minute as reported in publications (US 2009 from survey average estimate,14 Switzerland 2007 from single center report,5 Scotland 2016 from regional averageb and Wales 2016 reported by a single NHS trustc). Corresponding values inflated to 2016 USD
4.3. Economics of colorectal procedures
The unmet needs for colorectal procedures will vary widely by the type of intervention. In the case of colectomies, surgeries can last hours and blood losses can be considerable. One study examining colectomy complications and their impact on hospital reimbursements found colectomy payments to increase by 81% per complication over the average for uncomplicated procedures, and prolonged ventilation to be the most expensive complication, more than doubling mean payment.16
4.4. LigaSureTM technology impact on colectomy
In general, fewer studies report on costs or economics related to surgical procedures than do for clinical outcomes. However, direct cost analyses for LigaSureTM technology have been reported for colectomy procedures, where the devices have been compared both to conventional ligation methods1,6 (Figure 4-2), and to other energy devices5 (Figure 4-3). Considered across the range of colectomy procedures, LigaSureTM technology has demonstrated significant cost savings (up to $400 per procedure in 2016 USD)1 in comparison to conventional ligation. For specific variants of colectomy, left hemicolectomy, total hemicolectomy, and proctectomy have also shown savings. Right hemicolectomy in the indicated study showed an increase in costs; the authors hypothesize that this contrary result may be due to the reduced complexity of right hemicolectomy compared to the others performed in the study.1
b Table RX140X_2016, http://www.isdscotland.org/Health-Topics/Finance/Costs/Detailed-Tables/Theatres.asp c Freedom of information request FoI.13.319, http://www.cardiffandvaleuhb.wales.nhs.uk/freedom-of-information-disclosure-log-20-2

Global Value Dossier: LigaSureTM Technology 20
Compared to other energy devices, LigaSureTM devices have been shown to be superior in terms of lower costs per procedure compared to monopolar scissors.5 Results indicate a significant reduction of 22% in operating room supply costs compared to monopolar scissors (p = 0.011),d,5 while costs were equivalent to those for ultrasonic coagulating shears (p = 0.18).d,5 Since the per procedure costs averaged over a year are comparable between LigaSureTM and ultrasonic technologies, other factors such as surgeon satisfaction in handling of the devices (Figure 3-12) may become a contributing factor in decisions regarding which technology to use.
Figure 4-2 Per procedure cost analysis results of LigaSureTM devices compared to conventional ligation in colectomy
-$600
-$500
-$400
-$300
-$200
-$100
$0
$100
$200
TC PC LC RC All All
∆ C
ost
s (2
01
6 U
SD
)
38
Colectomy EconomicsLS vs OAE
***
Adamina 2011Tou
2011
** *
*
*
*
All, cases where costs were not separated according to type of colectomy; LC, left hemicolectomy; PC, proctectomy; RC, right hemicolectomy; TC, total colectomy; A randomized controlled trial1 and a meta-analysis6 examining LigaSureTM technology disposable instrument1,6 and total procedure cost differences are shown. In each study, averaged across all types of colectomy, LigaSureTM devices resulted in statistically significant (at the 95% confidence level) savings compared to clips and staples. Asterisks indicate p-values (* = p ≤ 0.05; ** = p ≤ 0.01; *** = p ≤ 0.001). When stratified by surgery, most individual procedures also result in cost savings, with the exception of right hemicolectomy. Bars indicate mean price differences (inflated to 2016 USD from original reported values), error bars are estimated standard deviations.
d Values calculated from two-tailed t-test, performed using reported costs from Hübner et al., 2008

Global Value Dossier: LigaSureTM Technology 21
Figure 4-3 Per procedure cost analysis results of LigaSureTM devices compared to other energy devices in colectomy
$0
$500
$1,000
$1,500
$2,000
$2,500
$3,000
Additional OR Tot/pt 100/yr Tot/pt 200/yr
Co
sts
(20
16
US
D)
28
Colectomy EconomicsLS vs OAE
NR
NR
* **LigaSureTM Technology
Monopolar Scissors
Ultrasonic technology
An analysis of colectomy costs in left colectomies5 revealed statistically significant differences (at the 95% confidence level) across the three energy devices used, where inference testing was reported. Asterisks above the bars indicate p-values (* = p ≤ 0.05; ** = p ≤ 0.01). Costs were divided into additional costs, costs for the operating room, and analyses were performed to determine the potential for savings with costs per case if a center performs 100 or 200 surgeries per year. In these latter analyses, costs were shown to be significantly lower for LigaSureTM devices in comparison to monopolar scissors, while largely overlapping with costs for LigaSureTM and ultrasonic devices. Bars indicate medians with estimated standard deviations and values above are p-values from three-armed analysis of variance (Kruskal-Wallis). Costs have been converted and inflated to 2016 USD from 2007 EUR.

Global Value Dossier: LigaSureTM Technology 22
5. Conclusions
Diseases affecting the lower human digestive tract range in severity and impact on a patient’s life. Indications for surgery include both benign and malignant morbidities and surgical interventions may require removal of the colon in whole or in part. Depending on the indication, outcomes may focus more on survival in the case of neoplasia, or quality of life measures in relieving patient symptoms for lower-mortality conditions such as ulcerative colitis.
LigaSureTM technology for vessel dividing/sealing and tissue division is designed for intraoperative hemostasis. The devices and the associated power generators have been successfully applied in various settings around the world, and for a variety of surgeries involving the human colon. These procedures include the resection of the colon from right1,3 to transverse3 to left1,3,5 hemicolectomies, anterior resections9 and total colectomy.1 Relative to conventional ligation (clips and staples), LigaSureTM technology has achieved many superior patient outcomes. Operative times,1-4,6 and blood loss2,3,6 during colon resection are two parameters where improvements have been achieved with LigaSureTM device use. LigaSureTM technology has also been shown not to increase rates of overall,4,6 intra-operative1,2 and post-operative1,2,4 complications.
Fewer comparisons between LigaSureTM technology and other energy devices have been reported than in comparison to conventional methods of ligation. Compared to monopolar shears, LigaSureTM devices have demonstrated shorter operative times6 and non-significantly reduced blood loss6 and equivalent lengths of hospital stays.6 Results for ultrasonic devices with respect to operative parameters such as time5,9 and blood loss,5,9 and total complication rates5,8,9 are equivalent to those achieved with LigaSureTM devices.
In terms of their economic impact, LigaSureTM devices have the potential to lower operational costs. Demonstrated time savings relative to conventional ligation in colectomy1-4 would result in less consumption of hospital resources such as operating room occupancy. The potential for this effect has been noted by surgeons who report that higher device costs would be offset by reduced staffing and anesthesia costs.3 A further advantage for physicians is that staplers and clip appliers require reloads, whereas the LigaSureTM device can be used throughout the procedure.13 Direct analysis of costs has supported these potential savings, finding the use of LigaSureTM devices in comparison to conventional ligation to be cost saving, with up to USD400 saved per procedure, for colectomy surgeries considered together.1,6
Where surgical intervention resection or removal of the colon is indicated, LigaSureTM devices are a viable option demonstrating the potential for improved patient outcomes, and benefits to payers in comparable or reduced material costs and the potential for savings in use of other care center resources.

Global Value Dossier: LigaSureTM Technology 23
6. Source data tables
Refer to section 1.2 for scope of literature presented in the following data tables.
6.1.Data table summary: LigaSureTM technology colectomy surgical outcome data
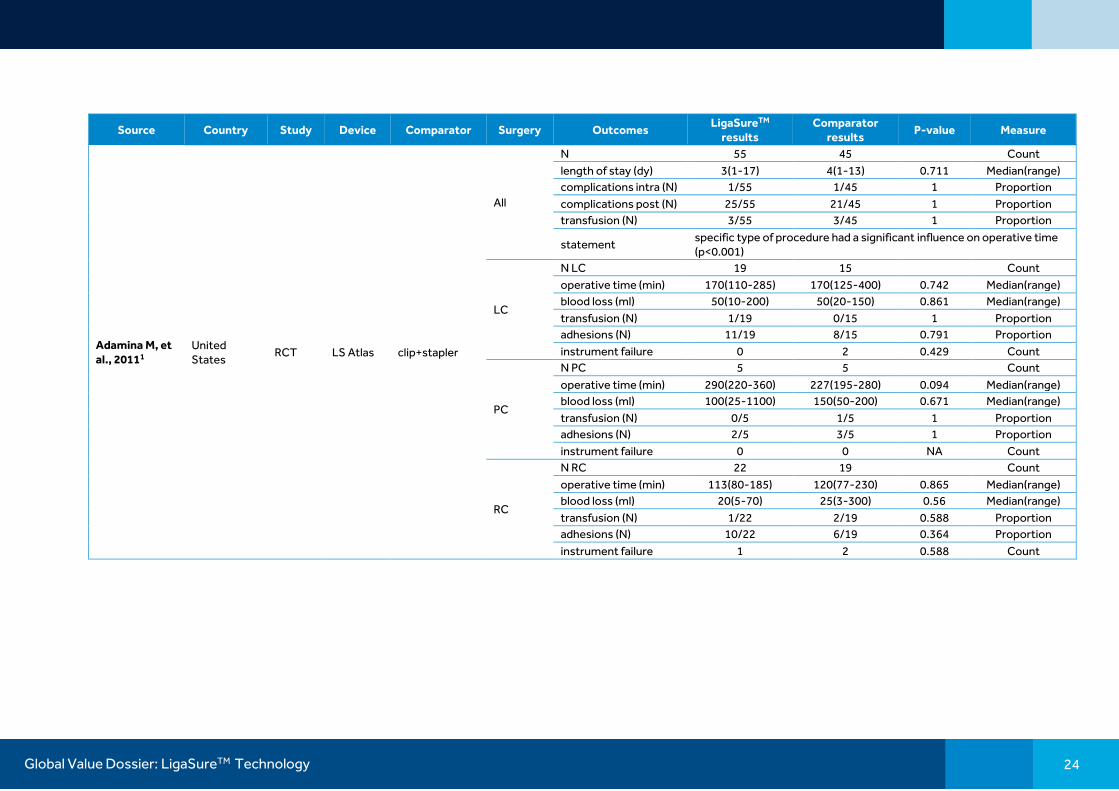
Table 6-1 Publication data reporting on LigaSureTM technology for clinical outcomes in colectomy
Source Country Study Device Comparator Surgery Outcomes LigaSureTM
results Comparator
results P-value Measure
Trilling B, et al., 20164
France retro NR* (95% LS, 5% UCS)
clip+stapler SIG
N 101 99
Count
time operative (min) 200.72 253.74 <0.001 Mean
length of stay (dy) 8.1 10.4 <0.001 Mean
complications all (N) 25/101 31/99 0.25 Proportion
complications major (N)
3/101 11/99 0.68 Proportion
transfusion (N) 3/101 1/99 0.56 Proportion
fistula (N) 0/101 3/99 0.25 Proportion
infection (N) 16/101 24/99 0.21 Proportion
delta Hg (g/dl) -12.78 -13.16 0.82 Mean
conversion to open (N) 9 14 0.27 Proportion
Di Lorenzo N, et al., 201213
Italy* MA NR UltracisionTM*
LCR N 200 197
Count
blood loss (SMD) -0.156
[-1.001,-0.031] 0.037 SMD[CI]
time operative (SMD) -0.723
[-1.296,-0.150] 0.013 SMD[CI]
Global Value Dossier: LigaSureTM Technology 24
Source Country Study Device Comparator Surgery Outcomes LigaSureTM
results Comparator
results P-value Measure
Adamina M, et al., 20111
United States
RCT LS Atlas clip+stapler
All
N 55 45
Count
length of stay (dy) 3(1-17) 4(1-13) 0.711 Median(range)
complications intra (N) 1/55 1/45 1 Proportion
complications post (N) 25/55 21/45 1 Proportion
transfusion (N) 3/55 3/45 1 Proportion
statement specific type of procedure had a significant influence on operative time (p<0.001)
LC
N LC 19 15
Count
operative time (min) 170(110-285) 170(125-400) 0.742 Median(range)
blood loss (ml) 50(10-200) 50(20-150) 0.861 Median(range)
transfusion (N) 1/19 0/15 1 Proportion
adhesions (N) 11/19 8/15 0.791 Proportion
instrument failure 0 2 0.429 Count
PC
N PC 5 5
Count
operative time (min) 290(220-360) 227(195-280) 0.094 Median(range)
blood loss (ml) 100(25-1100) 150(50-200) 0.671 Median(range)
transfusion (N) 0/5 1/5 1 Proportion
adhesions (N) 2/5 3/5 1 Proportion
instrument failure 0 0 NA Count
RC
N RC 22 19
Count
operative time (min) 113(80-185) 120(77-230) 0.865 Median(range)
blood loss (ml) 20(5-70) 25(3-300) 0.56 Median(range)
transfusion (N) 1/22 2/19 0.588 Proportion
adhesions (N) 10/22 6/19 0.364 Proportion
instrument failure 1 2 0.588 Count

Global Value Dossier: LigaSureTM Technology 25
Source Country Study Device Comparator Surgery Outcomes LigaSureTM
results Comparator
results P-value Measure
Adamina M, et al., 20111
United States
RCT LS Atlas clip+stapler TC
N TC 9 6
Count
operative time (min) -103.6
(-185.1,-22.3) 0.023 Mean(range)
operative time (min) 209(105-305) 312(185-400) 0.045 Median(range)
blood loss (ml) 50(5-250) 100(10-150) 0.406 Median(range)
transfusion (N) 1/9 0/6 1 Proportion
adhesions (N) 0/9 2/6 0.143 Proportion
instrument failure (N) 2 1 1 Count
Martin ST, et al., 201117
Ireland SA LS 5mm/LS 10mm
none
All N 802
Count
RC N 180
Count
LC N 96
Count
SIG N 347
Count
AR N 179
Count
All statement "Of 802 cases in which the LigaSureTM device was employed to divide major vascular structures, immediate effective vessel sealing was achieved in 99.8% (n = 800)"

Global Value Dossier: LigaSureTM Technology 26
Source Country Study Device Comparator Surgery Outcomes LigaSureTM
results Comparator
results P-value Measure
Tou S, et al., 20116
United Kingdom*
MA NR
clip+stapler All
N blood loss 52 48
Count
blood loss (ml) 217(167) 231(166) 0.67 Mean(SD)
blood loss (ml) -14.00
[-79.31,51.31] 0.67 Mean[CI]
time operative (min) 179(62) 190(70) 0.41 Mean(SD)
N complications all 52 48
Count
complications all (N) 1/52 0/48 0.53 Proportion
MES All
N blood loss 20 21
Count
blood loss (ml) 108.6(139.1) 138.5(115.1) 0.45 Mean(SD)
time operative (min) 104.7(31.8) 144.8(43.4) 0.00078 Mean(SD)
time operative (min) -40.1
[-63.48,-16.72] 0.00078 Mean[CI]
length of stay (dy) 9.2(6.7) 9.7(5.8) 0.8 Mean(SD)
length of stay (dy) -0.5
[-3.33,4.33] 0.8 Mean[CI]
N complications all 36 31
Count
complications all (N) 12/36 14/31 0.38 Proportion
UCS All
N blood loss 91 90
Count
blood loss (ml) +3.74
[-11.55,19.04] 0.63 Mean[CI]
time operative (min) +3.22
[-8.87,+15.31] 0.6 Mean[CI]
length of stay (dy) -0.41
[-1.31,+0.49] 0.42 Mean[CI]
N complications all 106 102
Count
complications all (N) 22/106 17/102 0.45 Proportion

Global Value Dossier: LigaSureTM Technology 27
Source Country Study Device Comparator Surgery Outcomes LigaSureTM
results Comparator
results P-value Measure
Nakajima K, et al., 20102
Japan retro LS Atlas clip + Harmonic
ScalpelTM*
PC (HALS-RP)
N 37 29
Count
blood loss (ml) 185(0-900) 365(140-2045) <0.05 Median(range)
time operative (min) 255(177-390) 340(225-480) <0.05 Median(range)
length of stay (dy) 30(19-165) 30(17-84)
Median(range)
complications intra (N) 0/37 1/29
Proportion
complications post (N) 12/37 16/29
Proportion
transfusion (N) 6/37 9/29
Proportion
complications infection (N)
4/37 8/29
Proportion
Takiguchi N, et al., 20103
Japan
RCT (MC)
LS Atlas clip+stapler
All (RC, Trans, LC, SIG, AR)
N 45 32
Count
blood loss (ml) 217.3(225.9) 304.5(365.7) 0.238 Mean(SD)
time operative (min) 187.5(70.7) 208.3(70.4) 0.207 Mean(SD)
length of stay (dy) 14.2(11.2) 14.1(7.1) 0.962 Mean(SD)
complications all (N) 9 (complics) 8 (complics) ns Proportion
RCT (SC)
LS Atlas clip+stapler
All (RC, Trans, LC, SIG, AR)
N 22 15
Count
blood loss (ml) 150.5(132.8) 381.9(443.5) 0.0465 Mean(SD)
time operative (min) 156.5(42.7) 202.3(55.4) 0.02 Mean(SD)
length of stay (dy) 11.0(3.96) 12.1(5.8) 0.506 Mean(SD)
Global Value Dossier: LigaSureTM Technology 28
Source Country Study Device Comparator Surgery Outcomes LigaSureTM
results Comparator
results P-value Measure
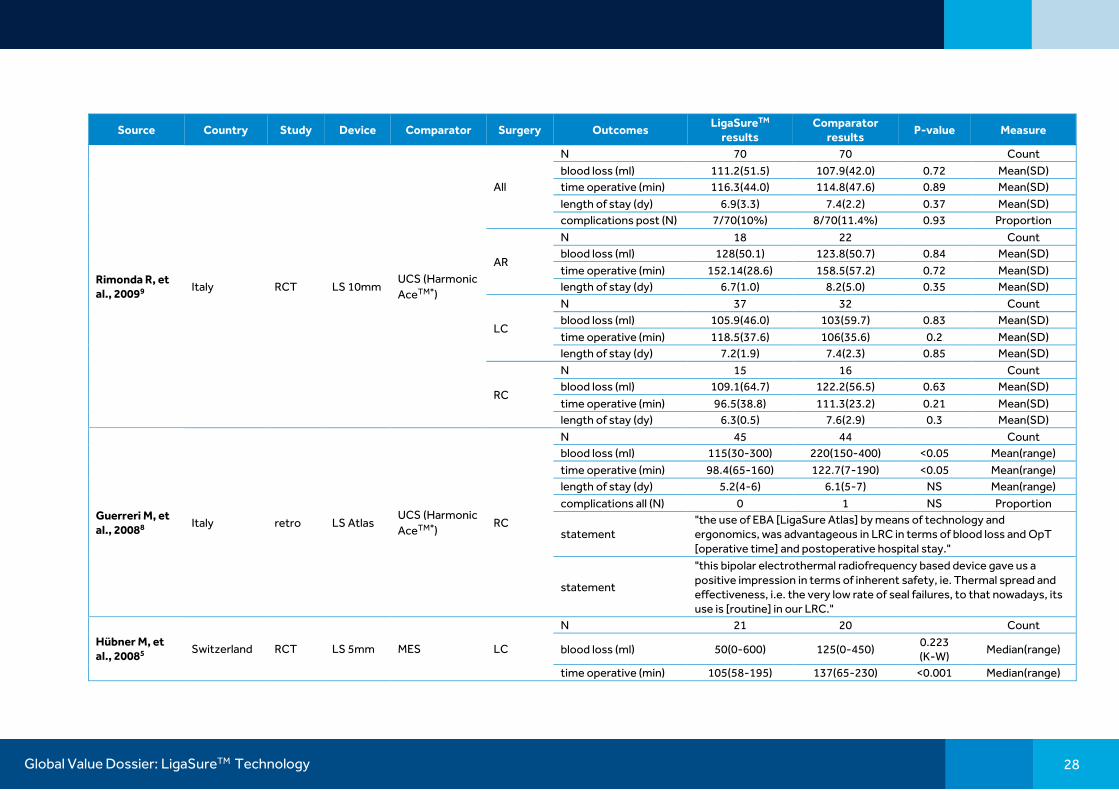
Rimonda R, et al., 20099
Italy RCT LS 10mm UCS (Harmonic
AceTM*)
All
N 70 70
Count
blood loss (ml) 111.2(51.5) 107.9(42.0) 0.72 Mean(SD)
time operative (min) 116.3(44.0) 114.8(47.6) 0.89 Mean(SD)
length of stay (dy) 6.9(3.3) 7.4(2.2) 0.37 Mean(SD)
complications post (N) 7/70(10%) 8/70(11.4%) 0.93 Proportion
AR
N 18 22
Count
blood loss (ml) 128(50.1) 123.8(50.7) 0.84 Mean(SD)
time operative (min) 152.14(28.6) 158.5(57.2) 0.72 Mean(SD)
length of stay (dy) 6.7(1.0) 8.2(5.0) 0.35 Mean(SD)
LC
N 37 32
Count
blood loss (ml) 105.9(46.0) 103(59.7) 0.83 Mean(SD)
time operative (min) 118.5(37.6) 106(35.6) 0.2 Mean(SD)
length of stay (dy) 7.2(1.9) 7.4(2.3) 0.85 Mean(SD)
RC
N 15 16
Count
blood loss (ml) 109.1(64.7) 122.2(56.5) 0.63 Mean(SD)
time operative (min) 96.5(38.8) 111.3(23.2) 0.21 Mean(SD)
length of stay (dy) 6.3(0.5) 7.6(2.9) 0.3 Mean(SD)
Guerreri M, et al., 20088
Italy retro LS Atlas UCS (Harmonic
AceTM*) RC
N 45 44
Count
blood loss (ml) 115(30-300) 220(150-400) <0.05 Mean(range)
time operative (min) 98.4(65-160) 122.7(7-190) <0.05 Mean(range)
length of stay (dy) 5.2(4-6) 6.1(5-7) NS Mean(range)
complications all (N) 0 1 NS Proportion
statement "the use of EBA [LigaSure Atlas] by means of technology and ergonomics, was advantageous in LRC in terms of blood loss and OpT [operative time] and postoperative hospital stay."
statement
"this bipolar electrothermal radiofrequency based device gave us a positive impression in terms of inherent safety, ie. Thermal spread and effectiveness, i.e. the very low rate of seal failures, to that nowadays, its use is [routine] in our LRC."
Hübner M, et al., 20085
Switzerland RCT LS 5mm MES LC
N 21 20
Count
blood loss (ml) 50(0-600) 125(0-450) 0.223 (K-W)
Median(range)
time operative (min) 105(58-195) 137(65-230) <0.001 Median(range)

Global Value Dossier: LigaSureTM Technology 29
Source Country Study Device Comparator Surgery Outcomes LigaSureTM
results Comparator
results P-value Measure
(K-W)
length of stay (dy) 7(3-31) 8.5(5-29) 0.446 (K-W)
Median(range)
complications all (N) 10/21 10/20 0.375 Proportion
CO2=smoke prod (l/min)
0.54(0-2.60) 1.18(0-2.48) 0.042 (K-W)
Median(range)
surgeon satisfaction bleeding control
8.4 5.1 <0.001 (K-W)
Median VAS (SD NR)
surgeon satisfaction handling
7.9 8.8 <0.001 (K-W)
Median VAS (SD NR)
surgeon satisfaction Overall
8 7.7 0.425 (K-W)
Median VAS (SD NR)
surgeon satisfaction safety
8.6 6 <0.001 (K-W)
Median VAS (SD NR)
Hübner M, et al., 20085
Switzerland RCT LS 5mm UCS (Harmonic
AceTM*) LC
N 21
Count
blood loss (ml) 50(0-600) 50(0-500) 0.223 (K-W)
Median(range)
time operative (min) 105(58-195) 90(45-177) <0.001 (K-W)
Median(range)
length of stay (dy) 7(3-31) 7(3-28) 0.446 (K-W)
Median(range)
complications all (N) 10/21 6/20 0.375 Proportion
CO2=smoke prod (l/min)
0.54(0-2.60) 0.99
(0.34-1.74) 0.042 (K-W)
Median(range)
surgeon satisfaction bleeding control
8.4 7.9 <0.001 (K-W)
Median VAS (SD NR)
surgeon satisfaction handling
7.9 4.8 <0.001 (K-W)
Median VAS (SD NR)
surgeon satisfaction Overall
8 7.7 0.425 (K-W)
Median VAS (SD NR)
surgeon satisfaction safety
8.6 7.8 <0.001 (K-W)
Median VAS (SD NR)
Campagnacci R, et al., 20077
Italy retro LS V 5mm
UCS AR N 18 16
Count
blood loss (ml) 185(100-285) 495(280-900) 0.002 Mean(range)

Global Value Dossier: LigaSureTM Technology 30
Source Country Study Device Comparator Surgery Outcomes LigaSureTM
results Comparator
results P-value Measure
time operative (min) 153(130-220) 201(145-320) NS Mean(range)
length of stay (dy) 6.8(5-8) 7.3(6-8) NS Mean(range)
LC
N 50 47
Count
blood loss (ml) 150(70-220) 455(270-845) <0.001 Mean(range)
time operative (min) 140(120-170) 176(95-240) NS Mean(range)
length of stay (dy) 6.5(5-7) 7.3(6-8) NS Mean(range)
RC
N 32 37
Count
blood loss (ml) 115(30-160) 370(150-680) <0.001 Mean(range)
time operative (min) 111(70-195) 133(95-190) NS Mean(range)
length of stay (dy) 5.2(4-6) 6.1(5-7) NS Mean(range)
Hübner M, et al., 200718
Switzerland SA* (RCT)
LS 10mm none LC
N 15
Count
blood loss (ml) 200(50-400)
Median(range)
time operative (min) 210(160-420)
Median(range)
length of stay (dy) 6(3-28)
Median(range)
LS 5mm none LC
N 15
Count
blood loss (ml) 100(25-300)
Median(range)
time operative (min) 200(110-330)
Median(range)
length of stay (dy) 5(3-14)
Median(range)
All, mixed types of colectomy, results not separated for specific type (types included are listed when reported); AR, anterior resection; CI, 95% confidence interval; CO2 usage, volume in liters per minute used during surgery, which authors used as proxy for smoke generated by each device to keep surgical field clear; complics, complications (study report of total number of complications without specification of how many patients experienced them); dy, days; HALS-RP, hand-assisted laparoscopic restorative proctocolectomy; K-W, Kruskal Wallis test for analysis of variance; LC, left hemicolectomy; LS, LigaSureTM, MA, meta-analysis; MC, multicenter; MES; monopolar electrosurgical scissors; NA, not applicable (test statistics are incalculable when, for example, there are no events in either treatment group); NR, not reported; NS, not significant; OR, operating room; PC, proctectomy; RC, right hemicolectomy; RCT, randomized controlled trial; retro, retrospective study; SA*(RCT), single arm randomized controlled study (single arm due to comparison between two LigaSureTM products); SC, single center; SIG, sigmoidectomy; Sig/pval, significance/p-value from statistical testing; SMD, standardized mean difference; TC, total colectomy; Trans, transverse colon resection; UCS, ultrasonic coagulation shears.
None of the colectomy studies reported specifically which generator was used with the LigaSureTM device. In the study of Trilling et al., 2016,4 authors compared electrosurgical vessel sealing (EVSS) to conventional ligation. Of the 100 devices in the EVSS arm, 95 were LigaSureTM while 5 were ultrasonic coagulation shears. No subdivision was reported. In the study of Hübner et al., 2007,18 the comparison performed was a randomized controlled trial between LigaSureTM 5mm and 10mm devices. For the purposes of this report, it is therefore considered single arm since both are LigaSureTM devices. Statistical significance (p-values) are shown as reported; refer to individual figures within the document for results of independent inference testing from provided data.
In the study of Takiguchi N, et al., 2010,3 the randomized controlled trial was performed across multiple centers (MC). A subset analysis for a single center (SC) focused on the location with the highest surgical volume.

Global Value Dossier: LigaSureTM Technology 31
6.2.Data table summary: LigaSureTM technology economic data
Table 6-2 Publication data reporting on economics related to LigaSureTM technology use
Study Country Study Surgery Device Generator Comparator Outcomes LigaSureTM results Comparator
results P-value Measure
Adamina M, et al., 20111
United States
RCT
All LS Atlas NR clip+stapler N 55 45
count
costs (2010 USD)
-$80.7 (-$152.1,-$9.4)
0.043 Mean
(range)
LC LS Atlas NR clip+stapler N LC 19 15
count
costs (2010 USD)
-$88.2 (-163.6,-12.8)
0.037 Mean
(range)
PC LS Atlas NR clip+stapler N PC 5 5
count
costs (2010 USD)
-$366.9 (-$643.8,-$90.0)
0.012 Mean
(range)
RC LS Atlas NR clip+stapler N RC 22 19
count
costs (2010 USD)
+$92.6 (+$27.6,+$157.5)
0.012 Mean
(range)
TC LS Atlas NR clip+stapler N TC 9 6
count
costs (2010 USD)
-$377.7 (-$583.9,-$171.5)
0.005 Mean
(range)
Tou S, et al., 20116
United Kingdom*
MA All NR NR clip+stapler
costs (2004 USD)
-83.00 [-114.68,-51.32]
<0.00001 Mean[CI]
MES costs (2004 USD)
-267.00 [-475.61,-58.39]
0.012 Mean[CI]
Martin ST, et al., 2011
Ireland SA AR
LS 5mm/ LS 10mm
NR none statement
"Laparoscopic division of the major mesenteric vessels with LigaSureTM may reduce operative costs as it obviates the need for endoscopic clip applicators or vascular staplers to divide the mesenteric vascular pedicles."

Global Value Dossier: LigaSureTM Technology 32
Study Country Study Surgery Device Generator Comparator Outcomes LigaSureTM results Comparator
results P-value Measure
Hubner M, et al., 20085
Switzerland RCT LC LS 5mm NR
MES
N 21 20
Count
costs (2007 EUR) Additional
0 (0-127) 102
(4-635) Median (range)
costs (2007 EUR) OR
812 (450-1515) 1045 (505-1786)
Median (range)
costs (2007 EUR) Tot/pt 100/yr
1204 (840-2031) 1382 (752-2386) 0.021 (K-W)
Median (range)
costs (2007 EUR) Tot/pt 200/yr
1185 (820-2011) 1382 (752-2386) 0.009 (K-W)
Median (range)
UCS (Harmonic
AceTM*)
N 21 20
count
costs (2007 EUR) Additional
0 (0-127) 13 (0-131)
Median (range)
costs (2007 EUR) OR
812 (450-1515) 699 (350-1375)
Median (range)
costs (2007 EUR) Tot/pt 100/yr
1204 (840-2031) 1138 (784-1818) 0.021 (K-W)
Median (range)
costs (2007 EUR) Tot/pt 200/yr
1185 (820-2011) 1105 (752-1786) 0.009 (K-W)
Median (range)
In the study by Adamina et al.1 , costs for LigaSureTM device use versus conventional ligation were not reported. Only the difference in cost with associated confidence interval was indicated in the publication. Where the surgery type is shown as “All”, the authors did not separate results by type of colectomy. AR, anterior resection; CI, 95% confidence interval; EUR, euros; K-W, Kruskal Wallis test for analysis of variance; LC, left hemicolectomy; LS, LigaSureTM, MA, meta-analysis; MES; monopolar electrosurgical scissors; NR, not reported; OR, operating room; PC, proctectomy; RC, right hemicolectomy; RCT, randomized controlled trial; SA, single arm study, TC, total colectomy; Tot/pt [100/200]/yr, total (costs) per patient, assuming the given number of procedures are performed per year; UCS, ultrasonic coagulation shears; USD, United States dollars.

Global Value Dossier: LigaSureTM Technology 33
7. Structured literature search details
7.1.Searches performed
Structured searches were performed to identify literature reporting on clinical applications of LigaSureTM technology. The searches were divided into two streams: one to identify the most recent clinical evidence of the use of LigaSureTM devices (within the last 10 years) in colorectal surgery procedures (including colectomies and hemorrhoidectomies), and a second parallel search to identify all clinical applications of LigaSureTM technology, regardless of time, to identify settings in which the devices have been used in patient care. The search was performed on February 27, 2017.
Table 7-1 Structured searched in PubMed to identify relevant LigaSureTM technology data
Index Aim Search string Hits
#1 LigaSureTM by product name ligasure*[tiab] OR ligasuretm[tiab] OR ligasurev*[tiab] 614
#2 Generic names for LigaSureTM
EBVS[tiab] OR BVSS[tiab] OR ((bipolar[tiab] OR ((high[tiab] OR advanced[tiab]) AND energy[tiab]) OR radiofrequency[tiab]) AND (diathermy[tiab] OR cautery[tiab] OR electrocautery[tiab] OR electrocauterization[tiab] OR electrocauterisation[tiab] OR cauterization[tiab] OR cauterisation[tiab] OR coagulation[tiab] OR ((vessel[tiab] OR tissue[tiab]) AND (sealing[tiab] OR sealer[tiab])))) OR electrosurgical[tiab] OR electrocoagulation[tiab] OR electrocoagulation[MeSH]
16,742
#3 Publication years of interest "2007/01/01"[PDat]:"2018/12/31"[PDat] 9,418,446
#4 Invalid publication types "Case Reports" [ptyp] OR "Clinical Conference" [ptyp] OR "Comment" [ptyp] OR "Editorial" [ptyp] OR "Letter"[ptyp] OR "Retracted Publication"[ptyp] OR "Congresses"[ptyp] OR "Duplicate Publication"[ptyp]
3,240,780
#5 Non-clinical data "ex vivo"[tiab] OR cadaver[tiab] OR "deceased donor"[tiab] 78,271 #6 Animal data Search terms for animal studies19 6,291,401
#7
LigaSureTM (by name or generic), restricted to publication years, excluding animal, non-clinical, and non-primary data
(#1 OR #2) AND #3 NOT (#4 OR #5 OR #6) 3,656
#8 All colorectal procedures
colectomy[tiab] OR sigmoidectomy[tiab] OR hemicolectomy[tiab] OR “colon resection”[tiab] OR “bowel resection”[tiab] OR colectomy[MeSH] OR ((colon[tiab] OR colorectal[tiab]) AND (polyp[tiab] OR polyps[tiab] OR polypectomy[tiab])) OR hemorrhoidectomy[tiab] OR haemorrhoidectomy[tiab] OR Hemorrhoids[MeSH] OR hemorrhoidectomy[MeSH] OR
120,805

Global Value Dossier: LigaSureTM Technology 34
colostomy[MeSH] OR “Colorectal Surgery”[MeSH] OR “colorectal cancer”[tiab]
#9 LigaSureTM + colorectal #7 AND #8 164
The original searches designed above revealed few relevant comparative studies reporting on LigaSureTM device usage in colectomy, although broader searches indicated wider use of the technology. For colectomy surgeries only, then, the above searches were supplemented with hand searches, manual screening of article contents (to confirm usage of a LigaSureTM device when not otherwise mentioned in the abstract) and the inclusion of publications after 2007, which may also have referenced pre-2007 data.
The second search, to reveal all clinical instances of LigaSureTM device use, including incidental mentions of use of the technology even if not the focus of the study, was performed using EMBASE. This database includes coverage of non-PubMed-indexed journals and congress reports to thus provide a comprehensive survey of LigaSureTM technology use (Table 7-2). A differential search was performed May 2017 to retrieve new records from 2017 and updated or added from 2016, yielding 166 publications to screen for additional settings where LigaSureTM technology has been used.
Table 7-2 Structured search in EMBASE to identify use of LigaSureTM devices
Index Aim Search string Hits
1 LigaSureTM-specific technology (referenced by name) excluding ex vivo data and select animals
((ligasure or ligasurev or ligasuretm) not (preclinical or "ex vivo" or cadaver or animal or dog or cat or pig or veterinary or veterinarian)).mp.
1,390
Results from the various searches were exported from their respective databases as search strings (PubMed) and .RIS files (EMBASE) for integration into the Sourcerer software utility for literature screening and review. Duplicate articles returned from the different sources were automatically removed.
7.2.Screening literature results
7.2.1. Screening general search (EMBASE) results
The purpose of the EMBASE search as described (Section 7.1) was to capture as many references (by name) of LigaSureTM device use in both peer-reviewed and non-peer-reviewed literature. As such, the results were not screened for exclusion criteria, but for surgery type and geographical location to verify clinical application of the technology.

Global Value Dossier: LigaSureTM Technology 35
7.2.2. Screening returned results for evidence (PubMed)
The articles returned from the PubMed searches were subjected to screening to identify articles relevant to the targeted indication (colorectal surgery) for further deeper analysis. The criteria, and rationale are presented in Table 7-3.
Table 7-3 Description of exclusion criteria
Criterion Explanation
Data pre-2007 Although the article was published after 2007 according to the search terms, the data referenced within cover a range prior to 2007. This criterion was only applied for the hemorrhoidectomy search.
Articles with no abstract At the level of top level screening, no informed decision regarding evidence or quality can be made without an abstract
Editorial/commentary Articles that are commentaries or letters responding to other articles are not included for evidence recovery
Non-clinical Articles which do not present any relevant clinical data, including patient surveys and experimental/ex vivo studies which were captured
Fewer than 20 patients For higher quality evidence, studies of fewer than 20 patients are excluded
Non-targeted surgery For a given surgical search area, if the focus of surgery of the article is for a different kind of procedure, the study is excluded. Examples include the capture of an author listing example surgeries where LigaSureTM technology has been used in the abstract, while the main study is not the current target.
Not vessel-sealing focused
The mention of LigaSureTM or related technology is incidental and not the focus of the study with no data relevant to the performance of the technology
Not LigaSureTM technology
The reference by generic name to the technology cannot be conclusively identified as LigaSureTM at abstract level, or the reference to generic terms in the search such as electrocautery catches technology not relevant to bipolar vessel sealing

Global Value Dossier: LigaSureTM Technology 36
8. Data references 1 Adamina M, Champagne BJ, Hoffman L, Ermlich MB, et al. Randomized clinical trial comparing
the cost and effectiveness of bipolar vessel sealers versus clips and vascular staplers for laparoscopic colorectal resection. Br J Surg. 2011;98(12):1703-12. doi:10.1002/bjs.7679. PMID:21997317
2 Nakajima K, Nezu R, Ito T, Nishida T. Hand-assisted laparoscopic restorative proctocolectomy for ulcerative colitis: the optimization of instrumentation toward standardization. Surg Today. 2010;40(9):840-4. doi:10.1007/s00595-009-4157-8. PMID:20740347
3 Takiguchi N, Nagata M, Soda H, Nomura Y, et al. Multicenter randomized comparison of LigaSure versus conventional surgery for gastrointestinal carcinoma. Surg Today. 2010;40(11):1050-4. doi:10.1007/s00595-009-4234-z. PMID:21046504
4 Trilling B, Riboud R, Abba J, Girard E, et al. Energy vessel sealing systems versus mechanical ligature of the inferior mesenteric artery in laparoscopic sigmoidectomy. Int J Colorectal Dis. 2016;31(4):903-8. doi:10.1007/s00384-016-2508-7. PMID:26841803
5 Hubner M, Demartines N, Muller S, Dindo D, et al. Prospective randomized study of monopolar scissors, bipolar vessel sealer and ultrasonic shears in laparoscopic colorectal surgery. Br J Surg. 2008;95(9):1098-104. doi:10.1002/bjs.6321. PMID:18690630
6 Tou S, Malik AI, Wexner SD, Nelson RL. Energy source instruments for laparoscopic colectomy. Cochrane Database Syst Rev. 2011; 10.1002/14651858.CD007886.pub2(5):CD007886. doi:10.1002/14651858.CD007886.pub2. PMID:21563161
7 Campagnacci R, de Sanctis A, Baldarelli M, Rimini M, et al. Electrothermal bipolar vessel sealing device vs. ultrasonic coagulating shears in laparoscopic colectomies: a comparative study. Surg Endosc. 2007;21(9):1526-31. doi:10.1007/s00464-006-9143-2. PMID:17287913
8 Guerrieri M, Sanctis A, Baldarelli M, Nisi M, et al. Electrothermal bipolar energy-based device in laparoscopic right colectomy: our experience. Minerva Chir. 2008;63(6):455-60. PMID:19078877
9 Rimonda R, Arezzo A, Garrone C, Allaix ME, et al. Electrothermal bipolar vessel sealing system vs. harmonic scalpel in colorectal laparoscopic surgery: a prospective, randomized study. Dis Colon Rectum. 2009;52(4):657-61. doi:10.1007/DCR.0b013e3181a0a70a. PMID:19404071
10 Wilson MZ, Hollenbeak CS, Stewart DB. Laparoscopic colectomy is associated with a lower incidence of postoperative complications than open colectomy: a propensity score-matched cohort analysis. Colorectal Dis. 2014;16(5):382-9. doi:10.1111/codi.12537. PMID:24373345
11 Toh JW, Stewart P, Rickard MJ, Leong R, et al. Indications and surgical options for small bowel, large bowel and perianal Crohn's disease. World J Gastroenterol. 2016;22(40):8892-8904. doi:10.3748/wjg.v22.i40.8892. PMID:27833380
12 Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205-13. PMID:15273542
13 Di Lorenzo N, Franceschilli L, Allaix ME, Asimakopoulos AD, et al. Radiofrequency versus ultrasonic energy in laparoscopic colorectal surgery: a metaanalysis of operative time and blood loss. Surg Endosc. 2012;26(10):2917-24. doi:10.1007/s00464-012-2285-5. PMID:22580873
14 Macario A. What does one minute of operating room time cost? J Clin Anesth. 2010;22(4):233-6. doi:10.1016/j.jclinane.2010.02.003. PMID:20522350

Global Value Dossier: LigaSureTM Technology 37
15 Macario A, Dexter F, Sypal J, Cosgriff N, et al. Operative time and other outcomes of the electrothermal bipolar vessel sealing system (LigaSureTM) versus other methods for surgical hemostasis: A meta-analysis. Surgical Innovation. 2008;15(4):284-291. PMID:18945705
16 Liu JB, Berian JR, Chen S, Cohen ME, et al. Postoperative Complications and Hospital Payment: Implications for Achieving Value. J Am Coll Surg. 2017; 10.1016/j.jamcollsurg.2017.01.041. doi:10.1016/j.jamcollsurg.2017.01.041. PMID:28137536
17 Martin ST, Heeney A, Pierce C, O'Connell PR, et al. Use of an electrothermal bipolar sealing device in ligation of major mesenteric vessels during laparoscopic colorectal resection. Tech Coloproctol. 2011;15(3):285-9. doi:10.1007/s10151-011-0707-3. PMID:21761166
18 Hubner M, Hahnloser D, Hetzer F, Muller MK, et al. A prospective randomized comparison of two instruments for dissection and vessel sealing in laparoscopic colorectal surgery. Surg Endosc. 2007;21(4):592-4. doi:10.1007/s00464-006-9034-6. PMID:17279307
19 Hooijmans CR, Tillema A, Leenaars M, Ritskes-Hoitinga M. Enhancing search efficiency by means of a search filter for finding all studies on animal experimentation in PubMed. Lab Anim. 2010;44(3):170-5. doi:10.1258/la.2010.009117. PMID:20551243

Global Value Dossier: LigaSureTM Technology 38
9. Geographical references
G1. Rieger, N. A. & Lam, F. F. Single-incision laparoscopically assisted colectomy using standard laparoscopic instrumentation. Surg. Endosc. Other Interv. Tech. 24, 888–890 (2010). (PMID: 19760335)
G2. Brunner, W. et al. Single-access laparoscopic sigmoid resections. Surg. Endosc. Other Interv. Tech. 25, S28–S28 (2011).
G3. Kim, D. Y. & Boushey, R. P. The Use of Alternative Energy Sources and New Techniques for the Treatment of Hemorrhoidal Disease. Semin. Colon Rectal Surg. 18, 181–186 (2007).
G4. Zhang, H. et al. Transanal single-port laparoscopic total mesorectal excision in the treatment of rectal cancer. Tech. Coloproctol. 17, 117–23 (2013). (PMID: 22936590)
G5. Arslani, N., Patrlj, L., Rajkovic, Z., Papes, D. & Altarac, S. A randomized clinical trial comparing Ligasure versus stapled hemorrhoidectomy. Surg. Laparosc. Endosc. Percutan. Tech. 22, 58–61 (2012). (PMID: 22318061)
G6. Talha, A., Bessa, S. & Abdel Wahab, M. Ligasure, Harmonic Scalpel versus conventional diathermy in excisional haemorrhoidectomy: a randomized controlled trial. ANZ J Surg (2014). doi:10.1111/ans.12838 (PMID: 25214362)
G7. Kössi, J., Luostarinen, M., Kontula, I. & Laato, M. Laparoscopic sigmoid and rectal resection using an electrothermal bipolar vessel sealing device. J Laparoendosc Adv Surg Tech A 17, 719–722 (2007). (PMID: 18158799)
G8. Trilling, B., Riboud, R., Abba, J., Girard, E. & Faucheron, J. L. Energy vessel sealing systems versus mechanical ligature of the inferior mesenteric artery in laparoscopic sigmoidectomy. Int. J. Colorectal Dis. 31, 903–908 (2016). (PMID: 26841803)
G9. Vestweber, B. et al. Single-incision laparoscopic surgery: Outcomes from 224 colonic resections performed at a single center using SILSTM. Surg. Endosc. Other Interv. Tech. 27, 434–442 (2013). (PMID: 22806519)
G10. Basdanis, G., Papadopoulos, V. N., Michalopoulos, A., Apostolidis, S. & Harlaftis, N. Randomized clinical trial of stapled hemorrhoidectomy vs open with Ligasure for prolapsed piles. Surg. Endosc. Other Interv. Tech. 19, 235–239 (2005). (PMID: 15573239)
G11. Fok, K. L., Cheung, M. H. Y., Poon, C. M. & Lee, K. W. LigaSure-assisted versus diathermy day case haemorroidectomy: A randomized controlled trial. Ambul. Surg. 14, no pagination-no pagination (2008).
G12. Khanna, R., Khanna, S., Bhadani, S., Singh, S. & Khanna, A. K. Comparison of Ligasure Hemorrhoidectomy with Conventional Ferguson’s Hemorrhoidectomy. Indian J Surg 72, 294–297 (2010). (PMID: 21938191)
G13. Bouini, N. R. et al. Randomised Clinical Trial Comparing Ligasure Hemorrhoidectomy with Conventional Hemorrhoidectomy. J. Maz. Univ. Med. Sci. 22, 67–73 (2012).
G14. Baig, M. N., Moftah, M., Deasy, J., Mcnamara, D. A. & Cahill, R. A. Implementation and usefulness of single-access laparoscopic segmental and total colectomy. Color. Dis. 14, 1267–1275 (2012). (PMID: 22309248)
G15. Swaid, F. et al. Totally laparoscopic versus laparoscopic-assisted left colectomy for cancer: a retrospective review. Surg. Endosc. Other Interv. Tech. 30, 2481–2488 (2016). (PMID: 26335075)
G16. Franceschilli, L. et al. Radiofrequency versus conventional diathermy Milligan-Morgan hemorrhoidectomy: A prospective, randomized study. Int. J. Colorectal Dis. 26, 1345–1350 (2011). (PMID: 21519801)
G17. Tsunoda, A. et al. Randomized controlled trial of bipolar diathermy vs ultrasonic scalpel for closed hemorrhoidectomy. World J Gastrointest Surg 3, 147–152 (2011). (PMID: 22110846)
G18. Sakr, M. F. & Moussa, M. M. LigaSure hemorrhoidectomy versus stapled hemorrhoidopexy: A prospective, randomized clinical trial. Dis. Colon Rectum 53, 1161–1167 (2010). (PMID: 20628280)
G19. Peralta, G. et al. Massive gastrointestinal bleeding: A rare case of extrarenal, visceral, rectal fibromuscular displasia. Surg. Endosc. Other Interv. Tech. 28, 323 (2014).
G20. Nieuwenhuis, D. H., Draaisma, W. A., Verberne, G. H. M., Van Overbeeke, A. J. & Consten, E. C. J. Transanal endoscopic operation for rectal lesions using two-dimensional visualization and standard endoscopic instruments: A prospective cohort study and comparison with the literature. Surg. Endosc. Other Interv. Tech. 23, 80–86 (2009). (PMID: 18443874)

Global Value Dossier: LigaSureTM Technology 39
G21. Bakhtiar, N., Moosa, F. A., Jaleel, F., Qureshi, N. A. & Jawaid, M. Comparison of Hemorrhoidectomy by ligasure with conventional milligan morgan’s Hemorrhoidectomy. Pakistan J. Med. Sci. 32, 657–661 (2016). (PMID: 27375709)
G22. Szyca, R., Dratwa, S., Tomaszewski, S. & Leksowski, K. Closed hemorrhoidectomy with LigaSure - A prospective study. Pol. Przegl. Chir. 78, 1415–1420 (2006).
G23. Martian, B. V et al. Wise steps in laparoscopic right hemicolectomy: Standardization of the technique in curent use. Surg. Endosc. Other Interv. Tech. 30, S33–S33 (2016).
G24. Tulina, I. A., Tsarkov, P. V & Kravchenko, Ay. Laparoscopic ‘no touch’ intersphincteric rectal resection: Three step technique. Surg. Endosc. Other Interv. Tech. 28, S175–S175 (2014).
G25. Zubaidi, A., AlDeghaither, S., Alkhayal, K. & Al-Obeed, O. Single-incision laparoscopic colorectal surgery: A report of 33 cases in Saudi Arabia. Ann. Saudi Med. 36, 282–287 (2016). (PMID: 27478914)
G26. Kecmanovic, D. M. et al. Bulk agent Plantago ovata after Milligan-Morgan hemorrhoidectomy with LigasureTM. Phyther. Res. 20, 655–658 (2006). (PMID: 16708408)
G27. Tan, K. Y. et al. Randomized clinical trial comparing LigaSure haemorrhoidectomy with open diathermy haemorrhoidectomy. Tech. Coloproctol. 12, 93–97 (2008). (PMID: 18545884)
G28. Yun, J. A. et al. Single-incision laparoscopic right colectomy compared with conventional laparoscopy for malignancy: Assessment of perioperative and short-term oncologic outcomes. Surg. Endosc. Other Interv. Tech. 27, 2122–2130 (2013). (PMID: 23319285)
G29. Castellví, J. et al. LigasureTM versus diathermy hemorrhoidectomy under spinal anesthesia or pudendal block with ropivacaine: A randomized prospective clinical study with 1-year follow-up. Int. J. Colorectal Dis. 24, 1011–1018 (2009). (PMID: 19396451)
G30. Hubner, M. et al. Prospective randomized study of monopolar scissors, bipolar vessel sealer and ultrasonic shears in laparoscopic colorectal surgery. Br. J. Surg. 95, 1098–1104 (2008). (PMID: 18690630)
G31. Chen, C. W., Lai, C. W., Chang, Y. J. & Hsiao, K. H. Modified LigaSure hemorrhoidectomy for the treatment of hemorrhoidal crisis. Surg. Today 44, 1056–1062 (2014). (PMID: 23812901)
G32. Pattana-arun, J., Sooriprasoet, N., Sahakijrungruang, C., Tantiphlachiva, K. & Rojanasakul, A. Closed vs ligasure hemorrhoidectomy: A prospective, randomized clinical trial. J. Med. Assoc. Thail. 89, 453–458 (2006). (PMID: 16696389)
G33. Teksöz, S. et al. Comparison of a vessel sealing system with a conventional technique in hemorrhoidectomy. Balkan Med. J. 28, 189–192 (2011).
G34. Vadamalayan, B. et al. Laparoscopic colectomy for ulcerative colitis with associated auto-immune liver disease and portal hypertension. J. Pediatr. Gastroenterol. Nutr. 62, 329 (2016).
G35. Adamina, M., Champagne, B. J., Hoffman, L., Ermlich, M. B. & Delaney, C. P. Randomized clinical trial comparing the cost and effectiveness of bipolar vessel sealers versus clips and vascular staplers for laparoscopic colorectal resection. Br J Surg 98, 1703–1712 (2011). (PMID: 21997317)
©2017 Medtronic. All rights reserved. Medtronic, Medtronic logo, and Further, Together are trademarks of Medtronic. TM* Third party brands are trademarks of their respective owners. All other brands are trademarks of a Medtronic company. US171094