Embed Size (px)
Citation preview

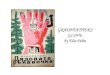
Study Name: “Glove: Use for safety or over-use?”*
HISTORY HAND HYGIENE & GLOVE USE: THE FUTURE
Today, the aim of glove use is for the protection of both the care provider and the patient.
Occupational exposure to blood and body fluids presents a major safety risk for bloodborne viruses to all health care workers (HCW).
The elimination of routine glove use from contact precautions
would reduce wastage and improve cost savings without a concomitant increase in infections.
A modified glove use approach with a cultural shift would improve
the safety of patient-centred care.
Refresh WHO 5 Moments with explicit reminders to change gloves between Moments.
RECOMMENDATION:
Requirements:Compliance with WHO 5 Moments including before donning PPE and after removing PPERemoval of all PPE on exiting room/ward followed by immediate hand hygiene
Identification of:Non-sterile glove boxes have been reported to be contaminated with bacteria HCWs to evaluate risk of exposure to blood and body fluids before donning glovesIncreased hand hygiene by eliminating gloves for ‘dry’ contacts with patient under contact precautions to reduce cross-contamination by gloved hands.
Contaminated gloves should be changed during an episode of care that had the HCW’s hands been ungloved would have involved several hand hygiene events.
HCWs have become accustomed to feeling safe with gloves, and this feeling may have averted their need for hand hygiene.
Feedback of hand hygiene is complicated by falsely enhanced compliance rates produced by the Hawthorne Effect.
HCWs find integrating changes of gloves into the principles of the 5 Moments notoriously difficult.
•
•
•
•
•
1758
1899
Gloves were made from sheep caecum in an attempt to protect the surgeon’s hands during surgery, vaginal examination, and autopsies.
Glove use moved out of the operating theatre onto the ward. Gloves on the ward were used in conjunction with handwashing after every patient but only for “grossly contaminated hands with pathogens”.
The American Hospital Association published the first hospital infection
control manual. This recommendation suggested that the target of the
equipment was the safety of the HCWs.
The consequence of multiple changes to guidelines raised
concerns about poor compliance with hand hygiene
associated with glove use.
Gloves specified for anticipated contact with blood and specified body fluids, and hands were to be washed immediately after glove removal An over-reliance on glove use produced an increased risk of the transmission of pathogens.
•
•
The Lancet supported the use of thin, sterile, rubber gloves for possible exposures to body fluids.
The disposable glove emerged.
The pre-packaging of gloves transformed gloves into an essential accessible protective item.
William Halsted, a surgeon, advocated gloves for the protection of patients from surgical
infections during hernia operations.
1957
1958
1960
1966
1968
1980s
1990
2018
High hand hygiene compliance is accepted as the most cost-effective infection prevention activity.
With the current emphasis on gloves as a protective barrier, hand hygiene compliance remains low.
There remains an overreliance on gloves in absence of integrating hand hygiene in to the WHO 5 Moments.
The role of HCWs’ hands in the transmission of pathogens to patients is undisputed.
AFTER BODYDDFLU
ID
EXPOSURE RISK3 AFTER CONTACT
WITH PATIENT SURROUNDINGS5
2BEFORE A
PROCEDURECLEAN / ASEPTIC
AFTERPATIENT CONTACT4
BEFOREPATIENTCONTACT1
Gloves are part of personal protective equipment (PPE)
for all potential or expected exposures to blood and body fluid.
*Jain S, Clezy K, McLaws ML. | https://doi.org/10.1016/j.ajic.2017.08.029
AFTER CONTACTWITH PATIENT SURROUNDINGS5
AFTERPATIENT CONTACT4
2BEFORE A
PROCEDURECLEAN / ASEPTIC
BEFOREPATIENTCONTACT1
AFTER BODYDDFLU
ID
EXPOSURE RISK3
GLOVES: USED FOR SAFETY OR OVER-USED?




![3D Interactions with a Passive Deformable Haptic Glove · worlds with an ultrasonic glove [1], see Figure 2. This paper explores the use of a passive deformable haptic (PDH) glove,](https://img.pdfslide.net/doc/110x75/5fbfdc889fdae73ffa6b5a7f/3d-interactions-with-a-passive-deformable-haptic-glove-worlds-with-an-ultrasonic.jpg)





















![Cyborg Glove ExcerptNick and Tesla’s Super Cyborg Gadget Glove [Excerpt]](https://img.pdfslide.net/doc/110x75/577cc47a1a28aba711996e65/cyborg-glove-excerptnick-and-teslas-super-cyborg-gadget-glove-excerpt.jpg)

