Embed Size (px)
Citation preview
INDIAN JOURNAL OF PEDIATRICS
Vol. 37 May, 1970 No. 268
ORIGINAL ARTICLES
GLUCOSE-6-PHOSPHATE DEHYDROGENASE DEFICIENCY IN THE NEWBORN AND ITS RELATION TO SERUM BILIRUBIN*
SUSHMA GUPTA, O. P. GHAi and R. K. CttANDRA
New Delhi
A deficiency of the enzyme glucose- 6-phosphate dehydrogenase is one of the most widely distributed metabolic errors of erythrocytes. Its incidence and clinical presentation varies consi- derably among different ethnic groups (Dacie 1967). It may express itself as drug-induced hemolytic anemia, infec- tion-induced hemolytic an;mia, chronic non-spherocytic hemolytic anemia, favism, or it may be asymptomatic (Beutler 1967). Among certain ethnic groups glucose-6-phosphate dehydro- genase (G-6-PD) deficiency is known to be associated with significant neonatal hyperbilirubinemia, some times even leading to kernicterus (Dacie 1967). This fact, however, is not remarkable
* From the Department of Pediatrics, All India Institute of Medical Sciences, New Delhi-16.
Correspondence and reprint requests : Dr. R K. Chandra, Assistant Professor of Pediatrics, All India Institute of Medical Sciences, New ~lhi-I 6,
among Negroes and Iraqi Jews (Zinkham 1963, Szeinberg et al. 1963). An attempt was made in this study to estimate the incidence of G-6-PD deficiency in this part of the country and to study its relationship with serum bilirubin level in the neonatal period.
Materials and Methods
Five hundred newborn infants born at the All India Institute of Medical Sciences Hospital, New Delhi (all consecutive deliveries except on holidays) and the Victoria Zenana Hospital, Delhi (all deliveries on one day in a week), were studied. No selection of the cases was made. A detailed information of the racial and ethnic background of both parents of each infant was sought. In addition to the period of gestation and birth weight, any complication during the antenatal, perinatal or post-natal
170 INDIAN JOURNAL OF PEDIATRICS VOL. 37 NO. 268
period was carefully recorded. A history of neonatal jaundice following drugs or infections among the family members and relations were carefully noted. A detailed clinical examina- tion of the infants was done to detect jaundice, any overt congenital malfor- mation or infection. Cases of neonatal jaundice due to a known cause such as Rh ol ABO incompati- bility or septicemia were not included in the study.
All the five hundred newborns were examined for G-6.PD deficiency by the spot test of Fairbanks and Beutler (1962) on the 1st or the 2nd day of life. Serum bilirubin was estimated in all deficient infants on the 2nd, 4th and 6th day after birth. Serum bilirubin (total and differential) was also estimated on the 2rid, 4th and 6th day of birth in 100 newborns picked at random from among the 500 surveyed. The affected infants, their family members and 50 normal
infants (normal by the spot test) selected at random from among the 500 newborns were a!so examined by the methylene blue test of Oski and Growney (1965), Serum bilirubin was determined by Michaelssons' modifi- cation of the Jendrassik Groff Noslin method (1961).
Observations
The study material comprised 500 newborn babies, of whom 238 were boys. The deficiency trait was detec- ted in five infants; all were males.
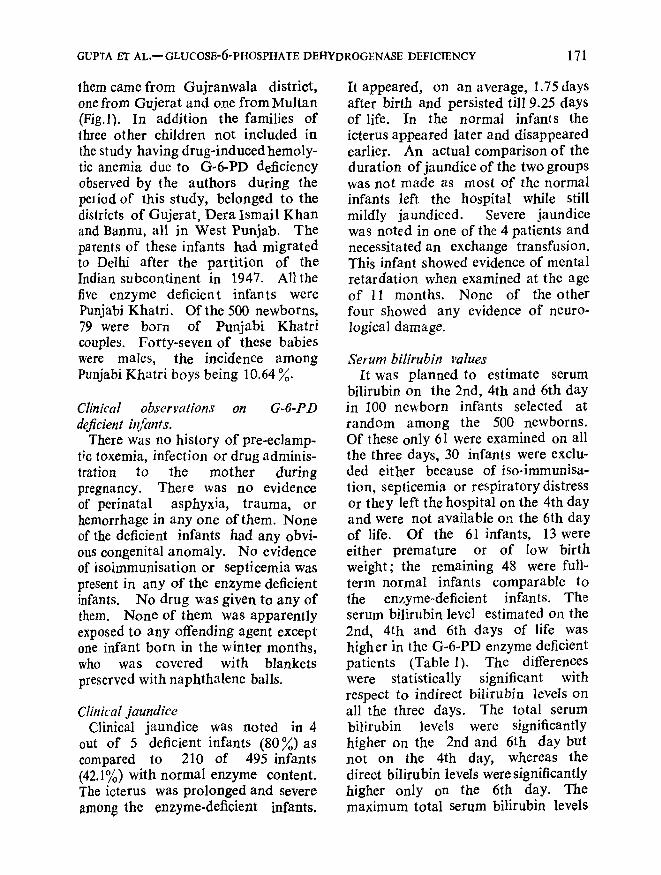
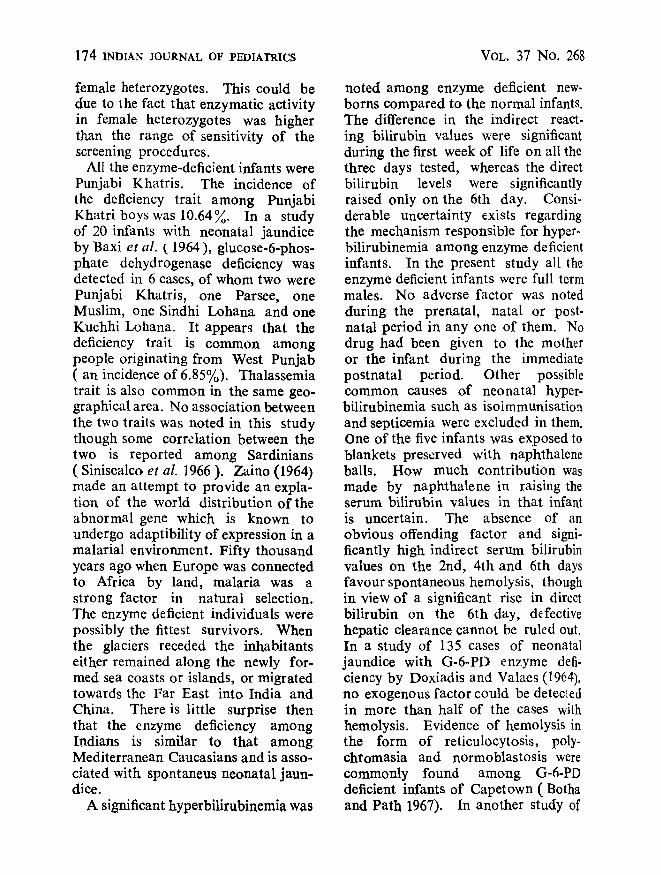
Ethnic background. The ethnic background of the 500 newborns studied was: West Punjabis 172 (73 boys), natives of Delhi 121 (57 boys), East Punjabis 82 (48 boys), from Uttar Pradesh 91 (42 boys) and others 34 (18 boys). The families of all the five enzyme deficient infants originated flom West Punjab (northern part of West Pakistan). Three of
WEST PAKISTAN
B - - G U J R A T ( 2 )
ANNU G U J R A N W A L A ( 3 )
DERA ISMAIL KHAN./, . ~ - ~ - e /
N(1)
Fig. 1. Places of or ig in of the enzyme deficient infants.
GUPTA El" AL.-- GLUCOSE-6-PHOSPHATE DEHYDROGENASE DEFICIENCY 171
them came from Gujranwala district, one from Gujerat and one from Multan (Fig.l). In addition the families of three other children not included in the study having drug-induced hemoly- tic anemia due to G-6-PD deficiency observed by the authors during the peliod of this study, belonged to the districts of Gujerat, Dera Ismail Khan and Bannu, all in West Punjab. The parents of these infants had migrated to Delhi after the partition of the Indian subcontinent in 1947. Allthe five enzyme deficient infants were Punjabi Khatri. Of the 500 newborns, 79 were born of Punjabi Khatri couples. Forty-seven of these babies were males, the incidence among Punjabi Khatri boys being 10.64 ~o.
Clinical observations on G-6-PD deficient i~Cants.
There was no history of pre-eclamp- t;c toxemia, infection or drug adminis- tration to the mother during pregnancy. There was no evidence of perinatal asphyxia, trauma, or hemorrhage in any one of them. None of the deficient infants had any obvi- ous congenital anomaly. No evidence of isoimmunisation or septicemia was present in any of the enzyme deficient infants. No drug was given to any of them. None of them was apparently exposed to any offending agent except one infant born in the winter months, who was covered with blankets preserved with naphthalene balls.
Cliuical jaundice Clinical jaundice was noted in 4
out of 5 deficient infants (80~o)as compared to 210 of 495 infants (42.1~o) with normal enzyme content. The icterus was prolonged and severe among the enzyme-deficient infants.
It appeared, on an average, 1.75 days after birth and persisted till 9.25 days of life. In the normal infants the icterus appeared later and disappeared earlier. An actual comparison of the duration of jaundice of the two groups was not made as most of the normal infants left the hospital while still mildly jaundiced. Severe jaundice was noted in one of the 4 patients and necessitated an exchange transfusion. This infant showed evidence of mental retardation when examined at the age of 11 months. None of the other four showed any evidence of neuro- logical damage.
Serum bilirubin values It was planned to estimate serum
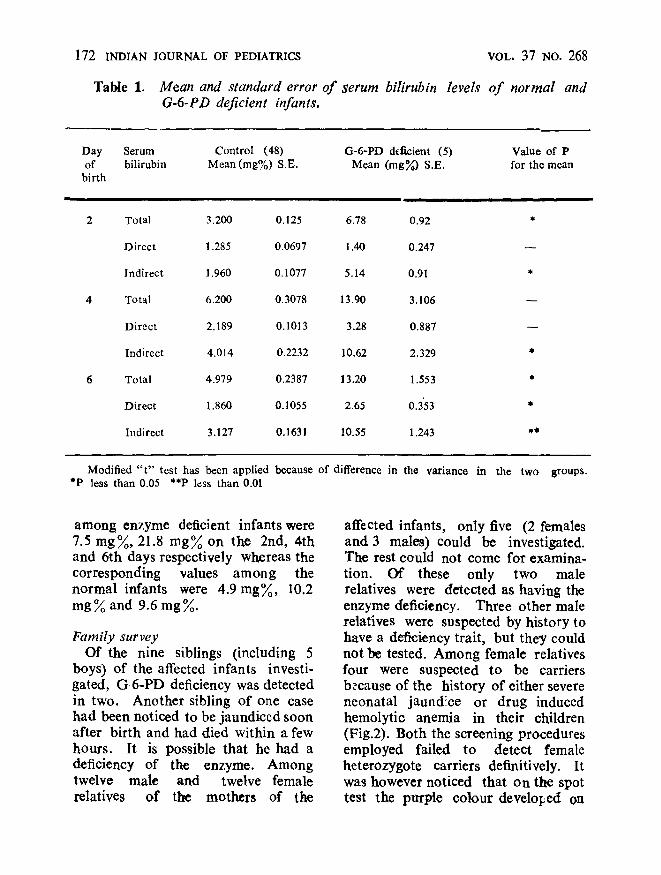
bilirubin on the 2nd, 4th and 6th day in 100 newborn infants selected at random among the 500 newborns. Of these only 61 were examined on all the three days, 30 infants were exclu- ded either because of iso-immunisa- lion, septicemia or respiratory distress or they left the hospital on the 4th day and were not available on the 6th day of life. Of the 61 infants, 13 were either premature or of low birth weight; the remaining 48 were full- term normal infants comparable to the enzyme-deficient infants. The serum bilirubin level estimated on the 2nd, 4th and 6th days of life was higher in the G-6-PD enzyme deficient patients (Table 1). The differences were statistically significant with respect to indirect bilirubin levels on all the three days. The total serum bilirubin levels were significantly higher on the 2nd and 6th day but not on the 4th day, whereas the direct bilirubin levels were significantly higher only on the 6th day. The maximum total serum bilirubin levels
172 INDIAN JOURNAL OF PEDIATRICS
Table 1. Mean and standard error of serum bilirubin G-6-PD deficient infants.
VOL. 37 NO. 268
levels o f normal and
Day Serum Control (48) G-6-PD deficient (5) of bilirubin Mean(rag%) S.E. Mean ( m g ~ ) S.E.
birth
Value of P for the mean
2 Total 3.200 0.125 6.78 0.92 *
Direct 1.285 0.0697 1.40 0.247 - -
Indirect 1.960 0.1077 5.14 0.91 *
4 Total 6.200 0.3078 13.90 3.106 - -
Direct 2.189 0.1013 3.28 0.887 - -
Indirect 4.014 0.2232 10.62 2.329 *
6 Total 4.979 0.2387 13.20 1.553 *
Direct 1.860 0.1055 2.65 0.353 *
Indirect 3.127 0.1631 10.55 1.243 **
Modified " t " test has been applied because of difference in the variance in the two groups. *P less than 0.05 **P less than 0.01
among enzyme deficient infants were 7.5 mg~o, 21.8 rag% on the 2nd, 4th and 6th days respectively whereas the corresponding values among the normal infants were 4.9mg%, 10.2 mg~o and 9.6 mg%.
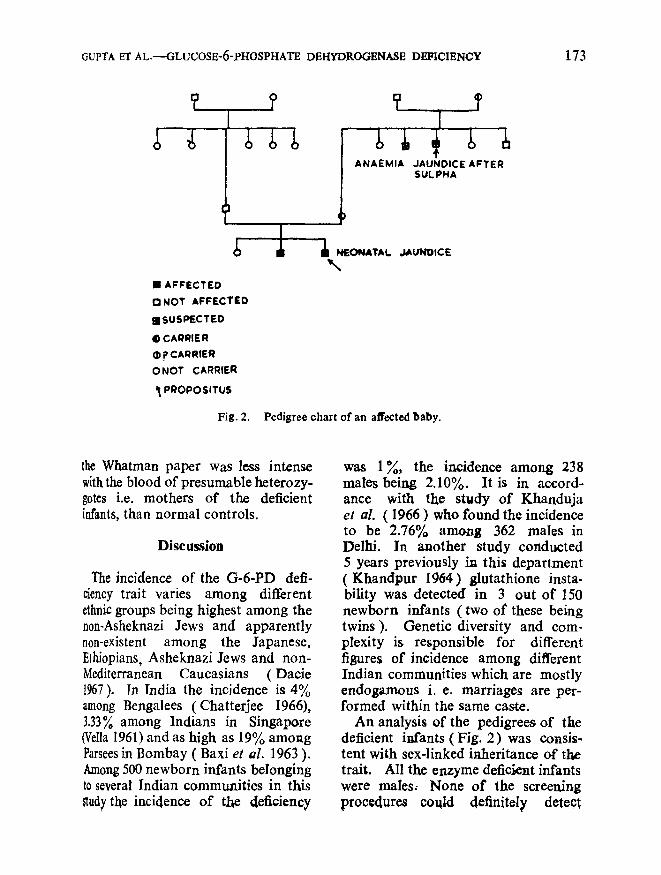
Family survey Of the nine siblings (including 5
boys) of the affected infants investi- gated, G 6-PD deficiency was detected in two. Another sibling of one case had been noticed to be jaundiced soon after birth and had died within a few hours. It is possible that he had a deficiency of the enzyme. Among twelve male and twelve female relatives of the mothers of the
affected infants, only five (2 females and 3 males)could be investigated. The rest could not come for examina- tion. Of these only two male relatives were detected as having the enzyme deficiency. Three other male relatives were suspected by history to have a deficiency trait, but the5' could not be tested. Among female relatives four were suspected to be carriers because of the history of either severe neonatal jaund!ce or drug induced hemolytic anemia in their children (Fig.2). Both the screening procedures employed failed to detect female heterozygote carriers definitively. It was however noticed that on the spot test the purple colour developed on
GUPTA ET AL.----GLUCOSE-6-PHOSPHATE DEHYDROGENASE DEFICIENCY 173
�9 AFFECTED Q NOT AFFECTED
aSUSPECTED
O CARRIER (~ ? CAR RIER ONOT CARRIER
PROPOSITUS
Fig. 2.
_
ANAEMIA JAUNDICE AFTER SULPNA
dl NEONATAL JAUNDICE \
Pedigree chart of an affected baby.
the Whatman paper was less intense with the blood of presumable heterozy- gotes i.e. mothers of the deficient infants, than normal controls.
Discussion
The incidence of the G-6-PD deft- eiency trait varies among different ethnic groups being highest among the n0n-Asheknazi Jews and apparently non-existent among the Japanese, Ethiopians, Asheknazi Jews and non- Mediterranean Caucasians ( Dacie t967). In India the incidence is 4% among Bengalees ( Chatterjee I966), 3.33% among Indians in Singapore (VeUa 1961) and as high as I9% among Parsecs in Bombay ( Baxi et al. 1963 ). Among 500 newborn infants belonging to several Indian communities in this sludy the incidence of the deficiency
was 1~,, the incidence among 238 males being 2.10%. It is in accord- ance with the study of Khanduja et al. ( 1966 ) who found the incidence to be 2.76% among 362 maIes in Delhi. In another study conducted 5 years previously in this department (Khandpur 1964) glutathione insta- bility was detected in 3 out of 150 newborn infants ( two of these being twins ). Genetic diversity and com- plexity is responsible for different figures of incidence among different Indian communities which are mostly endogamous i. e. marriages are per- formed within the same caste.
An analysis of the pedigrees of the deficient infants ( Fig. 2) was consis- tent with sex-linked inheritance of the trait. All the enzyme deficient infants were males: None of the screening procedures could definitely, detect
174 1NDIAN JOURNAL OF PEDIATRICS VOL. 37 NO. 268
female heterozygotes. This could be due to the fact that enzymatic activity in female heterozygotes was higher than the range of sensitivity of the screening procedures.
All the enzyme-deficient infants were Punjabi Khatris. The incidence of the deficiency trait among Punjabi Khatri boys was 10.64~o. In a study of 20 infants with neonatal jaundice by Baxi et al. (1964), glucose-6-phos- phate dehydrogenase deficiency was detected in 6 cases, of whom two were Punjabi Khatris, one Parsee, one Muslim, one Sindhi Lohana and one Kuchhi Lohana. It appears that the deficiency trait is common among people originating from West Punjab ( an incidence of 6.85%). Thalassemia trait is also common in the same geo- graphical area. No association between the two traits was noted in this study though some correlation between the two is reported among Sardinians ( Siniscalco et al. 1966 ). Zaino (1964) made an attempt to provide an expia- tion of the world distribution of the abnormal gene which is known to undergo adaptibility of expression in a malarial environment. Fifty thousand years ago when Europe was connected to Africa by land, malaria was a strong factor in natural selection. The enzyme deficient individuals were possibly the fittest survivors. When the glaciers receded the inhabitants either remained along the newly for- med sea coasts or islands, or migrated towards the Far East into India and China. There is little surprise then that the enzyme deficiency among Indians is similar to that among Mediterranean Caucasians and is asso- ciated with spontaneus neonatal jaun- dice.
A significant hyperbilirubinemia was
noted among enzyme deficient new- borns compared to the normal infants. The difference in the indirect react- ing bilirubin values were significant during the first week of life on all the three days tested, whereas the direct bilirubin levels were significantly raised only on the 6th day. Consi- derable uncertainty exists regarding the mechanism responsible for hyper- bilirubinemia among enzyme deficient infants. In the present study all the enzyme deficient infants were full term males. No adverse factor was noted during the prenatal, natal or post- natal period in any one of them. No drug had been given to the mother or the infant during the immediate postnatal period. Other possible common causes of neonatal hyper- bilirubinemia such as isoimmunisation and septicemia were excluded in them. One of the five infants was exposed to blankets preserved with naphthalene balls. How much contribution was made by naphthalene in raising the serum bilirubin values in that infant is uncertain. The absence of an obvious offending factor and signi- ficantly high indirect serum bilirubin values on the 2nd, 4th and 6th days favour spontaneous hemolysis, though in view of a significant rise in direct bilirubin on the 6th day, d~fective hepatic clearance cannot be ruled out. In a study of 135 cases of neonatal jaundice with G-6-PD enzyme defi- ciency by Doxiadis and Valaes (1964), no exogenous factor could be detecled in more than half of the cases with hemolysis. Evidence of hemolysis in the form of reticulocytosis, poly- chromasia and normoblastosis were commonly found among G-6-PD deficient infants of Capetown ( Botha and Path 1967). In another study of

GUPTA ET AL.--GLUCOSE-6-PHOSPHATE DEHYDROGENASE DEFICIENCY 175
Chinese enzyme deficient infants, significantly raised first day serum bi[irubin values wzre taken as an indication of increased hemolysis (Tsung et al. 1964). In a recent study in Singapore, Brown and Boon (1968) came to the conclusion that hyperbilirtlbinelni~t among enzyme deficient infants is influenced by phy- siological hyperbilirubinemia in that ethnic group. In an average normal infant, excessive hemolysis contributes little to the total bilirubinemia. f~yperbilirubinemia among enzyme deficient infants appears as a result of slightly excessive hemolysis over baseline bilirubin levels. Doxiadis et al. (1964) postulated a second genetic factor operating in certain families with the enzyme deficiency trait, which is further responsible for hyperbilirubinemia.
Levine et al. (1964} noted perinatal hypoxia in 5 of the 7 enzyme-deficient Bantu infants. In the present study none of the enzyme deficient infants were exposed to any obvious meta- bolic stres . Metabolic stresses such as cidosis, hypoxia and hypoglyce-
rnis can cause hyperbilirubinemia ar~ong enzyme deficient subjects by excessive hemolysis or decreased hepatic clearance or both. Generalised deficiency of the enzyme in various tissues including the liver ( among Caucasians ) could be another factor leading to defective hepatic metabo- lisr~ which is easily triggered off by r~in0r metabolic disturbances. Among r~etabolic stresses, asymptomatic hypoglycemia is a likely possibility though it is difficult to prove.
We aregrateftH to Dr. D.K. Guha, Pediatrician, Victoria Zcl~ana Ho:~pital. Delhi, for facilitating collectionof blood samples from his unit.
References
Baxi, A.J., Balakrishnan, V., Und~via, J.V. and Sanghvi, L.D. (1963). Glucose-6-phosphate dehydrogenase deficiency in Parsee community in Bombay. lndianJ, rued. Sc. 17,493.
Baxi, A.J., Undevia, J.V. and Bhatia, H.M. (1964). Role of glucose-6-phosphate dehydro- genase defi=iency in acute hemolytic crisis and neonatal jaundice. Ibid. 18, 574, Beutler, E.(1967). Glucose-6-phosphate dehy-
drogenase defi:iency-diagnosis clinical and genetic implications. Amer. J. Clin. Path. 47, 303. Botha, M.C. and Path, F.C. (1967). Glucose-6
phosphate-dehydrogenasr deficiency and neo- natal jaundice among population groups of Capotown. South Aft. reed. J. 41, 174. Brown, W.R. and Boon, W.H. (1968). Hyper-
bilirubinemia and kernicterus in glucose-6- phosphate-dehydrogenaso deficient infants in Singapore. Pediatrics, 41, ]055. Chatterjee, J.B. (1966). Hemogtobinopathies,
glucose-6-phosphate-dehydrogenase deficiency and allied problems in Indian subcontinent, Bull. W.H.O. 35, 837. Dacie, J,V. (1967). The Hemolytic Anemias-
Congenital and Acquired. Part IV, Drug induced haemolytic anemias, paroxysmal noc- turnal hemoglobinuria, hemolytic disease of the newborn, p. 1005. J.&A. Churchill, London. Doxiadis, S.A. and Valaes, T. (1961). The
clinical picture of G-6-PD defiziency in early infancy. Arch. Dis. Childh. 39, 545. Fairbanks, V.F. and Beutler, E. (1962). A
simplo method for detection of erythrocyte glucose-6-phosphate-dehydrogenase (G-6-PD- spot test). Blood, 20, 591.
Khandpur, S.C. (1964). Glutathione insta- bility of erythrocytes in the newbown infants. Thesis M.D. Pediatrics, A.I.1.M.S. New Delhi.
Khanduja, P.C., Aggarwat, K.IN., Julka, S., Bhargava, S.K. and Taneja, P.N. (1966). Incidence of glucose-6-phospha te-dehydro genase deficiency and some observations in patients with hemoglobinuria. Indian J. Pediat. 43, 341.
Levine, S.E., Chariton, R.W. and Frieman, I. )1964). Gtucose-6-phosphate-dchydrogenase deficiency and neonatal jaundice in South African Bantu infants. Z Pediat. 65, 757.
Michaelson, M. (1961). Bilirubin determina- tion in serum and urine, J. Clin. Lab. reed. 43, 56.
176 INDIAN JOURNAL OF PEDIATRI(~ VOL. 37 NO. 268
Oski, F.A. and Growrmy, P.M. (1965). A simple micromethod for detection of erythro- cyte G-6-PD deficiency. Y. Pediat. 66, 91.
Siniscalco, M,, Bernini, L., Filtipi, G., Latte, B., Meerkhan, P., Piomeili, S. and Rattazi, M. (1966). Population genetics of hemoglobin variants, thalassaemia and G-6-PD &ficiency with particular reference to malarial bypothesis. Bull. W.H.O. 34, 379.
Tsung, Cho Lu, Wei, H,, Blackwell, R.Q. (1964). Increased incidence of severe hyper-
bilirubinemia among Chinese infants with G-6- PD deficiency. Pediatrics, 37, 994. Vella, F. (1961). The incidence of erythroeyte
glucose-6-phosphate dehydrogenase deficiency in Singapore. Experlentia, 17, 181. Zaino, E.C. (1964). Paleontologic thalassenaia.
Ann. ~N.Y. Acad. Sc. 119, 402. Zinkham, W.H. (1963). Peripheral blood and
bilirubin values in normal full term primaquine sensitive Negro infants. Effect of Vitamin K. Pediatrics, 31,983.