Embed Size (px)
Citation preview

American Journal of Medical Genetics 32:395-401 (1989)
Glutaric Aciduria Type 11: Review of the Phenotype and Report of an Unusual Glomerulopathy
Golder N. Wilson, Jean-Pierre de Chadarevian, Paige Kaplan, James P. Loehr, Frank E. Frerman, and Stephen I. Goodman Department of Anatomical Pathology, Saint Christopher’s Hospital for Children, Department of Pediatrics, Temple University School of Medicine (J-P.deC.); and Department of Pediatrics, Uniuersity of Pennsylvania, Philadelphia (P.K.); Department of Pediatrics, University of Texas Southwestern Medical Center, Dallas, Texas (G. W.); and Department of Pediatrics, University of Colorado School of Medicine, Denver (J.P.L., F.E.F., S.I.G.).
A male infant with glutaric aciduria I1 second- ary to electron transfer flavoprotein: ubiqui- none oxidoreductase deficiency is compared to previously reported cases of glutaric aci- duria 11. A common pattern of anomalies in patients with malformations (8/16) includes macrocephaly, large anterior fontanelle, high forehead, flat nasal bridge, telecanthus, and malformed ears. Abnormalities such as hy- potonia, cerebral gliosis, heterotopias, hepa- tomegaly, hepatic periportal necrosis, poly- cystic kidneys, and genital defects in glutaric aciduria I1 are reminiscent of those in Zell- weger syndrome, whereas elevations of glu- taric, ethylmalonic, adipic, and isovaleric acids are quite distinctive. A unique ultra- structural alteration of the glomerular base- ment membrane was observed in the propos- ita. This manifestation may represent an early stage in renal cyst formation and pro- vide a diagnostic criterion for glutaric aci- duria I1 when enzyme studies are unavailable.
KEY WORDS: ethylmalonic-adipic aciduria, electron transfer flavopro- tein, Zellweger syndrome, metabolic dysplasia syn- drome, autosomal recessive inheritance
INTRODUCTION An interesting group of organellar metabolic disorders
with embryologic effects has been characterized [Datta et al., 1984; Hoganson et al., 19871. These prenatal “met-
Received for publication July 25, 1988; revision received Novem-
Address reprint requests to Golder N. Wilson, UT Southwestern ber 4, 1988.
Medical School, 5323 Harry Hines, Dallas, TX 75235. 01989 Alan R. Liss, Inc.
abolic dysplasia syndromes,” to use the term of Opitz [Friedman et al., 19801, provide biochemical access to human morphogenesis and to organellar biology. Glutaric aciduria (GA) type I1 is one of them and was first iden- tified in 1976 [Przyrembel et al.]. Subsequently, many patients were reported under this same heading. They had in common nonketotic hypoglycemia, acidosis, neu- rologic symptoms, and organic aciduria. Most of them presented neonatally with elevated urinary glutaric acid, ethylmalonic acid, isovaleric acid, and such dicarboxylic acids as adipic acid. Many severely affected patients have had concurrent congenital malformations [Bohm et al., 1982; Hoganson et al., 19871; other patients classified as GA I1 [Goodman et al., 1980; Dusheiko et al., 19791 or as ethylmalonic adipic aciduria [Mantagos et al., 19791 have had longer survival and no congenital anomalies.
Delineation of the specific enzymatic defects leading to GA I1 made it clear the condition is a phenotype produced by at least two mitochondrial disorders. Assays for mitochondrial electron transfer flavoprotein (ETF) and its dehydrogenase (electron transfer flavopro- tein:ubiquinone oxidoreductase, ETF:QO] have demon- strated that deficiency of either enzyme may lead to the multiple blocks in acyl CoA oxidation that occur in GA I1 [Goodman and Frerman, 19841. Congenital anomalies have been reported more frequently in association with ETF:QO deficiency [Frerman and Goodman, 19851, but a patient with polycystic kidneys and ETF deficiency has recently been encountered (Frerman and Goodman, un- published observations). We report on an infant with a GA I1 secondary to ETF:QO deficiency whose anomalies include a very unusual ultrastructural alteration of the glomerular basement membrane (GBM). Albeit observed for the first time, the GBM morphology is thought to be very distinctive and possibly characteristic of GA I1 sec- ondary to ETF:QO. It may also represent the basic defect leading to the development of renal cysts in this condi- tion.
CLINICAL REPORT An 11-day-old boy was transferred for intensive neo-
natal care because of respiratory distress. Birth weight was 2,706 g after uncomplicated vaginal delivery and 39-

396 Wilson et al.
week gestation to a 29-year-old gravida 2, para 1 mother. The mother had been maintained on a 2,000-calorie diet for gestational diabetes and had taken antinausea medi- cation during the first trimester. Family history indicated that the father had a twin with spina bifida and a sister who died in the first week of life with a congenital heart defect. Both parents were French Canadian with no known consanguinity.
Physical examination showed a responsive infant with generalized hypotonia. Head circumference was 34 cm (less than 3rd centile). The face was unusual, with frontal bossing, “coarse” appearance with bulbous nose, highly arched palate, and micrognathia. There was a large an- terior fontanelle and pectus excavatum. The infant re- sponded initially to intubation, continuous positive air- way pressure, and supplementary oxygen but subse- quently had intermittent episodes of respiratory distress thought to result from aspiration and bacterial pneu- monia. Results of laboratory investigations included normal cranial and abdominal ultrasonography, normal electromyogram and nerve conduction, computerized tomographic (CT scan) demonstrating subarachnoid hemorrhage, electroencephalogram (EEG) showing non- specific irregularities in the left midtemporal region, and barium swallow showing decreased esophageal motility with pharyngonasal and gastroesophageal reflux. Labo- ratory studies included mild acidosis without a significant anion gap; pyruvate and lactate were 1-%-fold elevated on one occasion. The chromosomes were normal. Endo- tracheal tube cultures showed presence of Klebsiella, Pseudomonas, and Staphylococcus aureus on two occa- sions and the child was treated with ampicillin and gentamicin from age 2-4 weeks. At 2 months, a urine metabolic screen demonstrated elevated ethylmalonic acid (32.8 mg/g creatinine; normal 2-10) and elevated adipic acid. Serum carnitine was 22.9 pmol/ml free (nor- mal 43.4 ? 4.4) and 31.1 total (normal 50.0 * 4.2). A trial of therapy with riboflavin (1 mg/kg/day IV), carnitine (100 mg/kg/day per nasogastric tube), and fat restriction was performed for 1 week. Transient improvement in alertness and neuromuscular tone was noted, but high- dose Septra’” therapy had simultaneously been intro- duced for suspected Pneumocystitis carinii infection (cul- ture negative). Normal serum carnitine, normal urine adipic acid, and decreased urine ethyl malonic acid (15.1 mg/g creatinine) were documented after 4 days of treat- ment. The subsequent course was one of progressive coma and respiratory insufficiency, ending in cardiorespiratory failure a t age 3% months.
RESULTS Enzyme Assays
Assays for ETF and ETF:QO in fibroblasts were per- formed by the methods of Frerman and Goodman [1985]. ETF activity was 0.9 milliunits/mg of protein (controls average 1.04 f 0.26, n = 11) and ETF:QO activity was 0.1 milliunits/mg of protein (controls 14.1 & 2.9, n = 20).
Autopsy Findings Gross autopsy findings included a weight of 4.8 kg (5th
centile); head circumference 39 cm (10th centile); alveolar
damage secondary to oxygen toxicity; diffuse gliosis of the cerebrum, brainstem, and cerebellum with foci of leukomalacia; thrombosis of the inferior vena cava and renal veins; Meckel diverticulum, and incomplete descent of the right testis. Microscopic changes included diffuse reactive gliosis in the white matter of the cerebrum, cerebellum, spinal cord, and most markedly in the brain- stem. Myelination appeared unremarkable. The esopha- geal musculature, myenteric plexus, and the psoas muscle appeared normal. Fatty infiltration was moderate but clearly evident in the centrilobar regions of the liver. Search for fatty change in other organs was not at- tempted.
Renal Pathology
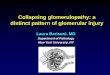
Histopathological study of the kidneys disclosed very moderate focal and segmental mesangial proliferation with increased mesangial matrix (Fig. 1). In the cortical subcapsular zones, microscopic cysts lined by epithelial cells could be seen. These originated from cystically dilated Bowman capsule since underdeveloped and im- mature-looking glomerular tufts were noted arising from their walls. The tubules and interstitium were unremark- able. Ultrastructural study of several glomeruli showed mesangial cell and matrix increase and a striking, wide- spread abnormality of the GBM, which had lost its normal trilaminar appearance. Instead, the lamina densa appeared either irregularly attenuated or thickened with segmental lamellation and reticulation (Fig. 2). Both the lamina rara externa and interna were also irregular and, in many places, new formation of a thin lamina densa immediately underlying either the podocytes or the endo- thelial cells could be seen (Fig. 3). In some segments,
Fig. 1. Light microscopic appearance of the glornerular change: seg- mental mesangial proliferation (arrows). Stain is PAS, magnification X400.

Glutaric Aciduria Type I1 397
attenuation of the GBM laminae was extreme (Fig. 4), and the complete dissolution of the GBM allowed direct contact between the epithelial cells and the endothelium. In addition, throughout the glomerular capillary loops, very unusual irregularly shaped but roughly spherical particles measuring approximately 50 pm were present. They were located within the interstices of the reticulated and lamellated GBM and within the lamina rara externa. In some segments, they seemed clustered freely in the subepithelial space (Fig. 3). The major foot-processes were swollen and broadened, with loss of filtration slits. Proliferation of the minor processes of the podocytes, intraepithelial osmiophilic bodies and endothelial swell-
ing were also observed. No significant change was rec- ognized in the tubules.
DISCUSSION
While most patients with GA I1 have been male, there is only one report [Coude et al., 19811 that suggests X- linked inheritance, and recent evidence suggests that ornithine transcarbamylase deficiency was responsible for death in infancy of the male relatives of the proposita. The presence of consanguinity in three families and the finding of ETF [Loehr, unpublished] or ETF:QO activi- ties [Frerman and Goodman, 19851 in obligate carriers
Fig. 2. Electron micrographic illustration of the glomerular changes. The GBM is segmentally lamellated and reticulated (arrows). Throughout the GBM, dense small particles are visible. In addition, there is partial effacement of the major foot-processes of the epithelial cells (EP) and marked proliferation of the minor processes. Some epithelial cells contain large osmophilic bodies (open arrows). Magnification X7,500.

398 Wilson et al.
Fig. 3. Very severely affected loops with predominantly subepithelial particles. Magnification x17,500.
intermediate between control and patient values suggests that both forms of GA I1 are autosomal recessive traits.
Metabolic alterations in GA I1 are summarized in Table I and presumably derive from the coupling of several acyl CoA dehydrogenases with ETF and ETF:QO [Goodman and Frerman, 19841. Elevation of isovaleric acid or its glycine conjugate produces a distinctive odor, although the two findings are not always correlated in the case reports. Elevation of several dicarboxylic acids (nine patients), long-chain fatty acids (three patients including the proposita), and the cognate organic acids probably cause the depletion of carnitine observed in some patients. Our patient exhibited transient clinical improvement and normalization of serum carnitine on a regimen of riboflavin, carnitine, and fat restriction. How- ever, simultaneous antibiotic therapy complicates inter- pretation of this result.
Our patient had only moderate elevation of urinary organic acids, yet fibroblast ETF:QO activity was unde- tectable. Since a high index of suspicion and repeated urinary metabolic screening may be required to identify GA I1 patients, their pattern of anomalies and pathologic changes assumes considerable importance. The clinical and pathologic manifestations of the proposita support and expand a characteristic phenotype for GA 11, as summarized in Table I. The prominent forehead, flat nasal bridge, and malformed ears of the proposita have been seen in a t least two GA I1 patients, and the large fontanelle was seen in five. Although the latter manifes- tation is typical of Zellweger syndrome, other manifes-
tations, such as bitemporal hollowing and tented upper lip, are never mentioned. One patient of Sweetman et al. [ 19801 had a short nose with anteverted nares.
The general effects on the fetus associated with the GA I1 have included intrauterine growth retardation, breech presentation, and premature delivery; these were not confined to patients with neonatal disease or congen- ital malformations. External anomalies have included macrocephaly (four patients), dolichocephaly (one pa- tient), hypospadias (two patients), cryptorchidism (three patients), equinovarus (one patient), simian creases (two patients), and whorl dermatoglyphic patterns (one pa- tient). Internal anomalies included cystic kidneys (seven patients), aberrant renal vessels (one patient), and con- genital heart defects (patent ductus and ventricular sep- tal defect, one patient).
Histopathologic abnormalities in GA I1 include fat deposition in heart, liver, and proximal tubular epithe- lium of the kidney. There were gliotic and heterotopic changes in the brain that were similar to those of Zell- weger syndrome, but not the severe lissencephaly, de- myelination, and sudanophilic granules that can be seen in the latter disorder [Wilson et al., 19861. Periportal hepatic fibrosis (two patients) and hypoplastic extrahe- patic biliary ducts (two patients) were also reminiscent of Zellweger syndrome, but the hepatomegaly (six pa- tients) and liver failure were much less severe (Table I). An interesting ultrastructural finding in GA I1 was re- ported by Harkin et al. [1986]. Small (0.4-0.8 nm in diameter) cytoplasmic membrane-limited bodies were ob-

Glutaric Aciduria Type I1 399
Fig. 4. Extreme attenuation ofthe GBM which is interrupted in several places (arrows). The endothelium is barely recognizable. The capillary lumen (CL) contains fibrin strands. The epithelial cells (EP) contain many osmophilic bodies. Magnification X11,750.
served in brain and kidney. In the brain, they occurred in the cerebral cortex, pons, and cerebellum; in the kid- ney, they were within the glomerular podocytes and in cells from the proximal tubule. The electron microscopic particles observed by Harkin et al. [1986] appear to be different from those in the proposita because they were smaller, enclosed in membranes, and had a broader tissue distribution within and outside of the kidney.
The GBM alteration observed in our patient is very distinctive, and we are not aware of any disease in which a similar change was reported including renal vein throm- bosis. As the GBM alteration was found in a case of GA I1 secondary to ETF:QO deficiency, it is reasonable to hypothesize i t may be genetically closely associated with,
or a consequence of, this enzymatic defect and possibly responsible for the development of cysts in the kidneys of patients who have GA 11. This hypothesis remains to be proved. However, reviewing the 16 cases of GA I1 found in the literature, we note that six cases were mentioned as having large kidneys, with some being clearly macrocystic; of those, three had ETF:QO defi- ciency, whereas the enzymatic defect in the remaining three was not established. Further ultrastructural studies on GA I1 patients will be required to determine the frequency and specificity of GBM alterations in ETF and ETF:QO deficiency. Since these defects are so closely related biochemically, it is likely that they will share a spectrum of anomalies and pathologic changes similar to

400 Wilson et al.
TABLE I. Morphologic and Metabolic Manifestations of GA I1 Case
Feature Sex Gestation (wks) Birth weight (kg) S u r v i v a 1
Odor Craniofacial
Macrocephaly Large fontanel High forehead Hypertelorism Flat nasal bridge Bulbous nose High palate Malformed ears Micrognathia
Fatty heart Hepatomegaly Fatty liver Large kidneys Fatty renal tub.
Hypotonia Gliosis Heterotopias
Metabolite" Glutaric Ethyl-malonic Adipic" Isovaleric'
ETF defic ETF: 90 defic
Internal
CNS
Enzyme
1
M t
__ 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 F F M M M F M F M M M M F F M t 38 37 t t 40 31 35 36 t t 35
2.9 2.5 2.7 3.6 2.9 1.4 2.1 1.8 2.6 3.7 2.2 70h 5y 19y I d 87h 5m Id 96h 2m l h 5d 4Ihd Ah 5d 3d
+ + + + + + + + +
+ + +
+ + + + + + + + + + + + + +
+ + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + +
+ + + + + + + +
+ + + +
+ + + + + + +
+ + +
+ + * + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + +
+ + + + +
Index M
2.7 3%m
39
+ +
+
Number positive
3 Premature 5 IUGR
l lM,5F
10 Neonatal death
6
4 6 3 3 5 1 2 4 2
5 7
1 2 6 3
9 7 3
17 10 9 5
2 6
' Urine, other dicarboxylic acids, ' or isovalerylglycine, t-term, Ab-abortus, IUGR-intrauterine growth retardation. Patients from reports of 1-Przyrembel et al., 1976; 2-Mantagos et al., 1979; 3-Dusheiko et al., 1979; 4, 5-Sweetman et al., 1980; 6-Goodman et al., 1980; 7-Gregerson et al., 1980; 8-Coude et al., 1981; 9-Goodman et al., 1982; l0,ll-Lehnert et al., 1982; 12-Goodman et al., 1983; 13,14-Bove et al., 1984; 15-Harkin et al., 1986; 16-Hoganson et al., 1987.
those outlined in Table I. The characteristic GBM alter- ations defined in our patient could serve as an additional diagnostic tool in GA 11, especially in autopsies where enzymatic studies are not available. Furthermore, should tissue be still available, such studies could be performed retrospectively on previously published cases. They could also be valuable for differentiation of GA I1 from Zell- weger syndrome and other peroxisomal disorders, in which the overlap of clinical, histologic, and metabolic findings is striking [Hoganson et al., 19871.
REFERENCES Bohm N, Uy J, Kiehling M, Lehnert W (1982): Multiple acylCoA
dehydrogenation deficiency (glutaric aciduria type II), congenital polycystic kidneys, and symmetric warty dysplasia of the cerebral cortex in two newborn brothers. 11. Morphology and pathogenesis. Eur J Pediatr 139:60-65.
Datta NS, Wilson GN, Hajra AK (1984): Deficiency of enzymes cata- lyzing the biosynthesis of glycerol-ether lipids in Zellweger syn- drome. A new category of metabolic disease involving the absence of peroxisomes. New Engl J Med 1?:1080-1083.
Dusheiko G, Kew MC, Joffe BI, Lewin JR, Mantagos S, Tanaka K (1979): Recurrent hypoglycemia associated with glutaric aciduria type I1 in an adult. N Engl J Med 301:1405-1409.
Frerman FE, Goodman SI (1985): Deficiency of electron transfer fla- voprotein or electron flavoprotein: Ubiquinone oxidoreductase in glutaric acidemia I1 fibroblasts. Proc Nat Acad Sci USA 824517- 4520.
Friedman A, Betzhold J, Hong R, Gilbert EF, Viseskul C, Opitz cJM (1980): Clinicopathologic conference: A three-month-old infant with failure to thrive, hepatomegaly, and neurologic impairment. Am J Med Genet 7:1?1-186.
Goodman SI, Frerman FE (1984): Glutaric acidemia type I1 (multiple acyl-CoA dehydrogenation deficiency). J Inherited Metab Dis ?
Goodman SI. McCahe ERB. Fennessev PV. Mace J W (1980): Multiole (Suppl 1): 33-39.
B~~~ J, Chalmers RA, T~~~~~ B, watson D, G~~~ R, ~ ~ ~ l i ~ ~ J, ~i~~ G, pett, TB, Lindenbaum R, ~ ~ ~ ~ h i ~ ~ ~ ~ l i F, Saudubray (1984): prenatal diagnosis of dysmorphic neonatal-lethal type 11 glutaric
acyl-CoA'dehydrogenase deficiency (glutaric aciduAa type 11) 4th transient hypersarcosinemia and sarcosinuria: Possible inherited deficiency of an electron transfer flavoprotein. Pediatr Res 1412- 1 7 I d . acidiiria. Lancet, 1 :846-847. . ~~~ ~~~~ ... ~ ~ ~
Coud& FX, ogier H, charpentier C, ~h~~~~~~~ G , checoury A, Am6dke. Manesme o, Saudubray JM, Frbzal (1981): Neonatal glutaric aciduria t w e 11: An X-linked recessive inherited disorder. Hum
Goodman SI, Reale M, Berlow S (1983): Glutaric acidemia type 11: A form with deleterious intrauterine effects. J Pediatr 102:411-413.
Goodman SI, Stene DO, McCabe ERB, Norenberg MD. Shikes RH. Genet 59:263-265. Stumpf DA, Blackburn GK (1982): Glutaric acidemia type 11: Clin-

Glutaric Aciduria Type I1 401
ical, biochemical, and morphologic considerations. J Pediatr 100:946-950.
Gregersen N, Kolvraa S, Rasmussen K, Christensen E, Brandt NJ, Ehbesen F, Hansen FH (1980): Biochemical studies in a patient with defects in the metabolism of acyl-CoA and sarcosine: Another pos- sible case of glutaric aciduria type 11. J Inher Metab Dis 357-72.
Harkin JC, Gill WL, Shapira E (1986): Glutaric acidemia type 11: Phenotypic findings and ultrastructural studies of brain and kidney. Arch Path Lab Med 110:399-401.
Hoganson G, Berlow S, Gilbert EF, Frerman F, Goodman S, Schweitzer L (1987): Glutaric acidemia type I1 and flavin-dependent enzymes in morphogenesis. BD:OAS 23(1):65-74.
Lehnert W, Wendel U, Lindenmaier S, Bohm N (1982): Multiple acyl- CoA dehydrogenation deficiency (glutaric aciduria type II), congen-
ital polycystic kidneys, and symmetric warty dysplasia of the cerebral cortex in two brothers. I. Clinical, matabolical and biochemical findings. Eur J Pediatr 139:56-59.
Mantagos S, Gene1 M, Tanaka K (1979): Ethylmalonic-adipic aciduria: In vivo and in vitro studies indicating deficiency of activities of multiple acyl-CoA dehydrogenases. J Clin Invest 64:1580-1589.
Przyrembel H, Wendel U, Becker K, Bremer HJ, Bruinvis L, Ketting D, Wadman SK (1976): Glutaric aciduria type 11: Report on a previously undescribed metabolic disorder. Clin Chim Acta 66227- 239.
Sweetman L, Nyhan WL, Trauner DA, Merritt TA, Singh M (1980): Glutaric aciduria type 11. J Pediatr 96:1020-1026.
Wilson GN, Holmes RD, Custer J , Lipkowitz JL, Stover J , Datta N , Hajra A (1986): Zellweger syndrome: Diagnostic assays, syndrome delineation, and potential therapy. Am J Med Genet 24:69-82.