Embed Size (px)
Citation preview

Glycoprotein IIb/IIIa Antagonists: A Systematic Review of Randomized Clinical Trials in Patients Undergoing Percutaneous Coronary Intervention
Technology Report
Issue 49 January 2005

Cite as: Ho C, Banerjee S, Martin J, Labinaz M, Chen S, Mensinkai S. Glycoprotein IIb/IIIa antagonists: a systematic review of randomized clinical trials in patients undergoing percutaneous coronary intervention [Technology report no 49]. Ottawa: Canadian Coordinating Office for Health Technology Assessment; 2005. Reproduction of this document for non-commercial purposes is permitted provided appropriate credit is given to CCOHTA. CCOHTA is a non-profit organization funded by the federal, provincial and territorial governments. Legal Deposit - 2005 National Library of Canada ISBN: 1-894978-54-4 (print) ISBN: 1-894978-55-2 (online) PUBLICATIONS MAIL AGREEMENT NO: 40026386 RETURN UNDELIVERABLE CANADIAN ADDRESSES TO CANADIAN COORDINATING OFFICE FOR HEALTH TECHNOLOGY ASSESSMENT 600-865 CARLING AVENUE OTTAWA ON K1S 5S8
Publications can be requested from:
CCOHTA 600-865 Carling Avenue
Ottawa ON Canada K1S 5S8 Tel. (613) 226-2553 Fax. (613) 226-5392
Email: [email protected]
or download from CCOHTA’s web site: http://www.ccohta.ca

Canadian Coordinating Office for Health Technology Assessment
Glycoprotein IIb/IIIa Antagonists: A Systematic Review of
Randomized Clinical Trials in Patients Undergoing Percutaneous Coronary Intervention
Chuong Ho MD MSc1 Srabani Banerjee PhD1 Janet Martin PharmD2
Marino Labinaz MD FRCPC FACC3 Stella Chen BSc MD1
Shaila Mensinkai MA MLIS1
January 2005
1 Canadian Coordinating Office for Health Technology Assessment, Ottawa ON 2 London Health Sciences Centre, Department of Pharmacy Services, London ON 3 University of Ottawa Heart Institute, Division of Cardiology, Ottawa ON

i
Reviewers
These individuals kindly provided comments on this report.
External Reviewers Mark Eisenberg, MD MPH Associate Professor of Medicine Divisions of Cardiology and Clinical Epidemiology McGill University Montreal QC
Cynthia Jackevicius, BScPhm MSc PharmD FCSHP Assistant Professor Faculty of Medicine University of Toronto Toronto ON
CCOHTA Scientific Advisory Panel Reviewers Ruth L. Collins-Nakai, MD MBA FRCPC FACC Cardiologist Edmonton AB
This report is a review of existing public literature, studies, materials and other information and documentation (collectively the “source documentation”) which are available to CCOHTA. The accuracy of the contents of the source documentation on which this report is based is not warranted, assured or represented in any way by CCOHTA and CCOHTA does not assume responsibility for the quality, propriety, inaccuracies or reasonableness of any statements, information or conclusions contained in the source documentation. CCOHTA takes sole responsibility for the final form and content of this report. The statements and conclusions in this report are those of CCOHTA and not of its Panel members or reviewers. Authorship
Dr. Chuong Ho led the protocol development, supervised the literature review, wrote the draft, revised the report and prepared the report for publication. Drs. Srabani Banerjee, Janet Martin and Stella Chen worked with Dr. Ho to evaluate the relevance of articles, assess their quality, extract data and complete the report. Dr. Marino Labinaz provided clinical expertise; and contributed to the draft and subsequent revisions. Ms. Shaila Mensinkai was responsible for designing and executing the literature search strategies; for writing the section and associated appendix on literature searching; and for verifying and formatting the references. Acknowledgements The authors are grateful to the CCOHTA staff members who helped us complete this project. We thank Dr. Andrew Hills for his early involvement with the project. Conflicts of Interest No conflicts of interests were declared by any of the authors.

2
REPORT IN BRIEF January 2005 Glycoprotein Inhibitor Drugs for Treatment of Heart Attacks and Unstable Angina
Technology Name Glycoprotein (GP) IIb/IIIa inhibitor drugs (abciximab, eptifibatide and tirofiban)
Disease/Condition Myocardial infarction (heart attack) and acute coronary syndrome, including unstable angina, occur when coronary arteries are blocked by platelet-rich blood clots and a build-up of cholesterol and fatty material. In percutaneous coronary interventions (PCIs), which are medical procedures that relieve the blockage, a catheter is threaded through the skin into the artery to widen it. While PCIs improve coronary blood flow, re-narrowing of the vessel, death and myocardial infarction commonly occur.
Technology Description GP IIb/IIIa inhibitor drugs were developed to prevent platelet activation and clumping, which are pivotal factors in blood clot formation and other significant complications after PCIs.
The Issue Using GP IIb/IIIa inhibitors could be a promising treatment for patients undergoing a PCI for acute coronary syndrome or myocardial infarction. There is a need to assess how well these drugs work and their safety.
Assessment Objectives This systematic review aims to assess the efficacy and safety of intravenously administered GP IIb/IIIa in patients undergoing a PCI for the treatment of acute myocardial infarction or acute coronary syndrome.
Methods We used a literature search to identify 25 comparative trials that examined the clinical efficacy of GP IIb/IIIa inhibitor drugs in nearly 30,000 patients undergoing a PCI. A meta-analysis of the data was performed.
Conclusions • GP IIb/IIIa inhibitor drugs significantly reduce
myocardial infarction and re-narrowing of coronary arteries at seven days, 30 days and six months after a PCI.
• Most of the evidence is derived from trials on abciximab, the most widely studied agent. Eptifibatide and tirofiban are not found to be superior to abciximab.
• The death rate with abciximab treatment is reduced. The reduction is only significant at 30 days after a PCI. Eptifibatide and tirofiban are not associated with any significant reduction in the risk of death.
• The beneficial effect of GP IIb/IIIa inhibitors must be weighed against the potential for a significant increase in minor bleeding.
This summary is based on a comprehensive health technology assessment available from CCOHTA’s web site (www.ccohta.ca): Ho C, Banerjee S, Martin J, Labinaz M, Chen S, Mensinkai S. Glycoprotein IIb/IIIa antagonists: a systematic review of randomized clinical trials in patients undergoing percutaneous coronary intervention.
Canadian Coordinating Office for Health Technology Assessment (CCOHTA) 600-865 Carling Avenue, Ottawa ON Canada K1S 5S8 Tel: 613-226-2553 Fax: 613-226-5392 www.ccohta.ca
CCOHTA is an independent, not-for-profit organization that supports informed health care decision-making by
providing unbiased, reliable information about health technologies.

iii
EXECUTIVE SUMMARY The Issue Cardiovascular disease, which is the leading cause of hospital admissions for Canadian men and women (when childbirth and pregnancy are excluded), is the leading cause of death in Canada. Ischemic heart disease, including acute coronary syndrome and myocardial infarction (MI), is the greatest contributor to cardiovascular deaths in Canada. Several surgical procedures, including coronary artery bypass grafts (CABGs) and percutaneous coronary interventions (PCIs), have been used to improve the clinical outcomes of patients with ischemic coronary artery disease. The goal of a PCI is to relieve coronary stenosis and improve blood flow. PCIs, however, are associated with complications such as death, MI and restenosis requiring urgent repeat revascularization. Platelet aggregation, mediated by the cross-linking of glycoprotein IIb/IIIa (GP IIb/IIIa) receptors on adjacent platelet membranes, is pivotal in the development of clinical complications after a PCI. Consequently, the inhibition of GP IIb/IIIa receptors by pharmacologic agents could be a promising therapeutic modality for patients undergoing a PCI. Objective The objective of this report is to review the clinical effectiveness of GP IIb/IIIa antagonists in patients who are undergoing PCI. The report is intended to help formulary decision makers and others who are involved in the provision of anticoagulation.
This objective is accomplished by addressing the following questions:
• What is the evidence of benefit and harm of marketed intravenous GP IIb/IIIa antagonists in patients who are undergoing PCI?
• What are the outcomes of each of the GP IIb/IIIa antagonists (i.e., from head-to-head comparisons)?
Methods Published literature was obtained by searching multiple databases using a defined strategy and by hand searching the bibliographies of selected papers. A meta-analysis was performed. Results
A total of 25 randomized controlled trials (RCTs) focusing on the use of GP IIb/IIIa antagonists were identified. These included 15 trials of abciximab, four of eptifibatide, two of tirofiban and four head-to-head trials; and involved a total of 29,323 patients. Major clinical outcomes on which GP IIb/IIIa antagonists were found to have statistically significant effects include death at 30 days; MI at seven days, 30 days and six months; revascularization at seven days, 30 days and six months; and minor bleeding. The drugs reduce the odds of death at 30 days by 28%, of MI at seven days by 41%, of MI at 30 days by 37% and of MI at six months by 35%. The drugs also reduce revascularization at seven days, 30 days and six months by 51%, 34% and 14% respectively. The use of GP IIb/IIIa antagonists, however, significantly increases the odds of minor bleeding by 80%. The increase in major bleeding is not significant. Calculations show that 296 patients need to be treated to save one life at 30 days, 37

iv
patients need to be treated to prevent one MI at seven days, 47 patients need to be treated to prevent one MI at 30 days and 37 patients need to be treated to prevent one MI at six months. Revascularization events at seven days, 30 days and six months can also be prevented by treating 46 patients, 59 patients and 49 patients respectively. Also, 39 patients need to be treated with the drugs for one event of minor bleeding to occur. Conclusions GP IIb/IIIa inhibitors as a class significantly reduce MI and the need for revascularization at seven days, 30 days and six months in patients undergoing a PCI. Significant reductions in mortality were only detected at 30 days. Most of the evidence is derived from trials on abciximab, the most widely studied agent. The small-molecule agents (eptifibatide and tirofiban) are not associated with any significant reduction in the risk of death. Small trials have failed to show the superiority of the small-molecule agents over abciximab. The beneficial effect of GP IIb/IIIa inhibitors is tempered by a significant increase in minor bleeding.

v
TABLE OF CONTENTS EXECUTIVE SUMMARY ................................................................................................... iii 1 INTRODUCTION........................................................................................................... 1
1.1 Background............................................................................................................... 1 2 THE ISSUE...................................................................................................................... 3 3 OBJECTIVES ................................................................................................................. 3 4 METHODS ...................................................................................................................... 4
4.1 Literature Search Strategy......................................................................................... 4 4.2 Selection Criteria and Method .................................................................................. 4
4.2.1 Selection criteria ............................................................................................ 4 4.2.2 Selection method............................................................................................ 4
4.3 Data Extraction and Abstraction Strategy................................................................. 4 4.4 Strategy for Quality Assessment............................................................................... 5 4.5 Data Analysis Method............................................................................................... 5
5 RESULTS ........................................................................................................................ 6
5.1 Quantity and Quality of Research Available ............................................................ 6 5.2 Trial Characteristics .................................................................................................. 7 5.3 Data Analysis and Synthesis..................................................................................... 8
5.3.1 Abciximab...................................................................................................... 8 5.3.2 Eptifibatide................................................................................................... 15 5.3.3 Tirofiban ...................................................................................................... 15 5.3.4 Abciximab, eptifibatide and tirofiban .......................................................... 15 5.3.5 Abciximab versus eptifibatide and abciximab versus tirofiban................... 23 5.3.6 Summary of findings.................................................................................... 23
6 DISCUSSION ................................................................................................................ 23 7 CONCLUSIONS ........................................................................................................... 26 8 REFERENCES.............................................................................................................. 27 Appendix 1: Literature Search Strategies ............................................................................... 31 Appendix 2: Trial Quality Assessment Form ......................................................................... 35 Appendix 3: Baseline Patient Characteristics ......................................................................... 36 Appendix 4: Inclusion and Exclusion Criteria of Trials ......................................................... 43 Appendix 5: Use of Concomitant Medications....................................................................... 49 Appendix 6: Definitions of Composite End-Point (CEP)....................................................... 53

vi
Appendix 7: Included Trials of GP IIb/IIIa Antagonists ........................................................ 56 Appendix 8: Results from Trials on Abciximab ..................................................................... 59 Appendix 9: Results from Trials on Eptifibatide.................................................................... 66 Appendix 10: Results from Trials on Tirofiban...................................................................... 69 Appendix 11: Results from Head-to-head Trials .................................................................... 70 Appendix 12: Summary of Findings....................................................................................... 72

1
1 INTRODUCTION
1.1 Background Cardiovascular diseases, including myocardial infarction (MI), cardiovascular accidents, heart failure and heart valve disease, are the leading cause of hospital admissions for Canadian men and women (when childbirth and pregnancy are excluded). They are the leading cause of death in Canada. Ischemic heart disease is the greatest contributor to cardiovascular deaths in Canada.1 Several surgical procedures, including coronary artery bypass grafts (CABGs) and percutaneous coronary interventions (PCIs), have been used to improve the clinical outcomes of patients with ischemic coronary artery disease. PCIs are the most common method of coronary revascularization, with over one million procedures performed annually. PCIs involve percutaneous transluminal coronary angioplasty (PTCA), atherectomy and coronary stenting with the latter being the most common technique used. In all cases, the goal is to relieve coronary stenosis and improve blood flow. PCIs are associated with severe local vascular trauma, including arterial dissection, thrombosis, spasm and micro- and macroembolization of atherosclerotic and thrombotic material. As a result, PCIs lead to complications such as death, MI and urgent repeat revascularization. In PTCA, a catheter with a small balloon is radiographically guided, usually from the femoral artery, to a narrowed or blocked segment of a coronary artery. The balloon is then inflated to split the atheromatous plaque, thus dilating the coronary artery lumen. Patients are treated with anticoagulants before and after PTCAs, which are undertaken by interventional cardiologists in a cardiac catheterization laboratory. Over 24,000 angioplasties are performed in Canada annually (1996 data).1 After a successful PTCA, up to 30% of patients experience restenosis, defined as an angiographic renarrowing of the dilated segment, within six months of the dilatation. Patients experiencing restenosis may develop clinical evidence of myocardial ischemia and may need repeat PTCA. In coronary stenting, an intraluminal prosthesis (stent) is placed to scaffold the treated vessel and maintain its patency. The addition of a stent reduces the risk of abrupt reclosure and restenosis after coronary angioplasty, but it also increases the risk of thrombus formation at the implantation site. While the recent introduction of drug eluting stents used with GP IIb/IIIa inhibitors and heparin has reduced the risk of restenosis, stenotic complications have not been mitigated. The restenotic complications of PCIs can be managed using mechanical interventions (prolonged balloon inflation, reperfusion catheter, stent placement, intra-aortic balloon pump) or pharmacologic therapies [inotropic support, vasopressors, vasodilators, fibrinolytics, glycoprotein IIb/IIIa (GP IIb/IIIa) antagonists].
1.2 Technology Overview The discovery of the pivotal role of platelets in the pathophysiology of acute coronary syndromes and PCIs has been one of the major cardiovascular advances of the 20th century. Platelet adhesion, activation and aggregation are key steps in the vascular response to injury

2
after a PCI. The final pathway of platelet aggregation is mediated by the GP IIb/IIIa receptor, which is significantly up-regulated when platelets become activated. Platelets adhere to each other via the GP IIb/IIIa receptor and its ligands, including fibrinogen and von Willebrand factor. When the importance of the GP IIb/IIIa receptor was realized, this led to the development of three intravenous antagonists: abciximab, eptifibatide and tirofiban. Abciximab, which is a large molecule that binds irreversibly to the platelet GP IIb/IIIa receptors, tends to have a prolonged antiplatelet effect. It also binds to other integrins, including the AvB3 receptor on platelets, vascular smooth muscle cells and endothelial cells; and the Mac-1 receptor on activated monocytes and macrophages. The significance of its binding to the latter two integrins has not been elucidated. Eptifibatide is a cyclic heptapeptide that binds directly to the GP IIb/IIIa receptor, while tirofiban is a small molecule that binds to the RGD sequence of the GP IIb/IIIa receptor. Eptifibatide and tirofiban bind reversibly to the platelet and quickly dissociate when plasma levels drop, resulting in a short antiplatelet effect. They do not to bind to other integrins. Because of the pharmacologic action of GP IIb/IIIa antagonists, there is an increased risk of bleeding that is inherent to these agents when considered alone or with other antiplatelet therapies and antithrombotic agents. Theoretically, abciximab may lead to a greater increase in the risk of bleeding relative to eptifibatide and tirofiban. The increased risk of bleeding is of concern in patients who require intervention procedures shortly after an infusion of the drugs. Consequently, the bleeding risk associated with GP IIb/IIIa antagonists must be considered concomitantly with the benefits. It is also not evident that the use of GP IIb/IIIa antagonists after PCIs provides a sustained benefit in the prevention of restenosis. Three intravenous GP IIb/IIIa antagonists have been approved for use in Canada: the monoclonal antibody fragment of the GP IIb/IIIa receptor, abciximab (Reopro™; Centocor/Lilly); the cyclic heptapeptide, eptifibatide (Integrilin™; Cor Therapeutics); and the non-peptide tyrosine derivative, tirofiban (Aggrastat™; Merck & Co.). Abciximab, eptifibatide and tirofiban are indicated for the prevention of cardiac ischemic complications in patients with high risk acute coronary syndrome (ACS) for whom a PCI is planned or anticipated. Only abciximab and eptifibatide are indicated for adjunct therapy initiated at the time of a PCI. Eptifibatide and tirofiban (but not abciximab) are indicated for the medical management of patients presenting with the symptoms of unstable angina UA/non-Q-wave myocardial infarction (NQWMI) when a PCI is not planned. This review, however, only focuses on the use of GP IIb/IIIa inhibitors in patients undergoing a PCI. Several randomized clinical trials (RCTs) have compared abciximab, eptifibatide and tirofiban to placebo. There have also been some head-to-head comparisons. As a result of the large number of RCTs, a systematic review is warranted. In this report, we review the available evidence from RCTs of the clinical benefit and harm associated with the use of GP IIb/IIIa antagonists in patients undergoing PCIs.

3
Table 1: Intravenous GP IIb/IIIa antagonists approved for use in Canada
Drug DIN Strength/ Dosage Form
Cost per Unit Dose Used
Abciximab (Reopro; Centocor/Lilly)
02216973 10 mg/5 mL vial $536.65 bolus 0.25 mg/kg + infusion 0.125 µg/kg/minute (maximum 10 µg/kg/minute) for 12 hours
Eptifibatide (Integrilin; Cor Therapeutics)
02240352 02240351
20 mg/10 mL bolus vial 75 mg/100 mL infusion vial
$38.00 $111.25
bolus 180 µg/kg x 2 + infusion2 µg/kg/minute for 12 hours (range 12 to 24 hours)
Tirofiban (Aggrastat; Merck Frosst)
02240705 02240706
12.5 mg/50 mL concentrated solution vial 12.5 mg /250 mL infusion solution bag
$322.88 bolus 10 µg/kg + infusion 0.15 µg/kg/minute for 12 hours (range 12 to 24 hours)
2 THE ISSUE It is not evident that the use of GP IIb/IIIa antagonists after PCIs provides a sustained benefit regarding clinical outcomes such as death and MI; and the need for revascularization in patients with ischemic heart disease. The pharmacologic action of the drugs also favours a risk of bleeding. With the widespread use of GP IIb/IIIa antagonists in ischemic heart disease, which is the greatest contributor to cardiovascular deaths in Canada, a systematic review of RCTs is needed to clarify the clinical benefit and harm of these drugs. 3 OBJECTIVES The objective of this report is to review the clinical effectiveness of GP IIb/IIIa antagonists in patients who are undergoing PCI. The report is intended to help formulary decision makers and others who are involved in the provision of anticoagulation.
This objective is accomplished by addressing the following questions:
• What is the evidence of benefit and harm of marketed intravenous GP IIb/IIIa antagonists in patients who are undergoing PCI?
• What are the outcomes of each of the GP IIb/IIIa antagonists (i.e., from head-to-head
comparisons)?

4
4 METHODS This systematic review was performed in accordance with QUORUM recommendations.2
4.1 Literature Search Strategy Published literature was obtained by searching multiple databases on the OVID online system, including MEDLINE®, EMBASE®, BIOSIS Previews®, Current Contents® and HealthSTAR. The search strategy focused on the objectives of the report and was built on descriptors; trade and generic names for glycoprotein antagonists licensed in Canada; their registry numbers; and descriptors and text words for the patient population (Appendix 1). A clinical filter was used to restrict retrieval to relevant studies. There were no date or language restrictions. Regular alerts were established on the DIALOG® system until April 2004 for MEDLINE®, EMBASE® and BIOSIS Previews® databases to retrieve newer citations. Searches were also performed on the Cochrane Library, 2001 to 2004. Updates were performed on PubMed to retrieve pre-Medline and other records. The last PubMed update was in April 2004. Selected published bibliographies were hand searched for additional information. Grey literature was retrieved by searching the web sites and databases of HTA and related agencies, major associations and trial registries. The Internet was searched using search engines and subject gateways.
4.2 Selection Criteria and Method
4.2.1 Selection criteria
Trials were selected for inclusion if they satisfied each of the following criteria: • randomized controlled trials (study design) • patients undergoing a PCI (population group) • GP IIb/IIIa antagonists (eptifibatide, tirofiban and abciximab) as interventions • GP IIb/IIIa antagonist or placebo as comparators • at least one death, MI or revascularization; or a composite endpoint (CEP) as outcomes. We excluded trials of patients with ACS who were not intended to undergo a PCI.
4.2.2 Selection method
Two reviewers (CH and JM) independently selected the relevant trials. Disagreements were resolved by discussion.
4.3 Data Extraction Strategy After the selection of relevant trials, data were extracted using a structured form. The form was designed to capture information on the trial (first author, year of publication, journal,

5
publication status, period and country of study, number of centres, sources of funding, study design, sample size), the characteristics of patients (age, gender, smoking status, health conditions and prior treatments) the intervention (drug, dosage, route of administration and concomitant medications), the outcomes (death, MI, revascularization and CEP) and the adverse events (bleeding and thrombocytopenia). Data were extracted by two reviewers (CH and JM or CH and SB) and verified for accuracy by CH and SB.
4.4 Strategy for Quality Assessment The quality of the included trials was evaluated using the Jadad five-point scale.3 This scale assesses randomization (0 to 2 points), double-blinding (0 to 2 points) and withdrawals or drop-outs (0 to 1 point), with higher values indicating superior quality. The concealment of allocation was categorized as adequate, inadequate or unclear. The quality was rated using a quality assessment form (Appendix 2) that was based on the Jadad scale.
4.5 Data Analysis Method In most trials, the outcomes investigated were death, MI, revascularization and CEP. The primary endpoint was defined as all-cause mortality at 30 days, six months and 12 months. The secondary endpoints included new onset AMI; need for repeat revascularization (rTVR); stroke; and composite outcomes, including two or more of death, MI and rTVR. The harm endpoints included major hemorrhage, minor hemorrhage, the need for transfusion and thrombocytopenia. We used the same definition of MI as the one used by the study authors, who most commonly defined it with ECG and enzymatic criteria. rTVR was usually defined as the need for a repeat PCI and CABG. The composite endpoint that was most commonly reported was death or MI. Major hemorrhage was most commonly defined according to the TIMI criteria or the GUSTO criteria. The need for transfusions was defined as the number of patients requiring one or more transfusions of any blood product. Thrombocytopenia was defined as platelets <100,000/mm3. Profound thrombocytopenia was defined as platelets <50,000/mm3. All comparisons were between GP IIb/IIIa antagonists (abciximab, eptifibatide or tirofiban) and placebo or control with no placebo. In some trials, the dosage of concomitant therapies, such as heparin, was not the same across different arms. In these cases, (e.g., in EPILOG, the two treatment arms were abciximab+standard dose heparin and abciximab+low dose heparin; and the control arm was placebo+standard dose heparin), outcomes data from arms with the same concomitant therapy (i.e., in EPILOG, abciximab+standard dose heparin and placebo+standard dose heparin) were used for comparison as matched comparators. In matched comparator analysis, the main difference between the arms is the presence or absence of the GP IIb/IIIa antagonist. Subsequently, all treatment arms, regardless of the difference in concomitant therapies, were compared to control arms all comparators. Whenever possible, analyses were performed on an intention-to-treat basis (patients were analyzed according to their allocated treatment), irrespective of whether they received treatment.

6
To compare the outcomes in different treatment arms, odds ratios (OR) with the corresponding 95% confidence intervals (CI) were computed and forest plots were generated using Stata 7.0 software. If no events were observed in both arms, the trial was omitted from the meta-analysis, because it provided no information about relative event rates. ORs were computed such that a value of <1 indicated that the GP IIb/IIIa treatment arm was better. The chi-square test was used to assess effect size variance, with p<0.10 indicating significant heterogeneity across trials. The ORs were pooled using the fixed effects model (when heterogeneity was absent) and the random effects model. Results using the more conservative random effects model were reported for all outcomes. Only figures with statistically significant results were shown. To facilitate interpretation of the clinical significance of the results, numbers needed to treat (NNT) and number needed to harm (NNH) were calculated for all statistically significant outcomes. Statistical significance was defined as p<0.05 or 95% confidence intervals of the OR that did not include unity. 5 RESULTS
5.1 Quantity and Quality of Research Available We identified 838 abstracts in our original searches of multiple databases. In addition, 234 subsequent alerts were screened up to February 2004. Of these, 135 reports were retrieved. After the elimination of reports that did not satisfy our selection criteria, there were 48 relevant reports describing 25 unique trials (Figure 1). The median Jadad quality score was 4 (range 2 to 5). The most common quality element not met (or not reported adequately in the trials) was double-blinding.
5.2 Trial Characteristics Twenty-five RCTs were included in the analysis.4-28 Appendix 3 outlines the baseline characteristics of the participants. Appendix 4 outlines inclusion and exclusion criteria. Appendix 5 outlines the concomitant medications. Appendix 6 summarizes the different definitions of CEPs. No RCTs were conducted exclusively in Canada. Of the 18 multicentre trials, six included patients from Canada. Most of the patients were from the US. All RCTs were placebo-controlled trials except CADILLAC, COMPARE, ISAR-2, PRICE, TARGET and TEAM, which did not include placebo in the comparator arm(s). Fifteen trials were double-blinded. Abciximab was evaluated in 15 trials 4-6,8-10,12,14,16,18,20-23,28 eptifibatide in four trials,13,15,17,19 and tirofiban in two trials.11,26 Four trials were head-to-head trials.7,24,25,27 The length of

7
follow-up ranged from in-hospital stay to seven years (Appendix 7). Details about the included RCTs appear in Appendix 7. A total of 29,323 patients were enrolled in the 25 RCTs. The 21 RCTs that compared glycoprotein IIb/IIIa inhibitors to placebo or control involved 23,941 patients. No clinically important differences in baseline characteristics were apparent between patients randomized to glycoprotein IIb/IIIa inhibitors (14,040) or placebo or control (9,901). The mean or median age reported in the trials ranged from 58 to 63 years. Among participants, 74% were male, 35% had a history of MI and 21% had diabetes.
Figure 1: Selected reports
937 citations excluded
838 citations identified from electronic search and broad screened
135 potentially relevant reports retrieved for further scrutiny (full text, if available)
87 reports excluded: • did not contain sufficient
information (7) • no additional trial information (8) • trial design not appropriate for
review (72)
234 citations identified from other sources
48 relevant reports describing 25 unique trials

8
5.3 Data Analysis and Synthesis The results from the included trials are presented in Appendices 8 to 11. Only forest plots with statistically significant results using all comparators are shown.
5.3.1 Abciximab
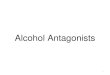
The results from the trials on abciximab are shown in Appendix 8 Tables 1 to 15. a) Death The effects of abciximab on death at seven days, 30 days, six months and one year are calculated. No clear benefit is shown for the abciximab group, when it is compared to the control group, except for the 30-day mortality outcome when all comparators are used (Figure 2). There is a 42% reduction in the odds of death at seven days. The result is not statistically significant. The overall estimate shows a statistically significant 28% reduction in the odds of death at 30 days, when all comparators are used.
Figure 2: Effect of abciximab on death at 30 days
Heterogeneity chi-squared=4.17 (d.f.=10) p=0.940 I-squared (variation in OR attributable to heterogeneity)=0.0%
.
0.001 0.01 0.1 1 10 100
Study
Odds ratio (95% CI)
Number of events Treatment Control
0.87 (0.42, 1.77) EPIC 12/696 21/1,403 0.75 (0.26, 2.18) CAPTURE 8/635 6/630 0.50 (0.18, 1.44) EPILOG 7/939 7/1,853 0.81 (0.27, 2.49) EPISTENT 5/809 8/1,590 1.21 (0.36, 4.02) RAPPORT 5/242 6/241 0.31 (0.01, 7.91) Galassi 1/52 0/54 0.43 (0.13, 1.42) ISAR-2 9/200 4/201 0.49 (0.16, 1.47) ADMIRAL 10/151 5/149 0.81 (0.45, 1.48) CADILLAC 24/1,030 20/1,052 0.24 (0.03, 2.22) Petronio 4/45 1/44 1.00 (0.20, 4.97) ISAR-REACT 3/1,080 3/1,079
0.72 (0.53, 0.99) Overall (95% CI)

9
There is a 16% reduction in the odds of death at six months, when matched comparators or all comparators are used. The results are not statistically significant. There is a 19% and 18% reduction in the odds of death at one year, when matched comparators or all comparators are used respectively. The results are not statistically significant. b) Myocardial infarction (MI) The effects of abciximab on MI in the various trials at seven days, 30 days, six months and one year are described in the forest plots in Figures 3 to 6. The use of abciximab is associated with a statistically significant decrease in the subsequent odds of MI at seven days, 30 days, six months and one year. The pooled estimate at one year, however, is associated with statistically significant heterogeneity for both sets of comparison (matched and all comparators). Accordingly, interpretation of the clinical benefit at one year should be done cautiously. The overall estimate in Figure 3 shows a statistically significant 49% reduction in the odds of MI at seven days, when all comparators are used. When only matched comparators are used, there is a statistically significant 58% reduction in the odds of MI.
Figure 3: Effect of abciximab on MI at seven days
Heterogeneity chi-squared=0.65 (d.f.=3) p=0.885 I-squared (variation in OR attributable to heterogeneity)=0.0% The overall estimate in Figure 4 shows a statistically significant 44% reduction in the odds of MI at 30 days, when all comparators are used. There is also a statistically significant 50% reduction in the odds of MI at 30 days, when matched comparators are used.
.
0.001 0.01 0.1 1 10 100
Study
Odds ratio (95% CI)
Number of events Treatment Control
0.22 (0.02, 2.14) EUR CO-OP 4/30 1/30
0.49 (0.15, 1.66) RAPPORT 8/242 4/241
0.61 (0.23, 1.58) ERASER 8/71 11/154
0.47 (0.08, 2.69) Tamburino 4/53 2/54
0.51 (0.26, 0.98) Overall (95% CI)

10
Figure 4: Effect of abciximab on MI at 30 days
Heterogeneity chi-squared=14.14 (d.f.=11) p=0.225 I-squared (variation in OR attributable to heterogeneity)=22.2% The overall estimate in Figure 5 shows a statistically significant 37% reduction in the odds of MI at six months, when all comparators are used. When only matched comparators are used, there is a statistically significant 38% reduction in the odds of MI.
Figure 5: Effect of abciximab on MI at six months
.0.001 0.01 0.1 1 10 100
Study Odds ratio (95% CI)
Number of events Treatment Control
0.69 (0.50, 0.94) EPIC 73/696 105/1,403 0.54 (0.36, 0.80) CAPTURE 73/635 41/630 0.49 (0.37, 0.66) EPILOG 93/939 95/1853 0.88 (0.44, 1.78) RAPPORT 18/242 16/241 0.54 (0.40, 0.74) EPISTENT 83/809 93/1,590 0.64 (0.26, 1.56) 9/71 13/154 0.50 (0.12, 2.02) ADMIRAL 6/151 3/149 1.51 (0.81, 2.80) CADILLAC 171/1,030 26/1,052 0.33 (0.01, 8.41) Petronio 1/45 0/44 0.32 (0.01, 8.06) Tamburino 1/53 0/54
0.63 (0.51, 0.78) Overall (95% CI)
.0.001 0.01 0.1 1 10 100
Study
Odds ratio (95% CI)
Number of events Treatment Control
0.64 (0.45, 0.91) EPIC 60/696 80/1,403 0.48 (0.30, 0.78) CAPTURE 52/635 26/630 0.41 (0.29, 0.57) EPILOG 81/939 69/1,853 0.48 (0.35, 0.67) EPISTENT 78/809 78/1590 0.80 (0.31, 2.05) RAPPORT 10/242 8/241 0.36 (0.07, 1.95) Galassi 5/52 2/54 0.11 (0.01, 2.30) Chen 3/20 0/22 0.33 (0.03, 3.18) ISAR-2 3/200 1/201 0.50 (0.09, 2.77) ADMIRAL 4/151 2/149 0.87 (0.33, 2.26) CADILLAC 9/1,030 8/1,0520.33 (0.01, 8.41) Petronio 1/45 0/44
0.98 (0.63, 1.52) ISAR-REACT 41/1,080 40/1,079
0.56 (0.46, 0.69) Overall (95% CI)
ERASER
Heterogeneity chi-squared=13.31 (d.f.=9) p=0.149 I-squared (variation in OR attributable to heterogeneity)=32.4%

11
The overall estimate in Figure 6 shows a statistically significant 35% reduction in the odds of MI at one year, when all comparators are used. The chi-squared test, however, shows statistically significant heterogeneity. When only matched comparators are used, there is a statistically significant 38% reduction in the odds of MI, with the chi-squared test also showing statistically significant heterogeneity.
Figure 6: Effect of abciximab on MI at one year
Heterogeneity chi-squared=8.42 (d.f.=3) p=0.038 I-squared (variation in OR attributable to heterogeneity)=64.4% c) Revascularization The effects of abciximab on revascularization at 30 days and six months are described in the forest plots in Figures 7 and 8. Overall, a statistically significant decrease in the need for revascularization is observed for abciximab at 30 days and six months. The clinical benefit at one year is unclear, because of the lack of statistical significance when all comparators are used. The pooled estimate for this comparison is also associated with statistically significant heterogeneity. At seven days, there is a 58% and 67% reduction in the odds of revascularization, when matched comparators or all comparators are used respectively. The results are not statistically significant. The overall estimate shows a statistically significant 40% reduction in the odds of revascularization at 30 days, when all comparators are used (Figure 7). When only matched comparators are used, there is statistically significant 43% reduction in the odds of revascularization.
.
0.01 0.1 1 10
Study
Odds ratio (95% CI)
Number of events Treatment Control
0.73 (0.54, 0.99) EPIC 77/696 117/1,403
0.48 (0.36, 0.64) EPILOG 98/939 98/1,853
0.57 (0.43, 0.77) EPISTENT 91/809 108/1,590
1.11 (0.63, 1.96) CADILLAC 23/1,030 26/1,052
0.65 (0.49, 0.86) Overall (95% CI)

12
Figure 7: Effect of abciximab on revascularization at 30 days
Heterogeneity chi-squared=12.00 (d.f.=10) p=0.285 I-squared (variation in OR attributable to heterogeneity)=16.6% At six months (Figure 8), the overall estimate shows a statistically significant 15% reduction in the odds of revascularization, when all comparators are used. The overall estimate shows a statistically significant 17% reduction in the odds of revascularization, when matched comparators are used. There is a 10% reduction in the odds of revascularization at one year, when all comparators are used. The result, however, is not statistically significant. The chi-squared test also shows statistically significant heterogeneity. When matched comparators are used, the overall estimate shows a statistically significant 17% reduction in the odds of revascularization.
.
0.001 0.01 0.1 1 10 100
Study
Odds ratio(95% CI)
Number of events Treatment Control
0.55 (0.38, 0.79) EPIC 56/696 64/1,403 0.74 (0.52, 1.06) CAPTURE 78/635 59/630 0.37 (0.24, 0.57) EPILOG 48/939 36/1,853 0.74 (0.40, 1.39) EPISTENT 17/809 25/1,590 0.71 (0.40, 1.27) RAPPORT 30/242 22/241 0.15 (0.01, 3.78) ERASER 1/71 0/154 2.86 (0.11, 74.31) Chen 0/20 1/22 0.58 (0.21, 1.64) ISAR-2 10/200 6/201 0.55 (0.25, 1.21) ADMIRAL 19/151 11/149 0.54 (0.33, 0.87) CADILLAC 48/1,030 27/1,052 1.43 (0.54, 3.78) ISAR-REACT 7/1,080 10/1,079
0.60 (0.49, 0.73) Overall (95% CI)

13
Figure 8: Effect of abciximab on revascularization at six months
Heterogeneity chi-squared=6.33 (d.f.=9) p=0.707 I-squared (variation in OR attributable to heterogeneity)=0.0% d) Composite End Point (CEP) The use of abciximab was associated with a 24% reduction in the odds of occurrence of CEP at one year, although the confidence interval was at the limit of statistical significance (CI 0.58, 1,00). The pooled estimate was associated with statistically significant heterogeneity, so caution should be used in the interpretation of the result. e) Adverse events Bleeding The effects of abciximab on major and minor bleeding complications are calculated. The effect of abciximab on minor bleeding is shown in Figure 9. No statistically significant increase in the risk of major bleeding is reported. The pooled estimate for major bleeding is associated with statistically significant heterogeneity. Interpretation of the results should be done with caution. There is a statistically significant 70% increase in the risk of minor bleeding (Figure 9).
.
0.001 0.01 0.1 1 10 100
Study Odds ratio (95% CI)
Number of events Treatment Control
0.78 (0.64, 0.96) EPIC 205/696 346/1,403 0.95 (0.74, 1.23) CAPTURE 171/635 164/630 0.96 (0.78, 1.17) EPILOG 180/939 343/1,853 0.93 (0.60, 1.44) RAPPORT 53/242 50/241 0.72 (0.41, 1.27) EPISTENT 21/809 30/1,590 0.91 (0.41, 1.99) ERASER 11/71 22/154 0.68 (0.38, 1.19) ADMIRAL 36/151 26/149 0.76 (0.58, 1.00) CADILLAC 134/1,030 108/1,052 0.33 (0.03, 3.26) Petronio 3/45 1/44 0.48 (0.16, 1.40) Tamburino 11/53 6/54
0.85 (0.77, 0.94) Overall (95% CI)

14
Figure 9: Effect of abciximab on minor bleeding
Thrombocytopenia The use of abciximab was associated with a statistically significant 61% increase in the risk of thrombocytopenia (platelets count <100,000/mm3) (Figure 10).
Figure 10: Effect of abciximab on thrombocytopenia
.0.001 0.01 0.1 1 10 100
Study
Odds ratio (95% CI)
Number of events Treatment Control
0.32 (0.01, 8.24) EUR CO-OP 1/30 0/30 2.39 (1.24, 4.63) CAPTURE 13/635 30/630 1.55 (1.05, 2.29) EPILOG 35/939 105/1,853 1.69 (0.92, 3.10) EPISTENT 14/809 46/1,590 1.45 (0.96, 2.18) RAPPORT 55/242 72/241 1.96 (0.17, 22.31) Galassi 1/52 2/54 1.42 (0.21, 9.52) Chen 2/20 3/22 4.01 (1.45, 11.11) ADMIRAL 5/151 18/149 2.21 (0.52, 9.46) Petronio 3/45 6/44 2.00 (0.18, 22.74) Tamburino 1/53 2/54
1.70 (1.36, 2.13) Overall (95% CI)
.
0.001 0.01 0.1 1 10 100
Study Odds ratio (95% CI)
Number of events Treatment Control
1.29 (0.80, 2.09) EPIC 24/696 62/1,403 0.32 (0.01, 8.24) 1/30 0/30 1.52 (0.49, 4.74) EPILOG 4/939 12/1,853 2.94 (0.12, 73.92) Galassi 0/52 1/54 0.29 (0.01, 7.51) Chen 1/20 0/22 2.36 (0.71, 7.85) ADMIRAL 4/151 9/149 2.10 (1.22, 3.60) CADILLAC 20/1,030 42/1,052 3.00 (0.12, 75.31) Tamburino 0/53 1/54
1.61 (1.17, 2.22) Overall (95% CI)
EUR CO-OP
Heterogeneity chi-squared=5.77 (d.f.=9) p=0.763 I-squared (variation in OR attributable to heterogeneity)=0.0%
Heterogeneity chi-squared=4.42 (d.f.=7) p=0.731 I-squared (variation in OR attributable to heterogeneity)=0.0%

15
5.3.2 Eptifibatide
The results from the trials on eptifibatide are shown in Appendix 9 Tables 1 to 4. The data show that the use of eptifibatide is not associated with a statistically significant reduction in the risk of death or revascularization at 30 days, six months or one year. It is associated, however, with a statistically significant reduction in the risk of MI at seven days and six months (Appendix 9, Table 5).
5.3.3 Tirofiban
The results from the trials on tirofiban are shown in Appendix 10 Tables 1 to 2. The data show that the use of tirofiban is not associated with a statistically significant reduction in the risk of death or MI. It significantly reduces the need for revascularization at seven days. The effects of tirofiban on major clinical outcomes are summarized in Appendix 10, Table 3. 5.3.4 Abciximab, eptifibatide and tirofiban
The effects of glycoprotein antagonists as a class (abciximab, eptifibatide or tirofiban) are shown in Figures 11 to 22. The pooled estimates represent the effect of GPIIB/IIIIa antagonists when all comparators are used. a) Death The use of GP IIb/IIIa antagonists is associated with a statistically significant 28% reduction of death at 30 days (Figure 11). There was a 30%, 15% and 20% reduction in the odds of death at seven days, 30 days and one year respectively. These results are not statistically significant.
Figure 11: Effect of abciximab, eptifibatide or tirofiban on death at 30 days
Heterogeneity chi-squared=5.81 (d.f.=15) p=0.983 I-squared (variation in OR attributable to heterogeneity)=0.0%
.
0.001 0.01 0.1 1 10 100
Study
Odds ratio (95% CI)
Number of events Treatment Control
0.87 (0.42, 1.77) EPIC 12/696 21/1,403 0.48 (0.03, 7.84) IMPACT 1/49 1/101 0.75 (0.26, 2.18) CAPTURE 8/635 6/630 0.50 (0.18, 1.44) EPILOG 7/939 7/1,853 0.59 (0.30, 1.18) IMPACT-II 15/1,328 18/2,682 1.13 (0.43, 2.93) RESTORE 8/1,070 9/1,071 0.81 (0.27, 2.49) EPISTENT 5/809 8/1,590 1.21 (0.36, 4.02) RAPPORT 5/242 6/241 0.31 (0.01, 7.91) Galassi 1/52 0/54 0.43 (0.13, 1.42) ISAR-2 9/200 4/201 0.49 (0.16, 1.47) ADMIRAL 10/151 5/149 0.66 (0.18, 2.33) ESPRIT 6/1,024 4/1,040 0.81 (0.45, 1.48) CADILLAC 24/1,030 20/1,052 2.01 (0.08, 49.44) Juergens 0/358 1/536 0.24 (0.03, 2.22) Petronio 4/45 1/44 1.00 (0.20, 4.97) ISAR-REACT 3/1,080 3/1,079
0.72 (0.56, 0.94) Overall (95% CI)

16
b) Myocardial Infarction (MI) The effects of abciximab, eptifibatide and tirofiban on MI are shown in Figures 12 to 14. The overall estimates show a statistically significant 41%, 37% and 35% reduction in the odds of MI at seven days, 30 days and six months respectively.
Figure 12: Effect of abciximab, eptifibatide or tirofiban on MI at seven days
Figure 13: Effect of abciximab, eptifibatide or tirofiban on MI at 30 days
.
0.001 0.01 0.1 1 10 100
Study
Odds ratio (95% CI)
Number of events Treatment Control
0.64 (0.45, 0.91) EPIC 60/696 80/1,403 0.97 (0.09, 10.96) IMPACT 1/49 2/101 0.48 (0.30, 0.78) CAPTURE 52/635 26/630 0.41 (0.29, 0.57) EPILOG 81/939 69/1,853 0.83 (0.64, 1.06) IMPACT-II 107/1,328 181/2,682 0.73 (0.49, 1.08) RESTORE 61/1,070 45/1,071 0.48 (0.35, 0.67) EPISTENT 78/809 78/1,590 0.80 (0.31, 2.05) RAPPORT 10/242 8/241 0.36 (0.07, 1.95) Galassi 5/52 2/54 0.11 (0.01, 2.30) Chen 3/20 0/22 0.33 (0.03, 3.18) ISAR-2 3/200 1/201 0.50 (0.09, 2.77) ADMIRAL 4/151 2/149 0.61 (0.44, 0.85) ESPRIT 99/1,024 64/1,040 0.87 (0.33, 2.26) CADILLAC 9/1,030 8/1,052 0.92 (0.45, 1.91) Juergens 13/358 18/536 0.33 (0.01, 8.41) Petronio 1/45 0/44 0.98 (0.63, 1.52) ISAR-REACT 41/1,080 40/1,079 0.63 (0.54, 0.74) Overall (95% CI)
.
0.001 0.01 0.1 1 10 100
Study Odds ratio (95% CI)
Number of events Treatment Control
0.22 (0.02, 2.14) EUR CO-OP 4/30 1/30 0.16 (0.01, 1.88) Harrington 2/19 1/54 0.67 (0.44, 1.02) RESTORE 57/1,070 39/1,071 0.49 (0.15, 1.66) RAPPORT 8/242 4/241 0.61 (0.23, 1.58) ERASER 8/71 11/154 0.58 (0.41, 0.81) ESPRIT 92/1,024 56/1,040 0.47 (0.08, 2.69) Tamburino 4/53 2/54
0.59 (0.46, 0.75) Overall (95% CI)
Heterogeneity chi-squared=23.03 (d.f.=16) p=0.113 I-squared (variation in OR attributable to heterogeneity)=30.5%
Heterogeneity chi-squared=2.32 (d.f.=6) p=0.888 I-squared (variation in OR attributable to heterogeneity)=0.0%

17
Figure 14: Effect of abciximab, eptifibatide or tirofiban on MI at six months
Heterogeneity chi-squared=15.81 (d.f.=11) p=0.148 I-squared (variation in OR attributable to heterogeneity)=30.4%
c) Revascularization The effects of abciximab, eptifibatide and tirofiban on revascularization are shown in Figures 15 to 17. The use of GP IIb/IIIa antagonists is associated with a statistically significant reduction in the need for revascularization at seven days, 30 days and 6 months. The overall estimates show a statistically significant 51%, 34% and 14% reduction in the odds of revascularization at seven days, 30 days and six months respectively.
.
0.001 0.01 0.1 1 10 100
Study
Odds ratio (95% CI)
Number of events Treatment Control
0.69 (0.50, 0.94) EPIC 73/696 105/1,403 0.54 (0.36, 0.80) CAPTURE 73/635 41/630 0.49 (0.37, 0.66) EPILOG 93/939 95/1,853 0.81 (0.58, 1.14) RESTORE 81/1,070 67/1,071 0.88 (0.44, 1.78) RAPPORT 18/242 16/241 0.54 (0.40, 0.74) EPISTENT 83/809 93/1,590 0.64 (0.26, 1.56) ERASER 9/71 13/154 0.50 (0.12, 2.02) ADMIRAL 6/151 3/149 0.65 (0.48, 0.89) ESPRIT 106/1,024 73/1,040 1.51 (0.81, 2.80) CADILLAC 17/1,030 26/1,052 0.33 (0.01, 8.41) Petronio 1/45 0/44 0.32 (0.01, 8.06) Tamburino 1/53 0/54
0.65 (0.55, 0.77) Overall (95% CI)

18
Figure 15: Effect of abciximab, eptifibatide or tirofiban on revascularization at seven days
Heterogeneity chi-squared=7.87 (d.f.=5) p=0.164 I-squared (variation in OR attributable to heterogeneity)=36.4%
Figure 16: Effect of abciximab, eptifibatide or tirofiban on revascularization at 30 days
.
0.001 .01 0.1 1 10 100
Study
Odds ratio (95% CI)
Number of events Treatment Control
0.55 (0.38, 0.79) EPIC 56/696 64/1,403 0.13 (0.01, 2.61) EUR CO-OP 3/30 0/30 0.74 (0.52, 1.06) CAPTURE 78/635 59/630 0.37 (0.24, 0.57) EPILOG 48/939 36/1,853 0.81 (0.60, 1.09) IMPACT-II 74/1,328 122/2,682 0.79 (0.56, 1.11) RESTORE 81/1,070 65/1,071 0.74 (0.40, 1.39) EPISTENT 17/809 25/1,590 0.71 (0.40, 1.27) RAPPORT 30/242 22/241 0.15 (0.01, 3.78) ERASER 1/71 0/154 2.86 (0.11, 74.31) Chen 0/20 1/22 0.58 (0.21, 1.64) ISAR-2 10/200 6/201 0.55 (0.25, 1.21) 19/151 11/149 0.82 (0.45, 1.49) ESPRIT 24/1,024 20/1,040 0.54 (0.33, 0.87) CADILLAC 48/1,030 27/1,052 0.38 (0.11, 1.30) Juergens 7/358 4/536 1.43 (0.54, 3.78) ISAR-REACT 7/1,080 10/1,079
0.66 (0.56, 0.77) Overall (95% CI)
.0.001 0.01 0.1 1 10 100
Study
Odds ratio (95% CI)
Number of events Treatment Control
0.06 (0.00, 1.15) EUR CO-OP 6/30 0/30 0.05 (0.01, 0.49) Harrington 5/19 1/54 0.64 (0.43, 0.96) RESTORE 64/1,070 42/1,071 0.66 (0.34, 1.31) RAPPORT 22/242 15/241 0.15 (0.01, 3.78) ERASER 1/71 0/154 0.53 (0.20, 1.45) ESPRIT 11/1,024 6/1,040
0.49 (0.29, 0.84) Overall (95% CI)
ADMIRAL
Heterogeneity chi-squared=18.60 (d.f.=15) p=0.233 I-squared (variation in OR attributable to heterogeneity)=19.3%

19
Figure 17: Effect of abciximab, eptifibatide or tirofiban on revascularization at six months
Heterogeneity chi-squared=6.47 (d.f.=11) p=0.840 I-squared (variation in OR attributable to heterogeneity)=0.0% d) Composite End Point (CEP) The effects of abciximab, eptifibatide and tirofiban on CEP are shown in Figures 18 to 20. The use of GP IIb/IIIa antagonists is associated with a statistically significant reduction in the risk of CEP. The overall estimates show a statistically significant 39%, 36% and 27% reduction in the odds of CEP at seven days, 30 days and six months respectively. The pooled estimates at 30 days and six months, however, were associated with statistical heterogeneity.
.
0.001 0.01 0.1 1 10 100
Study Odds ratio (95% CI)
Number of events Treatment Control
0.78 (0.64, 0.96) EPIC 205/696 346/1,403 0.95 (0.74, 1.23) CAPTURE 171/635 164/630 0.96 (0.78, 1.17) EPILOG 180/939 343/1,853 0.86 (0.70, 1.05) RESTORE 256/1,070 227/1,071 0.93 (0.60, 1.44) RAPPORT 53/242 50/241 0.72 (0.41, 1.27) EPISTENT 21/809 30/1,590 0.91 (0.41, 1.99) ERASER 11/71 22/154 0.68 (0.38, 1.19) ADMIRAL 36/151 26/149 0.90 (0.67, 1.22) ESPRIT 96/1,024 89/1,040 0.76 (0.58, 1.00) CADILLAC 134/1,030 108/1,052 0.33 (0.03, 3.26) Petronio 3/45 1/44 0.48 (0.16, 1.40) Tamburino 11/53 6/54
0.86 (0.78, 0.94) Overall (95% CI)

20
Figure 18: Effect of abciximab, eptifibatide or tirofiban on CEP at seven days
Heterogeneity chi-squared=4.96 (d.f.=5) p=0.420 I-squared (variation in OR attributable to heterogeneity)=0.0%
Figure 19: Effect of abciximab, eptifibatide or tirofiban on CEP at 30 days
Heterogeneity chi-squared=25.78 (d.f.=14) p=0.028 I-squared (variation in OR attributable to heterogeneity)=45.7%
.
0.01 0.1 1 10 100
Study
Odds ratio (95% CI)
Number of events Treatment Control
0.74 (0.56, 0.99) EPIC 89/696 138/1,403 0.53 (0.17, 1.68) IMPACT 6/49 7/101 0.67 (0.48, 0.93) CAPTURE 101/635 71/630 0.42 (0.32, 0.56) EPILOG 109/939 97/1,853 0.82 (0.66, 1.02) IMPACT-II 151/1,328 256/2,682 0.83 (0.63, 1.08) RESTORE 130/1,070 110/1,071 0.54 (0.40, 0.73) EPISTENT 87/809 97/1,590 0.80 (0.48, 1.32) RAPPORT 39/242 32/241 0.21 (0.04, 1.05) Galassi 8/52 2/54 0.57 (0.08, 3.80) Chen 3/20 2/22 0.45 (0.20, 0.97) ISAR-2 21/200 10/201 0.38 (0.17, 0.85) ADMIRAL 22/151 9/149 0.62 (0.45, 0.85) ESPRIT 108/1,024 71/1,040 0.64 (0.44, 0.93) CADILLAC 72/1,030 48/1,052 1.00 (0.50, 2.00) Juergens 14/358 21/536
0.64 (0.56, 0.75) Overall (95% CI)
.
0.001 0.01 0.1 1 10 100
Study
Odds ratio (95% CI)
Number of events Treatment Control
0.07 (0.01, 0.58) EUR CO-OP 10/30 1/30 0.64 (0.47, 0.88) RESTORE 108/1,070 72/1,071 0.64 (0.35, 1.16) RAPPORT 30/242 20/241 0.53 (0.21, 1.34) ERASER 9/71 11/154 0.62 (0.44, 0.86) ESPRIT 95/1,024 62/1,040 0.30 (0.06, 1.57) Tamburino 6/53 2/54
0.61 (0.50, 0.75) Overall (95% CI)

21
Figure 20: Effect of abciximab, eptifibatide or tirofiban on CEP at six months
Heterogeneity chi-squared=29.85 (d.f.=11) p=0.002 I-squared (variation in OR attributable to heterogeneity)=63.2% e) Adverse events Bleeding The effects of abciximab, eptifibatide and tirofiban on minor and major bleeding are calculated. The use of GP IIb/IIIa antagonists is not associated with a statistically significant increase (29%) in the odds of major bleeding but it is associated with a significant 80% increase in the odds of minor bleeding (Figure 21).
.
0.01 0.1 1 10 100
Study
Odds ratio (95% CI)
Number of events Treatment Control
0.79 (0.65, 0.95) EPIC 244/696 418/1,403 1.00 (0.79, 1.27) CAPTURE 196/635 195/630 0.53 (0.41, 0.67) EPILOG 138/939 154/1,853 0.88 (0.72, 1.07) RESTORE 279/1,070 254/1,071 1.01 (0.68, 1.50) RAPPORT 68/242 68/241 0.61 (0.46, 0.81) EPISTENT 98/809 124/1,590 0.80 (0.42, 1.55) ERASER 18/71 33/154 0.42 (0.20, 0.90) ADMIRAL 24/151 11/149 0.74 (0.59, 0.94) ESPRIT 187/1,024 148/1,040 0.82 (0.64, 1.04) CADILLAC 163/1,030 140/1,052 0.21 (0.07, 0.64) Petronio 17/45 5/44 0.38 (0.13, 1.10) Tamburino 13/53 6/54
0.73 (0.63, 0.86) Overall (95% CI)

22
Figure 21: Effect of abciximab, eptifibatide or tirofiban on minor bleeding
Thrombocytopenia The effects of abciximab, eptifibatide and tirofiban on the rates of thrombocytopenia (platelets count<100,000/mm3) are shown in Figure 22. The use of GP IIb/IIIa antagonists is associated with a statistically significant 41% increase in the odds of thrombocytopenia.
Figure 22: Effect of abciximab, eptifibatide or tirofiban on thrombocytopenia
.
0.001 0.01 0.1 1 10 100
Study
Odds ratio (95% CI)
Number of events Treatment Control
0.32 (0.01, 8.24) EUR CO-OP 1/30 0/30 3.93 (1.61, 9.62) IMPACT 7/49 40/101 2.39 (1.24, 4.63) CAPTURE 13/635 30/630 1.55 (1.05, 2.29) EPILOG 35/939 105/1,853 1.69 (0.92, 3.10) EPISTENT 14/809 46/1,590 1.45 (0.96, 2.18) RAPPORT 55/242 72/241 1.96 (0.17, 22.31) Galassi 1/52 2/54 1.42 (0.21, 9.52) Chen 2/20 3/22 4.01 (1.45, 11.11) ADMIRAL 5/151 18/149 1.60 (0.88, 2.91) ESPRIT 18/1,024 29/1,040 5.12 (1.16, 22.55) Juergens 2/358 15/536 2.21 (0.52, 9.46) Petronio 3/45 6/44 2.00 (0.18, 22.74) Tamburino 1/53 2/54
1.80 (1.47, 2.21) Overall (95% CI)
.
0.001 0.01 0.1 1 10 100
Study Odds ratio (95% CI)
Number of events Treatment Control
1.29 (0.80, 2.09) EPIC 24/696 62/1,403 0.32 (0.01, 8.24) EUR CO-OP 1/30 0/30
3.52 (0.18, 69.45) IMPACT 0/49 3/101 1.52 (0.49, 4.74) EPILOG 4/939 12/1,853 1.12 (0.75, 1.68) IMPACT-II 35/1,328 79/2,682 2.00 (0.18, 22.09) RESTORE 1/1,070 2/1,071 2.94 (0.12, 73.92) Galassi 0/52 1/54 0.29 (0.01, 7.51) Chen 1/20 0/22 2.36 (0.71, 7.85) ADMIRAL 4/151 9/149 2.10 (1.22, 3.60) 20/1,030 42/1,052 3.00 (0.12, 75.31) Tamburino 0/53 1/54
1.41 (1.10, 1.81) Overall (95% CI)
CADILLAC
Heterogeneity chi-squared=6.74 (d.f.=10) p=0.749 I-squared (variation in OR attributable to heterogeneity)=0.0%
Heterogeneity chi-squared=11.04 (d.f.=12) p=0.525 I-squared (variation in OR attributable to heterogeneity)=0.0%

23
5.3.5 Abciximab versus eptifibatide and abciximab versus tirofiban
The results from head-to-head trials are shown in Appendix 11 Tables 1 to 4. There are four direct comparative randomized trials: TARGET (comparing abciximab to tirofiban), PRICE (comparing abciximab to eptifibatide), TEAM (comparing abciximab to eptifibatide and tirofiban) and COMPARE (comparing abciximab to eptifibatide and tirofiban). There is no observed difference in mortality between the agents in these trials. In TEAM, the incidence of MI is found to be lower with abciximab than with tirofiban. These trials, however, include a small number of patients and are underpowered.
5.3.6 Summary of findings
The findings on the statistically significant effects of abciximab, eptifibatide or tirofiban on major clinical outcomes are summarized in Appendix 12 Table 1.
6 DISCUSSION The effect of abciximab, eptifibatide and tirofiban on PCI outcomes has been studied in 25 randomized clinical trials, including 15 trials of abciximab, four of eptifibatide, two of tirofiban and four head-to-head trials, with a total of 29,323 patients. Do GP IIb/IIIa antagonists work? When considered as a class, the aggregate effect of abciximab, eptifibatide and tirofiban results in a statistically significant 28% reduction [OR 0.72; 95% CI (0.56 to 0.94)] in the odds of death at 30 days and a non-significant 15% reduction [OR 0.85; 95% CI (0.68 to 1.07)] at six months. At one year, abciximab and eptifibatide are associated with a non-significant 20% reduction [OR 0.80; 95% CI (0.64 to 1.0)] in the odds of mortality. This effect translates into six fewer deaths at one year per 1,000 patients treated. As a result, GP IIb/IIIa inhibitors provide a survival benefit in patients undergoing a PCI. Most of the data on mortality in this meta-analysis are derived from trials with abciximab. While a previous meta-analysis29 suggests that there is a long-term mortality benefit with abciximab, our meta-analysis does not show a statistically significant reduction in mortality when trials with only abciximab are included. There are no one-year data available with tirofiban. Therefore, extrapolation of the results to this agent and calculation of a class effect cannot be done. The ESPRIT trial shows no statistically significant reduction at one year with eptifibatide. The effect of abciximab on reducing MI is more profound. At 30 days, there is a 37% reduction in the odds of MI [OR 0.63; 95% CI (0.54 to 0.74)], which is maintained at six months [OR 0.65; 95% CI (0.55 to 0.77)]. These results translate into 19 fewer MIs at 30 days per 1,000 patients treated. Do GP IIb/IIIa antagonists cause harm? The use of these agents is associated with an increase in major [OR 1.29; 95% CI (0.98 to 1.68)] and minor [OR 1.80; 95% CI (1.47 to 2.21)] bleeding. The 80% increase in the odds of minor bleeding is statistically significant, while the increase in major bleeding is not.

24
Do different glycoprotein antagonists produce clinically significant different results? In comparison to the low molecular weight glycoprotein antagonists eptifibatide and tirofiban, abciximab has a longer action at the platelet site. Whether this translates to meaningful differences in clinical outcomes has been addressed in four direct comparative randomized trials: TARGET, PRICE, TEAM and COMPARE. Although the results of this systematic review suggest that there is a class effect, no difference in mortality between the agents is observed in any trial. The overall event rate, however, is low and the trials are underpowered to detect a difference in mortality. In one trial, the incidence of MI is lower with abciximab compared with tirofiban. The trials comparing eptifibatide to abciximab or to tirofiban do not detect any difference in clinical outcomes, but they involve a small number of patients and are underpowered. When the trials of abciximab are compared with the trials of eptifibatide or of tirofiban, the outcomes attributable to each agent do not generally differ. While the magnitude of reduction in mortality associated with eptifibatide and tirofiban is comparable to that of abciximab, the confidence intervals associated with eptifibatide and tirofiban are wider. Particular benefits of certain agents are suggested in specific subsets such as patients with diabetes mellitus, but no prospective randomized trials have been conducted to confirm the findings of these retrospective analyses. Limitations: Quality of Analysis and Confidence in Results In interpreting the results of this meta-analysis, several limitations must be noted. • Patient inclusion and exclusion criteria vary between trials. For example, some trials
include patients with acute evolving MI, while other trials only include lower risk patients undergoing a non-urgent PCI.
• The dosing regimens of the GP IIb/IIIa inhibitors vary over time. In the EPIC trial, abciximab is given as a bolus in one arm of the trial and a bolus followed by a 12-hour infusion in the other arm. Only the bolus and 12-hour infusion regimen is used in all subsequent trials with abciximab. The dosage of heparin varies in the abciximab arms and the control arms in several trials with abciximab. The same limitation with respect to dosing regimens applies to eptifibatide. In IMPACT-II, the lower doses of eptifibatide used may have been insufficient to provide adequate platelet inhibition and may explain the lack of measurable efficacy.
• The techniques used in PCIs have evolved over the period of this meta-analysis. Initially, balloon angioplasty was the predominant technique. Coronary stent implantation is now used for most patients. Recently, drug eluting stents have been used, but no trials with GP IIb/IIIa inhibitors have been performed.
Our results must be interpreted in light of the quality of the included randomized trials. While the quality scores rank high for the included trials (median Jadad score of 4/5), there are variations in the definitions of outcomes, the types of patients included and the concomitant treatments provided. Some patients were receiving other cardioprotective agents at baseline [i.e., acetylsalicylic acid (ASA), thienopyridines, angiotensin converting enzyme inhibitors, beta-blockers or statins], but these concomitant therapies are not standardized. Recent evidence suggests that patients receiving optimal platelet inhibition

25
with clopidogrel will not benefit further from GP IIb/IIIa antagonists.28 The co-administration of heparin also varies across trials. Sub-analysis by heparin dose is impossible to do in this analysis, but further study of the optimal concomitant dose of heparin is required. Because of the above reasons, data analysis is done in two ways. Outcome data are pooled using matched comparators and all comparators. Appendix 12 Table 2 compares the overall effect of abciximab on different outcomes from using matched comparators or all comparators. The comparison shows that the effect of abciximab, when only matched comparators are used, is lightly but consistently greater than when all comparators are used, except for the outcomes of death at 30 days. This may reflect the fact that, in many trials, the control arm is composed of a placebo plus high dose heparin, while the treatment arm is composed of a GP IIb/IIIa antagonist plus low dose heparin. The difference in heparin dosage may have reduced the effect of the GP IIb/IIIa antagonists when this group is compared with the control arm. This emphasizes the importance to clinical investigators of keeping the concomitant therapies in the control and treatment arms as similar as possible, to determine the precise effect of the drug under study. To obtain accuracy in meta-analyses, it is important to separate the analyses according to concomitant therapies to determine an objective estimate effect of treatment. Applicability of Results to Current Canadian Practice The trials that are included in this review were published between 1994 to 2004. Therefore, practice changes over the past decade may affect the results. In the earlier trials of higher risk patients (where most of the benefit has been shown), the patients were less likely to be receiving other antiplatelets and were less likely to be stented. Since both these factors have been shown to improve outcomes, the results of earlier trials may be less applicable to the current population. Furthermore, whether drug eluting stents would affect the results remains to be studied. As there is a significant increase in the odds of minor bleeding associated with the use of GP IIb/IIIa antagonists, physicians should pay attention to the balance between the benefits of reduced cardiovascular events and the risk of increased complications. The lack of definitive superiority data for one agent over the other has resulted in variability in the selection of agents. An individual physician’s interpretation of the data on subgroups, his or her familiarity with the agent, its cost and the presence of renal failure have all played varying roles in determining which agent is used during a PCI.

26
7 CONCLUSIONS A total of 25 RCTs of the use of glycoprotein antagonists involving 29,323 patients, have been reviewed, including 14 trials of abciximab, four of eptifibatide, two of tirofiban and four head-to-head trials. GP IIb/IIIa inhibitors as a class significantly reduce MI and the need for revascularization at seven days, 30 days and six months in patients undergoing a PCI. Significant reductions in mortality were detected only at 30 days. Most of the evidence is derived from trials on abciximab, the most widely studied agent. The small-molecule agents (eptifibatide and tirofiban) are not associated with any significant reduction in the risk of death. Small trials have failed to show the superiority of the small-molecule agents over abciximab. The beneficial effect of GP IIb/IIIa inhibitors is tempered by a significant increase in minor bleeding.

27
8 REFERENCES
1. Heart and Stroke Foundation of Canada. The changing face of heart disease and stroke in Canada 2000. Ottawa: The Foundation; 1999. Available: http://www.hc-sc.gc.ca/hpb/lcdc/bcrdd/hdsc2000/pdf/card2ke.pdf (accessed 2004 Aug 4).
2. Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving the quality of reports of meta-analyses of randomised controlled trials: the QUOROM statement. Quality of Reporting of Meta-analyses. Lancet 1999;354(9193):1896-900.
3. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 1996;17(1):1-12.
4. ERASER Investigators. Acute platelet inhibition with abciximab does not reduce in-stent restenosis (ERASER study). Circulation 1999;100(8):799-806.
5. Randomised placebo-controlled trial of abciximab before and during coronary intervention in refractory unstable angina: the CAPTURE Study. Lancet 1997;349(9063):1429-35.
6. Montalescot G, Barragan P, Wittenberg O, Ecollan P, Elhadad S, Villain P, et al. Platelet glycoprotein IIb/IIIa inhibition with coronary stenting for acute myocardial infarction. N Engl J Med 2001;344(25):1895-903.
7. PRICE Investigators. Comparative 30-day economic and clinical outcomes of platelet glycoprotein IIb/IIIa inhibitor use during elective percutaneous coronary intervention: Prairie ReoPro versus Integrilin Cost Evaluation (PRICE) Trial. Am Heart J 2001;141(3):402-9.
8. Neumann FJ, Kastrati A, Schmitt C, Blasini R, Hadamitzky M, Mehilli J, et al. Effect of glycoprotein IIb/IIIa receptor blockade with abciximab on clinical and angiographic restenosis rate after the placement of coronary stents following acute myocardial infarction. J Am Coll Cardiol 2000;35(4):915-21.
9. Brener SJ, Barr LA, Burchenal JE, Katz S, George BS, Jones AA, et al. Randomized, placebo-controlled trial of platelet glycoprotein IIb/IIIa blockade with primary angioplasty for acute myocardial infarction. Circulation 1998;98(8):734-41. Available: http://circ.ahajournals.org/cgi/reprint/98/8/734.pdf.
10. EPISTENT Investigators (Evaluation of Platelet IIb/IIIa Inhibitor for Stenting). Randomised placebo-controlled and balloon-angioplasty-controlled trial to assess safety of coronary stenting with use of platelet glycoprotein-IIb/IIIa blockade. Lancet 1998;352(9122):87-92.
11. RESTORE Investigators (Randomized Efficacy Study of Tirofiban for Outcomes and REstenosis). Effects of platelet glycoprotein IIb/IIIa blockade with tirofiban on adverse cardiac events in patients with unstable angina or acute myocardial infarction undergoing coronary angioplasty. Circulation 1997;96(5):1445-53. Available: http://circ.ahajournals.org/cgi/content/full/96/5/1445.
12. EPILOG Investigators. Platelet glycoprotein IIb/IIIa receptor blockade and low-dose heparin during percutaneous coronary revascularization. N Engl J Med 1997;336(24):1689-96.
13. IMPACT-II Investigators. Integrilin (eptifibatide) to Minimize Platelet Aggregation and Coronary Thrombosis-II. Randomised placebo-controlled trial of effect of eptifibatide on complications of percutaneous coronary intervention: IMPACT-II. Lancet 1997;349(9063):1422-8.

28
14. Simoons ML, de Boer MJ, van den Brand MJ, van Miltenburg AJ, Hoorntje JC, Heyndrickx GR, et al. Randomized trial of a GPIIb/IIIa platelet receptor blocker in refractory unstable angina. Circulation 1994;89(2):596-603.
15. O'Shea JC, Hafley GE, Greenberg S, Hasselblad V, Lorenz TJ, Kitt MM, et al. Platelet glycoprotein IIb/IIIa integrin blockade with eptifibatide in coronary stent intervention: the ESPRIT trial: a randomized controlled trial. JAMA 2001;285(19):2468-73.
16. EPIC Investigators. Use of a monoclonal antibody directed against the platelet glycoprotein IIb/IIIa receptor in high-risk coronary angioplasty. N Engl J Med 1994;330(14):956-61.
17. Tcheng JE, Harrington RA, Kottke-Marchant K, Kleiman NS, Ellis SG, Kereiakes DJ, et al. Multicenter, randomized, double-blind, placebo-controlled trial of the platelet integrin glycoprotein IIb/IIIa blocker Integrelin in elective coronary intervention. IMPACT Investigators. Circulation 1995;91(8):2151-7.
18. Galassi AR, Russo G, Nicosia A, Tamburino C, Foti R, Rodi G, et al. Usefulness of platelet glycoprotein IIb/IIIa inhibitors in coronary stenting for reconstruction of complex lesions: procedural and 30 day outcome. Cardiologia 1999;44(7):639-45.
19. Harrington RA, Kleiman NS, Kottke-Marchant K, Lincoff AM, Tcheng JE, Sigmon KN, et al. Immediate and reversible platelet inhibition after intravenous administration of a peptide glycoprotein IIb/IIIa inhibitor during percutaneous coronary intervention. Am J Cardiol 1995;76(17):1222-7.
20. Chen YH, Chen JW, Wu TC, Ding PY, Wang SP, Chang MS. Safety and efficacy of the platelet glycoprotein IIb/IIIa inhibitor abciximab in Chinese patients undergoing high-risk angioplasty. Chin Med J (Taipei) 2000;63(1):8-15.
21. Petronio AS, Musumeci G, Limbruno U, De Carlo M, Baglini R, Paterni G, et al. Abciximab improves 6-month clinical outcome after rescue coronary angioplasty. Am Heart J 2002;143(2):334-41.
22. Stone GW, Grines CL, Cox DA, Garcia E, Tcheng JE, Griffin JJ, et al. Comparison of angioplasty with stenting, with or without abciximab, in acute myocardial infarction. N Engl J Med 2002;346(13):957-66.
23. Tamburino C, Russo G, Nicosia A, Galassi AR, Foti R, Scriffignano V, et al. Prophylactic abciximab in elective coronary stenting: results of a randomized trial. J Invasive Cardiol 2002;14(2):72-9.
24. Batchelor WB, Tolleson TR, Huang Y, Larsen RL, Mantell RM, Dillard P, et al. Randomized COMparison of Platelet Inhibition With Abciximab, TiRofiban and Eptifibatide During Percutaneous Coronary Intervention in Acute Coronary Syndromes: the COMPARE Trial. Comparison of measurements of platelet aggregation with Aggrastat, Reopro and Eptifibatide. Circulation 2002;106(12):1470-6.
25. Kini AS, Richard M, Suleman J, Perez N, Lee P, Fisher EA, et al. Effectiveness of tirofiban, eptifibatide, and abciximab in minimizing myocardial necrosis during percutaneous coronary intervention (TEAM pilot study). Am J Cardiol 2002;90(5):526-9.
26. Juergens CP, White HD, Belardi JA, Macaya C, Soler-Soler J, Meyer BJ, et al. A multicenter study of the tolerability of tirofiban versus placebo in patients undergoing planned intracoronary stent placement. Clin Ther 2002;24(8):1332-44.
27. Topol EJ, Moliterno DJ, Herrmann HC, Powers ER, Grines CL, Cohen DJ, et al. Comparison of two platelet glycoprotein IIb/IIIa inhibitors, tirofiban and abciximab, for the prevention of ischemic events with percutaneous coronary revascularization. N Engl J Med 2001;344(25):1888-94.

29
28. Kastrati A, Mehilli J, Schühlen H, Dirschinger J, Dotzer F, ten Berg JM, et al. A clinical trial of abciximab in elective percutaneous coronary intervention after pretreatment with clopidogrel. N Engl J Med 2004;350(3):232-8.
29. Anderson KM, Califf RM, Stone GW, Neumann FJ, Montalescot G, Miller DP, et al. Long-term mortality benefit with abciximab in patients undergoing percutaneous coronary intervention. J Am Coll Cardiol 2001;37(8):2059-65.
30. Scarborough RM. Eptifibatide. Platelet antiaggregatory, glycoprotein IIb/IIIa antagonist, fibrinogen receptor antagonist. Drugs Future 1998;23(6):585-90.
31. Tcheng JE, Kandzari DE, Grines CL, Cox DA, Effron MB, Garcia E, et al. Benefits and risks of abciximab use in primary angioplasty for acute myocardial infarction: the Controlled Abciximab and Device Investigation to Lower Late Angioplasty Complications (CADILLAC) trial. Circulation 2003;108(11):1316-23.
32. Topol EJ. Prevention of cardiovascular ischemic complications with new platelet glycoprotein IIb/IIIa inhibitors. Am Heart J 1995;130(3 Pt 2):666-72.
33. Topol EJ, Ferguson JJ, Weisman HF, Tcheng JE, Ellis SG, Kleiman NS, et al. Long-term protection from myocardial ischemic events in a randomized trial of brief integrin beta3 blockade with percutaneous coronary intervention. EPIC Investigator Group. Evaluation of Platelet IIb/IIIa Inhibition for Prevention of Ischemic Complication. JAMA 1997;278(6):479-84.
34. Topol EJ, Lincoff AM, Kereiakes DJ, Kleiman NS, Cohen EA, Ferguson JJ, et al. Multi-year follow-up of abciximab therapy in three randomized, placebo-controlled trials of percutaneous coronary revascularization. Am J Med 2002;113(1):1-6.
35. Kereiakes DJ, Lincoff AM, Miller DP, Tcheng JE, Cabot CF, Anderson KM, et al. Abciximab therapy and unplanned coronary stent deployment: favorable effects on stent use, clinical outcomes, and bleeding complications. EPILOG Trial Investigators. Circulation 1998;97(9):857-64. Available: http://circ.ahajournals.org/cgi/reprint/97/9/857.pdf.
36. Lincoff AM, Tcheng JE, Califf RM, Kereiakes DJ, Kelly TA, Timmis GC, et al. Sustained suppression of ischemic complications of coronary intervention by platelet GP IIb/IIIa blockade with abciximab: one-year outcome in the EPILOG trial. Circulation 1999;99(15):1951-8. Available: http://circ.ahajournals.org/cgi/reprint/99/15/1951.pdf.
37. Topol EJ, Mark DB, Lincoff AM, Cohen E, Burton J, Kleiman N, et al. Outcomes at 1 year and economic implications of platelet glycoprotein IIb/IIIa blockade in patients undergoing coronary stenting: results from a multicentre randomised trial. Lancet 1999;354(9195):2019-24.
38. Lincoff AM, Califf RM, Moliterno DJ, Ellis SG, Ducas J, Kramer JH, et al. Complementary clinical benefits of coronary-artery stenting and blockade of platelet glycoprotein IIb/IIIa receptors. N Engl J Med 1999;341(5):319-27.
39. Labinaz M, Madan M, O'Shea JO, Kilaru R, Chin W, Pieper K, et al. Comparison of one-year outcomes following coronary artery stenting in diabetic versus nondiabetic patients (from the Enhanced Suppression of the Platelet IIb/IIIa Receptor With Integrilin Therapy [ESPRIT] Trial). Am J Cardiol 2002;90(6):585-90.
40. Gibson CM, Goel M, Cohen DJ, Piana RN, Deckelbaum LI, Harris KE, et al. Six-month angiographic and clinical follow-up of patients prospectively randomized to receive either tirofiban or placebo during angioplasty in the RESTORE trial. J Am Coll Cardiol 1998;32(1):28-34.

30
41. Moliterno DJ, Topol EJ, TARGET International Steering Committee. A direct comparison of tirofiban and abciximab during percutaneous coronary revascularization and stent placement: rationale and design of the TARGET study. Am Heart J 2000;140(5):722-6.
42. Moliterno DJ, Yakubov SJ, DiBattiste PM, Herrmann HC, Stone GW, Macaya C, et al. Outcomes at 6 months for the direct comparison of tirofiban and abciximab during percutaneous coronary revascularisation with stent placement: the TARGET follow-up study. Lancet 2002;360(9330):355-60.

31
Appendix 1: Literature Search Strategies Legend: Search Syntax ! Explode the search term. Retrieve the search concept plus all narrower related terms. exp Explode the search term. Retrieve the search concept plus all narrower related terms. ? Truncation symbol, one character. $ Truncation symbol, any number of characters. * Truncation symbol, any number of characters. adj Proximity operator. Words must be adjacent. adj# Proximity operator. Words must be adjacent within specified number. () Proximity operator. Words must be adjacent. (n) Proximity operator (terms are near to each other, in any order). (#n) Proximity operators (terms are near each other within specified number of words). near Proximity operator (terms are near each other in any order). Next Proximity operator. Words must be adjacent. ti Search in record title. ab Search in record abstract. de Descriptor i.e subject heading (a controlled thesaurus term). / Descriptor i.e subject heading (a controlled thesaurus term). ME Medical subject heading. tw Text word. rn Registry number. mp Major headings including title, keywords, subject headings, abstract, heading word, registry number. “ “ Search phrases. MeSH Medical subject heading. pt Publication type. Databases Ovid Technologies, Inc: MEDLINE® HealthSTAR EMBASE® BIOSIS Previews® Current Contents® DIALOG® Alerts: MEDLINE® EMBASE® BIOSIS Previews® Search and updates on PubMed and the Cochrane Library (CD-ROM, 2001,2002, 2003, 2004) Web sites of HTA and related agencies, trial registers and other databases were searched for grey literature.
For eg: NICE, AHRQ; University of York NHS Centre for Reviews and Dissemination – CRD database; LILACS; National Research Register; CMA Infobase;
Multiple-file Search on OVID Technologies
1. exp platelet glycoprotein gpiib-iiia complex/ [MEDLINE]
2. exp glycoprotein iib/ OR glycoprotein iiia/ [EMBASE]
3. abiciximab/ or eptifibatide/ or tirofiban/ [BIOSIS, EMBASE]
4. (abciximab or reopro).mp. 5. (eptifibatide or integrilin or intigrilin).mp. 6. (gpiib$ or gp2b$ or glycoproteiniib$ or
glycoprotein2b$).mp. 7. 143653-53-6.rn. or 144494-65-5.rn. or
188627-80-7.rn. 8. (tirofiban or abciximab or eptifibatide or
reopro or aggrastat or integrelin or integrilin).tw,mp.
9. ((gp or glycoprotein) adj iib).mp. 10. or/1-9 11. exp myocardial ischemia/ or angina,
unstable/ or exp coronary disease/ or myocardial infarction/ [MEDLINE]
12. unstable angina pectoris/ or exp heart infarction/ or exp heart muscle ischemia/ or

32
restenosis/ or exp coronary artery disease/ [EMBASE]
13. myocardial ischemia/ or heart attack/ or heart failure/ [BIOSIS]
14. coronary atherosclerosis/ or coronary restenosis/ or unstable angina/ or unstable angina pectoris/ [BIOSIS ]
15. unstable angina.mp, tw.or restenosis.mp or heart adj3 attack$.mp,tw or coronary disease$.mp,tw. or myocardial infarct$
16. or/11-15 17. exp angioplasty, transluminal, percutaneous
coronary/ [MEDLINE] 18. exp stents/ [MEDLINE] and coronary.mp. 19. percutaneous transluminal angioplasty/ or
coronary stent/ [EMBASE] 20. percutaneous transluminal coronary
angioplasty/ or coronary stenting/ or coronary stent/ [BIOSIS]
21. ((pci or percutaneous adj coronary adj intervention$).mp, tw.
22. ((balloon adj angioplast$).mp, tw. 23. PTCA.mp. 24. percutaneous transluminal coronary
angioplast$.mp,tw. 25. exp atherectomy, coronary/ 26. (coronary adj atherectomy).mp,tw. 27. (directional or rotational or extraction).mp,
tw. 28. ((24 or 25 or 26) and 27) 29. (transluminal adj extraction
atherectomy).mp. 30. (transluminal adj extraction adj
catheter$).mp. 31. or/17-23, 28-30 32. 16 and 31 33. 32 and 10 34. exp meta analysis/ or exp clinical trial/ or
placebo/ major clinical study/ or exp controlled study/ or crossover procedure/ or exp comparative study/ or exp evidence based medicine/ [EMBASE]
35. meta-analysis/ or clinical trial/ or placebo/ or randomized clinical trial/ or randomized controlled trial/ or comparative study/ or evidence-based medicine/ [BIOSIS]
36. exp clinical trials/ or meta analysis/ or comparative study/ or evidence based medicine/ or cross-over studies/ or meta-analysis.pt. or controlled clinical trial.pt.or randomized controlled trial.pt. or exp epidemiologic research design/ [MEDLINE]
37. (meta analysis or metaanal$ or meta analy$).mp.tw.
38. crossover$.mp,tw. or cross-over$.mp,tw.
39. controlled clinical trial$.tw,mp. 40. (research adj2(integrati$ or
overview)).tw,mp. 41. (quantitative adj2 (review$ or overview$ or
synthes?s)).tw,mp. 42. ((methodologic or systematic or
collaborative) adj2 (review$ or overview$)).tw,mp.
43. (multicent$ adj stud$).tw,mp. 44. (multicent$ adj trial$).tw,mp. 45. comparative adj stud$.tw,mp. 46. ((singl$ or doubl$ or treble$ or tripl$) adj5
(blind$ or mask$ or dumm$) 47. (placebo$ or prospectiv$ or random$ or
rct$).mp,tw. 48. or/34-47 49. 33 and 48 50. human$ or people or person$.tw.mp 51. 49 and 50 52. remove duplicates from 51 Total hits 781 records Medline 126 records Embase 644 records Biosis Previews 6 records HealthSTAR 3 records Current Contents 2 records
Search performed 14 November 2001.
DIALOG® Alerts
Bi-weekly alerts were set up for MEDLINE®, EMBASE®, BIOSIS Previews® on the DIALOG® system until April 2004.
1. Platelet glycoprotein gpiib-iiia complex/de or glycoprotein iib/ or glycoprotein iiia/
2. abiciximab/de or eptifibatide/de or tirofiban/ de
3. RN=143653-53-6 OR RN=144494-65-5 OR RN=188627-80-7
4. abciximab/ti,ab or reopro/ti,ab or aggrastat/ti,ab or integrilin/ti,ab or integrelin/ti,ab
5. (gpiib?/ti,ab or gp2b? or glycoproteiniib? or glycoprotein2b?)/ti,ab
6. tirofiban/ti,ab or aggrastat/ti,ab or eptifibatide/ti,ab
7. (gp(1n)iib? or glycoprotein(1n)iib? or gp(1n)2b? or glycoprotein(1n)2b?)/ti,ab
8. S1:S7 (adds sets together) 9. angina, unstable/de or coronary disease!/de
or myocardial infarction!/de 10. myocardial ischemia!/de or heart attack/de
or heart failure/de or coronary restenosis/de

33
or unstable angina/de or unstable angina pectoris/de
11. coronary()restenosis/ti,ab or unstable()angina/ti,ab
12. S9:S11 (adds sets together) 13. angioplasty, transluminal, percutaneous
coronary/de 14. percutaneous transluminal coronary
angioplasty/de or coronary stenting/de or coronary stent/de or percutaneous transluminal angioplasty/de
15. (pci or coronary()intervention? or coronary()angioplast?)/ti,ab
16. atherectomy, coronary!/de 17. transluminal()extraction()atherectom?/ti,ab 18. transluminal()extraction()catheter?/ti,ab 19. stents!/de and coronary 20. s13:s19 (adds sets together) 21. meta-analysis/de or clinical trial!/de or
placebo/de or randomized clinical trial/de or comparative study/de or randomized controlled trial/de or evidence-based medicine/de
22. clinical trials!/de or evidence based medicine/de or epidemiologic research design!/de or dt=meta-analysis or dt=controlled clinical trial or dt=randomized controlled trial
23. (meta(1n)analy? or metaanaly? or meta()analy?)/ti,ab
24. (crossover? or cross-over?)/ti,ab 25. ((singl? or doub? or trebl? or
tripl?)(5n)(blind? or mask? or dumm?))/ti,ab 26. (placebo? or prospectiv? or random? or
rct?)/ti,ab 27. s21:s26 (adds sets together) 28. human? or people? or person? 29. s8 and s12 and s20 and s27 and s28
The Cochrane Library (2001, 2002, 2003, 2004) The numerical drug qualifiers were not used for the Cochrane search as they are ignored by the software used by the Cochrane Library. Human limit applied.
1. Platelet Glycoprotein GPIIB-IIIA Complex:ME
2. (abciximab or integrilin or integrelin or tirofiban or aggrastat or glycoprotein*)
3. (gpiib or glycoproteiniib*) 4. (glycoprotein next iib*) or (gp next iib*) 5. (#1 or #2 or #3 or #4) 6. MYOCARDIAL ISCHEMIA explode tree 1
(MeSH) 7. ANGINA UNSTABLE explode tree 1
(MeSH) 8. (myocardi* next infarct*)
9. (heart next attack*) 10. ((coronary next disease*) or (coronary next
syndrome*)) 11. (unstable next angina) 12. (#6 or #7 or #8 or #9 or #10 or #11 or #11) 13. (#5 and #12) 14. ATHERECTOMY CORONARY single
term (MeSH) 15. CATHETER ABLATION single term
(MeSH) 16. ANGIOPLASTY TRANSLUMINAL
PERCUTANEOUS CORONARY single term (MeSH)
17. MYOCARDIAL REVASCULARIZATION explode tree 2 (MeSH)
18. STENTS single term (MeSH) and coronary
19. ( ((percutaneous next coronary next intervention*) or (percutaneous next transluminal next coronary next angioplasty) or ptca or pci or (balloon next angioplast*))
20. (#15 or #16 or #17 or #18 or #19) 21. # 13 and #20
PubMed PubMed updates were performed periodically to retrieve pre-Medline and additional references. Pubmed automatically explodes MeSH headings. Human limit applied. Last update was performed on April 19, 2004.
1. Platelet Glycoprotein GPIIb-IIIa Complex [MeSH]
2. eptifibatide OR abciximab OR tirofiban OR aggrastat OR integrelin OR integrilin OR reopro [Title/Abstract]
3. 143653-53-6 OR 144494-65-5 OR 188627-80-7 [EC/RN Number]
4. “GP IIB*” OR “glycoprotein IIb*” OR gp2b* OR glycoproteinIIb* OR gpIIb OR gp2b* [Title/Abstract]
5. #1 OR #2 OR #3 OR #4 6. Angina, Unstable [MeSH] 7. Coronary Disease [MeSH] 8. Myocardial Infarction [MeSH] 9. Myocardial Ischemia [MeSH] 10. Coronary Restenosis [MeSH] 11. “Unstable angina” OR “heart attack*” OR
“coronary disease*” OR “myocardial infarct*” OR “coronary restenosis”
12. #6 OR #7 OR #8 OR #9 OR #10 OR #11 13. Angioplasty, Transluminal, Percutaneous
Coronary [MeSH] 14. Stents [MeSH] AND coronary 15. PCI OR PTCA [Text Word]

34
16. Coronary Intervention* OR Balloon angioplast* [Title/Abstract]
17. Atherectomy, Coronary [MeSH] 18. #13 OR #14 OR #15 OR #17 19. Clinical Trials [MeSH] 20. Epidemiologic Research Design [MeSH] 21. Comparative Study [MeSH] 22. Clinical Trial [PT] 23. Randomized Controlled Trial [PT] 24. Meta-Analysis [PT] 25. (random OR randomized OR controlled
clinical trials OR randomised OR clinical trial OR clinical trials OR double blind OR double blinded OR multicentre trials OR multicentre trial OR meta-analysis OR metaanalyses OR metaanalysis OR meta-analysis OR research integration OR
research overviews OR quantitative review OR quantitative reviews OR research overview OR methodological overviews OR systematic reviews OR systematic overviews OR integrative research OR systematic review OR quantitative synthesis OR comparative study OR comparative studies OR rct OR rcts OR cross-over study OR cross-over studies OR crossover study OR crossover studies OR single blind OR single blinded OR double blind OR double blinded OR triple blind OR triple blinded OR treble blind OR treble blinded OR dummy OR sham) [Text Word]
26. #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25
27. #5 AND #12 AND #18 AND #26

35
Appendix 2: Trial Quality Assessment Form Reference Reviewer
No category Score 1 Randomization
Was the study described as randomized (i.e., Including words such as randomly, random, randomization)? A trial reporting that it is “randomized” receives one point: yes=1, no=0.
Trials describing an appropriate method of randomization (table of random numbers, computer generated) receive an additional point: appropriate=1, not appropriate=0.
If the report describes the trial as randomized and uses an inappropriate method of randomization (eg. date of birth, hospital numbers), a point is deducted: inappropriate=-1.
2 Double-blinding
Was the study described as double-blind? A trial reporting that it is “double-blind” receives one point: yes=1, no=0.
Trials describing an appropriate method of double-blinding (identical placebo: colour, shape, taste) receive an additional point: yes=1, no=0.
If the report describes a trial as double-blind and uses an inappropriate method (e.g., comparison of tablets versus injection with no dummy), a point is deducted: inappropriate=-1.
3 Withdrawals and dropouts
Was there a description of withdrawals and dropouts? A trial reporting the number and reasons for withdrawals or dropouts receives one point. If there is no description, no point is given: yes=1, no=0.
Total score (for categories 1 to 3)
(0 to 2=low, 3 to 4=moderate, 5=high)
Adequacy level
4 Adequacy of allocation concealment
Central randomization; numbered or coded bottles or containers; drugs prepared by a pharmacy; serially numbered, opaque, sealed envelopes=adequate
Alternation; reference to case record number or date of birth=inadequate Allocation concealment is not reported or fits neither category=unclear

36
Appendix 3: Baseline Patient Characteristics Study Patient Characteristics Interventions
ADMIRAL6 Abciximab Placebo Mean age (years) 60 62 Male (%) 85 78 Hypertension (%) 34 41 Diabetes (%) 15 20 Hyperlipidemia (%) 40 37 Current smoker (%) 45 40 Prior MI (%) 14 7 Prior unstable angina (%) 9 7 Prior stable angina (%) 12 15 Prior PTCA (%) 18 10 Prior CABG (%) 10 13 CADILLAC22 PTCA PTCA+
abciximab Stenting Stenting+
abciximab Median age (years) 59 60 60 59 Male (%) 71 74 73 74 Prior MI (%) 14 16 12 13 Prior PTCA (%) 12 12 9 12 Prior CABG (%) 2 2 1 2 Diabetes (%) 15 16 16 19 Hypertension (%) 45 52 50 46 Hyperlipidemia (%) 36 41 38 38 Current smoker (%) 42 44 45 42 CAPTURE5 Abciximab Placebo Mean age (years) 61 61 Male (%) 73 72 Prior MI (%) 42 38 Prior angina (%) 49 51 Diabetes (%) 15 13 Hypertension (%) 43 41 Current smoker (%) 38 41 Prior PTCA (%) 13 14 Prior CABG (%) 2 3

37
Study Patient Characteristics Interventions
Chen et al.20 c7E3 Fab (abciximab)
Placebo
Age (years) 70 70 Male (%) 91 100 Hypertension (%) 68 65 Diabetes (%) 36 35 Hypercholesterolemia (%) 18 15 Current smoker (%) 36 55 Prior MI (%) 41 50 Prior PCI (%) 9 15 Prior CABG (%) 5 0 COMPARE24 Abciximab Eptifibatide Tirofiban
(dose in PRISM-
PLUS trial)
Tirofiban (dose in
RESTORE trial)
Mean age (years) 58 59 64 66 Male (%) 86 63 81 64 Diabetes (%) 28 16 19 57 Hypercholesterolemia (%) 81 68 56 86 Smoking (%) 38 37 44 36 Prior MI 43 32 38 36 EPIC16 c7E3 Fab
(abciximab) bolus+infusion
c7E3 Fab (abciximab)
bolus +placebo infusion
Placebo bolus+
infusion
Median age (years) 62 60 61 Male (%) 71 72 73 Prior MI (%) 59 59 54 Diabetes (%) 23 23 26 Hypertension (%) 54 55 55 Vascular disease (%) 13 13 12 Hypercholesterolemia (%) 55 59 57 History of smoking (%) 68 71 65 Prior PCI (%) 22 20 25 Prior CABG (%) 16 14 15

38
Study Patient Characteristics Interventions
EPILOG12 Abciximab+ standard heparin
Abciximab+low heparin
Placebo+ standard heparin
Median age (years) 60 60 60 Male (%) 73 71 72 Diabetes (%) 22 23 24 Prior MI (%) 21 21 20 Prior angina (%) 80 78 79 Prior CABG (%) 12 13 13 EPISTENT10 Balloon+
abciximab Stent+
abciximab Stent+ placebo
Mean age (years) 60 59 59 Male (%) 75 75 75 Hypertension (%) 55 48 55 Diabetes (%) 20 20 21 Smoker (%) 35 37 39 Prior MI (%) 49 49 55 Prior CABG (%) 8 8 11 ERASER4 Abciximab
12 hours infusion
Abciximab 24 hours infusion
Placebo
Median age (years) 62 58 58 Male (%) 75 84 77 Hypertension (%) 47 52 51 Diabetes (%) 13 19 11 Smoker (%) 29 36 28 Prior PCI (%) 13 12 17 ESPRIT15 Eptifibatide Placebo Median age (years) 62 62 Male (%) 73 72 Hypertension (%) 59 59 Diabetes (%) 20 21 Hyperlipidemia (%) 58 59 Smoker (%) 24 23 Stable angina (%) 39 38 Prior MI (%) 32 31 Prior unstable angina (%) 32 33 Prior PCI (%) 23 24 Prior CABG (%) 10 10

39
Study Patient Characteristics Interventions
Galassi18 Abciximab+ heparin
Placebo+ heparin
Mean age (years) 61 63 Male (%) 87 89 Family history of CAD (%) 44 40 Diabetes (%) 28 27 Hypertension (%) 33 35 Hypercholesterolemia (%) 22 27 Smoking (%) 72 67 Prior MI (%) 65 69 Prior unstable angina (%) 52 46 Harrington19 Eptifibatide Placebo Median age (years) 61 58 Male (%) 72 84 Hypertension (%) 67 74 Diabetes (%) 31 21 Hyperlipidemia (%) 56 58 Smoking (%) 74 68 Family history of CAD (%) 57 63 Prior MI (%) 52 26 Prior CABG (%) 20 42 IMPACT17 Eptifibatide
(4-hour infusion)
Eptifibatide (12-hour infusion)
Placebo
Median age (years) 62 60 62 Male (%) 81 73 71 Hypertension (%) 46 59 55 Diabetes (%) 25 12 24 Hyperlipidemia (%) 58 59 63 Family history of ischemic
heart disease (%) 46 38 57
Smoking (%) 69 57 76 Prior MI (%) 42 47 40 Prior angina (%) 77 86 77 Prior PTCA (%) 35 45 39 Prior CABG (%) 10 16 27

40
Study Patient Characteristics Interventions
IMPACT-II13 Eptifibatide low dose
Eptifibatide high dose
Placebo
Median age (years) 62 60 60 Male (%) 73 76 75 Hypertension (%) 54 55 54 Diabetes (%) 23 23 22 Hyperlipidemia (%) 55 56 53 Smokers (%) 65 65 66 Prior MI (%) 41 41 40 Prior CABG (%) 16 17 15 Prior intervention (%) 28 31 29 ISAR-II8 Abciximab Usual care Mean age (years) 61 60 Male (%) 76 78 Arterial hypertension (%) 61 64 Diabetes (%) 14 13 Hypercholesterolemia (%) 64 63 Smoker (%) 60 48 Prior PTCA (%) 6 7 Prior CABG (%) 2 6 ISAR-REACT28
Abciximab+low dose heparin
Placebo+high dose heparin
Mean age (years) 65 66 Male (%) 77 76 Arterial hypertension (%) 54 55 Diabetes (%) 21 20 Current smoker (%) 18 17 Hypercholesterolemia (%) 54 53 Angina class III / IV (%) 40 40 Prior MI (%) 32 33 Prior CABG (%) 10 9 Juergens26 Tirofiban Placebo Mean age (years) 59 59 Male (%) 83 83 Hypertension (%) 48 56 Diabetes (%) 17 13 Current smoker (%) 18 16 Prior MI (%) 46 46 Stable angina pectoris (%) 49 49 Unstable angina (%) 48 44

41
Study Patient Characteristics Interventions
Petronio21 Abciximab+ low heparin
Placebo+ low heparin
Mean age (years) 60 61 Male (%) 66 64 Diabetes (%) 18 18 Prior MI 9 11 Prior CABG (%) 0 2 PRICE7 Abciximab Eptifibatide Median age (years) 63 63 Male (%) 67 68 Hypertension (%) 68 71 Diabetes (%) 25 33 Hyperlipidemia (%) 56 65 Smoker (%) 63 71 Prior CABG (%) 22 20 Prior PCI (%) 37 37 RAPPORT9 Abciximab Placebo Median age (years) 60 62 Male (%) 73 72 Hypertension (%) 46 50 Diabetes (%) 23 22 Current smoker (%) 41 41 Prior MI (%) 17 21 Prior revascularization (%) 14 14 RESTORE11 Tirofiban Placebo Mean age (years) 59 59 Male (%) 72 72 Hypertension (%) 54 56 Diabetes (%) 20 20 Hypercholesterolemia (%) 50 49 History of smoking (%) 64 67 Prior MI (%) 35 34 Prior PTCA (%) 21 20 Prior CABG (%) 6 8

42
Study Patient Characteristics Interventions
Simoons (EUR CO-OP)14
c7E3 Fab Placebo
Median age (years) 61 60 Male (%) 67 80 Prior MI (%) 20 17 Prior angina (%) 27 47 Prior PTCA (%) 13 17 Prior CABG (%) 0 7 Tamburino23 Abciximab+
low heparin Placebo+ standard heparin
Mean age (years) 61 63 Male (%) 87 88 Family history of CAD (%) 44 40 Hypertension (%) 33 35 Diabetes (%) 28 27 Hypercholesterolemia (%) 22 27 Smoking (%) 72 67 Unstable angina (%) 53 61 Prior MI (%) 65 69 TARGET27 Tirofiban Abciximab Mean age (years) 62 63 Male (%) 74 73 Hypertension (%) 64 65 Diabetes (%) 23 23 Smoker (%) 65 64 Prior MI (%) 40 39 Prior PTCA (%) 29 30 Prior CABG (%) 17 17 TEAM25 Tirofiban Eptifibatide Abciximab Mean age (years) 65 years in
entire cohort
Male (%) 65% in entire cohort
Systemic hypertension (%) 88% in entire cohort
Diabetes (%) 35% in entire cohort
Prior angina at rest (%) 47% in entire cohort
Prior MI (%) 25% in entire cohort

43
Appendix 4: Inclusion and Exclusion Criteria of Trials Study Inclusion Criteria Exclusion Criteria
ADMIRAL6 Scheduled for primary coronary revascularization, ≥18 years of age, first symptoms of acute MI ≤12 hours before enrolment, ST-segment elevation of ≥1 mm in >2 contiguous leads of ECG
Bleeding diathesis, received thrombolytic agents for current episode, neoplasm, recent stroke, uncontrolled hypertension, recent surgery, oral anticoagulant therapy, limited life expectancy, childbearing potential, known contraindications to therapy with Aspirin, ticlopidine or heparin
CADILLAC22 ≥18 years of age; presence for ≥30 minutes but ≤12 hours of symptoms consistent with acute MI; presence of ST-segment elevation in >2 contiguous leads or left bundle-branch block, high grade stenosis and associated abnormalities in regional wall motion
In cardiogenic shock, bleeding diathesis, allergy to study drug, major surgery or gastrointestinal or genitourinary bleeding in the last 6 months, cerebrovascular event in the last 2 years, permanent residual neurologic defect, history of leukopenia, thrombocytopenia, hepatic or renal dysfunction, recently received a thrombolytic agent, non-cardiac illness associated with life expectancy of <1 year, participation in another study
CAPTURE5 Patients with refractory unstable angina, latest episode of ischemia should have occurred <48 hours before enrolment, all patients had undergone angiography and had significant coronary artery disease with culprit lesion suitable for angioplasty
Recent MI (unless creatine kinase values returned to <2 times upper limit of normal); features of persisting ischemia that require immediate intervention; ≥50% occlusion of left main coronary artery; culprit lesion in a bypass graft; bleeding risk factors (surgery, gastro-intestinal or genitourinary bleeding in the last 6 weeks); cerebrovascular accident in the last 2 years; planned administration of oral anticoagulants, intravenous dextran or thrombolytic agent before or during PTCA; underlying medical conditions such as persistent hypertension despite treatment; bleeding diathesis; history of autoimmune disease; platelet count <100×109/L
Chen20 Scheduled to undergo coronary angioplasty, high risk for abrupt vessel closure and not at high risk for bleeding
≥80 yrs of age, bleeding diathesis, major surgery in the last 6 weeks, stroke ≤2 years before study entry, planned stent implantation, directional atherectomy or rotational atherectomy

44
Study Inclusion Criteria Exclusion Criteria COMPARE24 Unstable angina or non-ST-
elevation MI, a planned PCI Prior treatment with platelet GP IIb/IIIa antagonist within the last 30 days, any relative or absolute contraindication to platelet GP IIb/IIIa inhibition
EPIC16 Patients at high risk for abrupt vessel closure and scheduled to undergo coronary angioplasty or directional atherectomy
≥80 years of age, bleeding diathesis, major surgery in the last 6 weeks, stroke ≤2 years before study entry
EPILOG12 Patients undergoing elective or urgent PC/I, >21 years of age, with a target lesion in which there was stenosis of ≥60% in the vessel
Acute MI, unstable angina with associated ECG changes during previous 24 hours, planned stent implantation or rotational atherectomy, PCI performed within previous 3 months, left main coronary artery stenosis of ≥50% not protected by collateral vessels, concurrent warfarin therapy or a baseline prothrombin time >1.2 times control value, cerebrovascular accident in the last 2 years or a residual neurologic deficit, intracranial neoplasm, aneurysm, arteriovenous malformation, history of vasculitis, known hemorrhagic diathesis, active internal bleeding, hypertension with SBP >180 mm Hg or DBP >100 mm Hg, major surgery, gastrointestinal bleeding or genitourinary bleeding in the last 6 weeks
EPISTENT10 Patients scheduled to undergo elective or urgent percutaneous coronary revascularization were eligible if target lesions had caused stenosis of ≥60% amenable to balloon angioplasty or stenting; and target vessel not an unprotected left-mainstem stenosis
Bleeding diathesis, intracranial neoplasm, history of stroke in the last 2 years, uncontrolled hypertension (SBP >180 mm Hg, DBP >100 mm Hg), recent surgery, or percutaneous coronary intervention in the last 3 months, concurrent warfarin therapy or an international normalized ratio of >1.5 at baseline
ERASER4 Patients with a de novo target coronary artery stenosis of ≥50% in a vessel of diameter 2.75 mm to 3.5 mm and to be referred for intracoronary stent implantation
MI ≤72 hours before randomization, evident intracoronary thrombus, coronary intervention on non-target lesion in the last 6 months, planned debulking before stent placement, expected inability to access target lesion by intravascular ultrasound (i.e., calcified plaque or tortuous vessel), standard contraindications to use of abciximab

45
Study Inclusion Criteria Exclusion Criteria ESPRIT15 Intent to treat a native coronary
artery with stent implantation in those without clear eligibility for GP IIb/IIIa inhibitor
MI ≤24 hours before randomization and ongoing chest pain precipitating urgent referral for PCI, PCI ≤90 days, previous stent implantation at target location, staged PCI anticipated ≤30 days after randomization, treatment with GP IIb/IIIa inhibitor or thienopyridine ≤30 days before randomization, stroke or transient ischemic attack in the last 30 days, history of hemorrhagic stroke, bleeding diathesis or evidence of abnormal bleeding ≤30 days before randomization, major surgery in the last 6 weeks, uncontrolled hypertension (>200/100 mm Hg), platelet count <100,000/µL or a serum creatinine level of >4.0 mg/dL
Galassi18 Patients with demonstrable ischemia and target de novo complex lesion stenosis ≥70% in a native vessel; and treated by stent implantation
Acute MI, bleeding diathesis, thrombocytopenia, active internal bleeding, severe uncontrolled hypertension, stroke in the last 2 years, major surgery or trauma ≤6 weeks before study entry
Harrington19 Patients undergoing elective coronary intervention with an FDA-approved device
History of bleeding disorder, recent gastrointestinal bleeding, major surgery in the last 6 weeks, major trauma or coronary bypass surgery in the last 6 months, previous coronary angioplasty during index hospital admission, stroke or other central nervous system structural abnormality, severe hypertension, known pregnancy, prothrombin time >1.2 times control, hematocrit <30%, platelet count <100, 000/µL, creatinine >4.0 mg/dL
IMPACT17 Patients scheduled for elective coronary balloon angioplasty or directional coronary atherectomy
History of bleeding disorder, recent gastrointestinal bleeding, major surgery in the last 6 weeks, stroke or other central nervous system structural abnormality, severe hypertension, pregnancy elevation of baseline prothrombin time (>1.2 times control), hematocrit <30%, platelet count <100, 000/µL, creatinine >4.0 mg/dL

46
Study Inclusion Criteria Exclusion Criteria IMPACT-II13 Patients scheduled for elective,
urgent or emergency coronary intervention with an FDA-approved device
Bleeding diathesis, severe hypertension (SBP >200 mm Hg or DBP >100mm Hg on therapy), major surgery in the last 6 weeks, stroke or other disorders of central nervous system, pregnancy, gastrointestinal or genitourinary bleeding in the last 30 days, other major illness
ISAR-28 Patients with acute MI undergoing revascularization by stent placement <48 hours after onset of pain: typical anginal pain lasting >30 minutes; ST-segment elevation of ≥1 mm in >2 contiguous leads; or elevation in creatine kinase to ≥3 times the upper limit of normal with concomitant rise in MB isoenzyme; or coronary artery occlusion with angiographic appearance of fresh thrombus
Inability to give informed consent and contraindications to one of the study drugs
ISAR-REACT28
Patients with coronary artery disease who were to undergo elective PCI in native coronary vessels between May 2000 and February 2003; and had been pretreated with 600 mg of clopidogrel >2 hours before intervention
MI in the last 14 days; unstable angina with ST-segment changes of >0.1mV in >2 electrocardiographic leads at rest; troponin T level of >0.03 ng/mm or both; target lesion in venous bypass graft; chronic occlusion; target lesion with angiographically visible thrombus; left ventricular ejection fraction of <30%; hemodynamic instability, type I diabetes, pericarditis or cancer; stroke in prior 3 months; active bleeding or bleeding diathesis; trauma or major surgery in preceding month; suspected aortic dissection; receiving oral anticoagulation therapy; glycoprotein IIb/IIIa inhibitor in the last 14 days; severe, uncontrolled hypertension (systolic BP >180 mm Hg); hemoglobin level of <10 g/dL or hematocrit <34%; had platelet count of <100,000/mm3 or >600,000/mm3; known allergic reaction to study medication; were or might be pregnant
Juergens26 Patients scheduled to undergo PTCA with intracoronary stent placement
Thrombolytic therapy ≤24 hours or elevated levels of creatine kinase at baseline, allergic to or unable to tolerate Aspirin or heparin, abciximab in the last 14 days of procedure, ticlopidine or clopidogrel or low-molecular weight heparin within 12 to 24 hours of

47
Study Inclusion Criteria Exclusion Criteria randomization, PTCA in the last 14 days or likely to undergo planned repeat PTCA as a staged procedure, target vessel was unprotected left main stenosis, bleeding disorder in the last 3 months, persistent SBP >180 mm Hg or persistent DBP >105 mm Hg, stroke or other intracranial pathology ≤1 year, recent major surgery, recent trauma, recent cardiopulmonary resuscitation, active peptic ulcer disease, pericarditis, significant retinopathy, suspected aortic dissection, uncontrolled cardiac arrhythmia, other hemodynamically significant cardiac disease, clinically important medical illness that would make survival for duration of study unlikely, serum creatinine level >2.5 mg/dL, hemoglobin <11 g/dL, international normalized ratio <1.5, platelet count <150,000/mm3, unable to give informed consent
Petronio21 Consecutive patients admitted on an emergency basis, <24 hours from onset of chest pain, because of suspected failure of thrombolysis for acute MI
Patients who did not undergo PTCA or other coronary intervention because of milder or reduced clinical signs of failed thrombolysis at time of coronary angiography
PRICE7 >21 years of age, undergoing elective coronary balloon angiography with or without stent implantation at 1 of 2 designated medical centres
Acute MI <48 hours, unstable angina with new or presumably new concomitant ST-segment or T-wave abnormalities, hemodynamic instability <12 hours, degenerated saphenous vein graft lesions, American College of Cardiology (ACC)/American Heart Association (AHA) type C lesions, history of hemorrhagic diathesis, major surgery or trauma <6 weeks before randomization, baseline platelet count <100,000 mm3, planned rotational atherectomy, baseline serum creatinine level >3 mg/dL, administration of abciximab or eptifibatide in the last 7 days of randomization, planned staged interventional procedure during index hospitalization, participation in other clinical research studies in the last 30 days of randomization

48
Study Inclusion Criteria Exclusion Criteria RAPPORT9 <12 hours after onset of acute MI,
referred for primary angioplasty Severe thrombocytopenia, baseline prothrombin time >1.2 times control, ongoing internal bleeding or recent major surgery, previous stroke, severe uncontrolled hypertension, PTCA of infarct artery in the last 3 months, cardiogenic shock or prolonged resuscitation, vasculitis, administration of abciximab or fibrinolytic therapy, inability to give written informed consent
RESTORE11 Patients undergoing coronary interventions ≤72 hours after presentation with acute coronary syndrome (unstable angina or acute MI)
Thrombolytic therapy in the last 24 hours, contraindication to anticoagulation, history of platelet disorder or thrombocytopenia, stroke or other intracranial pathology likely to predispose to bleeding, scheduled for elective stent placement if angioplasty using rotablator or transluminal extraction catheter device planned
Simoons (EUR CO-OP)14
Between 21 and 75 years of age, having exhibited at least one episode of angina with concomitant dynamic ST-T segment changes, >1 episode of ischemia had to occur despite bed rest and medical treatment with intravenous heparin and nitrates, coronary angiography performed ≤24 hours after most recent episode of ischemia
Exhibited features of ongoing ischemia requiring immediate intervention, prior PTCA of same coronary segment in the last 6 months, previous myocardial Q-wave infarction in the last 7 days, female with childbearing potential, recent major trauma (resuscitation, surgery or gastrointestinal or genitourinary bleeding in the last 6 weeks, hepatic or renal disorder, bleeding diathesis, platelet count <100,000/mm3, autoimmune disorders)
Tamburino30 With demonstrable reversible ischemia and severe coronary stenoses requiring stent implantation
Saphenous graft lesion, thrombocytopenia, bleeding diathesis, stroke in the last 2 years, active internal bleeding, uncontrolled hypertension, major surgery or trauma in the last 6 weeks
TARGET27 Patients scheduled to undergo coronary stenting procedure of newly stenotic or restenotic atherosclerotic lesion in native vessel or bypass graft
Cardiogenic shock or acute MI with ECG evidence of ST-segment elevation, serum creatinine level ≥2.5 mg/dL, ongoing bleeding, bleeding diathesis, platelet count <120,000 mm3
TEAM25 Patients with high risk clinical features of post-MI, pain at rest or complex angiographic lesions
High risk of bleeding, MI in the last 72 hours; vein graft PCI, chronic total occlusion, elevated CK-MB values at baseline, prior abciximab use for ≤1 year, eptifibatide or tirofiban infusion ≤24 hours before PCI

49
Appendix 5: Use of Concomitant Medications Study Treatment Arms Aspirin Heparin Nitrates Calcium
Channel Blocker
Beta- Blocker
ADMIRAL6 Abciximab Placebo
Yes, dose not reported
Initial bolus of 70 U/kg and additional adjusted dose if necessary
N/R N/R N/R
CADILLAC22 PTCA PTCA+ abciximab Stenting Stenting+ abciximab
324 mg orally or 250 mg intra-venously
5,000 U before catheter-ization
N/R N/R Yes, dose not reported
CAPTURE5 Abciximab Placebo
Minimum dose of 50 mg/d
Adjusted dose
Yes, dose not reported
Yes, dose not reported
Yes, dose not reported
Chen20 Abciximab Placebo
325 mg orally
Adjusted dose
N/R N/R N/R
COMPARE24 Abciximab Eptifibatide Tirofiban (dose in PRISM-PLUS) Tirofiban (dose in RESTORE)
325 mg before and after PCI
Adjusted dose
N/R N/R N/R
EPIC16 Abciximab (bolus +infusion) Abciximab bolus +placebo infusion Placebo (bolus +infusion)
325 mg orally
Initial bolus of 10,000 U to 12,000 U followed by adjusted dose of heparin
N/R N/R N/R

50
Study Treatment Arms Aspirin Heparin Nitrates Calcium Channel Blocker
Beta- Blocker
EPILOG12 Abciximab+ standard heparin Abciximab+low heparin Placebo+ standard heparin
325 mg orally
N/R N/R N/R N/R
EPISTENT10 Stent+abciximab Balloon angioplasty+ abciximab Stent+placebo
325 mg orally
Weight adjusted dose
N/R N/R N/R
ERASER4 Abciximab, 12 hours infusion Abciximab, 24 hours infusion Placebo
≥200 mg orally, ≥2 hours before procedure
Adjusted dose
100 µg to 300 µg
N/R N/R
ESPRIT15 Eptifibatide Placebo
Yes, dose not reported
Weight adjusted dose
N/R N/R N/R
Galassi18 Abciximab+low heparin Placebo+heparin
325 mg orally
N/R N/R N/R N/R
Harrington19 Integrelin Placebo
325 mg orally
Adjusted dose
N/R N/R N/R
IMPACT17 Integrelin+4 hours infusion Integrelin+ 12 hours infusion Placebo
325 mg orally
Weight adjusted dose
N/R N/R N/R
IMPACT13 Eptifibatide (135/0.5) Eptifibatide (135/0.75) Placebo
325 mg orally
Weight adjusted dose
N/R N/R N/R

51
Study Treatment Arms Aspirin Heparin Nitrates Calcium Channel Blocker
Beta- Blocker
ISAR-28 Abciximab+low heparin Standard heparin
500 mg intra-venously before catheteri-zation
5,000 U intra-venously before catheteri-zation
N/R N/R N/R
ISAR-REACT28
Abciximab+low dose heparin Placebo+high dose heparin
325 mg/d to 500 mg/d before procedure, orally; 100 mg/d to 325 mg/d after procedure
70 U/kg heparin used in abciximab group, while 100 U/kg to 140 U/kg heparin used in placebo group
Yes, dose not reported
Yes, dose not reported
Yes, dose not reported
Juergens26 Tirofiban Placebo
300 mg to 325 mg before procedure orally; and 75 mg to 325 mg thereafter
Bolus of heparin given based on standard procedure of local cathe-terization laboratory and additional adjusted dose if required
N/R N/R N/R
Petronio21 Abciximab+low heparin Placebo+low heparin
300 mg daily for patients who received coronary stent
10 U/kg/h of heparin for those with cardio-genic shock while treated by balloon pump
N/R N/R Routinely adminis-trated to all patients if well tolerated
PRICE7 Abciximab Eptifibatide
325 mg orally
Weight adjusted dose
N/R N/R N/R
RAPPORT9 Abciximab Placebo
Yes, dose not reported
Weight adjusted dose
Left to investi-gator’s discretion
Left to investi-gator’s discretion
Left to investi-gator’s discretion

52
Study Treatment Arms Aspirin Heparin Nitrates Calcium Channel Blocker
Beta- Blocker
RESTORE11 Tirofiban Placebo
325 mg orally
Weight adjusted dose before and during procedure
N/R N/R N/R
Simoons (EUR COOP)14
Abciximab Placebo
Minimum dose of 80 mg/d
Adjusted dose
50 µg/min to 200 µg/min
Continued as before randomi-zation
Continued as before randomi-zation
Tamburino30 Abciximab +low heparin Placebo +standard heparin
325 mg orally
N/R N/R N/R N/R
TARGET27 Abciximab Tirofiban
250 mg to 500 mg
Weight adjusted dose before procedure
N/R N/R N/R
TEAM25 Abciximab Eptifibatide Tirofiban
325 mg orally, at start of PCI
Adjusted dose at start of PCI
N/R N/R N/R
N/R=not reported

53
Appendix 6: Definitions of Composite End-Point (CEP) Study Composite end-point ADMIRAL6 Primary end-point
• death • reinfarction • urgent revascularization of target vessel
Secondary end-point • death • reinfarction • any revascularization (PTCA/CABG on urgent or elective
basis) at 30 days and 6 months CADILLAC22 • death from any cause
• reinfarction • repeated intervention or revascularization of target vessel as a
result of ischemia or disabling stroke during first 6 months after index procedure
CAPTURE5 • death from any cause • MI • urgent intervention for treatment of recurrent ischemia
Chen20 Occurrence ≤30 days after randomization • death • non-fatal MI • unplanned surgical revascularization • unplanned repeat percutaneous procedure • unplanned implantation of coronary stent or insertion of
intra-aortic balloon pump for refractory ischemia COMPARE24 No composite end-points reported EPIC16 30-day end-point
• death from any cause • non-fatal MI • CABG or repeat percutaneous intervention for acute ischemia • insertion of stent due to procedural failure or placement of
intra-aortic counterpulsation balloon pump to relieve refractory ischemia
6-month end-point • death from any cause • MI • any surgical or repeat percutaneous revascularization for
recurrent ischemia (urgent or elective) EPILOG12 Primary efficacy end-point
• death from any cause • MI or reinfarction • severe myocardial ischemia requiring urgent bypass surgery
or repeated percutaneous coronary revascularization ≤30 days after randomization

54
Study Composite end-point Secondary efficacy end-point
• death • MI • coronary bypass surgery or repeated percutaneous
revascularization ≤6 months after randomization EPISTENT10 • death from any cause
• MI or reinfarction • severe myocardial ischemia requiring urgent bypass surgery or
revascularization ≤30 days of intervention ERASER4 • death
• MI • target lesion revascularization ≤6 months
ESPRIT15 Primary end-point • death • MI • urgent target vessel revascularization, or bailout GP IIb/IIIa
inhibitor use at 48 hours Secondary end-point
• death • MI • target vessel revascularization
Galassi18 • death • MI • revascularization • acute or subacute stent thrombosis
Harrington19 No composite end-points reported IMPACT17 • death from all causes
• MI • urgent coronary intervention • stent implantation • CABG for ischemia or threatened closure
IMPACT-II13 • death • MI • urgent repeat coronary intervention • urgent CABG • index placement of intracoronary stent for abrupt closure
ISAR-28 • death • recurrent non-fatal MI • target lesion revascularization
ISAR-REACT28 No composite end-points reported Juergens26 • death
• MI • cardiovascular death • urgent CABG or repeat PTCA for recurrent ischemia

55
Study Composite end-point Petronio21 Occurrence of major adverse cardiac events at 30-day and 6-month
follow-up • death • reinfarction • congestive heart failure • target lesion revascularization • recurrent ischemia
PRICE7 • death • non-fatal MI • urgent target vessel revascularization
RAPPORT9 • death from any cause • non-fatal reinfarction • any repeat target vessel revascularization ≤6 months (7 and 30
days for acute phase end-points) RESTORE11 • death
• MI • CABG surgery because of angioplasty failure or recurrent
ischemia • repeat target vessel angioplasty for recurrent ischemia • insertion of stent because of actual or threatened abrupt
closure of target artery Simoons (EUR CO-OP)14
• death • MI • recurrent ischemia requiring urgent intervention
Tamburino30 • death • MI • acute or subacute stent thrombosis • urgent or target lesion revascularization
TARGET27 • death • non-fatal MI • urgent target vessel revascularization after index procedure
TEAM25 • CK-MB elevation >8 times normal • Q-wave MI • urgent CABG • procedural death

56
Appendix 7: Included Trials of GP IIb/IIIa Antagonists Study Setting Design Treatment Arms Number of
Patients Follow-up
Times Jadad Scores
Funding Sources
ADMIRAL6 France, multi-centre
Double-blind, placebo-controlled RCT
Abciximab Placebo
149 151
30 days, 6 months
4/5 Eli Lilly
CADILLAC22,31 Multi-national, multi-centre
RCT PTCA PTCA+abciximab Stenting Stenting+ abciximab
518 528 512 524
30 days, 6 months, 1 year
5/5 Guidant, Lilly Research Labora-tories, Mallin-krodt
CAPTURE5 Multi-national, multi-centre
Placebo-controlled RCT
Abciximab Placebo
630 635
30 days, 6 months
N/A
Chen et al.20 Taiwan, single-centre
Double-blind, placebo-controlled RCT
Abciximab Placebo
22 20
30 days 2/5 N/A
COMPARE24 US, single-centre
Open label RCT
Abciximab Eptifibatide Tirofiban (dose in PRISM-PLUS) Tirofiban (dose in RESTORE)
22 20 16 15
7 days 2/5 COR Therapeu-tics Merck & Co.
EPIC16, 32-34 US, multi-centre
Double-blind, placebo-controlled RCT
Abciximab (bolus +infusion) Abciximab bolus+placebo infusion Placebo (bolus+infusion)
708 695 696
30 days, 6 months, 3 years, 7 years
4/5 Centocor
EPILOG12,35,36 US, Canada, multi-centre
Double-blind, placebo-controlled RCT
Abciximab+standard dose heparin Abciximab+low dose heparin Placebo+standard dose heparin
918 935 939
30 days, 6 months, 1 year
4/5 Centocor, Eli Lilly and Company

57
Study Setting Design Treatment Arms Number of Patients
Follow-up Times
Jadad Scores
Funding Sources
EPISTENT10,37,38 US, Canada, multi-centre
Placebo-controlled RCT
Stent+abciximab Balloon angioplasty+ abciximab Stent+placebo
794 796 809
30 days, 6 months, 1 year
5/5 Centocor
ERASER4 Multi-national, multi-centre
Double-blind, placebo-controlled RCT
Abciximab, 12 hours infusion Abciximab, 24 hours infusion Placebo
79 75 71
Discharge or 7 days, 6 months
5/5 N/A
ESPRIT15,39 US, Canada, multi-centre
Double-blind, placebo-controlled RCT
Eptifibatide Placebo
1,040 1,024
48 hours, 30 days, 6 months, 1 year
5/5 COR Thera-peutics Inc.
Galassi et al.18 Italy, single-centre
Open-label, placebo-controlled RCT
Abciximab+low dose heparin Placebo+standard dose heparin
54 52
30 days
1/5 N/A
Harrington et al.19
US, multi-centre
Placebo-controlled RCT
Eptifibatide Placebo
54 19
During hospital stay
3/5 N/A
IMPACT17 US, multi-centre
Double-blind, placebo-controlled RCT
Eptifibatide+4 hours infusion Eptifibatide+12 hours infusion Placebo
52 49 49
30 days
3/5 COR Thera-peutics Inc.
IMPACT-II13 US, multi-centre
Double-blind, placebo-controlled RCT
Eptifibatide (135/0.5) Eptifibatide (135/0.75) Placebo
1,349 1,333 1,328
30 days, 6 months
5/5 COR Thera-peutics Inc., Schering-Plough Inc.
ISAR-28,29 Germany Single-blind, RCT
Abciximab+low heparin Standard dose heparin
201 200
30 days, 1 year
3/5 Lilly
ISAR-REACT28 Multi-national, multi-centre
Double-blind, placebo-controlled RCT
Abciximab+low dose heparin Placebo+high dose heparin
1,079 1,080
30 days
5/5 N/A

58
Study Setting Design Treatment Arms Number of Patients
Follow-up Times
Jadad Scores
Funding Sources
Juergens et al.26 Multi-national, multi-centre
Double-blind, placebo-controlled RCT
Tirofiban Placebo
536 358
30 days
4/5 N/A
Petronio et al.21 Italy, single-centre
Placebo-controlled RCT
Abciximab+low dose heparin Placebo+low dose heparin
44 45
30 days, 6 months
2/5 N/A
PRICE7 US, multi-centre
Double-blind RCT
Abciximab Eptifibatide
163 157
During hospital stay, 30 days
2/5 Schering-Plough Inc. COR Thero-peutics Inc. Guidant / Advanced Cardio-vascular Systems
RAPPORT9 US, multi-centre
Double-blind, placebo-controlled RCT
Abciximab Placebo
241 242
7 days, 30 days, 6 months
3/5 Centocor, Eli Lilly and Company
RESTORE11,40 Multi-national, multi-centre
Double-blind, placebo-controlled RCT
Tirofiban Placebo
1,071 1,070
2 days, 7 days, 30 days, 6 months
3/5 N/A
Simoons et al. (EUR CO-OP)14
Euro-pean, multi-centre
Double-blind, placebo-controlled RCT
Abciximab Placebo
30 30
During hospital stay
4/5 Centocor
Tamburino et al.23 Italy, single-centre
Open-label, RCT
Abciximab+low dose heparin Placebo+standard dose heparin
54 53
During hospital stay, 6 months
2/5 N/A
TARGET27,41,42
Multi-national, multi-centre
Double-blind RCT
Abciximab Tirofiban
2,411 2,398
30 days, 6 months, 1 year
5/5 Merck
TEAM25 US, single centre
Single- blind RCT
Abciximab Eptifibatide Tirofiban
63 61 56
During hospital stay, 30 days
2/5 Merck Inc. COR Thera-peutics Inc.

59
Appendix 8: Results from Trials on Abciximab Table 1: Results from ADMIRAL trial6
MI
Death
Revasculari-
zation CEP Treatment
Arms Time Points
n % n % n % n %
Abciximab (n=149) Placebo (n=151)
30 days 6 months 30 days 6 months
2 3 4 6
1.3 2.0 2.6 4.0
5 5 10 11
3.4 3.4 6.6 7.3
11 26 19 36
7.4 17.4 12.6 23.8
9 11 22 24
6.0 7.4 14.6 15.9
Table 2: Results from CADILLAC trial22,31
MI
Death
Revasculari-
zation CEP Treatment
Arms Time Points
n % n % n % n %
PTCA+ abciximab (n=528) and stenting+ abciximab (n=524) PTCA (n=518) and stenting (n=512)
30 days 6 months 1 year 30 days 6 months 1 year
8 26 26 9 17 23
0.8 2.5 2.5 0.9 1.7 2.2
20 35 43 24 38 45
1.9 3.3 4.1 2.3 3.7 4.4
27 108 162 48 134 177
2.6 10.3 15.4 4.7 13.0 17.2
48 140 178 72 163 190
4.6 13.3 16.9 7.0 15.8 18.4
Table 3: Results from CAPTURE trial5
MI
Death
Revasculari-
zation CEP Treatment
Arms Time Points
n % n % n % n %
Abciximab (n=630) Placebo (n=635)
30 days 6 months 30 days 6 months
26 41 52 73
4.1 6.5 8.2 11.5
6 17 8 14
1.0 2.7 1.3 2.2
59 164 78 171
9.4 26.0 12.3 26.9
71 195 101 196
11.3 31.0 15.9 31.0

60
Table 4: Results from Chen20
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % n % n % n %
Abciximab (n=22) Placebo (n=20)
30 days 30 days
0 3
0 15
0 0
0 0
1 0
4.5 0
2 3
9.1 15.0
Table 5: Results from EPIC trial16,32-34
MI
Death
Revasculari-
zation CEP Treatment
Arms Time Points
n % n % n % n %
Abciximab (bolus+ infusion) (n=708) Abciximab bolus+ placebo infusion (n=695) Placebo (bolus+ infusion) (n=696)
30 days 6 months 1 year 30 days 6 months 1 year 30 days 6 months 1 year
37 49 55 43 56 62 60 73 77
5.2 6.9 7.8 6.2 8.1 8.9 8.6 10.5 11.1
12 22 30 9 18 29 12 24 31
1.7 3.1 4.2 1.3 2.6 4.2 1.7 3.4 4.5
23 161 178 41 185 207 56 205 221
3.2 22.7 25.1 5.9 26.6 29.8 8.0 29.4 31.8
59 191 216 79 227 251 89 244 266
8.3 27.0 30.5 11.4 32.7 36.1 12.8 35.1 38.2

61
Table 6: Results from EPILOG trial12
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % N % n % n %
Abciximab+ standard dose heparin (n=918) Abciximab+ low dose heparin (n=935) Placebo+ standard dose heparin (n=939)
30 days 6 months 1 year 30 days 6 months 1 year 30 days 6 months 1 year
35 48 50 34 47 48 81 93 98
3.8 5.2 5.4 3.6 5.0 5.1 8.6 9.9 10.4
4 13 17 3 10 16 7 16 24
0.4 1.4 1.9 0.3 1.1 1.7 0.7 1.7 2.6
21 167 246 15 176 251 48 180 289
2.3 18.2 26.8 1.6 18.8 26.8 5.1 19.2 30.8
49 76 87 48 78 90 109 138 151
5.3 8.3 9.5 5.1 8.3 9.6 11.6 14.7 16.1
Table 7: Results from EPISTENT trial10,37,38
MI
Death
Revasculari-
zation CEP Treatment
Arms Time Points
n % n % n % n %
Stent+ abciximab (n=794) Balloon angioplasty+ abciximab (n=796) Stent+ placebo (n=809)
30 days 6 months 1 year 30 days 6 months 1 year 30 days 6 months 1 year
36 41 47 42 52 61 78 82 91
4.5 5.2 5.9 5.3 6.5 7.7 9.6 10.3 11.2
2 4 8 6 14 17 5 10 19
0.3 0.5 1.0 0.8 1.8 2.1 0.6 1.2 2.3
10 13 121 15 17 159 17 21 126
1.3 1.6 15.2 1.9 2.1 20.0 2.1 2.6 15.6
42 51 160 55 73 201 87 98 194
5.3 6.4 20.2 6.9 9.2 25.3 10.8 12.1 24.0

62
Table 8: Results from ERASER trial4
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % n % n % n %
Abciximab+ 12 hours infusion (n=79) Abciximab+ 24 hours infusion (n=75) Placebo (n=71)
7 days 30 days 6 months 7 days 30 days 6 months 7 days 30 days 6 months
4 N/R 6 7 N/R 7 8 N/R 9
5.1 7.6 9.3 9.3 11.3 12.7
0 N/R 0 0 N/R 0 0 N/R 2
0 0 0 0 0 2.8
0 0 12 0 0 10 1 1 11
0 0 15.2 0 0 13.3 1.4 1.4 15.5
4 N/R 16 7 N/R 17 9 N/R 18
5.1 20.3 9.3 22.7 12.7 25.4
N/R=not reported
Table 9: Results from Galassi18
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % n % n % n %
Abciximab+ low dose heparin (n=54) Placebo+ standard dose heparin (n=52)
30 days 30 days
2 5
3.7 9.6
0 1
0 1.9
0 0
0 0
2 8
3.7 15.4

63
Table 10: Results from ISAR-2 trial8,29
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % n % n % n %
Abciximab+ low dose heparin (n=201) Standard dose heparin (n=200)
30 days 1 year 30 days 1 year
1 N/R 1 N/R
0.5 1.5
4 12 9 17
2.0 6.0 4.5 8.5
6 N/R 9 N/R
3.0 5.0
10 N/R 21 N/R
5.0 10.5
N/R=not reported
Table 11: Results from ISAR-REACT trial28
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % n % n % n %
Abciximab+ low dose heparin (n=1,079) Placebo+ high dose heparin (n=1,080)
30 days 30 days
40 41
4 4
3 3
0.3 0.3
10 7
1 1
N/R N/R
N/R N/R
N/R=not reported

64
Table 12: Results from Petronio21
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % n % n % n %
Abciximab+ low dose heparin (n=44) Placebo+ low dose heparin (n=45)
30 days 6 months 30 days 6 months
0 0 1 1
0 0 2.2 2.2
1 1 4 2
2.3 2.3 8.9 4.4
N/R 1 N/R 3
2.3 6.7
N/R 5 N/R 17
11.4 37.8
N/R=not reported
Table 13: Results from RAPPORT trial9
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % n % n % n %
Abciximab (n=241) Placebo (n=242)
7 days 30 days 6 months 7 days 30 days 6 months
4 8 16 8 10 18
1.7 3.3 6.6 3.3 4.1 7.4
3 6 10 4 5 11
1.2 2.5 4.1 1.7 2.1 4.5
15 22 50 22 30 53
6.2 9.1 20.7 9.1 12.4 21.9
20 32 68 30 39 68
8.3 13.3 28.2 12.4 16.1 28.1
Table 14: Results from Simoons (EUR CO-OP)14
MI
Death
Revasculari-
zation CEP Treatment
Arms Time Points
n % n % n % n %
Abciximab (n=30) Placebo (n=30)
In hospital 30 days In hospital 30 days
1 N/R 4 N/R
3.3 13.3
0 N/R 1 N/R
0 3.3
0 0 3
0 0 20.0
1 N/R 7 N/R
3.3 33.3
N/R=not reported

65
Table 15: Results from Tamburino30
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % n % n % n %
Abciximab+ low dose heparin (n=54) Placebo+ standard dose heparin (n=53)
In hospital 6 months In hospital 6 months
2 0 4 1
3.7 0 7.5 1.9
0 0 1 0
0 0 1.9 0
0 6 0 11
0 11.1 0 20.8
2 6 6 13
3.7 11.1 11.3 24.5

66
Appendix 9: Results from Trials on Eptifibatide Table 1: Results from ESPRIT trial15,39
MI
Death
Revasculari-
zation CEP Treatment
Arms Time Points
n % n % n % n %
Eptifibatide (n=1,040) Placebo (n=1,024)
48 hours 30 days 6 months 1 year 48 hours 30 days 6 months 1 year
56 64 73 N/R 92 99 106 N/R
54 6.2 7.0 9.0 9.7 10.4
1 4 8 14 2 6 14 20
0.1 0.4 0.8 1.3 0.2 0.6 1.3 2.0
6 20 89 N/R 11 24 96 N/R
0.6 1.9 8.6 1.1 2.3 9.4
62 78 148 N/R 95 113 187 N/R
6.0 7.5 14.2 9.3 11.0 18.3
N/R=not reported
Table 2: Results from Harrington19
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % n % n % n %
Eptifibatide (n=54) Placebo (n=19)
In hospital In hospital
1 2
1.9 10.5
0 0
0 0
1 5
1.9 26.3
N/R N/R
N/R=not reported

67
Table 3: Results from the IMPACT trial17
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % n % n % n %
Eptifibatide+4 hours infusion Eptifibatide+12 hours infusion Placebo (n=49)
30 days 30 days 30 days
1 2 1
1.9 2.0 2.0
1 0 1
1.9 0 2.0
N/R N/R N/R
5 2 6
9.6 4.1 12.2
N/R=not reported
Table 4: Results from IMPACT-II trial13
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % n % n % n %
Eptifibatide (135/0.5) (n=1,349) Eptifibatide (135/0.75) (n=1,333) Placebo (n=1,328)
30 days 30 days 30 days
89 92 107
6.6 6.9 8.1
7 11 15
0.5 0.8 1.1
57 65 74
4.2 4.9 5.6
124 132 151
9.2 9.9 11.4

68
Table 5: Effects of eptifibatide on major clinical outcomes
Outcome Period Number of Trials
OR (95% CI)
7 days 1 0.49 (0.04, 5.43) 30 days 3 0.60 (0.33, 1.08) 6 months 1 0.56 (0.23, 1.34)
Death
1 year 1 0.68 (0.34, 1.36) 7 days 2 0.56 (0.37, 0.84) 30 days 2 0.83 (0.65, 1.06)
MI
6 months 1 0.65 (0.48, 0.89) 7 days 2 0.21 (0.02, 1.95) 30 days 2 0.81 (0.62, 1.06)
Revascularization
6 months 1 0.90 (0.67, 1.22) 7 days 1 0.62 (0.44, 0.86) 30 days 3 0.73 (0.59, 0.91)
CEP
6 months 1 0.74 (0.59, 0.94) Minor bleeding 2 2.36 (0.98, 5.64) Major bleeding 3 1.27 (0.60, 2.70)

69
Appendix 10: Results from Trials on Tirofiban Table 1: Results from Juergens26
MI
Death
Revasculari-
zation CEP Treatment
Arms Time Points
n % n % n % n %
Tirofiban (n=536) Placebo (n=358)
30 days 30 days
18 13
3.4 3.6
1 0
0.2 0
4 7
0.7 2.0
21 14
3.9 3.9
Table 2: Results from RESTORE trial11,40
MI
Death
Revasculari-
zation CEP Treatment
Arms Time Points
n % n % n % n %
Tirofiban (n=1,071) Placebo (n=1,328)
7 days 30 days 6 months 7 days 30 days 6 months
39 45 67 57 61 81
2.7 4.2 6.3 5.3 5.7 7.6
4 9 19 4 8 15
0.4 0.8 1.8 0.4 0.7 1.4
42 65 227 64 81 256
3.9 6.1 21.2 6.0 7.6 23.9
72 110 254 108 130 279
6.7 10.3 23.7 10.1 12.1 26.1
Table 3: Effects of tirofiban on major clinical outcomes
Outcome Period Number of Trials OR (95% CI)
7 days 1 1.00 (0.25, 4.01) 30 days 2 1.18 (0.47, 2.95)
Death
6 months 1 1.27 (0.64, 2.51) 7 days 1 0.67 (0.44, 1.02) 30 days 2 0.77 (0.54, 1.08)
MI
6 months 1 0.81 (0.58, 1.14) 7 days 1 0.64 (0.43, 0.96) 30 days 2 0.70 (0.41, 1.19)
Revascularization
6 months 1 0.86 (0.70, 1.05) 7 days 1 0.64 (0.47, 0.88) 30 days 2 0.85 (0.66, 1.09)
CEP
6 months 1 0.88 (0.72, 1.07) Minor bleeding 1 5.12 (1.16, 22.55) Major bleeding 2 1.14 (0.39, 3.30)

70
Appendix 11: Results from Head-to-head Trials Table 1: Results from COMPARE trial24
MI
Death
Revasculari-
zation CEP Treatment
Arms Time Points
n % n % n % n %
Abciximab (n=22) Eptifibatide (n=20) Tirofiban (dose of PRISM-PLUS) (n=16) Tirofiban (dose of RESTORE) (n=15)
In hospital In hospital In hospital In hospital
N/R N/R N/R N/R
1 0 1 0
4.5 0 6.3 0
0 0 1 0
0 0 6.3 0
N/R N/R N/R N/R
N/R=not reported
Table 2: Results from PRICE trial7
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % n % n % n %
Abciximab (n=163) Eptifibatide (n=157)
In hospital 30 days In hospital 30 days
6 7 8 9
3.7 4.3 4.5 5.1
1 1 0 1
0.6 0.6 0 0.6
1 2 1 2
0.6 1.2 0.6 1.3
8 9 8 10
4.9 5.5 5.1 6.4

71
Table 3: Results from TARGET trial27
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % n % n % n % Abciximab (n=2,411) Tirofiban (n=2,398)
30 days 6 months 1 year 30 days 6 months 1 year
130 159 N/R 165 191 N/R
5.4 6.6 6.9 8.0
10 25 N/R 12 26 N/R
0.4 1.0 0.5 1.1
17 208 N/R 17 194
0.7 8.6 0.8 8.1
145 345 N/R 182 356
6.0 14.7 7.6 14.8
N/R=not reported
Table 4: Results from TEAM trial25
MI
Death
Revasculari-zation
CEP Treatment Arms
Time Points
n % n % n % n %
Abciximab (n=63) Eptifibatide (n=61) Tirofiban (n=56)
In hospital 30 days In hospital 30 days In hospital 30 days
N/R 1 N/R 1 N/R 2
1.6 1.6 3.6
N/R 1 N/R 1 N/R 0
1.6 1.6 0
N/R 1 N/R 0 N/R 1
1.6 0 1.8
1 N/R 1 N/R 1 N/R
1.6 1.6 1.8
N/R=not reported

72
Appendix 12: Summary of Findings Table 1: Effects of abciximab, eptifibatide or tirofiban on major clinical outcomes
Clinical
Outcome Number
of Patients
GP IIb/IIIa Group (% of
events)
Control Group (% of
events)
Odds Ratio (95% CI)
Number Needed to Treat (from odds ratio and control event rate using Cates calculator)
Death at 30 days 23,434
0.83 1.22 0.72 (0.56, 0.94)
296 (188, 1382)
MI at 7 days 5,153
4.31 6.97 0.59 (0.46, 0.75)
37 (28, 61)
MI at 30 days 21,412
4.41 6.08 0.63 (0.54, 0.74)
47 (38, 67)
MI at 6 months 16,046
5.73 8.29 0.65 (0.55, 0.77)
37 (29, 57)
Revascularization at 7 days
5,046
2.47 4.44 0.49 (0.29, 0.84)
46 (33, 147)
Revascularization at 30 days
23,416
3.44 5.19 0.66 (0.56, 0.77)
59 (46, 88)
Revascularization at 6 months
16,046
15.21 17.40 0.86 (0.78, 0.94)
49 (31, 115)
Minor bleeding 10,751 5.6 3.5 1.80 (1.47,2.21)
39* (26,65)
* Number needed to harm.
Table 2: Overall effect of abciximab: comparison between matched and all comparators
Outcome Matched Comparator OR (95% CI)
All Comparator OR (95% CI)
Death at 30 days 0.75 (0.53, 1.07) 0.72 (0.53, 0.99) Death at 6 months 0.84 (0.64, 1.09) 0.84 (0.66, 1.07) Death at 1 year 0.81 (0.61, 1.08) 0.82 (0.65, 1.03)
MI at 30 days 0.50 (0.41, 0.61) 0.56 (0.46, 0.69) MI at 6 months 0.62 (0.49, 0.79) 0.63 (0.51, 0.78) MI at 1 year 0.62 (0.46, 0.85) 0.65 (0.49, 0.86) Revascularization at 30 days 0.57 (0.47, 0.69) 0.60 (0.49, 0.73) Revascularization at 6 months 0.83 (0.74, 0.94) 0.85 (0.77, 0.94) Revascularization at 1 year 0.83 (0.74, 0.94) 0. 90 (0.77, 1.05)