Embed Size (px)
Citation preview
ww.sciencedirect.com
j o u rn a l o f s u r g i c a l r e s e a r c h x x x ( 2 0 1 4 ) 1e6
Available online at w
ScienceDirect
journal homepage: www.JournalofSurgicalResearch.com
Goal orientation in surgical residents: a study of themotivation behind learning
Rebecca L. Hoffman, MD,a,* Cristina Hudak-Rosander, MS,b
Jashodeep Datta, MD,a Jon B. Morris, MD,a and Rachel R. Kelz, MD, MSCEa
aDepartment of Surgery, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PennsylvaniabDepartment of Psychology, University of Utah, Salt Lake City, Utah
a r t i c l e i n f o
Article history:
Received 29 October 2013
Received in revised form
31 December 2013
Accepted 6 January 2014
Available online xxx
Keywords:
Goal orientation
Resident
Surgery
Education
Satisfaction
Burnout
Professionalism
* Corresponding author. Department of SurgeStreet, Philadelphia, PA 19104. Tel.: þ1 267 2
E-mail address: [email protected]/$ e see front matter ª 2014 Elsevhttp://dx.doi.org/10.1016/j.jss.2014.01.005
a b s t r a c t
Background: The subconscious way in which an individual approaches learning, goal
orientation (GO), has been shown to influence job satisfaction, job performance, and
burnout in nonmedical cohorts. The aim of this study was to adapt and validate an in-
strument to assess GO in surgical residents, so that in the future, we can better understand
how differences in motivation affect professional development.
Materials and methods: Residents were recruited to complete a 17-item survey adapted from
the Patterns of Adaptive Learning Scales (PALS). The survey included three scales assessing
GO in residency-specific terms. Items were scored on a 5-point Likert scale, and the psy-
chometric properties of the adapted and original PALS were compared.
Results: Ninety-five percent of residents (61/64) participated. Median age was 30 y and 33%
were female. Mean (standard deviation) scale scores for the adapted PALS were: mastery
4.30 (0.48), performance approach (PAP) 3.17 (0.99), and performance avoid 2.75 (0.88). Mean
(standard deviation) scale scores for the original PALS items were: mastery 3.35 (1.02), PAP
2.76 (1.15), and performance avoid 2.41 (0.91). Cronbach alpha were a ¼ 0.89 and a ¼ 0.84 for
the adapted PAP and avoid scales, respectively, which were comparable with the original
scales. For the adapted mastery scale, a ¼ 0.54. Exploratory factor analysis revealed five
factors, and factor loadings for individual mastery items did not load consistently onto a
single factor.
Conclusions: This study represents the first steps in the development of a novel tool to
measure GO among surgical residents. Understanding motivational psychology in resi-
dents may facilitate improved education and professional development.
ª 2014 Elsevier Inc. All rights reserved.
1. Introduction attain competence; performance approach (PAP) orientation,
The subconscious way in which an individual approaches a
learning task, known as goal orientation (GO), has been shown
to influence job satisfaction, job performance, and burnout
in nonmedical cohorts [1e3]. There are three subtypes of
GO: mastery orientation (MG), in which learners strive to
ry, Perelman School of M75 3290; fax: þ1 215 662 7penn.edu (R.L. Hoffman).ier Inc. All rights reserved
in which learners strive to demonstrate competence; and
performance avoid (PAV) orientation, in which learners strive
to avoid demonstrating incompetence. For the PAV-oriented
person, the prospect of potential failure is likely to elicit
anxiety, encourage self-protective withdrawal, and disrupt
concentration and task involvement [4,5]. In addition,
edicine at the University of Pennsylvania, 4 Maloney 3400 Spruce983.
.

j o u r n a l o f s u r g i c a l r e s e a r c h x x x ( 2 0 1 4 ) 1e62
neuroticism and emotional instability have been negatively
correlated with performance orientations [6].
GO can be used to understand and predict how people will
respond when faced with concrete achievement situations.
Because surgical residents face such situations daily, whether
in the operating room, taking a written or oral examination, or
engaging in feedback, studying GO may be particularly useful
in this population. For example, themastery-oriented resident
may view technical ability as something that can be improved
with effort and persistence, believe that effort leads to suc-
cess, and view feedback as useful information about how to
correct errors and develop competency. The performance-
oriented resident, however, may believe that the ability is
fixed and exert a tremendous amount of effort to compensate
for low ability. This resident may view specific negative
feedback as an overall judgment of one’s competency, which
can be particularly devastating and nonproductive [7].
Although both a mastery- and performance-oriented resi-
dent may exhibit competency, the notable difference may be
in the deleterious long-term effects on an individual’s
persistence, or lack thereof, in the face of failure and task
choice [4]. Further emphasizing the importance of the GO
construct, studies in both airline pilots and surgeons have
found that self-regulation and self-monitoring during com-
plex decision making rely on an understanding of one’s own
internal emotions juxtaposed with external environmental
factors [8,9]. Therefore, the ability of a resident to understand
his or her own GO might enhance their development of more
safe, patient oriented, and educational operative experiences.
Similarly, an increased awareness of and sensitivity to
different types of motivational behavior in the learning envi-
ronment by medical educators may help to enhance the
development of leadership, team building, self-assessment,
and job performance skills [10].
With the understanding that GO may be an important
construct to study among surgical residents, it is important to
identify a reliable and validmethod of assessing this construct
in medical cohorts. Relying on behavioral observations alone
is not sufficient, as both amastery- and performance-oriented
resident may exert the same degree of engagement to prove
task competency. In addition, individuals may manifest
various combinations of GO depending on the situation.
Because of this, the best way to study GO is to use self-report
measures. Although the measures of GO exist, they have not
yet been adapted and validated for use in medical cohorts.
To facilitate future study of the potential importance of GO
among surgical residents, we sought to adapt and validate a
well-studied GO instrument for use in the surgical resident
population to begin to understand the subconscious way in
which surgical residents approach tasks associated with
professional development.
2. Methods
2.1. Study population and setting
This study was deemed exempt from ongoing review by the
Institutional Review Board of the University of Pennsylvania.
After 2013American Board of Surgery In-Training Examination,
64 residents enrolled in a university-based surgical residency
programwere recruited to complete a 17-item survey designed
to test GO. The study population included both categorical and
preliminary surgical residents who were representative of 11
countries and 16 different states. Participants reviewed a
written study description, and inclusion was voluntary. Resi-
dents were made aware that their participation would not
affect their status within the program.
2.2. Educational setting
The sponsor hospital is a large (772-bed) urban, university-
based hospital with approximately 37,000 admissions annu-
ally, 1135 residents and fellows and 182 surgical faculty.
Educational conferences include twice weekly departmental
faculty-led didactics (one of which is a SCORE-based confer-
ence) [11], weekly morbidity and mortality conference,
monthly grand rounds and supplemental service-based con-
ferences. All residents (100%) complete a research fellowship
after the third clinical year.
2.3. Scale development
The Patterns of Adaptive Learning Scales (PALS) was devel-
oped by educational psychologists to examine the relation-
ship between the learning environment and students’
motivation, affect and behavior among school-aged children
[12]. Our survey instrument was adapted for use in graduate
surgical education using a subset of the PALS. The adapted
PALS included three scales assessing students’ personal
achievement GO (mastery, PAP, and PAV GO) in residency-
specific terms (Table 1). For instance, when the original PALS
referenced “class work,” “students,” and “teachers,” the
adapted PALS was translated into “situations,” “residents,”
and “attendings.”
2.4. Data collection
Study data were collected and managed using the Research
Electronic Data Capture tool hosted at the University of
Pennsylvania. Research Electronic Data Capture is a secure,
web-based application designed to support data capture for
research studies, providing: (1) an intuitive interface for
validated data entry; (2) audit trails for tracking data manip-
ulation and export procedures; (3) automated export pro-
cedures for seamless data downloads to common statistical
packages; and (4) procedures for importing data from external
sources [13].
2.5. Analytic strategy
Items were scored on a 5-point Likert scale (1 ¼ not at all true,
3 ¼ somewhat true, and 5 ¼ very true), and scale scores were
determined by averaging the scores for each item (Table 1). To
determine if the adapted PALS was a valid measure of GO
among surgical residents, the psychometric properties of the
adapted PALS were compared with those of the original PALS
using exploratory factor analysis and calculating Cronbach
alpha for each of the three subscales.
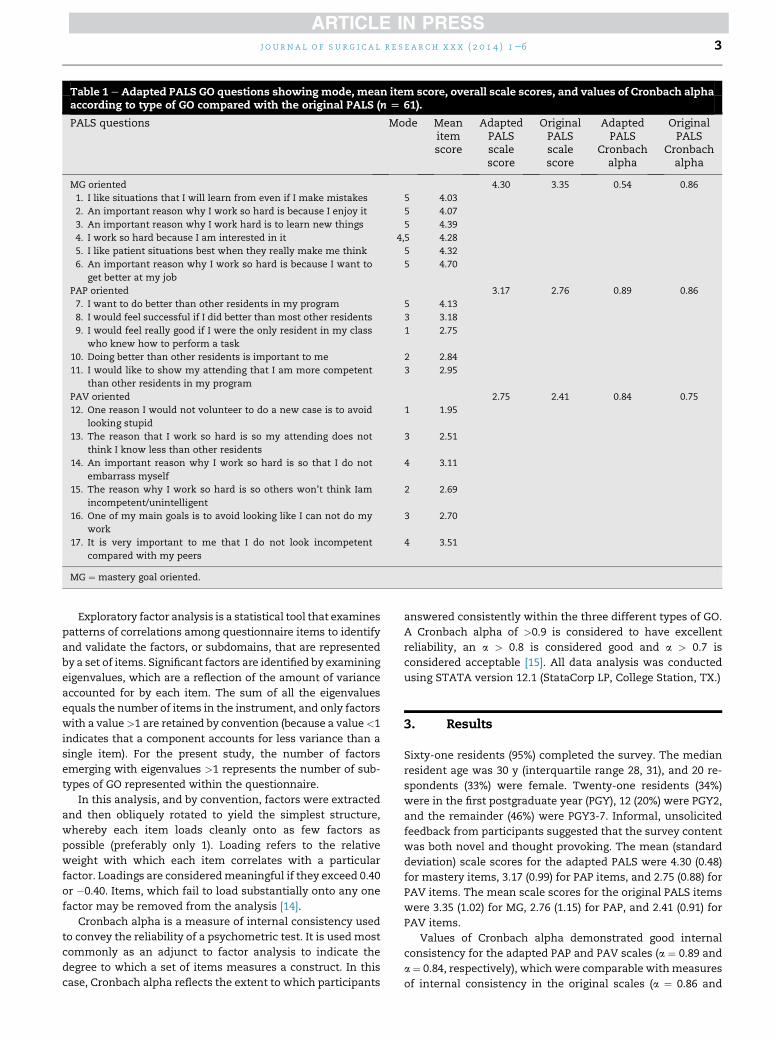
Table 1 eAdapted PALS GO questions showingmode, mean item score, overall scale scores, and values of Cronbach alphaaccording to type of GO compared with the original PALS (n [ 61).
PALS questions Mode Meanitemscore
AdaptedPALSscalescore
OriginalPALSscalescore
AdaptedPALS
Cronbachalpha
OriginalPALS
Cronbachalpha
MG oriented 4.30 3.35 0.54 0.86
1. I like situations that I will learn from even if I make mistakes 5 4.03
2. An important reason why I work so hard is because I enjoy it 5 4.07
3. An important reason why I work hard is to learn new things 5 4.39
4. I work so hard because I am interested in it 4,5 4.28
5. I like patient situations best when they really make me think 5 4.32
6. An important reason why I work so hard is because I want to
get better at my job
5 4.70
PAP oriented 3.17 2.76 0.89 0.86
7. I want to do better than other residents in my program 5 4.13
8. I would feel successful if I did better than most other residents 3 3.18
9. I would feel really good if I were the only resident in my class
who knew how to perform a task
1 2.75
10. Doing better than other residents is important to me 2 2.84
11. I would like to show my attending that I am more competent
than other residents in my program
3 2.95
PAV oriented 2.75 2.41 0.84 0.75
12. One reason I would not volunteer to do a new case is to avoid
looking stupid
1 1.95
13. The reason that I work so hard is so my attending does not
think I know less than other residents
3 2.51
14. An important reason why I work so hard is so that I do not
embarrass myself
4 3.11
15. The reason why I work so hard is so others won’t think Iam
incompetent/unintelligent
2 2.69
16. One of my main goals is to avoid looking like I can not do my
work
3 2.70
17. It is very important to me that I do not look incompetent
compared with my peers
4 3.51
MG ¼ mastery goal oriented.
j o u rn a l o f s u r g i c a l r e s e a r c h x x x ( 2 0 1 4 ) 1e6 3
Exploratory factor analysis is a statistical tool that examines
patterns of correlations among questionnaire items to identify
and validate the factors, or subdomains, that are represented
by a set of items. Significant factors are identified by examining
eigenvalues, which are a reflection of the amount of variance
accounted for by each item. The sum of all the eigenvalues
equals the number of items in the instrument, and only factors
with a value>1 are retained by convention (because a value<1
indicates that a component accounts for less variance than a
single item). For the present study, the number of factors
emerging with eigenvalues >1 represents the number of sub-
types of GO represented within the questionnaire.
In this analysis, and by convention, factors were extracted
and then obliquely rotated to yield the simplest structure,
whereby each item loads cleanly onto as few factors as
possible (preferably only 1). Loading refers to the relative
weight with which each item correlates with a particular
factor. Loadings are consideredmeaningful if they exceed 0.40
or �0.40. Items, which fail to load substantially onto any one
factor may be removed from the analysis [14].
Cronbach alpha is a measure of internal consistency used
to convey the reliability of a psychometric test. It is used most
commonly as an adjunct to factor analysis to indicate the
degree to which a set of items measures a construct. In this
case, Cronbach alpha reflects the extent to which participants
answered consistently within the three different types of GO.
A Cronbach alpha of >0.9 is considered to have excellent
reliability, an a > 0.8 is considered good and a > 0.7 is
considered acceptable [15]. All data analysis was conducted
using STATA version 12.1 (StataCorp LP, College Station, TX.)
3. Results
Sixty-one residents (95%) completed the survey. The median
resident age was 30 y (interquartile range 28, 31), and 20 re-
spondents (33%) were female. Twenty-one residents (34%)
were in the first postgraduate year (PGY), 12 (20%) were PGY2,
and the remainder (46%) were PGY3-7. Informal, unsolicited
feedback from participants suggested that the survey content
was both novel and thought provoking. The mean (standard
deviation) scale scores for the adapted PALS were 4.30 (0.48)
for mastery items, 3.17 (0.99) for PAP items, and 2.75 (0.88) for
PAV items. The mean scale scores for the original PALS items
were 3.35 (1.02) for MG, 2.76 (1.15) for PAP, and 2.41 (0.91) for
PAV items.
Values of Cronbach alpha demonstrated good internal
consistency for the adapted PAP and PAV scales (a ¼ 0.89 and
a ¼ 0.84, respectively), which were comparable withmeasures
of internal consistency in the original scales (a ¼ 0.86 and

Table 3 e Summary of results.
� The adapted PALS survey was designed to evaluate three
domains of goal orientation: mastery, PAP, and PAV.
� The adapted PALS survey demonstrated good internal
consistency for the PAP and PAV orientations.
� Additional work is needed to refine items used to test
mastery goal orientation in the surgical resident population.
� In its current form, the adapted PALS can be used to inform
residents about their goal orientation.
j o u r n a l o f s u r g i c a l r e s e a r c h x x x ( 2 0 1 4 ) 1e64
a ¼ 0.75, respectively). For the adapted MG scale, the value of
Cronbach alpha suggested poor internal consistency (a¼ 0.54),
in contrast to the original PALS MG scale (a ¼ 0.86).
Results of an exploratory factor analysis revealed five fac-
tors with Eigenvalues >1, in contrast to the three factors that
were represented in the original PALS. Examination of factor
loadings for individual items suggests that the MG scale items
did not consistently load on to a single factor. When items
were removed from the factor analysis which loaded onto
multiple factors or did not load onto the original three tested
factors, the overall value of Cronbach alpha did not change
dramatically (0.814 versus 0.819), and items meant to load
together in fact loaded together under the same factor
(Table 2). These final three factors accounted for 77% of the
total variance in the data. The two mastery-oriented ques-
tions of six that remained had good internal consistency
(a ¼ 0.87). All of the PAP items and three of six PAV remained
in the model and demonstrated a Cronbach alpha of a ¼ 0.79,
which is comparable with the original PALS survey (0.79). See
Table 3 for a summary of the results.
4. Discussion
Motivational theory is a novel construct in medical education
with practical applications in surgical education. The ability of
a program to understand its residents’ GOs could improve the
value of feedback for individual residents, facilitate appro-
priate goal setting on an individual basis, optimize the
educational value of the experience, and reduce burnout and
attrition. This study represents the first step toward the
development of an innovative tool to describe and understand
GO among surgical residents. In this study using factor anal-
ysis, we were able to successfully adapt and validate two of
three scales of GO (PAP and PAV) that comprise the PALS in-
strument for use in a population of surgical residents in a
Table 2 e Factor loadings in exploratory factor analysis.
Mastery goal oriented
An important reason why I work so hard is because
I enjoy it
0.94
I work so hard because I am interested in it 0.95
PAP oriented
I want to do better than other residents in my program 0.88
I would feel successful if I did better than most
other residents
0.75
I would feel really good if I were the only resident in my
class who knew how to perform a task
0.77
Doing better than other residents is important to me 0.82
I would like to show my attending that I am more
competent than other residents in my program
0.84
PAV oriented
An important reason why I work so hard is so that I do
not embarrass myself
0.89
The reason why I work so hard is so others won’t think
I am incompetent/unintelligent
0.82
It is very important to me that I do not look incompetent
compared with my peers
0.53*
* Also loaded weakly with PAP (0.41).
university-based training program. In addition, we found that
the adapted PALS instrument required minimal time to com-
plete and was of substantial interest to surgical residents.
Although the original PALS has been used to assess the GO of
school-age and college-age students, other methods of
assessing GO have been used in graduate school or other adult
populations [16e18]. In preparation for this study, we chose
the PALS because of its easily adaptable scale and brevity,
which made it appropriate for use in the field of surgical ed-
ucation. The low internal consistency and loading of the
mastery items onto additional factors in the PALS adaptation
suggests that the mastery scale needs additional modification
before wide-scale administration. It is likely that the sophis-
ticated nature of our study population, in terms of their life-
time educational experience, demands more detail in the
survey items to capture the mastery component of GO.
One of the important considerations in survey develop-
ment is the appropriateness of the measure to the population
being tested. Because surgical residents represent both a
unique student and professional population with substantial
demands on their time, surveys need to be succinct, and the
validity of their adaptation ascertained first in a pilot popu-
lation. In our adaptation, we have shown that, with the
exclusion of seven items from the original survey, we were
able to retain the three domains of GO in our adapted in-
strument and were able to preserve the overall validity of the
scale.
The Accreditation Council for Graduate Medical Education
Outcome Project in 1999 changed the accreditation process
from the assessment of a program’s potential to educate to the
evaluation of its actual accomplishments through an exami-
nation of program outcomes. The new competency-based
education is now centered on learner performance in reach-
ing specific objectives [19,20]. Interestingly, little effort has
focused on understanding the psychology of the adult learner
and their individual approaches to meet these new
competency-based objectives. Zweig and Webster [6] very
aptly note that with so many resources spent on developing
and delivering training content, little research goes into the
role trainees themselves play as recipients of this training.
With this innovative adaptation of the PALS for the surgical
resident population, we were able to identify at least three
motivational constructsdmastery, PAP, and PAV. That is to
say, surgical residents are not simplymotivated bymastery of
surgical skill in the traditional sense of the word. The moti-
vation for excellence in their chosen profession is complex,
and includes, in addition to the pure desire to attain and
demonstrate knowledge (mastery orientation), the somewhat
impure desire to outperform their peers and to avoid looking

j o u rn a l o f s u r g i c a l r e s e a r c h x x x ( 2 0 1 4 ) 1e6 5
incompetent (performance orientation). In fact, of the three
constructs tested, it was the PAP and PAV GOs, which
demonstrated the highest internal consistency. This finding is
consistent with previous research on intraoperative decision
making, where surgeons acknowledged that competing pri-
orities related to specific sociocultural norms (the constant
need to demonstrate success and avoid looking incompetent)
versus the responsibility for patient safety and the provision of
quality care influenced their care [8,9].
Latham and Brown showed that the purposeful and indi-
vidualized creation of learning goals increased the satisfac-
tion of MBA students with their respective programs [21].
Furthermore, given current discourse regarding trainees
commitment to patients in the era of work hour reform, an
awareness of GO may help residents to acknowledge the
competing priorities that surgeons face during their careers
(of dedication to patients versus dedication to demonstrating
their identity as a “successful” surgeon) and to develop into
true professionals, aware of how what motivates them im-
pacts on patient care [8,9].
This pilot study has several limitations. Although the
response rate (95%) was excellent (low nonresponder bias), this
survey was performed with residents at a single institution,
somewhat limiting generalizability. As the survey was admin-
istered after the American Board of Surgery In-Training Exam-
ination, test fatigue, anxiety, and mood may have influenced
survey responses resulting inunmeasuredbias. However, given
the completeness of data collection and exceptional response
rate, test fatigue is unlikely to have influenced the study find-
ings. Moreover, as the purpose of the study was to validate the
instrument, the direction of any potential bias on the individual
items would be unlikely to alter the validity of the study find-
ings. Furthermore, capturing a larger number of residents may
have improved the factor analysis. Also, the fact that the
mastery items did not load onto a single consistent factor sug-
gests that the adaptation of the original scale for these items
mayhavebeen testingdifferent components ofmastery, or that
the itemswere not sensitive enough to test the construct in this
population. Nonetheless, the results demonstrate that the
survey tool was able to differentiate between the mastery and
performance motivational constructs, and that surgical resi-
dents aremotivated in their learning, at least in part, by each of
these intrinsic orientations.
The strength of this pilot study is its unique perspective on
surgical education, whereby the trainees themselves are the
subject of the research rather than the subject being a new
educational model or style. This is the first time that GO has
been studied in residents, which is surprising given that sur-
gical residents are recognized as one of the most highly
motivated groups of students. As such, the instrument needs
to bemodified to better capture residents’mastery orientation
and validated in a larger population. Once validation is ach-
ieved, combining the adapted PALS with other validated
questionnaires to measure burnout, job satisfaction, leader-
ship, feedback quality, and professionalism related to the
management of competing priorities may identify more spe-
cific areas of intervention. For instance, awareness of GO and
the implications of each style may allow faculty and trainees
to develop more individualized and attainable goals that
would promote satisfaction and improved performance.
Understanding GO in residents is an interesting and
important new direction in surgical education research given
its potential effect on important components of the training
experience and its impact on future professional develop-
ment. This pilot study represents the first promising step in
this new area of research.
5. Conclusions
Understanding GO in surgical residents, a highly motivated,
unique population of students, is important to improve the
delivery of education. The adapted survey demonstrated high
and comparable reliability in two of three constructs. In this
population, mastery GO is a much more complex and so-
phisticated construct than can be measured with the current
adaptation. This pilot represents the first step in the adapta-
tion of a tool to identify potentially maladaptive mechanisms
of achievement.
Acknowledgment
Author contributions: R.L.H. and C.H.-R. were responsible for
conception and design. R.L.H., C.H.-R., and R.R.K. were
responsible for analysis and interpretation. R.L.H., J.D., R.R.K.,
and J.B.M. were responsible for data collection. R.L.H. and
R.R.K. participated in article writing. C.H.-R., J.D., J.B.M., and
R.R.K. involved in critical appraisal and revision.
r e f e r e n c e s
[1] Cordes CL, Dougherty TW. A review and integration ofresearch on job burnout. Acad Manage Rev 1993;18:621.
[2] Janssen O, Van Yperen NW. Employees’ goal orientation,the quality of leader-member exchange, and the outcomesof job performance and job satisfaction. Acad Manag J 2004;47:368.
[3] Harris BS, Smith ML. The influence of motivational climateand goal orientation on burnout: an exploratory analysisamong division I collegiate student-athletes. Athletic Insight2009;11. http://www.athleticinsight.com/.
[4] Elliot AJ, Harackiewicz JM. Approach and avoidanceachievement goals and intrinsic motivation: a meditationalanalysis. J Pers Soc Psychol 1996;70:461.
[5] Dweck CS. Motivational processes affecting learning. AmPsychol 1986;41:1040.
[6] Zweig D, Webster J. What are we measuring? Anexamination of the relationships between the big-fivepersonality traits, goal orientation, and performanceintentions. Person Individ Diff 2004;36:1693.
[7] VandeWalle D. A goal orientation model of feedback-seekingbehavior. Hum Res Manag Rev 2003;13:581.
[8] Leung A, Luu S, Regehr G, et al. First, do no harm: balancingcompeting priorities in surgical practice. Acad Med 2012;87:1368.
[9] Epstein RM, Siegel DJ, Silberman J. Self-monitoring in clinicalpractice: a challenge for medical educators. J Contin EducHealth Prof 2008;28:5.

j o u r n a l o f s u r g i c a l r e s e a r c h x x x ( 2 0 1 4 ) 1e66
[10] Payne SC, Youngcourt SS. A meta-analytic examination ofthe goal orientation Nomological Net. J Appl Psychol 2007;92:128.
[11] Surgical Council on Resident Education, SCORE. http://www.surgicalcore.org/index. Accessed 10/20/13.
[12] Midgley C, Maehr ML, Hruda LZ, et al. Manual for thepatterns of adaptive learning scales (PALS). Ann Arbor, MI:University of Michigan; 2000.
[13] Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG.Research electronic data capture (REDCap) - a metadata-driven methodology and workflow process for providingtranslational research informatics support. J Biomed Inform2009;42:377.
[14] Floyd FJ, Widaman KF. Factor analysis in the developmentand refinement of clinical assessment instruments. PsycholAssess 1995;7:286.
[15] Cortina JM. What is coefficient alpha? an examination oftheory and applications. J Appl Psychol 1993;78:98. 2007.
[16] Midgley C, Kaplan A, Middleton M, et al. Development andvalidation of scales assessing students’ achievement goalorientation. Contemp Educ Psychol 1998;23:113.
[17] Ryan AM, Hicks L, Midgley C. Social goals, academic goals,and avoiding seeking help in the classroom. J EarlyAdolescence 1997;17:152.
[18] Zweig DI, Webster J. Are goal orientation and self-efficacydifferent? A validation of scales. Paper presented at the 15th
annual meeting of the Society for Industrial andOrganizational Psychology, New Orleans, LA 2000.
[19] Swing S. The ACGME outcome project: a retrospective andprospective. Med Teach 2007;29:648.
[20] Joyce B. Introduction to competency-based residencyeducation: 2006 ACGME. http://ortho.ucsd.edu/educational/documents/CompetenciesforACGME.pdf. Accessed 5/6/13.
[21] Latham GP, Brown TC. The effect of learning vs. outcomegoals on self-efficacy, satisfaction and performance in anMBA program. App Psych Int Rev 2006;55:606.