Embed Size (px)
Citation preview
AUGUST 2005 • PODIATRY MANAGEMENTwww.podiatrym.com 187
and musculoskeletal conditions1-10.The modernization of the externalfixation apparatus and the configura-
tion of small, lightweight, bone fixa-tion or bone—lengthening deviceshave potentiated a myriad of utiliza-
tions in the forefoot. This article willexamine some of the different usagesof the mini-external fixators, includ-ing their role in hallux limitus,arthrodesis, non-union, osteomyelitis,and brachymetatarsia.
LigamentotaxisHallux limitus is a common dis-
order affecting the first metatarsalphalangeal joint (MTPJ) and is de-fined as a restriction in dorsiflexionof the hallux at the first MTPJ. Thisprogressive degenerative joint disor-der has long captured the interests of
Continued on page 188
Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Contin-uing Medical Education by the Council on Podiatric Medical Education.
You may enroll: 1) on a per issue basis (at $17.50 per topic) or 2) per year, for the special introductory rate of $109 (yousave $66). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the nearfuture, you may be able to submit via the Internet.
If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned cred-its. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test atno additional cost. A list of states currently honoring CPME approved credits is listed on pg. 196. Other than those entities cur-rently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be acceptable byany state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best efforts to ensurethe widest acceptance of this program possible.
This instructional CME program is designed to supplement, NOT replace, existing CME seminars. Thegoal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high quality manuscriptsby noted authors and researchers. If you have any questions or comments about this program, you can write or call us at: PodiatryManagement, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us at [email protected].
Following this article, an answer sheet and full set of instructions are provided (p. 196).—Editor
Continuing
Medical Education
Since the inception of externalskeletal fixation in the mid-nine-teenth century, there have been
a number of potentially revolutionaryadvances in both the design and ap-plication of external fixation. In addi-tion to its utilization in the manage-ment of traumatic fractures, externalfixation is also a critical technology inthe treatment algorithm of Charcotdeformity, limb lengthening, symp-tomatic non-union, mal-alignmentcorrection, as well as other congenital
By Charles Zelen, DPM, Glenn Wein-raub, DPM, Stephanie Wu, DPM
Use of Mini-ExternalFixation in
Forefoot Surgery
These lightweight devices haverevolutionized forefoot surgery.
Goals and Objectives
After reading this article, the pod-iatric physician should be able to:
1) Appreciate the advantagesand disadvantages for the use ofexternal fixation in foot andankle surgery.
2) Appreciate the various fore-foot applications for mini exter-nal fixators in podiatric surgery.
3) Understand the relative in-dications and contraindicationsfor as well as the limitations tothe use of external fixation in theforefoot.
Superficial pin tractinfections are an
accepted complication of callus distraction.
Use of Mini-ExternalFixation in
Forefoot Surgery
These lightweight devices haverevolutionized forefoot surgery.
S U R G I C A L P O D I A T R YS U R G I C A L P O D I A T R Y
trauma to the first metatarsal pha-langeal joint, septic arthritis, muscleimbalance, and metabolic/autoim-mune disorders.
The symptoms of hallux limi-tus vary depending on the degreeof joint degeneration, and stagingof the progression. Proposed treat-ments span the spectrum from con-servative care to surgical interven-
tion. The treatment algorithm isoften tailored to the progressivestate of the disease. Treatment goalsare primarily aimed at pain reduc-tion, and increased range of motionvia joint decompression. While nu-merous osteotomies have been pro-posed to achieve joint decompres-sion and improve range of motion,it is imperative to maintain boththe metatarsal parabola and jointstability about the first MTPJ.
Ligamentotaxis, or distractionof the first metatarsal phalangealjoint with a mini external fixator, isa relatively new approach for thetreatment of hallux limitus.11 Jointdistraction was first proposed in theankle joint as a disease modifyingtreatment of osteoarthritisis. Liga-mentotaxis is an extrapolation ofthe same principles onto the firstMTPJ for the treatment of halluxlimitus. Ligamentotaxis is based onthe hypothesis that arthrodiastasiswill release mechanical stress onthe osteoarthritic cartilage whilemaintaining intermittent intra-ar-ticular fluid pressure to help stimu-late the cartilage’s intrinsic repara-tive mechanism. In an in vitrostudy, low physiological levels ofintermittent fluid pressure, in theabsence of mechanical stress, werefound to stimulate cartilage matrixsynthesis in osteoarthritic cartilage,with no appreciable effect on nor-mal cartilage.12
This cartilage stimulation wasaccompanied by a decrease in theproduction of the catabolic cy-tokines interleukin 1 and tumornecrosis factor alpha; it had no de-tectable effect on the release of pro-teoglycans12. Proteoglycan aggre-gate is the major extra-cellular ma-trix component in cartilage. It com-prises about 18% of the dry weightof hyaline cartilage and plays amajor role in hyaline cartilage’sability to resist compression forces.Intermittent fluid pressure was alsonoted to reduce the inhibition ofproteoglycan synthesis that was in-duced by mononuclear cells isolat-ed from the synovial fluid of pa-tients with osteoarthritis12.
Joint distraction with an exter-nal fixator has considerable clinicalappeal as it is minimally invasiveand does not burn any bridges tofuture treatments. Even if this pro-
Continued on page 189
188 www.podiatrym.comPODIATRY MANAGEMENT • AUGUST 2005
Forefoot Surgery...
many. Several theories thatpostulate the etiopathogenesis of
hallux limitus have been suggested.These theories include met primus el-evatus, hypermobility associated withabnormal pronation, length aberra-tions of the first metatarsal or thefirst proximal phalanx, direct macro-
Contin
uing
Medica
l Edu
catio
n
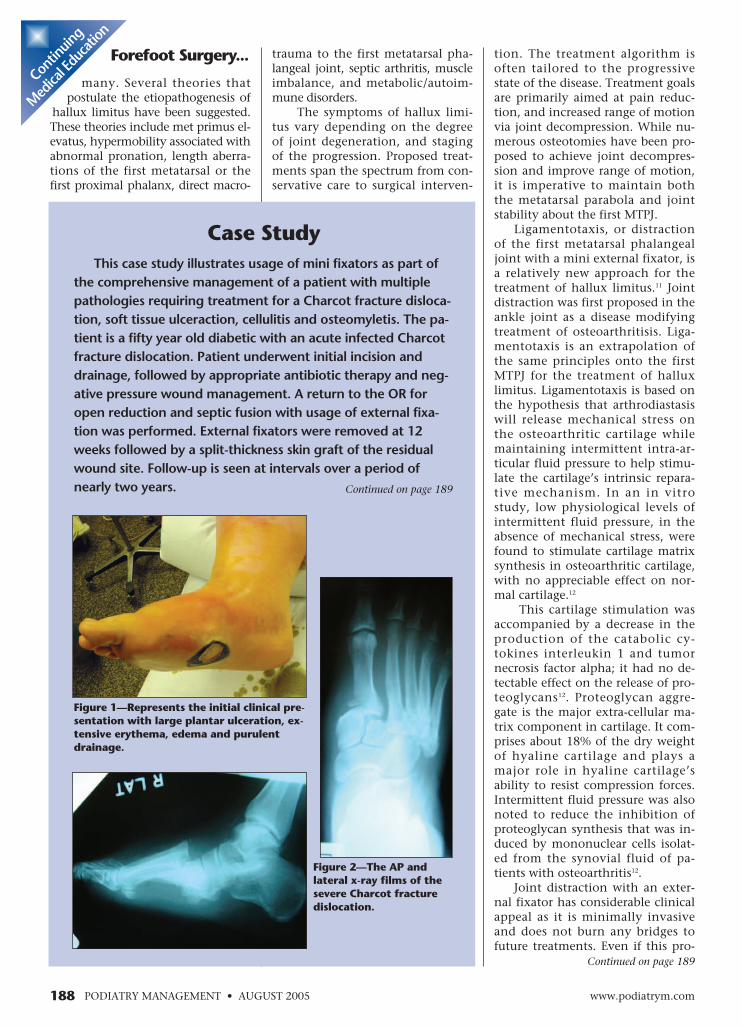
Case StudyThis case study illustrates usage of mini fixators as part of
the comprehensive management of a patient with multiplepathologies requiring treatment for a Charcot fracture disloca-tion, soft tissue ulceraction, cellulitis and osteomyletis. The pa-tient is a fifty year old diabetic with an acute infected Charcotfracture dislocation. Patient underwent initial incision anddrainage, followed by appropriate antibiotic therapy and neg-ative pressure wound management. A return to the OR foropen reduction and septic fusion with usage of external fixa-tion was performed. External fixators were removed at 12weeks followed by a split-thickness skin graft of the residualwound site. Follow-up is seen at intervals over a period ofnearly two years.
Figure 1—Represents the initial clinical pre-sentation with large plantar ulceration, ex-tensive erythema, edema and purulentdrainage.
Figure 2—The AP andlateral x-ray films of thesevere Charcot fracturedislocation.
Continued on page 189

cedure provides only temporary re-lief and clinical results slowly dete-riorate over time, it offers a mini-mally invasive option to forestallmore definitive and committedprocedures. Joint distraction utiliz-ing external fixation has demon-strated efficacy in the treatment ofankle osteoarthritis in preliminarystudies. In one open prospectivestudy with a 1+ year follow-up, sig-nificant decrease in pain and im-provement in function were notedin 75% of the 57 patients with se-vere ankle osteoarthritis who weretreated with joint distraction13.
Full weight-bearing and ambu-lation were permitted during thedistraction period. These patientsshowed radiographic evidence ofdiminished subchondral sclerosissecondary to the peri-articular os-teopenia during the distraction pe-riod, and progressive widening ofthe joint space on follow-up13. Al-though the results look promising,the follow-up period is relativelyshort and effects of this procedureover time remain unpredictable14.At present, there is no publisheddata pertaining to the applicationof this technique in the treatmentof hallux limitus or rigidus. Thistreatment protocol is still consid-ered experimental and further re-search and analysis are necessary tounderstand, validate and refine thisnovel approach to first MTPJ os-teoarthritis.
BrachymetatarsiaBrachymetatarsia is a common
anomaly in which one or more ofthe metatarsal bones is abnormallyshort, resulting in a short toe.Brachymetatarsia most commonlyinvolves the fourth metatarsal and isbelieved to be secondary to prema-ture closure of the ephiphysealplate. It is normally idiopathic, but
may be associated with Down’s syn-drome, pseudo-hypoparathyroidism,Turner's syndrome, or Albright’shereditary osteodystrophy. Al-though brachymetatarsia is oftenconsidered a cosmetic problem, inmany instances there is painfulpathology associated with the short-ened metatarsal. Palliative treat-ments, including the use of orthoticor accommodative devices, may alle-viate the symptoms but do not solvethe underlying structural deformityand its associated psychologicalproblems. Through the years, therehave been a number of soft tissue
AUGUST 2005 • PODIATRY MANAGEMENTwww.podiatrym.com 189
Forefoot Surgery... and osseous proceduresproposed for the correctionof brachymetatarsia.
Traditionally, brachymetatar-sia has been surgically correctedusing one stage or two stage length-ening procedures with an interposi-tional bone graft, or synthetic im-plant. The amount of lengthening,however, was often limited by vas-cular structures. Elongation of themetatarsal using an external fixatorwas first reported by Skirving andNewman15. With evolution of theexternal fixator apparatus, gradualmetatarsal lengthening by callusdistraction or callotasis has gainedpopularity over the past twodecades. Both the latency periodand the rate of lengthening varyslightly in current literature. Therecommended latency periodranges between 5-10 days, and therate of lengthening ranges between0.5 mm to 1.0 mm/day14-20. Theconsolidation period is usually 6-8weeks.
ComplicationsCompared to the interpositional
bone graft or synthetic implant tech-niques, callus distraction preservesthe periosteal structures21 and is asafer and less traumatic option forthe treatment of brachymetatarsia.
Callotasis is, however, not voidof limitations and complications.As with any lengthening procedure,callus distraction of the metatarsalrequires careful monitoring of theprogress throughout both the dis-
traction and theconso l ida t ionphase. Many au-thors advocatesetting a ceilingon the maxi-mum amount ofl e n g t h e n i n g ,suggesting thatlengthening notexceed 40% ofthe originallength of themetatarsal15,16. Incases wherem e t a t a r s a llengthening ex-ceeded 40% ofthe pre-operativelength, signifi-cant metatarsal
Continuing
Medical Education
Post-operatively,external fixation as
compared to a plaster cast allows
for better care of skinand soft tissues.
Figure 3—Represents the patient status-postincision and drainage, with exposure of dislo-cated medial cuneiform.
Figure 4—Represents open reduction andseptic fusion of Charcot fracture dislocation.
Continued on page 190
Case Study (Continued)
Continued on page 190Continued on page 190

minor degrees of lengthening arerequired to prophylactically pre-vent symptomatic subluxation oraxial deviation of the joint.
Decreased range of motionabout the corresponding metatarsalphalangeal joint is a common com-plication following metatarsallengthening15,16,19. While normaljoint range of motion was neverachieved at follow-up in many pa-tients, most patients who arepleased with their improved cosmet-ic appearance are not bothered bythe lesser metatarsal joint limitus19.
Superficial pin tract infectionsare an accepted compli-cation of callus distrac-tion and are consideredby some authors to be anatural sequela of usingexternal fixation22. Com-plete resolution can usu-ally be achieved withlocal pin care and theadministration of oralantibiotics.
The use of callus dis-traction, via mini exter-nal fixation to help re-store the metatarsalparabola, requires bothexact control of theamount of distractionand scrupulous attentionto local factors. Althoughthere are complications,they may be minimizedby adjuvant soft tissueprocedures, and carefulmonitoring of theprogress throughout dis-traction and consolida-tion. As always, patientselection is extremely im-portant as compliance isa critical factor in thesuccess of this procedureand not every patient is acandidate for externalfixation.
Osteomyelitic BoneResection
Extrapolating on thebasic principles of exter-nal fixation, mini fixa-tors are often adapted forutilization in a variety offorefoot scenarios. Onesuch principle is themaintenance of length,
langeal joint, decreased range of mo-tion about the corresponding MTPJ,narrowing of the joint space, and ofcourse, pin tract infections15-20.
Subluxation or axial deviationof the corresponding metatarsalphalangeal joint is believed to besecondary to tension from tendonsand surrounding soft tissue struc-tures. Concomitant soft tissue re-leases, such as tendon lengtheningand stabilization of the metatarsalphalangeal joint with a K-wire,have been suggested19,20. These ad-junctive soft tissue releases are rec-ommended even in cases where
190 www.podiatrym.comPODIATRY MANAGEMENT • AUGUST 2005
Forefoot Surgery...
angulation was noted, alongwith large increases in joint stiff-
ness15,16. Recent studies advocatecombining shortening osteotomiesof adjacent metatarsals and pha-langes with metatarsal lengtheningto help avoid the associated com-plications of over—lengthening, yetstill establish an acceptablemetatarsal parabola17,18.
Other possible complications as-sociated with callus distraction in-clude subluxation or axial deviationof the associated metatarsal pha-
Contin
uing
Medica
l Edu
catio
n
Figure 8—Represents the opendorsal wound with exposed ante-rior tibial tendon, six weeks sta-tus post surgical reconstruction.
Figure 6—Represents the dorsal andlateral wound two weeks after openreduction and septic fusion.
Figure 7—Represents negative pressure woundmanagement and electrical bone stimulation aspart of the comprehensive management of thispatient.
Figure 5—Represents the immediate post-op-erative x-rays status post surgical reductionand fusion.
Continued on page 191
Case Study (Continued)
Continued on page 191
AUGUST 2005 • PODIATRY MANAGEMENTwww.podiatrym.com 191
delayed interpositional autogeneousgraft arthrodesis was performed fourweeks later24.
Another case study demonstrat-ed similar success in preservation ofthe first ray in a vascular insuffi-cient diabetic patient with a pene-trating ulcer and osteomyelitis ofthe first metatarsophalangealjoint25. External fixation providedstability to the resected joint and
especially about the first ray. Stageddebridement-arthrodesis has beenproposed as a first ray salvage pro-cedure in the treatment of os-teomyelitis and sepsis about thefirst MTPJ23-26. The initial salvagetreatment includes debridement ofall infected/necrotic osseous/softtissue structures, followed by place-ment of an antibiotic im-pregnated bone cementspacer23. Soft tissue con-tracture is a common oc-currence following the ex-cision of bone. Before theadvent of mini externalfixators, K-wires were mostoften used to help main-tain length while scar tis-sue fills up the void. Thesecond stage of the proce-dure, which usually occurs3-4 weeks later with clini-cal evidence of infectioncontrol, consists of bonecement and fixation re-moval and arthrodesis forthe first MTPJ with a bonegraft23.
External fixators are ef-ficacious at maintaininglength and are often usedfor this purpose, especiallywhen bone infections areinvolved. Several authorshave demonstrated suc-cessful use of external fixa-tion as part of the forefootsalvage procedure.
A mini external fixatorwas utilized as part of astaged treatment algorithmin a recently published casereport of first ray salvage ina diabetic patient with os-teomyelitis24. The patientpresented with a septic firstmetatarsal phalangeal jointand associated osteomyeli-tis of adjacent osseousstructures. A mini externalfixator was used followingaggressive debridementand placement of antibiot-ic impregnated polymethylmethacrylate bone cement.The mini external fixatorhelped maintain the fulllength of the first ray seg-ment until the infectionwas well-controlled and a
Forefoot Surgery... was left intact for fourweeks. This helped result inpermanent control of infec-tion and preservation of the hal-lux without recurrence of os-teomyelitis or ulceration25.
Similar success has been shownin fingers and hands. In a retro-spective study, the finger joints often patients with acute bacterialarthritis were surgically debrided
and stabilized, using a miniexternal fixation device forabout three weeks, withsubsequent fixation. Eightof the ten patients showedgood final results withoutsymptoms26.
Since preservation andcorrect alignment of the firstray is essential for foot stabil-ity, mini external fixationmay play an important rolein the limb salvage aboutthe first ray. First metatarsal-medial cuneiform fusionsand first metatarsal pha-langeal joint arthrodesis
First metatarsal-medialcuneiform fusion orlapidus arthrodesis is apowerful procedure indi-cated for the treatment ofhallux valgus with a highintermetatarsal angle andassociated hypermobility ofthe first ray. The metatar-socuneiform arthrodesiscorrects metatarsal primusadductus, and allows re-alignment of the firstmetatarsal at the apex ofthe deformity, along withstabilization of the first rayand medial column.
Arthrodesis of the firstmetatarsophalangeal jointhas been proposed as adefinitive procedure for se-vere hallux valgus, halluxrigidus, and rheumatoidarthritis. It was first de-scribed by Clutton in 1894,and since then has had sev-eral modifications by nu-merous authors.
Mini external fixatorsmay serve as alternatemodes of fixation for bothmetatarsal phalangeal jointfusions27-29 and firstmetatarsal-medial cuneiform
Continued on page 192
Continuing
Medical Education
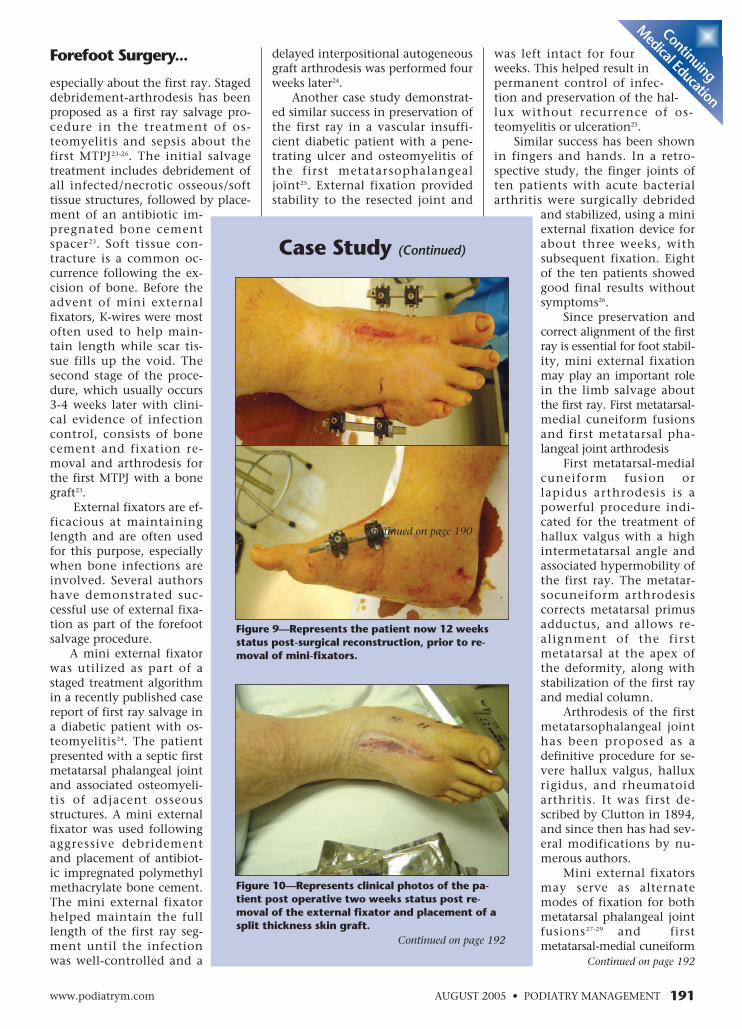
Figure 9—Represents the patient now 12 weeksstatus post-surgical reconstruction, prior to re-moval of mini-fixators.
Case Study (Continued)
Figure 10—Represents clinical photos of the pa-tient post operative two weeks status post re-moval of the external fixator and placement of asplit thickness skin graft.
Continued on page 192
Continued on page 190
Surgical management of an in-fected fusion varies depending onthe clinical presentation and thepresence of a solid arthrodesis. Anestablished bone infection early inthe bone healing phase may requirehardware removal to eliminate thenidus for continued infection. Inthese situations, a small monorailexternal fixator may be used to sta-bilize and distract the arthrodesissite after adequate bone debride-ment. The fusion site is distracteduntil the infection is controlled. Abone graft may then be inserted atthe fusion site and the mini exter-nal fixator utilized once again to
apply compression across thearthrodesis site. Septic joint de-struction presents an unfavor-able situation of soft tissues andchronic osteomyelitis and is as-sociated with high failure ratesof fusions. External fixation hasbeen shown to be a successfulalternative for arthrodeses inthese types of situations. In aprospective study, 15 patientswith bone and soft tissue infec-tions received ankle arthrodesisvia external fixation. Solid tibio-talar fusion was achieved andmaintained in 14 of the 15 pa-tients with a full weight-bearingstatus at one year follow-up31.
Fracture ManagementFractures of the metatarsals
and phalanges have traditionallybeen fixated with pins, wires,and screws. Mini external fixa-tion offers a viable alternative totraditional fixation methods forforefoot fractures. It avoids inter-nal dissection, yet provides frac-ture stability and allows earlymovement with mobilization ofjoints proximal and distal to thefracture32. Mini external fixatorsalso allow an avenue of fixationfor highly comminuted fracturesor complex intra-articular frac-tures that are not amenable tointernal fixation.
Intra-operatively, externalfixators can also serve as a tem-porary traction device to helpcondition the soft tissues and asa temporary distraction deviceto aid in reduction. Post-opera-tively, external fixation as com-pared to a plaster cast allows for
Continued on page 193
192 www.podiatrym.comPODIATRY MANAGEMENT • AUGUST 2005
Forefoot Surgery...
fusions29. This is especially truein patients who are not able to
maintain the long non-weight-bear-ing, post-operative recovery. Mini ex-ternal fixators, however, often playcritical roles in the treatment of post-operative complications such as non-unions and bone infections.
Delayed union or non-union isa well-known complication associ-ated with Lapidus. The incidence ofnon unions has been quoted ashigh as 12 percent. Mini externalfixators are often employed in thesurgical treatment of symptomatic
Contin
uing
Medica
l Edu
catio
n
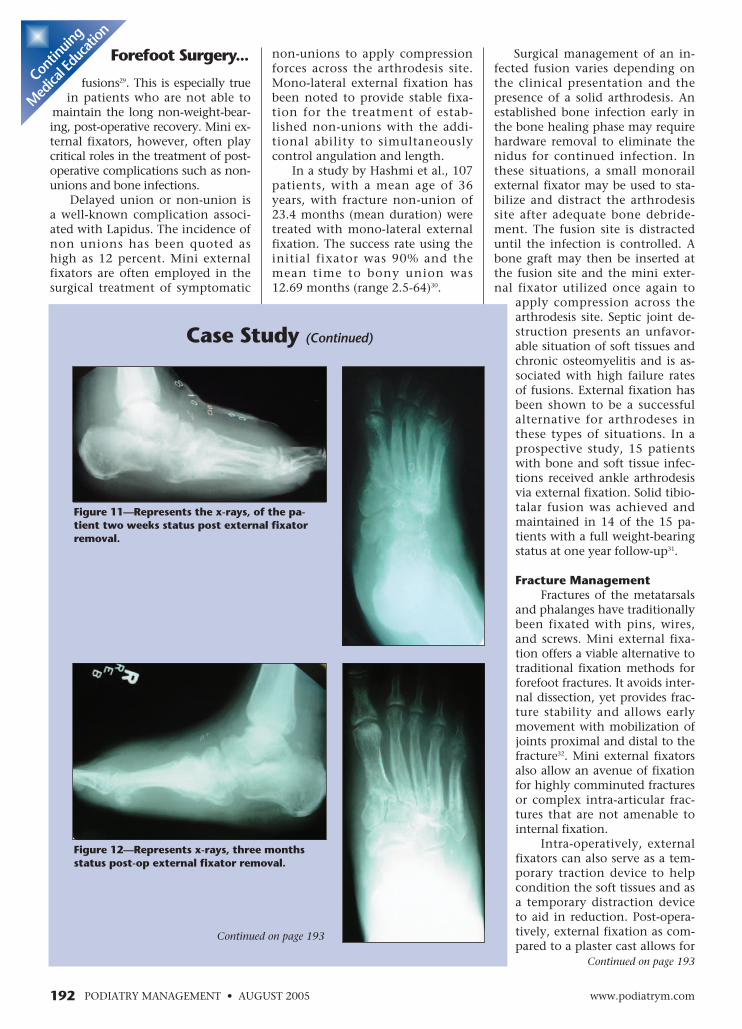
Figure 11—Represents the x-rays, of the pa-tient two weeks status post external fixatorremoval.
non-unions to apply compressionforces across the arthrodesis site.Mono-lateral external fixation hasbeen noted to provide stable fixa-tion for the treatment of estab-lished non-unions with the addi-tional ability to simultaneouslycontrol angulation and length.
In a study by Hashmi et al., 107patients, with a mean age of 36years, with fracture non-union of23.4 months (mean duration) weretreated with mono-lateral externalfixation. The success rate using theinitial fixator was 90% and themean time to bony union was12.69 months (range 2.5-64)30.
Case Study (Continued)
Figure 12—Represents x-rays, three monthsstatus post-op external fixator removal.
Continued on page 193
AUGUST 2005 • PODIATRY MANAGEMENTwww.podiatrym.com 193
SummaryExternal skeletal fixation is
unique in that it offers the flexibili-ty of additional compression or dis-traction at the clinician’s discretionin addition to applying stable, uni-form compression of osseous frag-ments. External fixation also offersmany advantages over traditionaltechniques of internal fixation, es-pecially in patients where adequatecompression is not achievable, suchas those with poor bone stock, pa-
better care of skin and soft tissues.In a recently published study,
ten patients with a mean age of25.2 years underwent external fixa-tion for acute Jones fractures. Clini-cal and radiography healing timeswere 5.7 and 6.5 weeks respectively.The mean follow-up was 46months and all patients were painfree and were able to resume theirpre-injury activity levels33.
Forefoot Surgery... tients who for one rea-son or another are unableto remain non-weight-bear-ing, or in cases where a deformi-ty limits access for proper, accuratefixation with appropriate anatomicreconstruction. Because of its versa-tility, external fixation is often se-lected as the alternative or remedytype of fixation.
Mini external fixators, when ap-plied correctly, may have numerousutilizations in the forefoot. They
provide excellentstability for fixationosteotomies andarthrodesis andallow patients toparticipate in theirown care. Externalfixation, however, isnot the universal an-swer for fixation ofbone. External fixa-tion is not for every-one. Contraindica-tions that includemoderate to severeperipheral arterialdisease without vas-cular surgical inter-vention, mental in-competence, andpsychological intol-erance to the frame,can be limiting fac-tors for utilization ofthis type of fixation.
The under-standing of the con-ditions under whichbone and soft tissuecan be regeneratedby distraction hasinspired differentapplications of thedistraction tech-niques with somepromising results. Asthe evolution of ex-ternal fixation con-tinues through re-search and develop-ment, new clinicalpossibilities of indi-cations and usageexpand. Further re-search and develop-ment with externalfixation needs to beperformed, and withtime, this treatment
Continuing
Medical Education
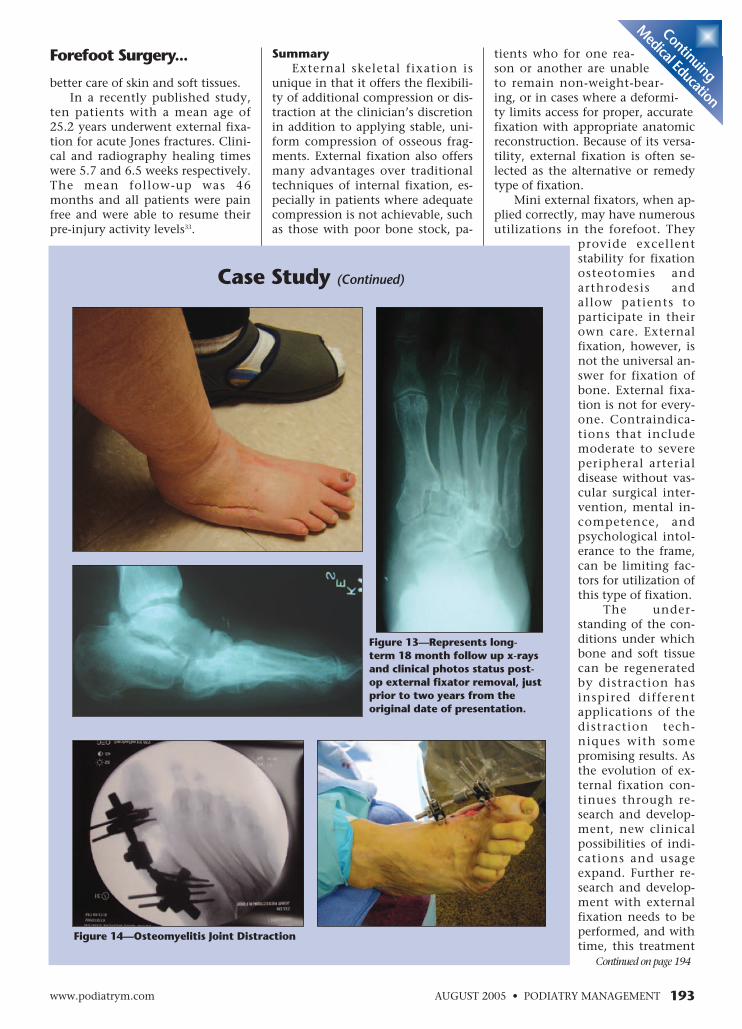
Figure 14—Osteomyelitis Joint Distraction
Case Study (Continued)
Figure 13—Represents long-term 18 month follow up x-raysand clinical photos status post-op external fixator removal, justprior to two years from theoriginal date of presentation.
Continued on page 194

spective study and in a randomizedcontrolled study, Arthritis Rheum. 2002Nov;46(11):2893-902.
14 van Roermund PM, MarijnissenAC, Lafeber FP, Joint distraction as analternative for the treatment of os-teoarthritis, Foot Ankle Clin. 2002Sep;7(3):515-27.
15 Masada K, Fujita S, Fuji T, Ohno H,Complications following metatarsallengthening by callus distraction forbrachymetatarsia, J Pediatr Orthop. 1999May-Jun;19(3):394-7.
16 Song HR, Oh CW, Kyung HS, KimSJ, Guille JT, Lee SM, Kim PT, Fourthbrachymetatarsia treated with distractionosteogenesis, Foot Ankle Int. 2003Sep;24(9):706-11.
17 Kim HT, Lee SH, Yoo CI, Kang JH,Suh JT, J Bone Joint Surg Br. 2003Jul;85(5):683-90.
18 Schimizzi A, Brage M,Brachymetatarsia, Foot Ankle Clin. 2004Sep;9(3):555-70, ix.
19 Kawashima T, Yamada A, Ueda K,Harii K, Treatment of brachymetatarsia bycallus distraction (callotasis), Ann PlastSurg. 1994 Feb;32(2):191-9.
20 Wada A, Bensahel H, TakamuraK, Fujii T, Yanagida H, Nakamura T,Metatarsal lengthening by callus dis-traction for brachymetatarsia, J Pedi-atr Orthop B. 2004 May;13(3):206-10.
21 Sen C, Kocaoglu M, Eralp L, CinarM, Bone lengthening of congenitallyshort metacarpus and metatarsus by thecallus distraction technique, Acta OrthopTraumatol Turc. 2003;37(2):154-61.
22 Cierny G 3rd, Zorn KE. Segmentaltibial defects. Comparing conventionaland Ilizarov methodologies. Clin Orthop1994; 301: 118-23.
23 Myerson MS, Miller SD, HendersonMR, Saxby T, Staged arthrodesis for sal-vage of the septic hallux metatarsopha-langeal joint, Clin Orthop. 1994Oct;(307):174-81.
24 Roukis TS, Landsman AS, Salvage ofthe first ray in a diabetic patient with os-teomyelitis, J Am Podiatr Med Assoc. 2004Sep-Oct;94(5):492-8.
25 Ris HB, Reber P, Preservation of thefirst ray in a diabetic patient with a pene-trating ulcer and arterial insufficiency byuse of debridement and external fixation,Eur J Vasc Surg. 1994 Jul;8(4):514-6.
26 de Vries H, van der Werken C,Treatment of septic arthritis of the handusing temporary intermittent immobi-lization with an external fixator, Ned Ti-jdschr Geneeskd. 1995 Aug5;139(31):1592-5.
27 Sharon SM, McClain J, An alterna-tive fixation technique when perform-ing hallux interphalangeal joint fusions,J Foot Surg. 1985 Mar-Apr;24(2):132-5
28 Calderone DR, Wertheimer SJ, Firstmetatarsophalangeal joint arthrodesis uti-
lizing a mini-Hoffman External Fixator, JFoot Ankle Surg. 1993 Sep-Oct;32(5):517-25.
29 Zgonis T, Jolly GP, Blume P, Exter-nal fixation use in arthrodesis of the footand ankle, Clin Podiatr Med Surg. 2004Jan;21(1):1-15
30 Hashmi MA, Ali A, Saleh M, Man-agement of non-unions with mono-lateralexternal fixation, Injury. 2001 Dec;32Suppl 4:SD30-4.
31 Kollig E, Esenwein SA, Muhr G,Kutscha-Lissberg F, Fusion of the septicankle: experience with 15 cases using hy-brid external fixation, J Trauma. 2003Oct;55(4):685-91.
32 Seibert FJ, Fankhauser F, Elliott B,Stockenhuber N, Peicha G, External fixa-tion in trauma of the foot and ankle, ClinPodiatr Med Surg. 2003 Jan;20(1):159-80.
33 Lombardi CM, Connolly FG, Sil-hanek AD, The use of external fixationfor treatment of the acute Jones frac-ture: a retrospective review of 10 cases, JFoot Ankle Surg. 2004 May-Jun;43(3):173-8.
194 www.podiatrym.comPODIATRY MANAGEMENT • AUGUST 2005
Forefoot Surgery...
will more than likely becomefully integrated into modern
clinical practice. ■
References1 Paul GW, The history of external fix-
ation, Clin Podiatr Med Surg. 2003Jan;20(1):1-8, v.
2 Heini PF, Gahrich U, Orler R, Theexternal fixator: a tool for evaluation ofcomplex low back pain problems, J SpinalDisord Tech. 2004 Feb; 17(1):8-14.
3 Cooper PS: Application of externalfixators for management of Charcot de-formities of the foot and ankle. FootAnkle Clin7:207-254, 2002.
4 Brinker MR, O'Connor DP, Ilizarovcompression over a nail for asepticfemoral nonunions that have failed ex-change nailing: a report of five cases. J Or-thop Trauma. 2003 Nov-Dec;17(10):668-76.
5 Saleh M, Yang L, Sims M, Limb re-construction after high energy trauma, BrMed Bull. 1999;55(4):870-84.
6 Lourie GM, Lins RE, Static externalfixation in the hand and carpus, HandClin. 1997 Nov;13(4):627-42.
7 LaBianco GJ, Vito GR, Kalish SR, Useof the Ilizarov external fixator in the treat-ment of lower extremity deformities, J AmPodiatr Med Assoc. 1996 Nov;86(11):523-31.
8 Kristiansen LP, Steen H, The Ilizarovexternal fixator and method. Treatmentof congenital and acquired deformities,Tidsskr Nor Laegeforen. 1996 Apr20;116(10):1216-8.
9 Lonner JH, Koval KJ,Golyakhovsky V, Frankel VH, Posttrau-matic nonunion of the distal tibialmetaphysis. Treatment using theIlizarov circular external fixator, Am JOrthop. 1995 May;Suppl:16-21.
10 Baker MJ, Offutt SM, External fixa-tion indications and patient selection, ClinPodiatr Med Surg. 2003 Jan;20(1):9-26.
11 Vito GR: Ligamentotaxis for halluxrigidus with external fixation. Paper pre-sented at the American College of Footand Ankle Surgeons Annual Meeting andScientific Seminar, February 12, 2000,Miami.
12 Van Valburg AA, van Roy HL,Lafeber FP, Bijlsma JW. Beneficial effectsof intermittent fluid pressure of lowphysiological magnitude on cartilageand inflammation in osteoarthritis. Anin vitro study, J Rheumatol. 1998Mar;25(3):515-20.
13 Marijnissen AC, Van RoermundPM, Van Melkebeek J, Schenk W, Ver-bout AJ, Bijlsma JW, Lafeber FP, Clinicalbenefit of joint distraction in the treat-ment of severe osteoarthritis of theankle: proof of concept in an open pro-
Contin
uing
Medica
l Edu
catio
n
Dr. Wu is Assis-tant Professor,Department ofSurgery at theDr. William M.Scholl Collegeof PodiatricMedicine atR o s a l i n dFranklin Uni-versity of Medi-cine and Science and is Fellow at theCenter for Lower Extremity Ambula-tory Research (CLEAR) at RosalindFranklin University.
Dr. Weinraub is Assistant ClinicalProfessor, Department of InternalMedicine at the University of VASchool of Medicine and Clinical Assis-tant Professor, Orthopaedic/PodiatricSurgery at the Virginia College of Os-teopathic Medicine.
Dr. Zelen is As-sistant ClinicalProfessor ofMedicine at theUniversity ofVirginia Schoolof Medicine,Chief of thePodiatry Sectionof the Depart-ment of Surgeryat Roanoke Memorial Hospital, andChief of the Podiatry Section of the De-partment of Orthopedics at Lewis GaleHospital. He is currently vice-presidentof the Virginia Podiatric Medical Asso-ciation and a Fellow of the AmericanProfessional Wound Care Association.
AUGUST 2005 • PODIATRY MANAGEMENTwww.podiatrym.com 195
A) skinB) boneC) vascular structuresD) patient tolerance
7) Mini external fixation may be aviable alternative to traditional fix-ation methods for forefoot frac-tures because
A) it avoids internal dissectionB) it allows early movementwith mobilization of jointsproximal and distal to the frac-tureC) it allows an avenue of fixa-tion for highly comminutedfractures or complex intra-ar-ticular fractures that are notamenable to internal fixation.D) all of the above
8) When using callus distractionfor the treatment ofbrachymetatarsia, many authorssuggest that lengthening not ex-ceed what percentage of the origi-nal length of the metatarsal?
A) 20%B) 40%C) 60%D) 80%
9) Possible complications associat-ed with callus distraction for thetreatment of brachymetatarsia in-clude:
A) subluxation or axial devia-tion of the associatedmetatarsal-phalangeal jointB) decreased range of motionabout the corresponding MTPJC) narrowing of the joint spaceD) all of the above
10) Ligamentotaxis is based on which of the following hypothesis?
A) arthrodiastasis will releasemechanical stress on the os-teoarthritic cartilage whilemaintaining intermittent intra-articular fluid pressure to helpstimulate the cartilage’s intrin-sic reparative mechanismB) arthrodiastasis will stretchthe soft tissues structures sur-rounding the joint to allow for
1) External fixation may be utilizedin the management of which ofthe following?
A) congenital and muscu-loskeletal conditionsB) Charcot deformityC) symptomatic nonunionD) all of the above
2) A mini external fixator may beutilized in the management of allof the following except:
A) brachymetatarsiaB) forefoot non unionsC) ankle arthrodesisD) forefoot fractures
3) Joint distraction was first pro-posed as a treatment for os-teoarthritis in which of the follow-ing joints?
A) kneeB) ankleC) hipD) first metatarsal-phalangealjoint
4) External fixation may be advan-tageous over traditional tech-niques of internal fixation in whichof the following situations?
A) patients with poor bonestockB) patient unable to maintainnon weight bearingC) it offers the flexibility of ad-ditional compression or distrac-tion at the clinician’s discretionD) all of the above
5) All of the following are con-traindications to external fixationuse except
A) severe to moderate periph-eral arterial disease withoutvascular surgical interventionB) there are no contraindica-tions, external fixation is for ev-eryoneC) mental incompetenceD) psychological intolerance tothe frame.
6) In treating brachymetatarsia,the amount of lengthening is mostlikely limited by which of the fol-lowing?
greater, pain free range of motionC) arthrodiastasis will limit mo-tion across the joint and ensurepatient complianceD) all of the above are correct
11) Joint distraction with an exter-nal fixator for the treatment of os-teoarthritis may have considerableclinical appeal because
A) it is minimally invasiveB) it does not burn any bridgesto future treatmentsC) it offers a way to forestallmore definitive and committedproceduresD) all of the above
12) Which of the following may beconsidered an accepted complica-tion of using external fixation andis considered by some authors tobe a natural sequela of using exter-nal fixation?
A) breakage of wires and pinsB) higher incidence of falls andinjuriesC) superficial pin tract infec-tionsD) all of the above
13) Successful use of callus distrac-tion via mini external fixation in thetreatment of brachymetatarsia de-pends on which of the following?
A) exact control of the amountof distractionB) careful monitoring of theprogress throughout distrac-tion and consolidationC) patient selectionD) all of the above
14) The role of mini external fixa-tion in the treatment of forefootosteomyelitis is to
A) Maintain length after boneresection to prevent soft tissuecontractureB) Provide easy access to thewound to facilitate physicianmonitoringC) To facilitate post-operativedressing changesD) All of the above
Continuing
Medical Education
E X A M I N A T I O N
See answer sheet on page 197.
Continued on page 196
196 PODIATRY MANAGEMENT • AUGUST 2005
15) With regard to arthrodesis of the firstmetatarsal-cuneiform joint or the first metatarsal-phalangeal joint, a mini external fixator may beused
A) as an alternate mode of fixation for thearthrodesisB) in the treatment of non unionsC) in the treatment of post-operative bone in-fectionsD) all of the above
16) When using callus distraction for the treat-ment of brachymetatarsia, over-lengthening ofthe affected metatarsal (beyond the recommend-ed length) would most likely result in which of thefollowing?
A) narrowing of joint spaceB) metatarsal angulation with large increasesin joint stiffnessC) pin tract infectionsD) all of the above
17) When using callus distraction for the treat-ment of brachymetatarsia, the recommended la-tency period
A) ranges between 1-2 daysB) ranges between 5-10 daysC) ranges between 1-2 monthsD) ranges between 5-10 months
18) Mini external fixators may be employed in thesurgical treatment of symptomatic non-union to
A) apply compression forces across thearthrodesis siteB) provide stable fixationC) simultaneously control angulation andlengthD) all of the above
19) When using callus distraction for the treat-ment of brachymetatarsia, the rate of metatarsallengthening usually ranges between
A) 0.5 mm to 1.0 mm/dayB) 1.0 mm to 2.0 mm/dayC) 0.5 cm to 1.0 cm/dayD) 1.0 cm to 2.0 cm/day
20) When using callus distraction for the treat-ment of brachymetatarsia, adjunctive soft tissueprocedures are often recommended to help pre-vent which of the following?
A) Pin tract infectionsB) Narrowing of joint spaceC) subluxation or axial deviation of the jointD) all of the above
E X A M I N A T I O N
(cont’d)
See answer sheet on page 197.
Contin
uing
Medica
l Edu
catio
n
PM’sCPME Program
Welcome to the innovative Continuing EducationProgram brought to you by Podiatry ManagementMagazine. Our journal has been approved as asponsor of Continuing Medical Education by theCouncil on Podiatric Medical Education.
Now it’s even easier and more convenientto enroll in PM’s CE program!
You can now enroll at any time during the yearand submit eligible exams at any time during yourenrollment period.
PM enrollees are entitled to submit ten examspublished during their consecutive, twelve–monthenrollment period. Your enrollment period beginswith the month payment is received. For example,if your payment is received on September 1, 2003,your enrollment is valid through August 31, 2004.
If you’re not enrolled, you may also submit anyexam(s) published in PM magazine within the pasttwelve months. CME articles and examinationquestions from past issues of Podiatry Man-agement can be found on the Internet athttp://www.podiatrym.com/cme. All lessonsare approved for 1.5 hours of CE credit. Please readthe testing, grading and payment instructions to de-cide which method of participation is best for you.
Please call (631) 563-1604 if you have any ques-tions. A personal operator will be happy to assist you.
Each of the 10 lessons will count as 1.5 credits;thus a maximum of 15 CME credits may beearned during any 12-month period. You may se-lect any 10 in a 24-month period.
The Podiatry Management Magazine CMEprogram is approved by the Council on PodiatricEducation in all states where credits in instruction-al media are accepted. This article is approved for1.5 Continuing Education Contact Hours (or 0.15CEU’s) for each examination successfully completed.
PM’s CME program is valid in all statesexcept Kentucky.
www.podiatrym.com
Home Study CME credits nowaccepted in Pennsylvania
Over, please
Please print clearly...Certificate will be issued from information below.
Name _______________________________________________________________________Soc. Sec. #______________________________Please Print: FIRST MI LAST
Address_____________________________________________________________________________________________________________
City__________________________________________________State_______________________Zip________________________________
Charge to: _____Visa _____ MasterCard _____ American Express
Card #________________________________________________Exp. Date____________________
Note: Credit card payment may be used for fax or phone-in grading only.
Signature__________________________________Soc. Sec.#______________________Daytime Phone_____________________________
State License(s)___________________________Is this a new address? Yes________ No________
Check one: ______ I am currently enrolled. (If faxing or phoning in your answer form please note that $2.50 will be charged to your credit card.)
______ I am not enrolled. Enclosed is a $17.50 check payable to Podiatry Management Magazine for each exam submitted. (plus $2.50 for each exam if submitting by fax or phone).
______ I am not enrolled and I wish to enroll for 10 courses at $109.00 (thus saving me $66 over the cost of 10 individual exam fees). I understand there will be an additional fee of $2.50 for any exam I wish to submit via fax or phone.
Note: If you are mailing your answer sheet, you must completeall info. on the front and back of this page and mail with yourcheck to: Podiatry Management, P.O. Box 490, East Islip,NY 11730. Credit cards may be used only if you are faxing orphoning in your test answers.
TESTING, GRADING AND PAYMENT INSTRUCTIONS(1) Each participant achieving a passing grade of 70% or
higher on any examination will receive an official computer formstating the number of CE credits earned. This form should be safe-guarded and may be used as documentation of credits earned.
(2) Participants receiving a failing grade on any exam will benotified and permitted to take one re-examination at no extra cost.
(3) All answers should be recorded on the answer formbelow. For each question, decide which choice is the best an-swer, and circle the letter representing your choice.
(4) Complete all other information on the front and back ofthis page.
(5) Choose one out of the 3 options for testgrading: mail-in,fax, or phone. To select the type of service that best suits yourneeds, please read the following section, “Test Grading Options”.
TEST GRADING OPTIONSMail-In GradingTo receive your CME certificate, complete all information
and mail with your check to:Podiatry Management
P.O. Box 490, East Islip, NY 11730There is no charge for the mail-in service if you have already
enrolled in the annual exam CPME program, and we receive this
E N R O L L M E N T F O R M & A N S W E R S H E E T
✄
197
Continuing
Medical Education
exam during your current enrollment period. If you are not en-rolled, please send $17.50 per exam, or $109 to cover all 10exams (thus saving $66 over the cost of 10 individual exam fees).
Facsimile GradingTo receive your CPME certificate, complete all information and
fax 24 hours a day to 1-631-563-1907. Your CPME certificate willbe dated and mailed within 48 hours. This service is available for$2.50 per exam if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment period),and can be charged to your Visa, MasterCard, or American Express.
If you are not enrolled in the annual 10-exam CPME pro-gram, the fee is $20 per exam.
Phone-In GradingYou may also complete your exam by using the toll-free ser-
vice. Call 1-800-232-4422 from 10 a.m. to 5 p.m. EST, Mondaythrough Friday. Your CPME certificate will be dated the same dayyou call and mailed within 48 hours. There is a $2.50 charge forthis service if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment peri-od), and this fee can be charged to your Visa, Mastercard, Ameri-can Express, or Discover. If you are not currently enrolled, the feeis $20 per exam. When you call, please have ready:
1. Program number (Month and Year)2. The answers to the test3. Your social security number4. Credit card information
In the event you require additional CPME information,please contact PMS, Inc., at 1-631-563-1604.
Enrollment/Testing Informationand Answer Sheet
✄
198 www.podiatrym.comPODIATRY MANAGEMENT • AUGUST 2005
LESSON EVALUATION
Please indicate the date you completed this exam
_____________________________
How much time did it take you to complete the lesson?
______ hours ______minutes
How well did this lesson achieve its educational objectives?
_______Very well _________Well
________Somewhat __________Not at all
What overall grade would you assign this lesson?
A B C D
Degree____________________________
Additional comments and suggestions for future exams:
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
EXAM #6/05Use of Mini-External Fixation
in Forefoot Surgery(Zelen, Weinraub, Wu)
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
Circle:
E N R O L L M E N T F O R M & A N S W E R S H E E T (cont’d)Con
tinuin
g
Medica
l Edu
catio
n





























