Embed Size (px)
Citation preview
EEC was first described by Eckholdtand Martins in 1804. The clinicalmanifestations of ectodermal dyspla-sia include cutaneous alterations (dry,thin, hyperkeratotic skin), trichodys-plasia (thin, sparse hair with little pig-mentation), onychodysplasia (brittleand dysplastic nails), dental anomalies(small or absent teeth with excessivecaries), and dyshidrosis (sweating dys-function). The cleft lip may or maynot be accompanied by a cleft palate.
Defects in other locations may alsobe associated with the classical EECtriad, such as the eyes, including defectsin the nasolacrimal duct, entropion,telecanthus, trichiasis, absent lashes,andmeibomian gland disfunction,manifest-
Continued on page 166
Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Contin-uing Medical Education by the Council on Podiatric Medical Education.
You may enroll: 1) on a per issue basis (at $20.00 per topic) or 2) per year, for the special introductory rate of $139 (yousave $61). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the nearfuture, you may be able to submit via the Internet.
If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned cred-its. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test atno additional cost. A list of states currently honoring CPME approved credits is listed on pg. 170. Other than those entitiescurrently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be accept-able by any state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best effortsto ensure the widest acceptance of this program possible.
This instructional CME program is designed to supplement, NOT replace, existing CME seminars.The goal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high qualitymanuscripts by noted authors and researchers. If you have any questions or comments about this program, you can write orcall us at: Podiatry Management, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us [email protected].
Following this article, an answer sheet and full set of instructions are provided (p. 170).—Editor
JANUARY 2009 • PODIATRY MANAGEMENTwww.podiatrym.com 165
claw deformity in 1829, and Cruveil-hier first used the term “lobster-claw”in 1842. Pedal ectrodactyly may existas a unilateral or bilateral deformityin many combinations with other de-formities (Figure 2). It may be presentas an isolated deformity or simulta-neously with similar defects in thehand. It most frequently presents aspart of a defect syndrome, includingdefects of the eye, palate, audition,and abnormalities of the kidneys.
Associated SyndromesSeveral syndromes have been asso-
ciated with ectrodactyly. One of themost common is the EEC syndromeconsisting of ectodermal dysplasia, ec-trodactyly, and cleft lip and palate.
By Mark A Caselli, DPM
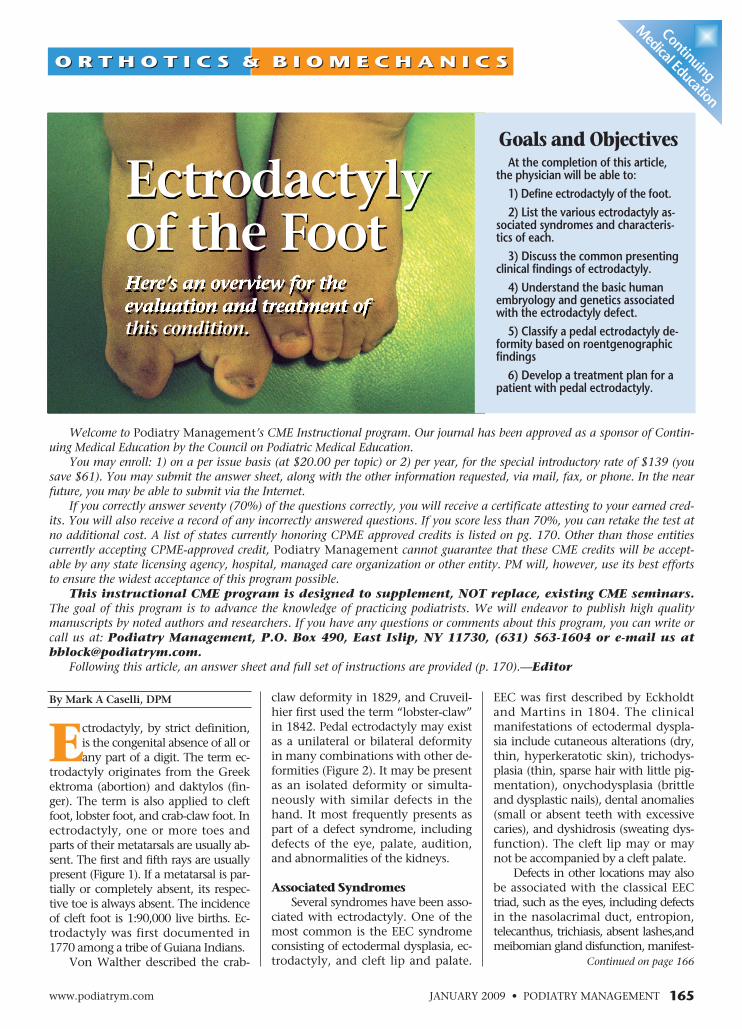
Ectrodactyly, by strict definition,is the congenital absence of all orany part of a digit. The term ec-
trodactyly originates from the Greekektroma (abortion) and daktylos (fin-ger). The term is also applied to cleftfoot, lobster foot, and crab-claw foot. Inectrodactyly, one or more toes andparts of their metatarsals are usually ab-sent. The first and fifth rays are usuallypresent (Figure 1). If a metatarsal is par-tially or completely absent, its respec-tive toe is always absent. The incidenceof cleft foot is 1:90,000 live births. Ec-trodactyly was first documented in1770 among a tribe of Guiana Indians.
Von Walther described the crab-
Here’s an overview for theevaluation and treatment ofthis condition.
Ectrodactylyof the Foot
Goals and ObjectivesAt the completion of this article,
the physician will be able to:1) Define ectrodactyly of the foot.2) List the various ectrodactyly as-
sociated syndromes and characteris-tics of each.3) Discuss the common presenting
clinical findings of ectrodactyly.4) Understand the basic human
embryology and genetics associatedwith the ectrodactyly defect.5) Classify a pedal ectrodactyly de-
formity based on roentgenographicfindings6) Develop a treatment plan for a
patient with pedal ectrodactyly.
Continuing
Medical Education
O R T H O T I C S & B I O M E C H A N I C SO R T H O T I C S & B I O M E C H A N I C S
lidimide syndrome and Nager acrofa-cial dysostosis; the fourth digit in con-genital hypothalamic hamartoblas-toma polydactyly syndrome. Tripha-langeal thumbs have been associatedwith ectrodactyly in a rare autosomaldominant syndrome. The combina-tion of polydactyly and oligodactylyhas been observed with both geneticand teratogen induced malformationsin experimental animals.
In Thalidomide embryopathy, thepolydactyly always occurs on thehands with a reductional abnormalityinvolving the feet. Autosomal reces-sive syndromes involving ectrodacty-ly have been described in a closed is-land population in Japan and in Mid-dle Eastern cultures where marriagebetween first cousins is encouraged.
Embryology and Genetics
Ectrodactyly in AfricaIn 1770, Jan Jacob Hartnick, a direc-
tor of the Dutch East India Company,made a reference to a touvinga or two-fingered tribe from Dutch Guyana inSouth America. They were slaves whoexhibited ectrodactyly, brought overfromCentral Africa. In the 1960’s, news-papers published interviews with unim-peachable witnesses who saw the phe-nomenon in Africa. Gelfland, et al., in1974 investigated a Wadoma tribesmanfrom the Zambezi valley of Zimbabwe.He was diagnosed as having “lobster
claw” defor-mity of bothfeet. Two ofhis cousinswere affect-ed and theconditionwas thoughtto be auto-somal domi-nant.
The anomaly was also seen in theTalaunda tribe from eastern Zimbabweand Botswana. The Talaunda migratedfrom eastern Zimbabwe and may havebeen of the same origins as the Wado-ma. In 1979, a magazine reported agroup of at least 100 “ostrich footed”men. Recent studies have found threefamilies of affected individuals amongthese tribes and concluded that the pre-vious tales of hundreds of ostrich-footedpersons belong in the realmof fantasy.
EmbryologyHuman limbs develop from interac-
tions between limb ectoderm andmesoderm. An important embryonicsomite-somatopleural relationship pre-cedes the emergence of the limb budduring the fourth week of gestation.The lower limb buds develop as lateralthickenings of the somatopleure. At thefifthweek, vertebrate limb buds developa thickened epithelium at their distaltips. This apical ectodermal ridge (AER)functions as a principle inducer of axiallimb elongation. The AER is required forprogressive specification of mesodermallimb parts and promotion of axialgrowth through influencing cell divi-sion. The ridge also protects subridgemesodermal cells from necrosis duringthe active period of limb development.
The deep midline cleft, character-Continued on page 167
166 www.podiatrym.comPODIATRY MANAGEMENT • JANUARY 2009
Ectrodactyly...
ing as blephoritis, corneal scar-ring, recurrent erosions, ble-
pharospasm, dry eye, and photophobia.Genitourinary system defects includehypospadias, hydronephrosis, renal age-nesis, and renal duplicity. Both deafnessandmental retardation are also associat-ed with EEC syndrome. The clinical ex-pression of the defects associated withEEC is very diverse, ectodermal dysplasiaoccurring 100%, lachrymal duct alter-ations 70-96.5%, ectrodactyly 78-88%,cleft lip/palate 58-88%, urinary alter-ations 15-55%, deafness 8-28%, andmental retardation 1-16%. The inci-dence of EEC is 1:190,000 live births.
Other SyndromesOther syndromes associatedwith ec-
trodactyly include Carpenter’s syn-drome (acrocephalopolysyndactyly typeII), DeLange syndrome (multiple con-genital anomaly/mental retardation(MCA/MR) disorder), Goltz syndrome(focal dermal hypoplasia (FDH) disor-der), Jarcho Levine syndrome (spondy-lothoracic dysplasia (STD) and spondy-locostal dysostosis (SCD) disorder), andMiller syndrome (post-axial acrofacialdysostosis). Raas-Rothschild, et al. de-scribed a syndrome of ectrodactyly,short stature, mental retardation, sen-sorineural deafness and abnormal faces.
Limb-reducing defects that can beassociated with ectrodactyly includeaplasia and hypoplasia of the tibia orfibula (i.e., Volkmann syndrome). Thisdistal extremity reduction may occurconcurrently with normal formation ofthe proximal limb segment. Ectrodacty-ly has also been found in patients withaplasia cutis congenital and epidermol-ysis bullosa. Pedal ectrodactyly, withoutsimilar upper extremity deficits, occursin 10% to 50%of cases of trisomy.(18)
Syndromes involving both poly-dactyly and ectrodactyly have beendescribed with the same digit usuallyinvolved (absence or duplication); thethumb in Fanconi anemia, Tha-
Continuing
MedicalEducation
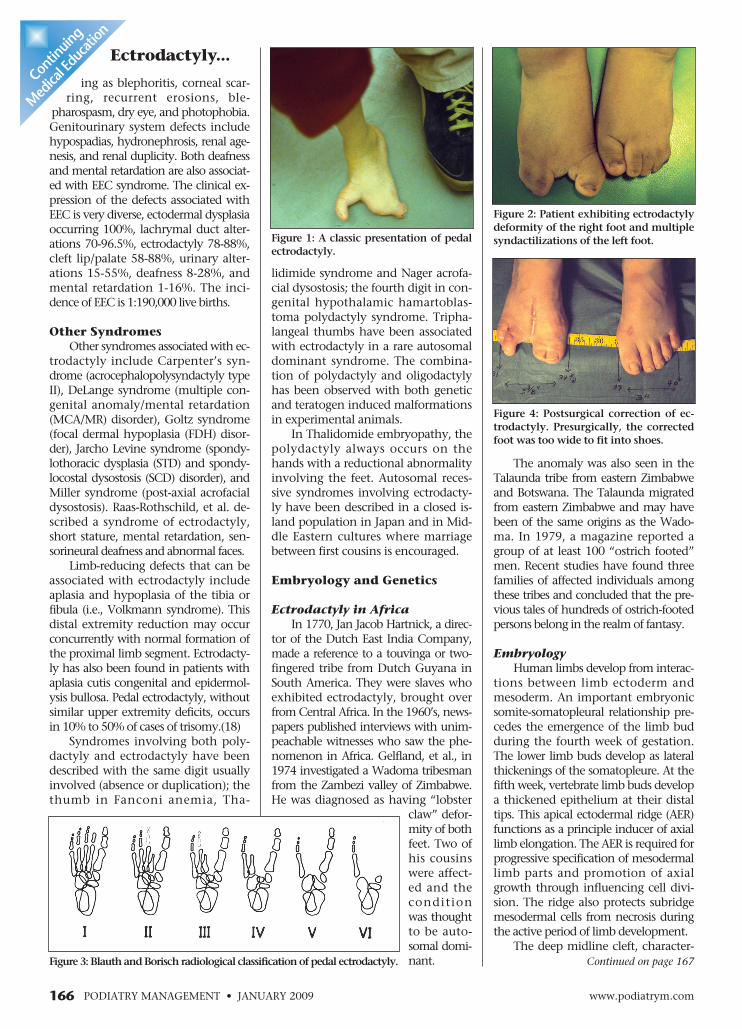
Figure 4: Postsurgical correction of ec-trodactyly. Presurgically, the correctedfoot was too wide to fit into shoes.
Figure 2: Patient exhibiting ectrodactylydeformity of the right foot and multiplesyndactilizations of the left foot.
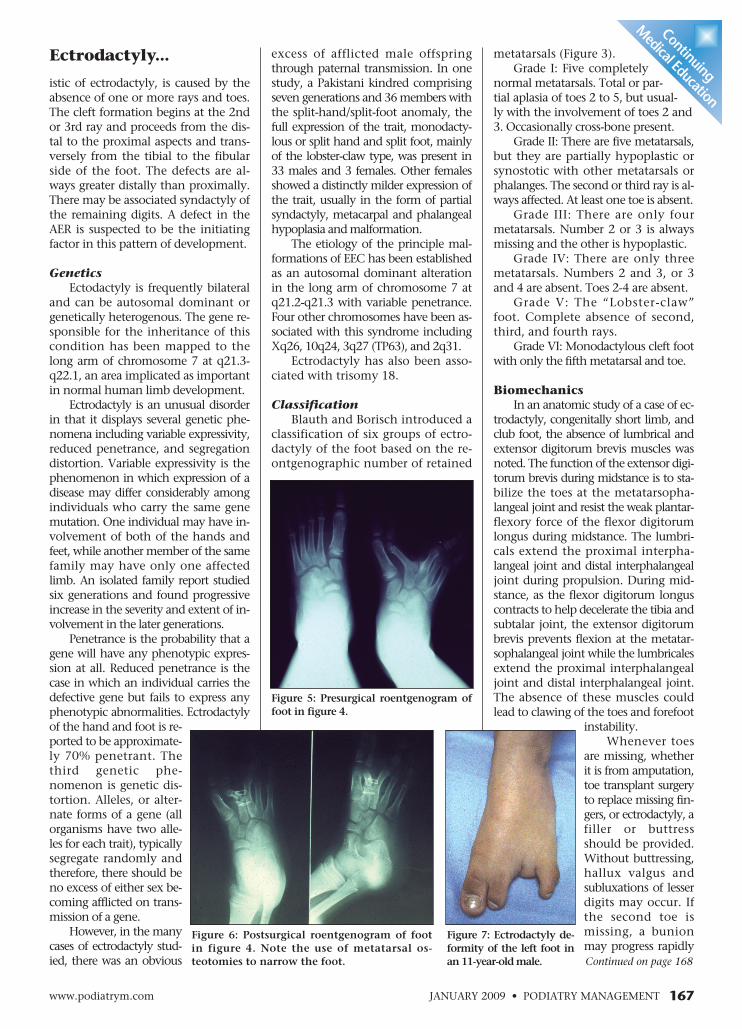
Figure3: BlauthandBorisch radiological classificationofpedal ectrodactyly.
Figure 1: A classic presentation of pedalectrodactyly.
JANUARY 2009 • PODIATRY MANAGEMENTwww.podiatrym.com 167
excess of afflicted male offspringthrough paternal transmission. In onestudy, a Pakistani kindred comprisingseven generations and 36members withthe split-hand/split-foot anomaly, thefull expression of the trait, monodacty-lous or split hand and split foot, mainlyof the lobster-claw type, was present in33 males and 3 females. Other femalesshowed a distinctly milder expression ofthe trait, usually in the form of partialsyndactyly, metacarpal and phalangealhypoplasia andmalformation.
The etiology of the principle mal-formations of EEC has been establishedas an autosomal dominant alterationin the long arm of chromosome 7 atq21.2-q21.3 with variable penetrance.Four other chromosomes have been as-sociated with this syndrome includingXq26, 10q24, 3q27 (TP63), and 2q31.
Ectrodactyly has also been asso-ciated with trisomy 18.
ClassificationBlauth and Borisch introduced a
classification of six groups of ectro-dactyly of the foot based on the re-ontgenographic number of retained
istic of ectrodactyly, is caused by theabsence of one or more rays and toes.The cleft formation begins at the 2ndor 3rd ray and proceeds from the dis-tal to the proximal aspects and trans-versely from the tibial to the fibularside of the foot. The defects are al-ways greater distally than proximally.There may be associated syndactyly ofthe remaining digits. A defect in theAER is suspected to be the initiatingfactor in this pattern of development.
GeneticsEctodactyly is frequently bilateral
and can be autosomal dominant orgenetically heterogenous. The gene re-sponsible for the inheritance of thiscondition has been mapped to thelong arm of chromosome 7 at q21.3-q22.1, an area implicated as importantin normal human limb development.
Ectrodactyly is an unusual disorderin that it displays several genetic phe-nomena including variable expressivity,reduced penetrance, and segregationdistortion. Variable expressivity is thephenomenon in which expression of adisease may differ considerably amongindividuals who carry the same genemutation. One individual may have in-volvement of both of the hands andfeet, while anothermember of the samefamily may have only one affectedlimb. An isolated family report studiedsix generations and found progressiveincrease in the severity and extent of in-volvement in the later generations.
Penetrance is the probability that agene will have any phenotypic expres-sion at all. Reduced penetrance is thecase in which an individual carries thedefective gene but fails to express anyphenotypic abnormalities. Ectrodactylyof the hand and foot is re-ported to be approximate-ly 70% penetrant. Thethird genetic phe-nomenon is genetic dis-tortion. Alleles, or alter-nate forms of a gene (allorganisms have two alle-les for each trait), typicallysegregate randomly andtherefore, there should beno excess of either sex be-coming afflicted on trans-mission of a gene.
However, in themanycases of ectrodactyly stud-ied, there was an obvious
Ectrodactyly... metatarsals (Figure 3).Grade I: Five completely
normal metatarsals. Total or par-tial aplasia of toes 2 to 5, but usual-ly with the involvement of toes 2 and3. Occasionally cross-bone present.
Grade II: There are five metatarsals,but they are partially hypoplastic orsynostotic with other metatarsals orphalanges. The second or third ray is al-ways affected. At least one toe is absent.
Grade III: There are only fourmetatarsals. Number 2 or 3 is alwaysmissing and the other is hypoplastic.
Grade IV: There are only threemetatarsals. Numbers 2 and 3, or 3and 4 are absent. Toes 2-4 are absent.
Grade V: The “Lobster-claw”foot. Complete absence of second,third, and fourth rays.
Grade VI: Monodactylous cleft footwith only the fifthmetatarsal and toe.
BiomechanicsIn an anatomic study of a case of ec-
trodactyly, congenitally short limb, andclub foot, the absence of lumbrical andextensor digitorum brevis muscles wasnoted. The function of the extensor digi-torum brevis during midstance is to sta-bilize the toes at the metatarsopha-langeal joint and resist the weak plantar-flexory force of the flexor digitorumlongus during midstance. The lumbri-cals extend the proximal interpha-langeal joint and distal interphalangealjoint during propulsion. During mid-stance, as the flexor digitorum longuscontracts to help decelerate the tibia andsubtalar joint, the extensor digitorumbrevis prevents flexion at the metatar-sophalangeal joint while the lumbricalesextend the proximal interphalangealjoint and distal interphalangeal joint.The absence of these muscles couldlead to clawing of the toes and forefoot
instability.Whenever toes
are missing, whetherit is from amputation,toe transplant surgeryto replace missing fin-gers, or ectrodactyly, afiller or buttressshould be provided.Without buttressing,hallux valgus andsubluxations of lesserdigits may occur. Ifthe second toe ismissing, a bunionmay progress rapidlyContinued on page 168
Continuing
Medical Education
Figure 7: Ectrodactyly de-formity of the left foot inan11-year-oldmale.
Figure 5: Presurgical roentgenogram offoot in figure 4.
Figure 6: Postsurgical roentgenogram of footin figure 4. Note the use of metatarsal os-teotomies to narrow the foot.

ther forefoot structural de-formation must also be in-cluded. A toe buttress man-ufactured in the office froma silicone putty compoundmay be used as a temporaryspacer, or if deemed appro-priate, as sole managementfor the least severe cases. Itshould be anchored on aflanged toe buttress runningunder the existing toes.Latex prostheses may beconstructed to plaster casts.Other alternatives includethe use of a shoe insert con-structed of Plastizote or lam-b’s wool, or a custom-mold-ed shoewith a spacer.
Case PresentationAn 11-year-old white male present-
ed with a chief complaint of absentthird and fourth toes, and a wide fifthtoe of his left foot (Figure 7). His rightfoot was normal. The patient was cur-rently having no problem fitting intoconventional shoe gear and was in nodiscomfort. His mother was concernedabout the curling of his most lateraltoe, which she claimed had been get-ting worse over the past year. She wasalso concerned about possible futureproblems with the deformity.
The patient’s past medical historywas unremarkable with no known al-lergies and no medications. There wasno family history of a similar prob-lem. The birth history was unevent-ful. Vascular and neurological find-ings were within normal limits.
Roentgenograms revealed the ab-sence of the distal, middle, and most ofthe proximal phalanx of the third toe,with syndactylization of the fourth andfifth toes of his left foot (Figure 8). Thetreatment plan was to fabricate a pair ofleather laminate orthoses from aneutralimpression cast of his feet. An accom-modative spacer was fitted on the leftorthosis to accommodate for the spacecreated by the deformity, and to act as abuttress for the lateral digit, reducing itstendency for adductovarus curling (Fig-ure 9). The patient was fitted with theorthoses and tolerated themwell.�
References1. AhmadM, Abbas H, Haque S, Flatz G.
X-Chromosomally inherited split-hand/splitfoot anomaly in a Pakistani kindred. HumGenet (1987) 75:169-173.
2. Blauth W, Borisch NC. Cleft feet: pro-
168 www.podiatrym.comPODIATRY MANAGEMENT • JANUARY 2009
Ectrodactyly...
because stage 2 in the develop-ment of a bunion is bypassed, lead-
ing to a stage 3 or 4 buniondeformity.
Approach to ManagementThe feet of patients with ectrodact-
lyly are usually functional, and ambu-lation is not a problem. The inabilityto fit into normal footwear is the mostcommon problem. Bursitis and painfulcallosities may develop as a result ofthe bony deformities and associatedabnormal distribution of weight. Themore severe forms of ectrodactyly cancause gait problems such as instabilityduring the propulsive phase. Idealtreatment would bring the size of thefoot into the normal range, fill thecleft, correct the secondary deformi-ties, andmaintain good function.
Surgical criteria for ectrodactyly caninclude the inability to fit into shoes andthe elimination of discomfort. Surgicalintervention, if deemed necessary,should be offered to the patient at a veryearly age to avoid further pathologicalchanges that can occur over time. Thereis no clearly defined surgical technique,though the surgical options that are de-scribed generally agree on resection ofthe rudimentary elements, osteotomiesat different levels, syndactylization,desyndactylization, hammertoe, andhallux valgus surgery (Figures 4, 5, 6).
Biomechanical management, ide-ally, should consist of a foot orthosis,the elements of which should in-clude: a posterior and central stabiliz-ing component to control the move-ments of the subtalar joint; an anteri-or component with a balancing effectto facilitate propulsion, stabilize thefront of the foot, and cushion thefirst and fifth metatarsal heads.
A filler for the cleft to impede fur-
Continuing
MedicalEducation
Dr. Caselli is StaffPodiatrist at theVA Hudson Val-ley Health CareSystem in Mon-trose, NY. and isan Adjunct Pro-fessor at the NewYork College ofP o d i a t r i cMedicine and anAdjunct Professor at Ramapo College ofNew Jersey. He is Former Chairman, Divi-sion of Orthopedic Sciences and Director,Department of Pediatrics atNYCPM
posals for a new classificationbased on roentgenographicmorphology. Clin Ortho (1990)258: 41-48.
3. Caldwell BD. Genetics ofsplit hand and split foot. J AmPodiatr Med Assoc (1996) 86(6):244-248.
4. Caselli MA, RubensteinD. Pedal ectrodactyly: abiomechnical approach tomanagement. J Foot Ankle Surg(1995) 34 (2): 215-219.
5. Cruveilhier J. AnatomicPathologique du Corps Hu-main, vol. 2. Paris: Balliere;1842. p. 38.
6. Drennan JC. Congenitaldeformities of the foot andankle. In Myerson MS (ed.).Foot and Ankle Disorders.Philadelphia, W.B. SaundersCompany, 2000. pp 645-657
7. Farrell HB McD. The two-toed Wado-ma-familial ectrodactyly in Zimbabwe. SAMed J (1984) 65:531
8. Giorgini RJ, Capa CJ, Potter GK. Twostage surgical correction of cleft foot. A seven-year follow-up of one case. J Am PodiatrAssoc (1985) 75:481
9. Helal A, Perry T, Ogden JA, Greene TL.Six generations of a family withmultiple limbdeficiencies. J PediatrOrthop (1993) 13:210.
10. Kelman GJ, Aronoff RC. Ectrodacty-ly-ectodermal dysplasia-clefting syndrome. JAmPodiatrMedAssoc (2000) 90(9): 460-464.
11. Libbie JC, Derk FF, Nardozza AJ. Ec-trodactyly: a unique case presentation. J AmPodiatrMedAssoc (1996) 86(8): 398-400.
12. Pena DA, Nova AM, Pena JA, RuizSH. Cleft foot and ectrodactyly-ectodermaldysplasia-cleft lip/palate syndrome. Review ofthe literature and report of two new cases.The Foot (2004) 14: 221-226.
13. Raas-Rothschild A, Aviram A, BenAmi T, Berger I, Bat-Miriam Katznelson M,Goodman RM. Newly recognized ectrodacty-ly/deafness syndrome. J Craniofac Genet DevBiol (1989) 9:121.
14. Von Walter P. Ueber die exarticula-tion der finder mit ihren mittelhandbein ausden handwurzelgelenken. J Chin U Augen-Heilkunde. (1829) 43: 1202.
Figure 8: Roengtgeno-gram of patient’s leftfoot with absent thirdtoe and syndactyly ofthe fourth and fifth toes.
Figure 9: Custom orthoses fabricated forpatient with filler to accommodate forectrodactyly deformity.
JANUARY 2009 • PODIATRY MANAGEMENTwww.podiatrym.com 169
7) A defect in the AER canresult in:A) Kidney abnormalitiesB) Cleft footC) DeafnessD) None of the above
8) The gene that is responsiblefor the inheritance of ectro-dactyly has been mapped tochromosome _______.A) 5B) 7C) 12D) 18
9) Genetically, variable expres-sivity is a phenomenon inwhich the expression of adisease:A) Appears the same in allwho have the same genemutation.B) May be radically differentin all who have the samegene mutation.C) Only occurs in femalefamily members.D) Only occurs in male fami-ly members.
10) Which one of the followingis most correct concerning theinheritance of ectrodactyly?A) It tends to skipgenerations.B) There is an excess ofafflicted males.C) There is an excess ofafflicted females.D) It becomes less severe inlater generations.
11) Which one of the followingis the key characteristic of
1) Which one of the followingterms is not a synonym for pedalectrodactyly?A) Cleft footB) Skew footC) Lobster footD) Crab-claw foot
2) What is the incidence of cleftfoot?A) 1:500 live birthsB) 1:10,000 live birthsC) 1:90,000 live birthsD) 1:190,000 live births
3) Which one of the following isnot part of the EEC syndrome?A) Ectodermal dysplasiaB) ChondromalasiaC) EctrodactylyD) Cleft lip
4) The clinical expression ofectrodactyly in EEC syndromepresents in _____% of cases.A) 8-28B) 15-55C) 78-88D) 100
5) Ectrodactyly is an associatedfinding in which one of thefollowing trisomy defects?A) Trisomy 8B) Trisomy 13C) Trisomy 18D) Trisomy 21
6) Embryologically, what is thefunction of the apical ectodermalridge (AER)?A) Induce axial limb elongation.B) Retard digital differentiation.C) Responsible for nail growth.D) None of the above.
Blauth and Borisch Grade Iectrodactyly?A) Five completely normalmetatarsalsB) Partially hypoplasticmetatarsalsC) At least one absent toeD) Classic “lobster-claw”foot appearance
12) The main characteristic ofBlauth and Borisch Grade IIIectrodactyly is:A) At least one absent toe.B) Only four metatarsals.C) Monodactylous cleftfoot.D) Only three metatarsals.
13) What Blauth and Borischgroup represents the classic“lobster-claw” foot?A) Grade IB) Grade IIIC) Grade VD) Grade VI
14) A foot with an ectro-dactyly defect was found tohave absent extensor digito-rum brevis and lumbricalmuscles. Which one of thefollowing is most likely to re-sult from the absence ofthese muscles?A) Weak push-off phase ofgaitB) Hallux valgusC) Clawing of toesD) Equinus gait
15) Which one of thefollowing has been found tobe the main problem of pa-
Continuing
Medical Education
E X A M I N A T I O N
See answer sheet on page 171.
Continued on page 170
170 PODIATRY MANAGEMENT
tients with ectrodactyly?A) Plantar callositiesB) Inability to fit in shoesC) Foot painD) Inability to ambulate
16) Which one of the following is the most com-mon gait problem in severe forms of ectrodactyly?A) Instability during propulsionB) Inversion sprains at heel contactC) Midstance pronationD) Drop foot
17) Absence of the second toe promotes whichone of the following deformities?A) HammertoesB) Hallux valgusC) Metatarsus adductusD) None of the above
18) Which of the following represents idealtreatment for pedal ectrodactyly?A) Normalize size of footB) Fill the cleftC) Maintain good functionD) All of the above
19) Which of the following is a consideration forsurgical intervention in the treatment of pedalectrodactyly?A) Inability to fit into shoesB) Elimination of discomfortC) Age of patientD) All of the above
20) Which one of the following orthotic modifica-tions is needed to prevent forefoot structuraldeformities such as hallux valgus in Grade II orabove type ectrodactyly?A) Rearfoot varus postingB) Forefoot varus postingC) Heel liftD) Toe filler
E X A M I N A T I O N
(cont’d)
See answer sheet on page 171.
Continuing
MedicalEducation
PM’sCPME Program
Welcome to the innovative Continuing EducationProgram brought to you by Podiatry ManagementMagazine. Our journal has been approved as asponsor of Continuing Medical Education by theCouncil on Podiatric Medical Education.
Now it’s even easier and more convenientto enroll in PM’s CE program!
You can now enroll at any time during the yearand submit eligible exams at any time during yourenrollment period.
PM enrollees are entitled to submit ten examspublished during their consecutive, twelve–monthenrollment period. Your enrollment period beginswith the month payment is received. For example,if your payment is received on September 1, 2006,your enrollment is valid through August 31, 2007.
If you’re not enrolled, you may also submit anyexam(s) published in PM magazine within the pasttwelve months. CME articles and examinationquestions from past issues of Podiatry Man-agement can be found on the Internet athttp://www.podiatrym.com/cme. Each lessonis approved for 1.5 hours continuing education con-tact hours. Please read the testing, grading and pay-ment instructions to decide which method of partici-pation is best for you.
Please call (631) 563-1604 if you have any ques-tions. A personal operator will be happy to assist you.
Each of the 10 lessons will count as 1.5 credits;thus a maximum of 15 CME credits may beearned during any 12-month period. You may se-lect any 10 in a 24-month period.
The Podiatry Management Magazine CMEprogram is approved by the Council on PodiatricEducation in all states where credits in instruction-al media are accepted. This article is approved for1.5 Continuing Education Contact Hours (or 0.15CEU’s) for each examination successfully completed.
www.podiatrym.com
Home Study CME credits nowaccepted in Pennsylvania
Over, please
Please print clearly...Certificate will be issued from information below.
Name _______________________________________________________________________Soc. Sec. #______________________________Please Print: FIRST MI LAST
Address_____________________________________________________________________________________________________________
City__________________________________________________State_______________________Zip________________________________
Charge to: _____Visa _____ MasterCard _____ American Express
Card #________________________________________________Exp. Date____________________
Note: Credit card is the only method of payment. Checks are no longer accepted.
Signature__________________________________Soc. Sec.#______________________Daytime Phone_____________________________
State License(s)___________________________Is this a new address? Yes________ No________
Check one: ______ I am currently enrolled. (If faxing or phoning in your answer form please note that $2.50 will be chargedto your credit card.)
______ I am not enrolled. Enclosed is my credit card information. Please charge my credit card $20.00 for each examsubmitted. (plus $2.50 for each exam if submitting by fax or phone).
______ I am not enrolled and I wish to enroll for 10 courses at $139.00 (thus saving me $61 over the cost of 10 individualexam fees). I understand there will be an additional fee of $2.50 for any exam I wish to submit via fax or phone.
Note: If you are mailing your answer sheet, you must completeall info. on the front and back of this page and mail with yourcredit card information to: Podiatry Management, P.O. Box490, East Islip, NY 11730.
TESTING, GRADING AND PAYMENT INSTRUCTIONS(1) Each participant achieving a passing grade of 70% or
higher on any examination will receive an official computer formstating the number of CE credits earned. This form should be safe-guarded andmay be used as documentation of credits earned.
(2) Participants receiving a failing grade on any exam will benotified and permitted to take one re-examination at no extra cost.
(3) All answers should be recorded on the answer formbelow. For each question, decide which choice is the best an-swer, and circle the letter representing your choice.
(4) Complete all other information on the front and back ofthis page.
(5) Choose one out of the 3 options for testgrading: mail-in,fax, or phone. To select the type of service that best suits yourneeds, please read the following section, “Test Grading Options”.
TEST GRADING OPTIONSMail-In GradingTo receive your CME certificate, complete all information
and mail with your credit card information to:Podiatry Management
P.O. Box 490, East Islip, NY 11730There is no charge for the mail-in service if you have already
enrolled in the annual exam CPME program, and we receive this
ENROL LMENT FORM & ANSWER SH E E T
�
171
Continuing
Medical Education
exam during your current enrollment period. If you are not en-rolled, please send $20.00 per exam, or $139 to cover all 10 exams(thus saving $61* over the cost of 10 individual exam fees).
Facsimile GradingTo receive your CPME certificate, complete all information and
fax 24 hours a day to 1-631-563-1907. Your CPME certificate willbe dated and mailed within 48 hours. This service is available for$2.50 per exam if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment period),and can be charged to your Visa, MasterCard, or American Express.
If you are not enrolled in the annual 10-exam CPME pro-gram, the fee is $20 per exam.
Phone-In GradingYou may also complete your exam by using the toll-free ser-
vice. Call 1-800-232-4422 from 10 a.m. to 5 p.m. EST, Mondaythrough Friday. Your CPME certificate will be dated the same dayyou call and mailed within 48 hours. There is a $2.50 charge forthis service if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment peri-od), and this fee can be charged to your Visa, Mastercard, Ameri-can Express, or Discover. If you are not currently enrolled, the feeis $20 per exam. When you call, please have ready:
1. Program number (Month and Year)2. The answers to the test3. Your social security number4. Credit card information
In the event you require additional CPME information,please contact PMS, Inc., at 1-631-563-1604.
Enrollment/Testing Informationand Answer Sheet
�
172 www.podiatrym.comPODIATRY MANAGEMENT • JANUARY 2009
ENROL LMENT FORM & ANSWER SH E E T (cont’d)Continuing
MedicalEducation
LESSON EVALUATION
Please indicate the date you completed this exam
_____________________________
How much time did it take you to complete the lesson?
______ hours ______minutes
How well did this lesson achieve its educationalobjectives?
_______Very well _________Well
________Somewhat __________Not at all
What overall grade would you assign this lesson?
A B C D
Degree____________________________
Additional comments and suggestions for future exams:
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
Circle:
EXAM #1/09Ectrodactyly of the Foot
(Caselli)
















