Embed Size (px)
Citation preview
[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES AND HANDOUTS]
3/8/181
Key Publications in Occupational & Environmental Health: the Year in ReviewEmerging and Re-Emerging Occupational Disease 2018
Samuel M. Goldman, MD, MPHAssociate Clinical ProfessorUCSF Division of Occupational & Environmental Medicine
Disclosures: None
2
3
Clinical Infectious Diseases
• CID 2017:XX (XX XXXX) • 1Histoplasmosis in the Dominican Republic
Outbreak of Severe Histoplasmosis Among Tunnel Workers—Dominican Republic, 2015Paige A. Armstrong,1 John D. Beard,2,a Luis Bonilla,3 Nelson Arboleda,3 Mark D. Lindsley,4 Sae-Rom Chae,5 Delia Castillo,6 Ramona Nuñez,6 Tom Chiller,4 Marie A. de Perio,7 Raquel Pimentel,6 and Snigdha Vallabhaneni4
1Epidemic Intelligence Service, Mycotic Diseases Branch, Division of Foodborne, Waterborne, and Environmental Diseases (DFWED), National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Centers for Disease Control and Prevention (CDC), Atlanta, Georgia; 2Epidemic Intelligence Service, Industrywide Studies Branch, Division of Surveillance, Hazard Evaluations and Field Studies, National Institute for Occupational Safety and Health (NIOSH), Cincinnati, Ohio; 3Centers for Disease Control and Prevention, Santo Domingo, Dominican Republic; 4Mycotic Diseases Branch and 5Epidemic Intelligence Service, Global Water, DFWED, NCEZID, CDC, Atlanta, Georgia; 6Dirección General de Epidemiología, Santo Domingo, Dominican Republic; and 7Hazard Evaluations and Technical Assistance Branch, Division of Surveillance, Hazard Evaluations and Field Studies, NIOSH, Cincinnati, Ohio
Background. Histoplasmosis is a fungal infection associated with exposure to bat guano. An outbreak of an unknown severe febrile illness occurred among tunnel workers in the Dominican Republic, and resulted in several deaths. We conducted an investi-gation to confirm etiology and recommend control measures.
Methods. A case was defined as fever and ≥2 symptoms consistent with histoplasmosis in a tunnel worker, July–September 2015. We interviewed workers and family members, reviewed medical records, tested serum and urine for Histoplasma antigen/antibody, and conducted a cohort study to identify risk factors for histoplasmosis and severe infection (intensive care).
Results. A crew of 36 male workers removed large amounts of bat guano from tunnels without respiratory protection for a median of 24 days per worker (range, 1–25 days). Median age was 32 years (range, 18–62 years); none were immunocompromised. Thirty (83%) workers had illness that met the case definition, of whom 28 (93%) were hospitalized, 9 (30%) required intensive care, 6 (20%) required intubation, and 3 (10%) died. The median time from symptom onset to antifungal treatment was 6 days (range, 1–11 days). Twenty-two of 34 (65%) workers had laboratory evidence of infection.
Conclusions. Severe illnesses and death likely resulted from exposure to large inocula of Histoplasma capsulatum spores in an enclosed space, lack of respiratory protection, and delay in recognition and treatment. Clinician education about histoplasmosis, improved laboratory capacity to diagnose fungal infections, and occupational health guidance to protect workers against endemic fungi are recommended in the Dominican Republic.
Keywords. fungi; histoplasmosis; outbreak; Dominican Republic; occupational.
Histoplasma capsulatum, the causative agent in histoplasmo-sis, is often found in association with bird or bat droppings [1]. Histoplasma capsulatum is present throughout the Americas and the Caribbean. Exposure to H. capsulatum typically occurs by inhalation of fungal spores, specifically the microconidia, following disruption of soil or other contaminated material. Once at body temperature (37°C), it transforms into the yeast phase. The average incubation period is 1–3 weeks, and clin-ical manifestations can range from asymptomatic infection to severe, disseminated disease [1]. Acute pulmonary histoplas-mosis is the most common symptomatic manifestation and is often self-limited, especially among healthy persons.
On 16 September 2015, the Dominican Republic Ministry of Health (DR MoH) requested assistance from the US Centers for
Disease Control and Prevention (CDC) with the investigation of an unknown severe febrile illness among several male tunnel work-ers. All men were members of a work crew tasked with removing bat guano from access tunnels to a hydroelectric dam. Workers were initially treated for leptospirosis, which is endemic to the area. Histoplasmosis was later considered when examination of one patient’s bronchoalveolar lavage (BAL) specimen demonstrated yeast cells, consistent with histoplasmosis; however, there was no local laboratory capacity to confirm the diagnosis. Three men had died and 25 others were hospitalized. Although histoplasmosis is endemic to the Americas, including other Caribbean islands such as Puerto Rico and Jamaica, cases had never been diagnosed in the DR [2]. Local physicians were unfamiliar with diagnosis and man-agement of histoplasmosis. CDC and the DR MoH investigated to confirm the etiology of the outbreak, elucidate clinical and occu-pational risk factors for histoplasmosis and severe disease, assess treatment outcomes, and identify control measures.
METHODS
Descriptive Epidemiology and Cohort Study
We defined a case of histoplasmosis as fever and ≥2 symptoms (chills, night sweats, weakness, joint pain, cough, headache,
M A J O R A R T I C L E
Published by Oxford University Press for the Infectious Diseases Society of America 2017. This work is written by (a) US Government employee(s) and is in the public domain in the US.DOI: 10.1093/cid/cix1067
Received 21 July 2017; editorial decision 22 November 2017; accepted 29 November 2017.aPresent affiliation: Department of Health Science, College of Life Sciences, Brigham Young
University, Provo, Utah.Correspondence: P. A. Armstrong, Centers for Disease Control and Prevention, 1600 Clifton
Rd NE, MS C-09, Atlanta, GA 30329 ([email protected]).
Clinical Infectious Diseases® 2017;XX(00):1–8
GOVERNMENT
XX
XXXX
Downloaded from https://academic.oup.com/cid/advance-article-abstract/doi/10.1093/cid/cix1067/4683412by University of California, San Fransisco useron 14 February 2018
§On September 16, 2015, Dominican Republic Ministry of Health requested CDC investigation of an unknown severe febrile illness in tunnel workers
Background
4
• Case definition: ‒ worked in tunnels to hydroelectric dam during July 30-Sept 2, 2015‒ fever and > 2 of: chills, night sweats, weakness, joint pain, cough,
headache, malaise, dyspnea, myalgias, diarrhea, vomiting• Case finding:
‒ Manual review of company payroll records‒ Interviews with workers to identify any other workers
• Questionnaire:‒ Interviews in Spanish‒ Demographics, medical conditions‒ Work history: days in tunnels, tasks, PPE
• Medical record review• Cohort study to identify risk factors for severe disease (ICU admission)
[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES AND HANDOUTS]
3/8/182
5
2 • CID 2017:XX (XX XXXX) • Armstrong et al
generalized malaise, dyspnea, myalgias, difficulty breathing, diarrhea, and vomiting) in a person who worked in the tunnels during 30 July–2 September 2015; this time period included all work performed on the tunnels. We reviewed company payroll records to identify all persons who had worked in the tunnels during that time period and interviewed workers to identify any additional persons exposed to the tunnels who may not have been on the official company records (eg, temporary substitutes for regular workers).
We interviewed tunnel workers in person in Spanish using a standardized questionnaire. For the 3 workers already deceased at the time of the interview, we spoke with an immediate family member. Worker interviews addressed demographic charac-teristics, underlying medical conditions, general information about the tunnels, number of days spent in the tunnels, tasks performed, and use of personal protective equipment.
We reviewed medical records from the local hospital where workers were initially hospitalized, and regional hospitals, where they were later transferred for care, using a standardized case report form that included clinical information, details of the hospital stay, treatment, and outcome.
We conducted a cohort study to identify risk factors for devel-oping histoplasmosis and severe disease (defined as admission to the intensive care unit [ICU]). The cohort included all workers exposed to the tunnels during 30 July–2 September 2015.
Laboratory Analysis
We collected serum and urine samples from tunnel workers and sent them to the CDC Mycotic Diseases Branch laboratory (Atlanta, Georgia) for analysis. Environmental sampling is not routinely performed and given the volume of guano involved in this outbreak, processing of environmental samples was not feasible. Histoplasma capsulatum antigen detection was per-formed on both urine and serum samples using an enzyme immunoassay (EIA) employing Histoplasma monoclonal ana-lyte-specific reagents (IMMY, Norman, Oklahoma), with a cut-off value of ≥0.5 ng/mL for a positive result. Before performing the assay, we treated serum with pronase at 56°C for 30 minutes followed by boiling for 5 minutes. We tested urine undiluted. Optical density EIA results were analyzed against a 7-point standard curve to provide a quantitative result [3]. EIA was cho-sen over other molecular methods as it can be performed on specimens that do not require invasive collection procedures, such as BAL or tissue biopsy. We performed qualitative H. cap-sulatum antibody detection using immunodiffusion on serum samples. In the outbreak setting, we considered an M band suf-ficient to conclude a positive result.
Statistical Analysis
We calculated medians and ranges for continuous variables, and frequencies and percentages for categorical variables. We evaluated unadjusted associations between demographic,
occupational, exposure, and clinical variables using the out-comes of histoplasmosis and severe disease. We used exact logistic regression models to estimate exact odds ratios and exact 95% confidence intervals (CIs). We assumed linear rela-tionships for continuous variables, but categorized them with category boundaries set either at the median or quartiles when the Akaike information criterion indicated that a linear term was not the best fit [4, 5]. We considered exact 2-sided P values of ≤.05 to be statistically significant. Due to the small size of our study, we also considered P values between .05 and .1 to be “bor-derline significant.” Statistical analyses were performed with SAS version 9.3 software (SAS Institute, Cary, North Carolina).
Ethics Approval
A local ethics committee in the DR and designated ethics officers at CDC determined that this was an emergency public health investigation and did not meet criteria for research.
RESULTS
Background on Tunnel Work
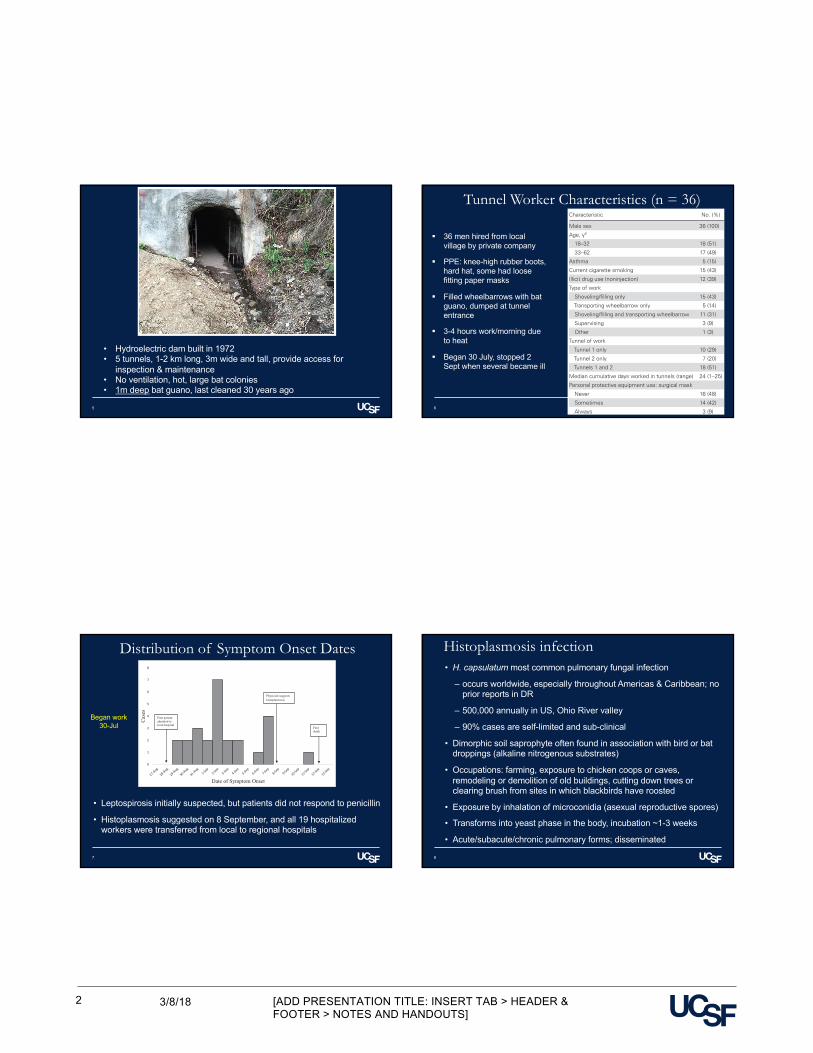
The dam was constructed in 1972 and provides hydroelectric energy to most of the surrounding communities. This embank-ment dam had 5 tunnels, each approximately 1–2 km long, which allow access to the dam for inspection and maintenance. Tunnel entrances were small (approximately 3 m wide and tall) (Figure 1). The tunnels lacked ventilation or illumination and were inhabited by large bat colonies. Bat guano up to 1 m deep had accumulated since the tunnels were last accessed approxi-mately 30 years ago.
A private company was contracted to clean the tunnels and recruited workers informally in a nearby town center. A total of 36 workers were exposed to the tunnels during July–September. Each worker was provided with a pair of knee-high rubber boots,
Figure 1. Entrance to a tunnel associated with severe histoplasmosis outbreak, Dominican Republic.
Downloaded from https://academic.oup.com/cid/advance-article-abstract/doi/10.1093/cid/cix1067/4683412by University of California, San Fransisco useron 14 February 2018
• Hydroelectric dam built in 1972• 5 tunnels, 1-2 km long, 3m wide and tall, provide access for
inspection & maintenance• No ventilation, hot, large bat colonies • 1m deep bat guano, last cleaned 30 years ago
Tunnel Worker Characteristics (n = 36)
6
• CID 2017:XX (XX XXXX) • 3Histoplasmosis in the Dominican Republic
a hard hat with an attached personal headlamp, and a shovel. Additionally, some workers received loose-fitting paper surgical masks. Workers were responsible for filling wheelbarrows with bat guano, transporting it outside, and depositing it immedi-ately near the tunnel entrance. They worked for 3–4 hours daily, 5 days per week, usually in the mornings. Work cleaning 2 of the tunnels began 30 July 30 and stopped 2 September, when a number of workers became ill.
Worker Interviews
All workers were male and the median age was 32 years (range, 18–62 years); 5 (15%) reported having asthma, 15 (43%) were current cigarette smokers, and 12 (39%) used illicit drugs (Table 1). Fifteen workers (43%) reported shoveling guano as their sole task, 5 (14%) reported only transporting the wheel-barrows containing guano, 11 (31%) engaged in both tasks, 3 (9%) supervised the work of others, and 1 (3%) performed other work (eg, holding a light). Ten (29%) workers worked in tunnel 1 only, 7 (20%) worked in tunnel 2 only, and 18 (51%) worked in both tunnels (4 workers worked 1–4 days in a third tunnel in addition to working in tunnels 1, 2, or both, but we did not consider the third tunnel in analyses because it could not have accounted for the large number of workers who be-came ill). The median number of days per worker spent in the tunnels was 24 (range, 1–25 days). Workers reported oppressive heat and difficulty breathing inside the tunnels while wearing the masks. Sixteen (48%) workers never used the masks, 14
(42%) used them sometimes, and 3 (9%) reported using them always (Table 1).
Clinical Presentation
The first ill worker presented to the local hospital on 28 August with an unknown febrile illness (Figure 2). By 4 September, 14 workers had been admitted to the local hospital. Leptospirosis was initially suspected as the cause of the outbreak because it is endemic to the region. However, the workers did not improve with penicillin, the treatment for leptospirosis. Physicians noted the common exposure to tunnel work among the admitted patients and reported the illnesses to the local health authori-ties. On 8 September, all 19 workers who had been admitted to the local hospital were transferred to regional hospitals, where a higher level of care was available to manage their unknown illness. Two of the 19 (11%) workers transferred from the local hospital to regional facilities required intubation within 1 day of arrival. At one regional facility, an astute physician, who had treated cases of histoplasmosis while training in Mexico, suggested the diagnosis of histoplasmosis given its association with exposure to bat guano. The same day, a pathologist noted yeast cells, suggestive of H. capsulatum by microscopy on a BAL specimen.
Thirty of the 36 (83%) exposed workers had illnesses that met the case definition. Symptom onset ranged between 21 August and 11 September 2015 (Figure 2). Twenty-eight (93%) work-ers were hospitalized, 9 (30%) required ICU admission, 6 (20%) were intubated, and 3 (10%) died (Table 2). The 3 workers who died were 21–36 years of age, had no known medical comor-bidities, and were nonsmokers. All 3 received voriconazole and intravenous steroids.
Nine of 30 (30%) case patients underwent bronchoscopy; 7 of these had BAL samples collected and 6 (86%) had BAL cul-tures positive for bacteria, consistent with ventilator-associated pneumonia. These samples were not available for further evalu-ation for H. capsulatum (Table 2).
Nineteen (68%) case patients had leukocytosis (white blood cell count >12 × 109/L) and 10 (36%) had aspartate aminotrans-ferase or alanine aminotransferase >120 U/L. Human immu-nodeficiency virus testing was performed for 15 (50%) case patients, and none were positive. Testing for leptospirosis, the original suspected pathogen, was performed for 23 (77%) case patients, and none were positive (Table 2).
Twenty-eight (93%) case patients received an antifungal, and the median time from symptom onset to first antifungal treatment was 6 days (range, 0–11 days). Voriconazole was the first antifungal administered to 16 (62% of those with data) case patients and 17 (61%) received >1 antifungal (not shown). Overall, 22 (79%) case patients received voriconazole, 14 (50%) received itraconazole, 9 (33%) received fluconazole, and 8 (29%) received amphotericin B during their treatment course. Twenty-six (87%) case patients received corticosteroids and 4
Table 1. Characteristics of Tunnel Workers (n = 36) and Tunnel Work in a Histoplasmosis Outbreak, Dominican Republic, 2015
Characteristic No. (%) Missing, No.
Male sex 36 (100)Age, ya 1 18–32 18 (51) 33–62 17 (49)Asthma 5 (15) 3Current cigarette smoking 15 (43) 1Illicit drug use (noninjection) 12 (39) 5Type of work 1 Shoveling/filling only 15 (43) Transporting wheelbarrow only 5 (14) Shoveling/filling and transporting wheelbarrow 11 (31) Supervising 3 (9) Other 1 (3)Tunnel of work 1 Tunnel 1 only 10 (29) Tunnel 2 only 7 (20) Tunnels 1 and 2 18 (51)Median cumulative days worked in tunnels (range) 24 (1–25) 1Personal protective equipment use: surgical mask 3 Never 16 (48) Sometimes 14 (42) Always 3 (9)
aCategory boundary set at the median among all workers.
Downloaded from https://academic.oup.com/cid/advance-article-abstract/doi/10.1093/cid/cix1067/4683412by University of California, San Fransisco useron 14 February 2018
§ 36 men hired from local village by private company
§ PPE: knee-high rubber boots, hard hat, some had loose fitting paper masks
§ Filled wheelbarrows with bat guano, dumped at tunnel entrance
§ 3-4 hours work/morning due to heat
§ Began 30 July, stopped 2 Sept when several became ill
Distribution of Symptom Onset Dates
7
4 • CID 2017:XX (XX XXXX) • Armstrong et al
(16%) received corticosteroids at least 1 day before treatment with antifungals (Table 2).
Laboratory Analysis
Thirty-four of the 36 exposed workers provided samples; we obtained 34 unique serum and 29 unique urine specimens. Urine and serum were available for 28 workers. Time from symptom onset to collection of specimen ranged from 5 to 33 days, with a median of 14 days. Eighteen (53%) serum and 13 (45%) urine samples were positive for H. capsulatum antigen. Additionally, immunodiffusion was performed on 31 serum samples, and 11 (35%) were positive. In total, 22 of the 34 (65%) workers tested had laboratory evidence of H. capsulatum infection.
Cohort Study
None of the variables examined in the cohort analysis—includ-ing age, presence of comorbidities, type of work, tunnel of work, days worked in tunnels, personal protective equipment use, days from symptom onset to antifungal treatment (ICU ad-mission only), symptoms (ICU admission only), and laboratory results (ICU admission only)—were significantly associated with histoplasmosis or severe disease (ICU admission) (Tables 3 and 4; and Supplementary Table 1). However, days worked in tunnels (P = .06) and difficulty breathing (P = .07) had border-line significant positive associations with severe disease.
DISCUSSION
This is the first report of an outbreak of histoplasmosis in the DR. Histoplasma capsulatum is endemic to the Caribbean re-gion, and outbreaks have been reported throughout Latin
America [2, 6–8]. Sporadic cases of histoplasmosis attributed to exposure in the DR have been diagnosed in travelers return-ing to their countries of origin [7]. Clinicians in the DR were largely unfamiliar with histoplasmosis and laboratories did not have the capacity to definitively diagnose the disease. It is possible that there have been previous cases and outbreaks of histoplasmosis in the DR that have gone unrecognized as the illness is often self-limited. The high mortality in a young healthy population likely brought more attention to this out-break, and the investigation led to the confirmation of histo-plasmosis in the DR.
Outbreaks of histoplasmosis tend to involve small numbers of people and fatalities are rare, even in resource-poor settings [6]. Several factors may have contributed to the high propor-tion of hospitalizations and deaths observed in this outbreak. Although local physicians and public health authorities quickly recognized that the ill workers had been exposed to tunnels, recognition of histoplasmosis and initiation of antifungal treat-ment were delayed. Furthermore, amphotericin B, the recom-mended treatment for severe pulmonary histoplasmosis, was not administered in the majority of cases despite decompensa-tion, and when administered, it was delayed [9]. The causes of this delay were likely multifactorial, and due to both unfamili-arity of physicians with guidelines and lack of access to the medication. Paucity of serologic or urine diagnostic capacity likely also contributed to the delay in definitive diagnosis and subsequent treatment. Aside from the delayed diagnosis and treatment, probable exposure to high H. capsulatum inocula in the tunnels, coupled with poor ventilation and inadequate oc-cupational precautions, contributed to the outbreak’s severity.
0
1
2
3
4
5
6
7
8
Cas
es
Date of Symptom Onset
First patient admitted to local hospital
First death
Physician suggests histoplasmosis
Figure 2. Dates of histoplasmosis symptom onset for 26 workers exposed to bat guano during maintenance of tunnels of a hydroelectric dam, Dominican Republic, 2015 (symptom onset dates are not shown for 4 workers due to 3 missing data and 1 extreme outlier).
Downloaded from https://academic.oup.com/cid/advance-article-abstract/doi/10.1093/cid/cix1067/4683412by University of California, San Fransisco useron 14 February 2018
• Leptospirosis initially suspected, but patients did not respond to penicillin
• Histoplasmosis suggested on 8 September, and all 19 hospitalized workers were transferred from local to regional hospitals
Began work30-Jul
Histoplasmosis infection
8
• H. capsulatum most common pulmonary fungal infection
‒ occurs worldwide, especially throughout Americas & Caribbean; no prior reports in DR
‒ 500,000 annually in US, Ohio River valley
‒ 90% cases are self-limited and sub-clinical
• Dimorphic soil saprophyte often found in association with bird or bat droppings (alkaline nitrogenous substrates)
• Occupations: farming, exposure to chicken coops or caves, remodeling or demolition of old buildings, cutting down trees or clearing brush from sites in which blackbirds have roosted
• Exposure by inhalation of microconidia (asexual reproductive spores)
• Transforms into yeast phase in the body, incubation ~1-3 weeks
• Acute/subacute/chronic pulmonary forms; disseminated

[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES AND HANDOUTS]
3/8/183
Histoplasma capsulatum
9
Small, oval yeast cells (2-4 um) packed with macrophages. Giemsa’s stain. 1000 x
In culture, produces hyaline, septate hyphae with microconidia. 400x
From: Carroll KC, et al. Jawetz, Melnick, & Adelberg’s Medical Microbiology, 27e
Diagnosis§ Visualization of yeast in sputum§ Culture takes up to 4 weeks§ Antigen testing of both urine and serum
~40-80% sensitive§ Antibody testing (immunodiffusion,
complement fixation, EIA), may take up to 4-8 weeks
§ PCR not ready for prime time…
Treatment
• None, if mild• Acute: Amphotericin B + corticosteroids• Chronic: itraconozole
10
• CID 2017:XX (XX XXXX) • 5Histoplasmosis in the Dominican Republic
Earlier diagnosis and treatment of histoplasmosis, combined with appropriate occupational precautions, might have pre-vented the 3 deaths observed in this outbreak.
A greater number of days spent in the tunnels was associ-ated with increased risk of severe disease, although this associ-ation was only borderline statistically significant, likely due to the small sample size. It is known that H. capsulatum can exist
in “hotspots,” or pockets within the environment. When these pockets are disrupted, large amounts of spores can be released into the air [1 ]. We suspect that such events occurred during this outbreak, exposing workers to large inocula within short periods of time. Workers’ proximity to these “hotspots” rather than their cumulative time spent in the tunnels may have deter-mined their risk of acquiring histoplasmosis. This hypothesis is
Table 2. Clinical Characteristics of Workers Who Met the Case Definition (n = 30) in Histoplasmosis Outbreak in the Dominican Republic, 2015
Characteristic No. (%) Missing, No.
Level of medical care Inpatient hospitalization 28 (93) Intensive care unit 9 (30)Mechanical ventilation 6 (20)Deaths 3 (10)Symptoms Fever 25 (83) Cough 23 (77) Headache 21 (70) Generalized malaise 15 (50) Difficulty breathing 11 (37) Myalgias 11 (37) Diarrhea 8 (27)Diagnostics CXR 20 (67) Bilateral infiltrates, No. (%) of workers who had a CXR 17 (85) Interstitial consolidation, No. (%) of workers who had a CXR 14 (70) CT chest scan 12 (40) Bilateral infiltrates, No. (%) of workers who had a CT chest scan 11 (100) 1 Interstitial consolidation, No. (%) of workers who had a CT chest scan 11 (100) 1 Bronchoscopy 9 (30) BAL, No. (%) of workers who had a bronchoscopy 7 (100) 2 Evidence of histoplasmosis on pathology, No. (%) of workers who had a BAL 2 (67) 4 Bacterial culture consistent with ventilator–associated pneumonia, No. (%) of workers who had a BAL 6 (86)Laboratory Leukocytosis (WBC >12 × 109/L) 19 (68) 2 AST or ALT >120 U/L 10 (36) 2 HIV (type unknown) 0 (0) 15 Leptospirosis (type unknown) 0 (0) 7Treatment Any antifungal 28 (93) Voriconazole, No. (%) of workers who had any antifungal 22 (79) Itraconazole, No. (%) of workers who had any antifungal 14 (50) Fluconazole, No. (%) of workers who had any antifungal 9 (33) 1 Amphotericin B, No. (%) of workers who had any antifungal 8 (29) Days from symptom onset to first antifungal treatment, No. (%) of workers who had any antifungala 4 0–4 7 (29) 5–6 6 (25) 7–8 6 (25) 9–11 5 (21) Any corticosteroid 26 (87) Corticosteroids prior to antifungal treatment, No. (%) of workers who had any antifungal and any corticosteroid 1 No 12 (48) Corticosteroids received on same day as antifungals 9 (36) Yes 4 (16)
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; BAL, bronchoalveolar lavage; CT, computed tomography; CXR, chest radiograph; HIV, human immunodefi-ciency virus; WBC, white blood cell count.aCategory boundaries set at the quartiles among all workers who met the case definition and who had any antifungal.
Downloaded from https://academic.oup.com/cid/advance-article-abstract/doi/10.1093/cid/cix1067/4683412by University of California, San Fransisco useron 14 February 2018
Clinical Characteristics in those meeting case definition (n=30/36)
Lab analyses:Serum and/or urine collected 5-33 days after symptom onset.
Antigen test positive in 53% serum, 45% urine
Antibody (immunodiffusion) positive in 35%
Characteristics associated with developing Histoplasmosis (none significant)
11
6 • CID 2017:XX (XX XXXX) • Armstrong et al
supported by the clustering of symptom onset during a 2-week period rather than over the entire duration of the tunnel work.
Increased education and awareness of histoplasmosis among clinicians is needed to respond to cases and future outbreaks in the DR, as early treatment with an appropriate antifungal can reduce morbidity and mortality [1]. As elsewhere in Latin America and the Caribbean, histoplasmosis is likely an im-portant cause of disease. In fact, we suspect that had convales-cent testing been performed, we would have detected exposure and antibody response in even more of the tunnel workers. In the acute setting, antibodies may not yet have formed and antigen-based testing can be falsely negative. Unfortunately, we were unable to collect convalescent sera in this outbreak in-vestigation [10]. Enhanced availability of histoplasmosis diag-nostics may help uncover an unrecognized burden of illness. Historically, antibody and antigen testing has been performed by only a limited number of laboratories worldwide. Newer diagnostic technologies, such as point-of-care loop-mediated isothermal amplification or lateral flow assays, could facilitate rapid detection and treatment, especially in resource-limited settings [11].
Because tunnels involved in this outbreak could not be closed for access, as they are needed for continued maintenance of the dam, using the occupational health and safety hierarchy of con-trols will be important for preventing additional illnesses [12].
Development of a site safety plan is an important step in min-imizing exposure, and provides direction for continued access and work in the tunnels. Additional methods, such as moisten-ing material prior to translocation, can reduce dust generation and spore dispersal [12]. Given the likely spore burden present in the guano, when removed it should be treated as biohaz-ard waste to minimize further disease [12]. Worker training is another key component and should address heat exhaustion, health risk communication, appropriate use of personal protec-tive equipment, and compliance with occupational health and environmental safety recommendations [12]. The US National Institute for Occupational Safety and Health (NIOSH) has devel-oped recommendations for the prevention of histoplasmosis in occupational settings [12]. NIOSH considers disposable N95 respirators to be the lowest acceptable level of protection needed when working in areas with the potential for H. capsulatum exposure [12]. In this outbreak, the tunnel workers were pro-vided with paper surgical masks that were not consistently worn and would not have provided adequate protection.
Applying the safe work practices discussed above to the set-ting of this outbreak may be challenging given the tropical cli-mate and limited resources. The tunnels are poorly ventilated and hot, likely limiting extended use of any type of respirator; furthermore, personal protective equipment can be costly. Specialists, such as an industrial hygienist, could help determine
Table 3. Associations Between Characteristics and Developing Histoplasmosis Among Tunnel Workers (n = 36) in the Dominican Republic, 2015
Characteristic
Histoplasmosis
Yes No Unadjusted Odds Ratio (Exact 95% CI) Exact P Value
Age, ya
18–32 14 (48) 4 (67) 1.00 Reference Reference 33–62 15 (52) 2 (33) 2.10 (.3–26.65) .72Asthma 4 (15) 1 (17) 0.87 (.06–51.28) >.99Current cigarette smoking 12 (41) 3 (50) 0.71 (.08–6.27) >.99Illicit drug use (noninjection) 9 (35) 3 (60) 0.37 (.03–3.81) .56Type of work Shoveling/filling only 13 (45) 2 (33) 1.00 Reference Reference Transporting wheelbarrow only 2 (7) 3 (50) 0.12 (.01–1.71) .15 Shoveling/filling and transporting wheelbarrow 10 (34) 1 (17) 1.51 (.07–99.71) >.99 Supervising 3 (10) 0 (0) 0.49b (.05–∞) >.99 Other 1 (3) 0 (0) 0.14b (.01–∞) >.99Tunnel of work Tunnel 1 only 10 (34) 0 (0) 3.39b (.53–∞) .30 Tunnel 2 only 5 (17) 2 (33) 0.72 (.07–10.36) >.99 Tunnels 1 and 2 14 (48) 4 (67) 1.00 Reference ReferenceCumulative days worked in tunnels (per additional day worked) 1.04 (.93–1.15) .46Personal protective equipment use: surgical mask Never 13 (48) 3 (50) 1.00 Reference Reference Sometimes 11 (41) 3 (50) 0.85 (.09–7.71) >.99 Always 3 (11) 0 (0) 0.8b (.09–∞) >.99
Data are presented as No. (%) unless otherwise indicated.
Abbreviation: CI, confidence interval.aCategory boundary set at the median among all workers.bMedian unbiased estimate.
Downloaded from https://academic.oup.com/cid/advance-article-abstract/doi/10.1093/cid/cix1067/4683412by University of California, San Fransisco useron 14 February 2018
p=0.15
Characteristics associated with developing severeHistoplasmosis (ICU admission, n=9)
12
• CID 2017:XX (XX XXXX) • 7Histoplasmosis in the Dominican Republic
the most appropriate and feasible options (see Supplementary Materials for full details).
Our study had several limitations that may have interfered with our ability to detect associations. First, we interviewed workers several weeks after work in the tunnels concluded, po-tentially introducing recall bias. Second, it is conceivable that given the widespread medical evaluation of exposed workers, some may have overreported symptoms. This could increase the number of cases detected, biasing the risk ratio toward the null. Finally, the small sample size limited our ability to adjust for potential confounders or to find risk factors associated with developing histoplasmosis or severe disease.
This outbreak adds to evidence that histoplasmosis is under-diagnosed in Latin America and the Caribbean [7, 13–17]. Increased awareness of the disease among clinicians and public health officials, improved diagnostic capacity, and access to antifungals is essential in helping to prevent severe illness and death. Occupational health precautions during higher-risk
activities, particularly those involving disturbances to bird and bat guano, could reduce worker exposure to H. capsulatum. Because workers are often at higher risk of exposure than the general population, the identification of high-risk environ-ments as well as the implementation of appropriate engineering and administrative controls and adequate personal protective equipment may help to prevent similar outbreaks in the future.
Supplementary DataSupplementary materials are available at Clinical Infectious Diseases online. Consisting of data provided by the authors to benefit the reader, the posted materials are not copyedited and are the sole responsibility of the authors, so questions or comments should be addressed to the corresponding author.
NotesDisclaimer. The findings and the conclusions in this report are those
of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention (CDC) or the National Institute for Occupational Safety and Health (NIOSH).
Financial support. This work was supported by the CDC and NIOSH.
Table 4. Associations Between Characteristics and Developing Severe Histoplasmosis (Defined as Admission to Intensive Care Unit) Among Tunnel Workers (n = 36) in the Dominican Republic, 2015
Characteristic
ICU Admission
Yes No Unadjusted Odds Ratio (Exact 95% CI) Exact P Value
Age, ya
18–32 3 (33) 15 (58) 1.00 Reference Reference 33–62 6 (67) 11 (42) 2.65 (.45–20.07) .38Asthma 0 (0) 5 (20) 0.41b (.00–2.52) .45Current cigarette smoking 3 (33) 12 (46) 0.59 (.08–3.54) .79Illicit drug use (noninjection) 1 (13) 11 (48) 0.16 (<.01–1.63) .17Type of work Shoveling/filling only 5 (56) 10 (38) 1.00 Reference Reference Transporting wheelbarrow only 1 (11) 4 (15) 0.52 (.01–7.42) >.99 Shoveling/filling and transporting wheelbarrow 2 (22) 9 (35) 0.46 (.04–3.73) .69 Supervising 1 (11) 2 (8) 1.00 (.01–23.97) >.99 Other 0 (0) 1 (4) 2.20b (.00–41.80) >.99Tunnel of work Tunnel 1 only 4 (44) 6 (23) 3.18 (.40–28.95) .36 Tunnel 2 only 2 (22) 5 (19) 1.94 (.13–22.90) .87 Tunnels 1 and 2 3 (33) 15 (58) 1.00 Reference ReferenceCumulative days worked in tunnels (per additional day worked) 1.18 (1.00–1.59) .06Personal protective equipment use: surgical mask Never 4 (50) 12 (48) 1.00 Reference Reference Sometimes 3 (38) 11 (44) 0.82 (.10–6.14) >.99 Always 1 (13) 2 (8) 1.47 (.02–36.16) >.99Days from symptom onset to first antifungal treatmentc,d
0–4 0 (0) 7 (47) 0.16a (.00–1.22) .13 5–6 4 (44) 2 (13) 1.89 (.12–37.87) >.99 7–8 3 (33) 3 (20) 1.00 Reference Reference 9–11 2 (22) 3 (20) 0.69 (.03–12.15) >.99
Data are presented as No. (%) unless otherwise indicated.
Abbreviations: CI, confidence interval, ICU, intensive care unit.aCategory boundary set at the median among all workers.bMedian unbiased estimate.cAmong only the 28 workers who had received any antifungal.dCategory boundaries set at the quartiles among all workers who met the case definition and who had received any antifungal.
Downloaded from https://academic.oup.com/cid/advance-article-abstract/doi/10.1093/cid/cix1067/4683412by University of California, San Fransisco useron 14 February 2018
[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES AND HANDOUTS]
3/8/184
Conclusions
13
• No prior history of Histo outbreaks in DR, likely unrecognized
• High proportion of hospitalization & death
‒ Delayed use of antifungals, and of Amphotericin B in particular
‒ Paucity of serologic or urine diagnostic capacity
‒ Probable high H. capsulatum inocula in tunnels
• Prevention
‒ Develop safety plan
‒ Moistening material prior to translocation
‒ PPE (N95 respirators at a minimum)
§ Largest case series of CTE§ The first major study to apply standard
clinicopathological and pathological criteria
14
Clinicopathological Evaluation of Chronic TraumaticEncephalopathy in Players of American FootballJesse Mez, MD, MS; Daniel H. Daneshvar, MD, PhD; Patrick T. Kiernan, BA; Bobak Abdolmohammadi, BA;Victor E. Alvarez, MD; Bertrand R. Huber, MD, PhD; Michael L. Alosco, PhD; Todd M. Solomon, PhD;Christopher J. Nowinski, PhD; Lisa McHale, EdS; Kerry A. Cormier, BA; Caroline A. Kubilus; Brett M. Martin, MS;Lauren Murphy, MBA; Christine M. Baugh, MPH; Phillip H. Montenigro, BA; Christine E. Chaisson, MPH;Yorghos Tripodis, PhD; Neil W. Kowall, MD; Jennifer Weuve, MPH, ScD; Michael D. McClean, ScD;Robert C. Cantu, MD; Lee E. Goldstein, MD, PhD; Douglas I. Katz, MD; Robert A. Stern, PhD;Thor D. Stein, MD, PhD; Ann C. McKee, MD
IMPORTANCE Players of American football may be at increased risk of long-term neurologicalconditions, particularly chronic traumatic encephalopathy (CTE).
OBJECTIVE To determine the neuropathological and clinical features of deceased footballplayers with CTE.
DESIGN, SETTING, AND PARTICIPANTS Case series of 202 football players whose brains weredonated for research. Neuropathological evaluations and retrospective telephone clinicalassessments (including head trauma history) with informants were performed blinded.Online questionnaires ascertained athletic and military history.
EXPOSURES Participation in American football at any level of play.
MAIN OUTCOMES AND MEASURES Neuropathological diagnoses of neurodegenerativediseases, including CTE, based on defined diagnostic criteria; CTE neuropathological severity(stages I to IV or dichotomized into mild [stages I and II] and severe [stages III and IV]);informant-reported athletic history and, for players who died in 2014 or later, clinicalpresentation, including behavior, mood, and cognitive symptoms and dementia.
RESULTS Among 202 deceased former football players (median age at death, 66 years[interquartile range, 47-76 years]), CTE was neuropathologically diagnosed in 177 players(87%; median age at death, 67 years [interquartile range, 52-77 years]; mean years of footballparticipation, 15.1 [SD, 5.2]), including 0 of 2 pre–high school, 3 of 14 high school (21%), 48 of53 college (91%), 9 of 14 semiprofessional (64%), 7 of 8 Canadian Football League (88%),and 110 of 111 National Football League (99%) players. Neuropathological severity of CTE wasdistributed across the highest level of play, with all 3 former high school players having mildpathology and the majority of former college (27 [56%]), semiprofessional (5 [56%]), andprofessional (101 [86%]) players having severe pathology. Among 27 participants with mildCTE pathology, 26 (96%) had behavioral or mood symptoms or both, 23 (85%) had cognitivesymptoms, and 9 (33%) had signs of dementia. Among 84 participants with severe CTEpathology, 75 (89%) had behavioral or mood symptoms or both, 80 (95%) had cognitivesymptoms, and 71 (85%) had signs of dementia.
CONCLUSIONS AND RELEVANCE In a convenience sample of deceased football players whodonated their brains for research, a high proportion had neuropathological evidence of CTE,suggesting that CTE may be related to prior participation in football.
JAMA. 2017;318(4):360-370. doi:10.1001/jama.2017.8334
Editorial page 338
Author Video Interview andJAMA Report Video
Supplemental content
CME Quiz atjamanetwork.com/learning
Author Affiliations: Authoraffiliations are listed at the end of thisarticle.
Corresponding Author: Ann C.McKee, MD, Neuropathology Service,VA Boston Healthcare System, CTECenter, Boston University Alzheimer’sDisease Center, Boston UniversitySchool of Medicine, 150 S HuntingtonAve, Boston, MA 02118 ([email protected]).
Research
JAMA | Original Investigation
360 (Reprinted) jama.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a UCSF LIBRARY User on 01/29/2018
Clinicopathological Evaluation of Chronic TraumaticEncephalopathy in Players of American FootballJesse Mez, MD, MS; Daniel H. Daneshvar, MD, PhD; Patrick T. Kiernan, BA; Bobak Abdolmohammadi, BA;Victor E. Alvarez, MD; Bertrand R. Huber, MD, PhD; Michael L. Alosco, PhD; Todd M. Solomon, PhD;Christopher J. Nowinski, PhD; Lisa McHale, EdS; Kerry A. Cormier, BA; Caroline A. Kubilus; Brett M. Martin, MS;Lauren Murphy, MBA; Christine M. Baugh, MPH; Phillip H. Montenigro, BA; Christine E. Chaisson, MPH;Yorghos Tripodis, PhD; Neil W. Kowall, MD; Jennifer Weuve, MPH, ScD; Michael D. McClean, ScD;Robert C. Cantu, MD; Lee E. Goldstein, MD, PhD; Douglas I. Katz, MD; Robert A. Stern, PhD;Thor D. Stein, MD, PhD; Ann C. McKee, MD
IMPORTANCE Players of American football may be at increased risk of long-term neurologicalconditions, particularly chronic traumatic encephalopathy (CTE).
OBJECTIVE To determine the neuropathological and clinical features of deceased footballplayers with CTE.
DESIGN, SETTING, AND PARTICIPANTS Case series of 202 football players whose brains weredonated for research. Neuropathological evaluations and retrospective telephone clinicalassessments (including head trauma history) with informants were performed blinded.Online questionnaires ascertained athletic and military history.
EXPOSURES Participation in American football at any level of play.
MAIN OUTCOMES AND MEASURES Neuropathological diagnoses of neurodegenerativediseases, including CTE, based on defined diagnostic criteria; CTE neuropathological severity(stages I to IV or dichotomized into mild [stages I and II] and severe [stages III and IV]);informant-reported athletic history and, for players who died in 2014 or later, clinicalpresentation, including behavior, mood, and cognitive symptoms and dementia.
RESULTS Among 202 deceased former football players (median age at death, 66 years[interquartile range, 47-76 years]), CTE was neuropathologically diagnosed in 177 players(87%; median age at death, 67 years [interquartile range, 52-77 years]; mean years of footballparticipation, 15.1 [SD, 5.2]), including 0 of 2 pre–high school, 3 of 14 high school (21%), 48 of53 college (91%), 9 of 14 semiprofessional (64%), 7 of 8 Canadian Football League (88%),and 110 of 111 National Football League (99%) players. Neuropathological severity of CTE wasdistributed across the highest level of play, with all 3 former high school players having mildpathology and the majority of former college (27 [56%]), semiprofessional (5 [56%]), andprofessional (101 [86%]) players having severe pathology. Among 27 participants with mildCTE pathology, 26 (96%) had behavioral or mood symptoms or both, 23 (85%) had cognitivesymptoms, and 9 (33%) had signs of dementia. Among 84 participants with severe CTEpathology, 75 (89%) had behavioral or mood symptoms or both, 80 (95%) had cognitivesymptoms, and 71 (85%) had signs of dementia.
CONCLUSIONS AND RELEVANCE In a convenience sample of deceased football players whodonated their brains for research, a high proportion had neuropathological evidence of CTE,suggesting that CTE may be related to prior participation in football.
JAMA. 2017;318(4):360-370. doi:10.1001/jama.2017.8334
Editorial page 338
Author Video Interview andJAMA Report Video
Supplemental content
CME Quiz atjamanetwork.com/learning
Author Affiliations: Authoraffiliations are listed at the end of thisarticle.
Corresponding Author: Ann C.McKee, MD, Neuropathology Service,VA Boston Healthcare System, CTECenter, Boston University Alzheimer’sDisease Center, Boston UniversitySchool of Medicine, 150 S HuntingtonAve, Boston, MA 02118 ([email protected]).
Research
JAMA | Original Investigation
360 (Reprinted) jama.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a UCSF LIBRARY User on 01/29/2018
Background: Chronic Traumatic Encephalopathy (CTE)
15
• A progressive neurodegeneration associated with repetitive head trauma and associated cognitive and behavioral syndrome
• Features noted in boxes in 1970s, football players in 2005 (Omalu et al, Neurosurgery, 2005;57(1))
• Large series (n=68) reported in 2013 with proposed staging scheme (McKee et al, Brain, 2013;136(1))
• Clinicopathological correlation developed 2014 (Mez et al, AlzheimersRes Ther, 2015;7(1))
• Standardized pathological criteria developed 2015 by NINDS & National Institute of Biomedical Imaging and Bioengineering (McKee et al, Acta Neuropathol, 2016;131)
Study Recruitment
16
• Brainbank created 2008 to study long-term effects of repetitive head
trauma through contact sports and military-related trauma
• Collaboration of VA Boston Healthcare System, Boston University,
Concussion Legacy Foundation (CLF)
• Inclusion criteria:
‒ Exposure to repetitive head trauma (e.g., contact sports, military service, or domestic violence)
‒ Playing American football was sufficient for inclusion
§ Beginning 2014, at least 2 years college-level play required
‒ Irrespective of clinical symptoms
‒ Postmortem interval < 72 hours
• Most donors’ kin approached the brainbank near the time of death
(81%), 9% referred by medical examiners, 6% “recruited” by CLF, 4%
enrolled in brainbank registry during life
[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES AND HANDOUTS]
3/8/185
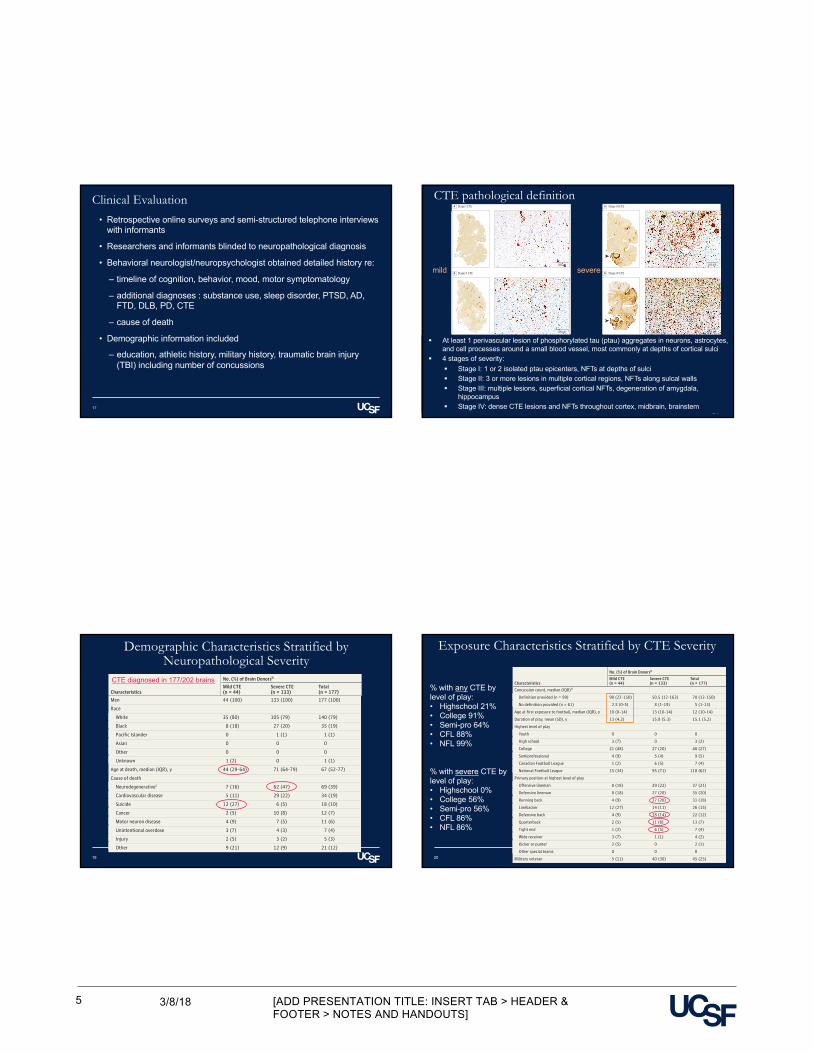
Clinical Evaluation
17
• Retrospective online surveys and semi-structured telephone interviews with informants
• Researchers and informants blinded to neuropathological diagnosis
• Behavioral neurologist/neuropsychologist obtained detailed history re:
‒ timeline of cognition, behavior, mood, motor symptomatology
‒ additional diagnoses : substance use, sleep disorder, PTSD, AD, FTD, DLB, PD, CTE
‒ cause of death
• Demographic information included
‒ education, athletic history, military history, traumatic brain injury (TBI) including number of concussions
18
including the hippocampus, amygdala, and entorhinal cor-tex (Figure 2, black arrowheads, and Figure 3). Neurofibril-lary tangles were also frequent in the thalamus, nucleusbasalis of Meynert, substantia innominata, substantia nigra,and locus coeruleus in severe CTE (Figure 3).
Deposition of amyloid-β was present in a subset of par-ticipants at all stages of CTE pathology, predominantly asdiffuse amyloid-β plaques, but neuritic amyloid-β plaquesand amyloid angiopathy were also present. In stage IV CTE,amyloid-β deposition occurred in 52 cases (91%). Depositionof TDP-43 and α-synuclein were found in all stages of CTEpathology; TDP-43 deposition occurred in 47 (83%) andα-synuclein deposition occurred in 23 (40%) stage IV CTEcases (Table 2).
Among the 25 football players without CTE, 9 showedno pathological abnormalities and 7 showed nonspecificchanges; eg, hemosiderin-laden macrophages (n = 7) andaxonal injury (n = 5). Other diagnoses included vascularpathology (n = 4), unspecified tauopathy not meeting crite-
ria for CTE (n = 3), AD (n = 2), argyrophilic grain disease(n = 1), and Lewy body disease (n = 1).
Data on informants were collected beginning in 2014.The median number of participating informants was 2(IQR, 1-3) per participant. Among all of the interviews,71 (64%) included a spouse/partner, 56 (51%) included anadult child, 27 (24%) included a sibling, 16 (14%) includeda parent, 13 (12%) included a non–first-degree relative, 8(7.2%) included a neighbor or friend, and 4 included otherinformants. Among the informants who knew the partici-pant the longest, the mean relationship length was 45.8years (SD, 1.5 years).
Among the 111 CTE cases with standardized informantreports on clinical symptoms, a reported progressive clinicalcourse was common in participants with both mild andsevere CTE pathology, occurring in 23 (85%) mild casesand 84 (100%) severe cases (Table 3). Behavioral or moodsymptoms were common in participants with both mild andsevere CTE pathology, with symptoms occurring in 26
Figure 1. Representative Images of Phosphorylated Tau Pathology at CTE Pathological Stages I and II
100 μm
A Stage I CTE
100 μm
B Stage II CTE
CTE indicates chronic traumatic encephalopathy; NFT, neurofibrillary tangle;ptau, phosphorylated tau. For all images, 10-µm paraffin-embedded tissuesections were immunostained with microscopic mouse monoclonal antibodyfor phosphorylated tau (AT8) (Pierce Endogen). Positive ptau immunostainingappears dark red, hematoxylin counterstain; calibration bar indicates 100 µm.Stage I CTE is characterized by 1 or 2 isolated perivascular epicenters of ptauNFTs and neurites (ie, CTE lesions) at the depths of the cortical sulci. In stage II,3 or more cortical CTE lesions are found. All hemispheric tissue section imagesare 50-µm sections immunostained with mouse monoclonal antibody CP-13,directed against phosphoserine 202 of tau (courtesy of Peter Davies, PhD,Feinstein Institute for Medical Research; 1:200); this is considered to be an early
site of tau phosphorylation in NFT formation.28 Positive ptau immunostainingappears dark brown. A, Former college football player with stage I CTE. Twoperivascular ptau CTE lesions are evident at sulcal depths of the frontal cortex;there is no neurofibrillary degeneration in the medial temporal lobe (openarrowhead). Perivascular CTE lesion: neurofibrillary tangles and dot-like andthreadlike neurites encircle a small blood vessel. B, Former NFL player withstage II CTE. There are multiple perivascular ptau CTE lesions at depths of sulciof the frontal cortex; there is no neurofibrillary degeneration in the medialtemporal lobe (open arrowhead). Perivascular CTE lesion: a cluster of NFTs andlarge dot-like and threadlike neurites surround a small blood vessel.
Research Original Investigation Evaluation of Chronic Traumatic Encephalopathy in Football Players
364 JAMA July 25, 2017 Volume 318, Number 4 (Reprinted) jama.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a UCSF LIBRARY User on 01/29/2018
(96%) mild cases and 75 (89%) severe cases. Impulsivity,depressive symptoms, apathy, and anxiety occurred in 23(89%), 18 (67%), 13 (50%), and 14 (52%) mild cases and 65(80%), 46 (56%), 43 (52%), and 41 (50%) severe cases,respectively. Additionally, hopelessness, explosivity, beingverbally violent, being physically violent, and suicidality(including ideation, attempts, or completions) occurred in18 (69%), 18 (67%), 17 (63%), 14 (52%), and 15 (56%) mildcases, respectively. Substance use disorders were also com-mon in participants with mild CTE, occurring in 18 (67%)mild cases. Symptoms of posttraumatic stress disorder wereuncommon in both groups, occurring in 3 (11%) mild casesand 9 (11%) severe cases.
Cognitive symptoms were common in participants withboth mild and severe CTE pathology, with symptoms occur-ring in 23 (85%) mild cases and 80 (95%) severe cases.Memory, executive function, and attention symptomsoccurred in 19 (73%), 19 (73%), and 18 (69%) mild cases and76 (92%), 67 (81%), and 67 (81%) severe cases, respectively.
Additionally, language and visuospatial symptoms occurredin 54 (66%) and 44 (54%) severe cases, respectively. Apremortem diagnosis of AD and a postmortem (but blindedto pathology) consensus diagnosis of dementia were com-mon in severe cases, occurring in 21 (25%) and 71 (85%),respectively. There were no asymptomatic (ie, no mood/behavior or cognitive symptoms) CTE cases. Motor symp-toms were common in severe cases, occurring in 63 (75%).Gait instability and slowness of movement occurred in 55(66%) and 42 (50%) severe cases, respectively. Symptomfrequencies remained similar when only pure CTE cases(ie, those with no neuropathological evidence of comorbidneurodegenerative disease) were considered (eTable in theSupplement).
Among the 111 CTE cases with standardized informantreports on clinical symptoms, 47 (42.3%; median age atdeath, 76 years [IQR, 63-81 years]) initially presented withcognitive symptoms, 48 (43.2%; median age at death, 66years [IQR, 54-73 years]) initially presented with behavior or
Figure 2. Representative Images of Phosphorylated Tau Pathology at CTE Pathological Stages III and IV
100 μm
100 μm
A Stage III CTE
B Stage IV CTE
CTE indicates chronic traumatic encephalopathy; NFT, neurofibrillary tangle;ptau, phosphorylated tau. For all images, 10-µm paraffin-embedded tissuesections were immunostained with microscopic mouse monoclonal antibodyfor phosphorylated tau (AT8) (Pierce Endogen). Positive ptau immunostainingappears dark red, hematoxylin counterstain; calibration bar indicates 100 µm.In stage III CTE, multiple CTE lesions and diffuse neurofibrillary degenerationof the medial temporal lobe are found. In stage IV CTE, CTE lesions and NFTsare widely distributed throughout the cerebral cortex, diencephalon,and brain stem.6 All hemispheric tissue section images are 50-µm sectionsimmunostained with mouse monoclonal antibody CP-13, directed againstphosphoserine 202 of tau (courtesy of Peter Davies, PhD, Feinstein Institutefor Medical Research; 1:200); this is considered to be an early site of
tau phosphorylation in NFT formation.28 Positive ptau immunostaining appearsdark brown. A, Former NFL player with stage III CTE. There are multiple largeCTE lesions in the frontal cortex and insula; there is diffuse neurofibrillarydegeneration of hippocampus and entorhinal cortex (black arrowhead).Perivascular CTE lesion: a dense collection of NFTs and large dot-like andthreadlike neurites enclose several small blood vessels. B, Former NFL playerwith stage IV CTE. There are large, confluent CTE lesions in the frontal,temporal, and insular cortices and there is diffuse neurofibrillary degenerationof the amygdala and entorhinal cortex (black arrowhead). Perivascular CTElesion: a large accumulation of NFTs, many of them ghost tangles, encompassseveral small blood vessels.
Evaluation of Chronic Traumatic Encephalopathy in Football Players Original Investigation Research
jama.com (Reprinted) JAMA July 25, 2017 Volume 318, Number 4 365
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a UCSF LIBRARY User on 01/29/2018
CTE pathological definition
§ At least 1 perivascular lesion of phosphorylated tau (ptau) aggregates in neurons, astrocytes, and cell processes around a small blood vessel, most commonly at depths of cortical sulci
§ 4 stages of severity:§ Stage I: 1 or 2 isolated ptau epicenters, NFTs at depths of sulci§ Stage II: 3 or more lesions in multiple cortical regions, NFTs along sulcal walls§ Stage III: multiple lesions, superficial cortical NFTs, degeneration of amygdala,
hippocampus§ Stage IV: dense CTE lesions and NFTs throughout cortex, midbrain, brainstem
mild severe
the cerebral cortex (Figure 1 and Figure 2). In cases withmild CTE pathology (stages I and II), isolated perivascularCTE lesions were found at the sulcal depths of the cerebralcortex, most commonly in the superior and dorsolateralfrontal cortices, but also in the lateral temporal, inferiorparietal, insula, and septal cortices (Figure 1). Neurofibril-lary tangles were sparse in other cortical regions, and therewas no diffuse neurofibrillary degeneration of the medial
temporal lobe structures (Figure 1, open arrowheads). Neu-rofibrillary tangles were also found in the locus coeruleus,substantia nigra, and substantia innominata (Figure 3) inmild CTE. In cases with severe CTE pathology, perivascularCTE lesions were large and confluent (Figure 2). Neurofibril-lary tangles were widely distributed in the superficial lami-nae of cortical regions and there was severe neurofibrillarydegeneration of the medial temporal lobe structures,
Table 1. Demographic and Exposure Characteristics of 177 American Football Players Diagnosed With CTE,Stratified by Neuropathological Severitya
Characteristics
No. (%) of Brain Donorsb
Mild CTE(n = 44)
Severe CTE(n = 133)
Total(n = 177)
Men 44 (100) 133 (100) 177 (100)
Race
White 35 (80) 105 (79) 140 (79)
Black 8 (18) 27 (20) 35 (19)
Pacific Islander 0 1 (1) 1 (1)
Asian 0 0 0
Other 0 0 0
Unknown 1 (2) 0 1 (1)
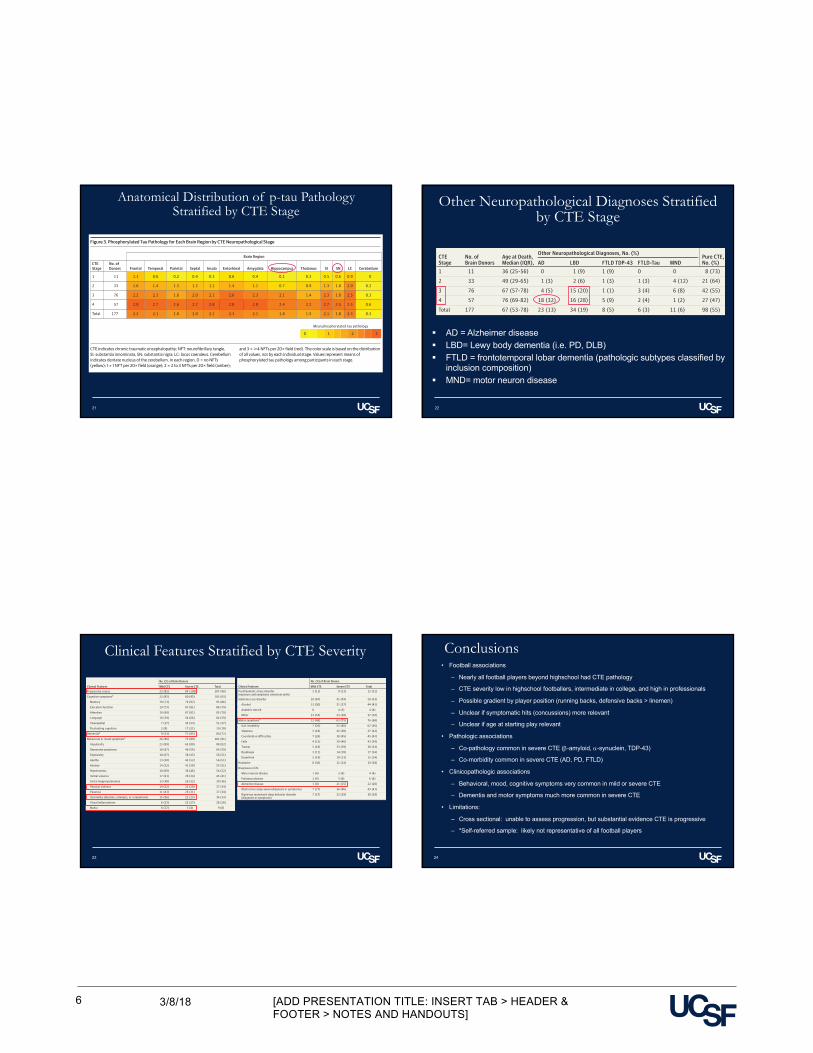
Age at death, median (IQR), y 44 (29-64) 71 (64-79) 67 (52-77)
Cause of death
Neurodegenerativec 7 (16) 62 (47) 69 (39)
Cardiovascular disease 5 (11) 29 (22) 34 (19)
Suicide 12 (27) 6 (5) 18 (10)
Cancer 2 (5) 10 (8) 12 (7)
Motor neuron disease 4 (9) 7 (5) 11 (6)
Unintentional overdose 3 (7) 4 (3) 7 (4)
Injury 2 (5) 3 (2) 5 (3)
Other 9 (21) 12 (9) 21 (12)
Concussion count, median (IQR)d
Definition provided (n = 99) 90 (22-150) 50.5 (12-163) 70 (12-150)
No definition provided (n = 61) 2.5 (0-5) 8 (1-19) 5 (1-13)
Age at first exposure to football, median (IQR), y 10 (8-14) 13 (10-14) 12 (10-14)
Duration of play, mean (SD), y 13 (4.2) 15.8 (5.3) 15.1 (5.2)
Highest level of play
Youth 0 0 0
High school 3 (7) 0 3 (2)
College 21 (48) 27 (20) 48 (27)
Semiprofessional 4 (9) 5 (4) 9 (5)
Canadian Football League 1 (2) 6 (5) 7 (4)
National Football League 15 (34) 95 (71) 110 (62)
Primary position at highest level of play
Offensive lineman 8 (18) 29 (22) 37 (21)
Defensive lineman 8 (18) 27 (20) 35 (20)
Running back 4 (9) 27 (20) 31 (18)
Linebacker 12 (27) 14 (11) 26 (15)
Defensive back 4 (9) 18 (14) 22 (12)
Quarterback 2 (5) 11 (8) 13 (7)
Tight end 1 (2) 6 (5) 7 (4)
Wide receiver 3 (7) 1 (1) 4 (2)
Kicker or punter 2 (5) 0 2 (1)
Other special teams 0 0 0
Military veteran 5 (11) 40 (30) 45 (25)
Abbreviations: CTE, chronictraumatic encephalopathy; IQR,interquartile range.a Mild CTE (CTE neuropathological
stages I and II) is characterized bysparse to frequent perivascular CTElesions at the sulcal depths of thecerebral cortex. Severe CTE (CTEneuropathological stages III and IV)consists of multiple CTE lesions inthe cerebral cortex and moderate tosevere neurofibrillary degenerationof medial temporal lobe,diencephalon, and brain stem.
b Data are expressed as No. (%)unless otherwise indicated.
c Includes dementia-relatedand parkinsonian-related causesof death.
d Median estimates of the numberof concussions reportedper participant. Beginningin 2014, informants were reada formal definition of concussionprior to being asked aboutconcussion history.
Evaluation of Chronic Traumatic Encephalopathy in Football Players Original Investigation Research
jama.com (Reprinted) JAMA July 25, 2017 Volume 318, Number 4 363
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a UCSF LIBRARY User on 01/29/2018
19
Demographic Characteristics Stratified by Neuropathological Severity
CTE diagnosed in 177/202 brains
20
the cerebral cortex (Figure 1 and Figure 2). In cases withmild CTE pathology (stages I and II), isolated perivascularCTE lesions were found at the sulcal depths of the cerebralcortex, most commonly in the superior and dorsolateralfrontal cortices, but also in the lateral temporal, inferiorparietal, insula, and septal cortices (Figure 1). Neurofibril-lary tangles were sparse in other cortical regions, and therewas no diffuse neurofibrillary degeneration of the medial
temporal lobe structures (Figure 1, open arrowheads). Neu-rofibrillary tangles were also found in the locus coeruleus,substantia nigra, and substantia innominata (Figure 3) inmild CTE. In cases with severe CTE pathology, perivascularCTE lesions were large and confluent (Figure 2). Neurofibril-lary tangles were widely distributed in the superficial lami-nae of cortical regions and there was severe neurofibrillarydegeneration of the medial temporal lobe structures,
Table 1. Demographic and Exposure Characteristics of 177 American Football Players Diagnosed With CTE,Stratified by Neuropathological Severitya
Characteristics
No. (%) of Brain Donorsb
Mild CTE(n = 44)
Severe CTE(n = 133)
Total(n = 177)
Men 44 (100) 133 (100) 177 (100)
Race
White 35 (80) 105 (79) 140 (79)
Black 8 (18) 27 (20) 35 (19)
Pacific Islander 0 1 (1) 1 (1)
Asian 0 0 0
Other 0 0 0
Unknown 1 (2) 0 1 (1)
Age at death, median (IQR), y 44 (29-64) 71 (64-79) 67 (52-77)
Cause of death
Neurodegenerativec 7 (16) 62 (47) 69 (39)
Cardiovascular disease 5 (11) 29 (22) 34 (19)
Suicide 12 (27) 6 (5) 18 (10)
Cancer 2 (5) 10 (8) 12 (7)
Motor neuron disease 4 (9) 7 (5) 11 (6)
Unintentional overdose 3 (7) 4 (3) 7 (4)
Injury 2 (5) 3 (2) 5 (3)
Other 9 (21) 12 (9) 21 (12)
Concussion count, median (IQR)d
Definition provided (n = 99) 90 (22-150) 50.5 (12-163) 70 (12-150)
No definition provided (n = 61) 2.5 (0-5) 8 (1-19) 5 (1-13)
Age at first exposure to football, median (IQR), y 10 (8-14) 13 (10-14) 12 (10-14)
Duration of play, mean (SD), y 13 (4.2) 15.8 (5.3) 15.1 (5.2)
Highest level of play
Youth 0 0 0
High school 3 (7) 0 3 (2)
College 21 (48) 27 (20) 48 (27)
Semiprofessional 4 (9) 5 (4) 9 (5)
Canadian Football League 1 (2) 6 (5) 7 (4)
National Football League 15 (34) 95 (71) 110 (62)
Primary position at highest level of play
Offensive lineman 8 (18) 29 (22) 37 (21)
Defensive lineman 8 (18) 27 (20) 35 (20)
Running back 4 (9) 27 (20) 31 (18)
Linebacker 12 (27) 14 (11) 26 (15)
Defensive back 4 (9) 18 (14) 22 (12)
Quarterback 2 (5) 11 (8) 13 (7)
Tight end 1 (2) 6 (5) 7 (4)
Wide receiver 3 (7) 1 (1) 4 (2)
Kicker or punter 2 (5) 0 2 (1)
Other special teams 0 0 0
Military veteran 5 (11) 40 (30) 45 (25)
Abbreviations: CTE, chronictraumatic encephalopathy; IQR,interquartile range.a Mild CTE (CTE neuropathological
stages I and II) is characterized bysparse to frequent perivascular CTElesions at the sulcal depths of thecerebral cortex. Severe CTE (CTEneuropathological stages III and IV)consists of multiple CTE lesions inthe cerebral cortex and moderate tosevere neurofibrillary degenerationof medial temporal lobe,diencephalon, and brain stem.
b Data are expressed as No. (%)unless otherwise indicated.
c Includes dementia-relatedand parkinsonian-related causesof death.
d Median estimates of the numberof concussions reportedper participant. Beginningin 2014, informants were reada formal definition of concussionprior to being asked aboutconcussion history.
Evaluation of Chronic Traumatic Encephalopathy in Football Players Original Investigation Research
jama.com (Reprinted) JAMA July 25, 2017 Volume 318, Number 4 363
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a UCSF LIBRARY User on 01/29/2018
Exposure Characteristics Stratified by CTE Severity
the cerebral cortex (Figure 1 and Figure 2). In cases withmild CTE pathology (stages I and II), isolated perivascularCTE lesions were found at the sulcal depths of the cerebralcortex, most commonly in the superior and dorsolateralfrontal cortices, but also in the lateral temporal, inferiorparietal, insula, and septal cortices (Figure 1). Neurofibril-lary tangles were sparse in other cortical regions, and therewas no diffuse neurofibrillary degeneration of the medial
temporal lobe structures (Figure 1, open arrowheads). Neu-rofibrillary tangles were also found in the locus coeruleus,substantia nigra, and substantia innominata (Figure 3) inmild CTE. In cases with severe CTE pathology, perivascularCTE lesions were large and confluent (Figure 2). Neurofibril-lary tangles were widely distributed in the superficial lami-nae of cortical regions and there was severe neurofibrillarydegeneration of the medial temporal lobe structures,
Table 1. Demographic and Exposure Characteristics of 177 American Football Players Diagnosed With CTE,Stratified by Neuropathological Severitya
Characteristics
No. (%) of Brain Donorsb
Mild CTE(n = 44)
Severe CTE(n = 133)
Total(n = 177)
Men 44 (100) 133 (100) 177 (100)
Race
White 35 (80) 105 (79) 140 (79)
Black 8 (18) 27 (20) 35 (19)
Pacific Islander 0 1 (1) 1 (1)
Asian 0 0 0
Other 0 0 0
Unknown 1 (2) 0 1 (1)
Age at death, median (IQR), y 44 (29-64) 71 (64-79) 67 (52-77)
Cause of death
Neurodegenerativec 7 (16) 62 (47) 69 (39)
Cardiovascular disease 5 (11) 29 (22) 34 (19)
Suicide 12 (27) 6 (5) 18 (10)
Cancer 2 (5) 10 (8) 12 (7)
Motor neuron disease 4 (9) 7 (5) 11 (6)
Unintentional overdose 3 (7) 4 (3) 7 (4)
Injury 2 (5) 3 (2) 5 (3)
Other 9 (21) 12 (9) 21 (12)
Concussion count, median (IQR)d
Definition provided (n = 99) 90 (22-150) 50.5 (12-163) 70 (12-150)
No definition provided (n = 61) 2.5 (0-5) 8 (1-19) 5 (1-13)
Age at first exposure to football, median (IQR), y 10 (8-14) 13 (10-14) 12 (10-14)
Duration of play, mean (SD), y 13 (4.2) 15.8 (5.3) 15.1 (5.2)
Highest level of play
Youth 0 0 0
High school 3 (7) 0 3 (2)
College 21 (48) 27 (20) 48 (27)
Semiprofessional 4 (9) 5 (4) 9 (5)
Canadian Football League 1 (2) 6 (5) 7 (4)
National Football League 15 (34) 95 (71) 110 (62)
Primary position at highest level of play
Offensive lineman 8 (18) 29 (22) 37 (21)
Defensive lineman 8 (18) 27 (20) 35 (20)
Running back 4 (9) 27 (20) 31 (18)
Linebacker 12 (27) 14 (11) 26 (15)
Defensive back 4 (9) 18 (14) 22 (12)
Quarterback 2 (5) 11 (8) 13 (7)
Tight end 1 (2) 6 (5) 7 (4)
Wide receiver 3 (7) 1 (1) 4 (2)
Kicker or punter 2 (5) 0 2 (1)
Other special teams 0 0 0
Military veteran 5 (11) 40 (30) 45 (25)
Abbreviations: CTE, chronictraumatic encephalopathy; IQR,interquartile range.a Mild CTE (CTE neuropathological
stages I and II) is characterized bysparse to frequent perivascular CTElesions at the sulcal depths of thecerebral cortex. Severe CTE (CTEneuropathological stages III and IV)consists of multiple CTE lesions inthe cerebral cortex and moderate tosevere neurofibrillary degenerationof medial temporal lobe,diencephalon, and brain stem.
b Data are expressed as No. (%)unless otherwise indicated.
c Includes dementia-relatedand parkinsonian-related causesof death.
d Median estimates of the numberof concussions reportedper participant. Beginningin 2014, informants were reada formal definition of concussionprior to being asked aboutconcussion history.
Evaluation of Chronic Traumatic Encephalopathy in Football Players Original Investigation Research
jama.com (Reprinted) JAMA July 25, 2017 Volume 318, Number 4 363
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a UCSF LIBRARY User on 01/29/2018
% with severe CTE by level of play:• Highschool 0%• College 56%• Semi-pro 56%• CFL 86%• NFL 86%
% with any CTE by level of play:• Highschool 21%• College 91%• Semi-pro 64%• CFL 88%• NFL 99%
[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES AND HANDOUTS]
3/8/186
21
mood symptoms, and 16 (14.4%; median age at death, 65.5years [IQR, 39-78]) initially presented with both cognitivesymptoms and behavior or mood symptoms. Forty (85%) ofthose initially presenting with only cognitive symptomswere reported to have behavior or mood symptoms at thetime of death and 43 (90%) of those initially presenting withonly behavior or mood symptoms were reported to havecognitive symptoms at the time of death. Dementia waspresent at the time of death in 36 (77%) of those initiallypresenting with cognitive symptoms, 33 (69%) of those ini-tially presenting with behavior or mood symptoms, and 11(69%) of those initially presenting with both cognitive andbehavior or mood symptoms.
The most common primary cause of death was neuro-degenerative for all 3 groups (cognitive, 26 [55%]; behavioror mood, 16 [33%]; both cognitive and behavior or mood, 6[38%]). Substance use disorders, suicidality, and family his-tory of psychiatric illness were common among those whoinitially presented with behavior or mood symptoms, occur-ring in 32 (67%), 22 (47%), and 23 (49%) cases, respectively.
DiscussionIn a convenience sample of 202 deceased former players ofAmerican football who were part of a brain donation pro-gram, a high proportion were diagnosed neuropathologi-cally with CTE. The severity of CTE pathology was distrib-uted across the highest level of play, with all former highschool players having mild pathology and the majority offormer college, semiprofessional, and professional playershaving severe pathology. Behavior, mood, and cognitivesymptoms were common among those with mild and severeCTE pathology and signs of dementia were common amongthose with severe CTE pathology.
Nearly all of the former NFL players in this study hadCTE pathology, and this pathology was frequently severe.These findings suggest that CTE may be related to prior par-
ticipation in football and that a high level of play may berelated to substantial disease burden. Several other football-related factors may influence CTE risk and disease severity,including but not limited to age at first exposure to football,duration of play, player position, cumulative hits, and linearand rotational acceleration of hits. Recent work in living for-mer football players has shown that age at first exposuremay be related to impaired cognitive performance29 andaltered corpus callosum white matter30 and that cumulativehits may be related to impairment on self-report and objec-tive measures of cognition, mood, and behavior,31 althoughit is unclear if any of these outcomes are related to CTEpathology. Furthermore, it is unclear if symptomatic hits(concussions) are more important than asymptomatic hitsresulting in subconcussive injury. As with other neurode-generative diseases, age may be related to risk and patho-logical severity in CTE. It will be important for future stud-ies to resolve how different measures of exposure tofootball and age influence the outcome.
In cases with severe CTE pathology, accumulations ofamyloid-β, α-synuclein, and TDP-43 were common. Thesefindings are consistent with previous studies that show dep-osition of multiple neurodegenerative proteins after expo-sure to TBI32 and with work showing that neuritic amyloid-βplaques are associated with increased CTE neuropathologi-cal stage.33 Diagnoses of comorbid neurodegenerativediseases, including AD, Lewy body disease, motor neurondisease, and frontotemporal lobar degeneration, were alsocommon in cases with severe CTE pathology. Overall, 19%of participants with CTE had comorbid Lewy body disease,which aligns with a recent observation by Crane et al34
regarding the increased prevalence of Lewy body pathologyafter single TBI. Chronic traumatic encephalopathy was notassessed in the analysis by Crane et al; to investigate thepossibility of CTE after single TBI would require moreextensive sampling of the depths of the cortical sulci withptau immunostaining, as silver stains typically do notdetect CTE pathology.
Figure 3. Phosphorylated Tau Pathology for Each Brain Region by CTE Neuropathological Stage
Frontal
1
2
3
4
Total
CTEStage Temporal Parietal Septal Insula Entorhinal
Brain Region
Amygdala Hippocampus Thalamus SI SN LC Cerebellum
1.1
1.6
2.2
2.8
2.2
0.6
1.4
2.1
2.7
2.1
0.2
1.3
1.6
2.6
1.8
0.4
1.2
2.0
2.7
2.0
0.3
1.1
2.1
2.8
2.1
0.6
1.4
2.6
2.8
2.3
0.4
1.1
2.3
2.8
2.1
0.1
0.7
2.1
2.4
1.8
0.3
0.9
1.4
2.2
1.5
0.5
1.3
2.3
2.7
2.1
0.6
1.0
1.8
2.5
1.8
0.9
2.0
2.5
2.5
2.3
0
0.2
0.3
0.6
0.3
2 310
Mean phosphorylated tau pathology
11
33
76
57
177
No. ofDonors
CTE indicates chronic traumatic encephalopathy; NFT: neurofibrillary tangle,SI: substantia innominata, SN: substantia nigra; LC: locus coeruleus. Cerebellumindicates dentate nucleus of the cerebellum. In each region, 0 = no NFTs(yellow); 1 = 1 NFT per 20× field (orange); 2 = 2 to 3 NFTs per 20× field (amber);
and 3 = !4 NFTs per 20× field (red). The color scale is based on the distributionof all values, not by each individual stage. Values represent means ofphosphorylated tau pathology among participants in each stage.
Research Original Investigation Evaluation of Chronic Traumatic Encephalopathy in Football Players
366 JAMA July 25, 2017 Volume 318, Number 4 (Reprinted) jama.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a UCSF LIBRARY User on 01/29/2018
Anatomical Distribution of p-tau Pathology Stratified by CTE Stage
Behavioral,mood,and
cognitivesym
ptoms
were
com-
mon
among
participantswith
eithermild
orsevereCTE
pa-thology.In
participantswith
severeCTEpathology,therew
asm
arkedptau
pathologyin
brainregionsthathave
beenasso-
ciatedw
ithsym
ptomsfrequently
reported:impulsivity,de-
pressivesymptom
s,apathy,anxiety,andexplosivity(prefron-
talcortex,amygdala,locus
coeruleus);episodicm
emory
symptom
s(hippocampusand
entorhinalandperirhinalcor-
tices);andattention
andexecutive
functionsym
ptoms
(prefrontalcortex).Participantswith
mild
CTEpathology
of-ten
hadthese
symptom
sdespite
havingrelatively
circum-
scribedcorticalpathology
andabsence
ofptaupathology
inthe
hippocampus,entorhinalcortex,oram
ygdala.Thismay
suggestthatotherpathologiesnotcapturedbythepathologi-
caldataset,such
asneuroinflam
mation,axonalinjury,or
astrocytosis,orpathologiesinneuroanatom
icalregionsnotevaluated
contributeto
theseclinicalsym
ptoms.M
icroglialneuroinflam
mation
appearstoprecede
tauaccum
ulationin
CTE, 35suggestingitm
ayplay
arolein
earlysym
ptoms.
Informantsreported
that43%ofparticipantshad
behav-iororm
oodsym
ptomsastheirinitialpresentation.M
anyof
theseparticipants
hada
substanceuse
disorder,demon-
stratedsuicidality,orhad
afam
ilyhistory
ofpsychiatricill-
ness.Behaviorormood
symptom
smay
betheinitialpresen-tation
forasubsetofindividualswith
CTE,oralternatively,CTEptau
pathologymaylow
erthethresholdforpsychiatricm
ani-festationsin
susceptibleindividuals.These
clinicalobserva-tionsconfirm
andexpand
onpreviousreportsof2
primary
clinicalpresentationsofCTE. 9
Thereissubstantialevidence
thatCTEisa
progressive,neurodegenerative
disease.Inthis
study,107participants
(96%)had
aprogressive
clinicalcoursebased
oninform
antreport.In
addition,pathologicalseverityofCTE
wascorre-
latedw
ithage
atdeath(Table
3).How
ever,apostm
ortemstudy
evaluatesbrainpathology
atonly1tim
epointand
isby
definitioncross-sectional.In
addition,theparticipants
were
notobservedlongitudinally
duringlife.Although
asso-ciationsw
ithage
incross-sectionalsam
plescanresultfrom
age-relatedprogression
within
individuals,theycan
alsoarise
frombirth
cohorteffects,differentialsurvival,orage-related
differencesinhow
individualswere
selectedinto
thestudy.Population-based
prospectivestudies
areneeded
toaddressthe
issueofprogression
ofCTEpathology
andage
atsym
ptomonset.
ThestrengthsofthisstudyarethatthisisthelargestCTE
caseserieseverdescribedto
ourknowledge,m
orethandou-
blingthesizeofthe2013report, 6andthatallparticipantsw
ereexposed
toarelatively
similartypeofrepetitivehead
trauma
whileplayingthesam
esport.Inaddition,thecom
prehensiveneuropathologicalevaluation
andretrospective
clinicaldatacollection
wereindependentlyperform
edw
hileblindedtothe
findingsoftheotherinvestigators.
Thisstudyhad
severallimitations.First,a
majorlim
ita-tion
isascertainm
entbiasassociated
with
participationin
thisbrain
donationprogram
.Althoughthe
criteriaforpar-
ticipationw
erebased
onexposure
torepetitive
headtraum
aratherthan
onclinicalsignsofbrain
trauma,public
aware-
nessofapossible
linkbetw
eenrepetitive
headtraum
aand
Table 2. Neuropathological Findings in 177 American Football Players, Stratified by Severity of Phosphorylated Tau Pathology (CTE Stage)a
CTEStage
No. ofBrain Donors
Age at Death,Median (IQR), y
Neuropathological Features, No. (%) Other Neuropathological Diagnoses, No. (%) Pure CTE,No. (%)Aß DP NP AA TDP-43 αs AD LBD FTLD TDP-43 FTLD-Tau MND
1 11 36 (25-56) 2 (18) 2 (18) 1 (9) 1 (9) 2 (18) 1 (9) 0 1 (9) 1 (9) 0 0 8 (73)
2 33 49 (29-65) 8 (24) 8 (24) 5 (15) 7 (21) 10 (30) 3 (9) 1 (3) 2 (6) 1 (3) 1 (3) 4 (12) 21 (64)
3 76 67 (57-78) 45 (59) 41 (54) 25 (33) 29 (38) 26 (34) 16 (21) 4 (5) 15 (20) 1 (1) 3 (4) 6 (8) 42 (55)
4 57 76 (69-82) 52 (91) 52 (91) 42 (74) 32 (56) 47 (83) 23 (40) 18 (32) 16 (28) 5 (9) 2 (4) 1 (2) 27 (47)
Total 177 67 (53-78) 107 (61) 103 (58) 73 (41) 69 (39) 85 (48) 43 (24) 23 (13) 34 (19) 8 (5) 6 (3) 11 (6) 98 (55)
Abbreviations: AA, amyloid angiopathy; Aß, amyloid-β; AD, Alzheimer disease; αs, α-synuclein immunopositiveLewy bodies; CTE, chronic traumatic encephalopathy diagnosed neuropathologically; DP, diffuse Aß plaques;FTLD-tau, frontotemporal lobar degeneration-tau; FTLD TDP-43, frontotemporal lobar degeneration TDP-43;IQR, interquartile range; LBD, Lewy body disease; MND, motor neuron disease; NP, neuritic Aß plaques;TDP-43, TDP-43 immunopositive neurites or inclusions.a Pure CTE is defined as CTE with no neuropathological evidence of other comorbid neurodegenerative disease.
Stage I CTE is characterized by 1 or 2 perivascular CTE lesions at the depths of the cerebral sulci in the cerebralcortex. In stage II, 3 or more CTE lesions are found in multiple cortical regions. In stage III CTE, many CTE lesions,superficial cortical neurofibrillary tangles, and diffuse neurofibrillary degeneration of the entorhinal andperirhinal cortices, amygdala, and hippocampus are found. In stage IV CTE, CTE lesions and neurofibrillarytangles are densely distributed throughout the cerebral cortex, diencephalon, and brain stem with neuronal loss,gliosis, and astrocytic phosphorylated tau pathology.
EvaluationofChronicTraum
aticEncephalopathyinFootballPlayers
OriginalInvestigation
Research
jama.com
(Reprinted)JAM
AJuly25,2017
Volume
318,Number4
367
©2017
Am
ericanM
edicalAssociation.A
llrightsreserved.
Dow
nloaded From: by a U
CSF LIBR
AR
Y U
ser on 01/29/2018
22
Behavioral,mood,and
cognitivesym
ptoms
were
com-
mon
among
participantswith
eithermild
orsevereCTE
pa-thology.In
participantswith
severeCTEpathology,therew
asm
arkedptau
pathologyin
brainregionsthathave
beenasso-
ciatedw
ithsym
ptomsfrequently
reported:impulsivity,de-
pressivesymptom
s,apathy,anxiety,andexplosivity(prefron-
talcortex,amygdala,locus
coeruleus);episodicm
emory
symptom
s(hippocampusand
entorhinalandperirhinalcor-
tices);andattention
andexecutive
functionsym
ptoms
(prefrontalcortex).Participantswith
mild
CTEpathology
of-ten
hadthese
symptom
sdespite
havingrelatively
circum-
scribedcorticalpathology
andabsence
ofptaupathology
inthe
hippocampus,entorhinalcortex,oram
ygdala.Thismay
suggestthatotherpathologiesnotcapturedbythepathologi-
caldataset,such
asneuroinflam
mation,axonalinjury,or
astrocytosis,orpathologiesinneuroanatom
icalregionsnotevaluated
contributeto
theseclinicalsym
ptoms.M
icroglialneuroinflam
mation
appearstoprecede
tauaccum
ulationin
CTE, 35suggestingitm
ayplay
arolein
earlysym
ptoms.
Informantsreported
that43%ofparticipantshad
behav-iororm
oodsym
ptomsastheirinitialpresentation.M
anyof
theseparticipants
hada
substanceuse
disorder,demon-
stratedsuicidality,orhad
afam
ilyhistory
ofpsychiatricill-
ness.Behaviorormood
symptom
smay
betheinitialpresen-tation
forasubsetofindividualswith
CTE,oralternatively,CTEptau
pathologymaylow
erthethresholdforpsychiatricm
ani-festationsin
susceptibleindividuals.These
clinicalobserva-tionsconfirm
andexpand
onpreviousreportsof2
primary
clinicalpresentationsofCTE. 9
Thereissubstantialevidence
thatCTEisa
progressive,neurodegenerative
disease.Inthis
study,107participants
(96%)had
aprogressive
clinicalcoursebased
oninform
antreport.In
addition,pathologicalseverityofCTE
wascorre-
latedw
ithage
atdeath(Table
3).How
ever,apostm
ortemstudy
evaluatesbrainpathology
atonly1tim
epointand
isby
definitioncross-sectional.In
addition,theparticipants
were
notobservedlongitudinally
duringlife.Although
asso-ciationsw
ithage
incross-sectionalsam
plescanresultfrom
age-relatedprogression
within
individuals,theycan
alsoarise
frombirth
cohorteffects,differentialsurvival,orage-related
differencesinhow
individualswere
selectedinto
thestudy.Population-based
prospectivestudies
areneeded
toaddressthe
issueofprogression
ofCTEpathology
andage
atsym
ptomonset.
ThestrengthsofthisstudyarethatthisisthelargestCTE
caseserieseverdescribedto
ourknowledge,m
orethandou-
blingthesizeofthe2013report, 6andthatallparticipantsw
ereexposed
toarelatively
similartypeofrepetitivehead
trauma
whileplayingthesam
esport.Inaddition,thecom
prehensiveneuropathologicalevaluation
andretrospective
clinicaldatacollection
wereindependentlyperform
edw
hileblindedtothe
findingsoftheotherinvestigators.
Thisstudyhad
severallimitations.First,a
majorlim
ita-tion
isascertainm
entbiasassociated
with
participationin
thisbrain
donationprogram
.Althoughthe
criteriaforpar-
ticipationw
erebased
onexposure
torepetitive
headtraum
aratherthan
onclinicalsignsofbrain
trauma,public
aware-
nessofapossible
linkbetw
eenrepetitive
headtraum
aand
Table 2. Neuropathological Findings in 177 American Football Players, Stratified by Severity of Phosphorylated Tau Pathology (CTE Stage)a
CTEStage
No. ofBrain Donors
Age at Death,Median (IQR), y
Neuropathological Features, No. (%) Other Neuropathological Diagnoses, No. (%) Pure CTE,No. (%)Aß DP NP AA TDP-43 αs AD LBD FTLD TDP-43 FTLD-Tau MND
1 11 36 (25-56) 2 (18) 2 (18) 1 (9) 1 (9) 2 (18) 1 (9) 0 1 (9) 1 (9) 0 0 8 (73)
2 33 49 (29-65) 8 (24) 8 (24) 5 (15) 7 (21) 10 (30) 3 (9) 1 (3) 2 (6) 1 (3) 1 (3) 4 (12) 21 (64)
3 76 67 (57-78) 45 (59) 41 (54) 25 (33) 29 (38) 26 (34) 16 (21) 4 (5) 15 (20) 1 (1) 3 (4) 6 (8) 42 (55)
4 57 76 (69-82) 52 (91) 52 (91) 42 (74) 32 (56) 47 (83) 23 (40) 18 (32) 16 (28) 5 (9) 2 (4) 1 (2) 27 (47)
Total 177 67 (53-78) 107 (61) 103 (58) 73 (41) 69 (39) 85 (48) 43 (24) 23 (13) 34 (19) 8 (5) 6 (3) 11 (6) 98 (55)
Abbreviations: AA, amyloid angiopathy; Aß, amyloid-β; AD, Alzheimer disease; αs, α-synuclein immunopositiveLewy bodies; CTE, chronic traumatic encephalopathy diagnosed neuropathologically; DP, diffuse Aß plaques;FTLD-tau, frontotemporal lobar degeneration-tau; FTLD TDP-43, frontotemporal lobar degeneration TDP-43;IQR, interquartile range; LBD, Lewy body disease; MND, motor neuron disease; NP, neuritic Aß plaques;TDP-43, TDP-43 immunopositive neurites or inclusions.a Pure CTE is defined as CTE with no neuropathological evidence of other comorbid neurodegenerative disease.
Stage I CTE is characterized by 1 or 2 perivascular CTE lesions at the depths of the cerebral sulci in the cerebralcortex. In stage II, 3 or more CTE lesions are found in multiple cortical regions. In stage III CTE, many CTE lesions,superficial cortical neurofibrillary tangles, and diffuse neurofibrillary degeneration of the entorhinal andperirhinal cortices, amygdala, and hippocampus are found. In stage IV CTE, CTE lesions and neurofibrillarytangles are densely distributed throughout the cerebral cortex, diencephalon, and brain stem with neuronal loss,gliosis, and astrocytic phosphorylated tau pathology.
EvaluationofChronicTraum
aticEncephalopathyinFootballPlayers
OriginalInvestigation
Research
jama.com
(Reprinted)JAM
AJuly25,2017
Volume
318,Number4
367
©2017
Am
ericanM
edicalAssociation.A
llrightsreserved.
Dow
nloaded From: by a U
CSF LIBR
AR
Y U
ser on 01/29/2018
Other Neuropathological Diagnoses Stratified by CTE Stage
§ AD = Alzheimer disease§ LBD= Lewy body dementia (i.e. PD, DLB)§ FTLD = frontotemporal lobar dementia (pathologic subtypes classified by
inclusion composition)§ MND= motor neuron disease
23
CTE may have motivated players and their families withsymptoms and signs of brain injury to participate in thisresearch. Therefore, caution must be used in interpretingthe high frequency of CTE in this sample, and estimates ofprevalence cannot be concluded or implied from this
sample. Second, the VA-BU-CLF brain bank is not represen-tative of the overall population of former players of Ameri-can football; most players of American football have playedonly on youth or high school teams, but the majority of thebrain bank donors in this study played at the college or
Table 3. Clinical Features Reported in 111 American Football Players Diagnosed as Having CTE,Stratified by Neuropathological Severitya
Clinical Features
No. (%) of Brain Donors
Mild CTE Severe CTE TotalProgressive course 23 (85) 84 (100) 107 (96)
Cognitive symptomsb 23 (85) 80 (95) 103 (93)
Memory 19 (73) 76 (92) 95 (86)
Executive function 19 (73) 67 (81) 86 (79)
Attention 18 (69) 67 (81) 85 (78)
Language 10 (39) 54 (66) 64 (59)
Visuospatial 7 (27) 44 (54) 51 (47)
Fluctuating cognition 2 (8) 17 (21) 19 (18)
Dementiab 9 (33) 71 (85) 80 (72)
Behavioral or mood symptomsb 26 (96) 75 (89) 101 (91)
Impulsivity 23 (89) 65 (80) 88 (82)
Depressive symptoms 18 (67) 46 (56) 64 (59)
Explosivity 18 (67) 38 (45) 56 (51)
Apathy 13 (50) 43 (52) 56 (51)
Anxiety 14 (52) 41 (50) 55 (51)
Hopelessness 18 (69) 36 (46) 54 (52)
Verbal violence 17 (63) 28 (34) 45 (41)
Social inappropriateness 13 (48) 26 (32) 39 (36)
Physical violence 14 (52) 23 (28) 37 (34)
Paranoia 11 (41) 26 (31) 37 (34)
Suicidality (ideation, attempts, or completions) 15 (56) 21 (25) 36 (33)
Visual hallucinations 6 (23) 22 (27) 28 (26)
Mania 6 (22) 3 (4) 9 (8)
Posttraumatic stress disorder(exposure and symptoms consistent with)
3 (11) 9 (11) 12 (11)
Substance use disorder 18 (67) 41 (49) 59 (53)
Alcohol 13 (50) 31 (37) 44 (41)
Anabolic steroid 0 4 (5) 4 (4)
Other 14 (54) 23 (28) 37 (34)
Motor symptomsb 13 (48) 63 (75) 76 (68)
Gait instability 7 (26) 55 (66) 62 (56)
Slowness 5 (19) 42 (50) 47 (42)
Coordination difficulties 7 (26) 38 (45) 45 (41)
Falls 4 (15) 39 (46) 43 (39)
Tremor 5 (19) 33 (39) 38 (34)
Dysphagia 3 (11) 14 (18) 17 (16)
Dysarthria 5 (19) 10 (13) 15 (14)
Headache 8 (30) 11 (14) 19 (18)
Diagnoses in life
Motor neuron disease 1 (4) 3 (4) 4 (4)
Parkinson disease 1 (4) 5 (6) 6 (6)
Alzheimer disease 1 (4) 21 (25) 22 (20)
Obstructive sleep apnea (diagnosis or symptoms) 7 (27) 36 (46) 43 (41)
Rapid eye movement sleep behavior disorder(diagnosis or symptoms)
7 (27) 23 (29) 30 (29)
Abbreviation: CTE, chronic traumaticencephalopathy.a There were 111 participants with
standardized informant reports,including 27 participants with mildCTE and 84 participants with severeCTE. Sample sizes differed acrossclinical features because featuresmarked as unknown by the clinicianwere excluded. For participants withmild CTE, sample sizes ranged from25 to 27 and for participants withsevere CTE, sample sizes rangedfrom 78 to 84. Mild CTE (CTEneuropathological stages I and II) ischaracterized by sparse to frequentperivascular CTE lesions at the sulcaldepths of the cerebral cortex.Severe CTE (CTE neuropathologicalstages III and IV) consists of multipleCTE lesions in the cerebral cortexand moderate to severeneurofibrillary degeneration ofmedial temporal lobe,diencephalon, and brain stem.
b Symptoms were present in the lastyear of life.
Research Original Investigation Evaluation of Chronic Traumatic Encephalopathy in Football Players
368 JAMA July 25, 2017 Volume 318, Number 4 (Reprinted) jama.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a UCSF LIBRARY User on 01/29/2018
CTE may have motivated players and their families withsymptoms and signs of brain injury to participate in thisresearch. Therefore, caution must be used in interpretingthe high frequency of CTE in this sample, and estimates ofprevalence cannot be concluded or implied from this
sample. Second, the VA-BU-CLF brain bank is not represen-tative of the overall population of former players of Ameri-can football; most players of American football have playedonly on youth or high school teams, but the majority of thebrain bank donors in this study played at the college or
Table 3. Clinical Features Reported in 111 American Football Players Diagnosed as Having CTE,Stratified by Neuropathological Severitya
Clinical Features
No. (%) of Brain Donors
Mild CTE Severe CTE TotalProgressive course 23 (85) 84 (100) 107 (96)
Cognitive symptomsb 23 (85) 80 (95) 103 (93)
Memory 19 (73) 76 (92) 95 (86)
Executive function 19 (73) 67 (81) 86 (79)
Attention 18 (69) 67 (81) 85 (78)
Language 10 (39) 54 (66) 64 (59)
Visuospatial 7 (27) 44 (54) 51 (47)
Fluctuating cognition 2 (8) 17 (21) 19 (18)
Dementiab 9 (33) 71 (85) 80 (72)
Behavioral or mood symptomsb 26 (96) 75 (89) 101 (91)
Impulsivity 23 (89) 65 (80) 88 (82)
Depressive symptoms 18 (67) 46 (56) 64 (59)
Explosivity 18 (67) 38 (45) 56 (51)
Apathy 13 (50) 43 (52) 56 (51)
Anxiety 14 (52) 41 (50) 55 (51)
Hopelessness 18 (69) 36 (46) 54 (52)
Verbal violence 17 (63) 28 (34) 45 (41)
Social inappropriateness 13 (48) 26 (32) 39 (36)
Physical violence 14 (52) 23 (28) 37 (34)
Paranoia 11 (41) 26 (31) 37 (34)
Suicidality (ideation, attempts, or completions) 15 (56) 21 (25) 36 (33)
Visual hallucinations 6 (23) 22 (27) 28 (26)
Mania 6 (22) 3 (4) 9 (8)
Posttraumatic stress disorder(exposure and symptoms consistent with)
3 (11) 9 (11) 12 (11)
Substance use disorder 18 (67) 41 (49) 59 (53)
Alcohol 13 (50) 31 (37) 44 (41)
Anabolic steroid 0 4 (5) 4 (4)
Other 14 (54) 23 (28) 37 (34)
Motor symptomsb 13 (48) 63 (75) 76 (68)
Gait instability 7 (26) 55 (66) 62 (56)
Slowness 5 (19) 42 (50) 47 (42)
Coordination difficulties 7 (26) 38 (45) 45 (41)
Falls 4 (15) 39 (46) 43 (39)
Tremor 5 (19) 33 (39) 38 (34)
Dysphagia 3 (11) 14 (18) 17 (16)
Dysarthria 5 (19) 10 (13) 15 (14)
Headache 8 (30) 11 (14) 19 (18)
Diagnoses in life
Motor neuron disease 1 (4) 3 (4) 4 (4)
Parkinson disease 1 (4) 5 (6) 6 (6)
Alzheimer disease 1 (4) 21 (25) 22 (20)
Obstructive sleep apnea (diagnosis or symptoms) 7 (27) 36 (46) 43 (41)
Rapid eye movement sleep behavior disorder(diagnosis or symptoms)
7 (27) 23 (29) 30 (29)
Abbreviation: CTE, chronic traumaticencephalopathy.a There were 111 participants with
standardized informant reports,including 27 participants with mildCTE and 84 participants with severeCTE. Sample sizes differed acrossclinical features because featuresmarked as unknown by the clinicianwere excluded. For participants withmild CTE, sample sizes ranged from25 to 27 and for participants withsevere CTE, sample sizes rangedfrom 78 to 84. Mild CTE (CTEneuropathological stages I and II) ischaracterized by sparse to frequentperivascular CTE lesions at the sulcaldepths of the cerebral cortex.Severe CTE (CTE neuropathologicalstages III and IV) consists of multipleCTE lesions in the cerebral cortexand moderate to severeneurofibrillary degeneration ofmedial temporal lobe,diencephalon, and brain stem.
b Symptoms were present in the lastyear of life.
Research Original Investigation Evaluation of Chronic Traumatic Encephalopathy in Football Players
368 JAMA July 25, 2017 Volume 318, Number 4 (Reprinted) jama.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a UCSF LIBRARY User on 01/29/2018
Clinical Features Stratified by CTE Severity
CTE may have motivated players and their families withsymptoms and signs of brain injury to participate in thisresearch. Therefore, caution must be used in interpretingthe high frequency of CTE in this sample, and estimates ofprevalence cannot be concluded or implied from this
sample. Second, the VA-BU-CLF brain bank is not represen-tative of the overall population of former players of Ameri-can football; most players of American football have playedonly on youth or high school teams, but the majority of thebrain bank donors in this study played at the college or
Table 3. Clinical Features Reported in 111 American Football Players Diagnosed as Having CTE,Stratified by Neuropathological Severitya
Clinical Features
No. (%) of Brain Donors
Mild CTE Severe CTE TotalProgressive course 23 (85) 84 (100) 107 (96)
Cognitive symptomsb 23 (85) 80 (95) 103 (93)
Memory 19 (73) 76 (92) 95 (86)
Executive function 19 (73) 67 (81) 86 (79)
Attention 18 (69) 67 (81) 85 (78)
Language 10 (39) 54 (66) 64 (59)
Visuospatial 7 (27) 44 (54) 51 (47)
Fluctuating cognition 2 (8) 17 (21) 19 (18)
Dementiab 9 (33) 71 (85) 80 (72)
Behavioral or mood symptomsb 26 (96) 75 (89) 101 (91)
Impulsivity 23 (89) 65 (80) 88 (82)
Depressive symptoms 18 (67) 46 (56) 64 (59)
Explosivity 18 (67) 38 (45) 56 (51)
Apathy 13 (50) 43 (52) 56 (51)
Anxiety 14 (52) 41 (50) 55 (51)
Hopelessness 18 (69) 36 (46) 54 (52)
Verbal violence 17 (63) 28 (34) 45 (41)
Social inappropriateness 13 (48) 26 (32) 39 (36)
Physical violence 14 (52) 23 (28) 37 (34)
Paranoia 11 (41) 26 (31) 37 (34)
Suicidality (ideation, attempts, or completions) 15 (56) 21 (25) 36 (33)
Visual hallucinations 6 (23) 22 (27) 28 (26)
Mania 6 (22) 3 (4) 9 (8)
Posttraumatic stress disorder(exposure and symptoms consistent with)
3 (11) 9 (11) 12 (11)
Substance use disorder 18 (67) 41 (49) 59 (53)
Alcohol 13 (50) 31 (37) 44 (41)
Anabolic steroid 0 4 (5) 4 (4)
Other 14 (54) 23 (28) 37 (34)
Motor symptomsb 13 (48) 63 (75) 76 (68)
Gait instability 7 (26) 55 (66) 62 (56)
Slowness 5 (19) 42 (50) 47 (42)
Coordination difficulties 7 (26) 38 (45) 45 (41)
Falls 4 (15) 39 (46) 43 (39)
Tremor 5 (19) 33 (39) 38 (34)
Dysphagia 3 (11) 14 (18) 17 (16)
Dysarthria 5 (19) 10 (13) 15 (14)
Headache 8 (30) 11 (14) 19 (18)
Diagnoses in life
Motor neuron disease 1 (4) 3 (4) 4 (4)
Parkinson disease 1 (4) 5 (6) 6 (6)
Alzheimer disease 1 (4) 21 (25) 22 (20)
Obstructive sleep apnea (diagnosis or symptoms) 7 (27) 36 (46) 43 (41)
Rapid eye movement sleep behavior disorder(diagnosis or symptoms)
7 (27) 23 (29) 30 (29)
Abbreviation: CTE, chronic traumaticencephalopathy.a There were 111 participants with
standardized informant reports,including 27 participants with mildCTE and 84 participants with severeCTE. Sample sizes differed acrossclinical features because featuresmarked as unknown by the clinicianwere excluded. For participants withmild CTE, sample sizes ranged from25 to 27 and for participants withsevere CTE, sample sizes rangedfrom 78 to 84. Mild CTE (CTEneuropathological stages I and II) ischaracterized by sparse to frequentperivascular CTE lesions at the sulcaldepths of the cerebral cortex.Severe CTE (CTE neuropathologicalstages III and IV) consists of multipleCTE lesions in the cerebral cortexand moderate to severeneurofibrillary degeneration ofmedial temporal lobe,diencephalon, and brain stem.
b Symptoms were present in the lastyear of life.
Research Original Investigation Evaluation of Chronic Traumatic Encephalopathy in Football Players
368 JAMA July 25, 2017 Volume 318, Number 4 (Reprinted) jama.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a UCSF LIBRARY User on 01/29/2018
Conclusions
24
• Football associations
‒ Nearly all football players beyond highschool had CTE pathology
‒ CTE severity low in highschool footballers, intermediate in college, and high in professionals
‒ Possible gradient by player position (running backs, defensive backs > linemen)
‒ Unclear if symptomatic hits (concussions) more relevant
‒ Unclear if age at starting play relevant
• Pathologic associations
‒ Co-pathology common in severe CTE (b-amyloid, a-synuclein, TDP-43)
‒ Co-morbidity common in severe CTE (AD, PD, FTLD)
• Clinicopathologic associations
‒ Behavioral, mood, cognitive symptoms very common in mild or severe CTE
‒ Dementia and motor symptoms much more common in severe CTE
• Limitations:
‒ Cross sectional: unable to assess progression, but substantial evidence CTE is progressive
‒ *Self-referred sample: likely not representative of all football players

[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES AND HANDOUTS]
3/8/187
25
Environmental Exposures to Lead, Mercury, and Cadmium and Hearing Loss inAdults and Adolescents: KNHANES 2010–2012Yoon-Hyeong Choi1,2 and Sung Kyun Park3,41Department of Preventive Medicine, Gachon University College of Medicine, Incheon, Republic of Korea2Gachon Advanced Institute for Health Sciences and Technology, Incheon, Republic of Korea3Department of Epidemiology, University of Michigan School of Public Health, Ann Arbor, Michigan, USA4Department of Environmental Health Sciences, University of Michigan School of Public Health, Ann Arbor, Michigan, USA
BACKGROUND: The prevalence of hearing loss increases rapidly with aging. Hearing loss is common in all age groups, even in young adults and ado-lescents. A growing body of evidence has suggested that heavy metals have ototoxic effects, yet few epidemiological studies have investigated theassociation between heavy metals and hearing loss in a general population that includes adults and adolescents.OBJECTIVES: We examined the association between environmental exposures to lead, mercury, and cadmium and the risk of hearing loss in adultsand adolescents while controlling for potential confounding factors, including noise exposures and clinical factors.METHODS:We analyzed cross-sectional data from 5,187 adults and 853 adolescents in the Korean National Health and Nutrition Examination Survey2010–2012. Pure-tone average (PTA) of hearing thresholds at high frequency (3, 4, and 6 kHz) were computed, and hearing loss was defined as aPTA>25 dB in adults and PTA>15 dB in adolescents.RESULTS: In adults, the highest (vs. lowest) quartiles of blood lead and cadmium were associated with 1.70 (95% CI: 1.25, 2.31) and 1.47 (95% CI:1.05, 2.05) odds ratios for high-frequency hearing loss (p-trend<0:001 and= 0:007), respectively. In adolescents, the highest quartile (vs. lowest) ofblood cadmium had an odds ratio of 3.03 (95% CI: 1.44, 6.40) for high-frequency hearing loss (p-trend= 0:003), but blood lead was not associatedwith hearing loss. No significant association between blood mercury and hearing loss was suggested in either adults or adolescents.CONCLUSIONS: The results of the present study suggest that exposure to environmental lead and cadmium in adults and exposure to environmentalcadmium in adolescents may play a role in the risk of hearing loss. https://doi.org/10.1289/EHP565
IntroductionHearing loss is a commonly experienced chronic disorderthroughout the world. Although hearing loss is common even inyoung adults and school-age children, it is highly prevalent inolder adults (Agrawal et al. 2008; Shargorodsky et al. 2010).Hearing loss can affect communication and can therefore lead toa reduced quality of life and to a loss in economic activity(Agrawal et al. 2008). In adolescents, even slight hearing loss canlead to poor development of communication skills and psycho-logical function and can thus lower educational achievement(Anderson 1992; Northern and Down 2002).
A growing body of evidence from in vitro and animal studieshas demonstrated ototoxic effects of lead, cadmium, and mercury;possible underlying mechanisms of their ototoxic effects includeoxidative stress through depletion of glutathione and protein-bound sulfhydryl groups and related reductions in blood flow andlipid peroxidation in the cochlea, leading to latency in auditorynerve conduction and to an elevation of auditory thresholds (Park2015; Prasher 2009). Although high exposure to heavy metals,particularly to lead, in occupational settings and hearing loss hasbeen studied, little is known about the ototoxic effects of long-term exposure to low-level metals in the general population ofadults and adolescents. With regard to lead, a few studies of low-level exposure and hearing loss have been conducted in U.S.
older men (Park et al. 2010), general adults (Choi et al. 2012a),and adolescents (Shargorodsky et al. 2011); for cadmium, onecross-sectional study in U.S. general adults (Choi et al. 2012a)and one cross-sectional study in U.S. adolescents (Shargorodskyet al. 2011) have been conducted; for mercury, one cross-sectional study was conducted in U.S. general adolescents, but itfailed to observe a significant association (Shargorodsky et al.2011) despite the biological plausibility of mercury affecting theauditory brainstem response (Murata et al. 1999). Although expo-sure to lead, cadmium, and mercury has decreased considerablyin many countries, these heavy metals continue to be widely usedin a variety of consumer products, and environmental exposure tocadmium and mercury is known to be particularly high in AsianPacific people, including Koreans, because of dietary exposurevia consumption of contaminated food: for example, rice, fish,and shellfish (Park and Lee 2013a, 2013b). However, no epide-miologic studies have examined the association between environ-mental exposures to heavy metals and hearing loss in the Koreangeneral population.
In the present study, we examined the association betweenenvironmental heavy metal exposure and risk of hearing loss inadults and adolescents using data from the Korea National Healthand Nutrition Examination Survey (KNHANES) 2010–2012while controlling for potential confounding factors including var-ious noise exposures and clinical risk factors.
MethodsStudy PopulationThe KNHANES, conducted by the Korea Center for DiseaseControl and Prevention (KCDC) since 1998, is an ongoing seriesof cross-sectional surveys designed to determine health and nutri-tion states in a representative Korean population. The surveysconsist of three sections: Health and Behavior Interview, HealthExamination, and Nutrition Survey. KNHANES is a publiclyavailable data set. Because audiometric examination and bloodmetal measurements were conducted in KNHANES 2008–2012and information on detailed noise exposures, an important
Address Correspondence to Yoon-Hyeong Choi, 155 Gaetbeol-ro, Yeonsu-gu, Incheon, Republic of Korea, 21999. Telephone: 82-32-899-6586. E-mail:[email protected] is availableonline (https://doi.org/10.1289/EHP565).The authors declare they have no actual or potential competing financial
interests.Received 2 January 2016; Revised 27 May 2016; Accepted 19 September
2016; Published 8 June 2017.Note to readers with disabilities: EHP strives to ensure that all journal
content is accessible to all readers. However, some figures and SupplementalMaterial published in EHP articles may not conform to 508 standards due tothe complexity of the information being presented. If you need assistanceaccessing journal content, please contact [email protected]. Our staffwill work with you to assess and meet your accessibility needs within 3working days.
Environmental Health Perspectives 067003-1
A Section 508 –conformant HTML version of this articleis available at https://doi.org/10.1289/EHP565.Research
Environ Health Perspect. 2017 Jun 8;125(6):067003. doi: 10.1289/EHP565.
§ Limited data regarding low-level metals exposures
and auditory function
Background: Lead, Mercury, Cadmium & Hearing Loss
26
• Human studies (reviewed by Castellanos, Int. J. Environ. Res. Public Health 2016, 13)
‒ Pb:
§ Some threshold deficits in highly exposed occupational populations, inconsistent
§ Bone-lead dose-related association (Park et al, Hear Res, 2010;269)
§ cause of Beethoven’s deafness? (Stevens et al, Laryngoscope, 2013;123(11))
‒ Hg:
§ hearing deficits/deafness in methylmercury poisonings (Minimata, Japan, Iraq)
§ reduced auditory evoked potentials in children with high levels
§ No association in NHANES (Shargorodsky, Arch. Otolaryngol. Head Neck Surg. 2011, 137)
‒ Cd: hearing loss in highest NHANES quartile, but no dose-response (Shargorodsky)
• Proposed mechanisms
‒ Oxidative stress: depletion of glutathione, cochlear lipid peroxidation
‒ Blood flow alterations
Methods
27
• KHANES: cross-sectional surveys modeled on NHANES: Health & behavior interview; Health exam; Nutrition survey
‒ Representative population sampling since 1998
• Audiometric evaluations, blood metals, noise exposure information obtained 2010-2012
• 5,187 adults, 853 adolescents aged >12 with complete data (80% response rate)
• Audiometry: pure tone thresholds and averages (PTA) in sound-isolated room
‒ Speech-PTA: averages of 0.5, 1, 2, 4 kHz
‒ High-PTA: averages of 3, 4, 6 kHz
‒ Hearing loss defined as PTA >25 dB for adults, >15 dB for adolescents
• Blood metals (venous whole blood):
‒ Graphite furnace absorption spectrometry (lead, cadmium); gold amalgam (mercury)
‒ None of adult and 2 adolescents had levels below limit of detection for any metal
• Analytic covariates: age, sex, education, household income, smoking, BMI, diabetes, hypertension, self-reported noise
‒ occupational noise: “Ever worked in places exposed to loud noise >3 months”
‒ non-occupational: “Ever exposed to loud noise outside of work (e.g., power tools or loud music)”
Associations of blood metals and hearing in adults
28cadmium in whole blood [Agency for Toxic Substances andDisease Registry (ATSDR) 2010a,b]; the Korea OSHA referencefor occupational disease diagnosis are 40 lg=dL for lead and5lg=L for cadmium (KOSHA 2016). In our population, no adultexceeded that limit for lead and very few adults (0.1%) exceededthat limit for cadmium. Our findings, therefore, provide evidencethat low levels of lead and cadmium exposure, even below thelevels in the U.S. CDC guidance and the U.S. and Korea OSHAregulations, can influence hearing loss. Although the major histori-cal sources of lead exposure such as gasoline, paint, and solderhave decreased considerably in many countries, the use of leadcontinues to be widespread, and its accumulation in the humanbody can influence the development of chronic diseases (Hu et al.2006; Muntner et al. 2005). The major sources of cadmium expo-sure are cigarette smoke, ambient air pollution, and dietary intakeof contaminated vegetables, grain, and shellfish (Järup et al.1998), and a major source particularly in Korea includes high con-sumption of rice (Park and Lee 2013b). There is growing evidencethat current environmental levels of lead and cadmium haveadverse effects on various health outcomes including renal func-tion, hypertension, and macular degeneration (Hu et al. 1996;Navas-Acien et al. 2009; Tellez-Plaza et al. 2007; Wu et al. 2014)in addition to our findings for hearing loss; therefore, efforts toreduce environmental exposure to lead and cadmium are neededto improve public health.
The present study did not find evidence that blood mercury isassociated with an increased risk of hearing loss among adults oradolescents. This finding is consistent with the results of previousstudies of U.S. adolescents and Andean adults (Counter et al.1998; Counter et al. 2012; Shargorodsky et al. 2011). An epide-miologic study of general U.S. adolescents failed to observe sig-nificant associations between blood mercury and hearing loss(Shargorodsky et al. 2011), explaining that environmental levelsof exposure to mercury in U.S. adolescents (median levels of0:39–0:63lg=L blood mercury) may not have a detectable power
to observe a significant association with hearing loss. In studiesconducted in Andean gold-mining areas, no significant associa-tions between blood mercury (median level of 6 lg=L) and hear-ing thresholds were found in adults (sample size ranged from 29to 39) (Counter et al. 1998, 2012), yet a statistically significantassociation was found between blood mercury (median levels of7–23lg=L) and hearing thresholds in children. In the generalpopulation, the use of mercury is widespread: metallic and inor-ganic mercury exposure occur mainly through dental amalgamsand occupational exposure (gold mining and industrial settings),and exposure to methylmercury (known to be more common andmore toxic) occurs through dietary intake of fish and shellfish(ATSDR 1999). The present study used blood mercury as an ex-posure biomarker that captures both inorganic mercury and meth-ylmercury (ATSDR 1999). The levels of blood mercury in ourKNHANES population (medians of 3:53 lg=L for adults and1:96 lg=L for adolescents) are relatively higher than those foundin other countries owing to higher consumption of fish and shell-fish (Park and Lee 2013b) and rice (Lee et al. 2006). However,additional adjustment for fish consumption did not change theresults (Table S7). It is unclear whether confounding by fish con-sumption did not exist in this study or fish consumption from theFFQ did not capture actual omega-3 fatty acid consumptionbecause of measurement error. Given mercury’s neurotoxicity,including toward the auditory nervous system (Murata et al.1999), future studies with different types of biomarkers—such asurine (an indicator of elemental mercury) and hair (an indicator ofmethylmercury) along with a good measure of fish consumptionand omega-3 fatty acids—are warranted to confirm our findings.
The strengths and limitations of this study should be consid-ered. This study used data from a large representative sample ofthe Korean general population and was adjusted for importantpotential confounders, including recreational noise (i.e., loudnoise outside of work, earphone music in noisy places), occupa-tional noise, firearm noise, and clinically important risk factors
Table 3. Odds ratios (ORs) [95% confidence intervals (CIs)] of hearing loss (>25 dB) by blood lead, mercury, and cadmium levels in single-pollutant modelsin adults (n=5,187).
VariablesaSpeech-frequency PTAb High-frequency PTAc
No. hearing loss/No. participants ORs (95% CIs) No. hearing loss/No. participants ORs (95% CIs)LeadPer doubling of lead 1,124/5,187 1.15 (0.94, 1.41) 1,124/5,187 1.30 (1.08, 1.57)Lead quartile (mg/dL)Q 1 ð0:327–1:593Þ 170/1,296 1 (Reference) 276/1,296 1 (Reference)Q 2 ð1:594–2:146Þ 204/1,296 0.94 (0.65, 1.35) 420/1,296 1.13 (0.83, 1.53)Q 3 ð2:148–2:822Þ 330/1,298 1.29 (0.92, 1.78) 587/1,298 1.35 (1.00, 1.81)Q 4 ð2:823–26:507Þ 420/1,297 1.25 (0.87, 1.79) 810/1,297 1.70 (1.25, 2.31)
p-Trend 0.066 <0:001MercuryPer doubling of mercury 1,124/5,187 0.96 (0.84, 1.08) 1,124/5,187 0.98 (0.87, 1.09)Mercury quartile (lg=L)Q1 ð0:363–2:378Þ 284/1,296 1 (Reference) 469/1,296 1 (Reference)Q 2 ð2:379–3:528Þ 250/1,297 0.84 (0.61, 1.17) 460/1,297 0.89 (0.68, 1.16)Q 3 ð3:529–5:369Þ 267/1,296 0.79 (0.58, 1.09) 524/1,296 0.83 (0.63, 1.08)Q 4 ð5:370–60:678Þ 323/1,298 0.84 (0.63, 1.12) 640/1,298 0.89 (0.68, 1.17)
p-Trend 0.221 0.382CadmiumPer doubling of cadmium 1,124/5,187 1.18 (1.00, 1.39) 1,124/5,187 1.25 (1.08, 1.44)Cadmium quartile (lg=L)Q1 ð0:068–0:689Þ 140/1,293 1 (Reference) 289/1,293 1 (Reference)Q 2 ð0:690–1:033Þ 255/1,300 1.04 (0.73, 1.49) 489/1,300 1.10 (0.81, 1.49)Q 3 ð1:035–1:470Þ 340/1,299 1.22 (0.86, 1.72) 645/1,299 1.43 (1.06, 1.93)Q 4 ð1:471–6:422Þ 389/1,295 1.30 (0.88, 1.91) 670/1,295 1.47 (1.05, 2.05)
p-Trend 0.117 0.007
Note: Models were adjusted for age, age2, sex, education, body mass index, cigarette smoke, current diagnosis of hypertension, current diagnosis of diabetes, occupational noise, rec-reational noise, and firearm noise. PTA, pure tone average.aHearing loss was defined as pure tone average >25dB.bSpeech-frequency PTA at 0.5, 1, 2, and 4 kHz.cHigh-frequency PTA at 3, 4, and 6 kHz.
Environmental Health Perspectives 067003-6
*2.56
*US 90th percentile, 2012
*3.35
*1.14

[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES AND HANDOUTS]
3/8/188
29(i.e., diabetes, hypertension). Moreover, the present study wasconducted in two different subsets of adults and adolescents,allowing us to better understand different susceptibilities in theassociation between heavy metals and hearing loss. However,several limitations should be considered. First, our study is cross-sectional, so we cannot make an inference about the temporalcausation of exposures and hearing loss; there is a potential forreverse causality. Second, lead and mercury concentrations inblood mainly reflect recent exposures. Blood lead has a shorthalf-life (i.e., ∼ 30 d), enabling a measure of current lead expo-sure, whereas bone lead, with its long-term accumulation, enablesa measure of chronic exposure (Hu et al. 1998). Indeed, a previ-ous study using bone lead measurements supports its chroniceffect on aging-related hearing loss (Park et al. 2010). Third, wecannot rule out potential exposure misclassification and residualconfounding by noisy environments that were not captured by thedichotomous variables of occupational noise, recreational noise,and firearm noise. Fourth, no data were available for congenitalcytomegalovirus infection or for genetic defects. Subjects weretherefore not excluded on the basis of either condition, nor waseither condition controlled for as a covariate. Fifth, secondhandsmoke may be a potential confounder in adolescents, but we didnot adjust for it owing to a lack of data in KNHANES adoles-cents. Sixth, important potential confounders such as occupa-tional noise and clinical diseases were adjusted for in adults butwere not adjusted for in adolescents because of a lack of data.Given the low prevalence of occupational noise and clinical dis-eases in adolescent populations, their impacts would be minimal.Finally, the low prevalence of hearing loss in adolescents resultedin wider confidence intervals for the ORs; therefore, actual asso-ciations may be more significant than our observations.
ConclusionsIn summary, the present analysis of a well-defined representativesample of Korean adults found a significant association between
current exposures to environmental lead and cadmium in the gen-eral Korean population and the risk of hearing loss independentof known risk factors including various noise exposures and clini-cal risk factors. Cadmium exposure also seems to increase therisk of hearing loss in adolescents. However, we found no signifi-cant association between environmental mercury exposure andhearing loss in either adults or adolescents. Our findings have sig-nificant public health implications; efforts to reduce environmen-tal exposures to lead and cadmium are important to preventhearing loss in the general population. Further studies with pro-spective designs and wide ranges of exposure are needed to con-firm concerns related to causal inferences and problems ofreverse causality of the association.
AcknowledgmentsThis work was supported by the Basic Science Research Programthrough the National Research Foundation of Korea (NRF)funded by the Korea Ministry of Education (grant number2013R1A6A3A04059556) and by the Korea Ministry of Science,Information and Communication Technology (ITC), and Futureplanning (grant number 2015R1C1A2A01054768). S.K.P. wassupported by grants from the National Institute of EnvironmentalHealth Sciences (NIEHS) P30-ES017885 and the Center forDisease Control and Prevention (CDC)/National Institute forOccupational Safety and Health (NIOSH) T42-OH008455.
ReferencesAgrawal Y, Platz EA, Niparko JK. 2008. Prevalence of hearing loss and differences
by demographic characteristics among US adults: Data from the NationalHealth and Nutrition Examination Survey, 1999–2004. Arch Intern Med 168(14):1522–1530, PMID: 18663164, https://doi.org/10.1001/archinte.168.14.1522.
Anderson KL. 1992. Keys to effective hearing conservation programs: Hearing statusof school age children. In: Proceedings of the ASHA Audiology Superconference.Cherwo, E, ed. Rockville, MD:American Speech-Language-Hearing Association, ASHAReport 21, 38-47. http://www.asha.org/uploadedFiles/ASHAReports21.pdf [accessed 20May 2017].
Table 4. Odds ratios (ORs) [95% confidence intervals (CIs)] of hearing loss (>15 dB) by blood lead, mercury, and cadmium levels in single-pollutant modelsin adolescents (n=853).
VariablesaSpeech-frequency PTAb High-frequency PTAc
No. hearing loss/No. participants ORs (95% CIs) No. hearing loss/No. participants ORs (95% CIs)LeadPer doubling of lead 48/853 1.20 (0.48, 3.05) 95/853 1.26 (0.73, 2.16)Lead quartile (lg=dL)Q 1 ð0:260–0:975Þ 11/213 1 (Reference) 20/213 1 (Reference)Q 2 ð0:978–1:260Þ 12/213 1.17 (0.41, 3.32) 20/213 0.89 (0.39, 2.03)Q 3 ð1:261–1:557Þ 13/213 1.08 (0.38, 3.08) 31/213 1.88 (0.83, 4.25)Q 4 ð1:562–5:904Þ 12/214 1.24 (0.34, 4.49) 24/214 1.38 (0.63, 3.02)
p-Trend 0.803 0.181MercuryPer doubling of mercury 48/853 1.01 (0.53, 1.91) 95/853 0.73 (0.45, 1.20)Mercury quartile (lg=L)Q1 ð0:555–1:488Þ 13/213 1 (Reference) 32/213 1 (Reference)Q 2 ð1:490–1:956Þ 10/213 1.00 (0.36, 2.75) 20/213 0.64 (0.30, 1.36)Q 3 ð1:960–2:683Þ 11/214 0.60 (0.21, 1.75) 17/214 0.34 (0.16, 0.74)Q 4 ð2:687–8:409Þ 14/213 1.20 (0.41, 3.54) 26/213 0.58 (0.27, 1.26)
p-Trend 0.901 0.107CadmiumPer doubling of cadmium 48/853 1.41 (0.93, 2.14) 95/853 1.54 (1.12, 2.11)Cadmium quartile (lg=L)Q1 ð0:010–0:245Þ 12/214 1 (Reference) 20/214 1 (Reference)Q 2 ð0:246–0:341Þ 9/213 0.96 (0.33, 2.76) 17/213 1.06 (0.46, 2.46)Q 3 ð0:342–0:495Þ 9/213 0.93 (0.33, 2.66) 20/213 1.51 (0.68, 3.37)Q 4 ð0:496–2:067Þ 18/213 2.39 (0.98, 5.83) 38/213 3.03 (1.44, 6.40)
p-Trend 0.083 0.003
Note: Models were adjusted for age, age2, sex, education, body mass index, cigarette smoke, recreational noise, and firearm noise. PTA, pure tone average.aHearing loss was defined as PTA>15dB.bSpeech-frequency PTA at 0.5, 1, 2, and 4 kHz.cHigh-frequency PTA at 3, 4, and 6 kHz.
Environmental Health Perspectives 067003-7
Associations of blood metals and hearing in adolescents
*1.09
*US 90th percentile, 2012
*1.32
*0.34
Conclusions
30
• Adults: hearing loss is associated with blood levels of lead and cadmium
• Adolescents: hearing loss is associated with blood levels of cadmium
• No associations with mercury
• Study strengths
‒ Population-based, large
‒ Adjusted for numerous potential confounders
‒ Numerous sensitivity analyses (supplemental material), including adjusting for the other 2 metals, urinary cotinine, fish intake, cholesterol, age strata-specific
• Study weaknesses
‒ Limited ability to adjust for noise
‒ Interactions between noise and metals not tested
‒ Blood levels reflect relatively recent exposure
‒ Possible residual confounding
§ The first OP, tetraethylpyrophosphate (TEPP), was synthesized between 1801-1854 by one or more French chemists
§ Gerhard Schrader at I.G. Farbenindustrie synthesized the first commercially successful OP pesticide (E605, aka parathion) in 1944
§ German government pursued 2 development tracks: less toxic OPs for agriculture, and more toxic OPs for warfare (Tabun, Sarin and Soman)
§ Hundreds of OPs commercialized, with usage peaking during 1970s
§ OPs comprised ~33% pesticide usage in US in 2012; higher proportion in developing nations because of low cost
31
C O N T E M P O R A R Y R E V I E W
Organophosphorus Compounds at 80: Some Old andNew IssuesLucio G. Costa*,†,1
*Department of Environmental and Occupational Health Sciences, University of Washington, Seattle,Washington 98105; and †Department of Medicine and Surgery, University of Parma, Parma 43100, Italy1To whom correspondence should be addressed at Department of Environmental and Occupational Health Sciences, University of Washington, 4225Roosevelt, Suite 100, Seattle, WA 98105. Fax: (206) 685-4696. E-mail: [email protected].
ABSTRACTOne of the major classes of pesticides is that of the organophosphates (OPs). Initial developments date back almost 2centuries but it was only in the mid-1940s that OPs reached a prominent status as insecticides, a status that, albeitdeclining, is still ongoing. OPs are highly toxic to nontarget species including humans, the primary effects being an acutecholinergic toxicity (responsible for thousands of poisoning each year) and a delayed polyneuropathy. Several issues ofcurrent debate and investigation on the toxicology of OPs are discussed in this brief review. These include (1) possibleadditional targets of OPs, (2) OPs as developmental neurotoxicants, (3) OPs and neurodegenerative diseases, (4) OPs and the“aerotoxic syndrome,” (5) OPs and the microbiome, and (6) OPs and cancer. Some of these issues have been debated andstudied for some time, while others are newer, suggesting that the study of the toxicology of OPs will remain an importantscientific and public health issue for years to come.
Key words: organophosphates; agents; acetylcholinesterase; neurotoxicity; pesticides; neurotoxicology.
Both John Doull (see article by Eaton et al. in this issue) and myown mentor Sheldon D. Murphy started their career in theToxicity Laboratory at the University of Chicago (the Tox Lab),where they both received a PhD degree in Pharmacology andworked mostly on the toxicology of organophosphates (OPs). Asmagnificently recounted by Doull (2001), the laboratory was cre-ated in 1941 to evaluate potential chemical warfare agents, andwas closed in 1973, after it had changed its name to the U.S. AirForce Radiation Laboratory. John joined the Tox Lab in 1946 andgraduated with a PhD in Pharmacology 5 years later, whileSheldon arrived at the Tox Lab in 1955, fresh from a degree inPharmacy at South Dakota University. Ken Du Bois, who servedas lab director for 20 years (1953–1973), was mentor to John andSheldon, and both worked on various aspects of the toxicology ofOPs. John’s work was on the acute and chronic toxicity of OPs,while Sheldon focused on the biochemical basis for the potentia-tion of malathion. For decades research in the laboratory focusedon Du Bois’s interests in the toxicology of OPs; all the many stu-dents and postdocs who passed through his lab thus worked on
OPs, and include many luminaries in the field of toxicology (eg,Bob Neal, Jules Brodeur, Gary Carlson, Bob Tardiff), and manycontinued to work on OPs for all their career (eg, Marion Ehrich,Sheldon Murphy). I got my feet wet in OP toxicology researchwhen I joined Sheldon’s laboratory at the University of Texas inHouston as a postdoctoral fellow. The project I was given dealtwith the study of the biochemical mechanisms involved in thetolerance to OP toxicity that was associated with repeated expo-sures. Together with graduate student Bradley Schwab, we identi-fied the down-regulation of cholinergic muscarinic receptors as amain adaptive mechanism (Costa et al., 1982). My interest in OPtoxicology continued, and over the years I have worked on vari-ous mechanisms of OP neurotoxicity (eg, Costa 1988; 2006), on therole of paraoxonase-1 (PON1) in modulating OP toxicity (eg, Costaet al., 2013), and on the developmental toxicity of OPs (eg, Coleet al., 2012). Interest in OPs by the research community has beenstrong for decades, and there is no sign of a decrease (Figure 1).
This brief review is not intended to provide a comprehensivereview of the toxicology of OPs. For that, a number of excellent
VC The Author(s) 2017. Published by Oxford University Press on behalf of the Society of Toxicology.All rights reserved. For Permissions, please e-mail: [email protected]
1
TOXICOLOGICAL SCIENCES, 2017, 1–12
doi: 10.1093/toxsci/kfx266Advance Access Publication Date: December 7, 2017Contemporary Review
Downloaded from https://academic.oup.com/toxsci/advance-article-abstract/doi/10.1093/toxsci/kfx266/4706006by University of California, San Fransisco useron 14 February 2018
Background: OP Structure
32
• Most OP insecticides are phosphorothioates(P=S bond)
• Do not directly inhibit AChE• Bioactivated by CYP-mediated oxidative
desulfuration• Most nerve agents have P=O bond and don’t
require activation
Nerve agents
Carbamate

[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES AND HANDOUTS]
3/8/189
33
The former Russian spy Sergei Skripalwas deliberately poisoned with a nerve agent in a case that police are now treating as attempted murder, Scotland Yard’s assistant chief commissioner has confirmed this afternoon.…the police officer who was first to the spot where the pair were found in Salisbury on Sunday afternoon was now “seriously ill” in hospital.
“The medical and chemical evidence and the effects on the victims point to a sophisticated nerve toxin. The best known are VX and sarin.”
The Guardian, March 7, 2018
OP Toxicity: Acute cholinergic toxicity
34
§Acute cholinergic toxicity caused by inhibition of AChE
Normal hydrolysis of ACh by AChE at muscarinic & nicotinic synapses
OP binds at serine site, leaving group hydrolyzed. Prevents ACh binding
Non-enzymatic “aging” takes hours to days: OP irreversibly bound after hydrolysis of second alkyl group
Oxime rescue prevents aging
§ Cholinergic syndrome: sweating, salivation, bronchial secretion, bronchoconstriction, miosis, diarrhea, tremors, muscular twitching, dizziness, convulsions, coma…
OP-induced delayed polyneuropathy (OPIDP)
35
• Most common form of toxicity through 1940s, now rare
• Largest outbreak affected >30,000 U.S. early 1930s: “Jake leg” (The New Yorker, 9/15/03)
• Outbreak first detected in Oklahoma City, by Ephraim Goldfain, a Romanian emigrant and physician, who ran a clinic called the Reconstruction Hospital
• Jamaica Ginger patent medicine (70-90% EtOH) produced by Harry Gross and Max Reisman, of Hub Products, shipped barrels of jake around the country.
• Newly formed NIH identified toxicant as tri-ortho-cresylphosphate (TOCP), added to interfere with prohibition-era testing
• Multi-isomer TCP produced as “Lindol” by Celluloid Corporation
OP-induced delayed polyneuropathy (OPIDP)
36
§ Signs & symptoms: onset 2-3 weeks after exposure
• Tingling of hands & feet, sensory loss
• Progressive muscle weakness, flaccid paralysis distal skeletal muscles of LE & UE
• Ataxia
§ A distal sensorimotor axonopathy
• Bilateral degeneration of distal axons and terminals
• Primarily affects larger myelinated central & peripheral fibers
§ Mechanism: • binding (and aging) of neuropathy target esterase (NTE)• ? Temporary toxic gain of function• NTE function fully recovered by the onset of signs
§ OPIDP classically associated with TOCP, but also some insecticide OPs (leptophos, chlorpyrifos, trichlorfon)
§ OPs are tested for OPIDP in hens prior to commercialization

[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES AND HANDOUTS]
3/8/1810
Non-ACHE targets of OPs
§ Neuropathy target esterase (OPIDP). Effect: toxic gain of function.
§ Acylpeptide hydrolase (APH). Function: metabolizes beta-endorphin, other small peptides. Effect: inhibition
§ Fatty acid amide hydrolase (FAAH). Function: hydrolyzes various endocannabinoids (and THC). Effect: potently inhibited
§ Lipases (especially in CNS).
§ Oxidative stress (independent of AChE inhibition)
• Microglial activation
• CNS cytokine elevations
§ Inhibition of axonal transport
37
Moretto, 2005). In recent years, accumulating evidence suggeststhat perinatal exposure to OPs may cause developmental neuro-toxicity. Several epidemiological studies have found associa-tions between in utero or early childhood exposure to OPs andbehavioral abnormalities, particularly deficits in learning andmemory (reviewed in Eskenazi et al., 1999; Eaton et al., 2008;Mu~noz-Quezada et al., 2013; Gonz!alez-Alzaga et al., 2014; Reisset al., 2015). It has been pointed out that exposure to OPs, asshown by biological monitoring in children, though somewhatelevated in inner cities or farming communities, is still at levelsbelow those causing any AChE inhibition. Several animal stud-ies also showed developmental neurotoxicity effects of OPs,however, with few exceptions, effects were observed at levelscausing significant AChE inhibition (see details in Eaton et al.,2008; Timofeeva and Levin, 2010). As indicated earlier, OPs caninteract with targets other than AChE, and affect various cellu-lar processes in vitro or ex-vivo, often at dose levels that pro-duced no clear cholinergic signs of toxicity and at times thatproduce no AChE inhibition (reviewed in Eaton et al., 2008;Burke et al., 2017) For example, a recent in vitro study reportedthat chlorpyrifos and its oxon could inhibit axonal transport atconcentrations below those required for inhibiting AChE activ-ity (Gao et al., 2017a; Table 2). It should be noted that most of thehuman, animal and in vitro studies have focused on chlorpyri-fos, a widely used OP, and to a minor extent on diazinon, lead-ing to regulatory restrictions on their use. However, there is nostrong reason to believe that other OP compound may not sharesimilar novel mechanisms of action, and further research inthis area is certainly warranted.
OPs and Neurodegenerative Diseases: Is There a Link?
Aging is often associated with a wide variety of clinical andpathological conditions which can be classified as neurodegen-erative diseases. Typical examples of such diseases areParkinson’s disease (PD), Alzheimer’s disease (AD), or amyotro-phic lateral sclerosis (ALS). The etiology of these diseases is un-known and both environmental and genetic factors may play arole; oxidative stress and neuroinflammatory processes areprominent in most neurodegenerative diseases.
Parkinson’s disease is a neurodegenerative disorder charac-terized by a slow and progressive degeneration of dopaminergicneurons in the substantia nigra, with degeneration of nerve ter-minals in the striatum. Once loss of dopaminergic neurons hasreached about 80%, clinical signs appear which include restingtremor, rigidity, bradykinesia, and gait disturbances. Though ge-netic forms of PD have been associated with specific mutationsin a number of genes, the great majority of PD cases is sporadic,and may be due to environmental factors or to gene-environment interactions, ie, exposure of genetically suscepti-ble individuals to neurotoxic substances. Among theenvironmental factors believed to be associated with PD thereare certain pesticides such as the herbicide paraquat and the in-secticide rotenone. Acute exposure to OPs has been reported tocause Parkinsonism, but this was a pharmacological, reversiblephenomenon (Muller-Vahl et al., 1999). However, Chuang et al.(2017) recently reported an increased risk of PD after OP (andcarbamate) poisoning. In addition, positive association betweenchronic exposure to OPs and PD were found (eg, Wang et al.,2014), particularly in individuals with certain paraoxonase-1genotypes (Paul et al., 2017). The mechanism(s) by which OPsmay cause degeneration of dopaminergic neurons remains elu-sive, though oxidative stress and neuroinflammation have beensuggested (Wani et al., 2017). The emerging role of gut
microbiota in PD (Parashar and Udayabanu, 2017) and theeffects of OPs on the microbiome (see below) may represent an-other fruitful avenue for mechanistic investigations.
Alzheimer’s disease is by far the most common cause of de-mentia, followed by dementia with Lewy bodies. Its most com-mon symptom is memory loss for recent events, with diffusecortical and hippocampal atrophy, and accumulation of abnor-mally folded amyloid beta and of tau proteins in amyloid pla-ques and neuronal tangles (Khan and Bloom, 2016; Selkoe andHardy, 2016). Though anticholinesterase agents (eg, rivastig-mine) are used, with limited success, to mitigate cognitive defi-cits of AD, acute and/or chronic exposures to OPs have beeninvestigated as potential etiological factors in this disease. A re-view of the literature shows that evidence for such associationin human studies is weak, and suggested mechanisms are againoxidative stress and neuroinflammation (Zaganas et al., 2013;Sanchez-Santed et al., 2016; Hern!andez et al., 2016), though thegut and oral microbiomes (both affected by OPs) may be worthinvestigating (Tremlett et al., 2017).
Amyotrophic lateral sclerosis, also known as motor neurondisease or Lou Gehrig’s disease, is a progressive neurodegenera-tive disorder of the motor neuron system, characterized by pro-gressive weakness and wasting of striated muscle due to motorcortical and spinal neurodegeneration. Environmental factorspotentially involved in the etiopathogenesis of ALS have beeninvestigated to a very limited degree. Recently it has been pro-posed that OPIDP may represent a good model for ALS, suggest-ing that “the resemblances between OPIDP and ALS are strikingat the clinical, etiological, neuropathological, cellular, and mo-lecular levels” (Merwin et al., 2017). However, such argumentsand conclusions have been rebutted, largely based on the signif-icant differences between ALS and OPIDP (Lotti and Moretto,2017). Overall, while investigations on possible associations be-tween environmental factors and neurodegenerative diseasesremain of much relevance, evidence that OPs may play an etio-logical role in such diseases remains weak.
Are OPs Involved in the “Aerotoxic Syndrome”?
Over the past 2 decades, aircrew and some passengers on vari-ous airlines have complained of ill health following exposuresto toxic fumes in airplane cabins (Harrison and Mackenzie Ross,2016). Air drawn from outside is circulated around the engineand then pumped into the aircraft; such bleed air may be con-taminated with engine oil fumes which contain a number oftoxic substances (Shehadi et al., 2016). The varied and complexarrays of signs and symptoms reported following these episodes(often referred to as “fume events”) have been given the nameof “Aerotoxic Syndrome” (Harrison and Mackenzie Ross, 2016;Michaelis et al., 2017). Reported symptoms range from respira-tory tract irritation, to gastrointestinal effects, to CNS problemsof various types (tremors, disorientation, memory loss, and
Table 2. Inhibition of Axonal Transport by the OP Chlorpyrifos
End-point Chlorpyrifos Chlorpyrifos Oxon
Lowest effective concentration
Anterograde transport 100 nM 0.1 nMRetrograde transport 10 lM 10 nMAChE activity 10 lM 10 nM
Axonal transport was measured in rat cortical neurons. Adapted from Gao et al.(2017a).
6 | TOXICOLOGICAL SCIENCES, 2017
Downloaded from https://academic.oup.com/toxsci/advance-article-abstract/doi/10.1093/toxsci/kfx266/4706006by University of California, San Fransisco useron 14 February 2018
Emerging/debated hypotheses of OP toxicity
38
§ Developmental neurotoxicity
• Increasing evidence of effects of exposure in utero or in early childhood
• Effects in rodent models noted only at levels sufficient to inhibit AChE
• Deficits in learning & memory associated with low levels (Eskenazi, 1999, EHP)
‒ ? Relationship with slowed axonal transport
§ Aerotoxic syndrome
• Airline crew complaints of ill health x 2 decades
• Concerns about air quality (engine contaminants, use of pesticides)
• Symptoms varied: respiratory irritation, GI, CNS (tremors, disorientation, memory)
• Air monitoring: toluene, carbon monoxide, tri-cresyl phosphate (TCP, from hydraulic fluids)
‒ Levels of TCP quite low, both in air and in personnel
• “Issues related to the eventual roles of OPs in the airotoxic syndrome remain emotionally charged and scientifically weak”
§ Microbiome derangement
• Clear evidence of gut microbial changes in rodents fed small concentrations various OPs
• Recent human study found changes in human oral microbiome in farmworkers using OPs (Stanaway, 2017, Appl Environ Microbiol)
OPs and Neurodegeneration
39
132 | CHUANG et Al.
In the sex- specific analysis, the PD incidences in the OP poisoning cohort were higher than those in the control cohort, and the risk of PD was higher for both women (adjusted IRR=1.47, 95% CI=1.27- 1.70) and men (adjusted IRR=1.32, 95% CI=1.20- 1.45). In the interaction analysis, sex did not significantly modify the association between poi-soning and PD (P values for interaction, .08).
The age- specific analysis showed PD incidence increasing with age in both cohorts. However, the age- specific relative risk of PD was higher in the poisoning cohort than in the control cohort for all age groups. We stratify the urbanization level by the population density of the residential area into four levels, with level 1 as the most urban-ized region and level 4 as the least urbanized region. The urbanization level- specific adjusted IRR of PD for the poisoning cohort relative to the control cohort was significant for all urbanization levels, except
the second highest urbanization level. Occupation- specific analysis showed that blue- collar workers in the poisoning cohort, compared with those in the control cohort, exhibited a higher risk of PD (adjusted IRR=1.59, 95% CI=1.44- 1.77).
The comorbidity- specific risk and adjusted HR of PD for the poi-soning cohort and the control cohort were significant for both the subgroup without comorbidity (adjusted IRR=1.33, 95% CI=1.23- 1.45) and that with comorbidity (adjusted IRR=1.71, 95% CI=1.39- 2.11). The analysis was stratified by the duration of follow- up; compared with the control cohort, the poisoning cohort exhibited a significantly higher risk of developing PD in the first 1 follow- up years (adjusted IRR=3.01, 95% CI=2.77- 3.26), in the 2- 3 follow- up years (adjusted IRR=1.27, 95% CI=1.15- 1.40), and in more than 5 follow- up years (ad-justed IRR=1.39, 95% CI=1.26- 1.53).
The multivariable Cox proportional hazards regression analysis further evaluated the roles of sex, age, and baseline comorbidities in PD development (Table 3). The risk of PD exhibited a 10% incre-ment per 1 year of age. Patients whose occupation was not white collar had a higher risk of developing PD (adjusted IRR=1.30, 95% CI=1.20- 1.42). In the multivariable model, patients with depres-sion had the highest risk (adjusted IRR=3.25, 95% CI=2.91- 3.64), followed by those with dementia (adjusted IRR=2.50, 95% CI=2.08- 3.01).
Table 4 shows that the risk of PD increased with the severity of OP or CM poisoning. Patients with a seven- day or longer hospital stay were considered to be in the high severity group; otherwise, they were considered as low severity. The high severity cases had an ad-justed IRR of 1.53 (95% CI=1.37- 1.72); the low severity cases had an adjusted IRR of 1.19 (95% CI=1.09- 1.30). The poisoning cases with respiratory failure had an adjusted IRR of 1.63 (95% CI=1.43- 1.87); the cases without respiratory failure had an adjusted IRR of 1.21 (95% CI=1.11- 1.32).
TABLE 1 Characteristics of patients with organophosphate or carbamate poisoning and patients without poisoning
Organophosphate or carbamate poisoning
P- value
Yes (N=9128)
No (N=36 466)
n (%) n (%)
Age, year .99
20- 49 3840 (42.1) 15 352 (42.1)
50- 75 4403 (48.2) 17 588 (48.2)
≥75 885 (9.70) 3526 (9.67)
Mean (SD)a 53.8 (16.3) 53.3 (16.4) .02
Gender .99
Female 2717 (29.8) 10 857 (29.8)
Male 6411 (70.2) 25 609 (70.2)
Urbanization levelb <.001
1 (highest) 702 (7.69) 10 184 (27.9)
2 1912 (21.0) 10 853 (29.8)
3 1480 (16.2) 6188 (17.0)
4 (lowest) 5034 (55.2) 9241 (25.3)
Occupation <.001
White collar 2580 (28.3) 18 739 (51.4)
Blue collar 5787 (63.4) 13 801 (37.9)
Othersc 761 (8.34) 3926 (10.8)
Comorbidity
Depression 1500 (16.4) 176 (0.48) <.001
Stroke 806 (8.83) 1434 (3.93) <.001
Dementia 55 (0.60) 120 (0.33) <.001
Psychosis 116 (1.27) 32 (0.09) <.001
Chi- square test.at- test.bThe urbanization level was categorized by the population density of the residential area into four levels, with level 1 as the most urbanized region and level 4 as the least urbanized region.cOther occupations included primarily retired, unemployed, and low- income populations.
F IGURE 2 Comparison of cumulative incidence of Parkinson’s disease between patients with and those without organophosphate or carbamate poisoning
§ Parkinson’s disease (PD)
• Data strongest for PD
• Acute, reversible parkinsonism has been reported
• Recent study found increased risk of PD after OP poisoning (Chuang, 2017, Acta Neurol Scand)
• Several supportive epidemiologic studies
• Possible gene * OP interaction (paraoxonase-1, PON1)
• Proposed mechanisms: oxidative stress, neuroinflammation
§ Alzheimer’s disease (AD)/dementia/cognition
• Data generally weak and inconsistent for AD & OPs
• Recent study found accelerated cognitive decline associated with estimated ambient OP exposure (Paul, et al, 2018, Environ Res)
• Gulf War veterans exposed to sarin have cognitive deficits and reduced hippocampal volume (Chao 2017, JOEM)
§ ALS
• Limited evidence, though some resemblances with OPIDP
40
Questions?
[ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES AND HANDOUTS]
3/8/1811
Question 1:Which of the following statements about Histoplasma capsulatum
is NOT true ?
a) Most Histoplasmosis infections cause fulminant diseaseb) H. capsulatum is found throughout the Americas
c) H. capsulatum concentrates in bird and bat droppings
d) Intravenous Amphotericin B is the preferred treatment for severe disease
41
Question 2:What percentage of NFL football players had pathological
evidence of chronic traumatic encephalopathy?
a) 20%b) 50%
c) 75%d) 99%
42
Question 3:Which of the following toxicities may be associated with
organophosphates?
a) acute cholinergic syndromeb) delayed polyneuropathy
c) developmental neurotoxicityd) All of the above
43








![Resource Guide for Practice Learning · Role emerging occupational therapy : maximising occupation -focused practice / edited by Miranda Thew ... [et al.] (2011) Using occupational](https://img.pdfslide.net/doc/110x75/5ed56e7e11be98291d042369/resource-guide-for-practice-learning-role-emerging-occupational-therapy-maximising.jpg)