Embed Size (px)
Citation preview

American Journal of Medical Genetics 124A:296–302 (2004)
Clinical Report
Gonadal Mosaicism in SeverePallister–Hall Syndrome
David Ng,1* Jennifer J. Johnston,1 Joyce T. Turner,1 Eilis A. Boudreau,2 Edythe A. Wiggs,3
William H. Theodore,2 and Leslie G. Biesecker1
1Genetic Disease Research Branch, National Human Genome Research Institute, NIH, Bethesda, Maryland2Epilepsy Research Branch, National Institute of Neurological Disorders and Stroke, NIH, Bethesda, Maryland3Consultant, National Institute of Neurological Disorders and Stroke, NIH, Bethesda, Maryland
Pallister–Hallsyndrome(PHS,MIM#146510)is characterized by central and postaxialpolydactyly,hypothalamichamartoma(HH),bifid epiglottis, imperforate anus, renal ab-normalities, and pulmonary segmentationanomalies. It is inherited in an autosomaldominant pattern. Here, we describe a familywith two affected children manifestingsevere PHS with mental retardation, beha-vioral problems, and intractable seizures.Both parents are healthy, with normal intel-ligence, and have no malformations on phy-sical, laryngoscopic, and cranial MRI exam.The atypical presentation of these childrenand the absence of parental manifestationssuggested an autosomal recessive mode ofinheritance or gonadal mosaicism. Sequenc-ing of GLI3 revealed a two nucleotide dele-tion in exon 15 (c.3385_3386delTT) predictinga frameshift and premature stop at codon1129 (p.F1129X) in the children while bothparents have wild type alleles. Genotypingwith GLI3 intragenic markers revealed thatboth children inherited the abnormal allelefrom their mother thus supporting gonadalmosaicism as the underlying mechanism ofinheritance (paternity was confirmed). Thisis the first reported case of gonadal mosai-cism in PHS. The severe CNS manifestations
of these children are reminiscent of childrenwith non-syndromic HH who often haveprogressive mental retardation with beha-vioral problems and intractable seizures.We conclude that the phenotypic spectrumof PHS can include severe CNS manifesta-tions and that recurrence risks for PHSshould include a proviso for gonadal mosai-cism, though the frequency cannot be calcu-lated from a single case report.Published 2003 Wiley-Liss, Inc.{
KEY WORDS: hypothalamic hamartoma;mental retardation
INTRODUCTION
Pallister–Hall syndrome (PHS) is a pleiotropic devel-opmental anomaly syndrome with a wide spectrum ofseverity ranging from neonatal lethality [Hall et al.,1980] to polydactyly with asymptomatic bifid epiglottisand hypothalamic hamartoma (HH) [Biesecker andGrahman, 1996]. The major findings and diagnosticcriteria are reviewed by Biesecker et al. [1996]. Mostindividuals with PHS have normal cognitive devel-opment. Gelastic (or laughing seizures), generalized, orabsence seizures are associated with PHS in a minorityof patients. The seizures in PHS patients tend to be mildand are generally easy to control with medication.
In contrast, individuals with non-syndromic or iso-lated HH manifest severe, often progressive mentalretardation with behavioral problems and have seizuresthat are refractory to medical management [Frattaliet al., 2001; Weissenberger et al., 2001]. Other patientswith non-syndromic HH manifest precocious puberty.Based on this knowledge, it has been presumed thatpatients with syndromic HH have a good neurodevelop-mental prognosis whereas patients with isolated HHand neurologic manifestations have a poor prognosis.We report a case that contradicts current prognostic andgenetic data.
Grant sponsor: National Human Genome Research Institute(Intramural Research Funds); Grant sponsor: NIH.
*Correspondence to: Dr. David Ng, M.D., NIH-NHGRI, Building49, Room 4C72, Bethesda, MD 20892-4472.E-mail: [email protected]
Received 31 March 2003; Accepted 17 April 2003
DOI 10.1002/ajmg.a.20338
Published 2003 Wiley-Liss, Inc.{This article is a U.S. Government work and, as such, is in thepublic domain in the United States of America.

CLINICAL REPORTS
Case 1
The propositus is a 9-year-old African-Americanfemale. She was delivered at 32-weeks gestation bycesarean section for fetal decelerations and polyhy-dramnios. Her birth weight, birth length, and headcircumference (OFC) were normal. At birth, she hadshort broad hands and feet with partial cutaneoussyndactyly of the right fourth and fifth fingers andbilateral second and third toes, brachydactyly, bilateralpostaxial hexadactyly of the hands, bilateral dislocatedhips, genu recurvatum, imperforate anus, and mildmidfacial hypoplasia. Cranial MRI showed the presenceof a HH. Glucocorticoids and thyroid hormone replace-ment were initiated following the diagnosis of panhy-popituitarism. At 7 months of age, premature breastdevelopment was noted. Luprolide was prescribed forthe treatment of precocious puberty. By 3 months of age,she developed gelastic seizures. Generalized seizuresand behavioral problems (oppositional and obsessive–compulsive behavior) manifested at 5 years of age.
A loop colostomy was performed to treat her imperfo-rate anus. Two weeks later she had an ileal perforationand at ileostomy, malrotation of the small bowel wasfound. Histological exam of her ileal biopsy revealedaganglionosis. A second bowel obstruction at 6 years ofage required colonic revision. Recurrent obstructivesymptoms necessitated colectomy by 7 years of age.At 7 months of age, she underwent bilateral sixth fingerexcisions for cosmesis and a suprapatellar cord releaseto relieve tight heel cords. Her left fifth toe was am-putated at the age of 4 years.
The patient has global developmental delay. She satindependently at 11 months, crawled at 18 months,pulled to stand at 24 months, said her first words at age3 years, and was toilet trained by 3½ years of age. How-ever, since 7 years of age, she has lost cognitive skills.Specifically, she cannot tell time nor recognize words.
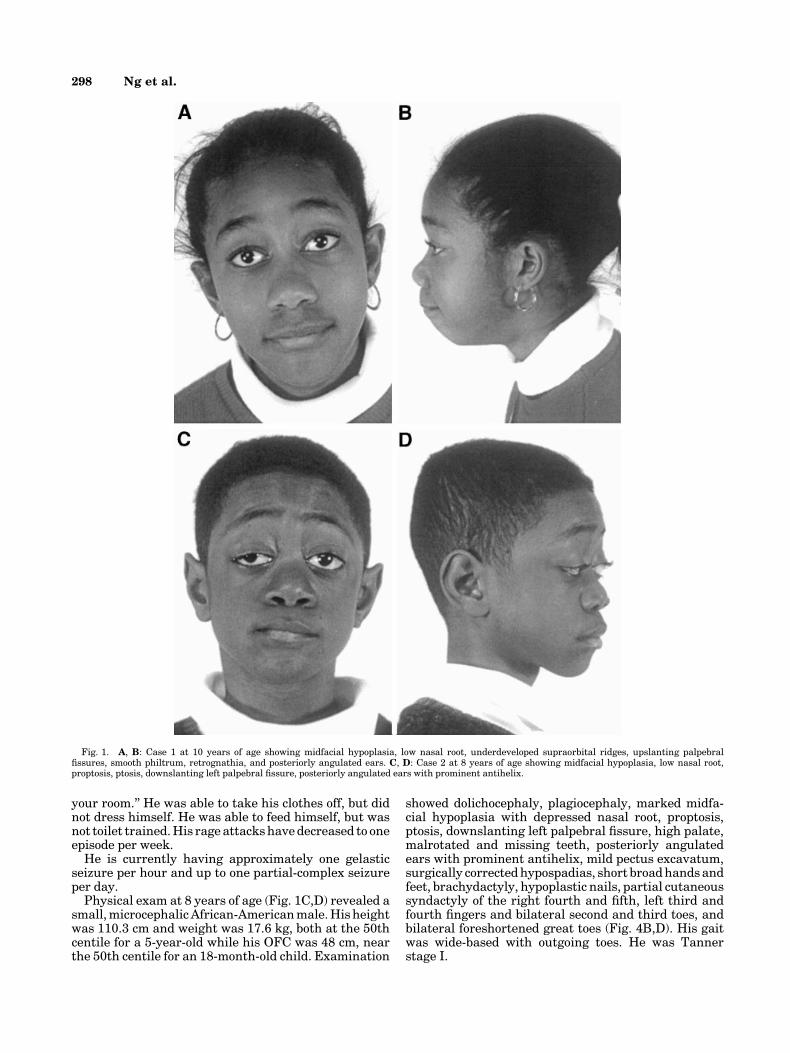
Physical examination at age 10 years (Fig. 1A,B)was notable for midfacial hypoplasia, depressed nasalroot, bilateral underdeveloped supraorbital ridges, bila-teral upslanting palpebral fissures, smooth philtrum,high palate, multiple upper buccal frenula, posteriorlyrotated ears, retrognathia, tracheostomy scar above thesternal notch, short broad hands and feet with brachy-dactyly and hypoplastic nails, absent proximal flexioncrease on the left second through fourth fingers, single,bridged left transverse palmar crease, wide gap betweenthe left third through fifth fingers, partial cutaneoussyndactyly of the right fourth and fifth fingers andbilateral second and third toes, evidence of surgicalexcision of bilateral postaxial fingers, a 2.5 cm leg lengthdiscrepancy, and an amputated left fifth toe (Fig. 2B,D).Breasts are Tanner stage II with inverted nipples.Abdominal exam reveals a transverse surgical scar andcolostomy bag in the left lower quadrant. Gait is broad-based with outgoing toes and forward-pitched torso.
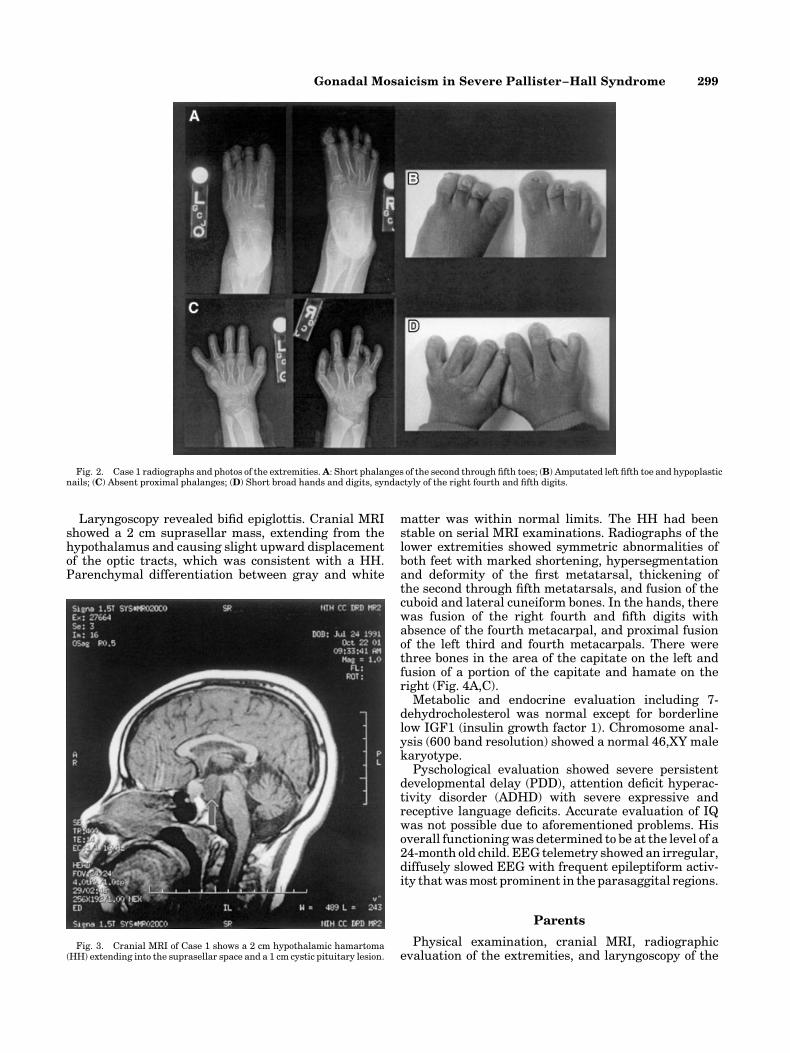
Laryngoscopic examination revealed a bifid epiglottis.Radiologic examination showed absent proximal pha-langes in the hands, absent epiphyses of the middle anddistal phalanges, shortened metacarpals and phalanges
of the second through fifth digits, the fourth metacarpalswere short, dysplastic, proximally tapered and did notarticulate with the carpal bones, the fifth metacarpalswere wide with bony prominence at the ulnar aspect,the right capitate is shortened, rounded, located in themid carpus and does not articulate with the thirdmetacarpal, status post left fifth digit metatarsal osteo-tomy, and dysplastic right third metatarsal, tapered atits proximal aspect and does not articulate with thetarsal bones (Fig. 2A,C). Cranial MRI revealed a 2 cmsuprasellar lesion consistent with a HH and a 1 cm cysticpituitary lesion (Fig. 3). The optic tracts were displacedsuperiorly. Parenchymal gray matter and white matterdifferentiation were within normal limits.
WISC-III (Wechsler Intelligence Scale for Children)testing showed a full scale IQ of 42. Metabolic causes ofcognitive regression were ruled out with normal levelsof biotinidase, urine organic acids, plasma amino acids,lactate, pyruvate, and 7-dehydrocholesterol. DSM-IV-TR axis I diagnosis is disruptive behavior disorder NOSand axis II diagnosis is mental retardation. EEG(electroencephalogram) telemetry revealed an irregu-lar, diffusely slowed EEG with intermittent bursts of3–4-Hz rhythmic slow waves that were predominant inthe anterior head regions. These bursts of slow waveswere sometimes seen during gelastic seizures.
Chromosome analysis (550 band resolution) was46,XX.
Case 2
Patient 2 is the 8-year-old brother of the propositusdescribed above. Prenatal ultrasound at 24 weeksshowed syndactyly of both hands. He was delivered bycesarean section at 36-weeks gestation for prematureuterine contractions and failure of labor to progress. Atbirth, his weight and length were normal. He had short,wide hands and feet with brachydactyly, partial cuta-neous syndactyly of the left third and fourth fingers andright fourth and fifth fingers, a gap between the first andsecond toes bilaterally, genu recurvatum of the rightknee, hypospadias, and imperforate anus. Colostomywas performed on the first day of life. Short segmentHirschsprung disease was diagnosed on biopsy. Aftercolostomy take down at 6 months of age, he developedprogressive constipation requiring chronic use of laxa-tives, enemas and manual disimpaction.
Cranial MRI revealed the presence of a HH. Thyroidhormone and glucocorticoid replacement were initiatedfor panhypopituitarism. Endocrine evaluation at age3 years revealed bilateral enlarged testes. Luprolide wasstarted for treatment of precocious puberty at 3 years.
Global developmental delay was noted from earlyinfancy. The patient sat at 12 months, crawledat 2 years,pulled to stand at 2½ years, walked at 3 years, and saidhis first words at age 5 years, however his enunciation ispoor, thus he has difficulty conveying his needs. Gelasticseizures developed between 2 and 3 years of age. Rageepisodes manifested by mood swings, oppositional, andself-injurious behavior began at age 4 years.
At 8 years of age he has a vocabulary of 15 words, but atthe time of evaluation he could only enunciate ‘‘mommy’’clearly. He followed simple commands such as ‘‘go to
Gonadal Mosaicism in Severe Pallister–Hall Syndrome 297
your room.’’ He was able to take his clothes off, but didnot dress himself. He was able to feed himself, but wasnot toilet trained. His rage attacks have decreased to oneepisode per week.
He is currently having approximately one gelasticseizure per hour and up to one partial-complex seizureper day.
Physical exam at 8 years of age (Fig. 1C,D) revealed asmall, microcephalic African-American male. His heightwas 110.3 cm and weight was 17.6 kg, both at the 50thcentile for a 5-year-old while his OFC was 48 cm, nearthe 50th centile for an 18-month-old child. Examination
showed dolichocephaly, plagiocephaly, marked midfa-cial hypoplasia with depressed nasal root, proptosis,ptosis, downslanting left palpebral fissure, high palate,malrotated and missing teeth, posteriorly angulatedears with prominent antihelix, mild pectus excavatum,surgically corrected hypospadias, short broad hands andfeet, brachydactyly, hypoplastic nails, partial cutaneoussyndactyly of the right fourth and fifth, left third andfourth fingers and bilateral second and third toes, andbilateral foreshortened great toes (Fig. 4B,D). His gaitwas wide-based with outgoing toes. He was Tannerstage I.
Fig. 1. A, B: Case 1 at 10 years of age showing midfacial hypoplasia, low nasal root, underdeveloped supraorbital ridges, upslanting palpebralfissures, smooth philtrum, retrognathia, and posteriorly angulated ears. C, D: Case 2 at 8 years of age showing midfacial hypoplasia, low nasal root,proptosis, ptosis, downslanting left palpebral fissure, posteriorly angulated ears with prominent antihelix.
298 Ng et al.
Laryngoscopy revealed bifid epiglottis. Cranial MRIshowed a 2 cm suprasellar mass, extending from thehypothalamus and causing slight upward displacementof the optic tracts, which was consistent with a HH.Parenchymal differentiation between gray and white
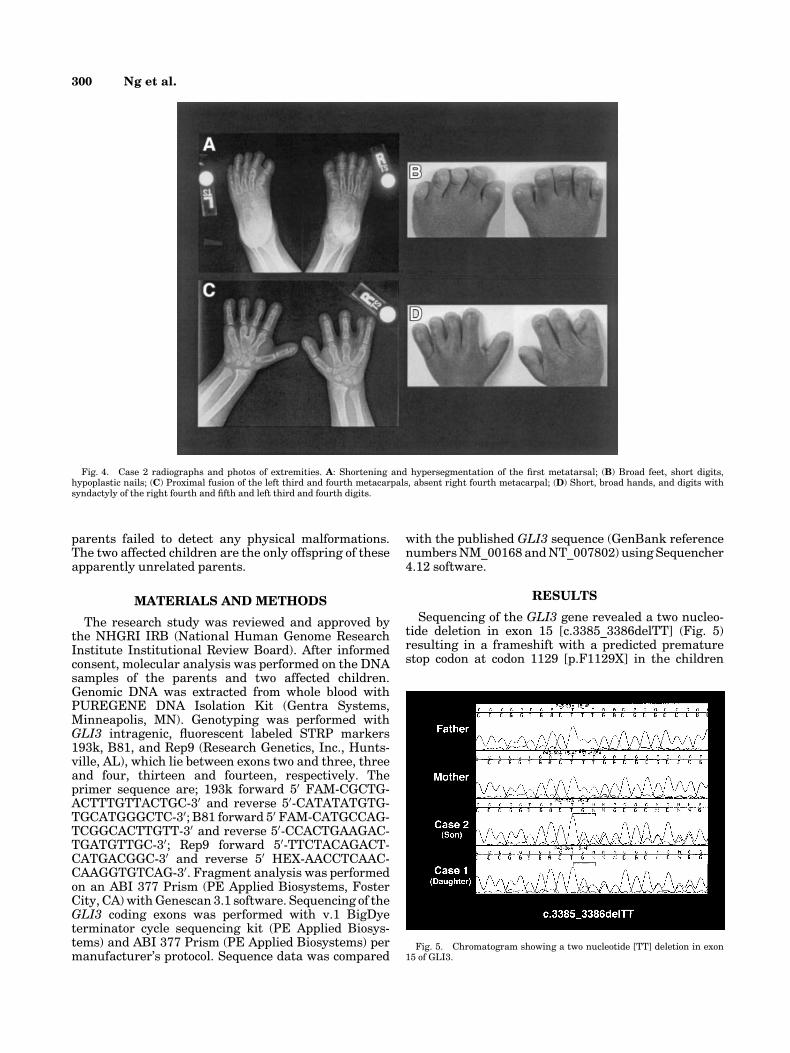
matter was within normal limits. The HH had beenstable on serial MRI examinations. Radiographs of thelower extremities showed symmetric abnormalities ofboth feet with marked shortening, hypersegmentationand deformity of the first metatarsal, thickening ofthe second through fifth metatarsals, and fusion of thecuboid and lateral cuneiform bones. In the hands, therewas fusion of the right fourth and fifth digits withabsence of the fourth metacarpal, and proximal fusionof the left third and fourth metacarpals. There werethree bones in the area of the capitate on the left andfusion of a portion of the capitate and hamate on theright (Fig. 4A,C).
Metabolic and endocrine evaluation including 7-dehydrocholesterol was normal except for borderlinelow IGF1 (insulin growth factor 1). Chromosome anal-ysis (600 band resolution) showed a normal 46,XY malekaryotype.
Pyschological evaluation showed severe persistentdevelopmental delay (PDD), attention deficit hyperac-tivity disorder (ADHD) with severe expressive andreceptive language deficits. Accurate evaluation of IQwas not possible due to aforementioned problems. Hisoverall functioning was determined to be at the level of a24-month old child. EEG telemetry showed an irregular,diffusely slowed EEG with frequent epileptiform activ-ity that was most prominent in the parasaggital regions.
Parents
Physical examination, cranial MRI, radiographicevaluation of the extremities, and laryngoscopy of the
Fig. 2. Case 1 radiographs and photos of the extremities. A: Short phalanges of the second through fifth toes; (B) Amputated left fifth toe and hypoplasticnails; (C) Absent proximal phalanges; (D) Short broad hands and digits, syndactyly of the right fourth and fifth digits.
Fig. 3. Cranial MRI of Case 1 shows a 2 cm hypothalamic hamartoma(HH) extending into the suprasellar space and a 1 cm cystic pituitary lesion.
Gonadal Mosaicism in Severe Pallister–Hall Syndrome 299
parents failed to detect any physical malformations.The two affected children are the only offspring of theseapparently unrelated parents.
MATERIALS AND METHODS
The research study was reviewed and approved bythe NHGRI IRB (National Human Genome ResearchInstitute Institutional Review Board). After informedconsent, molecular analysis was performed on the DNAsamples of the parents and two affected children.Genomic DNA was extracted from whole blood withPUREGENE DNA Isolation Kit (Gentra Systems,Minneapolis, MN). Genotyping was performed withGLI3 intragenic, fluorescent labeled STRP markers193k, B81, and Rep9 (Research Genetics, Inc., Hunts-ville, AL), which lie between exons two and three, threeand four, thirteen and fourteen, respectively. Theprimer sequence are; 193k forward 50 FAM-CGCTG-ACTTTGTTACTGC-30 and reverse 50-CATATATGTG-TGCATGGGCTC-30; B81 forward 50 FAM-CATGCCAG-TCGGCACTTGTT-30 and reverse 50-CCACTGAAGAC-TGATGTTGC-30; Rep9 forward 50-TTCTACAGACT-CATGACGGC-30 and reverse 50 HEX-AACCTCAAC-CAAGGTGTCAG-30. Fragment analysis was performedon an ABI 377 Prism (PE Applied Biosystems, FosterCity, CA) with Genescan 3.1 software. Sequencing of theGLI3 coding exons was performed with v.1 BigDyeterminator cycle sequencing kit (PE Applied Biosys-tems) and ABI 377 Prism (PE Applied Biosystems) permanufacturer’s protocol. Sequence data was compared
with the published GLI3 sequence (GenBank referencenumbers NM_00168 and NT_007802) using Sequencher4.12 software.
RESULTS
Sequencing of the GLI3 gene revealed a two nucleo-tide deletion in exon 15 [c.3385_3386delTT] (Fig. 5)resulting in a frameshift with a predicted prematurestop codon at codon 1129 [p.F1129X] in the children
Fig. 4. Case 2 radiographs and photos of extremities. A: Shortening and hypersegmentation of the first metatarsal; (B) Broad feet, short digits,hypoplastic nails; (C) Proximal fusion of the left third and fourth metacarpals, absent right fourth metacarpal; (D) Short, broad hands, and digits withsyndactyly of the right fourth and fifth and left third and fourth digits.
Fig. 5. Chromatogram showing a two nucleotide [TT] deletion in exon15 of GLI3.
300 Ng et al.
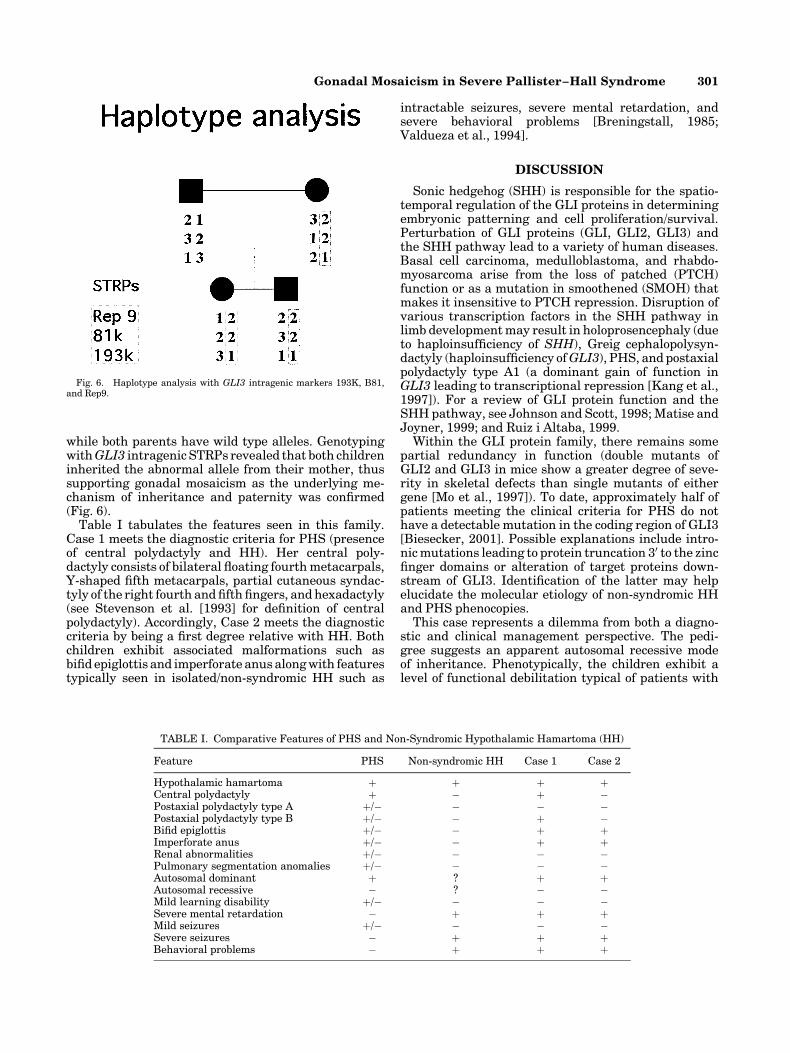
while both parents have wild type alleles. GenotypingwithGLI3 intragenic STRPs revealed that both childreninherited the abnormal allele from their mother, thussupporting gonadal mosaicism as the underlying me-chanism of inheritance and paternity was confirmed(Fig. 6).
Table I tabulates the features seen in this family.Case 1 meets the diagnostic criteria for PHS (presenceof central polydactyly and HH). Her central poly-dactyly consists of bilateral floating fourth metacarpals,Y-shaped fifth metacarpals, partial cutaneous syndac-tyly of the right fourth and fifth fingers, and hexadactyly(see Stevenson et al. [1993] for definition of centralpolydactyly). Accordingly, Case 2 meets the diagnosticcriteria by being a first degree relative with HH. Bothchildren exhibit associated malformations such asbifid epiglottis and imperforate anus along with featurestypically seen in isolated/non-syndromic HH such as
intractable seizures, severe mental retardation, andsevere behavioral problems [Breningstall, 1985;Valdueza et al., 1994].
DISCUSSION
Sonic hedgehog (SHH) is responsible for the spatio-temporal regulation of the GLI proteins in determiningembryonic patterning and cell proliferation/survival.Perturbation of GLI proteins (GLI, GLI2, GLI3) andthe SHH pathway lead to a variety of human diseases.Basal cell carcinoma, medulloblastoma, and rhabdo-myosarcoma arise from the loss of patched (PTCH)function or as a mutation in smoothened (SMOH) thatmakes it insensitive to PTCH repression. Disruption ofvarious transcription factors in the SHH pathway inlimb development may result in holoprosencephaly (dueto haploinsufficiency of SHH), Greig cephalopolysyn-dactyly (haploinsufficiency ofGLI3), PHS, and postaxialpolydactyly type A1 (a dominant gain of function inGLI3 leading to transcriptional repression [Kang et al.,1997]). For a review of GLI protein function and theSHH pathway, see Johnson and Scott, 1998; Matise andJoyner, 1999; and Ruiz i Altaba, 1999.
Within the GLI protein family, there remains somepartial redundancy in function (double mutants ofGLI2 and GLI3 in mice show a greater degree of seve-rity in skeletal defects than single mutants of eithergene [Mo et al., 1997]). To date, approximately half ofpatients meeting the clinical criteria for PHS do nothave a detectable mutation in the coding region of GLI3[Biesecker, 2001]. Possible explanations include intro-nic mutations leading to protein truncation 30 to the zincfinger domains or alteration of target proteins down-stream of GLI3. Identification of the latter may helpelucidate the molecular etiology of non-syndromic HHand PHS phenocopies.
This case represents a dilemma from both a diagno-stic and clinical management perspective. The pedi-gree suggests an apparent autosomal recessive modeof inheritance. Phenotypically, the children exhibit alevel of functional debilitation typical of patients with
TABLE I. Comparative Features of PHS and Non-Syndromic Hypothalamic Hamartoma (HH)
Feature PHS Non-syndromic HH Case 1 Case 2
Hypothalamic hamartoma þ þ þ þCentral polydactyly þ � þ �Postaxial polydactyly type A þ/� � � �Postaxial polydactyly type B þ/� � þ �Bifid epiglottis þ/� � þ þImperforate anus þ/� � þ þRenal abnormalities þ/� � � �Pulmonary segmentation anomalies þ/� � � �Autosomal dominant þ ? þ þAutosomal recessive � ? � �Mild learning disability þ/� � � �Severe mental retardation � þ þ þMild seizures þ/� � � �Severe seizures � þ þ þBehavioral problems � þ þ þ
Fig. 6. Haplotype analysis with GLI3 intragenic markers 193K, B81,and Rep9.
Gonadal Mosaicism in Severe Pallister–Hall Syndrome 301

non-syndromic HH although they have malformationsthat are typical of PHS. GLI3 mutation analysis andgenotyping of the family supports a maternal gonadalGLI3mutation as the underlying molecular mechanism.Although this provides an explanation for the inheri-tance pattern, it does not explain the severe seizuresand cognitive regression found in the children. Possibleexplanations include modifier genes or alteration oftarget proteins downstream of GLI3.
On a histological level, the HH occurring with syn-dromic and non-syndromic HH are non-distinguishable.There is no apparent explanation for the greater CNSsymptoms in these children, who meet clinical diag-nostic criteria for PHS and have a typical mutation(irrespective of its gonadal origin). Their mental retar-dation (cognitive decline in Case 1, static encephalo-pathy in Case 2), difficult to control seizures (gelastic,absence, generalized), and severe behavioral problemsare common in non-syndromic HH. Indeed, it is theCNS effects of the HH and not the associated phy-sical anomalies that are the primary problem for thisfamily. Foremost in urgency is the issue of seizuremanagement. Based on EEG telemetry, both childrenhave continuous epileptiform discharge throughoutthe day (despite treatment with levetiracetam andlamotrigine in Case 1; levetiracetam, lamotrigine, andcarbamazepine in Case 2). It is difficult to assess thedegree of harm that the seizures have caused in termsof the children’s mental retardation/cognitive declineand their behavioral difficulties. Surgical resection ofHH is the treatment of last recourse in such cases assurgical morbidity and mortality are frequent and canbe severe. HHs are classified according to size, location,and type of attachment [Breningstall, 1985; Valduezaet al., 1994]. Surgical resection is generally reserved fortype II HH (>1.5 cm in size) with the treatment goalbeing amelioration of seizure activity and or behavioralproblems. Unfortunately, the children presented herewere deemed poor surgical candidates due to the sizeand location of their hamartomas.
This case illustrates the need to thoughtfully in-terpret molecular testing of GLI3 for the purpose ofprognostication in families with a newborn exhibitingfeature of PHS. More than half of patients meeting theclinical criteria for PHS have mutations in the codingregion ofGLI3 (Biesecker [2001] and unpublished data).The great majority of this group can be expected tohave relatively benign CNS manifestations. Only a fewwill have severe or intractable seizures or significantcognitive deficits. The data presented here suggest thatuncommonly, a child with a typical PHS mutation mayhave severe CNS dysfunction. Due to biased ascertain-ment and small study size, we cannot estimate the re-lative frequencies of severe and mild PHS. In addition,recurrence risk estimates in a de novo case of PHS inan apparently unaffected family should take into ac-count the possibility of gonadal mosaicism in one of
the parents. The actual risk for gonadal mosaicism inPHS is unknown.
ELECTRONIC-DATABASE INFORMATION
Accession numbers and URLS for data in this articleare as follows: Online Mendelian Inheritance in Man(OMIM), http://www.ncbi.nlm.nih.gov/OMIM/for PHS[MIM 146510], Greig cephalopolysyndactyly syndrome[MIM 175700], postaxial polydactyly type A1 [MIM174200], GLI [MIM 165220], GLI2 [MIM 165230], GLI3[MIM 165240], PTCH [MIM 601309], SHH [600725],SMOH [MIM 601500].
ACKNOWLEDGMENTS
The authors thank the family described herein fortheir participation. This work was supported by intra-mural research funds from the National HumanGenome Research Institute, NIH.
REFERENCES
Biesecker LG. 2001. Genotype phenotype correlation in human GLI3disorders. Eur J Hum Genet 9(Suppl):76.
Biesecker LG, Grahman JM Jr. 1996. Pallister–Hall syndrome. J MedGenet 33:585–589.
Biesecker LG, Abbott M, Allen J, Clericuzio C, Feuillan P, Graham JM Jr,Hall J, Kang S, Olney AH, Lefton D, Neri G, Peters K, Verloes A. 1996.Report from the workshop on Pallister–Hall syndrome and relatedphenotypes. Am J Med Genet 65:76–81.
Breningstall GN. 1985. Gelastic seizures, precocious puberty, and hypotha-lamic hamartoma. Neurology 35:1180–1183.
Frattali CM, Liow K, Craig GH, Korenman LM, Makhlouf F, Sato S,Biesecker LG, Theodore WH. 2001. Cognitive deficits in children withgelastic seizures and hypothalamic hamartoma. Neurology 57:43–46.
Hall JG, Pallister PD, Clarren SK, Beckwith JB, Wiglesworth FW,Fraser FC, Cho S, Benke PJ, Reed SD. 1980. Congenital hypothalamichamartoblastoma, hypopituitarism, imperforate anus, and postaxialpolydactyly—a new syndrome? Part I: Clinical, causal, and pathogeneticconsiderations. Am J Med Genet 7:47–74.
Johnson RL, Scott MP. 1998. New players and puzzles in the Hedgehogsignaling pathway. Curr Opin Genet Dev 8:450–456.
Kang S, Graham JM Jr, Olney AH, Biesecker LG. 1997. GLI3 frameshiftmutations cause autosomal dominant Pallister–Hall syndrome.Nat Genet 15:266–268.
Matise MP, Joyner AL. 1999. Gli genes in development and cancer.Oncogene 18:7852–7859.
Mo R, Freer AM, Zinyk DL, Crackower MA, Michaud J, Heng HH, Chik KW,Shi XM, Tsui LC, Cheng SH, Joyner AL, Hui C. 1997. Specific andredundant functions of Gli2 and Gli3 zinc finger genes in skeletalpatterning and development. Development 124:113–123.
Ruiz i Altaba A. 1999. Gli proteins and Hedgehog signaling: developmentand cancer. Trends Genet 15:418–425.
Stevenson RE, Hall JG, Goodman RM. 1993. Human malformations andrelated anomalies. Vol II. New York: Oxford University Press. p 826.
Valdueza JM, Cristante L, Dammann O, Bentele K, Vortmeyer A, Saeger W,Padberg B, Freitag J, Hermann H. 1994. Hypothalamic hamartomas:With special reference to gelastic epilepsy and surgery. Neurosurgery34:949–958.
Weissenberger AA, Dell ML, Liow K, Theodore W, Frattali CM, HernandezD, Zametkin AJ. 2001. Aggression and psychiatric comorbidity inchildren with hypothalamic hamartomas and their unaffected siblings.J Am Acad Child Adolesc Psychiatry 40:696–703.
302 Ng et al.





























