Embed Size (px)
Citation preview
I
GONOCOCCAL ARTHRITIS
WITH OBSERVATIONS BASED ON A SERIESOF 388 CASES
DAVID LEES, D.S.O., M.B., D.P.H., F.R.C.S., F.R.C.P., Surgeonin Charge of Venereal Diseases Department, The Royal Infirmary,Edinburgh, and Edinburgh Corporation Venereal DiseasesClinics.
IN the literature on gonococcal arthritis the earliestreference is the record of a case in I507 by Van Forest.In I664 Martiniere 1 drew attention to this clinicalentity as a complication of gonorrhoea in his " Traite dela Maladie Venerienne." The first real presentation ofthe subject was given by Theophile Salle and Swediaur 2in I78I, who referred to it as " an inflammatory articularinfection dependent on gonorrhoea." The earliest descrip-tion in English medical literature is by Sir BenjaminBrodie,3 in i8i8, although John Hunter refers to it inone of his treatises in I786, and Astley Cooper in i8o6.With the discovery of the gonococcus by Neisser 4 in
I879, a controversy arose as to whether the same organismwas a factor in the production of the arthritis whichoccurred as a complication in cases of gonorrhoea. InI830, William Lawrence 5 had drawn attention to the truenature of gonococcal arthritis. In I883, Petrone 6discovered the organism in the joint fluid in two cases.This work was confirmed by others, and in I894 Hewes 7isolated the gonococcus from the blood of patientssuffering from polyarthritis.
Incidence.-The estimate of Osler 8 is 2-5 per cent. ofall cases. Lumb 9 finds the incidence to be o 5 per cent.in 50,000 cases. Klose,'0 reporting cases in Germanyprevious to the war, gives the figure as 2 per cent., whileduring the war he states that it was as high as IO per cent.Ireland," in reviewing the U.S. Army Medical Records,found 3 o3 per cent. in 259,899 cases. Chiari 12 gives theincidence as 3 per cent. in 45,000 cases. Harrison and
79
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
Pollock,13 in 8I2 cases in the British Army, gave thefigure as ir85 per cent.
In a consecutive series of over I3,000 cases of gonor-rhoea in Edinburgh hospitals, there have been 388 casesof arthritis. This gives a percentage figure of 2'9I-3-22 per cent. in males and i8i per cent. in females.Arthritis is stated to be four to five times as common inmen as in women. Thomas,'4 in a series of I07 cases,finds the proportion much larger, and attributes theincreased incidence in the male to the long poorly drainingurethra, and to the complicated structure of the prostateand vesicles.Our figures of the incidence, taken as they are from a
V.D. clinic, are probably exaggerated because there isa tendency on the part of doctors to send all cases ofacute joint complications to hospital ; this would increasethe percentage figure in our cases.Age Incidence.-Arthritis may complicate gonorrhoea
at any age, but it is more frequent in young men fromtwenty to thirty years of age, largely because gonorrhoeais more frequent then. In females the same age periodholds good. It occurred in the very young in associationwith ophthalmia neonatorum in two of our cases. Casesof this have been recorded, but are very rare. In a seriesof I50 cases of vulvo vaginitis in children we had no caseof arthritis as a complication. This is not the experienceof American workers.
Predisposing Causes.-The most important is lack oftreatment in the earlier stages of gonorrhoea. It is note-worthy that arthritis is rare in cases of anterior urethritisin the male and in cases of urethritis in the female. Ifthese cases are treated early and intelligently, the infectionrarely passes to the posterior urethra in the male or thecervix in the female. Another predisposing cause is tooactive exercise or heavy exercise during the acute stageof the disease; not infrequently the patient attributesthe joint condition to some trauma. In all cases ofgonococcal infection, alcoholism predisposes to metastaticcomplications, of which arthritis is the most frequent.Arthritis is always prone to recur, and one attack pre-disposes to a subsequent one. Recurrence of infectivemanifestations in a joint frequently follows a reinfectionor the lighting up of a chronic focus.
£Etiology.-In every case there is a primary focus of8o
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from

GONOCOCCAL ARTHRITIS
infection in some part of the body; the genital or urinarytract is the common site, but it may be the conjunctivaor other mucous surface. The infection of the joint ismetastatic, and the organism is carried by the bloodstream to the affected joint. The gonococcus was firstisolated from the blood by Thayer and Blumer.15 Colum-bini, and two years later Uysing,16 demonstrated it in thelymph stream. Zieler 17 believes that all gonorrhcealinfections begin as a septicaemia, and that the organismsdisappear quickly from the blood stream, or are presentin such small numbers as to make it difficult to find themby blood culture. It is interesting to note in this connec-tion that in cases of acute arthritis it is often difficult tofind the organisms in joint fluid after a few days. Theyseem to disappear from any encapsulated fluid after atime. This will be referred to later. There are somemild cases in which it is possible that the arthritis is dueto a toxaemia. Lofaro,18 in an examination of sixty-sevencases of gonorrhoea, found the organism in the blood inthirty-nine of them. The disease was in the subacute orchronic stage in all these cases. He believes that gono-cocci appear in the blood stream and survive in it onlywhen a virulent strain of bacteria is present, or when thesoil is suitable, and the patient susceptible. The fact thatgonococcal metastasis is so rare in gonorrhoea appearsto support Lofaro's contention.The metastasis has been recorded by Resnikow 19 as
early as the fourth day after exposure to infectiorn.The earliest case of joint infection we have seen
occurred five days after infection in a child suffering fromophthalmia.The opinion has been expressed that the arthritis may
be a toxic manifestation. While it is possible that someof the arthralgias are toxic in origin, there is ampleevidence that, in the more severe cases which lead to aserous or serofibrinous exudate, the joint tissues areinvaded by the gonococcus. Nasse and Rindfleisch,20 inI897, obtained pure cultures of gonococci from the jointfluid in I9 out of 30 cases, and Baur,21 in I9OI, in I9 outof 27 cases. Thomson,22 in I923, found the organism inthe joint fluid in ten cases. These workers emphasisethe importance of a good technique and special media.Thomson states that the culture requires to be incubatedfor at least ten days, as, in his experience, the growth of
8I
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
gonococcus did not show up until the seventh day in onecase and the tenth day in another. McDonagh 23 foundthe aspirated effusion from the joint to be sterilein nine cases. It is possible that, after the first fiveor six days, the organisms may localise themselves inthe synovial membrane, the cartilages, or the epiphyses,and that the intra-articular exudate which results fromthis localised infection is in the nature of a sterile serousexudate.
Site of Primary Focus.-In the male it is generallyaccepted that the prostate gland and the seminal vesiclesare the common foci from which the infection spreadsto the blood stream. It is difficult to prove this in acutecases because the whole urethral tract is the site of anacute infection in addition to the prostate and vesicles.In chronic cases, however, and in acute exacerbationsoccurring in the course of a chronic case, there is ampleevidence that these anatomical areas are the commonreservoir for latent gonococci.
Michel, 24 in examining thirty-three cases of arthritis,found in twelve of them that there was involvement ofthe anterior urethra only. In our series the posteriorurethra was involved in I00 per cent. of the cases, andwe were able to find evidence of prostatitis or vesiculitisin over go per cent. of these cases.
In adult female patients, the urethra and cervix wereinvolved in close on 8o per cent. of the cases of arthritis.The Bartholinian gland was infected in about 40 per cent.of the cases.We have referred to arthritis as a complication of
ophthalmia neonatorum. In I899, Clement Lucas 25published records of three cases which he had referredto in I885 and in I890. He states that Deutschmannisolated the organism in fluid aspirated from an inflamedjoint complicating a case of purulent ophthalmia. Sincethen cases have been reported by Johnstone, 26 Fischer,27Pritzi, 28 Herzfeld,29 and others.Two cases occurred in our series as a complication of
ophthalmia.In a series of 200 cases of vulvo-vaginitis in young girls,
there has been no case of arthritis. This is rather atvariance with the observation of McDonagh, who statesthat arthritis is not an uncommon complication of vulvo-vaginitis. In a series of cases reported in the American
82
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
GONOCOCCAL ARTHRITIS
Journal of Diseases of Children (Vol. III., I927), rectalgonorrhoea in children is stated to be a common cause ofmetastatic arthritis, fifty-three out of sixty-s,even casesshowing joint complications. In our experience rectalgonorrhoea is not common in children suffering fromvulvo-vaginitis.Time of Onset of Arthritis after Primary Infection.-
The earliest adult case which we have seen occurred fivedays after the urethral infection; in general, the jointmanifestations occur within the first four to five weeksin 8o per cent. of the cases. In complicated and chroniccases the onset of the arthritis may be later, and casesof arthritis have been recorded as occurring fifteen totwenty years after the onset of gonorrhoea. In these latecases the metastatic infection of the joint may followthe passage of an instrument for the treatment of stricture,or the lighting up of some latent focus in the cervix or inthe Fallopian tubes after a pelvic operation. These latecases are usually monarticular, or at the most involveone or two joints only.
Involvement of Joints.-The disease may be monarti-cular or polyarticular, the percentage in our cases beingI5 per cent. monarticular and 85 per cent. polyarticular.An arthritis occurring late in the course of the diseasetends to be monarticular. The large joints are involvedwith greater frequency than the small ones and the kneeis affected most frequently. The order of frequency inour series was as follows
Knee . . . . . 64-2 per cent.Ankle . . . . . 36-8Metatarso-phalangeal . . 34.7Shoulder . . . . . 231IWrist . . . . . I4IMetacarpo-phalangeal . .I36Elbow . . . . . II5Hip . . . . . 42Intervertebral . . . . 3-ITemporo-mandibular. . . 2-I
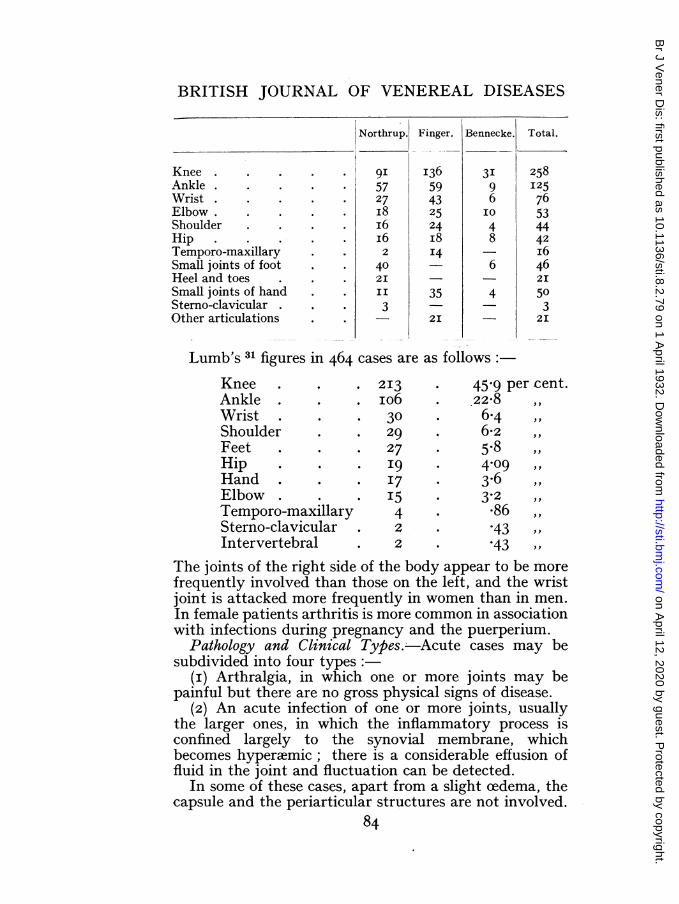
The statistics of Northrup,30 Finger, and Bennecke showthat the joints were involved in the following frequencyin a series comprising 704 cases
83
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
KneeAnkleWristElbow.ShoulderHipTemporo-maxillarySmall joints of footHeel and toesSmall joints of handSterno-clavicularOther articulations
Lumb's 31 figures in 464 cases are
KneeAnkleWristShoulderFeetHipHandElbowTemporo-maxillarySterno-clavicularIntervertebral
2I3io63029
27I9I7I5422
45.9 per cent.22-8 ,,6-46-2 ,,5-84-09
3-2386 ,,*43 ,,*43 ,,
The joints of the right side of the body appear to be morefrequently involved than those on the left, and the wristjoint is attacked more frequently in women than in men.In female patients arthritis is more common in associationwith infections during pregnancy and the puerperium.
Pathology and Clinical Types.- Acute cases may besubdivided into four types:
(i) Arthralgia, in which one or more joints may bepainful but there are no gross physical signs of disease.
(2) An acute infection of one or more joints, usuallythe larger ones, in which the inflammatory process isconfined largely to the synovial membrane, whichbecomes hyperaemic; there is a considerable effusion offluid in the joint and fluctuation can be detected.
In some of these cases, apart from a slight cedema, thecapsule and the periarticular structures are not involved.
84
Northrup.
9I5727i8i6I62
402III
3
Finger.
I3659432524i8'4
35
2I
Bennecke.
3I96IO
48
6
4
Total.
258I25
76534442i6462I
503
2I
as follows:
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from

GONOCOCCAL ARTHRITIS
In others the capsule and the periarticular structures arethickened and very cedematous, due to an inflammatoryexudate into them.
(3) An acute infection in which, in addition to thesynovial membrane, the cartilaginous surfaces becomeeroded and small flakes of necrosed articular cartilagebecome detached or are loosely attached to the ulceratedor eroded area.The effusion in this type of joint infection is more in
the nature of a serofibrinous exudate, and is less inamount than in the purely synovial type.The capsule and the periarticular tissues are nearly
always attacked, and are the site of fibroplastic changesfollowing on the serofibrinous exudate.
In some of these cases, especially in the smaller joints,the swelling is almost entirely periarticular and involvesthe capsule, the bursae, and the tendon sheaths surround-ing the joint. If the inflammation is unchecked, theserofibrinous exudate leads to the formation of intra- andperiarticular adhesions and subsequent deformity.
In a few cases, in the larger joints, there may be con-siderable destruction of the articular surfaces, the liga-ments give way, and subluxation of the joint follows withmarked deformity.
(4) An acute infection involving the synovial mem-brane and the articular surfaces with marked hypereemiaof all the vascular structures. The intra-articularexudate becomes purulent, and there is marked ulcerationand erosion of all the cartilaginous surfaces. This typeoccurs in the large joints, and periarticular changes areoften present. It is rarely met with. It is often statedthat purulent cases result from a mixed infection, butthe bacteriological studies of Young 32 have provedconclusively that in many cases the gonococcus is in pureculture and is alone responsible for the pyarthrosis.
Subacute and chronic cases may be subdivided intotwo main types
(i) A synovial type, involving especially the kneejoint. The synovial membrane is thickened, and thereis a moderate degree of effusion into the joint. If theamount of fluid is large and untreated it may produce alaxity of the ligaments. The periarticular structures arenot involved to any great extent.
This type may evolve from the untreated acute85
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
synovitis, or the joint condition may be subacute fromthe commencement if the metastatic infection is not avirulent one.
(2) A mixed type, involving both the synovial mem-brane and the articular surfaces, and frequently poly-articular in the smaller joints, in which the serofibrinousexudate is always fibroplastic, and leads to adhesions anddeformity. Proliferative, changes are more evident thandestructive ones, and the periarticular tissues are involvedin the fibroplastic process in almost every case.
It may result from an untreated acute case; in othersthe condition is subacute from the onset, with just aslight effusion of plastic lymph into the joint and aconsiderable amount of periarticular swelling.Symptoms and Signs.-The variability of the symp-
toms is a distinguishing feature. It depends on thevirulence of the infecting agent when it reaches the joint,and on the resistance of the tissues of the host. Thestage of exudation is rarely reached in mild cases, and theinflammation manifests itself clinically by the onset ofarthralgic pain, which flits from joint to joint withoutgiving rise to any physical signs of inflammation. Thispain is usually of short duration, but may last for days.In some cases, and especially if the primary focus isuntreated, it merges into a definite acute arthritis in-volving one or more joints. Pain is then a markedfeature, and the pain is persistent and is aggravated bymovement.
If the effusion is chiefly synovial, the swelling increasesrapidly, and involvement of one joint may be followedby another. As the joints swell, the pain becomes moreintense; the skin over the surface is red and cedematous.The presence of fluid can readily be detected in the joint,and the burs?e, in relation to the joint, are often distendedwith fluid. There is frequently an inflammatory tender-ness along the tendon sheaths and in the muscles actingon the joint.
If the infection is involving all the joint structuresand the periarticular tissues, there is not so much swellingin the joint cavity, because the effusion is more of aserofibrinous character, and is less in quantity. Thetissues surrounding the joint are cedematous and swollen,and feel thickened. The joint and the regions over thetendon sheaths are very tender to touch; they feel hot,
86
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
GONOCOCCAL ARTHRITIS
but the skin surface is not so red and the process doesnot advance so rapidly as in the synovial type; teno-synovitis is common. Movement of the joint aggravatesthe pain, and the muscle tissues are often the site of aninflammatory myositis. In both cases the temperaturereaction varies from IOI1 to IO3° F.
In the few cases in which the infection proceeds tosuppuration, the temperature rises still higher. Pain ismore severe because of the destruction of the cartilaginoussurfaces. Starting pains, especially at night, and sweat-ing, which is more characteristic of acute rheumatism,become prominent clinical features. Fluctuation can bedetected easily. The general health is more seriouslyaffected, and the patient looks ill.When the small joints of the hand and foot are affected,
pain, heat and redness are as prominent as in the largerjoints, but the swelling is not so pronounced. The tendonsheaths and periarticular tissues are invariably involved.Suppuration is extremely rare in small joints.
In subacute and chronic cases the swelling is often inthe nature of a hydrops. Swelling is the chief clinicalsign in hydrops. Movement is not limited except by theamount of fluid in the joint, and the pain is slight and isonly present on movement. The common site for hydropsis the knee joint. If the effusion is untreated it maydistend the joint and lead to laxity of the ligaments. It isvery apt to be recurrent if the original focus of infectionis not eradicated.
In subacute and chronic gonococcal osteoarthritis thesmaller joints are attacked more commonly, althoughthe larger joints are not immune. There is alwaysa considerable amount of periarticular swelling andcedema, but little joint exudate. The muscles actingin the joint show marked wasting, which makes thefusiform swelling of the joint more apparent. In thesubacute stages these joints are somewhat tender, butin chronic cases pain is only present if an attempt ismade to move the joint. In many of the untreated casesthere is marked limitation of movement, due to adhesionsset up by the serofibrinous exudate, and in some casesthe adhesions give the impression that the joint isankylosed.Diagnosis.-There is no great difficulty in the diagnosis
of acute gonococcal arthritis in the male if the clinician87
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
will remember to make tactful enquiries regardingurethral discharge, and look carefully for it. In somecases, however, with the onset of arthritis the signs ofurethral disease may lessen, but in all the urine remainsturbid, and examination per rectum will often revealsome enlargement of the prostate and of the vesiculaeseminales in such cases. Gentle massage of these organsenables us to express fluid, in which the gonococcus maybe demonstrated. It is more difficult to be accurate inthe diagnosis of acute cases when they follow on a slightexacerbation of a chronic focus of gonococcal infectionin the vesicles, or after the passage of an instrument forstricture.
In most acute cases the history, the discharge, andthe presence of gonococci in it make the diagnosis certain,except when a sufferer from gonorrhoea develops an acutearthritis from some other cause, such as tuberculosis.
If there is no obvious focus of gonococcal infection, itis always important to exclude this type of infection byrepeated examinations, when an acute, subacute orchronic affection of a joint is painful, persistent, andassociated with periarticular changes. If the organismcan be isolated from the joint fluid the diagnosis isdefinite, but failure to find the gonococcus in the fluiddoes not preclude its presence.
It is important in acute cases to be able to differentiatebetween acute rheumatism and a gonococcal arthritis.The following are the main distinctions:
Acute Rheumatismi. No evidence of genito-urinary
disease.2. Marked temperature reaction
and more prolonged constitu-tional upset and prostration.
3. Sweating very profuse, withacid odour.
4 Pain intense and aggravatedby the slightest touch.
5. Many joints involved, but aspain leaves one it flits toanother, and the first affectedappears to be free from dis-comfort.
6. Tendon sheaths and peri-articular tissues rarely in-volved.
Gonococcal ArthritisOften definite urogenital symp-toms and signs.Very moderate temperature reac-tion, and constitutional upsetslight, except in purulent cases.Very little sweating except inpurulent cases.Pain less intense.
May be limited to one joint, andusually one or two joints only,and pain does not leave a jointrapidly and pass to another.
Tendon sheaths very frequentlythe site of disease, and also peri-articular tissues.
88
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
GONOCOCCAL ARTHRITIS
7. More common in women. Less frequent in women.8. Often some cardiac complica- Cardiac complications very rare,
tion, such as endocarditis or and no acute condition in thepericarditis, and an active tonsil.focus of infection in the tonsil.
9. Symptoms and temperature Salicylates have little effect onreact extremely well to the the pain, the swelling, or theadministration of salicylates. temperature.
IO. Complement-fixation test of Complement fixation for gonor-blood negative. rheea test always positive.
ii. Temporo-mandibular joint May be involved.rarely involved.
Acute gonococcal arthritis must, in addition, be differen-tiated from arthritis following on pneumonia, dysentery,cerebro-spinal, typhoid, or scarlet fever, acute tonsilitis,and tuberculosis.An acute tuberculous arthritis is slower in its onset,
it is rarely polyarticular, the pain is not so severe at first,there is often epiphyseal involvement, and X-ray examina-tion will reveal a definite lesion of the bone, which is notcommon in gonorrhoea.
In pneumococcal cases the joint fluid almost alwaysshows the presence of pneumococci. In other cases ofpyogenic arthritis the typical signs of the active disease,such as scarlet and typhoid fever, etc., are of the greatesthelp in accurate diagnosis.
SUBACUTE AND CHRONIC CASES OF GONOCOCCAL ARTHRITISSubacute and chronic cases of gonococcal arthritis are
very difficult to diagnose from those due to other bacterialinfections, such as Bacillus coli, various streptococci andpneumococci, B. tuberculosis, B. Dysenteriae, and theStreptococcus rheumaticus. The various forms of chronicinfective, or " rheumatoid," arthritis, osteoarthritis, andthe early stages of the arthropathies or trophic distur-bances, as in tabes dorsalis or syringomyelia, maystimulate a chronic gonococcal joint.A subacute joint condition which is persistent and
shows periarticular changes should always prompt us toexclude a gonococcal infection. This necessitates anexamination for urethral discharge and of the urine;bacteriological tests of any secretion or of the centrifugeddeposit of the urine should follow, and, in addition, rectalpalpation and massage of the prostate and vesicles to
V.D. 89 H
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from

BRITISH JOURNAL -OF VENEREAL DISEASES
express their contents for examination by direct film orby culture. Even if gonococci are not demonstrated inany of the examinations, the presence of pus cells in theprostatic or seminal secretion is suspicious. It shouldlead us to give the patient an injection of an emulsioncontaining 200 to 400 millions of dead gonococci to stirup any latent focus of disease; the clinical and bacterio-logical tests are repeated 36 to 48 hours subsequent tothis injection.
Similarly, in a female, suffering from chronic arthritis,it is important to examine the urethra, the Bartholinianducts and glands, the endocervix, the Fallopian tubes,and the pelvic cellular tissues in searching for a focus ofinfection. Direct films and cultural tests are carried outafter administering an injection of polyvalent vaccine, orafter inserting a plug of gauze soaked in glycerine intothe endocervix. The best time to examine the female forsigns of latent gonorrhoea is post-menstrual.
In both sexes a positive result in the gonococcalcomplement-fixation test of the blood may help to-establish the aetiology of the joint affection. If anysuspicious sign of infection is found in either sex, thereaction to treatment is often of considerable assistancein diagnosis.
In distinction from chronic tuberculous joints, gono-coccal cases are more often polyarticular, with the excep-tion of a hydrops. The X-ray appearances are differentfrom those of tuberculosis. The fasciae and aponeurosisare more often affected in gonococcal affections, and araised temperature in the joint is more common intuberculosis. Wasting of the muscles acting on the jointis stated to be more common in tuberculosis, but this isalso a prominent feature of chronic gonococcal arthritis.
In differentiating from other forms of chronic infectivearthritis, the X-ray appearances in the cartilage andbone are helpful, especially in excluding an early rheuma-toid arthritis. A history of recurrent attacks of iritis ina patient suffering from arthritis strongly suggests agonococcal aetiology.
X-RAY APPEARANCES IN GONOCOCCAL ARTHRITISIn acute joint involvement this is of little assistance
except in differentiating from acute tuberculous disease.90
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
GONOCOCCAL ARTHRITIS
If the intra-articular exudate is marked there is an apparentincrease in the joint space. If the infection is involvingboth synovial and articular surfaces, the joint spacemay be decreased by the absorption of cartilage. Theseappearances, however, may result in any acute pyogenicarthritis, although in gonococcal cases they occur lessrapidly, and are rarely so extensive except when thearthritis sets in during pregnancy and the puerperium.The radiographic appearances in chronic gonococcal
arthritis simulate those of any chronic infective arthritis.In tuberculosis there is often definite evidence of osseouschange, especially in the region of the diaphysis, and thechanges are destructive, and not proliferative andreparative, as in gonorrhoea. In rheumatoid arthritisthere is distinct lipping of the articular surfaces, andalthough the joint space is diminished as in tuberculosis,the definition is usually better in non-tuberculous arth-ritis. When the activity of a tuberculous joint hasceased the definition becomes more distinct, but thearticular surfaces have a worm-eaten appearance.
COMPLEMENT-FIXATION TEST IN GONOCOCCAL ARTHRITISIn acute gonococcal arthritis the test gives a positive
reaction in a large number of the cases (75 per cent.), ifit is carried out later than ten days after the infection.In subacute and chronic cases in which the arthritis isgenerally later in appearing, the number of positiveresults is larger still, and is close on 8o per cent.A negative complement-fixation test does not exclude
gonorrhoea as the cause of the joint infection; a positivetest is strong confirmatory evidence of its oetiology. Thetest is of considerable value in obscure cases of jointinfection, in which the clinical findings in the genito-urinary tract are suggestive, but in which repeatedbacteriological tests have failed to show the gonococcus.If the fixation test, and at the same time cultural andbacteriological tests, are negative, it is the strongestpossible evidence that the joint condition is not due togonorrhoea.Thomson 33 found the test positive in twenty successive
cases of acute gonococcal arthritis, varying in durationfrom one to thirty days; in thirty-three chronic cases,of one to twelve months' duration or longer, 94 per cent.
9I- H 2
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
gave positive reactions. Wilson, Forbes and Schwartz 34found positive results in 47 per cent. of their acute cases, in73 per cent. of chronic cases, and in 6o per cent. ofdoubtful cases.
Horder,35 in reviewing the foregoing work, laysemphasis on the value of the test in chronic cases, becausein these " we are denied the advantages of direct bacterio-logical proof, the smaller percentage of positive resultsin acute and subacute cases is not such a material loss asmight at first be thought."
BesanSon, Weil and Rubinstein 36 found 87-5 per cent.of positive results. Fourteen cases of arthritis of non-gonococcal origin all gave negative results. There is, intheir opinion, no other type of arthritis which gives adefinite positive result, and hence the test, when positive,is of considerable assistance in cases of obscure aetiology.
In cases of undoubted gonorrhoeal arthritis, Thomasand Ivy 37 state that the test is simpler than a bacterio-logical examination, and gives more positive results.In acute cases IOO per cent. positives are found, and thereare no false positives in arthritis due to other conditions.Osmond,38 in a series of I,OOO tests, comprising 300 menand 700 women, considers that this test is at least asvaluable as the Wassermann test in syphilis. In un-doubted gonorrhoea he finds a high percentage of positives(86.5 per cent.), while false positives are extremely rare.Thomson's results are as follows:
Acute arthritis (I to 30 days) . ioO per cent. positive.Chronic arthritis (I to I2 months) 94Chronic rheumatism with no evi-
dence of gonorrhoea . . IOO ,, negative.Osmond stresses the value of the test as confirmatory
in diagnosis, and Thomson considers it a powerfuldiagnostic agent.
Cuti-Reaction.-An intradermal skin test on the prin-ciple of the Von Pirquet Test has been tried by Brewster 39in I,O0 cases ot gonorrhoea, including over IOO cases ofarthritis. The test was positive in over 8o per cent. of casesof gonorrhoea, and there were only o-6 per cent. of falsepositives. In gonococcal arthritis positive reactions wereobtained in 98 per cent. of the cases.Prognosis.-The prognosis in the first three groups of
gonococcal arthritis, (a) arthralgia, (b) acute and subacute92
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
GONOCOCCAL ARTHRITIS
synovitis, and (c) acute and subacute synovitis andarthritis, is invariably good, even if there is involvementof the periarticular structures, if treatment of the originalfocus of infection, and of the joint, is given on correctlines. In the fourth group, acute arthritis with suppura-tion, surgical interference is often required, and ther.may be considerable loss of function. Cases of subacuteor chronic hydrops react moderately well to treatment onthe same lines as the first three groups, but recovery isalways slow, and the joint condition is apt to recur.Cases of chronic osteoarthritis, in which adhesions havebeen allowed to develop, are very difficult to treat effec-tively. Although the joint condition can be madestationary, there is almost always some limitation ofmovement and loss of function.Luys 40 is rather pessimistic in stating that " acute
arthritis seldom ends by resolution. Its usual terminationis ankylosis." We have on record many cases which havecleared up completely without any evidence of ankylosis,while in this series of cases there was only one death, acase of gonococcal septicaemia complicated by kerato-dermia and an intercurrent pneumonia.
In the course of our work we have investigatednumerous cases of chronic infective arthritis because ofthese patients having given a history of previous gono-coccal infection. We have been impressed by the factthat the damage which may accrue to a joint from aprevious gonococcal infection which has not been cured,predisposes to the onset of rheumatoid arthritis in thejoint. In summing up prognosis, we can state that ifradiographic examination of the acutely infected jointshows no destruction of the articular surfaces, the prog-nosis is always good. If there are changes in the articularsurfaces, the prognosis for function must be guarded,although in many cases the patient can be assured ofhaving a useful joint with very little limitation of move-ment.
Treatment.-Whether the arthritis is due to the absorp-tion of toxins from the genital and urinary tract, as inarthralgia, and their transference to a joint, or to thespread of gonococci by the blood or lymph stream to thejoints, as in more severe cases, the rational treatment, oran essential part of it at least, must be to cut off the sourceof supply of toxins or organisms by treating the original
93
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
focus of infection in the genito-urinary canal and in thezones to which it may extend locally. Plisson 41 goes sofar as to state that the best preventative of gonococcalarthritis is the early and thorough treatment of theprimary infection. We are in complete agreement withthis statement, and it is noteworthy that, in 99 per cent.of all our cases, a joint complication had developedbefore the patient was treated or after ceasing treatmentbefore being cured. In only three cases did an arthritisdevelop in a case while under active treatment. Further,the infected joint must be treated locally, to relieve pain, toprevent the formation of adhesions, and to restore thelimb, and especially the joint, to its normal functionalactivity. In addition, in most of the joint cases we aredealing, as Horder 42 states, with a condition of pyaemia,and therefore specific treatment should be applied throughthe blood stream to influence the blood-borne infection.Lastly, the general condition of the patient must be treatedwith a view to raising the resistance to the infection.
There is great diversity of opinion as to the relativevalue of these methods, and still further diversity as tothe best methods of applying these four methods oftreatment:
(a) General.(b) To the original focus of infection.(c) To the infected joint.(d) Through the blood stream for the pyxemia or
septicaemia.(a) The General Condition of the Patient.-The most
important indication in acute arthritis is rest. At thesame time, the elimination of the toxins must be improvedby the administration of diuretics, by tepid sponging toinduce diaphoresis, by aperients, and by hot hip baths.Light nourishing diet with abundance of bland fluidsbetween meals is necessary to keep up nutrition. In acuteinfections of the female, Liquor Sedans 3i, and Tr. bella-donna minim v to x, is given thrice daily during eachmenstrual period to prevent a spread of the infection tothe upper genital tissues.Many drugs have been tried for the relief of the arthritic
pain. It is generally agreed that salicylates have littleeffect on the pain, although Bodenstab 43 stronglyadvocates their use and that of amidopyrin. In many of
94
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
GONOCOCCAL ARTHRITIS
our cases, novalgin was effective in giving relief frompain. In acute prostatitis and vesiculitis, suppositoriesof atropine and morphine are often indicated. In morechronic cases, iodides, syrup of iodide of iron, Frenchcodex iodine, and general tonics help to improve thegeneral condition.
(b) The Original Focus of Infection.-The earlier andthe more efficiently this is treated, the less likely is thedevelopment of any metastatic infection. If the infectionis confined to the anterior urethra, arthritis is rare, andthe aim in all cases of male infection is to confine it tothese limits. In female cases, if the infection, as a resultof early treatment, is confined to the urethra and thecervix, arthritis will be less prevalent.
In very acute cases of arthritis the treatment of theurethra may be difficult. Irrigation of the urethra andbladder with an antiseptic, such as potassium permanga-nate, is the best method in both sexes. Many other effi-cient antiseptics are available. If irrigation cannot becarried out, Styli of Citragan may be introduced into theurethra, as advocated by Kissmeyer.44
In female patients the Bartholinian gland and the cervixrequire local antiseptic treatment. In the former, theinjection of electrargol into the infected gland or duct,or complete excision of the gland, give good results; inthe latter, antiseptics, of which there is a large selection,should be applied to the cervix with dressed probes.
In cases of ophthalmia neonatorum, of vulvo-vaginitis,and of proctitis, local antiseptic treatment is alwaysrequired.When the infection in the genito-urinary canal is sub-
acute, other methods of eliminating the disease requireto be brought into use. The aim of these methods is thedrainage of the urinary canal and the associated zones ofinfection. In men, the focus of infection from which anarthritis emanates is often situated in the prostate glandand seminal vesicles. It is thus important to securedrainage from these areas by massage at intervals ofthree to five days. Massage of these tissues per rectumis of paramount importance in all cases of arthritis, andshould be practised as soon as the urethral infection hasbecome subacute. It lessens the pyaemic infection andhelps to eradicate the disease; if these areas are madefree from infection, recurrent attacks of arthritis do not
95
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
readily occur. At the same time, other areas of infection,such as Littre's glands, are treated by the careful applica-tion of such measures as suction and dilatation. If, inthe revolving stages of gonorrhoea, the infected areas inthe prostate and vesicles are slow in clearing up, thepassage of a large posterior sound or instillations of silvernitrate, I to 2 per cent., or of mercurochrome, I to 5 percent., into the posterior urethra or into the commonejaculatory duct, will often promote drainage and expe-dite recovery. In the subacute stages of infection in thefemale, instrumentation may also be required, such assuction of the urethra or cervix by Mills' negative pressurecatheters. A course of hot douching at a temperatureof I040 to II2° F., and the insertion of tampons bf 20 percent. ichthyol in glycerine, may be required in subacuteand chronic infections of the Fallopian tubes, or the pelviccellular tissues. A chronic infected Bartholinian glandshould be excised. In gross disease of the Fallopiantubes it may be necessary to remove the tubes after theacute condition has subsided.
OPERATIVE MEASURES DIRECTED TO STERILISINGTHE VESICLES
Vesicles.-We have drawn attention to the frequency ofinfection of the seminal vesicles in cases of arthritis inmen. This has led to the practice of applying antiseptictreatment direct to the infected vesicle through the vasdeferens in both acute and chronic cases. Vasotomy andsubsequent lavage of the vesicle with 20 C.C. of 5 per cent.collargol was introduced by Belfield 45 in I905, and hasbeen practised to a great extent chiefly by Americanworkers. In I920, Belfield 46 published a revised tech-nique of his operation. He bases the justification of thismethod of treatment on the physiology and histology ofthe seminal vesicles, and believes that it is the mostefficient method of sterilising the vesicles. Thomas 47advocates vasopuncture once only, and injection of5 per cent. collargol or 20 per cent. silver proteose as lesslikely to lead to permanent injury to the vas deferens.
Kidd,48 in I923, published the details of his operationof vasostomy, which differs slightly from that of Belfield.He recommends the temporary fixation of the vas to theskin surface for about seven days, to enable at least three
96
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
GONOCOCCAL ARTHRITIS
instillations of IO c.c. of 5 per cent. collosol silver to beintroduced in a period of one week. Wolbarst 49 recom-mends argyrol, 5 per cent., and also chlorazene solution,I in 200, as an instillation, and more recently, in I928,Belfield and Rolnick 50 have suggested for instillation asolution of aristol in cod liver oil (Io grms. of the formerin 30 c.c. of the latter, or goose oil).
These authors stress the excellent effect of this measurenot only on the infected vesicle, but on the concomitantarthritis. Wolbarst considers vasostomy the most de-pendable single measure for the relief of arthritis, andLowsley 51 states that it is an essential part of the treat-ment in association with autogenous vaccines. Kiddstates that all his cases were cured by vasostomy in threeweeks, and that the joint troubles disappeared rapidly.Wolbarst goes so far as to state that no case of arthritiscan be cured without this operation, an expression ofopinion with which we cannot agree. In our experience,vasotomy and vasostomy have not resulted in thespectacular cures claimed by those who advocate thisoperation; we have seen cases of arthritis on whom theoperation was performed by others without any appre-ciable improvement and certainly without cure.
In the acute and subacute cases in our series, practically98 per cent. were cured without any operative measures,and the affected joints were restored to good function.In chronic cases which are resistant to all other forms oftreatment there may be a field for vasostomy, if the vasis still patent, and if the vesicle is still infected. In ouropinion, those who advocate operation on the vesicle asthe main measure in the treatment of arthritis are apt toforget that in the greater number of these cases, andcertainly in acute cases, the gonococcal infection involvesthe prostate and possibly other zones of infection on whichvasostomy and instillation of antiseptics has no effect.
Other operations which have been practised are vesicu-lotomy and vesiculectomy. Drainage and excision of thevesicles were introduced in I9OI by Fuller. Thomas 52recommends vesiculotomy or drainage in cases of suppura-tion of the vesicle and in cases of perivesiculitis; on theother hand, L. L. Michel 53 states that he has not obtainedfavourable results from the operation, and A. H. Frei-berg 54 is emphatic that operation on the vesicles alonecannot possibly cure an infected joint. Thomas recom-
% 97
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
mends vesiculectomy in cases of perivesiculitis. Cunning-ham,55 and also Greenberg,56 claimed good results fromthis operation. In chronic cases, Cunningham considersthat vesiculectomy gives striking results in the relief ofpain, and in the reduction of articular, and especially ofperiarticular, swelling.
In our experience there are few, if any, cases of acutearthritis in which such a severe and difficult operation isnecessary. In chronic cases the operation cannot beexpected to clear up destructive lesions in the joint andcartilage. These operations should be reserved for casesin which every other form of therapy has been tried andfound ineffective.
Stellwagon and McCahey 57 inject 3 c.c. of Pregl'ssolution directly into the vesicle through the rectal wall.This is an aqueous isotonic solution of the sodium salt ofhydriodic acid and iodic acid with metallic iodine (0.04 percent.); after three to four injections into the vesicle theseauthors claim that in fourteen cases of acute vesiculitisthe arthritis was cured. This operation may favourablyinfluence the acute vesiculitis, but there is always a greatrisk of introducing a secondary infection into the punc-tured vesicle and a gonococcal infection to the rectum.Further, it is not rational to expect that a focus ofinfection in the joint will automatically subside as aresult of antiseptic treatment applied only to the contentsof the vesicle.Townsend 58 has reported favourable results from the
intraprostatic injection of what he terms " a normalphenol serum," in prostatitis and vesiculitis. Thismethod was tried in Franks' clinic in Berlin and discardedas valueless.
In three of our subacute cases vasostomy was per-formed, and instillations of collargol were made into thevesicle, but failed to effect a cure of the arthritis or thegonorrheea. We have also had under our care casesoperated on by others with moderate results.
(c) Methods of Treatment of the Affected Joint.-Theaim of local treatment to the joint is to relieve pain andbring about resolution of the synovial or periarticularswelling. Rest and immobilisation of the affected jointhelp to r.elieve pain; a light poroplastic splint or sand-bags will immobilise the lower limb; a sling is usuallyeffective in the case of the upper limb. Sedative applica-
98
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
GONOCOCCAL ARTHRITIS
tions should be applied to the joint, such as lead andopium, 20 per cent. ichthyol in glycerine, glycerine andbelladonna, antiphlogistine, or similar applications.
In subacute and chronic cases rest is not required tothe same extent, and local applications should be morestimulating. An ointment incorporating iodine, thymoland ichthyol, or one containing gr. 40 of acid salicylic inunguentum capsici, i oz., is a very effective counter-irritant to the infected joint. lodex or tincture of iodinemay be used, although the latter is apt to injure the skinsurface if applied continuously.
In the declining stages of an acute infection, and inchronic cases, the application of Ungt. Hydrarg Co.(Scott's dressing) is a mild stimulant, and assists vascu-larisation. Bier's passive hyperaemia can be applied in allacute and chronic cases, and is very valuable. It does notinterfere with other local treatment. It relieves painand assists in the absorption of inflammatory products.Baetzner 59 strongly advocates Bier's engorgement treat-ment daily for twenty-two hours with the limb elevated.He emphasises the need for keeping the limb red andhot, and not pale. Hot-air baths, ionisation, and otherphysio-therapeutic methods are helpful in relieving pain,but do not give any greater relief from pain than can beattained by simpler methods.
In dealing with all acute cases, with the exceptionpossibly of a pyarthrosis, and in subacute and chroniccases, the early institution of passive and voluntarymovement and massage of the affected joint, and of themuscles acting on it, are measures of paramount import-ance if the best functional results are to be obtained.Movement and massage must be practised as soon as theacute pain is relieved. This is the most effective way ofavoiding permanent joint disability, and does so in ourexperience, except in those cases which on X-ray examina-tion show signs of cartilaginous or osseous damage. Itprevents adhesions being formed from the serofibrinousexudate, and must always be an integral part of anymethod of treatment. In the literature on this aspect oftreatment, Collins 60 is almost the only advocate of morecomplete and longer immobilisation of the joint. Heapplies a plaster case to the joint for at least two weeks.It is then removed to permit of massage and passivemovement, and is reapplied for a further period of two
99
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
weeks. This method will certainly eliminate pain, butundoubtedly the risk of ankylosis is too great for it to berecommended.Diathermy.-Cumberbatch 61 introduced this method
of treatment of arthritis in I9I3, and with Robinson hehas reported very favourable results in gonococcalarthritis. They advise the application of the " highfrequency" alternating electric current to the infectedprostate and seminal vesicles at the same time. Thiscurrent produces deep-seated heat without leading toany chemical change in the tissues, or to nerve or musclestimulation. It is thus more valuable than the con-tinuous electric current. Further, the heat to which thetissues can be raised, II2° to II4° F., is stated to belethal for gonococci. Certainly, in vitro, gonococci areeither devitalised or destroyed by a temperature ofI02° to I05° F. Pelouze 62iS doubtful if the heat producedby diathermy to II2° F. will destroy the gonococcus invivo.Cumberbatch and Robinson's methods, published in
I923, appeared to be a very definite advance in thetherapy of gonococcal arthritis. In this country, veryfew further reports have been published in confirmationof their claims except by these same workers. VanPutte 63 reported good results in a few cases of chronicgonorrhoea. Acute cases, in his experience, did notrespond well to the treatment. Kovacs 64 found dia-thermy most effective in subacute and chronic cases.
In our experience over a period of six years, diathermy,when applied to the joints only, is not a cure. Diathermyto the focus of infection alone is no more successful.Diathermy applied to the joints, and also to the focusof infection in the prostate and vesicles, or in the cervix,is helpful. It relieves pain, reduces the swelling, andassists in vascularising the part. The temperature towhich the tissues are raised may devitalise the gono-coccus, but does not always eradicate it from the prostateand vesicles. Cell metabolism may be stimulated, andthe tissue resistance to the gonococcus may be increased.In estimating its value as compared with other methodswhich are more within the compass of the work of mostpractitioners, we are not convinced that it is very muchsuperior to the local application of heat to the joint, byantiphlogistine, and to hot rectal irrigations in acute
IOO
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
GONOCOCCAL ARTHRITIS
prostatic and vesicular infection. In subacute and chroniccases it cannot replace massage of the prostate andvesicles; it does not enable us to dispense with voluntaryand passive movements in restoring the joints to fullfunction. In addition, it rarely exercises any favourableeffect on the infection of the urethral canal, and unlessother local treatment is administered at the same timethere is always the definite possibility of a recurrence ofthe infection in the prostate and vesicles, or even in thejoints.Diathermy is a useful adjuvant form of treatment,
but by itself it is not a complete cure of either the pro-static and vesicular infection or the joint infection. Wecannot agree with the claim of Cumberbatch that " theresults of treatment by diathermy are far superior tothose obtained by any other method."Coyon and Gagey 65 treated five cases of arthritis by
radium to the joint. They claimed almost immediaterelief from pain, and very rapid improvement in acutecases. It is not, in their experience, efficacious afterankylosis has occurred. They recommend early mobilisa-tion at the same time. We have had no experience ofthis method.
OPERATIVE TREATMENT OF GONOCOCCAL ARTHRITISIn acute cases, aspiration of the affected joint, aspira-
tion followed by irrigation with antiseptics, and arthro-tomy followed by joint irrigation and drainage, have allbeen advocated and practised. In I899, O'Conor 66reported good results in ten cases treated by arthrotomy,irrigation and drainage. Klose 67 also favours this methodin selected cases, and especially if signs of subluxation arepresent, or if the joint condition does not show signs ofimprovement with three weeks conservative treatment.Harrison 68 and others state that aspiration of theacutely inflamed joint gives good results in the relief ofpain. Knauer 69 reports two cases of joints in whichcure was attained by aspiration only. Barzy 70 discussesthe merits of surgical treatment, suture without drainageand early mobilisation, and the advantages of intra-muscular injections of serum. The latter method heconsiders more satisfactory, but in some articulations,such as the wrist, and especially if the tendon sheaths are
IOI
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
involved, it may fail. In cases in which serum treatmentfails he advises emptying the joint of its contents. Jointpuncture, together with lavage and injections of I in 5,oooVuzin solution, is favoured by Mobitz,71 who obtainedexcellent results in the ten cases in which he used thismethod. Dufour, Thiers, and Alexewsky 72 claim mostfavourable results from aspiration of the infected joint,and reinjection of I0 to 20 c.c. of the aspirated fluid intothe subcutaneous tissues of the thigh. It is immaterial,they state, whether the fluid is serous or purulent, andthey claim that this method influences the original focusof infection favourably. Ballenger and Elder 73 reportedsuccessful results in twenty-seven cases of gonococcalarthritis by aspirating I5 to 20 C.C. of synovial fluid andreinjecting it into the gluteal muscles at two-day intervalswithout any other adjuvant treatment. Churchman 74aspirates the joint and washes it out in turn with salinesolution, hydrogen peroxide, and saline solution again.He then instils a solution of i in I,000 gentian violet intothe joint cavity and allows it to act for five minutes. Thisis reaspirated from the joint and a fresh supply of i inI0,000 gentian violet is injected and left in the jointcavity. Walther 75 also advocates joint puncture andlavage of the cavity in acute cases. Freiberg 76 considersthat the main site of the infection is the synovial mem-brane. He opens the joint by a small incision, flushes itout well with sterile water at a temperature of II5° F.,to kill the organisms, and closes the joint without drainage.*Plisson 77 also states that the best method of treating anacute joint is puncture or incision, followed by washingand closure of the joint. Antigonococcal serum dilutedwith physiological serum to I0 or 20 per cent. is thengiven by intra-articular injection. According to Klapp,78the best treatment is the periarticular or intra-articularinjection of Rivanol in a strength of i in I,000. No otherantiseptic, he considers, can be compared to it in itseffect on pyogenic and gonococcal arthritis. Ramond,Janet and Levy 79 tap the cavity, fill it with filtered air,and then inject 5 to io c.c. of iodised oil. They alsoadvocate using a 20 per cent. solution of sodium citrateto wash out the joint after aspiration. Lavage of thejoint with 2 per cent. formaldehyde and glycerine isrecommended by Walther,80 and we have found thisefficient in the few cases of pyarthrosis in our series.
I02
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
GONOCOCCAL ARTHRITIS
Mondor, 81' on the other hand, states that surgical interven-tion, especially incision of the joint, is uncertain as a cure,and may be followed by progressive ankylosis and jointdestruction. The only thing in its favour is, he states, theimmediate relief from pain and an improvement in thepatient's general condition, especially if there is evidenceof progressive destruction of the articular cartilages.
In our series only seven cases (I.3 per cent.) wereoperated on by arthrotomy and joint lavage. In thesecases there was a definite purulent arthritis, inwhich operation was necessary to stop the destructiveaction on tlre cartilages, and for the general condition ofthe patient. In all the other acute cases conservativemeasures were employed, such as temporary immo-bilisation, Biers congestion, local applications of anti-phlogistine, diathermy, hot-air baths, and other localmeasures. While these measures may not give asimmediate relief fro'm pain as arthrotomy or joint punc-ture, the end results are as good, if not better, than thosereported after many of the operative measures previouslymentioned, and the patient is not exposed to the risk ofa serous synovitis becoming a purulent arthritis throughthe entry of other organisms into the joint structures.In chronic cases of gonococcal arthritis the pain is rarelyso severe, and local applications of a stimulating characterare almost always indicated. In conjunction with thesemeasures we have used hot-air baths, diathermy, andcounter-irritants to stimulate an active hyperaemia. Biers'passive congestion is indicated in chronic cases, andhastens the absorption of inflammatory exudates.Massage and active movement are of considerable valuein restoring the limb to normal function. If there ismarked loss of mobility and the joint is in bad position,the joint should be examined by X-ray, and if the radio-graphic picture justifies the procedure, it is mobilisedunder general anmesthesia. If there is ankylosis, arth-rectomy may be required, particularly in the case of theknee joint. In all chronic cases we are convinced of theneed for the co-operation of an orthopaedic surgeon sothat the best functional results may be obtained. Incases of hydrops, aspiration of the joint will temporarilyrelieve the disability, but, in our experience, the jointcavity fills up again, unless the focus of infection in thegenitals is dealt with satisfactorily.
I03
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
(d) Specific Therapy through the Blood Stream.(i) Vaccines and Sera.-The literature on this aspect oftreatment is enormous, and in a review of sixty-eightarticles, Thomson82 states that sixty-six of these authorsgave favourable reports, while only two failed to find anybenefit from vaccines in gonococcal arthritis. The majo-rity of observers are thus of opinion that it is a valuabletherapeutic measure and a necessary part of the successfultreatment of gonococcal arthritis. Different types ofvaccine were administered in practically all our cases,and with excellent results. Many have advocated theuse of sensitised vaccines, that is, a vaccine which hasbeen subjected to treatment with its appropriate anti-serum during its preparation. The first stage of theimmunisation is thus performed in vitro, the vaccine isless toxic, and consequently a larger dose can be given.Cruveilhier,83 Broughton-Alcock,84 Haworth,85 andDopter and Pauron 86 all state that the administrationof sensitised vaccines alleviates pain quickly, and leadsto subsidence of the swelling. The initial dose which theseworkers used varied from IOO million gonococci byHaworth to 500 millions by Broughton-Alcock. Wewere able to observe several of Haworth's cases, and theresults (sixteen cures in seventeen cases of acute andsubacute arthritis) were extremely good. We have notused sensitised vaccines in any of the cases in thisseries.
In I9I9 Thomson 87 published his work on the separa-tion of gonococci from their toxins, and in I9I9 Thomsonand the writer 88 published the results obtained in thetreatment of cases of gonorrhoea and its complicationswith detoxicated vaccines.
This type of vaccine makes it possible to give a muchlarger dose of antigen, without giving rise to a severegeneral or focal reaction. In this way a larger output ofantibody by the patient is stimulated and is obtained.Considerable controversy was aroused by this work, andthe objection was raised that antibody and antisubstancescould not be produced by a non-toxic substance; further,the removal of toxins was said to be unsound, because,when injected, they have antigenic power and tend tostimulate antitoxin production and the conditions neces-sary for the formation of antibody.Without entering into these arguments, we have no
I04
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from

GONOCOCCAL ARTHRITIS
hesitation in stating that in the treatment of arthritis,detoxicated gonococcal vaccine has given consistentlygood results and has proved an invaluable adjuvant in theacute and subacute cases in which it has been administeredin this series. We have used it in over 250 cases, eitheralone or in combination with an autogenous vaccine, andcan state that it assists materially in the relief of painand swelling, in cutting short the disease, and in lesseningthe liability to complications.The initial dose varies with the patient's condition, and
should be from 2,000 to 5,ooo million gonococci; wehave increased the dose progressively up to Ioo,ooomillions in some cases. There is, in our experience, nomaterial advantage in giving the vaccine intravenouslyas compared with the simpler method of intramuscularor subcutaneous injection. This is at variance with thefindings of Fraser and Duncan,89 who gave a stock poly-valent vaccine up to 2,000 million organisms intra-venously; in their view, if no pyrexia followed itsadministration, no benefit seemed to accrue. We havecompared the results obtained with ordinary polyvalentvaccines, and are satisfied that the detoxicated vaccinehas many advantages, the chief of these being the morerapid effect on the original focus of infection, the quickerrelief from pain, the more rapid resolution of the joint,the absence of any negative phase, and the feeling ofwell-being which the patient often appreciates withintwenty-four hours after the injection. Sieur 90 reportsthat Costa, in close on I00 cases of acute gonococcalarthritis, obtained most favourable results in the reliefof pain and return of function in all cases by using apolyvalent vaccine prepared with formaldehyde. Lian,Poincloux and Copelovici-Cope 91 also report most success-ful results and complete return of function in all theiracute cases treated by vaccines. Similar results are quotedby Vallino and Macera 92 in cases of arthritis compli-cating vulvovaginitis. Sezary 93 considers vaccine therapyefficacious to a degree, and states that the dosage must beeffective, 6o,ooo to 8o,ooo million organisms in four or fiveinjections. He employed a lipovaccine with excellentresults. Michel 94 states that while occasional brilliantresults are obtained by vaccines, they were on the wholedisappointing. He believes that he gets better resultsfrom them by intravenous administration, due possibly
V.D. I05 I
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
to their action as a protein when administered by thisroute. He prefers non-specific proteins.
In over forty of our cases we tried the effect of " Arth-rigon," a polyvalent gonococcal vaccine containingurotropin. This method was first used by Rohrbach 95and Dorn.96 Bruck 97 was of opinion that it was superiorto any other form of vaccine, and could replace an auto-genous vaccine. Bardach,98 Martin Fischer,99 Freund',00and Pritzi 101 all report excellent results from its use inacute arthritis. On the other hand, Hagen 102 was notimpressed with the results of arthrigon and Roth,Klinger and Oppenheim103 state that it failed to influencegonococcal arthritis favourably. Complications duringtreatment occurred frequently in the cases treated witharthrigon by Habermann,104 who is not impressed withthe results. In thirty-three acute cases in this series whichwere treated with intravenous injections of arthrigon, wenoted an immediate and progressive improvement in thejoint condition, and also in the primary focus of infection.Eight chronic cases did not respond so quickly, butthere was a definite improvement in all of them, andin two cases of hydrops, the joint infection was curedby this method in combination with treatment of thelocal and focal infection. " Arthrigon," in our opinion,gives very good results in cases of acute and subacutearthritis.Another preparation which we have used is Gono-
Yatren, a suspension of polyvalent gonococci in a 3 percent. yatren solution. Like arthrigon, it gives a specificand non-specific reaction. Four acute cases reactedfavourably to Gono-Yatren, and at the same time therewas a marked improvement in the genito-urinary infec-tion. We tried the effect of gonococcal phylacogen in anearlier series of cases, and came to the same conclusionsas were reported by Harrison,105 that while in large dosesa phylacogen may give rapid relief to the pain of anarthritis, this preparation does not exercise any beneficialinfluence on the genito-urinary infection. The resultswere, i1i our opinion, largely dependent on the amountof protein shock produced by each injection.Serum treatment by antigonococcal serum has been
employed in the treatment of gonococcal arthritis withvarying results. Thomson, 103 reviewing fifty contribu-tions on this subject, found that forty-three authors
io6
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
GONOCOCCAL ARTHRITIS
considered it of some therapeutic value. It was firstused by Torrey.107 Rodgers and Torrey108 reported curesor marked improvement in 78 per cent. of acute cases.Porter,109 Louis,110 and Steelwagen 111 obtained goodresults with serum treatment, and Ballenger 112 had72 per cent. of cures in ninety cases. On the other hand,Fletcher,113 and also Briick,114 considered it a failure.Herbst 115 and Thomas 116 formed the opinion that it wasonly of value in chronic cases. Debre and Paraf 117consider that it is necessary to bring the antiserum incontact with the organism and inject it into the infectedjoint cavity after aspiration. They supplement this byintramuscular or intravenous injections of the antiserum,and reported very good results in fourteen out of fifteencases.We have not used gonococcal antiserum in any of our
cases. It has definite disadvantages as a method oftreatment in that it may produce an anaphylaxis at somefuture date if other antisera, e.g., antidiphtheritic, requireto be given. In addition, general serum reactions, urti-carial eruptions, and pain at the site of the injection arereported by several workers. Langeron and Bocca,"18although admitting that it relieves the joint pain andprevents septicaemia, state that it has no influence on theurethritis.Good results have been reported from the administra-
tion of non-specific sera by Soltau, Fenwick and Parkin-son."19 Fox120 and also Salter 121 recommend rectalinjections of IO c.c. antistreptococcal serum.
Antimeningococcal serum is favourably reported on byMalleterre 122 and by Chiari,'23 who in reviewing theliterature found thirteen cases reported cured out ofsixteen treated by this method.
Auto-serotherapy by aspirating fluid from the joint andre-injecting it subcutaneously near the articulation isfavourably commented on by Ramond,124 while Ballengerand Elder 125 strongly advocate its use and do not employany other local or general treatment. They state that theaspirated fluid must be turbid if it is to be effective,and they inject it intramuscularly into the buttock.Thomas,126 on the other hand, states that he has neverfound this method of any assistance.
Protein Therapy.-The resistance of the individual tomany infections can be increased by the administration
I07 1 2
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
of foreign proteins, and the pyrexia so produced is possiblythe chief factor in its action.Many proteins have been used in gonococcal arthritis,
such as horse serum, peptone, sterile milk, T.A.B. vaccine,and antidiphtheritic serum. Rodriguez 127 treated morethan I00 cases by antidiphtheritic serum with excellentresults.
In a number of our chronic cases, and in subacute casesnot responding to vaccine treatment, we have found thatthe production of a mild protein shock by the intra-muscular injection of 5 c.c. of sterile milk is often ofconsiderable value, if interspersed between successivedoses of vaccine.
In some of the most chronic cases, injections of peptonehave been even more successful, as it produces a greaterdegree of protein shock. The initial treatment by proteinshock, followed by vaccine treatment, is followed by quitefavourable results in many chronic cases. We have triedthe effect of repeated injections of milk in acute cases,and have not been impressed with the results.
Chemotherapeutic and Other Injections. A very largenumber of these substances have been recommended inarthritis, either alone or to supplement vaccine treatment.
Intramine and contramine are advocated by Mc-Donagh 128 in acute and chronic cases, prior to and laterin conjunction with vaccines. Young 129 and othersstate that they have obtained good results from theintravenous administration of Mercurochrome 220. Wehave tried this method in three cases and agree with theobservations of Brash and Bumpus,130 who consider it istoo toxic a preparation for routine administration. Inaddition, it did not in our cases cure the gonococcalinfection. Another chemo-therapeutic substance whichhas been tried in infective cases of arthritis and ingonococcal arthritis is ortho-iodoxybenzoic acid. Youngand Youmans 131 state that in hopeless cripples theyobtained marked improvement in 56 per cent. of cases,some of whose joint conditions were gonococcal in origin.Millard Smith 132 states that any arthritis giving rise topain, swelling and muscular spasm will benefit from theintravenous injection of this substance.We used this preparation in two cases of gonococcal,
and in one case of chronic infective arthritis, with noappreciable improvement. It was administered in doses
io8
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
GONOCOCCAL ARTHRITIS
of o-6 to o9 gm. dissolved in IOO c.c. of sterile salinesolution, and was given very slowly. It was apt to causevenous thrombosis, and the reactions were very severe;the patients were upset to such an extent that we decidedto discontinue the use of this drug. Stein and Traube 133had a similar experience, and found it valueless ingonococcal cases. The organic arsenical compounds havebeen tried in the treatment of gonococcal arthritis, andLamblin 134 considers that subcutaneous injections ofsulpharsenol are easily applied and are well tolerated.The patient's general condition and the pain improverapidly, and early mobilisation is possible. Girard andTrigher 135 are also impressed with its rapidity of actionin arthritis, while Duroeux, Tant and Bernard 136 statethat " at the present moment, arsenical treatment con-stitutes a veritable specific for the inflammatory complica-tions of gonorrhcwa. This treatment has very little effecton the concomitant urethritis. We have not usedsulpharsenol in arthritis per se, but have noted that incases of syphilis under arsenical treatment, who sufferedin addition from gonococcal arthritis, the response totreatment by vaccines has been particularly good.
In three cases of very severe polyarthritis with ageneral septicaemia and extensive keratodermia, we havefound that minute intravenous injections of neo-kharsivano0O25 to o o5 gm., administered every second or third day,have appeared to increase the patient's defensive mecha-nism and helped very materially to combat the septicaemiaprior to administering a course of vaccine therapy.
REFERENCES TO LITERATURE
(I) MARTINIE'RE: Traite de la Maladie Venerienne, I664.(2) SALLE, T., and SWEDIAUR: Quoted by A. Thomas, J.A.M.A.,
p. 2I74, December 24th, I927.(3) BRODIE, B. : "Pathology and Surgery," ist Edition., i8i8,
quoted by Brodie, M. W., Practit., 88, p. 34, I9I2.(4) NEISSER, A.: Centralblat F. d. Med. Wissenschaft., XVII, 497,
I879.(5) LAWRENCE, W.: Quoted by McDonagh, " Venereal Diseases,"
p. 3I3, I920.(6) PETRONE: Rev. Clin. di Bolivia, I883.(7) HEWES: Med. and Surg. Jour., Boston, I894.(8) OSLER, W.: " Principles and Practice of Medicine," gth Edition,
p. I27, I920.(9) LUMB, N. P.: " Gonococcal Infection in the Male," p. I5I (Bale,
Sons & Danielson), I920.IO9
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
(io) KLOSE, H.: Berlin Klin. Woch., Vol. XVI., 42, p. 983, I9I9.(II) IRELAND: Quoted by A. Thomas, J.A.M.A., p. 2I74, Decem-
ber 24th, 1927.(12) CHIARI: Centralbl.f. Grenzgeb. d. med. u. chir. Jena, p. 445, I9I4.(I3) HARRISON and POLLOCK: Quoted by A. Thomas, J.A.M.A.,
p. 2I74, December 24th, 1927.(I4) THOMAS, A.: J.A.M.A., p. 2I74, December 24th, I927.(15) THAYER and BLUMER: Arch. de Med. Exper. et d'anat. path.,
Paris, November, I895; also Johns Hopkins Hosp. Bull.,Vol. VII., p. 57, I896.
(i6) UYSING: Inaug. Dissert. Kiel, I908; quoted by Hunter,Brit. Med. Jour., March iIth, I905.
(I7) ZIELER, K.: Mediz. Klinik., February iith, I9I2.(i8) LOFARO, F.: II Polyklinic, February, I9II.(i9) Quoted by Cole, " Osler's Modem Medicine," Vol. III, p. I03,
I907.(20) NASSE and RINDFLEISCH: Arch. f. Klin. Chir. u. Samml. Klin.
Vortrage, I897.(2i) BAUR: Deut. Med. Woch. Vereinsber., p. 6o, I90I.(22) THOMSON, D.: " Gonorrhoea" (Oxf. Med. Publ.), p. 224, I923.(23) McDoNAGH, J. E. R.: "Venereal Diseases," p. 3I3, I920.(24) MICHEL, L. L.: New York Med. Jour., p. II24, June 28th, I9I9.(25) LuCAS, C.: Lancet, p. 250, January 28th, I899.(26) JOHNSTONE: Amer. Jour. Dis. of Children, February, I92I.(27) FISCHER, M.: Monatschr. f. Kinder. Leipsig. 29, October ioth,
I924.(28) PRITZI: Wien. Klin. Woch., 37, I3I2, December i8th, I924.(29) HERZFELD, G.: Trans. Med. Chir. Soc. Edin., January 2ISt,
I925; Brit. Med. Jour., p. 365, February 2ISt, I925.(30) NORTHUP: Quoted by Young, " Manual of Orthopaedic
Surgery," p. 529, Philadelphia, I905.(31) LUMB, N. P.: " Gonococcal Infection in the Male," p. I5I
(Bale, Sons & Danielson, London), I920.(32) YOUNG, H. H.: Johns Hopkins Hosp. Reports, Vol. IX., p 677.(33) THOMSON, D.: "Gonorrhoea " (Oxf. Med. Publ.), pp. 295 et seq.,
I923.(34) WILSON, FORBES and SCHWARTZ: Jour. ofImmunology, Vol.111,
No. 2, March, I923.(35) HORDER, T.: Lancet, p. I304, June 30th, I923.(36) BESANSON, WEIL and RUBENSTEIN: C. R. Soc. de Biologie,
p. 235, July 3rd, I925.(37) THOMAS and Ivy: Arch. of Int. Med. Chicago, Vol. 13, No. I,
January, I9I4.(38) OSMOND, T. E.: Lancet, p. I304, June 30th, 1923.(39) BREWSTER, G.: M. D. Thesis. Edin. Univ., 1927.(40) Luys: " Gonorrhoea," 2nd Edition (trans. by Foerster), I9I7.(4I) PLISSON, L.: Le Progryes Med., p. I543, October Ist, I927.(42) HORDER, T.: Lancet, pp. 1304, I3I3, June 30th, I925; Lancet,
p. i8, July 7th, 1923.(43) BODENSTAB, R.: Deutsch. Arch. F. Klin. Med., .159, I29-256,
March, I928.(44) KISSMEYER, Brit. Jour. of Ven. Dis., Vol. IV., p. I99, I928.
IIO
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
GONOCOCCAL ARTHRITIS
(45) BELFIELD, W. T.: J.A.M.A., XLIV., p. I277, I905; LIX.,p. I4I9, I9I2; LXI., p. I867, I9I3; Surg. Gyn. Obst., m.,p. 656, I906; XVI., p. 569, I9I3.
(46) BELFIELD, W. T.: J.A.M.A., LXXIV., p. I48, I920; LXXVI.,p. I290, I922.
(47) THOMAS, A.: Surg. Gyn. Obst., XXIV., p. 68, I9I7.(48) KIDD, F.: Lancet, p. 2I3, August 4th, I923.(49) WOLBARST, A. L.: " Gonococcal Infection in the Male," 2nd
Edition, p. 232 (H. Kimpton, London), I930.(5o) BELFIELD and ROLNICK: Quoted by Wolbarst, ibid., p. 234.(5i) LOWSLEY: New York Med. Jour., May 4th, I92I.(52) THOMAS, A.: Surg. Gyn. Obst., XXV., p. 68, II7.(53) MICHEL, L.: New York Med. Jour., June 28th, p. II24, II9.(54) FREIBERG, A. H.: J.A.M.A., Vol. 89, No. 26, p. 2I77, Decem-
ber 24th, I927.(55) CUNNINGHAM, J. H.: Surg. Gyn. Obst., XXXJI., No. 6, p. 50I,
June, I92I.(56) GREENBERG, G.: Med. Jour. and Record, 76, July 2ISt, I927.(57) STELLWAGON, T. C., and MCCAHEY, J. F.: Jour. of Urol., 18,
P. I, July, I927.(58) TOWNSEND, T. M.: Trans. Amer. Urolog. Assoc., I9I7.(59) BAETZNER: Med. Welt. Berlin, IV., 250, Berlin, I930.(6o) COLLINS, C. W.: J.A.M.A., p. I789, December 3rd, I92I.(6I) CUMBERBATCH and ROBINSON: "Treatment of Gonococcal
Infections by Diathermy ' (Heinemann), 1925.(62) PELOUZE, P. S.: "Gonococcal Urethritis," p. i6o (W. B.
Saunders), I928.(63) VAN PUTTEE, F. J.: Acta Derm.-Ven., Stockholm, 7, p. 358,
June, I926.(64) KOVACS, R.: J.A.M.A., Vol. 89, No. 24, p. 2I77, December 24th,
I927.(65) COYON, A., and GAGEY, J.: Bullet. Soc. de Therap., Mar. I2th,
I924.(66) O'CONOR, J.: Lancet, p. I585, December gth, I899.(67) KLOSE, H.: Berlin Klin. Woch., October 20th, IgIg.(68) HARRISON, L. W.: "Manual of Venereal Diseases," p. 260,
I920.(69) KNAUER: Lancet, p. I262, June I3th, I925.(70) BARZY: Bullet. et Me'm. Soc. Chir. de Paris, p. 888, June 27th,
I922.(7I) MOBITZ, W.: Munch. Med. Wochnschr., 67, pp. 843-844, I920.(72) DUFOUR, THIERS, and ALEXEWSKY: Jour. de Mid. et de Chir.
Prat., February ioth, I922.(73) BALLENGER and ELDER: Surg. Gyn. Obst., XXXIII., p. 574,
November, I92I.(74) CHURCHMAN, I. W.: J.A.M.A., p. I047, April I3th, I9I8;
p. 583, August 28th, I920.(75) WALTHER, H. WV. E.: Boston Med. and Surg. Jour., Vol. 170,
No. I5, I9I4-(76) FREIBERG, A. H.: J.A.M.A., p. 2I77, December 24th, I927.(77) PLISSON, L. : Le Progres Med., p. I543, October Ist, I927.(78) KLAPP: Quoted by Axhausen, Klin. Woch., No. i6, I927.
III
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
BRITISH JOURNAL OF VENEREAL DISEASES
(79) RAMOND, F., JANET, and LEVY, M.: Bull. et. Mem. Soc. Med. d.H6p. de Paris, 39, 200, February I5th, I923.
(8o) WALTHER, H. W. E.: Loc. cit.(8i) MONDOR, H. : Les Arthrites Gonococciques (Masson et Cie., Paris),
I928.(82) THOMSON, D.: " Gonorrhoea" (Oxf. Med. Publ.), p. 328, I923.(83) CRUVEILHIER, L.: Lancet, Vol. II., p. I3I, November 8th,
I9I0.(84) BROUGHTON-ALCOCK, W.: Comptes rend, des Sciences de la
Soc. Biol., Vol. 74, p. 623, I9I3.(85) HAWORTH, H. D.: Brit. Med. Jour., Vol. 1, p. 4, January 5th,
I9I8.(86) DOPTER and PAURON: Brit. Med. Jour., Vol. II., p. I609, I9I3.(87) THOMSON, D.: Lancet, 1, p. II02,I9I9; Science and Progress,
Vol. 14, No. 54, p. 326, I919; "Gonorrhoea " (Oxf. Med.Publ.), p. 335, I923.
(88) LEES, D.: Lancet, 1, p. II07, I919; Edin. Med. Jour., August,I9I9.
(89) FRASER, A. R., and DUNCAN, A. G. B.: Lancet, p. 248, January3ISt, I920.
(90) SIEUR: Bull. et Mem. Soc. de Chirug. de Paris, October 25th,I92I.
(9I) LIAN, C., POINCLOUX, P., and COPELOVICI-COPE, M.: Gaz. desHospitaux, p. io86, July 27th, I929.
(92) VALLINO, M. T., and MACERO, J. M.: Semana Medica, BuenosAires, 36, p. I64, January I7th, 1929.
(93) SEZARY, A.: Compt. rend. Soc. de Biol., Paris, 82, p. III,I9I9.
(94) MICHEL, L.: New York Med. Jour., June 28th, I929.(95) ROHRBACH, E.: Dermat. Zeitschr., Vol. XIX., I9I2.(96) DORN, F.: Dermat. Woch., Vol. 54, I9I2.(97) BRUCK, C.: Kolle Wassermann, Vol. IV., I9I2.(98) BARDACH, K.: Munch. Med. Woch., No. 47, I9I3.(99) MARTIN FISCHER: Monatschr. f. Kinder. Leipsig, 29, 10,
October ioth, I924.(IOO) FREUND, W. P.: Wien. Med. Woch., No. 25, I9I3.(IOI) PRITZI, 0.: Wien. Klin. Woch., 37, I3I2, December i8th, I924.(IO2) HAGEN, F.: Med. Klin. Berlin, Vol. 8, No. 7, I9I2.(I03) ROTH, KLINGER and OPPENHEIM: Quoted by D. Thomson,
" Gonorrhoea," p. 3I5, I923.(104) HABERMANN: Munch. Med. Woch., February 24th and
March 3rd, I9I4.(I05) HARRISON, L. W.: Lancet, Vol. II., p. I375, I9I3.(io6) THOMSON, D.: " Gonorrhoea" (Oxf. Med. Publ.), p. 352, I923.(I07) TORREY, J. C.: J.A.M.A., p. 26I, January 27th, I906;
Med. Record, New York, October 26th, I907.(IO8) TORREY, J. C., and RODGERS: J.A.M.A., Vol. 49, p. 9I8, I907.(I09) PORTER, F. J. W.: Lancet, Vol. II., p. I479, I907.(IIo) LouIs: Trans. Lond. Med. Soc., March I5th, I9IO.(III) STEELWAGEN, T. C.: Therapeutic Gazette, Detroit, April,
I9I0.(II2) BALLENGER, S. C.: New York Med. Jour., I909.
II2
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from
GONOCOCCAL ARTHRITIS
(I13) FLETCHER, L.: Wisconsin Med. Jour., reference Monatschr f.Dermat., No. I, I91I.
(II4) BRUCK, C.: Deutsch. Med. Woch., Vol. 35, P. 470, I909; KolleWassermann, 2nd Edition, Vol. IV., PP. 72I-736, I9I2.
(II5) HERBST, R. H.: J.A.M.A., p. I678, May, I9O8; IllinoisMed. Jour., Vol. 13, p. 689, I908; Amer. Magaz., N.Y.,August, I9IO.
(iI6) THOMAS, B. A.: J.A.M.A., Vol. 54,pp. 258, 362, I9IO.(II7) DEBRE', R., and PARAF, J.: Presse Medicale, Vol. 21, p. IO3.
II3; Compt. Rend. Soc. de Biol., December 6th, II3;Bull. de la Soc. Mid. des H6p., Paris, Vol. 43, No. 30, p. 9o8,IgIg.
(II8) LANGERON and BOCCA: Lyon Chir., June, I930.(II9) SOLTAU, FENWICK and PARKINSON: Med. Chir. Arch., London,
I906.(I20) Fox, F.: Brit. Med. Jour., Vol. I., p. 979, I9O6.(I21) SALTER, A. G.: Austral. Med. Gaz., Sydney, June, I9IO.(I22) MALLETERRE, F.: New York Med. Jour., Vol. 103, No. 22,
I906.(I23) CHIARI, 0. M.: Centralb. f. Grenzgeb. d. Med. u. Chir. Jena,
Vol. 18, No. 5, I9I4.(I24) RAMOND, L.: Midicin. Paris, Vol. III., No. 2, P. I54, I92I.(I25) BALLENGER and ELDER: Surg. Gynec. and Obstet., XX .,
p. 574, Nov., I92I.(I26) THOMAS, A.: J.A.M.A., p. 2I74, December 24th, I927.(I27) RODRIGUEZ, M.: Paris Med., 63, p. 434, November 26th,
I927.(I28) MCDONAGH, J. E. R.: "Venereal Diseases " (Heinemann),
P. 3I8, I920.(I29) YOUNG, A.: Quoted by A. I. Wolbarst, " Gonococcal Infec-
tion,' 2nd Edition, I930, pp. 92 and I36.(130) BRASH and BUMPUS: Ibid., p. 92.(I3I) YOUNG, A., and YOUMANS, J. B.: J.A.M.A., 87, pp. 746-752,
September 4th, I926.(132) SMITH, MILLARD: J.A.M.A., June gth, I928.(I33) STEIN, H. C., and TRAUBE, W.: J.A.M.A., p. i6o8, May i9th,
I928.(I34) LAMBLIN, J.: Jour. de Scien. Mid. de Lille, No. 8,
February i9th, I928.(I35) GIRARD and TRIGHER: Progre's Medical, No. i6, April I7th,
I920.(136) DUROEUX, TANT and BERNARD, R.: Bruxelles Mid.,
November i5th, I920.
(To be continued.)
II3
on April 12, 2020 by guest. P
rotected by copyright.http://sti.bm
j.com/
Br J V
ener Dis: first published as 10.1136/sti.8.2.79 on 1 A
pril 1932. Dow
nloaded from





























