Embed Size (px)
Citation preview

Government Sponsored Reinsurance – How It Might Improve Insurance Markets
Katherine Swartz Harvard School of Public Health
NAIC Health Innovations Working Group MeetingSeptember 22, 2008

Roadmap
• Who lacks health insurance – quick points
• Choice in targeting of subsidies: poor people, very sick people, insurers
• Government reinsurance program provides a back-end subsidy – and targets adverse selection concerns
• Reinsurance, requirements to buy coverage, and risk-adjustments to premiums
Katherine Swartz, Harvard School of Public Health Sept 2008

Who Lacks Health Insurance?
• 47 million Americans in 2006.
• 2.2 million more than in 2005, almost all of whom lost employer-based coverage.
• One in six nonelderly people.
• 29% had middle-class incomes.
• 57% are 19 to 44 years of age, 20% are children.
Katherine Swartz, Harvard School of Public HealthSept 2008

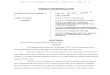
$10-19999, 17%
$20-29999, 17%
> median, 29%
< $10000, 16%
$30-48,201,
22%
Income of Uninsured in 2006

Probability of Being Uninsured by Middle Class Income for Adults,
1979 and 2006
21%
32%
6%
10%
0%
5%
10%
15%
20%
25%
30%
35%
1979 2006
< medianhouseholdincome> medianhouseholdincome
Katherine Swartz, Harvard School of Public Health, Sept 2008

17%
21.5%
12%10% 11%
14%12%
31%
27%
19%
15.3%13%
0%
5%
10%
15%
20%
25%
30%
35%
<19 19-24 25-34 35-44 45-54 55-64
Pro
ba
bili
ty
1979
2006
Probability of Being Uninsured by Age 1979-2006
Katherine Swartz, Harvard School of Public Health, Sept 2008

Implications
• Half of uninsured who are middle-class or not poor view premiums as too high for “value”
• High fraction of young adults are not insured – not good for risk pooling
• Nongroup and small group markets need stabilizing with more low-risk people
Katherine Swartz, Harvard School of Public HealthSept 2008

Subsidies• Usually targeted at low-income people
• But adverse selection creates risk in individual insurance markets – and higher premiums for people with incomes above “low income”
• Subsidies based on low income do not address adverse selection risk – they can exacerbate it become a transfer to insurers without altering risk to insurers
Katherine Swartz, Harvard School of Public Health Sept 2008

Risk of Adverse Selection
• “risk premium” for adverse selection risk
• Accurately predicting who is going to be in the top 1 or 2% of the expenditure distribution is impossible
• Left with “unaffordable” higher premiums and uninsured middle-class people
Katherine Swartz, Harvard School of Public Health Sept 2008

Forms of Competition
• Market segmentation– Companies specialize
• Selection mechanisms– Medical underwriting– Refusal to issue a policy– Exclusion of coverage for pre-existing
conditions– Many policies with different covered benefits
Katherine Swartz, Harvard School of Public HealthSept 2008

How to Address Risk Concerns
• Compensate insurers for covering people with extremely-high costs – keep insurers in market
• Shift burden of extremely-high-costs from insurers’ low-cost enrollees to broad population base
Katherine Swartz, Harvard School of Public HealthSept 2008

Reinsurance Targets Risk of Adverse Selection
• Reinsurance payouts based on who actually had high annual health spending – not predictions of risk
• Government-sponsored reinsurance is financed by broad tax base – shifts risk (and costs) of very sick people to general population
• Premiums decline, helping to stabilize private insurance market for everyone
Katherine Swartz, Harvard School of Public Health Sept 2008

Katherine Swartz, Harvard School of Public Health
13
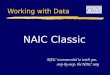
Risk Sharing by Layers of Reinsurance: % of Risk Retained by Insurer
$0
$100,000
$200,000
$300,000
$400,000
$50,000A
B
C
A
B
C
100%
25%
15%
5%
100%
10%
15%
12%
OR
$ of expenses per person

Why Excess-of-Loss Design?
• 1st goal: reduce insurers’ risk of individuals with very-high-costs – so insurers reduce premiums back-end subsidy to everyone
• 2nd goal: align incentives for insurers to manage individuals’ medical care
Katherine Swartz, Harvard School of Public HealthSept 2008

What Determines Cost of Public Reinsurance?
- Number of potential enrollees- Threshold and range of expenses to
be covered – layers of coverage – and where the range is in distribution of medical costs
- % of risk (costs) retained by originating insurer in layers
- Relevant medical expenses
Katherine Swartz, Harvard School of Public HealthSept 2008

Which Markets to Include?
• Small group and individual markets
• Goal is to address insurers’ concerns with potential for adverse selection want them to reduce use of selection mechanisms and lower premiums
Katherine Swartz, Harvard School of Public HealthSept 2008

Estimates of Costs
• Estimates at the national level run from $5B to $20B for the small group and individual markets with $50,000 threshold
• Compare with tax treatment of ESI: tax subsidy of $1,000-$1,200 per person
Katherine Swartz, Harvard School of Public HealthSept 2008

Financing Mechanisms
• Goal is to reduce insurers’ concerns about adverse selection and expand coverage
• Need new funds – not fees or taxes on insurers
• Broad tax base desired – extremely high medical costs are due to random events
Katherine Swartz, Harvard School of Public HealthSept 2008

Government as Reinsurer for Very-High-Cost People
• Less incentive for insurers to risk select since ex post determination of who is very-high-cost
• Broader population base pays for costs of very-high-cost people
• Incentive for management of care of high-cost people
• Premiums decline implicit subsidy
Katherine Swartz, Harvard School of Public HealthSept 2008

Targeting of Subsidies
• Balance between well-targeted aid to low-income people and goal of universal coverage
• Hurdle to universal coverage is risk premium in individual markets – which reinsurance addresses
• Back-end, less well-targeted subsidies make insurance more widely affordable (Healthy New York)
• Both types of subsidies needed
Katherine Swartz, Harvard School of Public Health Sept 2008

Summary
• Risk of very high-cost people makes individual premiums high
• Government reinsurance shifts this risk to general population – reducing premiums and creating incentive to manage medical care
• Creating affordability – but no free lunch
Katherine Swartz, Harvard School of Public Health Sept 2008