Embed Size (px)
Citation preview

GP28-A Vol. 25 No. 7
Replaces GP28-P Vol. 24 No. 9
Microwave Device Use in the Histology Laboratory; Approved Guideline
This document provides recommendations for reproducing the performance of microwave-accelerated procedures to prepare biological specimens in the histology laboratory. A guideline for global application developed through the Clinical and Laboratory Standards Institute consensus process.

Clinical and Laboratory Standards Institute Providing NCCLS standards and guidelines, ISO/TC 212 standards, and ISO/TC 76 standards The Clinical and Laboratory Standards Institute (CLSI) (formerly NCCLS) is an international, interdisciplinary, nonprofit, standards-developing, and educational organization that promotes the development and use of voluntary consensus standards and guidelines within the healthcare community. It is recognized worldwide for the application of its unique consensus process in the development of standards and guidelines for patient testing and related healthcare issues. Our process is based on the principle that consensus is an effective and cost-effective way to improve patient testing and healthcare services.
In addition to developing and promoting the use of voluntary consensus standards and guidelines, we provide an open and unbiased forum to address critical issues affecting the quality of patient testing and health care.
PUBLICATIONS
A document is published as a standard, guideline, or committee report.
Standard A document developed through the consensus process that clearly identifies specific, essential requirements for materials, methods, or practices for use in an unmodified form. A standard may, in addition, contain discretionary elements, which are clearly identified.
Guideline A document developed through the consensus process describing criteria for a general operating practice, procedure, or material for voluntary use. A guideline may be used as written or modified by the user to fit specific needs.
Report A document that has not been subjected to consensus review and is released by the Board of Directors.
CONSENSUS PROCESS
The CLSI voluntary consensus process is a protocol establishing formal criteria for:
• the authorization of a project
• the development and open review of documents
• the revision of documents in response to comments by users
• the acceptance of a document as a consensus standard or guideline.
Most documents are subject to two levels of consensus—“proposed” and “approved.” Depending on the need for field evaluation or data collection, documents may also be made available for review at an intermediate consensus level.
Proposed A consensus document undergoes the first stage of review by the healthcare community as a proposed standard or guideline. The document should receive a wide and thorough technical review, including an overall review of its scope, approach, and utility, and a line-by-line review of its technical and editorial content.
Approved An approved standard or guideline has achieved consensus within the healthcare community. It should be reviewed to assess the utility of the final document, to ensure attainment of consensus (i.e., that comments on earlier versions have been satisfactorily addressed), and to identify the need for additional consensus documents.
Our standards and guidelines represent a consensus opinion on good practices and reflect the substantial agreement by materially affected, competent, and interested parties obtained by following CLSI’s established consensus procedures. Provisions in CLSI standards and guidelines may be more or less stringent than applicable regulations. Consequently, conformance to this voluntary consensus document does not relieve the user of responsibility for compliance with applicable regulations.
COMMENTS
The comments of users are essential to the consensus process. Anyone may submit a comment, and all comments are addressed, according to the consensus process, by the committee that wrote the document. All comments, including those that result in a change to the document when published at the next consensus level and those that do not result in a change, are responded to by the committee in an appendix to the document. Readers are strongly encouraged to comment in any form and at any time on any document. Address comments to the Clinical and Laboratory Standards Institute, 940 West Valley Road, Suite 1400, Wayne, PA 19087, USA.
VOLUNTEER PARTICIPATION
Healthcare professionals in all specialties are urged to volunteer for participation in CLSI projects. Please contact us at [email protected] or +610.688.0100 for additional information on committee participation.

GP28-A ISBN 1-56238-563-1
Volume 25 Number 7 ISSN 0273-3099
Microwave Device Use in the Histology Laboratory; Approved Guideline Gary R. Login, DMD, DMSc Ellyn S. Beary, BS H. Skip Brown, BA, HT(ASCP) Cheryl H. Crowder, BA, HTL(ASCP) Maureen Doran, BA, HTL(ASCP) Richard T. Giberson, BA, MS H. M. Skip Kingston, PhD Anthony Leong, MD Max Robinowitz, MD Steven E. Slap, BA, MA, MPhil Franco Visinoni, PhD Abstract This document provides recommendations for quality assurance and safety procedures for microwave equipment use, and provides a means to understand and troubleshoot conditions that contribute to variability in microwave-accelerated procedures in human clinical, veterinary, and research histopathology laboratories. Safety issues unique to microwave instrumentation in histopathology laboratory settings are emphasized. In addition, the document discusses microwave device process control, procedure validation, and results verification. Clinical and Laboratory Standards Institute (CLSI). Microwave Device Use in the Histology Laboratory; Approved Guideline. CLSI document GP28-A (ISBN 1-56238-563-1). Clinical and Laboratory Standards Institute, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2005.
The Clinical and Laboratory Standards Institute consensus process, which is the mechanism for moving a document through two or more levels of review by the healthcare community, is an ongoing process. Users should expect revised editions of any given document. Because rapid changes in technology may affect the procedures, methods, and protocols in a standard or guideline, users should replace outdated editions with the current editions of CLSI/NCCLS documents. Current editions are listed in the CLSI catalog, which is distributed to member organizations, and to nonmembers on request. If your organization is not a member and would like to become one, and to request a copy of the catalog, contact us at: Telephone: 610.688.0100; Fax: 610.688.0700; E-Mail: [email protected]; Website: www.clsi.org

Number 7 GP28-A
ii
This publication is protected by copyright. No part of it may be reproduced, stored in a retrieval system, transmitted, or made available in any form or by any means (electronic, mechanical, photocopying, recording, or otherwise) without prior written permission from Clinical and Laboratory Standards Institute, except as stated below. Clinical and Laboratory Standards Institute hereby grants permission to reproduce limited portions of this publication for use in laboratory procedure manuals at a single site, for interlibrary loan, or for use in educational programs provided that multiple copies of such reproduction shall include the following notice, be distributed without charge, and, in no event, contain more than 20% of the document’s text.
Reproduced with permission, from CLSI publication GP28-A—Microwave Device Use in the Histology Laboratory; Approved Guideline (ISBN 1-56238-563-1). Copies of the current edition may be obtained from Clinical and Laboratory Standards Institute, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898, USA.
Permission to reproduce or otherwise use the text of this document to an extent that exceeds the exemptions granted here or under the Copyright Law must be obtained from Clinical and Laboratory Standards Institute by written request. To request such permission, address inquiries to the Executive Vice President, Clinical and Laboratory Standards Institute, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898, USA. Copyright ©2005. Clinical and Laboratory Standards Institute. Suggested Citation (Clinical and Laboratory Standards Institute. Microwave Device Use in the Histology Laboratory; Approved Guideline. CLSI document GP28-A [ISBN 1-56238-563-1]. Clinical and Laboratory Standards Institute, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898 USA, 2005.) Proposed Guideline February 2004 Approved Guideline February 2005 ISBN 1-56238-563-1 ISSN 0273-3099

Volume 25 GP28-A
iii
Committee Membership Area Committee on General Laboratory Practices Sheila M. Woodcock, ART, MBA Chairholder QSE Consulting Rose Bay, Nova Scotia, Canada Albert Rabinovitch, MD, PhD Vice-Chairholder Abbott Laboratories, Hematology Business Unit Santa Clara, California Eric Arendash, MT(ASCP) Centers for Medicare & Medicaid Services Philadelphia, Pennsylvania Miguel Azar, MD Dept. of Veterans Affairs Medical Center Minneapolis, Minnesota Lucia M. Berte, MA, MT(ASCP), SBB, DLM; CQA(ASQ)CQMgr Quality Systems Consultant Westminster, Colorado
Margaret M. Grimes, MD Virginia Commonwealth University Richmond, Virginia Theresa D. Stokeld, MBA, MT(ASCP)DLM Remel Inc. Lake Charles, Louisiana Advisors Kay M. Creed St. Mary’s Hospital Richmond, Virginia Steven I. Gutman, MD, MBA FDA Ctr. for Devices/Rad. Health Rockville, Maryland Gerald A. Hoeltge, MD The Cleveland Clinic Foundation Cleveland, Ohio
Stephen J. Sarewitz, MD Valley Medical Center Renton, Washington Jennifer Schiffgens, MBA, MT(ASCP) California Pacific Medical Center San Francisco, California Daniel W. Tholen, MS Dan Tholen Statistical Consulting Traverse City, Michigan Marla Thomas Litton Pathology Associates Blue Springs, Missouri Eleanor M. Travers, MD, MHA State of Connecticut Dept. of Public Health Hartford, Connecticut
Subcommittee on Microwave Ovens Gary R. Login, DMD, DMSc Chairholder Harvard School of Dental Medicine Boston, Massachusetts Ellyn S. Beary, BS NIST Gaithersburg, Maryland H. Skip Brown, BA, HT(ASCP) Lab Management Consultants Maryland Heights, Missouri Cheryl H. Crowder, BA, HTL(ASCP) Louisiana State University Baton Rouge, Louisiana Maureen Doran, BA, HTL(ASCP) SIU Medical School Carbondale, Illinois Richard T. Giberson, BA, MS Ted Pella, Inc. Redding, California
H. M. Skip Kingston, PhD Duquesne University Pittsburgh, Pennsylvania Anthony Leong, MD Hunter Area Pathology Services Newcastle, Australia Max Robinowitz, MD FDA Ctr. for Devices/Rad. Health Rockville, Maryland Franco Visinoni, PhD Milestone s.r.l. Fratelli, Italy Advisors Charles J. Churukian, BH, HT(ASCP) HTL University of Rochester Medical Center Rochester, New York Alton D. Floyd, PhD Norfolk Associates, Inc. Edwardsburg, Michigan
Stacie Kirsch Electron Microscopy Sciences Fort Washington, Pennsylvania Susan Meloan, BBA, HT(ASCP) HTL Medical College of Georgia North Augusta, South Carolina Diane G. Miller, HT(ASCP) Miller Consultant Services Beaverbow, Oregon Jan Minshew, HT(ASCP) HTL Leica Microsystems, Inc. Bannockburn, Illinois Shan-Rong Shi, PhD USC Keck School of Medicine Los Angeles, California Albert J.H. Suurmeijer, MD, PhD University Hospital Groningen Groningen, The Netherlands
Number 7 GP28-A
iv
Staff
Clinical and Laboratory Standards Institute Wayne, Pennsylvania Tracy A. Dooley, MLT(ASCP) Staff Liaison Donna M. Wilhelm Editor Melissa A. Lewis Assistant Editor Acknowledgement in Memoriam of our Subcommittee Member and Colleague The Clinical and Laboratory Standards Institute (CLSI) and the Subcommittee on Microwave Ovens acknowledge the contributions of Mr. Steven E. Slap, BA, MA, M Phil. Steve was one of the early promoters of the first commercial laboratory microwave device for histology. His energy and foresight stimulated many educational seminars, and he introduced many histologists to the benefits of microwave methods.

Volume 25 GP28-A
v
Contents
Abstract ....................................................................................................................................................i
Committee Membership........................................................................................................................ iii
Foreword.............................................................................................................................................. vii
1 Scope..........................................................................................................................................1
2 Introduction................................................................................................................................1
3 Definitions .................................................................................................................................2
4 Precautions and Safety...............................................................................................................5 4.1 Microwave Radiation Exposure Standards and Regulations ........................................5 4.2 Electrical Precautions ...................................................................................................7 4.3 Biological Precautions ..................................................................................................8 4.4 Chemical Handling Precautions....................................................................................8 4.5 High Temperature Precautions .....................................................................................9 4.6 Recommended Safety Procedures for Microwave Devices and Applications..............9 4.7 Microwave Safety Inspection .....................................................................................11
5 Principles of Microwave-Accelerated Methods.......................................................................12 5.1 Power Level ................................................................................................................13 5.2 Energy Absorption Mechanisms and Reaction Conditions ........................................14
6 Recommendations for Documenting Microwave Methods .....................................................15
7 Critical Descriptors for Microwave-Accelerated Procedures ..................................................15 7.1 Temperature Control and Measurement .....................................................................16 7.2 Microwave Power .......................................................................................................21 7.3 Specimen Handling.....................................................................................................22 7.4 Process Time...............................................................................................................26
8 Special Microwave Procedures................................................................................................27 8.1 Antigen Retrieval Protocol .........................................................................................27
9 Template for Documentation of Microwave Methods.............................................................29
10 Troubleshooting Results ..........................................................................................................30
References.............................................................................................................................................32
Summary of Delegate/Consensus Comments and Subcommittee Responses ......................................35
The Quality System Approach..............................................................................................................40
Related CLSI/NCCLS Publications ......................................................................................................41

Number 7 GP28-A
vi

Volume 25 GP28-A
vii
Foreword The ease and rapid pace with which microwaves have entered the clinical laboratory are raising many questions for laboratory administrators. Are laboratory personnel aware of and trained in safety issues unique to microwaves? Do laboratory directors have a quality assurance program for microwave procedures? Does the leadership of the national societies that represent medical and research communities have the information they need to respond to local and national regulatory agencies regarding the safe and efficacious use of microwave technology? Are equipment manufacturers promoting equipment that meets the highest safety standards? Several basic science and clinical research laboratories in North America, Europe, Asia, and Australia working independently during the past 31 years have identified important principles for using microwave technology reliably in laboratory medicine. This guideline emphasizes the scientific principles and practices involving the safe and effective use of microwave ovens in the histology laboratory. However, it is also important to be aware of national and local governmental regulatory requirements before microwave ovens are selected and used in clinical laboratories. The guideline only provides examples of the regulatory requirements that are current in the United States. Users in other countries are advised to consult with their national and local authorities for requirements.
Readers wishing for a quick start are directed to the following sections: • Table 4, Safe Laboratory Use of Microwave Devices; • Section 9, Template for Documentation of Microwave Methods; and • Section 10, Troubleshooting Results.
Key Words Antigen retrieval, biopsy, electron microscopy, fixation, histology, immunocytochemistry, immunohistochemistry, light microscopy, microwave, processing, resin curing, staining

Number 7 GP28-A
viii

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 1
Microwave Device Use in the Histology Laboratory; Approved Guideline 1 Scope This CLSI guideline is written for multiple audiences, including: laboratory technicians, microwave device manufacturers, microwave device resellers, compliance and safety officials, and administrators. The goals of this document are to 1) provide a scientific basis for reproducible sample preparation of biological specimens for diagnostic purposes; 2) advise laboratory personnel on the best safety guidelines; and 3) discuss the limitations of domestic microwave ovens in a hospital laboratory. Original sources are cited in the References section for those individuals seeking additional information.
NOTE: The reader is encouraged to supplement the information in this document with continuing education courses on microwave device safety and use. To ensure the success of microwave-accelerated procedures in the histopathology laboratory, this document provides: • general definitions of common microwave terminology; • detailed discussion of safety issues particular to microwave heating of samples; • guidelines to identify potential sources of variability; and • a “hands-on” troubleshooting guide to improve microwave-accelerated procedures.
2 Introduction Microwave-accelerated sample preparation of biological specimens is a field that continues to grow rapidly as evidenced by the number of innovative articles written each year. The reason for this increase in the microwave literature is simple. Microwave-accelerated procedures are useful in almost every step of sample preparation for microscopy. Microwave procedures speed up reaction processes and save time. Even more important, microwave procedures improve the retention of soluble antigens and often preserve antigen immunoreactivity better than conventional fixation methods.1,2 In short, microwave-accelerated techniques can be used to improve the efficiency of a variety of histopathology laboratory procedures, such as fixation, decalcification, processing of specimens for paraffin wax or resin embedding, and staining. Hundreds of laboratory procedures using microwave devices for histopathology have been published.1,3-5 A brief list of these procedures is provided in Table 1. Table 1. Application of Microwave-Accelerated Methods in Histopathology (see Sections 4.3 through 4.6 for Safety Precautions) 1,3-5 Examples of Microwave-Accelerated Methods Fixation of human and animal specimens
Histoprocessing Immunogold Protein A labeling
Fixation of marine specimens Decalcification Streptavidin-biotin-peroxidase labeling
In situ hybridization
Fixation of plant specimens Immunoperoxidase Immunofluorescence Rapid drying Fixation of insect specimens Antigen retrieval Lectin labeling Enzyme-linked
immunosorbent assay (ELISA)

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 2
Three types of microwave devices are being used in a histopathology laboratory setting: 1) microwave instruments specifically designed and certified as medical devices; 2) commercial grade microwave devices converted for laboratory/clinical use; and 3) consumer household microwave units modified for laboratory/clinical use. Laboratory microwave devices are designed with exhaust fans and safety features to protect the operator, sensors to protect the instrument, and sophisticated temperature monitoring and intricate electronics that allow improved quality control of the specimen. Household microwave units are designed for food preparation, and they are not certified for laboratory use unless they meet the requirements outlined in Section 4. All three types of microwave devices have a large chamber in which samples are heated. Large-chamber microwave devices are often described in the microwave literature as “large-cavity” or “multimodal devices.” For the purposes of this document, we will use the term “large-cavity microwave devices.” Several features have been added to microwave devices to reduce heating damage to biological specimens and microwave equipment (see Table 2). Manufacturers of laboratory microwave equipment have improved temperature control by adding temperature probes with feedback systems for process automation, specialized power supplies for generation of microwave power,4,6-10 controllable magnetron duty cycles,3 and variable power output.11 Highly specialized microwave devices have platforms with very high rotational speed,12 vacuum and pressure cycling,13-15 and hybrid equipment combining ultrasound and microwave irradiation.16 Table 2. Use of Large-Cavity Microwave Devices With Basic or Advanced Features
Histopathology Laboratory Procedure
Large-Cavity Microwave
Devices with Basic Functions
Large-Cavity Microwave Devices
with Advanced Functions
Rationale for Equipment Choice Drying Slides X Minimal control necessary Melting Agar X Minimal control necessary Enzyme/Antigen Retrieval X Minimal control necessary Staining (nontoxic reagents) X Minimal control necessary Staining (toxic reagents) X Exhaust fume safety Tissue Processing X Precise temperature control/exhaust
fume safety In situ Hybridization X Precise temperature control Decalcification X Process control, safety Fixation X Exhaust fume safety Resin Embedding X Exhaust fume safety To date, there are no regulations or benchmarks specifically for microwave devices in the clinical laboratory. There are, however, many regulations regarding electrical safety and general laboratory equipment safety that include microwave devices (see Section 4 for more details). In addition, the potential to overheat and damage diagnostic biological specimens in microwave procedures is great (e.g., tissue shrinkage, denatured connective tissue, pyknotic nuclei). The need for guidelines and quality assurance for microwave procedures is well recognized.4,17-26 3 Definitions This section provides a brief list of the most common terms and definitions to facilitate reading the microwave literature. A detailed report of terminology related to microwave safety has been published.27 Accuracy (of measurement) – Closeness of the agreement between the result of a measurement and a true value of the measurand (VIM93).28 Anode – A positively charged conductor by which electrons leave an electrical device.

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 3
Arcing – Electrical conduction through a gas in an applied electric field. Calorie (C) – 1) The amount of heat it takes to raise the temperature of 1000 grams or 1 kg of water one degree centigrade; NOTE: A Calorie is actually a kilocalorie or 1000 calories; 2) calorie (c) – The amount of heat it takes to raise the temperature of 1 gram of water 1 degree centigrade; NOTE: The cal/min is the unit of heat per minute. Cathode – Negatively charged conductor that is the source of electrons in an electrical device. Conduction – The flow of heat by conduction occurs via collisions between atoms and molecules in the substance and the subsequent transfer of kinetic energy; NOTE: When there exists a temperature gradient within a body, heat energy will flow from the region of high temperature to the region of low temperature. Convection – The flow of heat through a bulk, macroscopic movement of matter from a hot region to a cool region. Dielectric constant – The measure of a sample’s ability to obstruct the microwave energy as it passes through the medium; the loss (dielectric) factor measures the sample’s ability to dissipate that energy; NOTE: The term “loss” is used to indicate the amount of input microwave energy that is lost to the sample by being dissipated as heat in the sample. Diode – A device that conducts electric current run in one direction only. Dipolar molecules – Molecules that are configured such that electrons favor one region of the molecule, resulting in an uneven spatial distribution of electrons and charge so that one side is slightly negatively charged relative to the somewhat more positively charged other side. Dipole rotation – The net alignment, due to the electric field, of molecules in the sample that have permanent or induced dipole moments. Duty cycle (magnetron cycling) – Microwave power can be applied continuously but is usually pulsed. The power output of the magnetron is controlled by “cycling” the magnetron on and off at full power for some fraction of time to obtain an average power level. The duty cycle of a magnetron is the time the magnetron is ‘on’ divided by the total time of the cycling period; NOTE: Domestic microwave devices have relatively long cycling periods based on intervals of 1/6 min. (10 seconds) and longer as compared to laboratory analytical grade microwave equipment which has cycling periods of 1/60 min. (1 second), making heat control more difficult in household microwave devices. Entropy (thermodynamics) – A thermodynamic quantity representing the amount of energy in a system that is no longer available for doing mechanical work. Hertz – The derived Standardized International (SI) Units of inductance, defined as the frequency of one cycle per second, having units of S-l (reciprocal seconds).
Inductance – A magnetic field produced by the presence of an electric current. Ionic conduction – The conductive (i.e., electrophoretic) migration of dissolved ions in the applied electromagnetic field. Magnetron – A cylindrical diode with an anode and a cathode; NOTES: a) Superimposed on the diode is a magnetic field that is aligned with the cathode; b) A ring of mutually coupled resonant cavities is in the

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 4
anode so a potential of several thousand volts is reached across the diode; c) The released electrons, under the influence of the magnetic field, resonate, and the magnetron oscillates. Microwave field – Electromagnetic, nonionizing radiation that is produced by the magnetron; NOTES: a) The microwave field refers to the density of microwave energy in a defined space; b) This microwave energy density in a space is sometimes referred to as “field strength.” Microwaves – Electromagnetic energy between far infrared (IR) and radio waves that corresponds to wavelengths of 1 cm to 1 m; NOTE: The frequency range of these sources is between 30 GHz and 300 MHz with a frequency of 2450 MHz being the most common. Microwave-transparent – Having the property of transmitting microwaves, materials such as glass or plastics that do not absorb microwave energy. Mode stirrer – A device that disrupts standing microwave patterns and distributes the microwave energy more homogeneously throughout a microwave cavity. Power output of the magnetron – A measure of heat per unit time, i.e., 1 W = 14.33 cal/min; NOTE: The microwave energy output from the magnetron is generally measured in watts. Reflected power – The power that occurs when the traveling electromagnetic waves are reflected and the flow of energy is partly in the reverse direction; NOTES: a) Reflected microwave energy can result in overheating or a deficiency of microwave energy in localized areas; b) Devices that remove reflected microwaves have been designed to protect the magnetron from microwave energy reflected back into the wave-guide. Reproducibility – Precision under conditions where test results are obtained with the same method on identical test items in different laboratories with different operators using different equipment (ISO 5725-1).29 Sample – One or more parts taken from a system and intended to provide information on the system, often to serve as a basis for decision on the system or its production (ISO 15189)30; NOTE: For example, a volume of serum taken from a larger volume of serum (ISO 15189). Specific heat – The heat required to raise the temperature of one gram of a substance one degree centigrade.
Specimen – The discrete portion of a body fluid or tissue taken for examination, study, or analysis of one or more quantities or characteristics to determine the character of the whole. Thermodynamic – The branch of physics concerned with the conversion of different forms of energy; it is the study of the effects of work, heat, and energy on a system. Watt – 1) In electrical terms, one watt is the power produced by a current of one ampere flowing through an electric potential of one volt; 2) The power which in one second gives rise to energy of one joule; NOTES: a) The SI unit of power; power is the rate at which work is done, or (equivalently) the rate at which energy is expended; b) One watt is equal to a power rate of one joule (force per distance) of work per second of time. Wave-guide – A device that delivers the microwave energy from the magnetron to the microwave cavity.

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 5
4 Precautions and Safety Microwave techniques introduce unique safety considerations that are not encountered by technicians using traditional laboratory heating devices. Microwave irradiation has the capability of rapid high-temperature heating, with the potential for vaporization and pressurization. The majority of unsafe conditions or practices that can arise during the use of microwave systems in the laboratory are avoidable. It is essential that microwave units be operated in a manner that ensures maximum safety to the operator and laboratory personnel. In the U.S., many regulatory bodies (e.g., Food and Drug Administration [FDA], Occupational Safety and Health Administration [OSHA]) require compliance with provisions of the Code of Federal Regulations (CFR) and testing laboratories and certification organizations (e.g., Underwriters’ Laboratories [UL]). One such provision for laboratory equipment is 29 CFR 1910.399. This requirement states that an installation of equipment (including household microwave ovens) could be acceptable (to OSHA) and approved within the meaning of Subpart S requirement if it is accepted, certified, listed, labeled, or otherwise determined to be safe by a nationally recognized testing laboratory (NRTL). However, even if a device or equipment is “approved,” 29 CFR 1910.303(b) (2) requires that the “listed or labeled equipment should be used or installed in accordance with any instructions included in the listing or labeling.” NOTE: Current FDA and OSHA regulations do not prevent anyone from purchasing and using a microwave oven for other than its intended purpose. However, once a household or commercial microwave unit has been modified for use in a clinical laboratory (i.e., it is no longer considered to have been “designated to heat, cook, or dry food”), the original oven manufacturer is neither liable nor responsible for the compliance of the modified ovens. Thus, the person who is modifying the oven is subject to the provisions of Chapter V, Subchapter A- Drugs and Devices of the Federal Food, Drug, and Cosmetic (FFD&C) Act. Microwave-accelerated sample preparation is not exempt from traditional safety considerations, and references to general laboratory safety are available.31 (Please refer to the most current edition of CLSI/NCCLS document GP17—Clinical Laboratory Safety for additional information.) In this section, the unsafe conditions and practices that may occur in the preparation of biological specimens related to the operation of microwave devices are evaluated. A detailed discussion of relevant equipment standards, safety code requirements, and general safety guidelines relating to laboratory microwave systems is presented. A recommendation for periodic updating of safety information is included. NOTE: Readers are also encouraged to consult frequently updated resources on general microwave laboratory safety for additional information.32 Hazards related to microwave use for specimen preparation are organized into five groups: 1) radiation exposure standards and regulations; 2) electrical precautions; 3) biological precautions; 4) chemical environment; and 5) high-temperature hazards. 4.1 Microwave Radiation Exposure Standards and Regulations 4.1.1 Microwave Radiation Safety Studies into the biological effects of microwave radiation exposure have been extensively detailed (~1000 references) in several reviews dealing with scientific, industrial, and medical applications.27 Currently in the United States, microwave energy exposure from all large-cavity microwave devices operating at 2450 MHz is limited to 5 mW/cm2 at a distance of 5 cm from any surface of a product. 27 The maximum human exposure to radio frequency (RF) energy for operating in a safe workplace is <10 mW/cm2 averaged over

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 6
a six-minute period.33 Although no microwave leakage limit exists specifically for laboratory and scientific units, manufacturers of these products are subject to other Federal Drug Administration (FDA) regulations.34-36 Microwave device performance standards are incorporated in the Radiation Control for Health and Safety Act, Federal Law enacted in 1968.27 The FDA regulates microwave-heating devices under two different provisions of the FFD&C Act. Under the FFD&C Act, they are regulated as electronic products in Chapter V, subchapter C—Electronic Product Radiation Control. Under the Radiation Control provisions, the FDA regulates the manufacture of electronic products but not their use (written communication, April 2002). If the microwave-heating device is designed for heating, cooking, or drying food and “manufactured for use in homes, restaurants, food vending, or service establishments…” then it is subject to the Federal Performance Standards for Microwave and Radiofrequency Emitting Products, 21 CFR 1030.10 (written communication, April 2002). 4.1.2 CDRH Consumer Information—Microwave Device Radiation Ovens and Pacemakers: At one time there was concern that leakage from microwave ovens could interfere with certain electronic cardiac pacemakers. There was similar concern about pacemaker interference from electric shavers, auto ignition systems, and other electronic products. Because there are so many other products that also could cause this problem, FDA does not require microwave ovens to carry warnings for people with pacemakers. The problem has been largely resolved, since pacemakers are now designed so they are shielded against such electrical interference. However, patients with pacemakers may wish to consult their physicians about this electrical interference. Many references to other international standards are available and should be consulted if the user’s geographical location places the microwave under other jurisdictions.37 4.1.3 Microwave Equipment Classified as Medical Devices This section provides regulatory information primarily for microwave device manufacturers, microwave device resellers, compliance and safety officials, and administrators. The information below may also assist laboratory technicians making purchasing decisions of microwave devices that are in compliance with FDA and OSHA regulations. In the U.S., OSHA regulations require that, if microwave equipment is modified or the integrity of a safety device is violated, the product must be demonstrated to be safe by measuring the microwave radiation exposure potential.27 As long as damage, wear, or misuse have not lessened the effectiveness of the instrument, all the exposure limits of various national/international standards are met or exceeded. 27,38 The FFD&C Act defines a medical device as an instrument, apparatus, implement, machine, contrivance, implant, in vitro reagent, or other similar or related article including a component or accessory that is intended for use in the diagnosis of disease or other conditions, or in the cure, mitigation, treatment, or prevention of disease, in man or other animals.39 A summary of FDA regulations of Microwave Equipment is in Table 3.

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 7
Table 3. Summary of FDA Regulations of Microwave Equipment
21 CFR 1002.12
Abbreviated Report40
21 CFR 1002.30
Accidental Radiation Coverage33
21 CFR 1003 Defect of Failure to Comply35
Premarket Notification and Filing of
510(k), Registration and Listing MDR, etc.
21 CFR 820 GMP/QS
Regulation41
Microwave Heating for Nonmedical Use
X
X
X
Microwave Heating for Medical and/or Clinical Use
X
X
X
X
These regulations can be found in the FDA web pages: Nonmedical devices: http://www.fda.gov/cdrh/radhealth.html Medical devices: http://www.fda.gov/cdrh/devadvice If a manufacturer or user modifies a household microwave oven or commercially promotes histological use as an indication for use, then the microwave oven would be regarded by the FDA as a medical device (written communication, April 2002). The medical device would then be subject to provisions under Title 21 of the Code of Federal Regulations CFR 820.180 (records) and 820.198 (complaint files). The final classification of a microwave device for histological applications appears in 21 CFR 864.3010, Tissue Processing Equipment. Once a new or modified microwave device is classified, manufacturers should consult 21 CFR Section 864.9 to determine whether or not subsequent modifications meet limitations of exemption from Section 510(k) of the Act. The original oven manufacturer is no longer responsible for the compliance of a modified oven, and the person who is modifying the oven is subject to the provisions of Chapter V, subchapter A—Drugs and Devices of the FFD&C Act. Manufacturers subject to the FDA regulations include original manufacturers, importers, and persons who remanufacture products for distribution to others.27 Remanufacturing includes adapting a product for a new or intended use, such as converting household cooking devices for laboratory use, and reselling them.27 4.2 Electrical Precautions This section provides electrical safety information primarily for microwave device manufacturers, microwave device resellers, and compliance and safety officials, and administrators. Laboratory technicians are advised that according to OSHA household microwave ovens do not meet the more stringent door seal and endurance tests required for applications outside of the home. Microwave devices, like any appliance used in a laboratory, must be certified as electrically safe for laboratory use by a recognized testing laboratory (e.g., Underwriters Laboratories [UL], Canadian Standards Association [CSA], or Conformité Européene [ ], which means European Conformity). The unit must be grounded in accordance with the manufacturer’s specifications.27 In accordance with the policy of the end user’s institution, qualified service technicians must do electrical repairs. The use of metal accessories is not recommended unless they were designed and tested for use with the particular microwave equipment and are used according to the manufacturer’s specifications.

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 8
UL-listed household and commercial-use microwave ovens are evaluated to the applicable electrical requirements of the UL 923 standard for safety of microwave cooking appliances. The construction and type test requirements are substantially similar for household and commercial types except for the more stringent door seal and endurance tests for commercial types. Laboratory equipment is evaluated to the applicable requirements of UL 61010A-1, Standard for Safety of Electrical Equipment for Laboratory Use; Part 1: General Requirements (written communication, April 2002). The safety instructions in UL 923 state, “Use this appliance only for its intended use as described in the manual. Do not use corrosive chemicals or vapors in this appliance. This type of oven is specifically designed to heat, cook, or dry food. It is not designed for industrial or laboratory use” (written communication, August 2002). 4.3 Biological Precautions It is often impossible to know what might be infectious; therefore, all specimens are to be treated as potentially infectious and handled according to “standard precautions.” Standard precautions are guidelines that combine the major features of “universal precautions” and “body substance isolation” practices. Standard precautions cover the transmission of any pathogen and thus, are more comprehensive than universal precautions, which are intended to apply only to transmission of blood-borne pathogens. Standard precaution and universal precaution guidelines are available from the U.S. Centers for Disease Control and Prevention (Guideline for Isolation Precautions in Hospitals. Infection Control and Hospital Epidemiology. CDC. 1996;Vol 17;1:53-80.), (MMWR 1987; 36(suppl 2S):2S-18S), and (MMWR 1988;37:377-382, 387-388). For specific precautions for preventing the laboratory transmission of blood-borne infection from laboratory instruments and materials, and recommendations for the management of blood-borne exposure, refer to CLSI/NCCLS document M29—Protection of Laboratory Workers from Occupationally Acquired Infections. The utility of using microwave energy to destroy pathogens requires further study. Therefore, until more data becomes available, all potentially infectious specimens must be handled with standard precautions during and after the use of microwave irradiation. The inside walls of the microwave device should be cleaned with a nonabrasive, disinfectant solution. Chemical germicides registered with and approved by the EPA as “sterilants” can be used for decontamination in accordance with the manufacturer’s instructions. Microwave devices that are used for any laboratory procedure should not be used to heat food for human or animal consumption. 4.4 Chemical Handling Precautions Safety of the technician is the most important consideration in the sample preparation process. Microwave energy accelerates the rate of sample reactions, but it does not alter the fundamental chemistry involved. The technician is advised that any reagents that are dangerous to heat by conventional methods are likely to be more dangerous when heated in a microwave device because of the rapid rate of heating. If there is any concern about flammability of a reagent do not use it in a microwave oven. Combinations of reagents that are explosive, or so highly reactive as to be uncontrollable, fall into this category. Please check the Material Safety Data Sheet (MSDS) or with the manufacturer of the microwave device to determine safety and test data for a particular reagent or procedure to avoid unreasonable, hazardous misuse of laboratory microwave systems. 27,32 See http://www.sampleprep.duq.edu/dir/safety.html Handling chemicals in a microwave environment requires special considerations. Aqueous chemicals that are dangerous at room temperature (e.g., formaldehyde, osmium tetroxide, lead acetate) pose an added danger during and immediately after microwave irradiation. Chemicals that are warmed will volatilize in the microwave cavity. Opening the door of a microwave device that is not properly vented will allow the volatilized chemical vapors to enter the laboratory environment. Some types of ventilation hoods can function properly when a microwave device without an exhaust fan is properly placed in the system. End

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 9
users should consult a qualified ventilation specialist to determine if the laboratory hood and ventilation system are capable of functioning safely with the intended microwave device. Laboratory grade microwave devices equipped with exhaust fans and connected to an approved ventilation system will reduce the risk of chemical exposure hazard during microwave heating. The use of organic solvents and caustic chemicals may accelerate the deterioration of door seals and safety interlock switches.42 Transport of heated chemicals outside of the microwave cavity or ventilation hood should be done in a closed container. Chemically resistant gloves and goggles should be used to handle all containers containing hazardous materials that have been microwaved. All chemical spills should be handled with appropriate chemical spill precautions and the surfaces cleaned off immediately to prevent damage to the unit. NOTE: Do not use corrosive chemicals or vapors in microwave devices unless directed so in the device manual. Engineering controls, work practices, and personal protective equipment should be used in accordance with local and regional regulations (e.g., OSHA) and the end user’s institutional standards. Additional information about chemical safety according to OSHA standards can be found in documents such as Occupational Exposure to Hazardous Chemicals in Laboratories (29 CFR 1910.1450), Flammable and Combustible Liquids standard (29 CFR 1910.106), permissible limits in the Air Contaminants (29 CFR 1910.1000), and specific chemical standards in 29 CFR Subpart Z that apply. For safety concerns within the hospital, laboratories that must comply with 29 CFR 1910.1450 must designate “personnel responsible for implementation of the Chemical Hygiene Plan including assignment of a Chemical Hygiene Officer, and if appropriate, establishment of a Chemical Hygiene Committee” (written communication, August 2002). 4.5 High Temperature Precautions Microwave protocols for histology laboratories should specify the use of containers that are vented to prevent pressurization during microwave heating. Containers must be microwave compatible and not contain metal parts that may reflect microwave energy or cause arcing of microwave power. Although special containers are available for pressurization in a microwave, these are generally designed and used for acid digestion of samples for analytical elemental analyses27 or for high temperature sterilization and antigen retrieval. A protective thermal glove should be used when removing samples that are irradiated to high temperatures in a microwave (i.e., heated solutions may conductively heat the container). Spontaneous “volcanic” boiling can occur in liquids after microwave irradiation and upon removal of the sample from the microwave. This is attributed to localized super heating of the liquid which occurs secondary to bubble nucleation and coalescence of dissolved gases as a result of microwave heating. 27,43 The risk of spontaneous boil over in histopathology applications is more likely during high temperature heating procedures, such as microwave staining and antigen retrieval processes. 4.6 Recommended Safety Procedures for Microwave Devices and Applications Microwave devices designed for the laboratory may include safety features such as isolation of the fume exhaust from the device electronics, high volume exhaust, safety interlocks, and sensors for flammable solvents. Table 4 is designed to emphasize safe laboratory practices with microwave devices. Case histories of microwave accidents have been summarized. 27

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 10
Table 4. Safe Laboratory Use of Microwave Devices Procedure Safety Equipment Safety
Infectious Materials – Follow standard precautions for blood-borne pathogens with potentially infectious materials.44 (Please refer to the most current version of CLSI/NCCLS document M29—Protection of Labor-atory Workers from Occupationally Acquired Infections for additional information.)
Use a nonabrasive disinfectant to keep interior surfaces clean. Blot interior surfaces dry after each use to prevent local hot spots and corrosion. Clean spills immediately.
Ventilation – Microwave devices used in the clinical histology laboratory should be placed in an approved ventilation hood to contain airborne contaminants and potentially infectious agents. Microwave devices used outside of a fume hood should have an integral fume extractor that is certified by the manufacturer for use in a clinical laboratory (check owner’s manual). Microwave devices may be used outside of a hood with nonhazardous reagents (e.g., water, certain biological stains) determined by the user’s institution.
Do yearly inspections of a microwave’s fume exhaust system (check owner’s manual). Flammable and/or corrosive reagents must be removed from the fume hood prior to microwave device operation to prevent ignition of the reagents or chemical damage to the electronic safety systems in the device.27 Microwave devices without a built-in exhaust should be placed six inches from the plane of the hood face and not block airflow to slots of the baffle.45 Sash height should be adjusted to the lowest possible position to maximize containment (see the institutional safety officer for this determination). Routine performance tests on ventilation hoods such as face velocity and smoke visualization are required on ventilation hoods containing microwave devices and microwaves with extractor fans connected to a ventilation hood or other exhaust system.46
Leakage – Have certified personnel do annual monitoring for microwave leakage (<5 mW of microwave radiation per square centimeter at 5 cm from the surface). This safety check should be done to meet appropriate radiation regulatory standards for the institution.
Regularly inspect and clean dirty microwave door seals. Do not operate a microwave with any evidence of damaged door frames, hinges, or door latches.
Spills – For some applications, a secondary container may be used to collect spills (e.g., tray or plastic bag with a vent). Operators must use extra caution when using secondary containers not specifically designed for microwave procedures due to the higher risk of container leakage and contamination. NOTE: Secondary containers are very important when transporting samples to and from the microwave device.
Pressurization during microwave procedures can only be done in devices approved by the manufacturer for this purpose. In particular, containers with screw-type cover lids should not be used. A thorough discussion of the safety codes and standards relevant to pressurization vessels is available.27
Handling – Use utensils designed to handle containers after microwave heating to protect the operator from burns. Thermal mitts should be used to prevent thermal burns from handling containers after microwave heating. Chemically resistant gloves should be used to prevent skin exposure to hazardous chemicals or their vapors, which may have contaminated the outside of the container during microwave heating.
Use containers made from microwave-compatible materials (e.g., polyethylene, polypropylene, PTFE, PFA, borosilicate glass). NOTE: Use caution with laboratory glassware as trace amounts of lead oxide can lead to overheating and breakage. Metal placed alone in a microwave cavity will cause arcing.
Temperature – Monitor temperature to prevent overheating and specimen damage.
Temperature measurement devices must be manufacturer approved for use in a microwave cavity.
Electrical Safety Microwave devices should have UL, , or CSA certification for laboratory use.

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 11
4.7 Microwave Safety Inspection A safety inspection of the microwave device should be done on a regular basis, determined by the laboratory supervisor and the institution’s safety officer. Table 5 provides a template of a microwave device survey data sheet for use in microwave safety inspection. Table 5. Microwave Device Survey Data Sheet
Microwave Device Survey Data Sheet
Date: Department: Responsible Person: Location of Unit: Serial/ID#: Survey Instrument: Control Limit (1): 5 mW/cm2
Inspection Checklist
Yes No N/A Warning sign for radio frequency radiation posted Additional information or precautions included on warning label of microwave Safety interlock prevents the device from operating if the door is opened Instrument is inspected periodically to ensure proper condition (e.g., corrosion) Device is maintained in a sanitary condition A qualified authority certified in using microwave leakage instrumentation should determine microwave leakage of all microwave devices in the laboratory. Inexpensive microwave leakage detectors typically result in false-positive leakage readings and are not recommended. Call a qualified service representative to determine the cause and repair of any leakage. Do not attempt to repair the device yourself. DO NOT USE THE DEVICE UNTIL IT HAS BEEN REPAIRED. The institutional radiation safety officer will typically take leakage readings at a distance of 5 cm from the surface of the unit with a 100 mL water load in place while the device is operating at maximum power (see Figure 1). In addition to surveying leakage around the door and frame, other locations that must be checked for leakage include outlets in the device for ventilation tubes and thermocouple lines. Table 6 provides a template for recording microwave leakage readings.
5
1 2 3
7 8 9
64
Figure 1. Diagram of Microwave Door and Door Frame

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 12
Table 6. Template for Recording Microwave Leakage Readings
Door closed readings in mW/cm2
Position # Reading
1 2 3 4 5 6 7 8 9
Maximum reading _________ mW/cm2
Surveyed by: ___________________________ 5 Principles of Microwave-Accelerated Methods This section is intended for readers interested in learning about the principal features and operation of a microwave device and the mechanisms of microwave heating. This section provides basic background information for the recommendations presented in Section 6. The principal features of a microwave unit are illustrated in the cutaway diagram shown in Figure 2. The primary components include: (A) control pad; (B) power supply; (C) magnetron; (D) wave guide; (E) distributor; and (F) unit door and walls.47, 48
Figure 2. Principle Features of a Microwave Oven
Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 13
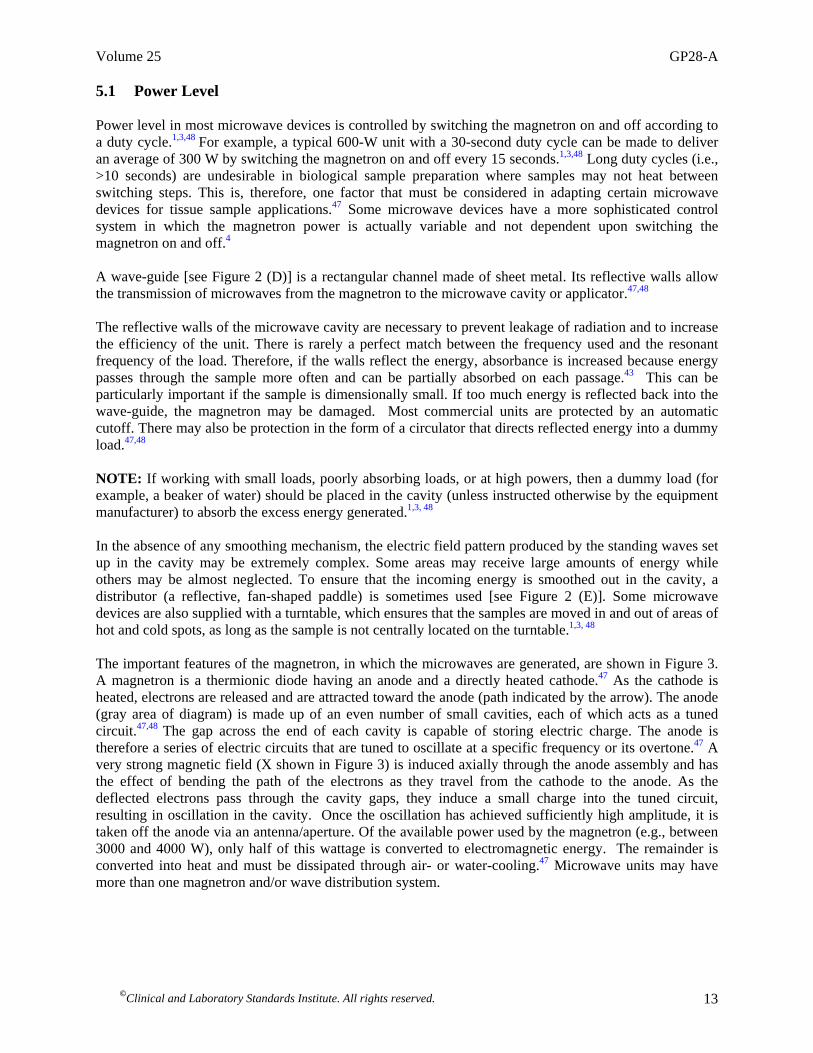
5.1 Power Level Power level in most microwave devices is controlled by switching the magnetron on and off according to a duty cycle.1,3,48 For example, a typical 600-W unit with a 30-second duty cycle can be made to deliver an average of 300 W by switching the magnetron on and off every 15 seconds.1,3,48 Long duty cycles (i.e., >10 seconds) are undesirable in biological sample preparation where samples may not heat between switching steps. This is, therefore, one factor that must be considered in adapting certain microwave devices for tissue sample applications.47 Some microwave devices have a more sophisticated control system in which the magnetron power is actually variable and not dependent upon switching the magnetron on and off.4 A wave-guide [see Figure 2 (D)] is a rectangular channel made of sheet metal. Its reflective walls allow the transmission of microwaves from the magnetron to the microwave cavity or applicator.47,48 The reflective walls of the microwave cavity are necessary to prevent leakage of radiation and to increase the efficiency of the unit. There is rarely a perfect match between the frequency used and the resonant frequency of the load. Therefore, if the walls reflect the energy, absorbance is increased because energy passes through the sample more often and can be partially absorbed on each passage.43 This can be particularly important if the sample is dimensionally small. If too much energy is reflected back into the wave-guide, the magnetron may be damaged. Most commercial units are protected by an automatic cutoff. There may also be protection in the form of a circulator that directs reflected energy into a dummy load.47,48 NOTE: If working with small loads, poorly absorbing loads, or at high powers, then a dummy load (for example, a beaker of water) should be placed in the cavity (unless instructed otherwise by the equipment manufacturer) to absorb the excess energy generated.1,3, 48 In the absence of any smoothing mechanism, the electric field pattern produced by the standing waves set up in the cavity may be extremely complex. Some areas may receive large amounts of energy while others may be almost neglected. To ensure that the incoming energy is smoothed out in the cavity, a distributor (a reflective, fan-shaped paddle) is sometimes used [see Figure 2 (E)]. Some microwave devices are also supplied with a turntable, which ensures that the samples are moved in and out of areas of hot and cold spots, as long as the sample is not centrally located on the turntable.1,3, 48 The important features of the magnetron, in which the microwaves are generated, are shown in Figure 3. A magnetron is a thermionic diode having an anode and a directly heated cathode.47 As the cathode is heated, electrons are released and are attracted toward the anode (path indicated by the arrow). The anode (gray area of diagram) is made up of an even number of small cavities, each of which acts as a tuned circuit.47,48 The gap across the end of each cavity is capable of storing electric charge. The anode is therefore a series of electric circuits that are tuned to oscillate at a specific frequency or its overtone.47 A very strong magnetic field (X shown in Figure 3) is induced axially through the anode assembly and has the effect of bending the path of the electrons as they travel from the cathode to the anode. As the deflected electrons pass through the cavity gaps, they induce a small charge into the tuned circuit, resulting in oscillation in the cavity. Once the oscillation has achieved sufficiently high amplitude, it is taken off the anode via an antenna/aperture. Of the available power used by the magnetron (e.g., between 3000 and 4000 W), only half of this wattage is converted to electromagnetic energy. The remainder is converted into heat and must be dissipated through air- or water-cooling.47 Microwave units may have more than one magnetron and/or wave distribution system.

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 14
Figure 3. Magnetron 5.2 Energy Absorption Mechanisms and Reaction Conditions Absorption of microwave radiation by samples and solutions is a phenomenon controlled by fundamental thermodynamic properties and is entirely different from conventional heating mechanisms.49,50 In conventional histology procedures, “standard devices” (such as hot plates, heating mantles, heating blocks, and conventional heat laboratory units) conduct heat to the reaction vessel. The solution is subsequently heated only through direct contact with the vessel walls.49,50 The heat is distributed via convection currents throughout the reagent-sample mixture. Because of the nature of this process, these heating methods are relatively slow. Hot-plate procedures are limited by the boiling points of the solutions. In addition, there can be variations between laboratories as a result of changes in atmospheric pressure, colligative properties (convection), and conductive heating properties of conventional apparatuses.49,50 In contrast, the use of microwave irradiation has a more direct, and thus controllable, heating mechanism and is less susceptible to the variables mentioned previously. Microwave systems use direct absorption of microwave radiation through essentially microwave-transparent vessel materials. Atmospheric pressure microwave systems can generate more stable temperature conditions and are not limited by heating mechanisms of convection or conduction.49,50 In microwave heating, energy is directly transferred to absorbing molecules in both the sample and reagents. An examination of the role played by each of the absorption mechanisms will assist the end user in understanding why unique conditions are achieved in microwave systems. There are two primary microwave-absorbing mechanisms: ionic conductance and dipole rotation. In simplified terms, ionic conductance refers to the phenomenon by which ions in solution migrate when an electromagnetic field is applied. The solution resistance to the free flow of ions results in friction that heats the solution. This mechanism is much less dependent on microwave frequency than is the dipole rotation mechanism. Dipole rotation is the alignment of a molecule dipole with the applied field. Molecular “friction” results from the very rapidly forced molecular movement caused by the oscillation of the applied field. At 2450 MHz, the dipoles align (lose entropy) and then randomize (gain entropy) 4.9 x 109 times per second, resulting in fast, efficient, and thermodynamically predictable power absorption.49,50

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 15
Water, methanol, and ethanol are examples of molecules likely to be used for tissue preparation. Microwave absorption by polar reagents (charged molecules) is very high. The importance of this information will be discussed in greater detail in Section 7.3.2. 6 Recommendations for Documenting Microwave Methods The reproducibility of microwave methods is often hampered by inadequate documentation. Far too frequently, microwave methods have not been documented well enough to adequately reproduce methods. Improved documentation could increase the usefulness of the method in histopathology laboratories. The following section will discuss what is critical to properly document microwave procedures. An analogy of microwave method documentation can be drawn from a description of hot-plate certification. Early procedures for hot plates most likely directed the user to heat the sample until “hot.” However, probably no information regarding what temperature or how long to run the process was specified. Similarly early microwave methods often instructed the client to heat the vessel at a designated power until the desired result was achieved.49 A completely documented microwave method will enhance the likelihood for reproducible results independent of the specific microwave unit. 7 Critical Descriptors for Microwave-Accelerated Procedures The most critical descriptors necessary to reproduce a microwave method are organized into four major headings: temperature, power, specimen handling, and time. Subsequent sections of this guideline elaborate on the descriptions of each of the categories outlined in Table 7.
Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 16
Table 7. Critical Descriptors for Microwave-Accelerated Procedures Temperature Control
• Temperature Measurement • Initial Temperature • Final Temperature (maximum temperature control)
Microwave Power • Line Voltage • Magnetron Cycling On and Off (partial and continuous powers) • Water Load • Determination of Microwave Power Output
Specimen Handling • Specimen Container
—Location —Dimensions —Composition —Multiple Samples —Water Loads and Other Microwave Absorbers
• Specimen Immersion —Solution Composition —Multiple Containers —Solution Mixing
• Samples —Grouping Samples of Similar Composition —Position of the Sample Within the Container —Sample Size
Process Time • Total Time • Time at Temperature
7.1 Temperature Control and Measurement
Temperature control is the single most important variable in a microwave procedure. The field of microwave sample preparation has moved toward using temperature feedback as the most widely accepted way to gain reproducible and accurate results. However, temperature measurement in a microwave environment is complicated by the nature of how microwave energy heats samples and by the type of probes that can be used in a microwave device. Variation of temperature in microwave-exposed materials depends on exposure level, the dielectric properties of the load, the thermal properties of the materials, and other physical properties such as vaporization, size of the object in relation to microwave frequency, the presence of other microwave absorbers in the vicinity of the sample (i.e., a water load), and the lack of homogeneity of the sample.3 7.1.1 Measuring Microwave Heating of Samples Insight into the complexity of measuring microwave heating of samples is provided below. 7.1.1.1 Exposure Level Microwave field intensity is not constant throughout the microwave cavity. Nonuniform microwave field patterns are present in all multimode microwave cavities. These varying power densities change with location, time, and the sample placement in the cavity. Since the variations in the field caused by absorbing samples cannot be modeled or predicted, methods are employed to increase the homogeneity of the field. Two such devices are the mode stirrer and the turntable or carousel that rotates the sample through the microwave field to evenly distribute the microwave energy. Field intensity is not uniform
Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 17
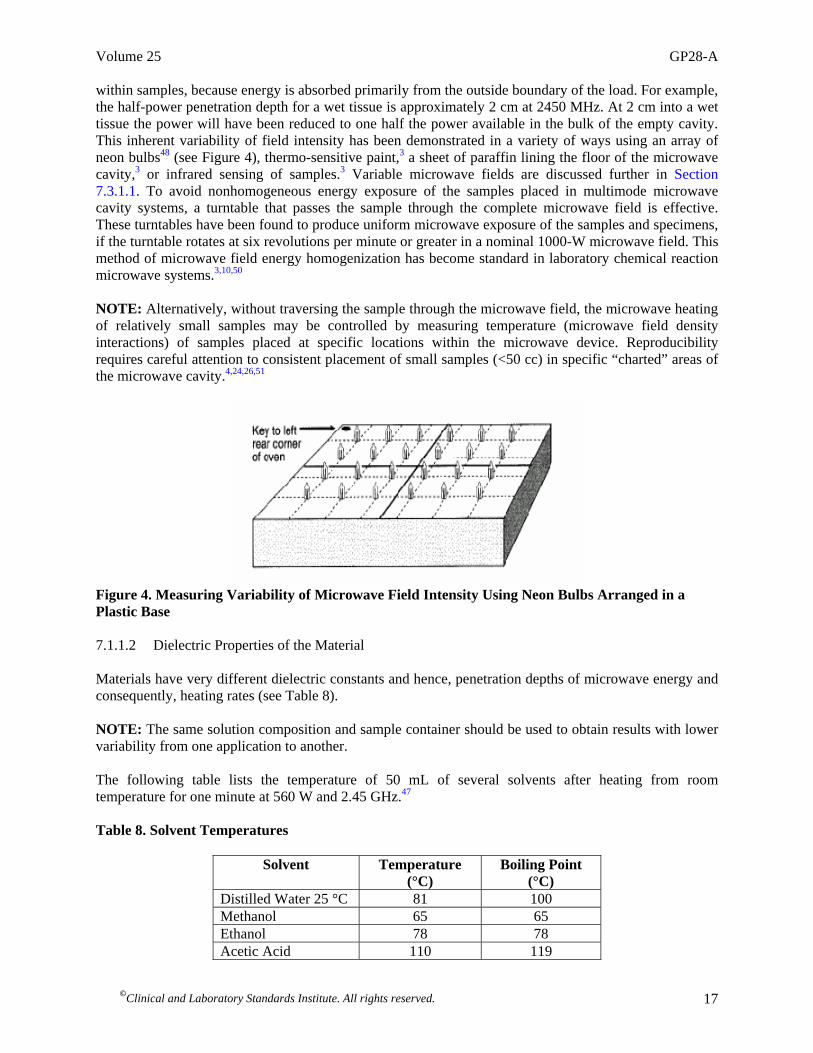
within samples, because energy is absorbed primarily from the outside boundary of the load. For example, the half-power penetration depth for a wet tissue is approximately 2 cm at 2450 MHz. At 2 cm into a wet tissue the power will have been reduced to one half the power available in the bulk of the empty cavity. This inherent variability of field intensity has been demonstrated in a variety of ways using an array of neon bulbs48 (see Figure 4), thermo-sensitive paint,3 a sheet of paraffin lining the floor of the microwave cavity,3 or infrared sensing of samples.3 Variable microwave fields are discussed further in Section 7.3.1.1. To avoid nonhomogeneous energy exposure of the samples placed in multimode microwave cavity systems, a turntable that passes the sample through the complete microwave field is effective. These turntables have been found to produce uniform microwave exposure of the samples and specimens, if the turntable rotates at six revolutions per minute or greater in a nominal 1000-W microwave field. This method of microwave field energy homogenization has become standard in laboratory chemical reaction microwave systems.3,10,50
NOTE: Alternatively, without traversing the sample through the microwave field, the microwave heating of relatively small samples may be controlled by measuring temperature (microwave field density interactions) of samples placed at specific locations within the microwave device. Reproducibility requires careful attention to consistent placement of small samples (<50 cc) in specific “charted” areas of the microwave cavity.4,24,26,51
Figure 4. Measuring Variability of Microwave Field Intensity Using Neon Bulbs Arranged in a Plastic Base 7.1.1.2 Dielectric Properties of the Material Materials have very different dielectric constants and hence, penetration depths of microwave energy and consequently, heating rates (see Table 8). NOTE: The same solution composition and sample container should be used to obtain results with lower variability from one application to another. The following table lists the temperature of 50 mL of several solvents after heating from room temperature for one minute at 560 W and 2.45 GHz.47 Table 8. Solvent Temperatures
Solvent Temperature (°C)
Boiling Point (°C)
Distilled Water 25 °C 81 100 Methanol 65 65 Ethanol 78 78 Acetic Acid 110 119

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 18
7.1.1.3 Antenna Properties of the Load This property is determined by the size of the sample relative to the wavelength of the microwave energy.52 For example, small droplet volumes do not absorb microwave energy as well as larger volumes. Also, tall samples do not absorb microwave energy as well as flat samples. NOTE: The same container size and shape and solution volume should be used to obtain results with lower variability from one application to another. 7.1.1.4 Thermal Properties of the Material The heat capacity of the object determines how quickly and evenly an object heats. Water has a higher specific heat than alcohol and therefore, requires more energy and time to heat than alcohol. NOTE: The same solution composition should be used to obtain results with lower variability from one application to another.
7.1.1.5 Other Physical Properties Vaporization is important with respect to small droplets typically used in histochemical procedures. The combination of large surface area and evaporative cooling determine the rate at which a small sample heats. NOTE: The same volume of sample should be used to obtain results with lower variability from one application to another. Again, the point must be emphasized that microwave heating is not uniform within the microwave cavity or within the samples.1,3 A single temperature measurement is rarely useful in process control. It is also important to note that rotating tables and mode stirrers reduce but do not eliminate variability in heating between multiple sample containers. Many laboratory-grade microwave units have a feature in which an aerator or magnetic stirrer is used to mix fluid during microwave heating. This approach has proven effective in minimizing temperature variation within a single, large volume. However, the aerator does not equilibrate temperature variation between containers located in different locations within the microwave cavity. NOTE: Independent temperature measurement should be performed in each sample container. 7.1.2 Temperature Measurement Devices Currently, five types of temperature measurement devices are used commercially in laboratory microwave systems for the direct measurement of the reaction temperature: thermocouples, fiber optics, infrared (IR), gas-filled bulbs, and liquid crystal temperature strips (LCTS). Each of these temperature measurement systems ideally overcomes the inherent problems and limitations of working in an electromagnetic field. 7.1.2.1 Thermocouple Measurement Devices Thermocouple measurement devices have been used for measuring temperatures for many years. In an electromagnetic field, this measurement can occasionally lead to problems when sensors are not correctly engineered. When thermocouples are exposed to microwaves, the microwaves couple with the thermocouple measurement circuitry.53 Errors are produced when the metal surface interacts with the electromagnetic field. A combination of shielding, grounding the shielding to the microwave cavity wall,

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 19
and electroplating the thermocouple with gold either eliminates or minimizes these errors.54 The gold-plated shielding essentially removes the thermocouple from the electromagnetic field. After calibration, thermocouples are useful from 0 °C to 400 °C in microwave systems, and typically are accurate to ±0.1 °C.49 The cost of these devices is low.
Many microwave units have a basic thermocouple measurement device built into the unit. Inexpensive probes are usually similar in dimension to meat probes in a domestic microwave unit. Such probes may only have an accuracy of ±5 °C and may be difficult to place in small sample containers.49 These probes are more likely to cause arcing and secondary heating (due to electric surface currents) of samples in contact with the metal probe during microwave irradiation. Built-in temperature probes are designed to monitor sample heating, but only of one sample container at a time. Stand-alone thermocouple measurement systems can be purchased at low cost, but they can only be used to measure temperature of samples after they have been removed from the microwave cavity.
CAUTION: Do not place any wire, such as a thermocouple, into a microwave device not specifically permitted by the manufacturer. Without grounding the shielding to the cavity wall, microwave energy can be transmitted along the surface of the shielding and into the laboratory.55 7.1.2.2 Fiber-Optic Systems Fiber-optic systems are microwave transparent and nonperturbing to the microwave field. Fiber-optics has been used in phosphorus-based and remote IR temperature sensors. Phosphorus fiber-optic sensors use a light source outside of the microwave cavity that emits an excitation wavelength that travels through the fiber-optic cabling to a phosphor tip.49 The measurement system converts the temperature-dependent fluorescent decay signal into a temperature measurement by comparing the decay rate with calibration values.56 After calibration, phosphorus fiber-optic thermometers are linear from 0 to 250 °C in microwave systems (dependent on the specific phosphor and fiber-optic cabling). They typically have an accuracy of ±2 °C, down to ±0.2 °C with calibration near the measurement temperature. These systems can measure multiple sample vessels at a time. The cost of these systems is very high.
7.1.2.3 Infrared Temperature Sensors Infrared (IR) temperature sensors have been used for direct and indirect temperature measurements. Direct IR sensors use fiber optics to directly measure the solution temperature.49 Indirect IR sensors measure the temperature of the sample vessel, usually the bottom,57 by the IR emission. The temperature of the sample vessel may lag behind the temperature of the solution.
IR sensors may, in the future, be adapted to measure the temperature of multiple sample vessels. As the turntable revolves, the IR sensor would measure the temperature of each vessel. If any one vessel surface reaches the selected target temperature, the microwave power would be shut off until the temperature has dropped below the programmed level. The cost of IR systems is typically medium to high. 7.1.2.4 Gas-Filled Bulb Thermometers Gas-filled bulb thermometers have recently been introduced.57 The measurement of temperature with these gas-filled bulbs is based on the gas law principle; the temperature is proportional to the internal gas pressure. After calibration, glass-bulb thermometers are linear from 0 to 250 °C and have an accuracy between ±2 and 5 °C.49 The cost of these devices is low.
7.1.2.5 Liquid Crystal Temperature Strips Liquid crystal temperature strips (LCTS) can measure temperature of the sample(s) or the sample vessel(s) (depending on placement of the strip) during microwave irradiation.48 LCTS can be monitored

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 20
during irradiation by direct observation through the microwave unit window or after sample removal from the unit cavity. LCTS typically appear black, but a bright green color becomes prominent when a temperature specific to the reaction temperature of the particular crystal on the strip is attained. Accuracy is within ±5 °C. There is no feedback control to the microwave device. The cost of LCTS is typically very low, and they are reusable. 7.1.3 A Recommended Temperature Measurement System
An electronic temperature probe should be accurate to ±2 °C and should be used according to the manufacturer’s recommendations and specifications. The end user should check these instruments periodically for accuracy. Many microwave devices have a single shielded microwave probe. This is useful for process control within a single container, but it is not capable of determining temperature in multiple containers. An independent, external, electronic temperature probe should be used to determine the temperature of a solution or sample immediately after the sample is removed from the microwave device. These temperature measurements can be used to troubleshoot areas within the microwave device in which there are insufficient heating or overheating of specimens (see Table 9). NOTE: Repeating the measurement three times, and using the average reading, will provide estimates with low uncertainty. For example, if the average temperature change were about 20 °C, experimental data such as 19 °C, 20 °C, and 21 °C would be reasonable just from the measurement aspect (this does not take into account any other source of uncertainty or variability). Table 9. Selecting an Electronic Temperature Probe for Microwave Procedures
Parameter Rationale Probe length ~ 1 cm Small enough to measure temperature changes in discrete areas
of small samples and solution volumes Probe equivalent to a 25-gauge needle diameter or thinner
Minimal mass so that it can quickly respond to temperature changes before the sample cools
+1.5 °C accuracy Immunohistochemical procedures require the most stringent temperature measurements
Response within 10 seconds Rapid probe response is essential for measuring temperature accurately within small sample volumes or multiple sample containers
Minimum 18” flexible length between probe and base unit
Facilitates ease of rapid probe placement
7.1.4 Initial Irradiation Temperature If a microwave device is not equipped with an accurate temperature control mechanism, then the laboratory personnel should adopt the practice of using solutions at the same starting temperatures for every use.
7.1.5 Final (Maximum) Irradiation Temperature The precise final temperature parameters supplied by the manufacturer or contained in published protocols should be followed. The temperature endpoint for tissue fixation is generally below 65 °C to prevent collagen denaturation and sample shrinkage. Most special stains in histology are done at a temperature below 60 °C.

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 21
Alternatively, staining and antigen retrieval procedures generally require final sample temperatures above 90 °C. NOTE: This parameter depends on the specific procedure being followed. 7.2 Microwave Power The consistency of the power output from a microwave device is directly related to the constancy of the line voltage to the unit and the performance of the magnetron. A simple calorimetric method can be used to determine microwave power output by the device (see Section 7.2.3). 7.2.1 Regulated Electrical Line Voltage on a Dedicated Circuit Microwave equipment should be used on a dedicated electrical circuit. Check with the institution’s electrical department for more information. Magnetron output wattage is dependent on input line voltage. Variance (e.g., decreased line voltage from the electrical utility company [brown outs]) will affect microwave power output. 7.2.2 Water Load
A water load is used as the primary absorber of microwave energy in a microwave. Recommendations contained in published protocols or in instructions supplied by the manufacturer should be followed. Some microwave devices can be damaged if they are operated with a solution volume below their minimum recommended by the manufacturer. This is especially important when using microwave devices for heating microliter volumes of reagents for certain immunostaining procedures. Other methods have been developed to smooth out nonuniform microwave field patterns.58
7.2.3 Power Output Determination Measure microwave unit power output to determine if the magnetron is functioning properly. These measurements should be performed at initial instrument set-up and quarterly thereafter. Magnetrons and power supply ratings vary due to manufacturing tolerances by as much as 10% between microwave units, after repair, and over the lifetime of the instrument.48 7.2.3.1 Method to Determine Power Output of a Large-Cavity Microwave Device The following steps describe a method to determine the power output of a large-cavity microwave device: (1) Place 1 L of distilled water in a 1-L narrow-mouth plastic bottle in the center of the microwave. NOTE: A narrow-mouth bottle is used to minimize heat loss from the container.
(2) Adjust the initial temperature to 25 °C ± 1 °C. (3) Irradiate the uncovered bottle for two minutes at 100% power.

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 22
(4) Carefully remove the bottle from the microwave device and place an appropriate cover of plastic or foil over the mouth of the container.
(5) Invert the container or use a magnetic stirrer to mix water for five seconds immediately after
irradiation to reduce temperature variation in the heated sample. (6) Measure the final temperature. NOTE: Perform the procedure three times to obtain sufficient readings to average. Procedures must be reported in terms of actual microwave power, not percentages set on the microwave unit. The following formula should be used: (change in temperature) x 35 = power in watts (35 is a constant for converting between calories and power). NOTE: If temperature measurement varies by more than 2 °C for a 700-W microwave device, an error of greater than 10% can result between sample processing batches. (18 °C x 35 = 630 W; 20 °C x 35 = 700 W; 22 °C x 35 = 770 W. Mean and standard deviation of three measurements is 700 W ± 70 W. 70/700 = 10%). Since a temperature difference is measured and linearity of the thermometer within the range is a reasonable assumption, the absolute accuracy of the thermometer is less important.49
7.2.4 Magnetron Duty Cycle (Magnetron “On-Time”) Longer cycle times in some microwave devices do not permit smooth transitions of temperature. Microwave devices with shorter controllable duty cycles or continuous variable power should be selected for use.
Lack of attention to the duty cycle settings can lead to overheating samples. For example, if the duty cycle is relatively long, at reduced power, the time that the magnetron is both on and off is longer, resulting in possible initial overheating followed by significant heat loss causing temperature swings in the sample.3,48 Some microwave devices use continuous variable power and do not have a duty cycle. Users should follow the manufacturer’s recommendations. 7.3 Specimen Handling Several factors in specimen handling will determine the variability of a procedure including container position, quantities of the solutions, and the number and types of microwave vessels. 7.3.1 Specimen Container 7.3.1.1 Container Location The container location should be marked on the microwave device floor to ensure reproducible container placement. A useful guide is an alphanumeric grid (see Figure 5) placed on the floor of the microwave device (see Figure 6).48

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 23
Figure 5. Alphanumeric Grid
Figure 6. Placement of Alphanumeric Grid for Determining Container Location The alphanumeric grid can be made from a plastic sheet with letters written along the right and left columns. Numbers are written along the top and bottom rows. The grid spacing is 1 cm. A large dot is marked in the top left corner to key the alphanumeric grid to the left rear corner of the microwave cavity (see Figures 5 and 6).
Microwave power can vary significantly within a microwave (see Figure 7). Wickersheim, et al showed a 70 °C difference in temperature within a 2-cm radius in a microwave oven56 (see Figure 8). A turntable does not eliminate these hot and cold spots; it simply circulates the sample(s) through these areas. Some laboratory microwave devices are designed for consistent sample placement and do not require an alphanumeric grid (check with the microwave device manufacturer).
Figure 7. Variance in Microwave Power

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 24
40
78
60
77
100
62
63
109
92
100
110
99
90
79
65
94
89
66
98
103
115
68
92
82
50
78
120
44
84
90
80
55
85
62
64
130
58
Back Wall of Oven Cavity
Front Door of Oven
y/cm
30
20
10
0
0 10 20 30
x/cm Figure 8. Microwave Temperature Differences Within a 2-cm Radius. Numeric readings are temperature, °C. (From Wickersheim K., M. Sun, and A. Kamal, 1990. A small microwave E-field probe utilizing fiberoptic thermometry. Journal of Microwave Power and Electromagnetic Energy. 25(3):141-148. Reprinted courtesy of the International Microwave Power Institute (Wickersheim, 1990). 7.3.1.2 Container Dimensions
The smallest container possible that the procedure will permit should be used. Do not interchange containers with different dimensions for a given procedure. In addition, the aspect ratio of the container used to hold the solution is important, i.e., for some given volume of solution, short, wide containers absorb microwave energy more efficiently than tall, narrow containers.48,59 Fifty to eighty percent of microwave energy is absorbed within the first 2 cm of a solution.48,59 Therefore, microwave heating may not be uniform throughout the volume of a solution. Some experts recommend using rectangular containers, because cylindrical containers may focus microwave energy (e.g., similar to a lens), resulting in sample overheating.59,60 7.3.1.3 Container Composition
Use microwave-transparent materials such as ceramics, sodium borosilicate glass, unleaded quartz, fluoropolymers, and nonpolar plastics like polypropylene, polyethylene, and PTFE compounds. Microwave-transparent materials do not absorb microwave energy and permit more uniform transmission of power to the sample.

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 25
7.3.1.4 Number of Containers When more than one container is heated in a microwave device, it is likely that the temperature will vary from container to container. Many experts recommend microwave units with a rotating table when heating multiple sample containers. The rotating table should rotate at six revolutions per minute.27 Another method for determining the best placement of multiple containers for uniform heating in the microwave cavity is by trial and error. Reproducible heating results depend on using consistent container placement, consistent load (with respect to container size, container shape, solution volume, and solution chemistry), and consistent bubble agitation within each container. Final irradiation temperature of each container is measured immediately after the microwave heating cycle ends. The locations of each container are marked on the floor of the microwave cavity with an indelible pen. This calibration should be checked periodically or immediately after a change is made to the microwave device.
Uneven distribution of microwave fields within the microwave cavity is the primary cause for uneven heating. Secondary causes include variation in airflow within the cavity and inconsistent agitation in the containers.
7.3.2 Specimen Immersion 7.3.2.1 Solution Composition in a Single Container Salt concentration, ionic conductivity, and polarity affect microwave absorption. An analytical-grade balance should be used to measure solution components. The balance should be calibrated to at least 1% accuracy.
Table 10 shows microwave (frequency 3 GHz) penetration depth (distance in which the intensity is reduced in half) in various solutions typically used in clinical laboratories. Table 10. Microwave (2.45 GHz) Penetration Depth in Various Materials (From Kok LP, Boon ME. Microwaves for the Art of Microscopy. Fourth revised edition. Leiden: Coulomb Press Leyden; 2003. Reprinted with permission).
Medium Depth Distilled water 25 °C 3.4 cm 0.1 M sodium chloride 2.0 cm Ethanol 7.0 cm Ethylene glycol 1.3 cm Epon resin 120 cm Paraffin wax (molten 55 °C) 150 m
7.3.2.2 Solution Composition in Procedures Using Multiple Containers The same solution should be used in all containers during a single procedure. Preparing the solution in bulk ensures a diluent of constant composition. Solutions with different compositions absorb microwave power differently (see Table 10). 7.3.2.3 Solution Agitation Solution agitation during microwave irradiation improves uniformity of sample heating. Examples of commonly used mixing methods are manual mixing by inverting the sample after it is removed from the microwave device or bubble agitation and magnetic stirring while the sample is in the microwave device (manufacturer dependent).
Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 26
Microwave energy is introduced through a wave-guide, thereby preferentially heating one surface of the container. Agitation prior to temperature measurement is necessary. 7.3.3 Samples 7.3.3.1 Grouping Samples of Similar Composition Samples with similar composition should be batch processed together. Fatty tissues (i.e., breast) and calcified tissues do not absorb microwave energy as readily as solid organ tissues such as liver (see Table 11).3 Table 11. 2.45 GHz Microwave Penetration Depth in Biological Tissues (From Kok LP, Boon ME. Microwaves for the Art of Microscopy. Fourth revised edition. Leiden: Coulomb Press Leyden; 2003. Reprinted with permission).
Medium Depth Muscle and skin 2.0 cm Fat and bone 9.0 cm
7.3.3.2 Position of the Sample Within the Sample Container
Specific procedures may require optimal positioning of the sample within its container.
Due to differences of absorption of microwave energy and shielding by some samples and reagents, position should follow guidelines for specific applications. For example, slides placed near other slides in a staining jar may receive less microwave energy from the field. Also, tissue samples in a fixative will receive more microwave exposure the closer they are to the outside wall of the container.
7.3.3.3 Sample Size
The smallest and thinnest sample size possible should be used. Thicker specimens require longer processing times. All sample preparation procedures are dependent on solution penetration and chemical reactivity with the biological sample.1,3,59 In addition, 80% of the microwave energy incident on a sample is absorbed within the first 1 cm of the sample depth. 7.4 Process Time Many published microwave protocols will distinguish between “total time” and “time at temperature.” 7.4.1 Total Time Total time defines the length of time that the specimen is exposed to microwave energy. This process includes the time it takes for the set temperature to be reached and the time the sample remains at that temperature. Increasing the power will decrease the total processing time. Heating time may be programmable on microwave devices by controlling power output or magnetron cycle time. Recommendations supplied by the manufacturer or contained in published protocols should be followed. 7.4.2 Time at Temperature Time at temperature is defined as the amount of time the sample remains in solution that has reached a preset incubation temperature. The time at temperature definition does not include the time needed to heat the sample to the preselected temperature. A temperature sensor is necessary for this function.

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 27
Multiple containers may not be maintained at the same temperature, because they are exposed to different microwave fields in different positions within the microwave cavity. This procedure is independent of the power setting. Recommendations supplied by the manufacturer or contained in published protocols should be followed. 8 Special Microwave Procedures Procedures that are often done in microwave devices and require additional explanation regarding control of parameters for reproducible results are described below. 8.1 Antigen Retrieval Protocol The antigen retrieval (AR) technique, which is predominantly based on high-temperature heating of tissues, is used as a nonenzymatic pretreatment for immunohistochemical staining of formalin-fixed, paraffin-embedded tissue sections. It has been widely applied in pathology and analytical morphology.18,22,23,60-63 (Please refer to the most current version of CLSI/NCCLS document MM4—Quality Assurance for Immunocytochemistry for additional information.) The use of a standardized AR protocol is recommended for all tissues that may have been over-fixed by exposure to formalin. Variables in the AR process include the choice of retrieval solution, pH, temperature, time, and heating method. Conventional heating in a laboratory dry-heat oven, microwave heating, pressure-cooking, steaming, and autoclaving all may give equivalent results if temperature and time are adjusted to optimal values. The microwave, pressure cooker, and steamer are easiest to use, but the final choice for each laboratory may be based upon availability of equipment and convenience. Once a heating method has been selected, each antibody procedure should be titrated to determine the optimal staining and retrieval conditions of the corresponding antigen, for tissues processed in that laboratory. A simple test panel (consisting of identical tissue samples) may be employed for this purpose, varying the pH and heating time to achieve accurate, true retrieval that is traceable to optimally fixed and processed tissue; one of the more commonly used retrieval solutions such as citrate buffer or Tris-HCl buffer with or without 5% (w/v) urea should be used. An example of this test battery approach is shown in Table 12.23 Table 12. Test Battery for Optimal pH and Heating Using Choice Antigen Retrieval (AR) Solution and Selected Heating Methods (Shi SR, Cote RJ, Yang C, et al. Development of an optimal protocol for antigen retrieval: A ‘test battery’ approach exemplified with reference to the staining of retinoblastoma protein (pRB) in formalin-fixed paraffin sections. J Pathol. Copyright© 1996. Pathological Society of Great Britain and Ireland. Reproduced with permission. Permission is granted by John Wiley & Sons Ltd. on behalf of the Pathological Society).
Heating Condition (Temperature x Time) pH Value of the Antigen Retrieval (AR) Solution
Mid-high (90 °C x 10 min)
High (100 °C x 10 min)
Super-high (>100 °C x 10 min)
Low (pH 1-2) Slide #1 Slide #4 Slide #7 Middle (pH 7-8) Slide #2 Slide #5 Slide #8 High (pH 9-10) Slide #3 Slide #6 Slide #9 8.1.1 Test Battery for Optimal pH and Heating The temperature of super-high at 120 °C may be reached by either autoclaving or microwave heating at a longer time or with a microwave-safe pressure cooker.64 In contrast, the low temperature of mid-high at 90 °C may be obtained by either a water bath or a microwave monitored with an electronic temperature probe or with LCTS. In addition to the nine slides used for this test battery, one more slide may be used for control without AR treatment. Tris-HCl buffer solution is recommended for this test; citrate buffer of pH 6.0 may be used to replace Tris-HCl buffer of pH 7-8, as the results are the same (see Table 12).64

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 28
Good immunohistochemical staining practice requires the use of valid positive and negative control tissues. For a discussion on the use of controls in IHC tests, please refer to the most current edition of CLSI/NCCLS document MM4—Quality Assurance for Immunocytochemistry. The antigen retrieval (AR) procedure: • is a controlled process that restores (recovers) antigenicity of proteins modified (or masked) by
fixation in formalin; and
• can be used to determine that the IHC result truly detects the presence or absence of target antigen (analyte) in the sample. If the IHC test is semiquantitative (i.e., 1, 2, 3+, or quantitative [in actual units of measure]) the IHC result after AR should be traceable to known samples that contain the target antigen (positive controls) and samples that lack the target antigen (negative controls).
– Examples of positive and negative tissue samples include human tumor samples that have been
analyzed with quantitative biochemical methods for the concentration of the target analyte, e.g., human breast cancer with biochemical analysis of estrogen and progesterone receptors; and human tumor cell lines with quantitative biochemical, immunological, and/or nucleic acid-based analyses (e.g., fluorescent in-situ hybridization [FISH]) of the target analyte (antigen).
– Normal human samples are excellent sources for positive and negative control samples. They may
be made into multiple tissue blocks and used as controls for all steps of the IHC testing process, including AR procedures.
The same “test battery” approach may be used for selected, preferred heating methods or preferred AR solutions by holding other variables (such as pH and time of heating) constant. The use of slide adhesives is recommended. In addition, do not allow slides to dry out during microwave staining; this can lead to artifacts in the background.

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 29
9 Template for Documentation of Microwave Methods The following template may be used for documentation of microwave methods.
Documentation of Microwave Methods
Procedure Name (e.g., fixation, staining, antigen retrieval [AR]) Microwave Device
Manufacturer: Model: Year: Rated Wattage: Actual Measured Wattage: Magnetron Cycle Time (if unit selection is available): Power Used for Procedure:
Process Time
Time at Temperature or Total Process Time: Sample
Sample Type (e.g., bone, fat, organ, plant, bacteria): Sample Dimensions: Typical Number of Samples Used:
Sample Container
Dimensions: Composition: Number of Containers Heated at One Time: Position of the Container Within the Cavity (alphanumeric coordinates): Use of a Water Load and Its Volume:
Sample Immersion
Solution Type (e.g., water, ethanol, salt concentration): Volume: Time in Solution:

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 30
10 Troubleshooting Results The troubleshooting guide summarizes key points in this document. The information presented here can be useful when introducing microwave procedures in the laboratory or customizing protocols for the microwave device. The guide summarizes results, possible causes of a particular problem, and trouble-shooting recommendations for microwave leakage, microwave fixation, microwave staining, microwave AR, and microwave curing of embedments. Table 13. Troubleshooting Guide48 Microwave Leakage:
Results Possible Causes Recommendations • Qualified inspection reveals
microwave leakage from device • Damage to door or frame • Faulty interlock switch • Wire leads from an external
thermometer are placed in door frame
• Corrosion/rust resulting in holes in the interior walls
• Do not use microwave • Call for service
• Sparks occur within microwave • Metal in microwave • Temperature probe is too close
to wall • Insufficient load
• Use plastic or glass in microwave
• Submerge tip of probe into water or specimen
• Add water load Microwave Fixation:
Results Possible Causes Recommendations • Nonuniform fixation of sample • Only edges of sample are fixed
• Sample is too large • Solution volume is too large
around sample • Excess heat around edges from
conductive heating • Sample placed in wrong
location of microwave • Microwave power is too low
• Improper infiltration
• Check power settings of microwave based on protocol and device power output
• Position sample based on published protocol
• Tissue dimensions ideally <0.3 cm thick x 1 cm2
• Minimize solution depth around sample to <1 cm
• Increase power or increase exposure time
• Bisect capsular specimens (lymph nodes, polyps)
• Bread loaf large specimens • Samples fragment during
irradiation
• Built-in temperature probe near samples results in localized overheating
• Place sample in a plastic tissue cassette to avoid contact with temperature probe
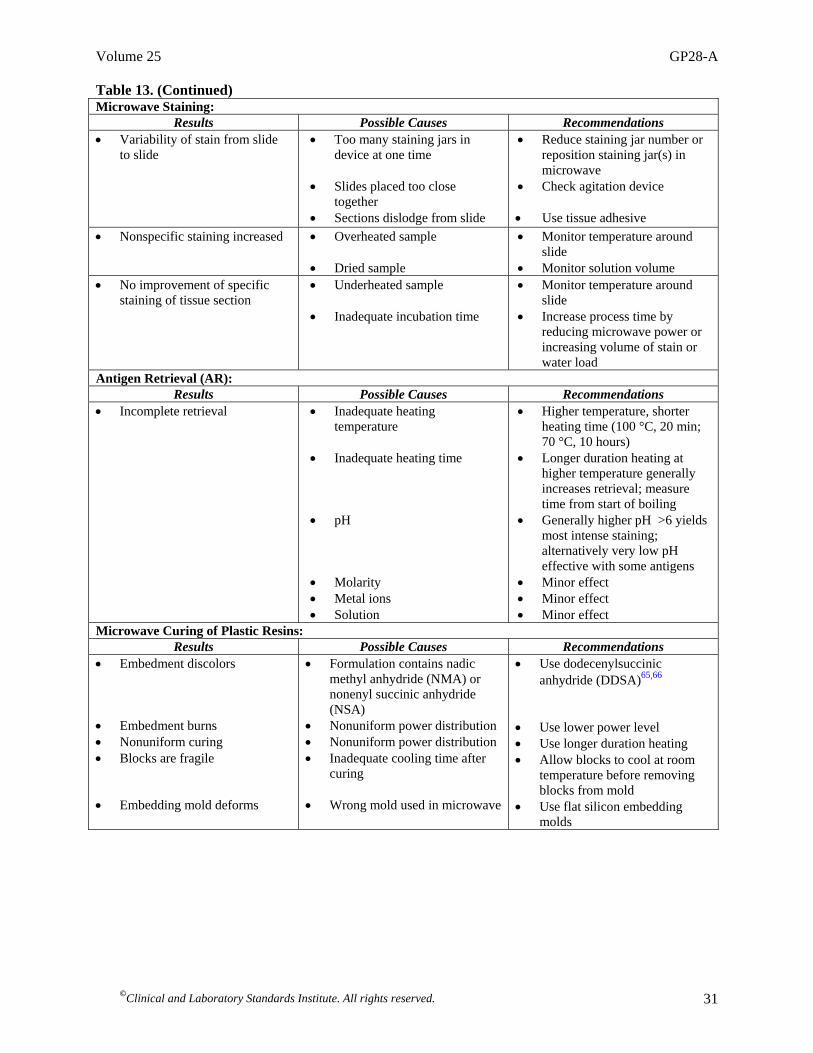
Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 31
Table 13. (Continued) Microwave Staining:
Results Possible Causes Recommendations • Variability of stain from slide
to slide • Too many staining jars in
device at one time • Slides placed too close
together • Sections dislodge from slide
• Reduce staining jar number or reposition staining jar(s) in microwave
• Check agitation device • Use tissue adhesive
• Nonspecific staining increased • Overheated sample • Dried sample
• Monitor temperature around slide
• Monitor solution volume • No improvement of specific
staining of tissue section • Underheated sample • Inadequate incubation time
• Monitor temperature around slide
• Increase process time by reducing microwave power or increasing volume of stain or water load
Antigen Retrieval (AR): Results Possible Causes Recommendations
• Incomplete retrieval • Inadequate heating temperature
• Inadequate heating time • pH
• Molarity • Metal ions • Solution
• Higher temperature, shorter heating time (100 °C, 20 min; 70 °C, 10 hours)
• Longer duration heating at higher temperature generally increases retrieval; measure time from start of boiling
• Generally higher pH >6 yields most intense staining; alternatively very low pH effective with some antigens
• Minor effect • Minor effect • Minor effect
Microwave Curing of Plastic Resins: Results Possible Causes Recommendations
• Embedment discolors • Embedment burns • Nonuniform curing • Blocks are fragile • Embedding mold deforms
• Formulation contains nadic methyl anhydride (NMA) or nonenyl succinic anhydride (NSA)
• Nonuniform power distribution • Nonuniform power distribution • Inadequate cooling time after
curing • Wrong mold used in microwave
• Use dodecenylsuccinic anhydride (DDSA)65,66
• Use lower power level • Use longer duration heating • Allow blocks to cool at room
temperature before removing blocks from mold
• Use flat silicon embedding molds

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 32
References 1 Login GR, Dvorak AM. Methods of microwave fixation for microscopy. A review of research and clinical applications: 1970-1992. Prog
Histochem Cytochem. 1994;27(4):1-127. 2 Leong AS-Y, Milios J, Duncis CG. Antigen preservation in microwave irradiated tissues: A comparison with formaldehyde fixation. J
Pathol. 1988;156:275-282. 3 Kok LP, Boon ME. Microwaves for the Art of Microscopy. 4th ed. Leyden: Coulomb Press; 2003. 4 Giberson RT, Demaree RS. Microwave Techniques and Protocols. Totowa, NJ: Humana Press; 2001. 5 Leong AS-Y, Daymon ME, Milios J. Microwave irradiation as a form of fixation for light and electron microscopy. J Pathol.
1985;146:313-321. 6 Login GR, et al. A novel microwave device designed to preserve cell structure in milliseconds. In: Snyder WB Jr., et al, eds. Microwave
Processing of Materials II. Pittsburgh, PA: Materials Research Society; 1991. 7 Barsony J, et al. Immunocytology with microwave fixed fibroblasts shows 1-alpha, 25-dihydroxyvitamin D3 dependent rapid and estrogen
dependent slow reorganization of vitamin D receptors. J Cell Biol. 1990;111:2385-2395. 8 Mizuhira V, Notoya M, Hasegawa H. New tissue fixation method for cytochemistry using microwave irradiation I. General remarks. Acta
Histochem Cytochem. 1990;18:501-523. 9 Medina MA, Deam AP, Stavinoha WB. Inactivation of brain tissue by microwave irradiation. In: Passonneau JV, et al, eds. Cerebral
Metabolism and Neural Function. New York, NY: Williams and Wilkins; 1980. 10 Kingston HMS, Haswell SJ, eds. Microwave-Enhanced Chemistry. Fundamentals, Sample Preparation, and Applications. Washington,
D.C.: American Chemical Society; 1997. 11 Mori T, et al. Improved power control during microwave heating in biological applications. Dent Mater J. 1992;11(2):197-203. 12 Barsony J, Marx SJ. Immunocytology on microwave-fixed cells reveals rapid and agonist-specific changes in subcellular accumulation
patterns for cAMP or cGMP. Proc Natl Acad Sci. 1990;87:1188-1192. 13 Boon ME, et al. The two-step vacuum-microwave method for histoprocessing. Eur J Morphol. 1995;33(4):349-358. 14 Kok LP, Boon ME. Ultrarapid vacuum-microwave histoprocessing. Histochem J. 1995;27(5):411-419. 15 Visinoni F, et al. Ultra-rapid microwave/variable pressure-induced histoprocessing. Description of a new tissue processor. J Histotechnol.
1998;21:219-224. 16 Yasuda K, et al. Application of ultrasound for tissue fixation: Combined use with microwave to enhance the effect of chemical fixation.
Acta Histochem Cytochem. 1992;25:237-244. 17 Leong AS, Sormunen RT. Microwave procedures for electron microscopy and resin-embedded sections. Micron. 1998;29(5):397-409. 18 Leong AS. International Lecture: Applications of Microwaves in Immunohistology. In: National Society for Histotechnology 23rd Annual
Symposium. Columbus, OH; 1997. 19 Leong AS. Microwaves in diagnostic immunohistochemistry. Eur J Morphol. 1996;34(5):381-383. 20 Leong AS-Y. Microwave fixation and rapid processing in a large throughput histopathology laboratory. Pathol. 1991;23:271-273. 21 Kok LP. Fundamentals of microwave-stimulated staining. In: Boon ME, Kok LP, eds. Standardization and Quantitation of Diagnostic
Staining in Cytology. Leyden: Coulomb Press; 1986. 22 Shi SR, Cote RJ, Taylor CR. Antigen retrieval techniques: Current perspectives. J Histochem Cytochem. 2001;49(8):931-937. 23 Shi SR, Cote RJ, Taylor CR. Antigen retrieval immunohistochemistry: Past, present, and future. J Histochem Cytochem. 1997;45(3):327-
343. 24 Login GR, Leonard JB, Dvorak AM. Calibration and standardization of microwave ovens for fixation of brain and peripheral nerve tissue.
Companion to Methods Enzymol. 1998;15(2):107-117. 25 Login GR, Tanda N, Dvorak AM. Calibrating and standardizing microwave ovens for microwave-accelerated specimen preparation. A
review. Cell Vision. 1996; 3(3):172-179. 26 Giberson RT, Demaree RS Jr. Microwave fixation: Understanding the variables to achieve rapid reproducible results. Microsc Res Tech.
1995;32:246-254.

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 33
27 Kingston HM, et al. Laboratory microwave safety. In: Kingston HMS, Haswell SJ, eds. Microwave-Enhanced Chemistry. Fundamentals,
Sample Preparation, and Applications. Washington, D.C.: American Chemical Society; 1997. 28 ISO. International Vocabulary of Basic and General Terms in Metrology. Geneva: International Organization for Standardization; 1993. 29 ISO. Accuracy (trueness and precision) of measurement methods and results – Part 1: General principles and definitions. ISO 5725-1.
Geneva: International Organization for Standardization; 1994. 30 ISO. Medical laboratories– Particular requirements for quality and competence. ISO 15189. Geneva: International Organization for Standardization; 2003. 31 CDC. Guidelines for Protecting the Safety and Health of Healthcare Workers. Cincinnati, OH. U.S. Department of Health and Human
Services; 1988. 32 Center for Microwave and Analytical Chemistry (C/MAC) SamplePrep Web™ at Duquesne University.
www.sampleprep.duq.edu/sampleprep. 33 OSHA. Nonionizing Radiation. 29 CFR §1919.97. U.S. Government Printing Office: Washington, D.C.; 2002. 34 CDRH. Food and Drugs: Records and Reports: Records to be Maintained by Manufacturers. 21 CFR §1002.30. U.S. Food and Drug
Administration. 35 CDRH. Food and Drugs: Notification of Defects or Failure to Comply. 21 CFR §1003. U.S. Food and Drug Administration; 2002. 36 CDRH. Food and Drugs: Repurchase, Repairs, or Replacement of Electronic Products. 21 CFR §1004. U.S. Food and Drug
Administration; 2002. 37 Thuery J. Microwave: Industrial, Scientific and Medical Applications. Norwood, MA: Artech House; 1992. 38 FDA. Performance Standards for Microwave and Radio Frequency Emitting Products. Microwave Ovens. 21 CFR §1030. U.S.
Government Printing Office: Washington, D.C.; 2002. 39 Federal Food, Drug, and Cosmetic Act: Section 201(h). 21 USC 321. 40 CDRH. Food and Drugs: Abbreviated Reports. 21 CFR §1002.12. U.S. Food and Drug Administration; 2002. 41 CDRH. Good Manufacturing Practice for Medical Devices. 21 CFR §820. U.S. Food and Drug Administration; 2002. 42 Kingston HM, Jassie LB. Safety guidelines for microwave systems in the analytical laboratory period. In: Kingston HM, Jassie LB, eds.
Introduction to Microwave Sample Preparation: Theory and Practice. Washington, D.C.: American Chemical Society; 1988. 43 Mudgett RE. Developments in microwave food processing. In: Schwartzberg HG, Rao M, eds. Biotechnology and Food Process
Engineering. New York, NY: Marcel Dekker, Inc.; 1990. 44 CDRH. Performance Standards for Microwave and Radio Frequency Emitting Products. 21 CFR §1030.12. U.S. Food and Drug
Administration; 2002. 45 American Industrial Hygiene Association. American National Standard for Laboratory Ventilation. ANSI/AIHAZ9.5-1992. 46 American Industrial Hygiene Association. American National Standard for the Recirculation of Air from Industrial Process Exhaust
Systems. ANSI/AIHA Z9.7-1998. 47 Mingos DMP, Baghurst DR. Applications of microwave dielectric heating effects to synthetic problems in chemistry. In: Kingston HMS,
Haswell SJ, eds. Microwave-Enhanced Chemistry. Fundamentals, Sample Preparation, and Applications. Washington, D.C.: American Chemical Society; 1997.
48 Login GR, Dvorak AM. The Microwave Toolbook. A Practical Guide for Microscopists. Boston, MA: Beth Israel Hospital; 1994. 49 Kingston HMS, et al. Environmental microwave sample preparation: Fundamentals, methods, and applications. In: Kingston HMS, Haswell
SJ, eds. Microwave-Enhanced Chemistry. Fundamentals, Sample Preparation, and Applications. Washington, D.C.: American Chemical Society; 1997:223-349.
50 Neas ED, Collins MJ. Microwave heating: Theoretical concepts and equipment. In: Kingston HM, Jassie LB, eds. Introduction to
Microwave Sample Preparation: Theory and Practice. Washington, D.C.: American Chemical Society; 1988:7-32. 51 Jensen FE, Harris KM. Preservation of neuronal ultrastructure in hippocampal slices using rapid microwave-enhanced fixation. J Neurosci
Methods. 1989;29:217-230. 52 Choi TS, et al. Advances in temperature control of microwave immunohistochemistry. Cell Vision. 1995;2(2):151-164. 53 Chakraborty DP, Brezovich IA. Error sources affecting thermocouple thermometry in RF electromagnetic fields. J Microw Power.
1982;17(1):17-28.

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 34
54 Kingston HM, Jassie LB, eds. Introduction to Microwave Sample Preparation Theory and Practice. American Chemical Society:
Washington, D.C.; 1988:(6)93-154. 55 Kingston HM, Jassie LB. Microwave energy for acid decomposition at elevated temperatures and pressures using biological and botanical
samples. Anal Chem. 1986;58:2534-2541. 56 Wickersheim KA, Sun MH, Kamal A. A small microwave E-field probe utilizing fiberoptic thermometry. J Microwave Power.
1990;25(3):141-148. 57 Lorentzen EM, Kingston HM. The advantage feedback controlled microwave assisted leaching under atmospheric pressure. In: Total
Microwave Processing Using Microwave Technologies. Federation of Analytical Chemistry and Spectroscopy Societies: Cincinnati, OH; 1995.
58 Giberson RT, Austin RL, Charlesworth J, Adamson G, Herrera GA. Microwave and digital imaging technology reduce turnaround times for
diagnostic electron microscopy. Ultrastruct Pathol. 2003;27(3):187-196. 59 Kok LP, Boon ME. Physics of microwave technology in histochemistry. Histochem J. 1990;22:381-388. 60 Cattoretti G, Suurmeijer A. Antigen unmasking on formalin-fixed paraffin-embedded tissues using microwaves: A review. Adv Anat Path.
1995;2:2-9. 61 Shi SR, Key ME, Kalra KL. Antigen retrieval in formalin-fixed, paraffin-embedded tissues: An enhancement method for
immunohistochemical staining based on microwave oven heating of tissue sections. J Histochem Cytochem. 1991;39(6):741-748. 62 Shi SR, Cote RJ, Taylor RC. Antigen retrieval immunohistochemistry and molecular morphology in the year 2001. Appl Immunohistochem
Molecul Morphol. 2001;9(2):107-116. 63 Leong AS, Milios J. An assessment of the efficacy of the microwave antigen-retrieval procedure on a range of tissue antigens. Appl
Immunohistochem. 1993;1(4):267-274. 64 Shi SR, Cote RJ, Yang C, et al. Development of an optimal protocol for antigen retrieval: A ‘test battery’ approach exemplified with
reference to the staining of retinoblastoma protein (pRB) in formalin-fixed paraffin sections. J Pathol. 1996;179(3):347-352. 65 Giammara BL, Birch DJ, Harper DO. Microwave polymerization of embedding resins for biological/biomedical electron microscopy. In:
Snyder WB, et al, eds. Microwave Processing of Materials II. Pittsburgh, PA: Materials Research Society; 1991:347-353. 66 Giammara B. Microwave embedment for light and electron microscopy using epoxy resins, LR White, and other polymers. Scanning.
1993;15:82-87.

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 35
Summary of Delegate/Consensus Comments and Subcommittee Responses GP28-P: Microwave Device Use in the Clinical Laboratory; Proposed Guideline General 1. The document should include microwave technology utilization in the blood bank. • This technology is outside the scope of this document. 2. Include comprehensive discussion(s) specific to the domestic microwave user. It should identify which procedures may be
suitable for domestic units (outside of regulatory limitations) in more detail than simply listing them in Table 2 and specifically how those methodologies may be carried out. Expound on the benefits of laboratory-grade microwave devices for certain applications, explaining why they are advantageous to the user in those specific instances.
• The document is a guideline regarding microwave device safety and reproducibility. The guideline reports well-
documented general principles that laboratory technicians can apply to any published protocol in any microwave device with an oven-like interior with the goal of improving reproducibility. This information is contained in Section 7, Critical Descriptors for Microwave-Accelerated Procedures and Section 10, Troubleshooting Results.
The document purposely does not describe specific methods, because these are already published in textbooks such as Kok LP, Boon ME. Microwaves for the Art of Microscopy. Leyden: Coulomb Press; 2003 and Giberson RT, Demaree RS. Microwave Techniques and Protocols. Totowa, NJ: Humana Press; 2001. Table 2 in the guideline refers to basic and advanced functionality of FDA- and OSHA-compliant microwave devices. The subcommittee thought it was important for laboratory technicians to also know this information, so they can make informed purchasing decisions depending on their intended applications.
3. Include a discussion of the limitations of domestic microwave devices and which methodologies are unsuitable for this type
of device and why. This information will allow those considering the purchase of microwave technology to make informed decisions appropriate for the procedures they intend to perform.
• This guideline is the first publication to collate, document, and discuss the limitations of domestic microwave ovens in
a hospital laboratory. Domestic microwave appliances do not meet FDA and OSHA guidelines for use in a hospital laboratory environment. Please refer to Section 4.2, Electrical Precautions.
4. Offer domestic microwave device users strategies to enable them to achieve reproducible results. • This information is outlined in Section 7, Critical Descriptors for Microwave-Accelerated Procedures and Section 10,
Troubleshooting Results. 5. This guideline calls it “immunohistochemistry” and uses the abbreviation IHC. The NCCLS document MM4-A uses the
word “immunocytochemistry” throughout. Though both are interchangeable, and though most histotechs seem to use the term “immunohistochemistry” or “IHC,” NCCLS should consider sticking with one of the terminologies for consistency.
• “Histo” refers to tissue seen at the light microscopy magnification, and “cyto” refers to cells seen at electron
microscope magnification. The term “immunohistochemistry” is more accurate in this document. 6. When written after a number, either use the word for a measurement (i.e., 400 Watts), or use the symbol (400 W) throughout
the document. This is varied throughout the document. • The symbol for a watts measurement (W) has been made consistent throughout the document.
Clinical and Laboratory Standards Institute consensus procedures include an appeals process that is described in detail in Section 8 of the Administrative Procedures. For further information, contact the Executive Offices or visit our website at www.clsi.org.

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 36
Section 2, Introduction 7. On page 1, last sentence, I would like to see this sentence rewritten to state, “Household microwave units are designed for
food preparation, and they are not certified for laboratory use; however, many laboratories have used them (effectively) for staining, heating agar, heat activated epitope retrieval, and drying slides, (as long as proper safety precautions are followed.)”
I think the average laboratorian trying to read this document will not understand what “Subpart S” or “Chapter V Subchapter A-Drug & Devices”; or 29CFR 1910 means. I think for the purposes of a user-friendly document, this sentence should be added in the text.
• The subcommittee acknowledges that domestic microwave ovens have been a cost-effective and successful piece of
equipment for many procedures in the laboratory. Their continued use is subject to the discretion of the individual laboratory and hospital administrators. However, since domestic microwave ovens unequivocally do not meet the electrical safety requirements of the FDA and OSHA for hospital laboratories, mention of domestic microwave oven use has been eliminated from this guideline.
This guideline is written for multiple audiences including laboratory technicians, microwave device manufacturers, microwave device resellers, compliance and safety officials, and administrators. Section 4.2, Electrical Precautions, is relevant to technicians who want to know what is necessary to make a domestic appliance compliant with FDA regulations for hospital laboratory use.
Section 3, Definitions 8. “Arcing” referred to relatively frequently in the text. Define “arc” and any implications with fire hazard. • This definition has been added as suggested. 9. The majority of histology professionals in the United States are histologic technicians (HT) with a high school diploma
and trained on the job. For most of these individuals, a background in the theory of chemistry and physics is minimal to nonexistent. Most HT with associate degrees, and the histotechnologists (HTL) with baccalaureate degrees, have not taken physics in high school or college. Therefore, their background knowledge of microwave radiation and electricity is minimal, at best.
It would be to the advantage of these readers to include more definitions in the front of the booklet, including units of measure.
Suggestions of words that need definitions under Section 3 include:
Hertz - include the symbol Hz. Include a brief definition of MHz and GHz. (page 3)
Inductance (page 3) Diode (page 3) Anode (page 3) Cathode (page 3)
Watt — including the symbol W. (page 3) Include W. page 4)
Cal/min (page 3) = calorie/minute Arcing (page 7) Thermodynamic (page 12) Microwave-transparent (page 12) Convection (page 12) Conduction (page 12) Entropy (page 12)

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 37
Incident wave (page 14)
Specific heat (page 15) • The definitions for the above terms have been added as suggested with the exception of “incident wave.” The term
“incident wave” has been replaced with “microwave frequency” (page 14). Section 4, Precautions and Safety 10. I believe that the safety sections of the document should be modified and enhanced to increase their value to the reader.
There seems to be an overwhelming emphasis in some of these sections on how domestic units violate various regulatory standards which are in some cases difficult to follow. I believe that this document should provide useful information pointing the reader to standards that may apply rather than attempting to interpret the standards in a lengthy discussion that may lose the reader. Ultimately compliance is up to the user. My suggestions are listed below:
a. It is puzzling that Section 4.1.1 (Microwave Radiation Safety) appears more concerned with FDA regulations than
microwave radiation safety. It never identifies the most basic hazard posed to individuals with pacemakers. I do not believe that the paragraph at the top of page 5 will be useful to the reader. This section is supposed to be about microwave radiation safety yet seems to be focused on the issue of “heating, cooking or drying food….and is manufactured for use in homes, restaurants, food vending or service establishments.” I see no relevance of these remarks to radiation safety concerns unless it can be demonstrated that domestic microwave devices pose a greater radiation hazard than other types of devices.
• Section 4.1.1 states that all microwave devices must comply with FDA regulations of microwave leakage. The
subcommittee did not find documentation about radiation hazards specific to domestic microwave devices, so this was not raised as a concern in the guideline. The FDA DOES require that a microwave device be used solely for the purpose for which it was designed, and this statement is reported in the guideline.
At one time there was concern that leakage from microwave ovens could interfere with certain electronic cardiac pacemakers. There was similar concern about pacemaker interference from electric shavers, auto ignition systems, and other electronic products. Because there are so many other products that also could cause this problem, FDA does not require microwave ovens to carry warnings for people with pacemakers. The problem has been largely resolved, since pacemakers are now designed so they are shielded against such electrical interference. However, patients with pacemakers may wish to consult their physicians about this (refer to Section 4 for further details).
b. In Section 4.1.2, the first paragraph appears to have no relevance to the title of this section and will be confusing to the
reader as it discusses “if the equipment is modified or integrity of the safety device is violated...” I have no idea what this has to do with classifying microwave equipment as medical devices. It appears to me that the content of Table 3 contains more useful information for the reader than the attempts in the text to interpret the regulations which are confusing and unclear. Likewise, the last paragraph on page 5 is equally confusing to the reader. Few practitioners will find the statement “If a manufacturer or user modifies a household microwave oven or commercially promotes histological use as an indication for use…” relevant to their circumstances. They may utilize a domestic device but are they “commercially” promoting histological use? In my opinion this section needs a major overhaul. It would seem to me that its intent could be summed up with a simple statement such as the following:
“Those who use microwave devices for other than that intended by the manufacturer must comply with standards of the Occupational Safety and Health Administration and the FDA.” The section can then point the reader to the specific regulations. I can't stress enough that clarity is key to reaching the reader.
• This guideline is written for multiple audiences including laboratory technicians, microwave device manufacturers,
microwave device resellers, compliance and safety officials, and administrators.
Section 4.2 is relevant to technicians who want to know what is necessary to make a domestic appliance compliant with FDA regulations for hospital laboratory use. This section is also necessary for microwave resellers to be aware that they cannot put their private label on a domestic microwave oven and promote it as a laboratory device. This type of device violates FDA regulations as noted in Table 3. The subcommittee thought it was important for laboratory technicians to also know this information so that they can make informed purchasing decisions. Additional text has been added as introductory sentences in Section 4.1.3 to clarify this section as follows: “This section provides regulatory information primarily for microwave device manufacturers, microwave device resellers, compliance and safety officials, and administrators. The information below may also assist laboratory technicians making purchasing decisions of microwave devices that are in compliance FDA and OSHA regulations.”
c. In Section 4.2, I find the second and third paragraphs of this section confusing. It appears to be saying that domestic
microwave devices and laboratory-grade devices are covered by different UL standards and that the UL standard for domestic devices does not cover laboratory applications. Couldn't this section’s message be stated more clearly and

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 38
succinctly as I’ve stated it here? My interpretation of this section is that domestic ovens are not tested according to UL 61010A-1, not that they were tested and failed to pass this electrical certification. It seems to me that the first paragraph covers the relevant points. The other commentary is difficult to follow and will likely lose the reader.
• The three paragraphs in Section 4.2 actually describe three independent criteria for electrical safety. Paragraph one
outlines that specific electrical safety codes can only be tested by recognized national testing agencies; e.g., recognized by OSHA (USA), CSA (Canada); or authorized to affix the mark (European States). Paragraph two states domestic microwave devices are not designed or tested to meet the more stringent door seal and endurance tests required in 61010A-1. Paragraph three informs the reader that the electrical safety code UL 923 is for domestic microwave ovens, and because their electrical system is not shielded from the microwave cavity they must not be used with caustic or corrosive vapors. Manufacturers are required to state in their instructions that household ovens are only for heating food.
Additional text has been added as introductory sentences in Section 4.2 to clarify this section as follows: “This section provides electrical safety information primarily for microwave device manufacturers, microwave device resellers, compliance and safety officials, and administrators. Laboratory technicians are advised that according to OSHA household microwave ovens do not meet the more stringent door seal and endurance tests required for applications outside the home.”
Section 4.3, Biological Precautions 11. The first sentence of the second paragraph in Section 4.3, Biological Precautions, suggests that some pathogens are
destroyed by microwave heating, but it never tells the reader which ones are and which ones are not. This statement refers to a publication that is ten years old. If more current studies do not exist or if the committee is not comfortable identifying which pathogens are neutralized by microwave heating, why not simply state “the utility of using microwave energy to destroy pathogens requires further study” followed by “all potentially infectious specimens must be handled with standard precautions during and after the use of microwave irradiation.” In the absence of definitive information, the first sentence becomes misleading as if to say, “Microwave irradiation may destroy your pathogen, or it may not!”
• The text in this section has been revised as suggested. Section 4.4, Chemical Handling Precautions 12. Section 4.4., Chemical Handling Precautions, is a good start but I feel that it should be substantially expanded. What
chemicals should absolutely not be used in a microwave device? Are there any that might explode or ignite? I feel strongly that this section needs to be much more informative and should even contain a comprehensive listing of chemicals commonly utilized in histology laboratories and any special precautions for microwave applications.
• This section has been expanded as suggested. Section 4.5, High Temperature Precautions 13. The last sentence in Section 4.5, High Temperature Precautions, states: “The risk of spontaneous boil over in histopathology
applications is more likely during microwave staining and heat-induced epitope retrieval.” More likely than what? If this statement is correct, why is this so? Is this possible result limited to a particular type of microwave device and if not, what can be done to reduce the likelihood of such an outcome? I believe that the reader will want to know if this can be explained in greater detail.
• The sentence has been modified to state, “…more likely during high temperature heating procedures, such as...”
The explanations provided in the literature for microwave-induced boil over are super heating and bubble nucleation (refer to cited references 27 and 43). Since there is no method provided in the literature to prevent spontaneous boil over, technicians should use protective thermal gloves when removing solutions heated to near boiling.
Section 7, Critical Descriptors for Microwave-Accelerated Procedures 14. With the word accuracy, can we add the symbol “±.” Such as, - page 16, 7.1.2.1, second paragraph, “. . . only have an accuracy of ±5 °C.” - page 17, 7.1.2.4, “... have an accuracy between ±2 and 5 °C.” - page 17, 7.1.2.5, " . . . is within ±5 °C.” • The symbol “±” has been added as suggested.

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 39
Section 7.1.2.1, Thermocouple Measurement Devices 15. ‘One hundred dollars’ – Should a dollar amount be quoted? • The text has been changed to read “low cost.” Section 7.1.2.3, IR Temperature Sensors 16. This section starts out with “IR Temperature Sensors,” and the reader has to go to the top of the page to find the definition of
“IR.” Page 17 — 7.1.2.5 starts out with “Liquid Crystal Temperature Strips,” and then abbreviated it in the first sentence to LCTS. The mode on page 17 appears for the LCTS seems clearer.
• The abbreviation “IR” has been spelled out in the title of this section as suggested.
Section 7.1.5, Final (Maximum) Irradiation Temperature 17. Second paragraph: Does staining really require the final sample temperature to be above 90 °C? • Most special stains in histology are done at a temperature range of 22 to 60 °C. Text has been added to reflect this. Section 7.2.3.1, Method to Determine Power Output of a Large-Cavity Microwave Device 18. #4 — "... place an appropriate cover of plastic or foil." The question is where? Over the mouth of the bottle? Around the
outside of the container? • Text has been added to clarify this. Section 7.3.1.2, Container Dimensions 19. Is the final recommendation to use rectangular containers? • There is no consensus about container shape within the subcommittee; however, the recommendation for rectangular
containers is based on cited literature (see cited references 59 and 60). Section 8, Special Microwave Procedures 20. This section alternates between heat-induced epitope retrieval (without indicating the HIER abbreviation) and AR (without
defining AR as antigen recovery or antigen retrieval. Suggest using HIER consistently, with the abbreviation. • The term “heat-induced epitope retrieval” has been replaced with “antigen retrieval” (AR) throughout this section. Table 13 21. “Microwave Curing — Results — Mold Deforms” — Before the word “mold,” insert “Embedding.” Mold, in histology,
can also mean “fungus.” • This text has been added as suggested.

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 40
The Quality System Approach Clinical and Laboratory Standards Institute subscribes to a quality system approach in the development of standards and guidelines, which facilitates project management; defines a document structure via a template; and provides a process to identify needed documents. The approach is based on the model presented in the most current edition of CLSI/NCCLS document HS1—A Quality Management System Model for Health Care. The quality system approach applies a core set of “quality system essentials” (QSEs), basic to any organization, to all operations in any healthcare service’s path of workflow (i.e., operational aspects that define how a particular product or service is provided). The QSEs provide the framework for delivery of any type of product or service, serving as a manager’s guide. The quality system essentials (QSEs) are: Documents & Records Equipment Information Management Process Improvement Organization Purchasing & Inventory Occurrence Management Service & Satisfaction Personnel Process Control Assessment Facilities & Safety GP28-A addresses the quality system essentials (QSEs) indicated by an “X.” For a description of the other CLSI/NCCLS documents listed in the grid, please refer to the Related CLSI/NCCLS Publications section on the following page.
Doc
umen
ts
& R
ecor
ds
Org
aniz
atio
n
Pers
onne
l
Equi
pmen
t
Purc
hasi
ng &
In
vent
ory
Proc
ess
Con
trol
Info
rmat
ion
Man
agem
ent
Occ
urre
nce
Man
agem
ent
Ass
essm
ent
Proc
ess
Impr
ovem
ent
Serv
ice
&
Satis
fact
ion
Faci
litie
s &
Safe
ty
X
Adapted from CLSI/NCCLS document HS1—A Quality Management System Model for Health Care.

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 41
Related CLSI/NCCLS Publications* GP17-A2 Clinical Laboratory Safety; Approved Guideline—Second Edition (2004). This document contains general
guidelines for implementing a high-quality laboratory safety program, which are provided in a framework that is adaptable within any laboratory.
MM4-A Quality Assurance for Immunocytochemistry; Approved Guideline (1999). This document provides
recommendations for the performance of immunocytochemical assays on cytologic and surgical pathology specimens. It is intended to promote a better understanding of the requirements, capabilities, and limitations of these diagnostic methods; to improve their intra- and interlaboratory reproducibility; and to improve their positive and negative predictive values in the diagnosis of disease.
* Proposed- and tentative-level documents are being advanced through the Clinical and Laboratory Standards Institute consensus process; therefore, readers should refer to the most recent editions.

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 42
NOTES

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 43
NOTES

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 44
NOTES

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 45
NOTES

Number 7 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 46
NOTES

Volume 25 GP28-A
©Clinical and Laboratory Standards Institute. All rights reserved. 47
NOTES

Active Membership (as of 1 January 2005)
Sustaining Members Abbott Laboratories American Association for Clinical Chemistry Bayer Corporation BD Beckman Coulter, Inc. bioMérieux, Inc. CLMA College of American Pathologists GlaxoSmithKline Ortho-Clinical Diagnostics, Inc. Pfizer Inc Roche Diagnostics, Inc. Professional Members American Academy of Family Physicians American Association for Clinical Chemistry American Association for Respiratory Care American Chemical Society American Medical Technologists American Society for Clinical Laboratory Science American Society for Microbiology American Society of Hematology American Type Culture Collection, Inc. Asociacion Mexicana de Bioquimica Clinica A.C. Assn. of Public Health Laboratories Assoc. Micro. Clinici Italiani- A.M.C.L.I. British Society for Antimicrobial Chemotherapy Canadian Society for Medical Laboratory Science - Société Canadienne de Science de Laboratoire Médical Canadian Standards Association Clinical Laboratory Management Association COLA College of American Pathologists College of Medical Laboratory Technologists of Ontario College of Physicians and Surgeons of Saskatchewan ESCMID International Council for Standardization in Haematology International Federation of Biomedical Laboratory Science International Federation of Clinical Chemistry Italian Society of Clinical Biochemistry and Clinical Molecular Biology Japan Society of Clinical Chemistry Japanese Committee for Clinical Laboratory Standards Joint Commission on Accreditation of Healthcare Organizations National Academy of Clinical Biochemistry National Association of Testing Authorities - Australia National Society for Histotechnology, Inc. New Zealand Association of Phlebotomy Ontario Medical Association Quality Management Program-Laboratory Service RCPA Quality Assurance Programs PTY Limited Sociedad Espanola de Bioquimica Clinica y Patologia Molecular Sociedade Brasileira de Analises Clinicas Taiwanese Committee for Clinical Laboratory Standards (TCCLS) Turkish Society of Microbiology Government Members Armed Forces Institute of Pathology Association of Public Health Laboratories BC Centre for Disease Control Caribbean Epidemiology Centre Centers for Disease Control and Prevention Centers for Medicare & Medicaid Services Centers for Medicare & Medicaid Services/CLIA Program
Chinese Committee for Clinical Laboratory Standards Commonwealth of Pennsylvania Bureau of Laboratories Department of Veterans Affairs Deutsches Institut für Normung (DIN) FDA Center for Devices and Radiological Health FDA Center for Veterinary Medicine FDA Division of Anti-Infective Drug Products Iowa State Hygienic Laboratory Massachusetts Department of Public Health Laboratories National Center of Infectious and Parasitic Diseases (Bulgaria) National Health Laboratory Service (South Africa) National Institute of Standards and Technology National Pathology Accreditation Advisory Council (Australia) New York State Department of Health Ontario Ministry of Health Pennsylvania Dept. of Health Saskatchewan Health-Provincial Laboratory Scientific Institute of Public Health; Belgium Ministry of Social Affairs, Public Health and the Environment Swedish Institute for Infectious Disease Control Industry Members AB Biodisk Abbott Laboratories Abbott Diabetes Care Acrometrix Corporation Advancis Pharmaceutical Corporation Affymetrix, Inc. Ammirati Regulatory Consulting Anna Longwell, PC A/S ROSCO AstraZeneca Pharmaceuticals Aventis Axis-Shield POC AS Bayer Corporation - Elkhart, IN Bayer Corporation - Tarrytown, NY Bayer Corporation - West Haven, CT BD BD Consumer Products BD Diagnostic Systems BD VACUTAINER Systems Beckman Coulter, Inc. Beckman Coulter K.K. (Japan) Bio-Development SRL Bio-Inova Life Sciences International Biomedia Laboratories SDN BHD bioMérieux, Inc. (MO) Biometrology Consultants Bio-Rad Laboratories, Inc. Bio-Rad Laboratories, Inc. – France Bio-Rad Laboratories, Inc. – Plano, TX Blaine Healthcare Associates, Inc. Bristol-Myers Squibb Company Canadian External Quality Assessment Laboratory Cepheid Chen & Chen, LLC Chiron Corporation ChromaVision Medical Systems, Inc. Clinical Micro Sensors The Clinical Microbiology Institute Cognigen CONOSCO Copan Diagnostics Inc. Cosmetic Ingredient Review Cubist Pharmaceuticals Dade Behring Inc. - Cupertino, CA Dade Behring Inc. - Deerfield, IL Dade Behring Inc. - Glasgow, DE Dade Behring Inc. - Marburg, Germany Dade Behring Inc. - Sacramento, CA David G. Rhoads Associates, Inc. Diagnostic Products Corporation Digene Corporation Eiken Chemical Company, Ltd. Elanco Animal Health Electa Lab s.r.l. Enterprise Analysis Corporation
F. Hoffman-La Roche AG Fort Dodge Animal Health Gen-Probe GenVault GlaxoSmithKline Greiner Bio-One Inc. Immunicon Corporation ImmunoSite, Inc. Instrumentation Laboratory International Technidyne Corporation I-STAT Corporation Johnson and Johnson Pharmaceutical Research and Development, L.L.C. K.C.J. Enterprises LifeScan, Inc. (a Johnson & Johnson Company) Machaon Diagnostics Medical Device Consultants, Inc. Merck & Company, Inc. Micromyx, LLC Minigrip/Zip-Pak Nanosphere, Inc. National Pathology Accreditation Advisory Council (Australia) Nippon Becton Dickinson Co., Ltd. Nissui Pharmaceutical Co., Ltd. Norfolk Associates, Inc. Novartis Pharmaceuticals Corporation Olympus America, Inc. Optimer Pharmaceuticals, Inc. Ortho-Clinical Diagnostics, Inc. (Rochester, NY) Ortho-McNeil Pharmaceutical (Raritan, NJ) Oxoid Inc. Paratek Pharmaceuticals Pfizer Animal Health Pfizer Inc Pfizer Italia Srl Powers Consulting Services Procter & Gamble Pharmaceuticals, Inc. QSE Consulting Radiometer America, Inc. Radiometer Medical A/S Replidyne Roche Diagnostics GmbH Roche Diagnostics, Inc. Roche Laboratories (Div. Hoffmann- La Roche Inc.) Sarstedt, Inc. Schering Corporation Schleicher & Schuell, Inc. Second Opinion SFBC Anapharm Streck Laboratories, Inc. SYN X Pharma Inc. Sysmex Corporation (Japan) Sysmex Corporation (Long Grove, IL) TheraDoc Theravance Inc. Thrombodyne, Inc. THYMED GmbH Transasia Engineers Trek Diagnostic Systems, Inc. Vetoquinol S.A. Vicuron Pharmaceuticals Inc. Vysis, Inc. Wyeth Research XDX, Inc. YD Consultant YD Diagnostics (Seoul, Korea) Trade Associations AdvaMed Japan Association of Clinical Reagents Industries (Tokyo, Japan) Associate Active Members 82 MDG/SGSCL (Sheppard AFB,
TX) Academisch Ziekenhuis -VUB (Belgium) Alfred I. duPont Hospital for Children (DE) All Children’s Hospital (FL) Allegheny General Hospital (PA) Allina Health System (MN) American University of Beirut Medical Center (NY) Anne Arundel Medical Center (MD) Antwerp University Hospital (Belgium) Arkansas Department of Health ARUP at University Hospital (UT) Associated Regional & University Pathologists (UT) Atlantic Health System (NJ)
Aurora Consolidated Laboratories (WI) AZ Sint-Jan (Belgium) Azienda Ospedale Di Lecco (Italy) Barnes-Jewish Hospital (MO) Baxter Regional Medical Center (AR) Baystate Medical Center (MA) Bbaguas Duzen Laboratories (Turkey) BC Biomedical Laboratories (Surrey, BC, Canada) Bermuda Hospitals Board Bo Ali Hospital (Iran) Bon Secours Hospital (Ireland) Brazosport Memorial Hospital (TX) Broward General Medical Center (FL) Cadham Provincial Laboratory (Winnipeg, MB, Canada) Calgary Laboratory Services (Calgary, AB, Canada) California Pacific Medical Center Canterbury Health Laboratories (New Zealand) Cape Breton Healthcare Complex (Nova Scotia, Canada) Carilion Consolidated Laboratory (VA) Carolinas Medical Center (NC) Cathay General Hospital (Taiwan) Central Texas Veterans Health Care System Centro Diagnostico Italiano (Milano, Italy) Chang Gung Memorial Hospital (Taiwan) Changi General Hospital (Singapore) Children’s Hospital (NE) Children’s Hospital & Clinics (MN) Children’s Hospital Medical Center (Akron, OH) Children’s Medical Center of Dallas (TX) Chinese Association of Advanced Blood Bankers (Beijing) CHR St. Joseph Warquignies (Belgium) City of Hope National Medical Center (CA) Clarian Health - Methodist Hospital (IN) CLSI Laboratories (PA) Community Hospital of Lancaster (PA) Community Hospital of the Monterey Peninsula (CA) CompuNet Clinical Laboratories (OH) Cook County Hospital (IL) Covance Central Laboratory Services (IN) Creighton University Medical Center (NE) Danish Veterinary Laboratory (Denmark) Detroit Health Department (MI) DFS/CLIA Certification (NC) Diagnósticos da América S/A (Brazil) Dr. Everett Chalmers Hospital (New Brunswick, Canada) Duke University Medical Center (NC) Dwight David Eisenhower Army Medical Center (GA) Eastern Health Pathology (Australia) Emory University Hospital (GA) Enzo Clinical Labs (NY) Evangelical Community Hospital (PA) Fairview-University Medical Center (MN) Florida Hospital East Orlando Focus Technologies (CA) Focus Technologies (VA) Foothills Hospital (Calgary, AB, Canada) Franciscan Shared Laboratory (WI) Fresno Community Hospital and Medical Center Gamma Dynacare Medical Laboratories (Ontario, Canada) Gateway Medical Center (TN) Geisinger Medical Center (PA) Guthrie Clinic Laboratories (PA) Hagerstown Medical Laboratory (MD) Harris Methodist Fort Worth (TX) Hartford Hospital (CT) Headwaters Health Authority (Alberta, Canada)

Health Network Lab (PA) Health Partners Laboratories (VA) Highlands Regional Medical Center (FL) Hoag Memorial Hospital Presbyterian (CA) Holy Cross Hospital (MD) Hôpital du Sacré-Coeur de Montreal (Montreal, Quebec, Canada) Hôpital Maisonneuve - Rosemont (Montreal, Canada) Hôpital Saint-Luc (Montreal, Quebec, Canada) Hospital Consolidated Laboratories (MI) Hospital for Sick Children (Toronto, ON, Canada) Hospital de Sousa Martins (Portugal) Hotel Dieu Grace Hospital (Windsor, ON, Canada) Huddinge University Hospital (Sweden) Hunter Area Health Service (Australia) Indiana University Innova Fairfax Hospital (VA) Institute of Medical and Veterinary Science (Australia) International Health Management Associates, Inc. (IL) Jackson Memorial Hospital (FL) Jacobi Medical Center (NY) John C. Lincoln Hospital (AZ) Johns Hopkins Medical Institutions (MD) Kadlec Medical Center (WA) Kaiser Permanente (MD) Kangnam St. Mary’s Hospital (Korea) Kantonsspital (Switzerland) Kimball Medical Center (NJ) King Abdulaziz Medical City – Jeddah (Saudi Arabia) King Faisal Specialist Hospital (Saudi Arabia) LabCorp (NC) Laboratoire de Santé Publique du Quebec (Canada) Laboratorio Dr. Echevarne (Spain) Laboratório Fleury S/C Ltda. (Brazil) Laboratorio Manlab (Argentina) Laboratory Corporation of America (NJ) LAC and USC Healthcare Network (CA) Lakeland Regional Medical Center (FL) Landstuhl Regional Medical Center (APO AE) Lawrence General Hospital (MA) LeBonheur Children’s Medical Center (TN) Lewis-Gale Medical Center (VA) L'Hotel-Dieu de Quebec (Canada) Libero Instituto Univ. Campus BioMedico (Italy) Lindy Boggs Medical Center (LA) Loma Linda Mercantile (CA) Long Beach Memorial Medical Center (CA) Louisiana State University Medical Center
Lourdes Hospital (KY) Maimonides Medical Center (NY) Marion County Health Department (IN) Martin Luther King/Drew Medical Center (CA) Massachusetts General Hospital (Microbiology Laboratory) MDS Metro Laboratory Services (Burnaby, BC, Canada) Medical College of Virginia Hospital Medical University of South Carolina Memorial Medical Center (Napoleon Avenue, New Orleans, LA) Methodist Hospital (Houston, TX) Methodist Hospital (San Antonio, TX) Michigan Department of Community Health Mid America Clinical Laboratories, LLC (IN) Middlesex Hospital (CT) Monmouth Medical Center (NJ) Montreal Children’s Hospital (Canada) Montreal General Hospital (Canada) National Serology Reference Laboratory (Australia) NB Department of Health & Wellness (New Brunswick, Canada) The Nebraska Medical Center New Britain General Hospital (CT) New England Fertility Institute (CT) New England Medical Center (MA) New York City Department of Health & Mental Hygiene NorDx (ME) North Carolina State Laboratory of Public Health North Central Medical Center (TX) North Shore - Long Island Jewish Health System Laboratories (NY) North Shore University Hospital (NY) Northwestern Memorial Hospital (IL) Ochsner Clinic Foundation (LA) Onze Lieve Vrouw Ziekenhuis (Belgium) Orlando Regional Healthcare System (FL) Ospedali Riuniti (Italy) The Ottawa Hospital (Ottawa, ON, Canada) OU Medical Center (OK) Our Lady of the Resurrection Medical Center (IL) Pathology and Cytology Laboratories, Inc. (KY) Pathology Associates Medical Laboratories (WA) Peking University Shenzhen Hospital (China) The Permanente Medical Group (CA) Piedmont Hospital (GA) Pocono Medical Center (PA) Providence Health Care (Vancouver, BC, Canada) Provincial Laboratory for Public Health (Edmonton, AB, Canada)
Queensland Health Pathology Services (Australia) Quest Diagnostics Incorporated (CA) Quintiles Laboratories, Ltd. (GA) Regional Health Authority Four (NB, Canada) Regions Hospital Rex Healthcare (NC) Rhode Island Department of Health Laboratories Riverside Medical Center (IL) Robert Wood Johnson University Hospital (NJ) Sahlgrenska Universitetssjukhuset (Sweden) St. Alexius Medical Center (ND) St. Anthony Hospital (CO) St. Anthony’s Hospital (FL) St. Barnabas Medical Center (NJ) St. Christopher’s Hospital for Children (PA) St-Eustache Hospital (Quebec, Canada) St. John Hospital and Medical Center (MI) St. John’s Hospital & Health Center (CA) St. Joseph Mercy Hospital (MI) St. Joseph’s Hospital – Marshfield Clinic (WI) St. Jude Children’s Research Hospital (TN) St. Mary of the Plains Hospital (TX) St. Mary Medical Center (CA) St. Michael’s Hospital (Toronto, ON, Canada) Ste. Justine Hospital (Montreal, PQ, Canada) Salem Clinic (OR) San Francisco General Hospital (CA) Santa Clara Valley Medical Center (CA) Seoul Nat’l University Hospital (Korea) Shands at the University of Florida South Bend Medical Foundation (IN) South Western Area Pathology Service (Australia) Southern Maine Medical Center Spartanburg Regional Medical Center (SC) Specialty Laboratories, Inc. (CA) State of Connecticut Dept. of Public Health State of Washington Department of Health Stony Brook University Hospital (NY) Stormont-Vail Regional Medical Center (KS) Sun Health-Boswell Hospital (AZ) Sunnybrook Health Science Center (ON, Canada) Sunrise Hospital and Medical Center (NV) Swedish Medical Center - Providence Campus (WA) Temple University Hospital (PA) Tenet Odessa Regional Hospital (TX) The Toledo Hospital (OH)
Touro Infirmary (LA) Tripler Army Medical Center (HI) Truman Medical Center (MO) UCLA Medical Center (CA) UCSF Medical Center (CA) UNC Hospitals (NC) Unidad de Patologia Clinica (Mexico) Union Clinical Laboratory (Taiwan) United Laboratories Company (Kuwait) Universita Campus Bio-Medico (Italy) University College Hospital (Galway, Ireland) University of Alabama-Birmingham Hospital University of Chicago Hospitals (IL) University of Colorado Hospital University of Debrecen Medical Health and Science Center (Hungary) University of Illinois Medical Center University of Maryland Medical System University of Medicine & Dentistry, NJ University Hospital University of the Ryukyus (Japan) University of Wisconsin Hospital The University of Texas Medical Branch The University of the West Indies University of Virginia Medical Center University of Washington USA MEDDAC-AK US LABS, Inc. (CA) UZ-KUL Medical Center (Belgium) VA (Tuskegee) Medical Center (AL) Valley Children’s Hospital (CA) Virginia Beach General Hospital (VA) Virginia Department of Health Virginia Regional Medical Center (MN) ViroMed Laboratories (MN) Washington Adventist Hospital (MD) Washoe Medical Center Laboratory (NV) Waterford Regional Hospital (Ireland) Wellstar Health Systems (GA) West Jefferson Medical Center (LA) Wilford Hall Medical Center (TX) William Beaumont Army Medical Center (TX) William Beaumont Hospital (MI) Winn Army Community Hospital (GA) Winnipeg Regional Health Authority (Winnipeg, Canada) Wishard Memorial Hospital (IN) Yonsei University College of Medicine (Korea) York Hospital (PA)
OFFICERS
BOARD OF DIRECTORS
Thomas L. Hearn, Ph.D., President Centers for Disease Control and Prevention Robert L. Habig, Ph.D., President Elect Abbott Laboratories Wayne Brinster, Secretary BD Gerald A. Hoeltge, M.D., Treasurer The Cleveland Clinic Foundation Donna M. Meyer, Ph.D., Immediate Past President CHRISTUS Health Glen Fine, M.S., M.B.A., Executive Vice President
Susan Blonshine, RRT, RPFT, FAARC TechEd Kurt H. Davis, FCSMLS, CAE Canadian Society for Medical Laboratory Science Mary Lou Gantzer, Ph.D. Dade Behring Inc. Lillian J. Gill, D.P.A. FDA Center for Devices and Radiological Health Carolyn D. Jones, J.D., M.P.H. AdvaMed J. Stephen Kroger, M.D., MACP COLA
Willie E. May, Ph.D. National Institute of Standards and Technology Gary L. Myers, Ph.D. Centers for Disease Control and Prevention Klaus E. Stinshoff, Dr.rer.nat. Digene (Switzerland) Sàrl James A. Thomas ASTM International Kiyoaki Watanabe, M.D. Keio University School of Medicine Judith A. Yost, M.A., M.T.(ASCP) Centers for Medicare & Medicaid Services

940 West Valley Road Suite 1400 Wayne, PA 19087 USA PHONE 610.688.0100 FAX 610.688.0700 E-MAIL: [email protected] WEBSITE: www.clsi.org ISBN 1-56238-563-1





























