Embed Size (px)
Citation preview
Grant Expenditure
Responsibility Reports
2011
USEF Equine Health
Research Fund
$24,126
For Research by
the University of
Minnesota into the
Epidemiology and
Pathology of
'Shivers'

Lay Summary: The Basis for “Shivers”, a Chronic Movement Disorder in Horses Description of the Problem: Shivers is a common, performance-limiting problem for owners of Warmbloods, Draft horses and Thoroughbreds. Horses with Shivers intermittently hold their hindlimb flexed and away from the body for seconds to minutes whilst the rump muscles and tail tremble. It is usually induced by backing up or picking up a hindlimb. In mild forms it represents a nuisance to farriers that have difficulty when the horse snatches their limb away and slams it to the ground. However, if it progresses, owners may not be able to pick up the feet and the exaggerated limb flexion will be apparent even when walking forward. In such cases it impairs performance. Many of today’s top show jumpers and dressage horses have mild signs of Shivers and owners worry about the disease progressing. Nothing is known about the cause, factors contributing to progression or ways to alleviate symptoms of Shivers. Minimal scientific research has been performed to date and this has produced speculation regarding the diagnostic signs required to diagnose ‘Shivers’, factors that might affect development and progression of signs and the benefit of a number of management and dietary changes. No pathologic changes have been described in the nervous system of Shivers horses. We believe that Shivers is a movement disorder arising from the central nervous system that results in abnormal coordination of the pattern of contraction and relaxation of flexor and extensor muscles both within the same limb and relative to other limbs. In this grant we 1) performed a web-based survey of hundreds of owners of horses with Shivers-like signs to fully characterize the clinical disease, treatment responses and progression and 2) performed a detailed histological evaluation of the entire central nervous system of Shivers horses to localize and characterize microscopic abnormalities in the nervous system of horses with Shivers. Accomplishments/Results: Surveys were obtained from 305 owners of horses with movement disorders and 50 video submissions were received. After viewing videos, Shivers was defined as: normal forward gaits combined with intermittent hyperflexion or prolonged extension of the hindlimbs induced by backwards walking and by manual lifting of the hindlimbs. Based on this definition, information was analyzed for 157 horses. Owners provided information on 50 healthy control horses of similar ages. Shivers horses were significantly taller than control horses being on average 17.1 hands high vs. the 16 hands for controls. There were almost six times more male horses with Shivers than females whereas similar numbers of male and female horses were present in the control group. Shivers horses were predominantly Warmbloods, Thoroughbreds and Draft horses whereas the control group had significantly more other breeds. Shivers horses were fed more fat in their diet than control horses, which was reported to produce on average a 25% improvement in Shivers signs. Increasing physical activity was reported to improve symptoms with >58% of horses showing about a 50% improvement with more activity. Tranquilizers helped temporarily when shoeing or trimming the hind feet. Progression of Shivers symptoms occurred in over 60% of horses.
Microscopic examination of the nervous system indicated that Shivers is characterized by moderate chronic degeneration of nerves located in the cerebellum and the spinal cord.

Relevance to the equine industry We now have both a clinical and a pathologic definition of Shivers. Shivers is a movement disorder that affects walking backwards and holding up a hindlimb. It is a chronic degenerative axonopathy that primarily affects tall horses, especially geldings, of Warmblood, Thoroughbred and Draft breeds. The disease progresses in more than 60% of cases, but symptoms can be decreased by keeping horses active and fit. Trimming of the hindfeet can be assisted by tranquilization.

UNIVERSITY OF MINNESOTA EQUINE CENTER Stephanie Valberg
1
USEF FINAL REPORT 2012
Title: Investigating the epidemiology and the pathology of ‘Shivers’
Department: Veterinary Population Medicine
______________________________________________________________
UNIVERSITY OF MINNESOTA EQUINE CENTER Stephanie Valberg
2
Title: Investigating the epidemiology and the pathology of ‘Shivers’ ABSTRACT IN SCIENTIFIC TERMS: “In the heyday of equine practice” Shivers was “as common as dirt”, states a comparative neuropathology text from 1962. Today Shivers is a still a common and vexing problem affecting Warmblood, Draft and some light breeds of horses. Shivers is characterized by abduction, hyperflexion and muscle tremors in the pelvic limb induced by backing or picking up that limb. In some horses, Shivers is intermittent and mainly represents a nuisance to farriers, however, in other cases it progresses to a total inability to pick up the feet, exaggerated limb flexion even when standing still or walking forward and it seriously impairs performance. The variable progression of this disease makes pre-purchase examinations challenging for veterinarians. Some Warmbloods which passed veterinary examination in Europe have been incapacitated by Shivers when they leave quarantine in the USA. Crucial information is needed to determine the cause of, and risk factors for, Shivers to assist veterinarians in making a definitive diagnosis, determining a prognosis and a successful strategy to manage horses with Shivers. While many of today’s top show jumpers and dressage horses show mild signs of Shivers, every year a proportion of affected horses develop severe signs and are euthanized due to the lack of therapeutic and preventative practices. Shivers has been proposed to be have traumatic, infectious, neurologic or genetic causes. However, only one histopathologic study of the nervous system in Shivers cases has been performed and this involved only two Belgian draft horses and basic H&E stains. No neuropathology was identified in this limited study but horses were found t ?? have polysaccharide storage myopathy (PSSM). Our subsequent study of 103 Belgian drafts concluded that PSSM did not cause Shivers because it was only present in 33% of the Shivers horses that were identified.2 The current proposal was the first step in a long term project that focuses the expertise of experienced equine neurologists, neuropathologists and kinesiologists on the movement disorder called Shivers. We believe that the basis for and best treatment of Shivers can only be determined through a detailed clinical, epidemiologic and neuropathologic study. Our hypothesis was that Shivers is a paroxysmal movement disorder that is induced by specific sub-conscious and reflex actions and results in intermittent bursts of mild to marked tetanic motor unit activity involving flexor and extensor muscles of the pelvic limbs and tail elevator muscles. In this grant we 1) identified characteristics, risk factors and potential treatment strategies through an epidemiologic study of Shivers and 2) characterized light microscopic lesions in Shivers utilizing tinctorial and immunohistochemical stains. We concluded that Shivers is a slowly progressive degenerative central axonopathy that begins between 2 and 10 years of age and primarily affects male Warmblood, Thoroughbred or Draft horses over 17 hands in height. Keeping horse active represents the only known means to minimize clinical signs. Results represent the first description of the epidemiology and neuropathology of Shivers in horses and will form the basis for defining the cause and potential treatments for this confounding condition.
UNIVERSITY OF MINNESOTA EQUINE CENTER Stephanie Valberg
3
SPECIFIC AIMS: Objective 1: To characterize the severity, inciting factors and progression of Shivers using an on line closed-ended epidemiologic questionnaire. Objective 2: To determine the nature and frequency of neurodegenerative lesions apparent in electron microscopy and special stains of the sensory and motor systems of horses with Shivers compared to age/breed matched controls. MATERIALS AND METHODS Objective 1: The epidemiology of Shivers Case definition: The clinical definition of Shivers used in the present study was normal forward walking and intermittent hyperflexion or prolonged extension of the hindlimbs induced by backwards walking and by manual lifting of the hindlimbs. Advanced Shivers was defined as the same criteria for Shivers plus intermittent hyperflexion of a hindlimb during forwards walking. Case Selection: Potential cases of Shivers were solicited through advertisements in national and international horse magazines and owners were directed to a web-based closed-ended questionnaire on the University of Minnesota Neuromuscular Laboratory (NMDL) website. Owners were asked to mail or upload a video of their horse being led in hand, walking forwards, walking backwards, circling (to the left and right) and when the owner manually lifted each limb for a minimum of ten seconds. Cases were included in the study if questionnaires were complete and legible and clinical signs were compatible with Shivers. Cases were divided into three groups: (1) Confirmed Shivers; horses were examined by one of the authors in person or by viewing the submitted video (2) Reported Shivers; horses diagnosed by the reported clinical signs without video analysis (3) Shivers with forward hyperflexion (Shivers FHF); horses examined by one of the authors in person or by viewing the submitted video that met the advanced Shivers case definition. Control Group: The owners of the Confirmed Shivers horses were asked to complete a questionnaire for 2-3 unaffected horses. These horses were free of signs of Shivers or other movement disorders, were older than 4 years, and lived in close geographical proximity to the Shivers-affected horse. The Control questionnaire was web-based and consisting of closed-ended questions pertaining to signalment, diet, use, previous illnesses or trauma and regular drug administration. Epidemiological Survey: The web-based questionnaire addressed questions pertaining to the owner; contact details, location, and the signalment [breed, date of birth, height, gender (male vs female), body condition] of the horse. Breeds were later grouped as Draft, Thoroughbred (TB) and Warmblood (WB) (or their crosses) and Other (Connemara,
UNIVERSITY OF MINNESOTA EQUINE CENTER Stephanie Valberg
4
Welsh breeds, Quarter horses, Standardbreds, Saddlebreds, Tennessee Walking horses, Missouri Fox Trotters, Paint, Morgan and ‘mixed breed’). Average daily time spent in a stall was recorded. Use of horse was grouped as pleasure (pleasure/trail or retired) competition (dressage, hunter/jumper, showing, eventing or racing) or draft work. Dietary information was recorded in terms of type of forage and commercial ration as well as weight fed per day. Supplements added to the horses’ diet were classed as no supplements fed, selenium, vitamin E, joint supplement, mineral block, salt block, electrolytes, hoof supplement, calmer, vitamin and mineral balancer and a probiotic. Clinical Signs: The age when owners first observed clinical signs of Shivers was recorded. Clinical signs that owners could check off included weakness, exercise intolerance, unexplained lameness, abnormal FW and BW, difficulty with the farrier or on manual lifting of the hindlimbs, abnormalities noted with the forelimbs, twitching of the face or muzzle, muscle atrophy and quivering. There was also a comment box for additional information. Progression of Shivers clinical signs were classified as improving (ranging from an improvement of clinical signs of 10-100%), worsening or remaining static (0% improvement in clinical signs). The time frame over which they improved or worsened was also determined (over weeks, months or years). Precipitating factors included airplane travel, major surgery, illness (requiring hospitalization or stall rest), abuse or neglect, trailer accident or long distance transportation (>6hrs) and were reported for the year preceding and subsequently Shivers symptoms beginning. Neurological, gastrointestinal, endocrine and lameness problems were also recorded. Any deterioration or improvement in signs following these precipitating factors or illness was recorded as improvement from 0-100%. Management, Activity Changes and treatments: Management changes including removal of hind-shoes or no farrier work on the hindlimbs were described. Activity changes were described as either an increase or decrease in the following categories; riding/training, pulling/labor or turnout. Owners were also asked to list which pharmacological therapies they may have tried to alleviate symptoms of Shivers and if they had any effect. The following list of therapies was provided; flunixin meglumine (Banamine), phenylbutazone, any muscle relaxer, phenytoin, a tranquilizer, acupuncture, chiropractics and herbs. A comments box was provided for additional therapies tried. Statistical Analysis: The answers obtained from the survey were downloaded to a spreadsheet and categorical data from the Confirmed Shivers, Reported Shivers and AS groups were organized into frequency tables (signalment data, use, diet, stall time, age of onset, disease progression, previous trauma, clinical signs, treatments), and the mean ± standard deviation was reported for the continuous data (age and height). The Confirmed Shivers, Reported Shivers and AS data was either compared using a One-way ANOVA (if continuous) or a Pearson’s Chi-square test or the Fischer’s Exact test (if categorical). No analysis of age was performed between the Confirmed Shivers and Control groups as this characteristic was used in selecting individuals for the Control group. The Confirmed Shivers data was compared to the Control data using Pearson’s Chi-square test or the Fischer’s Exact test where appropriate.
UNIVERSITY OF MINNESOTA EQUINE CENTER Stephanie Valberg
5
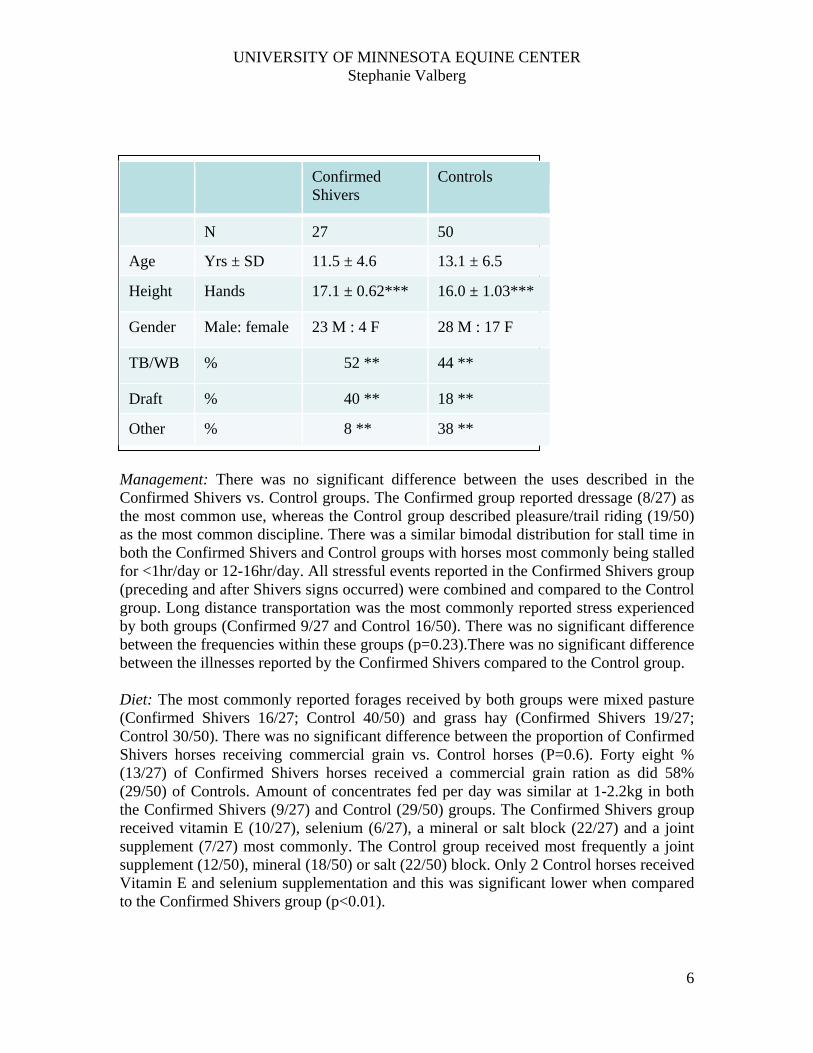
Multiple linear regression was used to generate a logistic regression model comparing the Confirmed Shivers data to the Control data. Results are expressed as mean + SD. Significance was set at p<0.05. RESULTS AIM 1: The epidemiology of Shivers Horses: Questionnaires were received from 305 horses and 50 videos were received. Based on the case definition, 157 horses were diagnosed with Shivers with 27 horses in the Confirmed Shivers, 67 horses in the Reported Shivers and 63 horses in the A groups. The majority of horses not included in the study showed an array of difficulty holding up the hindlimb only with normal backing or other gait abnormalities. Nine of 157 horses were examined at the University of Minnesota Equine Center (8 with Shivers and 1 with Advanced Shivers). Comparison of Confirmed Shivers cases versus Controls Signalment: The in mean (± SD) age, height, gender and breeds are shown in Table 1. The Confirmed Shivers group contained significantly more (p=0.002) Draft and TB/WB breeds and fewer Other breeds compared to the Control group. The proportion of male horses in Confirmed Shivers was significantly higher (p=0.04) than in the Control group. The mean height of Confirmed Shivers was significantly taller (p<0.0001) (173.1 ± 6.2 cm) than the Control group (161.0 ± 10.3). Body condition was reported to be ideal in both Confirmed Shivers and Controls. To ensure the difference in height between Confirmed Shivers and controls was not a result of differences in breeds or gender between the groups, the height of horses of the same breed or gender was compared between Confirmed Shivers and Control groups. There was no statistically significant difference in height between Confirmed Shivers and Control groups when compared within the three breed categories Draft, Warmbloods/TBs or Other. Similarly, there was no statistically significant difference in height of males Confirmed Shivers horses were combined. On average the Draft group was 22cm taller than the Other group (p<0.01) and 6.7cm taller than the TB/WB group (p<0.01). The TB/WB group was 15cm taller than the Other group (p<0.01). Males were significantly taller than the females (p=0.003). The mean male height was 167.64 ± 10.7 cm (16.2hh) and the females 159.30 ± 9.5 cm (15.3h). ?? Logistic Regression Model: The following criteria were included to build a model comparing the Confirmed Shivers and Control groups; height, gender, breed, age, stall time. Height was the only significant indicator of Shivers (p=0.004).
UNIVERSITY OF MINNESOTA EQUINE CENTER Stephanie Valberg
6
Confirmed Shivers
Controls
N 27 50
Age Yrs ± SD 11.5 ± 4.6 13.1 ± 6.5
Height Hands 17.1 ± 0.62*** 16.0 ± 1.03***
Gender Male: female 23 M : 4 F 28 M : 17 F
TB/WB % 52 ** 44 **
Draft % 40 ** 18 **
Other % 8 ** 38 **
Management: There was no significant difference between the uses described in the Confirmed Shivers vs. Control groups. The Confirmed group reported dressage (8/27) as the most common use, whereas the Control group described pleasure/trail riding (19/50) as the most common discipline. There was a similar bimodal distribution for stall time in both the Confirmed Shivers and Control groups with horses most commonly being stalled for <1hr/day or 12-16hr/day. All stressful events reported in the Confirmed Shivers group (preceding and after Shivers signs occurred) were combined and compared to the Control group. Long distance transportation was the most commonly reported stress experienced by both groups (Confirmed 9/27 and Control 16/50). There was no significant difference between the frequencies within these groups (p=0.23).There was no significant difference between the illnesses reported by the Confirmed Shivers compared to the Control group. Diet: The most commonly reported forages received by both groups were mixed pasture (Confirmed Shivers 16/27; Control 40/50) and grass hay (Confirmed Shivers 19/27; Control 30/50). There was no significant difference between the proportion of Confirmed Shivers horses receiving commercial grain vs. Control horses (P=0.6). Forty eight % (13/27) of Confirmed Shivers horses received a commercial grain ration as did 58% (29/50) of Controls. Amount of concentrates fed per day was similar at 1-2.2kg in both the Confirmed Shivers (9/27) and Control (29/50) groups. The Confirmed Shivers group received vitamin E (10/27), selenium (6/27), a mineral or salt block (22/27) and a joint supplement (7/27) most commonly. The Control group received most frequently a joint supplement (12/50), mineral (18/50) or salt (22/50) block. Only 2 Control horses received Vitamin E and selenium supplementation and this was significant lower when compared to the Confirmed Shivers group (p<0.01).
UNIVERSITY OF MINNESOTA EQUINE CENTER Stephanie Valberg
7
Frequency and Progression of Shivers: Signs of Shivers occurred similarly across groups with signs occurring most commonly on a daily basis when the horses were BW. Less than 12% of horses had signs less frequently than weekly and most horses showed a similar worsening of signs Improvement was noted in a small proportion of horses across groups; Where improvement was reported, it was mostly over months or years without total resolution of signs. There was no significant effect of breed on the progression of signs (p>0.05). There was no significant difference between the stresses noted, including those preceding and occurring 1 year after Shiver signs began. Long distance transportation was the most commonly reported stress both preceding and occurring within 1 year of Shivers signs. Where stress was experienced (either before or after onset of signs) 13-70% reported worsening, 24-40% reported no change and 3-7% reported improvement in signs. There was no significant difference in the illnesses noted in control and Shivers horses. Treatments: Many treatments were given. These included medications; alpha-2 agonists (n=19), NSAIDs (n=46), muscle relaxants (n=12), phenytoin (n=1), carbamazepine (n=1), gabapentin (n=1), and fluphenazine (n=1). Eight horses also received ‘Herbs’ to improve the clinical signs of Shivers. Previous acupuncture and chiropractic work was also reported, acupuncture was reported in 27 individuals over the three affected groups and chiropractics in 57 horses. There was no consistent improvement reported for any of the medications or herbal treatments with the exception of the alpha-2 agonists that appeared to provide temporary cessation of the signs to facilitate farrier work on the hind-limbs. MATERIALS AND METHODS Objective 2: The histopathology of Shivers Horses: Six horses (3 Warmblood and 3 Clysdesdales) with Shivers and 4 healthy age matched Warmblood or Thoroughbred control horses received a full neurologic examination. The Warmblood horses with Shivers comprised 2 Hanoverian mares and one Oldenburg gelding ranging in age from 5-6 yrs. The 3 Clydesdale geldings ranged in age from 3 to 8 yrs. The 4 control horses consisted of 2 Thoroughbreds, one mare and one gelding (6 yrs) and 2 Warmblood mares ranging on age from 4 to 10 yrs. Post-mortem examination: All horses were donated to the University of Minnesota and euthanized after neurologic examination. Within 30 min of euthanasia, samples of the biceps femoris, sacrocaudalis, gluteus medius, semimembranosus, vastus lateralis, cranial tibial and triceps muscles were removed for histology. The brain and spinal cord to the level of L1 was removed within an hour of euthanasia and placed in formalin. The spinal cord distal to L1 remained in situ and the sacrum was dissected free by disarticulating the femurs, severing the vertebral column at L1-S1 and severing the vertebrae distal to coccygeal 3. A sacrococcygeal dorsal laminectomy exposed the terminal spinal cord and cauda equina and the entire sacral block was placed in a tub containing 20% formalin to ensure rapid fixation. Nerve roots, ganglia and peripheral nerves were preserved intact as much as possible. Subsequently in situ cross-sections of spinal cord segments, sensory
UNIVERSITY OF MINNESOTA EQUINE CENTER Stephanie Valberg
8
and motor nerve root ganglia and sciatic nerve segments [especially branches supplying biceps femoris (abductor and flexors of stifle) and cranial tibial muscle (flexor of hock)] were removed. Muscle Histochemistry:. A ½ inch cube of tissue was mounted in cross-section andfrozen in isopentane chilled in liquid nitrogen. Sections 10 µm thick were cut with a cryostat. Samples were stained with H&E, modified Gomori Trichrome, nicotinamine adenine dinucleotide tetrazolium reductase (NADH), adenosine triphsphatase (pH 4.6) and periodic acid Schiff’s (PAS) stains. Staining of neurologic tissue: General neuropathologic changes were evaluated in H&E stains of the entire central nervous system. Selected cross-sections of the caudal spinal cord (S1 and S2) where lesions were most prominent were evaluated with special stains to enhance neuropathologic lesions. Immunohistochemical stains included Neurofilament (NF) for axonal degeneration, Silver stains, calbindin, calretinin and Glial fibrillary acidic protein for astrocyte reactivity. RESULTS AIM 2: The histopathology of Shivers Neurologic exam: No evidence of abnormal mentation, cranial nerve deficits or proprioceptive deficits was present in any of the horses. The Warmblood horses showed hyperflexion of the hindlimbs when backing, manually lifting the limb or moving sharply sideways. The Clydesdale horses had extreme hyperextension of the hindlimbs when backing and difficulty when manually holding up a limb. In addition, the Clydesdales showed other gait asymmetries such as placing the limbs across midline or occasional hyperflexion of a limb when walking forward. When asked to walk backwards all of the Shivers horses appeared mentally distressed with one Warmblood flinging her head at the handler each time she was asked to back up and one Clydesdale completely refusing to attempt more than one step.
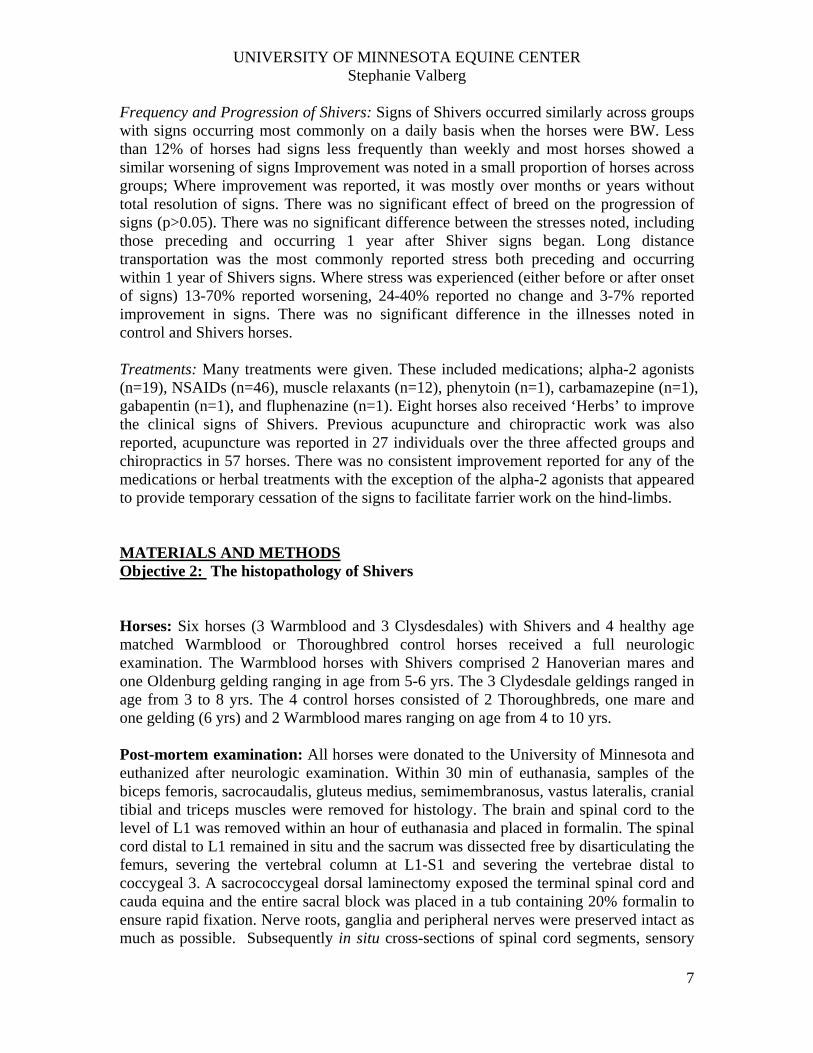
Muscle histochemistry: Muscle samples from all horses appeared normal in H&E stains. There was no evidence of myodegeneration or neurogenic atrophy in any of the muscle samples evaluated. In PAS stains for glycogen, the most significant finding was that the
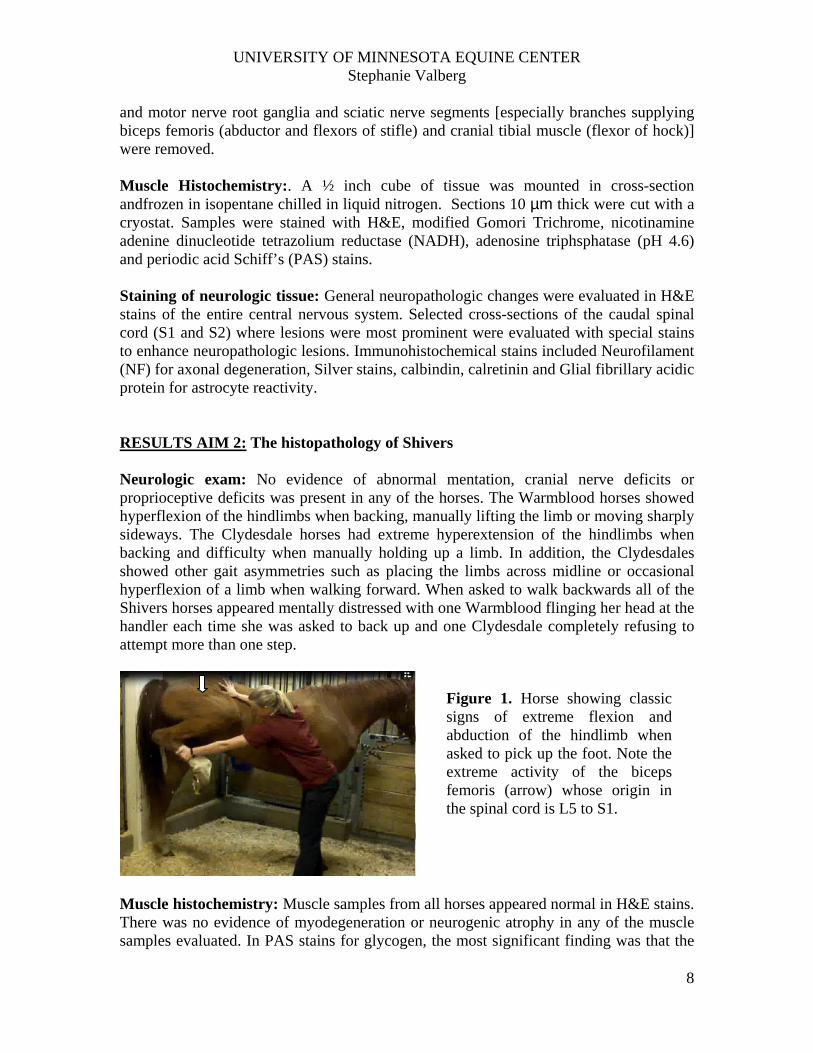
Figure 1. Horse showing classic signs of extreme flexion and abduction of the hindlimb when asked to pick up the foot. Note the extreme activity of the biceps femoris (arrow) whose origin in the spinal cord is L5 to S1.
UNIVERSITY OF MINNESOTA EQUINE CENTER Stephanie Valberg
9
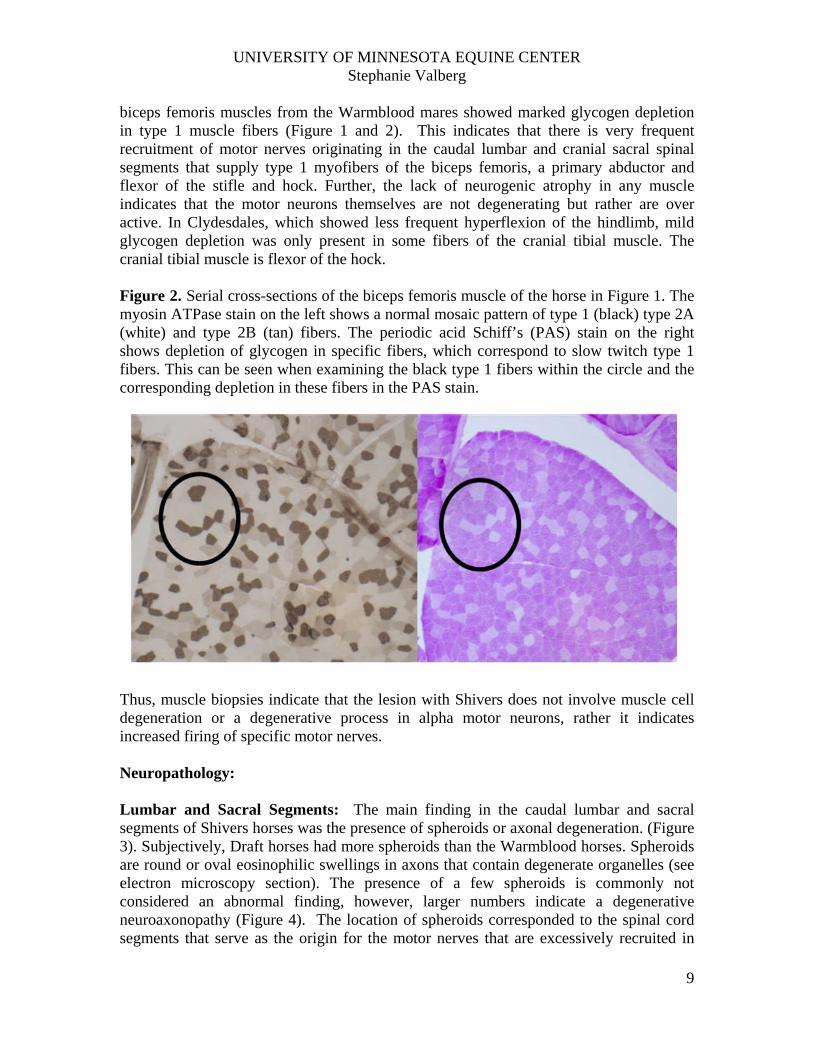
biceps femoris muscles from the Warmblood mares showed marked glycogen depletion in type 1 muscle fibers (Figure 1 and 2). This indicates that there is very frequent recruitment of motor nerves originating in the caudal lumbar and cranial sacral spinal segments that supply type 1 myofibers of the biceps femoris, a primary abductor and flexor of the stifle and hock. Further, the lack of neurogenic atrophy in any muscle indicates that the motor neurons themselves are not degenerating but rather are over active. In Clydesdales, which showed less frequent hyperflexion of the hindlimb, mild glycogen depletion was only present in some fibers of the cranial tibial muscle. The cranial tibial muscle is flexor of the hock. Figure 2. Serial cross-sections of the biceps femoris muscle of the horse in Figure 1. The myosin ATPase stain on the left shows a normal mosaic pattern of type 1 (black) type 2A (white) and type 2B (tan) fibers. The periodic acid Schiff’s (PAS) stain on the right shows depletion of glycogen in specific fibers, which correspond to slow twitch type 1 fibers. This can be seen when examining the black type 1 fibers within the circle and the corresponding depletion in these fibers in the PAS stain. Thus, muscle biopsies indicate that the lesion with Shivers does not involve muscle cell degeneration or a degenerative process in alpha motor neurons, rather it indicates increased firing of specific motor nerves. Neuropathology: Lumbar and Sacral Segments: The main finding in the caudal lumbar and sacral segments of Shivers horses was the presence of spheroids or axonal degeneration. (Figure 3). Subjectively, Draft horses had more spheroids than the Warmblood horses. Spheroids are round or oval eosinophilic swellings in axons that contain degenerate organelles (see electron microscopy section). The presence of a few spheroids is commonly not considered an abnormal finding, however, larger numbers indicate a degenerative neuroaxonopathy (Figure 4). The location of spheroids corresponded to the spinal cord segments that serve as the origin for the motor nerves that are excessively recruited in
UNIVERSITY OF MINNESOTA EQUINE CENTER Stephanie Valberg
10
Shivers horses. In immunohistochemiscal preparation with phosphorylated neurofilament (NF), axonal spheroids were strongly stained, indicating a large accumulation of this intermediate filament in the affected axonal segments (Fig 4). In affected areas, in H&E section, there was also mild gliosis that was confirmed by Glial fibrilary acidic protein (GFAP) inmmunohistochemistry. A large number of reactive astrocytes were detected in severely affected sacral segments as a consequent of loss of functional cellular elements. Thus, the present study is the first to identify neuropathology in Shivers horses and classifies this disorder as a degenerative neuroaxonopathy. Thoracic and cervical spinal cord: There were a number of axonal spheroids and “digestion chambers” randomly affecting the white and gray matter in Shivers horses. In contrast to lesions in the lumbosacral segments, these changes were discreet and distributed inconsistent across the 7 cervical and 13 thoracic segments. Peripheral nerve: Longitudinal and cross-sections of peripheral nerve and spinal cord ganglia revealed no histopathologic abnormalities. This supported muscle histology that indicated normal enervation of muscle fibers.
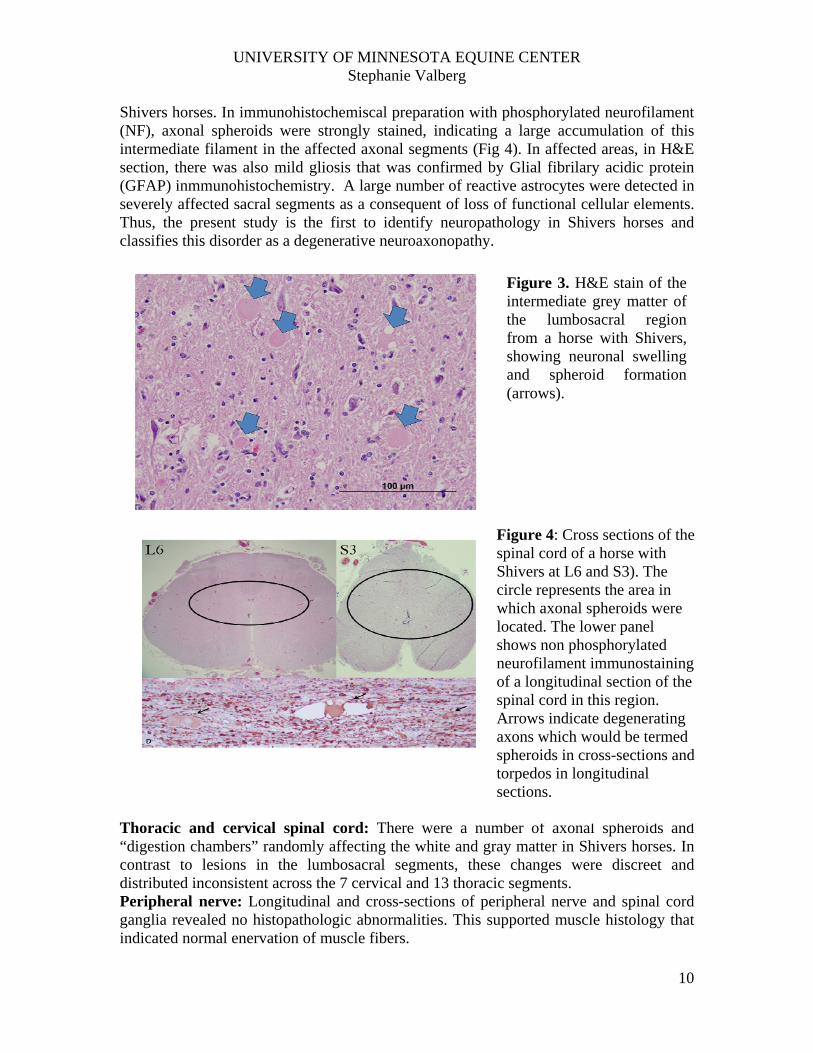
Figure 3. H&E stain of the intermediate grey matter of the lumbosacral region from a horse with Shivers, showing neuronal swelling and spheroid formation (arrows).
Figure 4: Cross sections of the spinal cord of a horse with Shivers at L6 and S3). The circle represents the area in which axonal spheroids were located. The lower panel shows non phosphorylated neurofilament immunostaining of a longitudinal section of the spinal cord in this region. Arrows indicate degenerating axons which would be termed spheroids in cross-sections and torpedos in longitudinal sections.
UNIVERSITY OF MINNESOTA EQUINE CENTER Stephanie Valberg
11
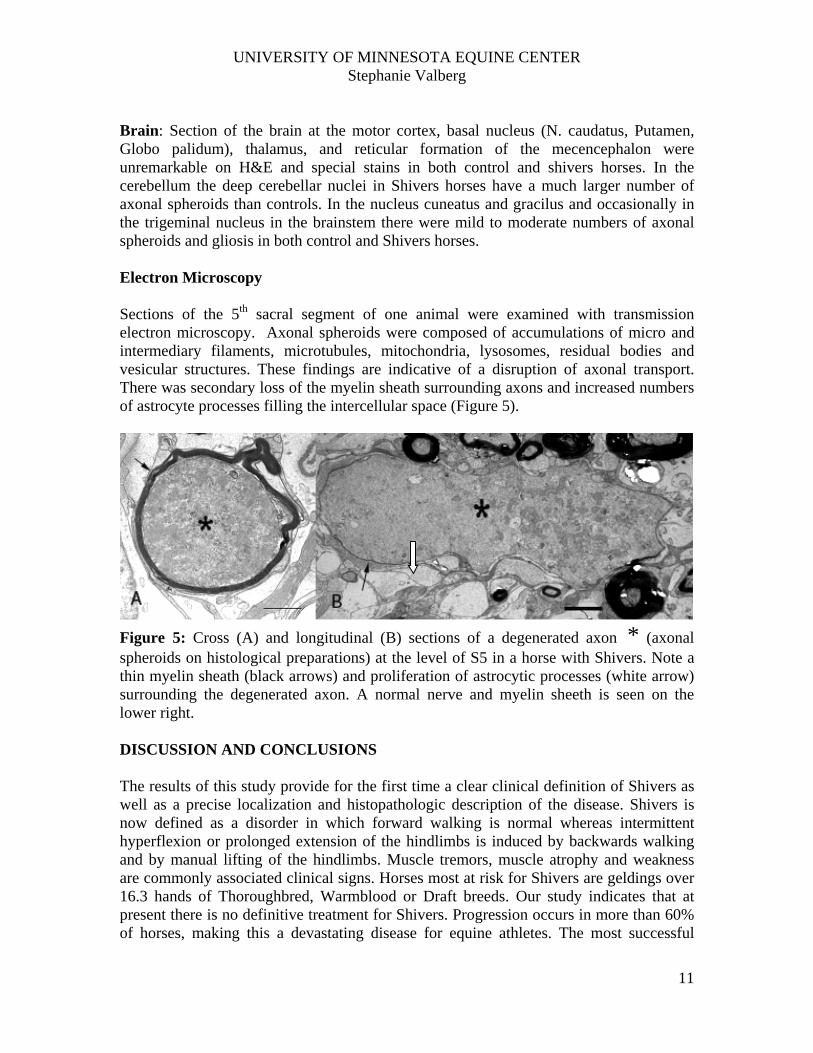
Brain: Section of the brain at the motor cortex, basal nucleus (N. caudatus, Putamen, Globo palidum), thalamus, and reticular formation of the mecencephalon were unremarkable on H&E and special stains in both control and shivers horses. In the cerebellum the deep cerebellar nuclei in Shivers horses have a much larger number of axonal spheroids than controls. In the nucleus cuneatus and gracilus and occasionally in the trigeminal nucleus in the brainstem there were mild to moderate numbers of axonal spheroids and gliosis in both control and Shivers horses. Electron Microscopy Sections of the 5th sacral segment of one animal were examined with transmission electron microscopy. Axonal spheroids were composed of accumulations of micro and intermediary filaments, microtubules, mitochondria, lysosomes, residual bodies and vesicular structures. These findings are indicative of a disruption of axonal transport. There was secondary loss of the myelin sheath surrounding axons and increased numbers of astrocyte processes filling the intercellular space (Figure 5).
Figure 5: Cross (A) and longitudinal (B) sections of a degenerated axon * (axonal spheroids on histological preparations) at the level of S5 in a horse with Shivers. Note a thin myelin sheath (black arrows) and proliferation of astrocytic processes (white arrow) surrounding the degenerated axon. A normal nerve and myelin sheeth is seen on the lower right. DISCUSSION AND CONCLUSIONS The results of this study provide for the first time a clear clinical definition of Shivers as well as a precise localization and histopathologic description of the disease. Shivers is now defined as a disorder in which forward walking is normal whereas intermittent hyperflexion or prolonged extension of the hindlimbs is induced by backwards walking and by manual lifting of the hindlimbs. Muscle tremors, muscle atrophy and weakness are commonly associated clinical signs. Horses most at risk for Shivers are geldings over 16.3 hands of Thoroughbred, Warmblood or Draft breeds. Our study indicates that at present there is no definitive treatment for Shivers. Progression occurs in more than 60% of horses, making this a devastating disease for equine athletes. The most successful

UNIVERSITY OF MINNESOTA EQUINE CENTER Stephanie Valberg
12
management strategy was to keep horses active which may help to delay the decline of important neuronal connections. The fact that Shivers primarily affects horses while walking backwards and not forwards suggests that specific neurons involved in coordinating flexor and extensor muscles of the hindlimb during backward locomotion are targeted in this disorder. Hindlimb locomotion is generated and regulated by interactions between spinal networks, supraspinal inputs, and sensory feedback from the periphery (Rossignol et al. 2006). At the core of the locomotor control system are spinal neuronal networks, so-called central pattern generators (CPGs), which can produce rhythmic-patterned outputs without supraspinal inputs or sensory feedback. The CPGs responsible for forelimb and hindlimb locomotion are localized in the intermediate grey matter of the cervical and lumbar spinal cord, respectively (Goulding 2009). It is thought that each limb is controlled by a separate CPG but that functional and anatomical connections exist to coordinate their activities. Neuronal pathways contained within the spinal cord are thought to be critical for quadrupedal coordination by coupling cervical and lumbar CPGs. CPGs may be multilayered where a timing module regulates temporal characteristics of the stepping behavior and a pattern module controls the specific groups of muscles required to execute the task. Backwards walking may utilize the same temporal modulator but a different pattern module than forwards walking (Boltona 2012). Our findings would be consistent with Shivers specifically affecting the hindlimb pattern module for backwards walking. We are, however, very intrigued by the most recent finding of a large number of axonal spheroids within the deep cerebellar nuclei of Shivers horses not present in controls. We are currently performing special stains to indentify the origin of the cerebellar neurons that exhibit axonal degeneration. Preliminary findings suggest that Purkinje cells may be involved which raises the possibility that Shivers may be due to abnormal mortoric regulation of locomotor patterns in Shivers horses. In conclusion, the results of this study show that Shivers is a slowly progressive degenerative central neuroaxonopathy which results in difficulty walking backwards and holding up the limb. No effective treatment was identified but progression may be slowed by keeping horses active and exercised. REFERENCES Boltona D.A.E. Misiaszek J.E. (2012) Compensatory balance reactions during forward and backward walking on a treadmill. Gait & Posture 35(4):681–684. Goulding M. (2009). Circuits controlling vertebrate locomotion: moving in a new direction. Nat.Rev. Neurosci. 10(7): 507-18. Hahn CN, Matiasek K, Dixon PM, Molony V, Rodenacker K, Mayhew IG. (2008) Histological and ultrastructural evidence that recurrent laryngeal neuropathy is a bilateral mononeuropathy limited to recurrent laryngeal nerves. Equine Vet J. 40(7):666-72.
UNIVERSITY OF MINNESOTA EQUINE CENTER Stephanie Valberg
13
Dixon PM, McGorum BC, Railton DI, Hawe C, Tremaine WH, Pickles K, McCann J. (2001) Laryngeal paralysis: a study of 375 cases in a mixed-breed population of horses Equine Vet J.33(5):452-8. Shivers presentations with abstracts or proceedings
1. Draper, J Bender, A Firshman, JD Baird, S Reed, IJ Mayhew and SJ Valberg. The epidemiology of Shivers. ACVIM forum 2012
2. Draper, J Bender, A Firshman, JD Baird, S Reed, IJ Mayhew and SJ Valberg. The epidemiology of Shivers. Points of Pride Research day, University of Minnesota 2012
3. Valberg SJ Movement Disorders in Horses: Shivers, Stringhalt and Other Conundrums ACVIM forum 2012
Submitted for publication ACE Draper BVetMed1, JB Bender DVM1, AM Firshman BVSc PhD1, JD Baird BVSc PhD2, S Reed DVM3, IJ Mayhew DVM PhD4 and SJ Valberg DVM PhD1 Epidemiology of Shivers in Horses
ACE Draper BVetMed MS1, AM Firshman BVSc PhD1, JD Baird BVSc PhD2, S Reed DVM3, IG Mayhew BVSc PhD4 R MacKay BVSc PhD5, T Trumble DVM PhD1, and SJ Valberg DVM PhD1 Posture and Movement Characteristics of Forward and Backward Walking in Horses with Shivers and Acquired Bilateral Stringhalt