Embed Size (px)
Citation preview

_____________________________________________________________________________________Gerd Richter, M.D., Ph.D., Professor of Internal Medicine, Director Clinical Ethics Consultation Service,University of Marburg, School of Medicine, IRB (Ethikkommission), Baldingerstrasse, D-35033Marburg, Germany; e-mail: [email protected].
Greater Patient, Family and Surrogate Involvement inClinical Ethics Consultation: The Model of Clinical EthicsLiaison Service as a Measure for Preventive Ethics
Gerd Richter
Introduction
Over the past decade clinical ethics has received growing attention inGermany as in most European countries. In the mid 1990s, most Europeancountries made efforts to establish healthcare ethics committees (HEC) andclinical ethics consultation services (CEC). The development of clinicalethics discourse and activities in Germany, however, was delayed andconsequently is still in its nascent state. Until the end of the 1990s, the onlyinstitutionalized bodies of ethical reflection were the research ethicscommittees at university medical centers and at the State PhysicianChambers. In March 1997, the Catholic and Protestant hospital associationin Germany recommended the implementation of HECs, modeled after theAmerican HECs. Consequently, the establishment of clinical ethicsconsultation in the form of HECs started in Germany in denominationalhospitals, which are generally smaller hospitals, followed by a small butincreasing number of community hospitals. Although university hospitals arestill reluctant to create HECs (Vollmann, Burchardi, & Weidtmann, 2004)due to the hierarchical structure of the German medical system, a scientificinitiative to foster ethics consultation was started in October 1998 by S.Reiter-Theil from the University of Freiburg (Reiter-Theil & Illhardt, 1999).At present, only some university medical centers (Hannover, Erlangen,Tuebingen) have established an HEC and few have an institutionalizedethics consultation service (e.g., Marburg, Freiburg). Due to the rigidGerman medical system and the strong physician driven hierarchy inGerman medical decision-making, the establishment and institutionalizationof clinical ethics in practice have a number of prejudices and fears toovercome. Expressions like “ethics consultant”, “ethical/moral knowledge
HEC Forum (2007) 19 (4): 327–340.DOI 10.1007/s10730-007-9047-0 © Springer 2007

and expertise”, and “clinical ethics committee” may often be misunderstoodby physicians and patients as representing an erosion of professionalautonomy, a further bureaucratization of the physician-patient relationship,with particular individuals who are legally authorized to dole out bindingjudgments, a supervisory body, or even an individual or group with specialmoral knowledge or virtue (Melley, 2001). In this regard, newly establishedHECs report a lack of requests for ethics consultations and report that the“distance” between clinical staff and HECs is very difficult to bridge. Oneapproach to overcome these types of issues is to develop an ethics liaisonservice similar to the one that is functioning successfully at the MarburgUniversity Medical Center (Richter, 2001). The ethics liaison service isdesigned to enable and empower physicians and other clinicians/health careprofessionals to address ethical questions and problems as they arise in thecourse of individual patient care without formal ethics consultation. It alsoinvolves patients, families, and surrogates in the discussion of ethical issuesin the course of patient care. The possible advantages and disadvantages ofimplementing such an approach for clinical ethics in the German context isdescribed in the following section.
Concepts of and Approaches to Clinical Ethics Consultation
The physician-patient-relationship in the German health care system ischanging dramatically under the influence of three factors: growingrecognition of the rights of individuals in medical decision making, valueheterogeneity, and the increasing complexity of decision making due totechnological development in all areas of medical care. These three factorscreate a greater necessity for physicians and other health care professionalsto spend more time with patients and create a need for patients to be moreactively involved in their health care, particularly in decision making. Thesesalient features drive medical decision making in Germany from a traditionalpaternalistic approach to a democratic shared decision making process.
Due to these changes in the clinical setting, the awareness of clinicalethics is growing and the need for ethics consultation is increasinglyrecognized. Some German physicians consider the introduction ofdemocratic decision making structures a threat to physician authority andpower (Reiter-Theil & Illhardt, 1999). They compare ethics consultation toan acting moral “police” that will erode the decision making authority ofphysicians. There is some concern that an increasing utilization of ethicsconsultation may move ethics to the periphery of clinical practice, which isbest to be left to experts. Clinical ethics, in general, and ethics caseconsultation, in particular, has to pay attention to these fears and introduce
328 HEC Forum (2007) 19 (4): 327–340.

concepts and procedures that are compatible with the German health carecontext.
If complexity of technology-driven modern health care, valueheterogeneity, individual rights, and the implications of a changingphysician-patient-relationship create a need for clinical ethics, we have to setup and define very carefully the goals of clinical ethics and ethicsconsultation. In preparation for an ethics case consultation service, it shouldbe clear that ethically and legally informed clinicians, especially physiciansand nurses, are the key moral problem solvers in patient care. The role ofethics case consultation has four elements that vary in constancy from caseto case: moral diagnostician (always), educator (always), mediator (whenneeded), and bridge to authority (when indicated).
Ethics consultation is a service provided by an individual consultant,team, or committee to address the ethical issues involved in a specificclinical case. The goals of clinical ethics and ethics consultation can bedescribed as follows (Fletcher & Siegler, 1996; Fletcher, 1991):• to maximize benefit and minimize harm to patients, families, health care
professionals and institutions by fostering a fair and inclusive decisionmaking process that honors patient/proxy preferences as well asindividual and cultural value differences among all parties to theconsultation (educator, mediator);
• to increase shared decision making in the resolution of ethical problemsin individual patient care (educator, mediator);
• to facilitate resolution of conflicts in a respectful atmosphere withattention to the interests, rights, and responsibilities of those involved(educator, mediator);
• to prevent poor outcome of cases involving ethical problems (mediator,educator);
• to increase knowledge of self and others (mediator, educator);• to inform institutional efforts at quality improvement, appropriate
resource utilization, and policy development by identifying the causes ofethical problems and to promote practices consistent with the highestethical norms and standards—organizational ethics (bridge to authority);and
• to assist individuals in handling current and future ethical problems byproviding education in health care ethics—to increase knowledge ofclinical ethics (educator).
In the light of these goals, a clinical ethics program has to cover thefollowing areas:• providing education in clinical ethics for clinicians, patients, surrogates,
and the larger community;
HEC Forum (2007) 19 (4): 327–340. 329

• doing policy studies and making recommendations for institutional andcommunity guidelines to address various ethical issues, e.g., DNR-orders, foregoing life-sustaining treatment, surrogate decision making,advance directives, brain death determination (policy development); and
• providing a process for case consultation at the bedside or conferenceroom (ethics consultation).
Clinical ethics case consultation needs to be woven into a clinical ethicsprogram and should not be separated from the other tasks. Ethicsconsultation can only be successful by carrying out each of these threedifferent objectives. The top priority for clinical ethics programs is not ethicscase consultation in itself, but rather education for clinicians to broaden theirethical perspectives and practice skills in participating in a shared decisionmaking process and working through ethical problems. Because cliniciansare the primary moral problem solvers in patient care, this role has to berespected by ethics consultation. By affirming the priority of education andthe primary role of clinicians as moral problem solvers, the impression thatthe standard for resolving ethical problems in patient care is ethics caseconsultation can be avoided. If ethics case consultation was the standard ofcare, clinicians would be obliged to request it for each identifiable ethicalproblem. Such a practice would displace clinicians as primary moralproblem solvers and result in disaster. Therefore, the approach of clinicalethics case consultation should be pragmatic and problem-centered andshould strive to enable and empower clinicians to deal appropriately withethical problems.
The irreducible contextual dimension is the key feature of clinical ethicsconsultation and any approach and methodology of clinical ethics must besensitive and responsive to it. Context-sensitive moral reasoning is thechallenge that every clinical ethicist must meet.
Clinical ethics case consultation can be provided in several ways: by anethics consultative group as a whole (such as a HEC), by a subgroup of aconsultative group, or by individual consultants. Starting with an officialrequest by the health care professionals or the patient/surrogate/family, theethics consultation service will be called into an actual patient case thatpresents difficult and unresolved ethical problems. All of these differentsettings to clinical ethics case consultation have advantages anddisadvantages, but each shares the feature of acting only on an alreadyexisting ethical dilemma or crisis in a concrete case of patient care (Kanoti &Youngner, 2003; Rushton, Youngner, & Skeel, 2003; DeRenzo, Vinicky, &Redman et al., 2006) and, therefore, have limited possibilities to trainclinicians in clinical ethics during daily work.
330 HEC Forum (2007) 19 (4): 327–340.

Clinical Ethics Liaison Service
To avoid ethical dilemmas or crises and to act preventively in regard toethical issues in concrete patient care, ethics liaison service is an additionaloption for ethics case consultation (Richter, 2001; DeRenzo, Vinicky, &Redman et al.; Agich, 2003). In an ethics liaison service, the clinical ethicistbelongs to the team of a unit (ICU) or department and does not get called inon particular cases for ethics consultation. Joining the medical team onroutine rounds and being available as a team member by beeper is a naturalenhancement to routine activities on a unit like an ICU. The task for theliaison clinical ethicist is to assist patients and the team in thinking throughpossible ethical issues relevant to a particular patient’s care within the timeframe optimal to the patient’s needs to avoid ethical dilemmas or crises.Accepting the involved clinicians as the primary decision makers in thecourse of patient care, the clinical ethicist facilitates clinical decision makingin regard to ethical issues without taking responsibility for direct patient careor in deciding for others. Respecting this crucial point, the clinical ethicistenables shared clinical decision making as a result of all parties involved in aparticular patient’s care (clinicians, patient, family) and does not act as anethics expert by making independent recommendations or decisions.Through this process, the focus and the task of the clinical ethicist isfundamentally different from other medical consultants.
By adopting the ethics facilitation approach, the regular and frequentpresence of the clinical ethicist has some advantages in comparison to theon-call ethicist or HEC. The liaison ethicist is able:• to be present frequently and regularly on the floor during daily work;• to anticipate ethical issues—discussion of cases and actions on rounds,
personal discussions or staff meetings before an ethical problem occursas a dilemma or crisis (preventive ethics);
• to provide a speedy response to any ethical concerns raised by staff,patients, families, or surrogates;
• to provide assistance and support for staff and patients (in choosing asurrogate decision maker, obtaining legal guardianship, to arrange staff-family/surrogate meetings, mediating conflicts between care givers andpatients/families/surrogates in withdrawing life sustaining treatment);
• to provide relevant and accurate information as an information resourceon ethical and legal issues whenever it is needed (DNR-order, life-forgoing treatment, living wills and advanced directives, patients rights);
• to enable and empower physicians and other clinicians to dealappropriately with ethical issues by themselves through informalteaching during rounds and staff conferences;
HEC Forum (2007) 19 (4): 327–340. 331

• to reduce bureaucracy by addressing ethical questions and problems asthey arise in the course of patient care without the necessity of formalethics consultation;
• to lower hierarchy (e.g., to enable everybody of the team to raise ethicalissues in patient care, to facilitate that everyone’s concerns andarguments are heard, to mediate intra-staff conflicts when disagreementwithin the therapeutic team arise about an individual patient’s care, toinsist and mediate that optimal moral discourse requires flatteningtraditional power hierarchies during moral discussion and ethicalarguments);
• to increase attention for clinical ethics within the hospital with a chancethat clinical ethics case consultation will spread out to other clinicaldepartments and services.
Stressing these features of an ethics liaison service, it becomes clear thatthis concept has many advantages. For example, with a clinical ethicistregularly on hand, sensitivity to the ethical dimensions of clinical practicecan be increased in all involved health care professionals. This might entailgreater and faster recognition of ethical problems arising in the course ofpatient care. With a clinical ethicist on the team, questions about ethicalissues can be asked and ethical problems can be discussed beforehand toprevent an ethical crisis or dilemma. Such a preventive approach is clearlybetter than a crisis-management approach to recurrent ethical problems andis superior to all other ethics consultation approaches when the ethicsconsultant has to be called in following the existence of an already evolvedethical crisis or dilemma. Preventive clinical ethics is able to handle non-dilemmatic ethical issues before an ethical crisis occurs.
Clinical Ethics Liaison Service at the University Surgery DepartmentMarburg
Marburg University Medical Center is a public 1,255-bed tertiary hospitalwith 28 clinical departments affiliated with the Philipps-University School ofMedicine. An ethics liaison service is much more time consuming for theclinical ethicist than ethics consultation on request, thus it may be mostsuitable for smaller organizational units in a hospital in which ethicalproblems arise recurrently in the course of patient care, such as an ICU.Taking this into account, an ethics liaison service was started in 1998 in thesurgical intensive care unit (SICU), which has 12 beds and belongs to thedepartment of trauma and reconstructive surgery and to the department ofvisceral, thoracic and vascular surgery. The liaison-approach to clinicalethics consultation also has been established in the internal medical intensive
332 HEC Forum (2007) 19 (4): 327–340.

care unit (MICU), the neonatal intensive care unit (NICU), and the intensivecare unit of the department of anesthesiology. Ordinary ethics consultationservice on request is also available.
The liaison ethics consultation service at the SICU was established in1998 (Richter, 2001). Before starting an ethics consultation service at theSICU, the clinical ethicist analyzed the need, negotiated with the chairmanof the surgery department, introduced the concept and goals of clinicalethics, clarified the setting by interviewing the senior physician, residents,and nurses and giving a grand rounds presentation on clinical ethicsconsultation. In explaining the concept of an ethics liaison service tophysicians, nurses, and other clinicians of the SICU, it became clear that thestart of such a service would be an experiment and an ongoing learningexperience. The ethics liaison service was introduced as a combined bottom-up/top-down approach: it was instituted both at the request of attendants,residents, and nurses and after negotiation and approval by the chairman.After clarifying the setting, the clinical ethicist joined the team and became amember of the SICU. During the first period (1998-2003), the liaison servicewas provided by an individual consultant, a physician-ethicist with abackground in internal medicine, gastroenterology, and philosophy/ethics. In2004, a medical sociologist with background in medicine, sociology, andethics was invited to join the team. In 2002, further development was madepossible through a newly created position for a physician-ethicist, who haspart time responsibilities for patient care and ethics (clinical ethics and IRBwork) and in 2003 of an additional position for a medical sociologist/ethicist.
The ethics facilitation approach (ASBH, 1998, pp. 5-7) based on themethod of clinical pragmatism was adopted by the clinical ethicist (Miller,Fins, & Bacchetta, 1996; Miller, Fletcher, & Fins, 1997; Fins, Bacchetta, &Miller, 1997; Fins, Miller, & Bacchetta, 1999). The physicians on the unitwere relieved that the clinical ethicist did not function as a moral decisionmaker. They learned to participate in a shared decision making process withthe patients, families, proxies, and nurses. It was clear from the beginningthat clinicians had to learn that clinical ethics consultation was indeeddifferent from medical consultation. In the beginning of the ethics liaisonservice, the clinical ethicist was asked explicitly to give recommendationsand advice and to make decisions. It was important to clarify the concept ofethics facilitation to the clinicians again and again so that the role of theclinical ethicist as educator and mediator became clear during the first yearof service.
The clinical ethicist meets with staff regularly once a week to go onrounds when the residents change shifts and during staff conferences. Theethicist accompanies rounds with the attendant, residents, medical students,
HEC Forum (2007) 19 (4): 327–340. 333
and nurses offering them a chance to ask questions where ethical problemsmight be an issue. Rounding with physicians, medical students, and nurses itbecame clear that the contextual dimension of clinical ethics consultationwas the most important point during these rounds. This broadening ofperspectives was very much appreciated by the staff. Most questions thatarose involved acceptance of advance directives, withdrawing life-sustainingtherapy, writing a DNR-order, choosing a surrogate decision maker,obtaining legal guardianship, and how to resolve a disagreement within thetherapeutic team about a patient’s care.
During a five year period (2000-2004), 595 cases were discussed forethical reasons on rounds with the clinical ethicist (Table 1). The majority ofthese cases are very familiar to any clinical ethicist. Exceptions to theseordinary clinical ethical issues are ethical problems originated in difficultiesin prognostication (151 cases), which is not reported as a frequent clinicalethical issue in bioethics literature. Christakis (1999) in his book DeathForetold: Prophecy and Prognosis in Medical Care, demonstrates howdifficult prognostication is and how important it is to a sound clinicaldecision making process. Prognosis is a fundamental, though implicit, basisfor many theoretical and practical ethical decisions in medical care, andprognostic uncertainty may considerably complicate such decisions.Prognostication and death are tightly interwoven and profoundly affectdecisions to initiate, withhold, or terminate life support in critically illpatients, especially in a SICU. Therefore, prognosis is a key element in theshared decision making process, especially with respect to end-of-life care toavoid disrespectful over-treatment. A prognosis can radically reshape thephysician’s and the patient’s therapeutic management of a conditionresulting, for example, in a shift from a curative to a palliative approach tocare. Prognosis is also a feature of the concept of futility because thisjudgment is based on a prognosis that the patient is unlikely to recoverspontaneously and that the intervention will likely be ineffective. Predictingrisks and benefits for patients in the presence of uncertainty is technicallydifficult and emotionally challenging for all physicians. Substantialuncertainty leads to one of two extremes in the formulation of prognoses(pessimism or optimism) and one of two extremes in therapeutic decisionmaking (aggressiveness or passivity). Each of these can harm patients. Whenprognostication in the course of patient care is unavoidable, physicians copewith difficulties in a number of ways, including recourse to certain cognitivebiases, magical ideas, and very often a ritualistic optimistic attitude. Theattitude not to abandon patients therapeutically at the end-of-life often leadsto a course of action that tends to avoid prognostication, but which may leadto disrespectful over-treatment. Needlessly incorrect prognoses harm
334 HEC Forum (2007) 19 (4): 327–340.

patients and contradict ethical sound decision making in medical care. Thediscussion of the course of critically ill patients in the SICU during ethicsrounds must take seriously the contextual dimension of an individual patient.Such consideration includes careful prognostication designed to reach thegoal of maximizing benefit while minimizing harm to patients, families,surrogates and to health care professionals. Indeed, it is crucial for carefulplanning of patient care.
DeRenzo et al. (2006) report on rounding with ICU teams as the preferredmodel for routine ethics case consultation. They conclude that the amount ofinvolvement and interaction with patients, families, and surrogate decisionmakers may be a flaw. They state that this model does not include much, ifany, interaction with patients or surrogates. Drawing upon our experiencewithin hundreds of non-dilemmatic ethics case consultations, theinvolvement of patients, families or surrogates was a regular goal of ethicaldiscussions about patient care. While rounding with the team, families andsurrogates were very often included in discussions or were invited to see thetreating physician or team to discuss ethical issues that arise in the patient’scare. Also, particular team conferences were offered to and arranged forfamilies and surrogates to think through ethical issues, and to reach aconsensus with the medical team (e.g., regarding withdrawing life-sustainingtreatment, writing DNR-orders, elaborating the patient’s will and wishes inthe course of a particularly patient’s treatment). Such discussions were veryoften mediated by the clinical ethicist. For the staff of the SICU, moraldiscourse in a particular case during ethics rounds triggered furtherinvolvement and discussions with families and surrogates. The prerequisitefor enhancing the involvement of patients, families, and surrogates is that allparties know that there is an ethicist on the team, who is introduced to themright at the beginning of the patient’s admission to the unit. This is of greatimportance because most of the patients of an intensive care unit have nodecision making capacity due to their physical and mental conditions.During the first year of the ethics liaison service, a policy was developed thatfor every patient who has no decision making capacity expected for morethan 24 to 48 hours a legal guardian should be appointed. In our opinion,seriously ill patients typically face major medical decisions as members of afamily rather than as isolated individuals and, therefore, familialrelationships give rise to moral responsibilities. These responsibilities arenurtured by an ethics of caring. Spouses, children, and other family membersprovide support, help, and care for patients whose lives are disrupted byillness and they are usually involved in the decision making process by thepatients themselves. Parents are intimately involved in the healthcare of theirchildren, and family members generally have the right and the responsibility
HEC Forum (2007) 19 (4): 327–340. 335

to speak for patients who are no longer capable of making decisions forthemselves (Fletcher, Miller & Spencer, 1997). During ethics rounds,patients are always introduced to the clinical ethicist on the team and areasked how much the family should be involved in their treatment plans,reaching informed consent for the degree of family involvement and respectfor patient confidentiality. By accepting familial situation of a patient, ratherthan using a strictly individualistic view, we try to take into consideration themoral dimensions of family life, which are part of the appropriate ethicalpractice of clinical medicine. When ethics rounds are a routine practice inthe daily life of an ICU setting and everybody, including patients, families,and surrogates, knows that an ethicist belongs to the team and that as ethicaldiscourse belongs to patients’ care planning, it is obvious that clinical ethicsconsultation is not an exception in daily clinical care. It is appreciated by thelarge majority of persons involved in the course of patient care. In thissetting, the will and wishes of the individual patient is at the center of theteam’s focus and the patient’s confidentiality can be respected. The mostimportant goal of ethics consultation is to maximize benefit and minimizeharm to patients, families, health care professionals, and institutions byfostering a fair and inclusive decision making process that honorspatient/proxy preferences and individual and cultural value differencesamong all parties to the consultation; together this goal can be achieved.
Physicians, nurses, and other staff of the SICU have accepted the ethicsliaison service, and highly appreciate the low bureaucratic, low hierarchicapproach to ethics consultation and easy access to clinical ethics resources.Evidence of the preventive measure of an ethics liaison service is that only14 of the 595 discussed cases reached the level of an official ethicsconsultation request during the reported 5 year period. Substantive ethicaldiscussion about complex ethical aspects of a patient’s care that hasimmediate relevance for medical decision making is important to avoidethical dilemmas and crises, as well as to achieve ethically appropriate careof patients. Out of 595 intensively discussed cases, 581 could be handled asnon-dilemmatic cases and serious conflicts could be avoided to thesatisfaction of all parties. Taking advantage of the ethics liaison service, theteam of the SICU became much more self-confident in handling ethicalissues in patient care.
In starting a clinical ethics consultation service on the SICU, rather than aHEC approach to ethics consultation, we avoided the experiences of manyHECs in Germany, which have struggled with only a small increase inrequests for ethics consultations in patient care over the last years. Incontrast, the local strategy in Marburg to start an ethics consultation programwith an ethics liaison service was accepted and was rapidly integrated into
336 HEC Forum (2007) 19 (4): 327–340.

daily health care. The successful implementation of the ethics liaison serviceat the SICU was followed by an extension of this service to various otherintensive care units (anesthesiology, pulmonary critical care, internalmedicine, pediatric and neonatal intensive care unit) and was accompaniedby an increasing number of formal ethics consultation requests fromdifferent departments of the University Medical Center Marburg.
Taking the hierarchical structure of the German medical system intoconsideration and reflecting on the experience in Marburg, it was initiallyadvantageous that the ethicist was a physician, but that should not be ajudgment in favor of physician ethicists versus ethicists with differentprofessional backgrounds. Since we successfully introduced a medicalsociologist as an additional ethics consultant, it has become clear that themedical community also accepts other professionals as clinical ethicists.
Drawing upon our experience within hundreds of non-dilemmatic ethicscase consultations and teaching clinical ethics consultation in a Germancurriculum most clinicians prefer a non-formal, lower bureaucratic approachto deal with clinical problems and also with ethical problems. They prefer anindividual clinical ethicist whom they know and trust over a committeeapproach. An ethics liaison service is most successful in reaching the prioritygoal of ethics consultation: serving patients by educating clinicians inclinical ethics. Such an approach makes access to clinical ethics much easierthan using official and formal ethics consultation requests or continuingmedical education. Learning clinical ethics in daily routine within arespected and trusted relationship, clinicians can overcome their notoriouslybad habits of collapsing ethical problems into medical or legal problems.They can listen to each other, including the clinical ethicist, patients, andfamilies, and non-defensively deliberate about ethical issues. With thiseducation-orientated approach to ethics consultation patients, families, andproxies have become more often and more deeply involved in discussions ofethical issues concerning the planning of care for their beloved ones andclinical ethics has become a much more accepted part of daily clinicalpractice than formal ethics consultation requests.
Besides the advantages of the ethics liaison service, there are also somelimitations and problems associated with this approach. DeRenzo et al.(2006) pointed out the following limitations of the rounding model of ethicsconsultation: 1) the ethicist’s focus is most heavily on the clinicianpresenting the case; 2) the prospect having the rounding ethicist coopted bythe clinicians; 3) rare interaction with patient and/or surrogate, which werejected (see above); and 4) the concern that the rounding ethicist is biasingin the same way as a “lone ranger” ad hoc clinical ethics consultant can bebiasing. The familiarity and good relationship with the clinical ethicist as a
HEC Forum (2007) 19 (4): 327–340. 337

team member can also create some difficulties or disadvantages to ethicsconsultation. Being too attached to individuals or, even worse, to a subgroupof the team (e.g., physicians or nurses), the clinical ethicist might loseobjectivity and not be able to foster a fair and inclusive decision makingprocess. Impartiality is a moral demand for all clinical ethicists doing caseconsultation, but more of a daily challenge for a liaison ethicist. In ourexperience, additional problems include documentation, reporting andsupervision within the approach of ethics liaison service. Ethics consultation,like other medical consultations, should be documented in the patient’smedical record. Good documentation requires an appropriate note in themedical record and a longer detailed account of the case suitable forevaluation and review (Agich, 2003; Fletcher & Moseley, 2003). The goalsof documentation are: 1) informing all hospital staff caring for the patient ofthe issue and important details of the consultation, 2) keeping an accuratehistory of all phases of the patient’s care, 3) aiding in education in clinicalethics and health law, and 4) aiding in quality assurance (Fletcher &Moseley, 2003). Although the ethics liaison consultant together with thephysician and nurse in charge write notes in the patient’s chart,documentation of the ethics input is different from formal ethics consultationrequests because the process of the ethics liaison service is more informaland consists of bedside discussions without the framework of formalconsultation. Whereas for official ethics consultations in various institutions,a record/documentation protocol/form is used, it is difficult or awkward todo the same in an ethics liaison service. Because of the importance of thedocumentation for report, review, evaluation, and quality management, weare still in the process of developing an ethics consultation report system thatis combined with the establishment of a HEC.
The combination of a HEC with an ethics liaison service, whose membersreport to the HEC on a regular basis to discuss, review, and supervisedecisions and to broaden both the perspectives of the individual ethicsconsultants and members of the HEC, seems to us the most promisingapproach to establish a self- reflexive and pragmatic clinical ethics service inlarge hospitals with intensive care units.
REFERENCES
Agich, G.J. (2003). Joining the team: ethics consultation at the ClevelandClinic. HEC Forum, 15, 310-322.
American Society for Bioethics and Humanities. (1998). Core competenciesfor health care ethics consultation: the report of the American Society for
338 HEC Forum (2007) 19 (4): 327–340.

( ) ( )
Bioethics and Humanities. Glenview: American Society of Bioethics andHumanities.
Christakis, N.A. (1999). Death foretold: prophecy and prognosis in medicalcare. Chicago: University of Chicago Press.
DeRenzo, E.G., Vinicky, J., Redman, B. et al. (2006). Rounding: a model forconsultation and training whose time has come. Cambridge QuarterlyHealthcare Ethics, 15 (2), 207-215.
Fins, J.J., Bacchetta, M.D. & Miller, F.G. (1997). Clinical pragmatism: amethod of moral problem solving. Kennedy Institute of Ethics Journal, 7,129-145.
Fins, J.J., Miller, F.G. & Bacchetta, M.D. (1998). Clinical pragmatism:bridging ethical theory and practice. Kennedy Institute of Ethics Journal,8, 37-42.
Fletcher, J.C. (1991). Ethics consultation: a service of clinical ethics.Newsletter of the Society for Biomedical Consultation, spring, 1-7.
Fletcher, J.C. & Siegler, M. (1996). What are the goals of ethicsconsultation? A consensus statement. J Clin Ethics, 7, 122-126.
Fletcher, J.C., Miller, F.G. & Spencer, E.M. (1997). Clinical ethics: history,content, and resources. In: J.C. Fletcher, P.A. Lombardo, M.F. Marshall,F.G. Miller (eds.), Introduction to clinical ethics, second edition.Frederick: University Publishing Group, pp. 3-20.
Fletcher, J.C. & Moseley, K.L. (2003). The structure and process of ethicsconsultation services. In: M.P. Aulisio, R.M. Arnold, S.J. Youngner(eds.), Ethics consultation. From theory to practice. Baltimore: JohnsHopkins University Press, pp. 96-120.
Kanoti, G.A. & Youngner, S. (2003). Clinical ethics consultation. In: S.G.Post, Encyclopedia of bioethics, third edition. New York: Macmillian, pp.439-443.
Melley, C. (2001). Clinical ethics consultation in Germany: a philosopher’sprognosis. HEC Forum, 13, 306-316
Miller, F.G., Fins, J.J. & Bacchetta, M.D. (1996). Clinical pragmatism: JohnDewey and clinical ethics. The Journal of Contemporary Health Law andPolicy, 13, 27-51.
Miller, F.G., Fletcher, J.C. & Fins, J.J. (1997). Clinical pragmatism: a casemethod of moral problem solving. In: J.C. Fletcher, P.A. Lombardo, M.F.Marshall, F.G. Miller, Introduction to clinical ethics, second edition.Frederick: University Publishing Group, pp. 21-40.
Reiter-Theil, S. & Illhardt, F.J. (1999). Initiative zur Ethik-Beratung in derMedizin. Ethik Med, 11, 219-221.
Richter, G. (2001). Ethics consultation at the University Medical Center-Marburg. HEC Forum, 13, 294-305.
HEC Forum (2007) 19 (4): 327–340. 339
Rushton, C., Youngner, S.J., & Skeel, J. (2003). Models for ethicsconsultation: individual, team, or committee. In: M.P. Aulisio, R.M.Arnold, S.J. Youngner (eds.), Ethics consultation. From theory topractice. Baltimore: Johns Hopkins University Press, pp. 88-95.
Vollmann, J., Burchardi, N., & Weidtmann, A. (2004). KlinischeEthikkomitees an deutschen Universitätskliniken. Dtsch MedWochenschr, 129, 1237-1242.
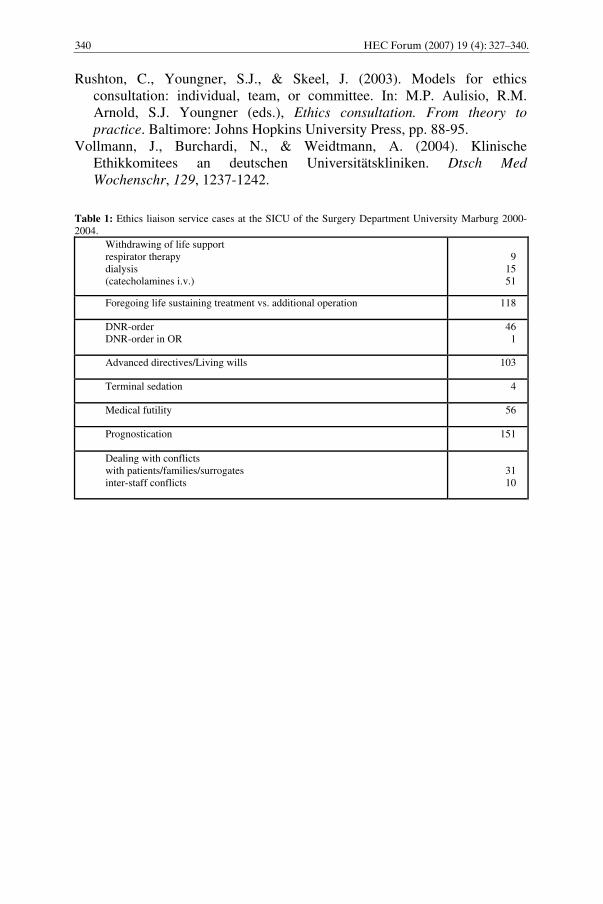
Table 1: Ethics liaison service cases at the SICU of the Surgery Department University Marburg 2000-2004.
Withdrawing of life supportrespirator therapydialysis(catecholamines i.v.)
91551
Foregoing life sustaining treatment vs. additional operation 118
DNR-orderDNR-order in OR
461
Advanced directives/Living wills 103
Terminal sedation 4
Medical futility 56
Prognostication 151
Dealing with conflictswith patients/families/surrogatesinter-staff conflicts
3110
340 HEC Forum (2007) 19 (4): 327–340.





























