Embed Size (px)
DESCRIPTION
The PROSPECT Trial. P roviding R egional O bservations to S tudy P redictors of E vents in the C oronary T ree. A Natural History Study of Atherosclerosis Using Multimodality Intracoronary Imaging to Prospectively Identify Vulnerable Plaque. Gregg W. Stone, MD - PowerPoint PPT Presentation
Citation preview

A Natural History Study of A Natural History Study of Atherosclerosis Using Multimodality Atherosclerosis Using Multimodality
Intracoronary Imaging to Prospectively Intracoronary Imaging to Prospectively Identify Vulnerable PlaqueIdentify Vulnerable Plaque
Gregg W. Stone, MDGregg W. Stone, MDPROSPECT InvestigatorsPROSPECT Investigators
PProviding roviding RRegional egional OObservations to bservations to SStudy tudy PPredictors redictors of of EEvents in the vents in the CCoronary oronary TTreeree
The The PROSPECTPROSPECT TrialTrial

The The PROSPECTPROSPECT TrialTrial
• Gregg W. StoneGregg W. Stone Scientific Advisory Board, Abbott Scientific Advisory Board, Abbott
Vascular Devices and Boston ScientificVascular Devices and Boston Scientific Consultant to InfraReDxConsultant to InfraReDx

• Most cases of sudden cardiac death and MI Most cases of sudden cardiac death and MI are believed to arise from plaque rupture with are believed to arise from plaque rupture with subsequent thrombotic coronary occlusion of subsequent thrombotic coronary occlusion of angiographically mild lesions (“vulnerable angiographically mild lesions (“vulnerable plaques”), the prospective detection of which plaques”), the prospective detection of which has not been achievedhas not been achieved
• The event rate attributable to progression The event rate attributable to progression of vulnerable plaque has never been of vulnerable plaque has never been prospectively assessedprospectively assessed
• Most cases of sudden cardiac death and MI Most cases of sudden cardiac death and MI are believed to arise from plaque rupture with are believed to arise from plaque rupture with subsequent thrombotic coronary occlusion of subsequent thrombotic coronary occlusion of angiographically mild lesions (“vulnerable angiographically mild lesions (“vulnerable plaques”), the prospective detection of which plaques”), the prospective detection of which has not been achievedhas not been achieved
• The event rate attributable to progression The event rate attributable to progression of vulnerable plaque has never been of vulnerable plaque has never been prospectively assessedprospectively assessed
The The PROSPECTPROSPECT TrialTrial
BackgroundBackground

0
5
10
15
20
25
30
0 3 6 9 12 15 18 21 24 27 30
Months of Follow-up
PROVE-IT TIMI-22PROVE-IT TIMI-224,162 Randomized Pts with ACS4,162 Randomized Pts with ACS
16% RR16% RR
P = 0.005P = 0.005
Pravastatin 40 mg/dPravastatin 40 mg/d
Atorvastatin 80 mg/dAtorvastatin 80 mg/d
26.3%26.3%
22.4%22.4%
Dea
th, M
I, U
A r
equ
irin
g h
osp
, D
eath
, MI,
UA
req
uir
ing
ho
sp,
reva
sc >
30d
, or
stro
ke (
%)
reva
sc >
30d
, or
stro
ke (
%)
Cannon CP et al. NEJM 2004;350:1495-1504Cannon CP et al. NEJM 2004;350:1495-1504
How many events were attributable to: 1) Restenosis, stent thrombosis, etc. vs. 2) Significant disease left behind, vs. 3) VP with rapid lesion progression?
How many events were attributable to: 1) Restenosis, stent thrombosis, etc. vs. 2) Significant disease left behind, vs. 3) VP with rapid lesion progression?
ACSACSmedian 7dmedian 7dPCI 69%PCI 69%

• We therefore performed a prospective, We therefore performed a prospective,
multicenter natural history study using 3 vessel multicenter natural history study using 3 vessel
multimodality intracoronary imaging to quantify multimodality intracoronary imaging to quantify
the clinical event rate due to atherosclerotic the clinical event rate due to atherosclerotic
progression and to identify those lesions which progression and to identify those lesions which
place pts at risk for unexpected adverse place pts at risk for unexpected adverse
cardiovascular eventscardiovascular events
• We therefore performed a prospective, We therefore performed a prospective,
multicenter natural history study using 3 vessel multicenter natural history study using 3 vessel
multimodality intracoronary imaging to quantify multimodality intracoronary imaging to quantify
the clinical event rate due to atherosclerotic the clinical event rate due to atherosclerotic
progression and to identify those lesions which progression and to identify those lesions which
place pts at risk for unexpected adverse place pts at risk for unexpected adverse
cardiovascular eventscardiovascular events
The The PROSPECTPROSPECT TrialTrial
BackgroundBackground

700 pts with ACS700 pts with ACSUA (with ECGUA (with ECGΔΔ) ) oror NSTEMI NSTEMI oror STEMI >24º STEMI >24º
undergoing PCI of 1 or 2 major coronary arteriesundergoing PCI of 1 or 2 major coronary arteries
at up to 40 sites in the U.S. and Europeat up to 40 sites in the U.S. and Europe
PCI of culprit lesion(s)PCI of culprit lesion(s)Successful and uncomplicatedSuccessful and uncomplicated
Formally enrolledFormally enrolled
Metabolic S.Metabolic S.• Waist circumWaist circum• Fast lipidsFast lipids• Fast gluFast glu• HgbA1CHgbA1C• Fast insulinFast insulin• CreatinineCreatinine
BiomarkersBiomarkers• Hs CRPHs CRP• IL-6IL-6• sCD40LsCD40L• MPOMPO• TNFTNFαα• MMP9MMP9• Lp-PLA2Lp-PLA2• othersothers
PI: Gregg W. StonePI: Gregg W. StoneSponsor: Abbott Vascular; Partner: VolcanoSponsor: Abbott Vascular; Partner: Volcano
The The PROSPECTPROSPECT TrialTrial

3-vessel imaging post PCI3-vessel imaging post PCICulprit artery, followed byCulprit artery, followed by
non-culprit arteriesnon-culprit arteries
Angiography (QCA of entire coronary tree)Angiography (QCA of entire coronary tree)
IVUSIVUS
Virtual histologyVirtual histology
Palpography (n=~350)Palpography (n=~350)
Repeat imagingRepeat imagingin pts with events in pts with events
Meds recMeds recAspirinAspirinPlavix 1yrPlavix 1yrStatinStatinRepeat biomarkersRepeat biomarkers@ 30 days, 6 months @ 30 days, 6 months
Proximal 6-8 Proximal 6-8 cm of each cm of each coronary coronary
arteryartery
Proximal 6-8 Proximal 6-8 cm of each cm of each coronary coronary
arteryartery
MSCTMSCTSubstudySubstudyN=50-100N=50-100 F/U: 1 mo, 6 mo,F/U: 1 mo, 6 mo,
1 yr, 2 yr,1 yr, 2 yr,±3-5 yrs±3-5 yrs
F/U: 1 mo, 6 mo,F/U: 1 mo, 6 mo,1 yr, 2 yr,1 yr, 2 yr,±3-5 yrs±3-5 yrs
The The PROSPECTPROSPECT TrialTrial

PROSPECT: PROSPECT: Primary EndpointPrimary Endpoint
MACE attributable to rapid angiographic MACE attributable to rapid angiographic progression of a progression of a non-culpritnon-culprit lesion*lesion*
•Cardiac deathCardiac death
•Cardiac arrestCardiac arrest
•Myocardial infarctionMyocardial infarction
•Unstable anginaUnstable angina
- Requiring revascularization- Requiring revascularization
- Requiring rehospitalization- Requiring rehospitalization
•Increasing anginaIncreasing angina
- Requiring revascularization- Requiring revascularization
- Requiring rehospitalization- Requiring rehospitalization
MACE attributable to rapid angiographic MACE attributable to rapid angiographic progression of a progression of a non-culpritnon-culprit lesion*lesion*
•Cardiac deathCardiac death
•Cardiac arrestCardiac arrest
•Myocardial infarctionMyocardial infarction
•Unstable anginaUnstable angina
- Requiring revascularization- Requiring revascularization
- Requiring rehospitalization- Requiring rehospitalization
•Increasing anginaIncreasing angina
- Requiring revascularization- Requiring revascularization
- Requiring rehospitalization- Requiring rehospitalizationMACE during FU were adjudicated by the CEC as attributable to culprit lesions (those treated during or before MACE during FU were adjudicated by the CEC as attributable to culprit lesions (those treated during or before the index hospitalization) or non culprit lesions (untreated areas of the coronary tree) based on angiography the index hospitalization) or non culprit lesions (untreated areas of the coronary tree) based on angiography (+ECGs, etc.) at the time of the event; events occurring in pts without angiographic follow-up were considered (+ECGs, etc.) at the time of the event; events occurring in pts without angiographic follow-up were considered indeterminate in origin. Rapid lesion progression = ↑ in QCA DS by >20% from baseline to FU.indeterminate in origin. Rapid lesion progression = ↑ in QCA DS by >20% from baseline to FU.
Hie
rarc
hic
alH
iera
rch
ical
Most severeMost severe
Least severeLeast severe

PROSPECT:PROSPECT: Methodology Methodology
Angiographic Core Lab AnalysisAngiographic Core Lab Analysis
• Performed on every coronary artery (main vessel and Performed on every coronary artery (main vessel and branch) visually branch) visually ≥≥1.5 mm in diameter1.5 mm in diameter
Detailed qualitative and quantitative parameters Detailed qualitative and quantitative parameters recorded for every 1.5 mm length segmentrecorded for every 1.5 mm length segment
Distance from ostia and at major branch points were Distance from ostia and at major branch points were registered and corrected for foreshortening after IVUS registered and corrected for foreshortening after IVUS co-registrationco-registration
Lesions with DS Lesions with DS ≥≥30% by 30% by visualvisual assessment identified assessment identified
Output available as lesions, CASS segments, and Output available as lesions, CASS segments, and vessels, by every mm, or any other parametervessels, by every mm, or any other parameter
• Performed on every coronary artery (main vessel and Performed on every coronary artery (main vessel and branch) visually branch) visually ≥≥1.5 mm in diameter1.5 mm in diameter
Detailed qualitative and quantitative parameters Detailed qualitative and quantitative parameters recorded for every 1.5 mm length segmentrecorded for every 1.5 mm length segment
Distance from ostia and at major branch points were Distance from ostia and at major branch points were registered and corrected for foreshortening after IVUS registered and corrected for foreshortening after IVUS co-registrationco-registration
Lesions with DS Lesions with DS ≥≥30% by 30% by visualvisual assessment identified assessment identified
Output available as lesions, CASS segments, and Output available as lesions, CASS segments, and vessels, by every mm, or any other parametervessels, by every mm, or any other parameter

• Gray-scale IVUS volumetric and cross-sectional analysis Gray-scale IVUS volumetric and cross-sectional analysis performedperformed
Each IVUS/VH frame co-registered to corresponding Each IVUS/VH frame co-registered to corresponding QCA location using fiduciary branch pointsQCA location using fiduciary branch points
IVUS lesions (IVUS lesions (≥3 consecutive frames with ≥3 consecutive frames with cross cross sectional plaque burden >40%) were characterizedsectional plaque burden >40%) were characterized
• IVUS-VH analysis performed using the latest classification IVUS-VH analysis performed using the latest classification tree (pcVH 2.1)tree (pcVH 2.1)
Plaque characterized as fibrotic, fibrofatty, necrotic core Plaque characterized as fibrotic, fibrofatty, necrotic core or dense calcium, and reported as absolute and relative or dense calcium, and reported as absolute and relative area/volumesarea/volumes
• Gray-scale IVUS volumetric and cross-sectional analysis Gray-scale IVUS volumetric and cross-sectional analysis performedperformed
Each IVUS/VH frame co-registered to corresponding Each IVUS/VH frame co-registered to corresponding QCA location using fiduciary branch pointsQCA location using fiduciary branch points
IVUS lesions (IVUS lesions (≥3 consecutive frames with ≥3 consecutive frames with cross cross sectional plaque burden >40%) were characterizedsectional plaque burden >40%) were characterized
• IVUS-VH analysis performed using the latest classification IVUS-VH analysis performed using the latest classification tree (pcVH 2.1)tree (pcVH 2.1)
Plaque characterized as fibrotic, fibrofatty, necrotic core Plaque characterized as fibrotic, fibrofatty, necrotic core or dense calcium, and reported as absolute and relative or dense calcium, and reported as absolute and relative area/volumesarea/volumes
PROSPECT:PROSPECT: Methodology Methodology
IVUS/VH Core Lab AnalysisIVUS/VH Core Lab Analysis

Lesions are classified into 5 main typesLesions are classified into 5 main types
1.1. Fibrotic Fibrotic
2.2. Fibrocalcific Fibrocalcific
3.3. Pathological intimal thickening (PIT)Pathological intimal thickening (PIT)
4.4. Thick cap fibroatheroma (ThCFA) Thick cap fibroatheroma (ThCFA)
5. 5. VH-thin cap fibroatheroma (VH-TCFA)VH-thin cap fibroatheroma (VH-TCFA)(presumed high risk)(presumed high risk)
PROSPECT:PROSPECT: Methodology Methodology
Virtual histology lesion classificationVirtual histology lesion classification

Index 2/13/06Index 2/13/06 Event 2/6/07Event 2/6/07
QCA PLCX DS 28.6%QCA PLCX DS 28.6% QCA PLCX DS 71.3%QCA PLCX DS 71.3%
PROSPECT 82910-012: PROSPECT 82910-012: 52 yo♂52 yo♂
2/13/06: 2/13/06: NSTEMI, PCI of MLADNSTEMI, PCI of MLAD
2/6/07 (51 weeks later): 2/6/07 (51 weeks later): NSTEMI attributed to LCXNSTEMI attributed to LCX

38
1. ThCFA1. ThCFA
*OM
5.3mm2
LesionLesion
*
1
prox
PROSPECT 82910-012: PROSPECT 82910-012: Index 2/13/06Index 2/13/06
Baseline PLCXBaseline PLCXQCA: RVD 2.82 mm, QCA: RVD 2.82 mm, DS 28.6%, length 6.8 DS 28.6%, length 6.8
mmmmIVUS: MLA 5.3 mmIVUS: MLA 5.3 mm22
VH: ThCFAVH: ThCFA

PROSPECT: PROSPECT: Event CategoriesEvent Categories
CEC adjudicated MACE during follow-upCEC adjudicated MACE during follow-up
• • Culprit lesion (stent) relatedCulprit lesion (stent) related
- Stent thrombosis- Stent thrombosis
- Restenosis- Restenosis
- New side branch lesion- New side branch lesion
• • Non culprit lesion relatedNon culprit lesion related
- With rapid lesion progression (by QCA) - With rapid lesion progression (by QCA) (classic “vulnerable plaque”)(classic “vulnerable plaque”)
- Without rapid lesion progression- Without rapid lesion progression
• • IndeterminateIndeterminate

• PI:PI: Gregg W. Stone; Gregg W. Stone; Co-PI:Co-PI: Patrick W. Serruys Patrick W. Serruys
European Co-PI:European Co-PI: Bernard de Bruyne Bernard de Bruyne
• Data management: Data management: Abbott Vascular; Zhen Zhang (lead statistician)Abbott Vascular; Zhen Zhang (lead statistician)
• Clinical events committee:Clinical events committee: CRF, Roxana Mehran (Chair), George Dangas CRF, Roxana Mehran (Chair), George Dangas
• Core laboratoriesCore laboratories
QCA: QCA: CRF, Alexandra Lansky (Director), Ecaterina CristeaCRF, Alexandra Lansky (Director), Ecaterina Cristea
IVUS, Virtual Histology: IVUS, Virtual Histology: CRF, Akiko Maehara (Director), Gary S. MintzCRF, Akiko Maehara (Director), Gary S. Mintz
Palpography: Palpography: Cardialysis, Marie-Angèle Morel Cardialysis, Marie-Angèle Morel
MSCT: MSCT: Thoraxcenter, Pim de Feyter (Director)Thoraxcenter, Pim de Feyter (Director)
Biomarkers: Biomarkers: CRL MedinetCRL Medinet
• DSMB:DSMB: Steve Steinhubl (Chair) Steve Steinhubl (Chair)
• Sponsor and Partner:Sponsor and Partner: Abbott Vascular and Volcano Corp. Abbott Vascular and Volcano Corp.
• Abbott Vascular Program Leads:Abbott Vascular Program Leads: Barry Templin and Wai-Fung Cheong Barry Templin and Wai-Fung Cheong
PROSPECT:PROSPECT: OrganizationOrganization

700 pts enrolled between Oct. 2004 and June 2006 700 pts enrolled between Oct. 2004 and June 2006 and followed for at least 3 yearsand followed for at least 3 years
Europe: Europe: 403 pts 403 pts enrolled at 18 sitesenrolled at 18 sites
U.S.: U.S.: 297 pts 297 pts enrolled at 19 sitesenrolled at 19 sites
66 pts66 pts Rotterdam (Serruys)Rotterdam (Serruys)
64 pts64 pts St. Thomas (McPherson)St. Thomas (McPherson)
54 pts54 pts Aalst (de Bruyne)Aalst (de Bruyne)
44 pts44 pts Elyria Memorial Hosp (Farhat)Elyria Memorial Hosp (Farhat)
40 pts40 pts St. Luke’s Hosp (Marso)St. Luke’s Hosp (Marso)
38 pts38 pts Gothenburg (Wennerblom)Gothenburg (Wennerblom)
32 pts32 pts Vigo (Iniguez)Vigo (Iniguez)
31 pts31 pts Toulouse (Fajadet)Toulouse (Fajadet)
30 pts30 pts South Carolina Heart (Foster)South Carolina Heart (Foster)
28 pts28 pts Antwerp (Verheye)Antwerp (Verheye)
To
p 1
0 en
rolle
rsT
op
10
enro
llers
PROSPECT:PROSPECT: EnrollmentEnrollment

PROSPECT:PROSPECT: Baseline Features Baseline Features
N = 697*N = 697*
*3 patients who were never consented were de-registered*3 patients who were never consented were de-registered

Age (yrs, median)Age (yrs, median) 58 [50, 66]58 [50, 66]
Gender (female)Gender (female) 24.0%24.0%
Diabetes mellitusDiabetes mellitus 16.9%16.9%
- Insulin requiring- Insulin requiring 3.0%3.0%
Current cigarette useCurrent cigarette use 47.1%47.1%
HypertensionHypertension 45.8%45.8%
HyperlipidemiaHyperlipidemia 40.0%40.0%
Prior MIPrior MI 10.5%10.5%
Single / double / triple vessel diseaseSingle / double / triple vessel disease 20% / 41% / 39%20% / 41% / 39%
Total arteries with vs. without PCITotal arteries with vs. without PCI 892, 1199892, 1199
PCI performed in 1 or 2 arteriesPCI performed in 1 or 2 arteries 72% / 28%72% / 28%
PCI of LAD / LCX / RCA (per artery)PCI of LAD / LCX / RCA (per artery) 41% / 27% / 32%41% / 27% / 32%
Median [IQR] follow-up (years)Median [IQR] follow-up (years) 3.4 [1.9, 3.9]3.4 [1.9, 3.9]
PROSPECT:PROSPECT: Baseline Features Baseline Features
N = 697N = 697

PROSPECT:PROSPECT: Imaging Summary Imaging Summary
Length of coronary arteries analyzed (core lab)Length of coronary arteries analyzed (core lab)
Mean (mm)Mean (mm)AngiographyAngiography
(N=697)(N=697)IVUS and VHIVUS and VH
(N=615)(N=615)
LMLM 9.3 ± 4.39.3 ± 4.3 9.0 ± 6.39.0 ± 6.3
LADLAD 155.7 ± 41.0155.7 ± 41.0 72.6 ± 33.272.6 ± 33.2
LCXLCX 135.4 ± 49.9135.4 ± 49.9 61.7 ± 35.961.7 ± 35.9
RCARCA 149.9 ± 44.7149.9 ± 44.7 81.6 ± 38.081.6 ± 38.0
Total per ptTotal per pt 446.2 ± 84.0446.2 ± 84.0 193.3 ± 81.6193.3 ± 81.6
Total all ptsTotal all pts 311,016311,016 118,670118,670

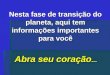
Virtual histologyVirtual histology(N=2689 lesions in 615 pts)(N=2689 lesions in 615 pts)
- Mean plaque composition-- Mean plaque composition-
Plaque subtypePlaque subtype N=2689N=2689
FibroticFibrotic 2.5%2.5%
FibrocalcificFibrocalcific 1.1%1.1%
PITPIT 35.9%35.9%
FibroatheromaFibroatheroma 59.9%59.9%
- Thick cap- Thick cap 37.8%37.8%
- VH-TCFA- VH-TCFA 22.1%22.1%
- Single, - Ca- Single, - Ca 5.4%5.4%
- Single, + Ca- Single, + Ca 0.5%0.5%
- Multiple, - Ca- Multiple, - Ca 9.8%9.8%
- Multiple, + Ca- Multiple, + Ca 6.4%6.4%
UnclassifiedUnclassified 0.7%0.7%
6.5%
59.4%
21.1%
13.0%
Dense calcium Fibrotic
Fibrofatty Necrotic core
PROSPECT:PROSPECT: Imaging Summary Imaging Summary

PROSPECT: PROSPECT: MACEMACEM
AC
E (
%)
MA
CE
(%
)
Time in YearsTime in Years00 11 22 33
All All Culprit lesion (CL) relatedCulprit lesion (CL) relatedNon culprit lesion (NCL) relatedNon culprit lesion (NCL) relatedIndeterminateIndeterminate
00
55
1010
1515
2020
2525
Number at riskNumber at risk
ALLALL 697697 557 557 506 506 480480
CL relatedCL related 697697 590590 543543 518518
NCL relatedNCL related 697697 595595 553 553 521521
IndeterminateIndeterminate 697697 634634 604 604 583583
12.9%12.9%
20.4%20.4%
11.6%11.6%
2.7%2.7%

PROSPECT: PROSPECT: MACEMACEM
AC
E (
%)
MA
CE
(%
)
Time in YearsTime in Years00 11 22 33
All All Culprit lesion (CL) relatedCulprit lesion (CL) relatedNon culprit lesion (NCL) relatedNon culprit lesion (NCL) relatedIndeterminateIndeterminate
00
55
1010
1515
2020
2525
Number at riskNumber at risk
20.4%20.4%
12.9%12.9%
11.6%11.6%
2.7%2.7%
13.2%13.2%
7.9%7.9%
6.4%6.4%
0.9%0.9%
18.1%18.1%
11.4%11.4%
9.4%9.4%
1.9%1.9%
ALLALL 697697 557 557 506 506 480480
CL relatedCL related 697697 590590 543543 518518
NCL relatedNCL related 697697 595595 553 553 521521
IndeterminateIndeterminate 697697 634634 604 604 583583

PROSPECT:PROSPECT: MACE MACE
3-year follow-up, non hierarchical3-year follow-up, non hierarchical
AllAll Culprit Culprit lesion relatedlesion related
Non culprit Non culprit lesion relatedlesion related
Indeter-Indeter-minateminate
Cardiac deathCardiac death 1.9% (12)1.9% (12) 0.2% (1)0.2% (1) 0% (0)0% (0) 1.8% (11)1.8% (11)
Cardiac arrestCardiac arrest 0.5% (3)0.5% (3) 0.3% (2)0.3% (2) 0% (0)0% (0) 0.2% (1)0.2% (1)
MI (STEMI or NSTEMI)MI (STEMI or NSTEMI) 3.3% (21)3.3% (21) 2.0% (13)2.0% (13) 1.0% (6)1.0% (6) 0.3% (2)0.3% (2)
Unstable anginaUnstable angina 8.0% (51)8.0% (51) 4.5% (29)4.5% (29) 3.3% (21)3.3% (21) 0.5% (3)0.5% (3)
Increasing anginaIncreasing angina 14.5% (93)14.5% (93) 9.2% (59)9.2% (59) 8.5% (54)8.5% (54) 0.3% (2)0.3% (2)
Composite MACEComposite MACE 20.4% (132)20.4% (132) 12.9% (83)12.9% (83) 11.6% (74)11.6% (74) 2.7% (17)2.7% (17)
Cardiac death, arrest or MICardiac death, arrest or MI 4.9% (31)4.9% (31) 2.2% (14)2.2% (14) 1.0% (6)1.0% (6) 1.9% (12)1.9% (12)
Rates are 3-yr Kaplan-Meier estimates (n of events)Rates are 3-yr Kaplan-Meier estimates (n of events)

PROSPECT:PROSPECT: MACE MACE
Sensitivity analysis*: Sensitivity analysis*: 3-year FU, non hierarchical3-year FU, non hierarchical
AllAll Culprit Culprit lesion relatedlesion related
Non culprit Non culprit lesion related*lesion related*
Cardiac deathCardiac death 1.9% (12)1.9% (12) 0.2% (1)0.2% (1) 1.8% (11)1.8% (11)
Cardiac arrestCardiac arrest 0.5% (3)0.5% (3) 0.3% (2)0.3% (2) 0.2% (1)0.2% (1)
MI (STEMI or NSTEMI)MI (STEMI or NSTEMI) 3.3% (21)3.3% (21) 2.0% (13)2.0% (13) 1.3% (8)1.3% (8)
Unstable anginaUnstable angina 8.0% (51)8.0% (51) 4.5% (29)4.5% (29) 3.8% (24)3.8% (24)
Increasing anginaIncreasing angina 14.5% (93)14.5% (93) 9.2% (59)9.2% (59) 8.8% (56)8.8% (56)
Composite MACEComposite MACE 20.4% (132)20.4% (132) 12.9% (83)12.9% (83) 13.3% (85)13.3% (85)
Cardiac death, arrest or MICardiac death, arrest or MI 4.9% (31)4.9% (31) 2.2% (14)2.2% (14) 2.9% (18)2.9% (18)
Rates are 3-yr Kaplan-Meier estimates (n of events)Rates are 3-yr Kaplan-Meier estimates (n of events) *Assuming all indeterminate events are non culprit related*Assuming all indeterminate events are non culprit related

MA
CE
(%
)M
AC
E (
%)
Time in YearsTime in Years00 11 22 33
NCL related, allNCL related, all 697697 595595 553 553 521 521
- without RLP- without RLP 697697 610610 577 577 551 551
- with RLP- with RLP 697697 620620 579 579 550 550
Number at riskNumber at risk
Non-culprit lesion (NCL) related, allNon-culprit lesion (NCL) related, all - Without rapid lesion progression (RLP)- Without rapid lesion progression (RLP) - With rapid lesion progression (RLP)- With rapid lesion progression (RLP)
PROSPECT: PROSPECT: NCL NCL MACEMACE
00
22
44
66
88
1010
1212 11.6%11.6%
6.7%6.7%
6.4%6.4%

MA
CE
(%
)M
AC
E (
%)
Time in YearsTime in Years00 11 22 33
Number at riskNumber at risk
Non-culprit lesion (NCL) related, allNon-culprit lesion (NCL) related, all - Without rapid lesion progression (RLP)- Without rapid lesion progression (RLP) - With rapid lesion progression (RLP)- With rapid lesion progression (RLP)
00
22
44
66
88
1010
1212 11.6%11.6%
6.7%6.7%
6.4%6.4%
2.9%2.9%
4.1%4.1%
6.4%6.4%
5.5%5.5%
4.9%4.9%
9.4%9.4%
NCL related, allNCL related, all 697697 595595 553 553 521 521
- without RLP- without RLP 697697 610610 577 577 551 551
- with RLP- with RLP 697697 620620 579 579 550 550
PROSPECT: PROSPECT: NCL NCL MACEMACE
Median time to eventNo RLP: No RLP: 223 [85, 663] days223 [85, 663] daysRLP: RLP: 401 [229, 666]401 [229, 666] days

PROSPECT:PROSPECT: Correlates of Correlates of Non Culprit Related Events Non Culprit Related Events
Baseline variables examined (n=152)Baseline variables examined (n=152)
Demographic, history and PE (n=19)Demographic, history and PE (n=19)
Labs (n=7; including CrCl, lipids, hgbA1C, CRP)Labs (n=7; including CrCl, lipids, hgbA1C, CRP)
Angio non core lab (n=1; visible lesions >30% DS) Angio non core lab (n=1; visible lesions >30% DS)
QCA measures (n=12)QCA measures (n=12)
IVUS area and volumetric measures (n=22)IVUS area and volumetric measures (n=22)
Virtual histology measures (n=74)Virtual histology measures (n=74)
Treatment related (n=1; # vessels stented)Treatment related (n=1; # vessels stented)
Medications in-hosp. and at discharge (n=16)Medications in-hosp. and at discharge (n=16)

PROSPECT:PROSPECT: Correlates of Correlates of Non Culprit Lesion Related EventsNon Culprit Lesion Related Events
Patient level events at median 3.4 yrsPatient level events at median 3.4 yrs (76 events in 689 pts*) (76 events in 689 pts*)
Baseline Demographic and Angiographic VariablesBaseline Demographic and Angiographic Variables
VariableVariable KM Rate (n)KM Rate (n) HR [95% CI]HR [95% CI] HR [95% CI]HR [95% CI] PP
Insulin DM (n=21)Insulin DM (n=21) 41.4% (6)41.4% (6) 4.07 [1.75, 9.46]4.07 [1.75, 9.46] 0.0010.001Non insulin DM (n=96)Non insulin DM (n=96) 16.3% (14)16.3% (14) 1.55 [0.86, 2.79] 0.14Non diabetic (n=569)Non diabetic (n=569) 10.7% (56)10.7% (56)
Hypertension (n=314)Hypertension (n=314) 14.7% (42)14.7% (42) 1.64 [1.03, 2.60]1.64 [1.03, 2.60] 0.040.04No hypertension (n=369)No hypertension (n=369) 9.1% (31)9.1% (31)
Prior PCI (n=75)Prior PCI (n=75) 23.1% (15)23.1% (15) 2.20 [1.25, 3.86]2.20 [1.25, 3.86] 0.0060.006No prior PCI (n=613)No prior PCI (n=613) 10.8% (61)10.8% (61)
≥≥1 visible angio lsn* (n=582)1 visible angio lsn* (n=582) 13.7% (73)13.7% (73) 4.72 [1.49, 14.98]4.72 [1.49, 14.98] 0.0080.008No visible angio lsn (n=107)No visible angio lsn (n=107) 3.2% (3)3.2% (3)
*Visually assessed DS >30%*Visually assessed DS >30%
01 5 10 15
Univariate, unadjusted. * 8 patients with indeterminate events were excluded.Univariate, unadjusted. * 8 patients with indeterminate events were excluded.

VariableVariable Rate (n)Rate (n) HR [95% CI]HR [95% CI] HR [95% CI]HR [95% CI] PP
MLA < median 5.9 mmMLA < median 5.9 mm22 (n=1336) (n=1336) 3.4% (45)3.4% (45) 7.53 [3.21, 17.65]]<0.0001<0.0001MLA ≥ median 5.9 mmMLA ≥ median 5.9 mm2 2 (n=1337)(n=1337) 0.4% (6)0.4% (6)
MLA ≤ 4.0 mmMLA ≤ 4.0 mm22 (n=496) (n=496) 5.4% (27)5.4% (27) 5.01 [2.89, 8.68]] <0.0001<0.0001MLA > 4.0 mmMLA > 4.0 mm2 2 (n=2177) (n=2177) 1.1% (24)1.1% (24)
PBPBMLAMLA ≥ median 0.55 (n=1337) ≥ median 0.55 (n=1337) 3.3% (44)3.3% (44) 66.37 [2.87, 14.15]]
<0.0001<0.0001PBPBMLAMLA < median 0.55 (n=1336) < median 0.55 (n=1336) 0.5% (7)0.5% (7)
PBPBMLAMLA ≥ 0.70 (n=242) ≥ 0.70 (n=242) 9.1% (22)9.1% (22) 7.94 [4.56, 13.81]
<0.0001<0.0001PBPBMLAMLA < 0.70 (n=2431) < 0.70 (n=2431) 1.2% (29)1.2% (29)
EEMEEMMLAMLA ≥ med 14.3 mm ≥ med 14.3 mm22 (n=1337) (n=1337) 1.4% (19)1.4% (19) 0.60 [0.34, 1.06]0.60 [0.34, 1.06] 0.080.08
EEMEEMMLAMLA < med 14.3 mm < med 14.3 mm22 (n=1336) (n=1336) 2.4% (32)2.4% (32)
Lsn length < med 11.6 mm (n=1336) Lsn length < med 11.6 mm (n=1336) 0.7% (10)0.7% (10) 4.01 [2.01, 8.02]] <0.0001<0.0001Lsn length ≥ med 11.6 mm (n=1337) Lsn length ≥ med 11.6 mm (n=1337) 3.1% (41)3.1% (41)
PROSPECT:PROSPECT: Correlates of Correlates of Non Culprit Lesion Related EventsNon Culprit Lesion Related Events
Lesion level eventsLesion level events (51 events from 2673 lesions in 609 pts at median 3.4 yrs)(51 events from 2673 lesions in 609 pts at median 3.4 yrs)
IVUS Characteristics (area data)IVUS Characteristics (area data)
MLA = minimal luminal area; PBMLA = minimal luminal area; PBMLAMLA = plaque burden at the MLA; EEM = plaque burden at the MLA; EEMMLAMLA = external elastic membrane at the MLA. = external elastic membrane at the MLA.
Data represent univariate associations, unadjusted. Data represent univariate associations, unadjusted.
01 5 10 15

VariableVariable Rate (n)Rate (n) HR [95% CI]HR [95% CI] HR [95% CI]HR [95% CI] PP
VH-TCFA (n=590)VH-TCFA (n=590) 4.4% (26)4.4% (26) 33.84 [2.22, 6.65]]<0.0001<0.0001
Not VH-TCFA (n=2065)Not VH-TCFA (n=2065) 1.2% (25)1.2% (25)
ThCFA (n=1005)ThCFA (n=1005) 1.8% (18)1.8% (18) 0.89 [0.50, 1.58]] 0.690.69Not ThCFA (n=1650)Not ThCFA (n=1650) 2.0% (33)2.0% (33)
PIT (n=964)PIT (n=964) 0.6% (6)0.6% (6) 0.23 [0.10, 0.53]] 0.0010.001Not PIT (n=1691)Not PIT (n=1691) 2.7% (45)2.7% (45)
Fibrotic (n=67)Fibrotic (n=67) 0% (0)0% (0) - 0.990.99Not Fibrotic (n=2588)Not Fibrotic (n=2588) 2.0% (51)2.0% (51)
Fibrocalcific (n=29)Fibrocalcific (n=29) 3.4% (1)3.4% (1) 1.75 [0.24, 12.63]] 0.580.58Not fibrocalcific (n=2626)Not fibrocalcific (n=2626) 1.9% (50)1.9% (50)
PROSPECT:PROSPECT: Correlates of Correlates of Non Culprit Lesion Related EventsNon Culprit Lesion Related Events
TCFA = thin cap fibroatheroma; ThCFA = thick cap fibroatheroma; PIT = pathologic intimal thickening. Univariate, unadjusted. TCFA = thin cap fibroatheroma; ThCFA = thick cap fibroatheroma; PIT = pathologic intimal thickening. Univariate, unadjusted.
Lesion level eventsLesion level events (51 events from 2655 lesions in 609 pts at median 3.4 yrs)(51 events from 2655 lesions in 609 pts at median 3.4 yrs)
Virtual Histology Plaque TypeVirtual Histology Plaque Type
01 5 10 15

PROSPECT:PROSPECT: Multivariable Correlates Multivariable Correlates of Non Culprit Lesion Related Eventsof Non Culprit Lesion Related Events
Independent predictors of lesion level Independent predictors of lesion level events by logistic regression analysisevents by logistic regression analysis
Variables entered into the model: Minimal luminal area (MLA); plaque burden at the MLA (PBVariables entered into the model: Minimal luminal area (MLA); plaque burden at the MLA (PBMLAMLA); );
external elastic membrane at the MLA (EEMexternal elastic membrane at the MLA (EEMMLAMLA) <median; lesion length ≥ median (mm); VH-TCFA.) <median; lesion length ≥ median (mm); VH-TCFA.
VariableVariable OR [95% CI]OR [95% CI] P valueP value
PBPBMLAMLA ≥70% ≥70% 4.99 [2.54, 9.79] <0.0001<0.0001
VH-TCFA VH-TCFA 3.00 [1.68, 5.37] 0.00020.0002
MLA ≤4.0 mmMLA ≤4.0 mm22 2.77 [1.32, 5.81] 0.0070.007
Lesion length ≥11.6 mmLesion length ≥11.6 mm 1.97 [0.94, 4.16]] 0.070.07
EEMEEMMLAMLA <14.3 mm <14.3 mm22 1.30 [0.62, 2.75]] 0.490.49

PROSPECT:PROSPECT: Correlates of Correlates of Non Culprit Lesion Related EventsNon Culprit Lesion Related Events
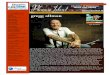
Lesion HRLesion HR 3.8 (2.2, 6.6) 5.0 (2.9, 8.7) 7.9 (4.6, 13.8) 6.4 (3.4, 12.2) 6.7 (3.4, 13.0) 10.8 (5.5, 21.0) 10.8 (4.3, 27.2)
P valueP value <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 Prevalence*Prevalence* 51.2%51.2% 49.1%49.1% 30.7%30.7% 17.4% 17.4% 15.4%15.4% 11.0%11.0% 4.6% 4.6%
*Likelihood of one or more such lesions being present per patient. PB = plaque burden at the MLA*Likelihood of one or more such lesions being present per patient. PB = plaque burden at the MLA

PROSPECT:PROSPECT: VH-TCFA and Non VH-TCFA and Non Culprit Lesion Related EventsCulprit Lesion Related Events
Lesion HRLesion HR 3.84 (2.22, 6.65) 6.41 (3.35, 12.24) 10.77 (5.53, 21.00) 10.81 (4.30, 27.22) P valueP value <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001<0.0001 Prevalence*Prevalence* 51.2%51.2% 17.4%17.4% 11.0%11.0% 4.6% 4.6%
*Likelihood of one or more such lesions being present per patient. PB = plaque burden at the MLA*Likelihood of one or more such lesions being present per patient. PB = plaque burden at the MLA

PROSPECT:PROSPECT: PIT and Non Culprit PIT and Non Culprit Lesion Related EventsLesion Related Events
Lesion HRLesion HR 0.24 (0.10, 0.56) 1.15 (0.36 3.70) 1.36 (0.19, 9.86) 2.85 (0.39, 20.67) P valueP value 0.001 0.001 0.81 0.81 0.76 0.76 0.30 0.30 Prevalence*Prevalence* 68.6%68.6% 17.2%17.2% 5.7%5.7% 2.6% 2.6%
*Likelihood of one or more such lesions being present per patient. PB = plaque burden at the MLA*Likelihood of one or more such lesions being present per patient. PB = plaque burden at the MLA

PROSPECT:PROSPECT: Conclusions Conclusions
• From this trial, the first prospective, natural history study of From this trial, the first prospective, natural history study of atherosclerosis using multimodality imaging to characterize the atherosclerosis using multimodality imaging to characterize the coronary tree, we can conclude that:coronary tree, we can conclude that:
• Approximately 20% of pts with ACS successfully treated with Approximately 20% of pts with ACS successfully treated with stents and contemporary medical Rx develop MACE within stents and contemporary medical Rx develop MACE within 3 years, with adverse events equally attributable to 3 years, with adverse events equally attributable to recurrence at originally treated culprit lesions (treatment recurrence at originally treated culprit lesions (treatment failure) and to previously untreated non culprit coronary failure) and to previously untreated non culprit coronary segmentssegments
• Approximately 12% of pts develop MACE from Approximately 12% of pts develop MACE from non culprit non culprit lesionslesions during 3 years of follow-up during 3 years of follow-up
• Patients treated with contemporary medical therapy who Patients treated with contemporary medical therapy who develop non culprit lesion events present most commonly with develop non culprit lesion events present most commonly with progressive or unstable angina, and rarely with cardiac death, progressive or unstable angina, and rarely with cardiac death, cardiac arrest or MIcardiac arrest or MI
• From this trial, the first prospective, natural history study of From this trial, the first prospective, natural history study of atherosclerosis using multimodality imaging to characterize the atherosclerosis using multimodality imaging to characterize the coronary tree, we can conclude that:coronary tree, we can conclude that:
• Approximately 20% of pts with ACS successfully treated with Approximately 20% of pts with ACS successfully treated with stents and contemporary medical Rx develop MACE within stents and contemporary medical Rx develop MACE within 3 years, with adverse events equally attributable to 3 years, with adverse events equally attributable to recurrence at originally treated culprit lesions (treatment recurrence at originally treated culprit lesions (treatment failure) and to previously untreated non culprit coronary failure) and to previously untreated non culprit coronary segmentssegments
• Approximately 12% of pts develop MACE from Approximately 12% of pts develop MACE from non culprit non culprit lesionslesions during 3 years of follow-up during 3 years of follow-up
• Patients treated with contemporary medical therapy who Patients treated with contemporary medical therapy who develop non culprit lesion events present most commonly with develop non culprit lesion events present most commonly with progressive or unstable angina, and rarely with cardiac death, progressive or unstable angina, and rarely with cardiac death, cardiac arrest or MIcardiac arrest or MI

PROSPECT:PROSPECT: Conclusions Conclusions
• While plaques which are responsible for unanticipated future MACE While plaques which are responsible for unanticipated future MACE are frequently angiographically mild, most untreated plaques which are frequently angiographically mild, most untreated plaques which become symptomatic have a large plaque burden and a small lumen become symptomatic have a large plaque burden and a small lumen area (which are detectable by IVUS but not by angiography)area (which are detectable by IVUS but not by angiography)
• Only about half of new events due to non culprit lesions exemplify the Only about half of new events due to non culprit lesions exemplify the classic notion of vulnerable plaque (rapid lesion progression of mild classic notion of vulnerable plaque (rapid lesion progression of mild angiographic lesions), while half are attributable to unrecognized and angiographic lesions), while half are attributable to unrecognized and untreated severe disease with minimal change over timeuntreated severe disease with minimal change over time
• The prospective identification of non culprit lesions prone to develop The prospective identification of non culprit lesions prone to develop MACE within 3 years can be enhanced by characterization of MACE within 3 years can be enhanced by characterization of underlying plaque morphology with virtual histology, with VH-TCFAs underlying plaque morphology with virtual histology, with VH-TCFAs representing the highest risk lesion typerepresenting the highest risk lesion type
• The combination of large plaque burden (IVUS) and a large necrotic The combination of large plaque burden (IVUS) and a large necrotic core without a visible cap (VH-TCFA) identifies lesions which are at core without a visible cap (VH-TCFA) identifies lesions which are at especially high risk for future adverse cardiovascular eventsespecially high risk for future adverse cardiovascular events
• While plaques which are responsible for unanticipated future MACE While plaques which are responsible for unanticipated future MACE are frequently angiographically mild, most untreated plaques which are frequently angiographically mild, most untreated plaques which become symptomatic have a large plaque burden and a small lumen become symptomatic have a large plaque burden and a small lumen area (which are detectable by IVUS but not by angiography)area (which are detectable by IVUS but not by angiography)
• Only about half of new events due to non culprit lesions exemplify the Only about half of new events due to non culprit lesions exemplify the classic notion of vulnerable plaque (rapid lesion progression of mild classic notion of vulnerable plaque (rapid lesion progression of mild angiographic lesions), while half are attributable to unrecognized and angiographic lesions), while half are attributable to unrecognized and untreated severe disease with minimal change over timeuntreated severe disease with minimal change over time
• The prospective identification of non culprit lesions prone to develop The prospective identification of non culprit lesions prone to develop MACE within 3 years can be enhanced by characterization of MACE within 3 years can be enhanced by characterization of underlying plaque morphology with virtual histology, with VH-TCFAs underlying plaque morphology with virtual histology, with VH-TCFAs representing the highest risk lesion typerepresenting the highest risk lesion type
• The combination of large plaque burden (IVUS) and a large necrotic The combination of large plaque burden (IVUS) and a large necrotic core without a visible cap (VH-TCFA) identifies lesions which are at core without a visible cap (VH-TCFA) identifies lesions which are at especially high risk for future adverse cardiovascular eventsespecially high risk for future adverse cardiovascular events