Embed Size (px)
Citation preview

Growth and Puberty Overview
BSME - School Nursing Course
June 2 2016
David Cremonesini
Topics
• Growth
• Short stature
• Early and late puberty
• Rickets


Familial influence
• Final adult height strongly influenced by genetics
• Mean 2.8cm difference in monozygotic twins yet mean 12cm difference in dizygotic
• 70-90% of child’s final height is genetically determined
• Malnutrition main cause of short stature in developed world
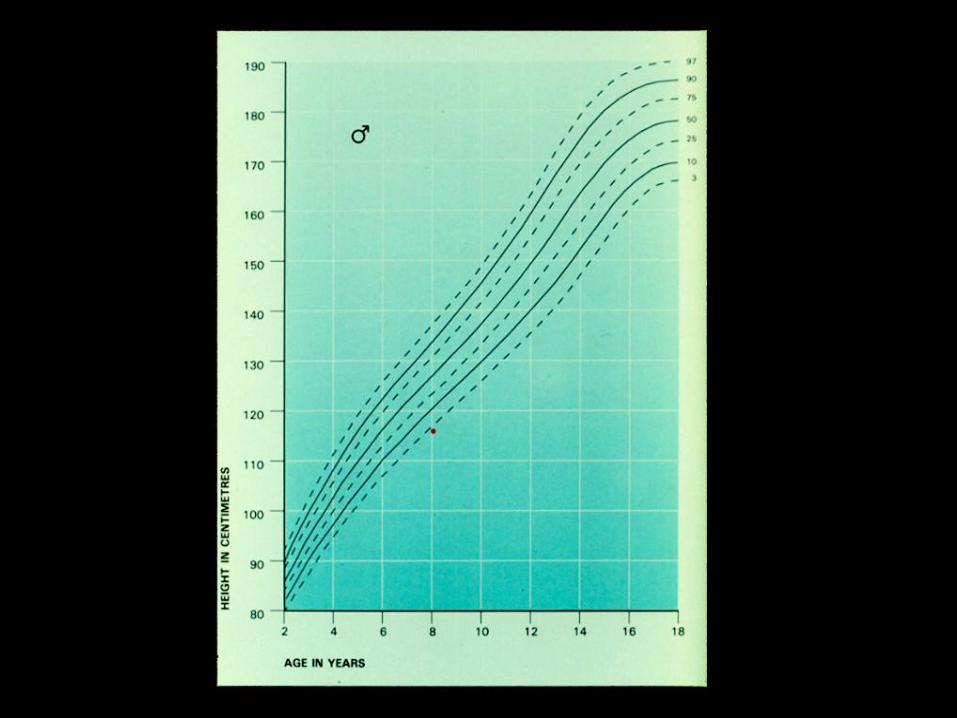
Case 1
• John is 8 years old
• He is shortest in the class
• Mother is worried something is wrong
• What might you ask/do?
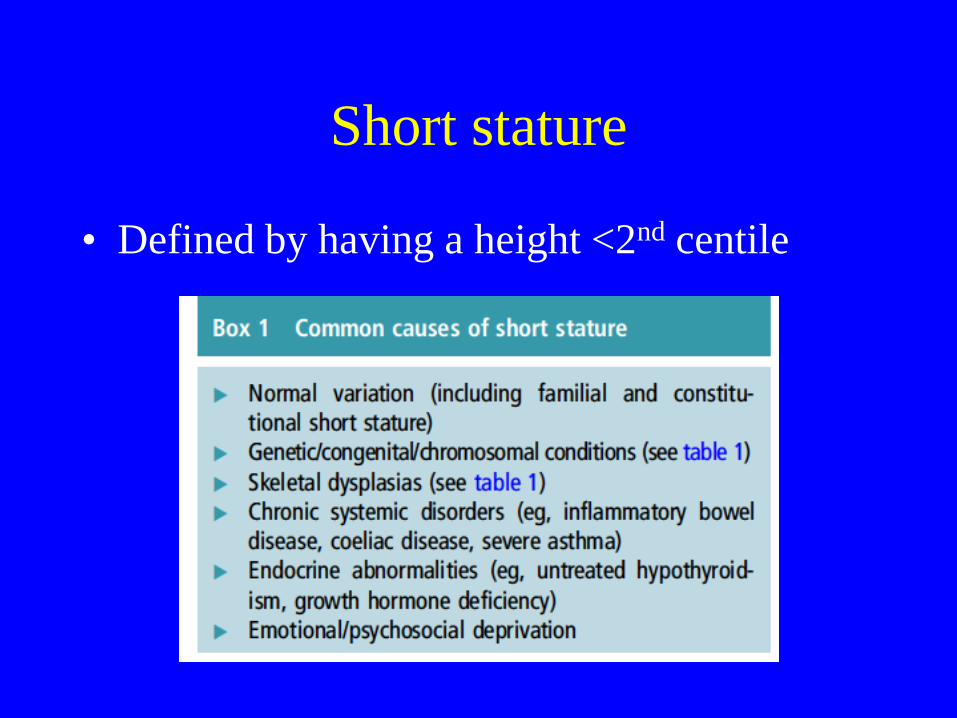
Short stature
• Defined by having a height <2nd centile
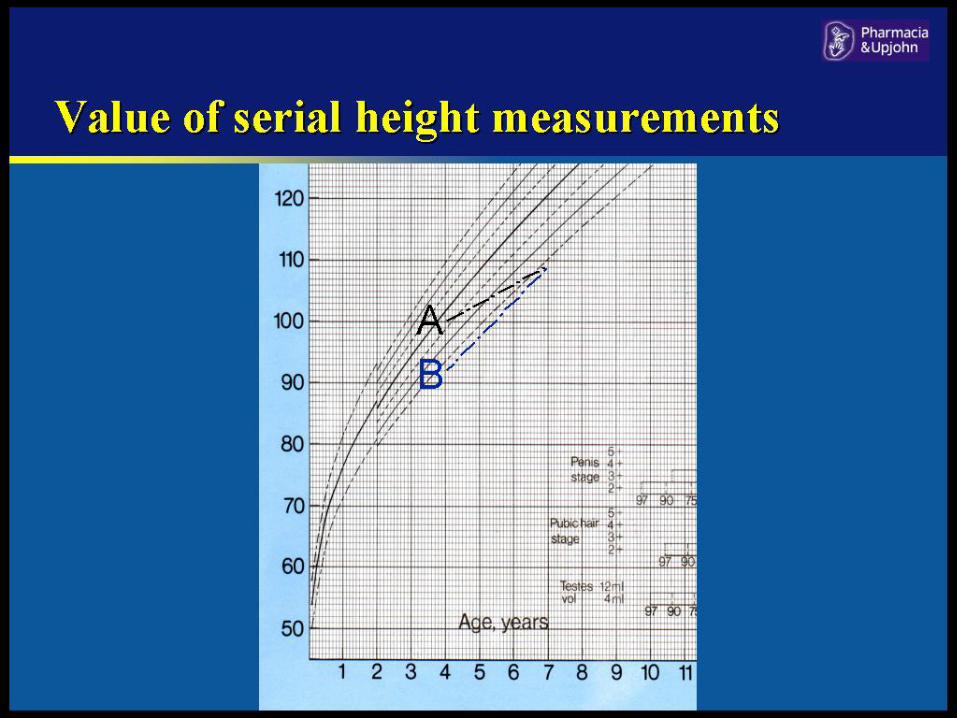
Examination
• Signs of chronic illness or genetic syndromes
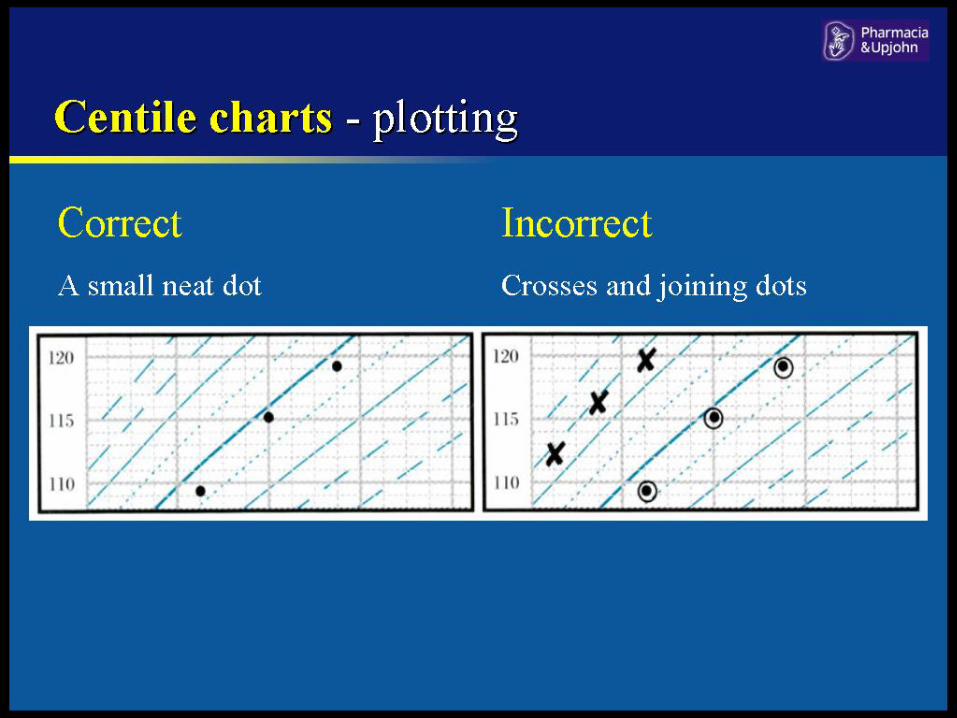
• Serial heights over time, ideally 6 mths apart
• Puberty assessment:
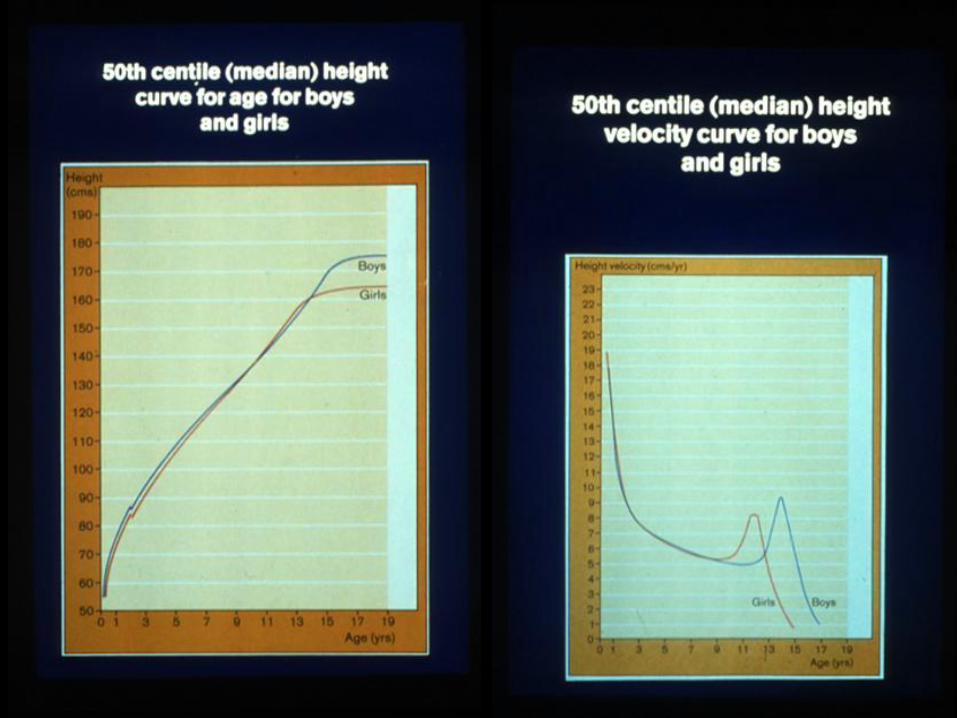
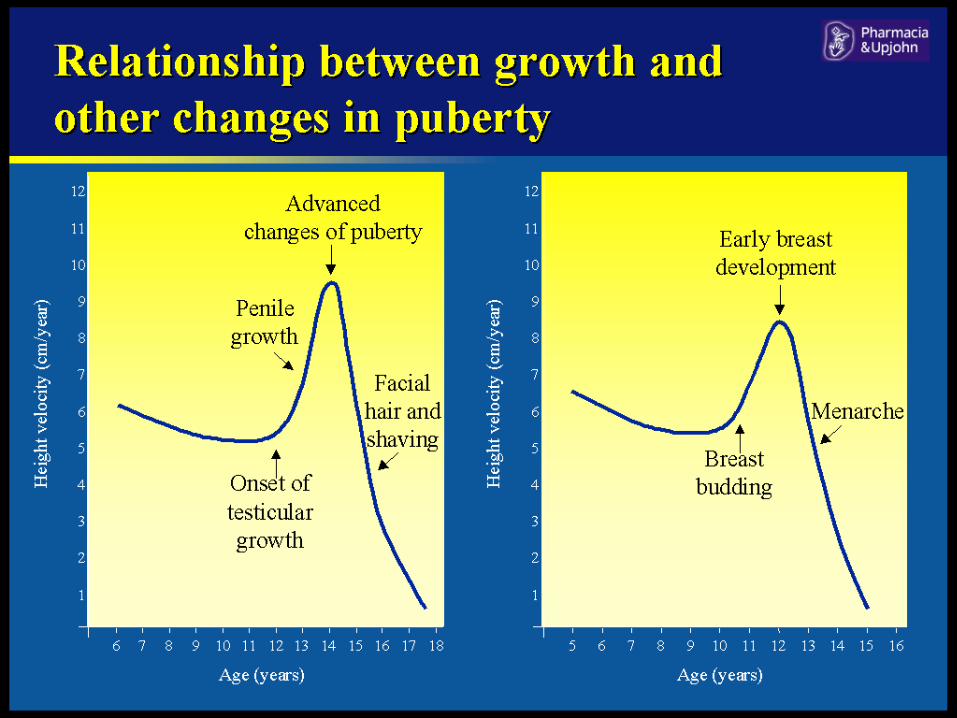
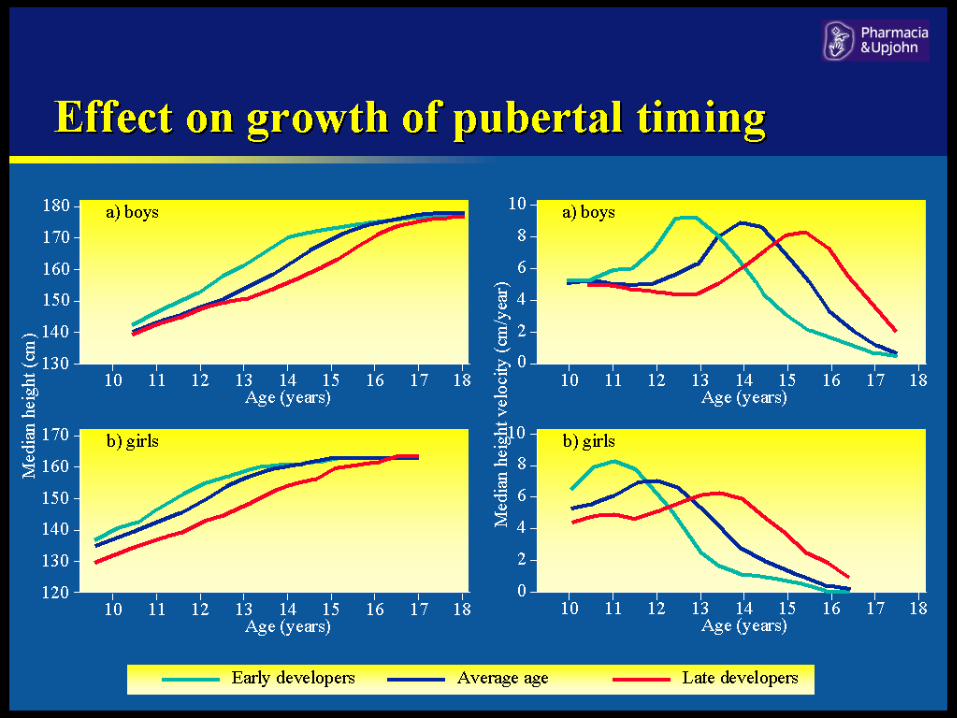
– Boys growth spurt towards end of puberty
typically around 14yrs
– Girls puberty earlier so spurt typically 12 yrs, 1
year before menstruation

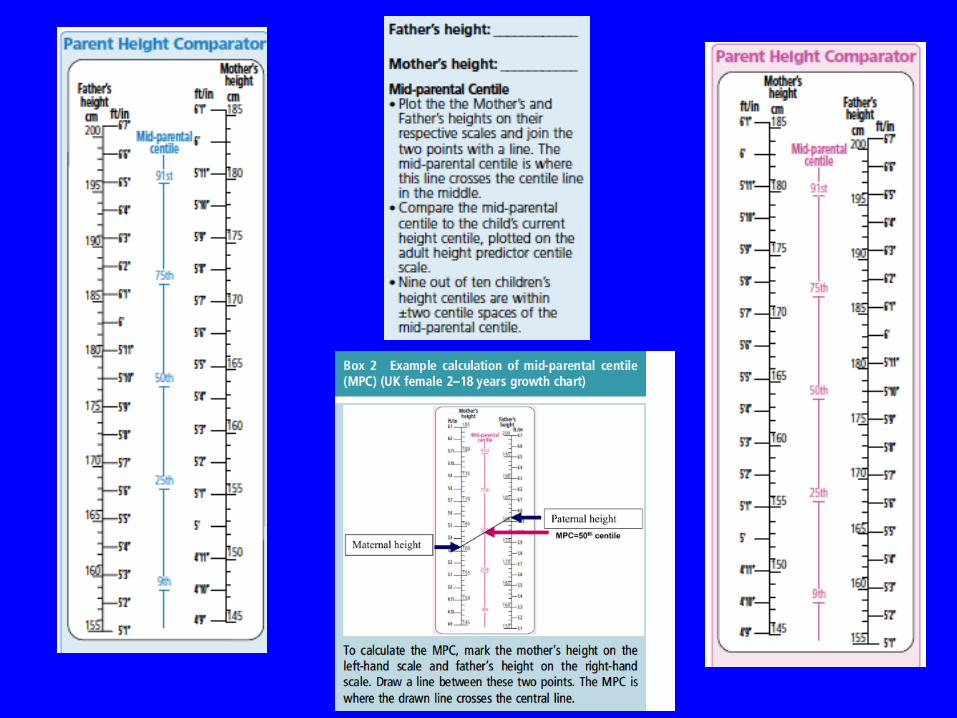
Parental heights
• Check mother and father’s height
• Work out height range based on
measurements and then can see if childs
current centile within range
• Then likely familial short stature


Investigations
• Blood count
• Renal/Liver profile
• Thyroid function
• ESR
• Bone profile
• Coeliac screen
• IGF-1 – can’t measure Growth Hormone
• Karyotype in girls – rule out Turners XO
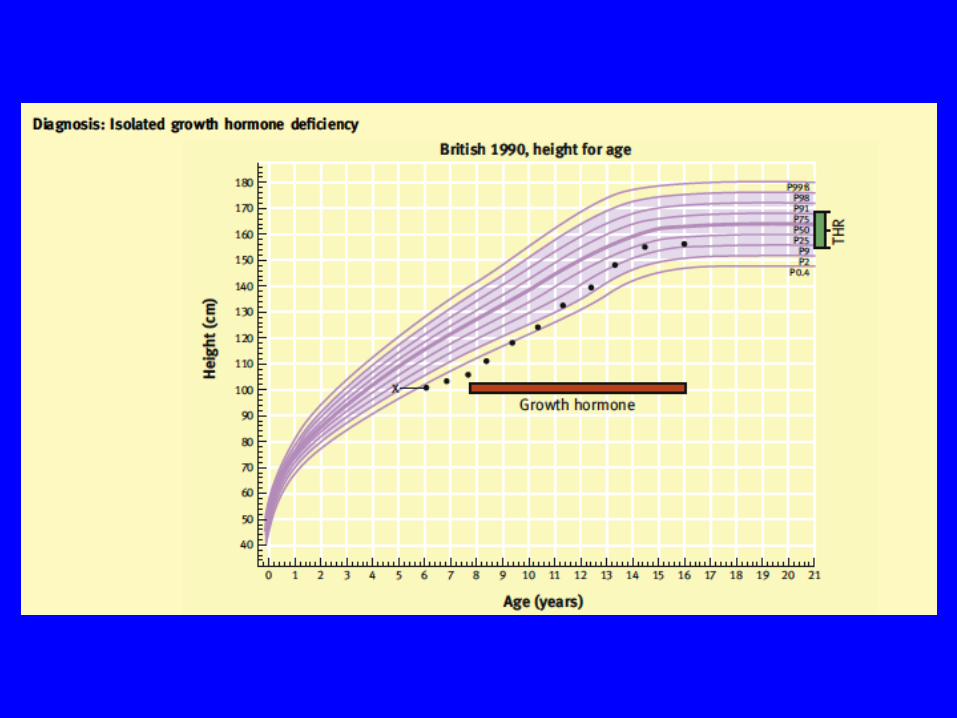
Further investigations
• Bone age
– If bones same age as chronological age, normal
growth but can be 18 months either side
• Growth Hormone stimulation test

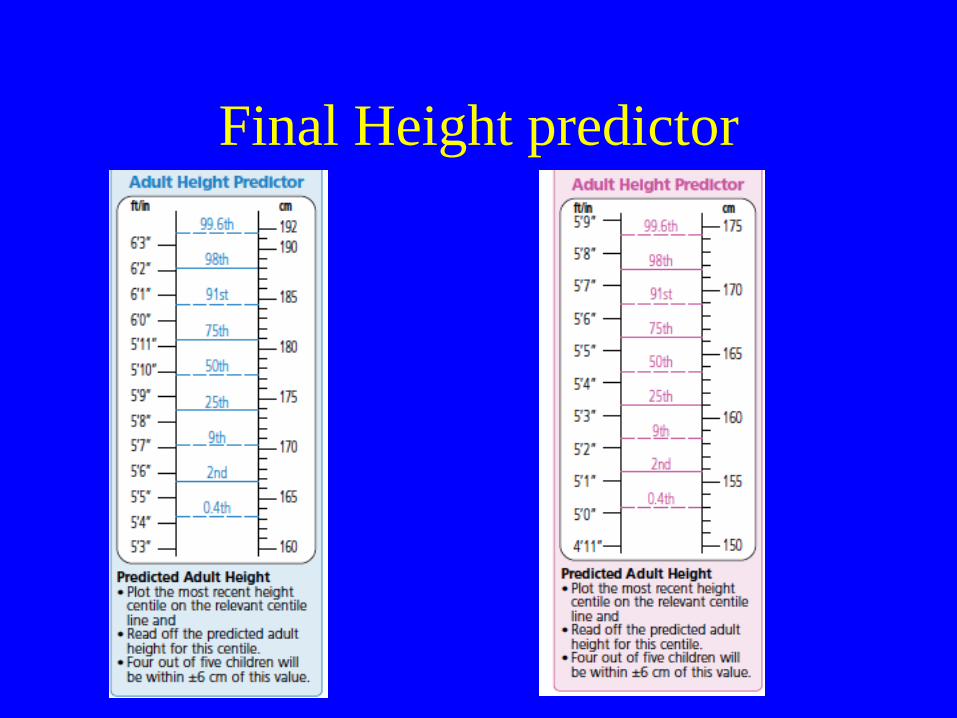
Final Height predictor
Puberty
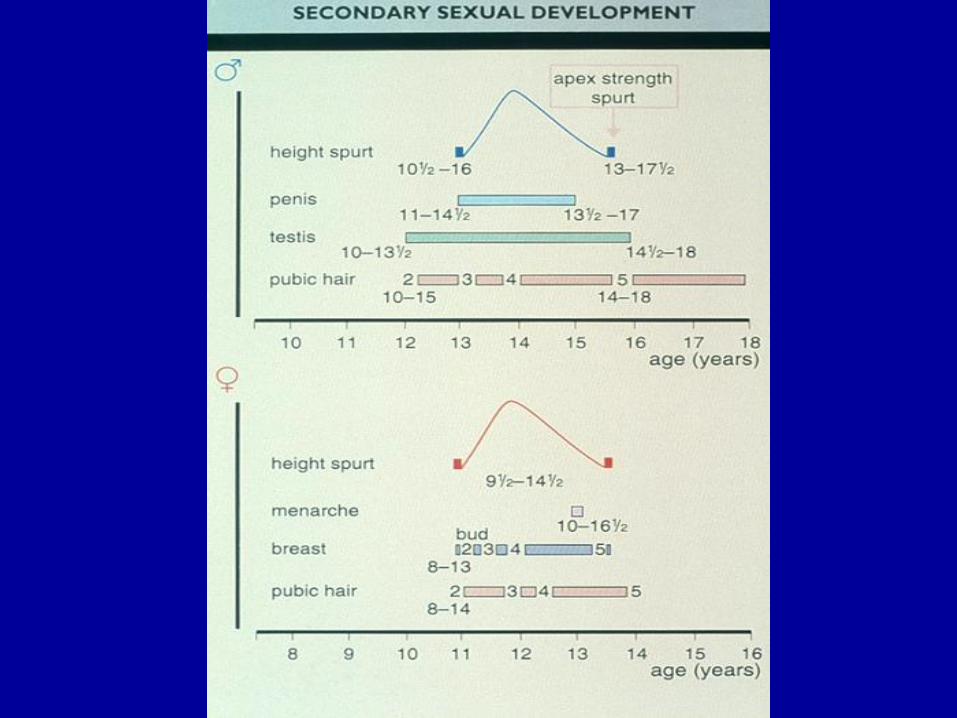
• Precocious (early) puberty defined as:
– In girls < 8 years appearance of secondary sexual characteristics (or < 9 years menarche)
– In boys < 9 years
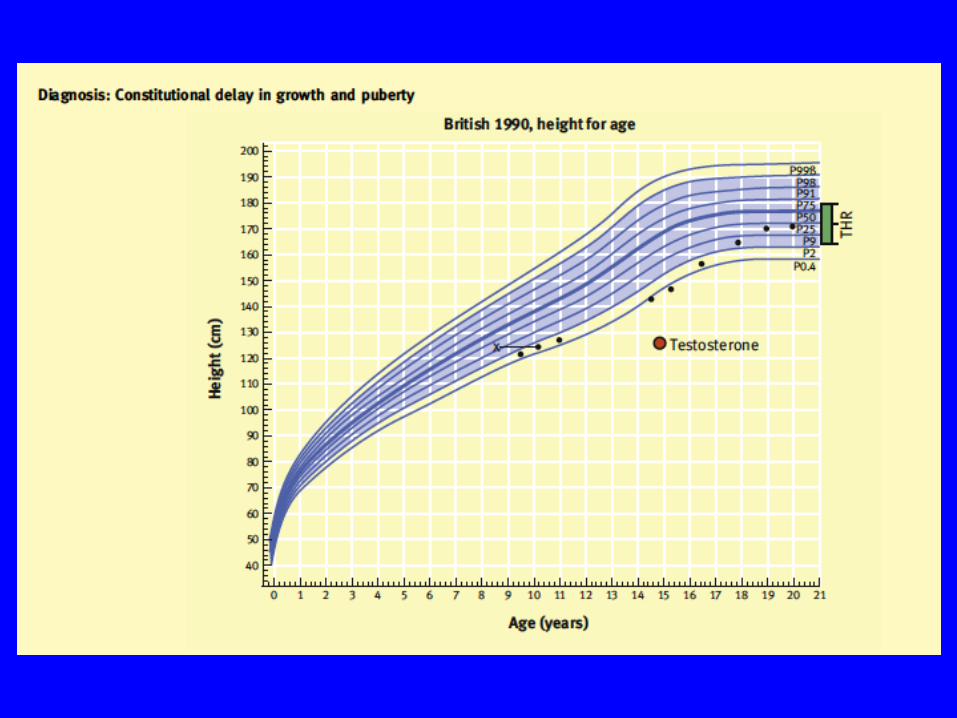
• Delayed puberty defined as:
– In girls no breast development by 13years, normal age around 11 years
– In boys no evidence of testis growth by 14 years (normally starts 11-12 years)
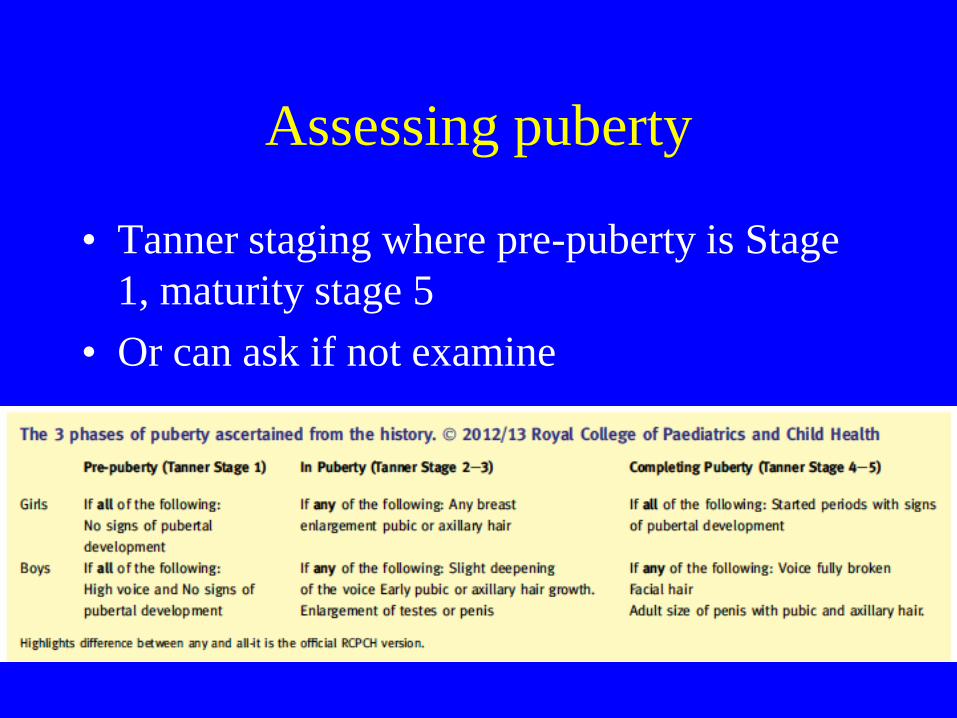
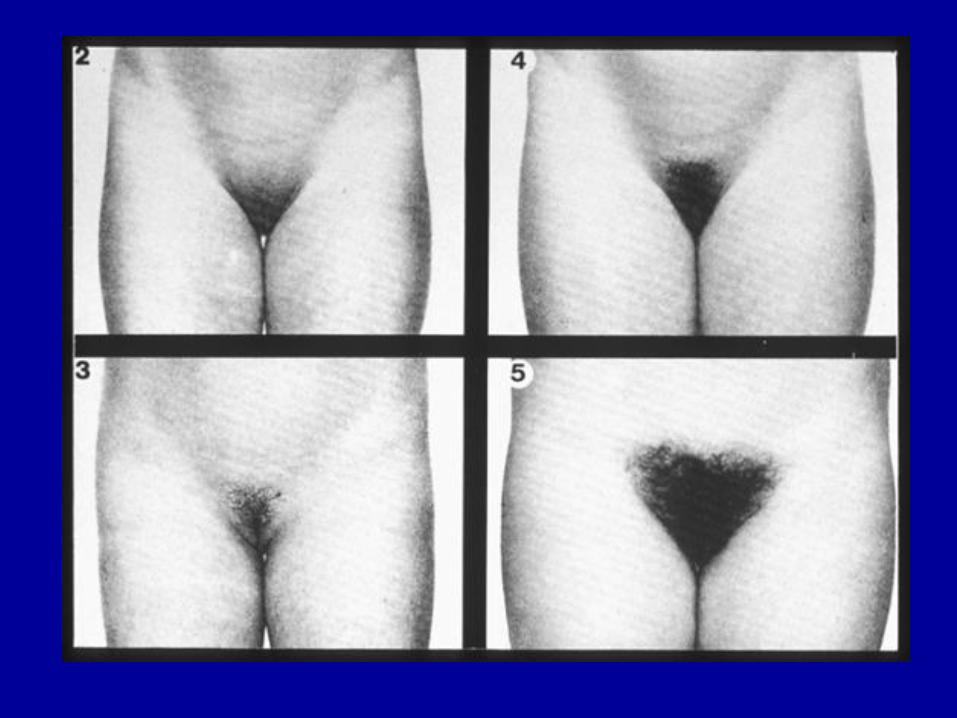
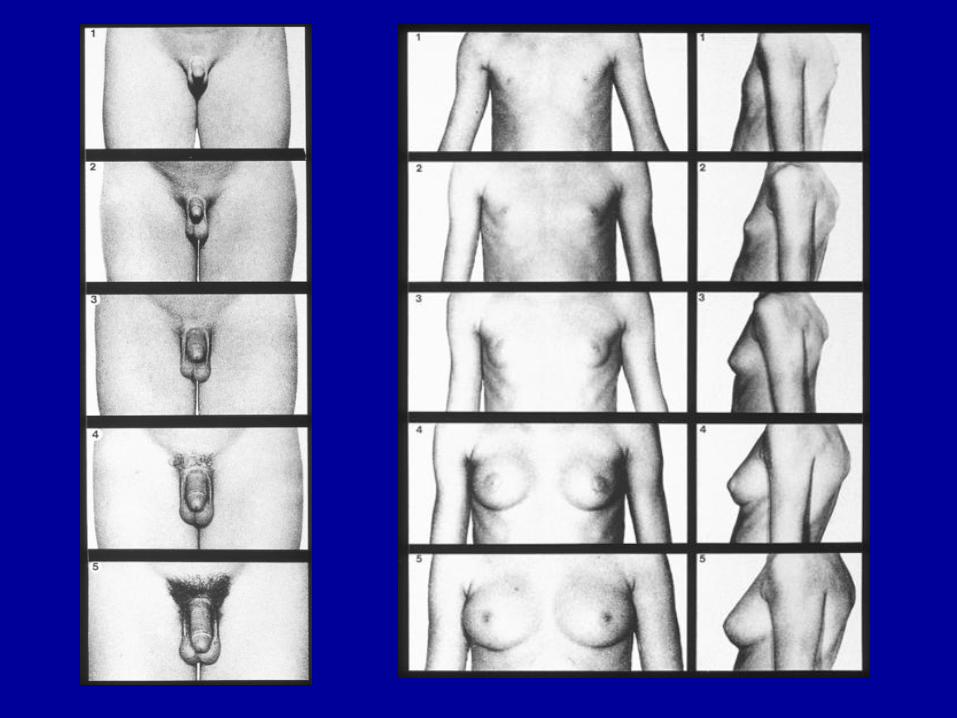
Assessing puberty
• Tanner staging where pre-puberty is Stage
1, maturity stage 5
• Or can ask if not examine

Treatment of delayed puberty
• Exclude serious organic disease/chromosomal
abnormality
• Reassure if above normal, but delay can
produce anxiety, low self-esteem, school
refusal. Counselling an option
• May consider low dose testosterone in boys to
boost growth/pubertal progress
• Treatment rare for girls but consider oestradiol

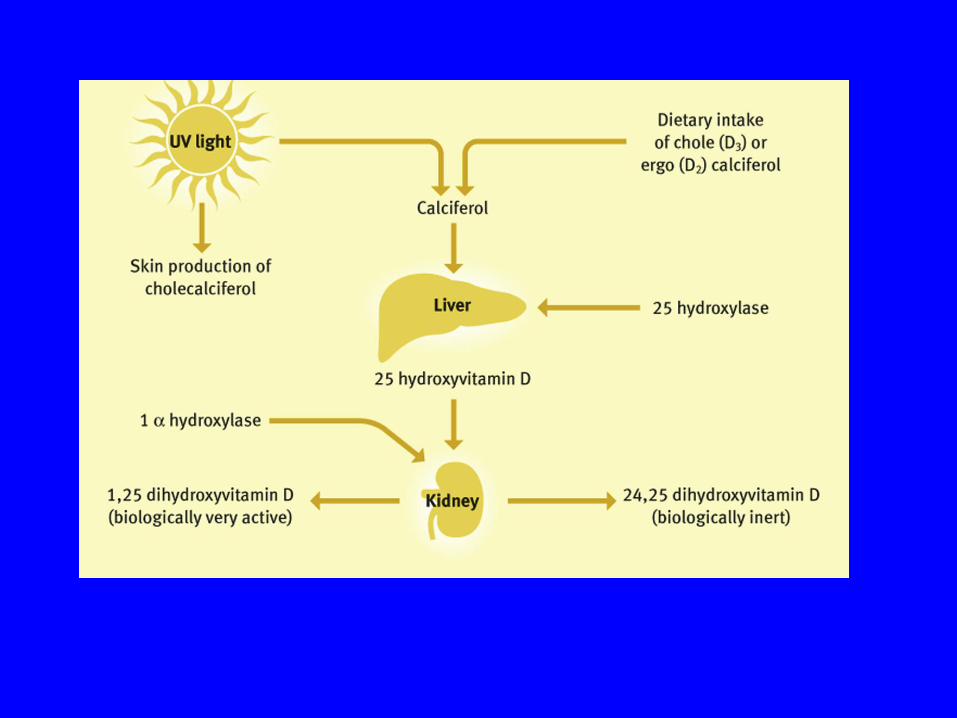
Rickets
• Either due to deficiency of calcium: – Nutritional Vit D deficiency
– Liver/kidney disease Vit D deficiency
• Or due to phosphate deficiency – Nutritional
– Genetic syndromes leading to kidney losses
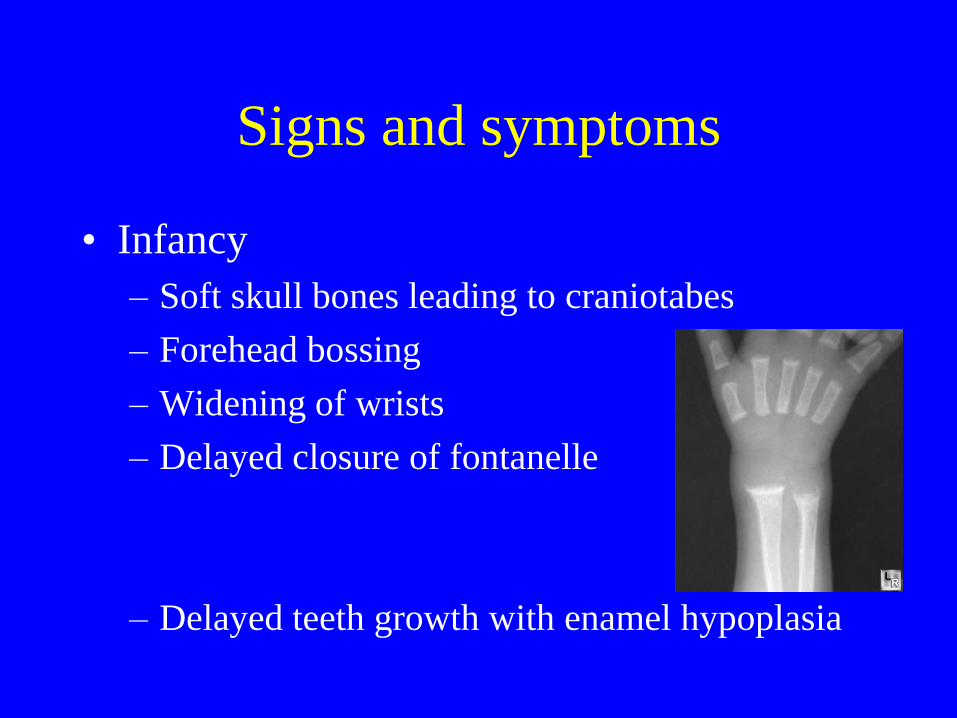
Signs and symptoms
• Infancy
– Soft skull bones leading to craniotabes
– Forehead bossing
– Widening of wrists
– Delayed closure of fontanelle
– Delayed teeth growth with enamel hypoplasia

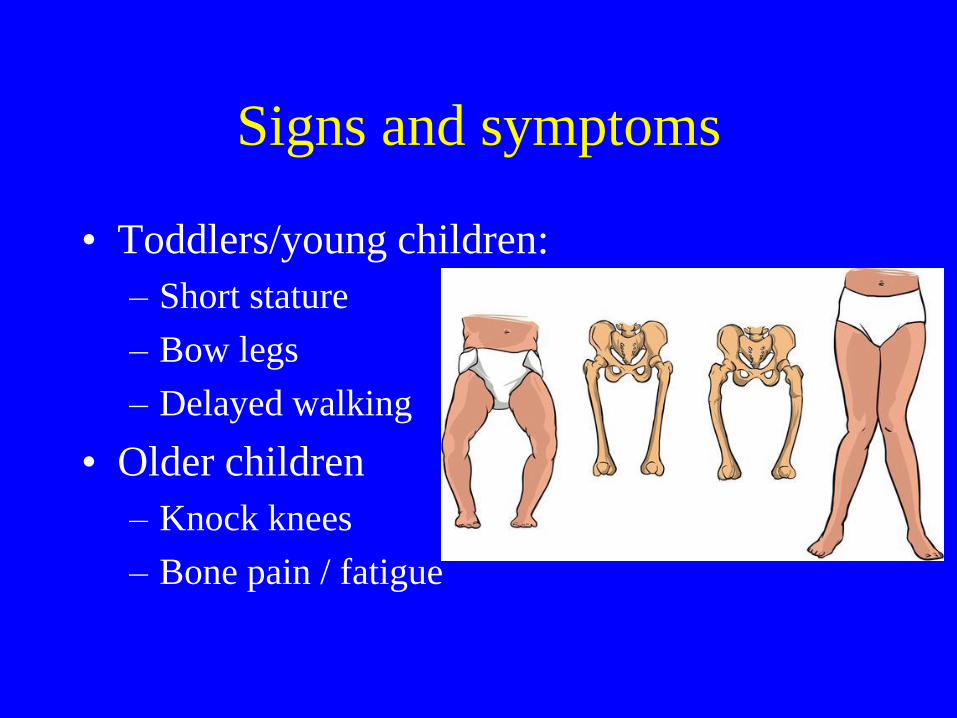
Signs and symptoms
• Toddlers/young children:
– Short stature
– Bow legs
– Delayed walking
• Older children
– Knock knees
– Bone pain / fatigue

Investigations
• Vit D, calcium, phosphate, parathyroid
hormone, x-rays.

Vit D deficient rickets treatment
• Sunlight exposure. In UK 15 mins exposure of hands, arms, face or back 2-3x a week april-september is sufficient.
• May need longer for dark-skinned children
• Foods – oily fish, fish oils, eggs
• Fortified foods like cereals / formula milk
• Vitamin D replacement (keep > 50nmol/L)
• Give to high risk groups up to age 4 eg breastfed babies