Embed Size (px)
Citation preview

Volume 8 • Number 1 • December 2003
266
Guided Tissue Regeneration for the Treatmentof Periodontal Intrabony and Furcation Defects.
A Systematic ReviewKevin G. Murphy* and John C. Gunsolley†
*Private practice, Baltimore, Maryland.† Department of Periodontics, College of Dental Surgery, University of Maryland, Baltimore.
Background: Many clinical studies have demonstrated that guided tissue regeneration (GTR) is a suc-cessful treatment modality of periodontal reconstructive surgery and it has become an accepted procedurein most periodontal practices.
Rationale: The purpose of this structured review was to assess the efficacy of guided tissue regenera-tion (GTR) procedures in patients with periodontal osseous defects compared with surgical controls onclinical, radiographic, adverse, and patient-centered outcomes. It extends the scope of previous GTR sys-tematic reviews, which were limited to randomized controlled studies, by the scope of outcome measuresexamined, and the duration of the study.
Focused Question: In patients with periodontal osseous defects, what is the effect of physical barrierscompared with surgical controls on clinical, radiographic, adverse, and patient-centered outcomes?
Search Protocol: An electronic search of the Cochrane Oral Health Group Trials Register and MEDLINEdatabases was performed. Manual searching of journals included Journal of Clinical Periodontology, Jour-nal of Periodontology, and Journal of Periodontal Research up to January 2002. This manual search alsoincluded review of relevant bibliographies. Two manufacturers of GTR devices were contacted regarding unpub-lished data.
Selection CriteriaInclusion criteria: Studies were selected for review if the evidence level was 3B (cohort) or above, at least
6 months duration, and compared a test GTR intervention with a surgical control.Exclusion criteria: Studies with experimental design problems; histologic or microbiological investigations;
or those with outcome measurements, study populations, or study duration not consistent with the inclu-sion criteria were excluded.
Primary outcome measures for intrabony defects were: clinical attachment level (CAL) gain, probingdepth reduction (PD), gingival recession (REC) reduction; for furcation defects: vertical probing attachmentlevel (VPAL) gain, vertical probing depth reduction (VPD), horizontal probing depth reduction (HPD), hor-izontal open probing attachment level gain (HOPA), and vertical open probing attachment level gain (VOPA).Meta-analysis was performed to compare GTR procedures to other surgical treatments and to examine theresulting clinical outcomes.
Main Results1. For the primary outcome variables, in both intrabony-defect and furcation-defect studies, GTR was
favored over open flap debridement (OFD) therapies (P <0.0001).2. No differences were detected among barrier types, but barrier types could explain some heterogene-
ity in the results.3. Augmentation of the GTR barrier with a particulate graft enhanced VPD (P <0.05), VPAL, and HOPA,
but none of the intrabony outcomes.Reviewer’s Conclusions: Overall, GTR is consistently more effective than OFD in the gain of clinical
attachment and probing depth reduction in the treatment of intrabony and furcation defects.Ann Periodontol 2003;8:266-302.
KEY WORDSComparative studies; guided tissue regeneration; outcomes assessment; membranes, barrier;periodontal diseases/surgery; review literature; surgical flaps; meta-analysis.
8011.qxd 12/30/03 3:33 PM Page 266

Ann Periodontol Murphy, Gunsolley
267
Many clinical studies have demonstrated thatguided tissue regeneration (GTR) is a success-ful treatment modality of periodontal recon-
structive surgery. The GTR technique delays the apicalmigration of the gingival epithelium by excluding thegingival connective tissue and allows granulation tissuederived from the periodontal ligament and osseous tis-sues to repopulate the space adjacent to the denudedroot surface. Several human biopsy GTR studies havedocumented new attachment resulting in new connec-tive tissue attachment and bone fill.1-3 Early proof-of-principle studies also demonstrated that GTR proceduresresulted in the improvement of clinical measures.4-7
However, patient-centered outcomes, such as patientcomfort, long-term tooth retention, dentition stability,absence of pain and esthetic appearance are seldomdiscussed in regenerative studies.8 Therefore, the sur-rogate outcomes of attachment level gain, reductionin probing depth, gingival recession, and alveolar bonechanges are considered the primary outcomes of GTRtherapies.9 This systematic review will attempt toexamine the efficacy of GTR on patient-centered andsurrogate outcomes.
The purpose of this systematic review was to assessthe efficacy of guided tissue regeneration (GTR) pro-cedures in patients with periodontal osseous defectscompared with surgical controls on clinical, radiogra-phic, adverse, and patient-centered outcomes.
FOCUSED QUESTIONIn patients with periodontal osseous defects, what is theeffect of physical barriers compared with surgical con-trols on clinical, radiographic, adverse, and patient-centered outcomes?
SEARCH PROTOCOLData Sources and Search StrategiesAn electronic search of the Cochrane Oral Health GroupTrials Register (CCTR) and MEDLINE databases wasperformed. The Journal of Clinical Periodontology, Jour-nal of Periodontology, and Journal of PeriodontalResearch, including reviews of relevant bibliographies,were manually searched up to January 2002. Two man-ufacturers of GTR devices were contacted regardingunpublished data.
The following search terms were used: (all terms usingthe “OR” operand): guided tissue regeneration, guided-tissue-regeneration, GTR, intra bony, intrabony defect;infrabony, infra bony, intra osseous, intraosseous defect,intra-osseous, furcation, furcation defect, complications,surgical complications, postoperative complications, sur-gical wound infection, and gingival recession.
Study TypesThe types of studies included for this review were: ran-domized controlled clinical studies (RCTs), systematic
reviews of RCTs, systematic reviews of cohort stud-ies, and cohort studies (CHT), systematic reviews ofcase-control studies, and case-control studies (CS).
Inclusion Criteria: Studies were limited to patientswith a diagnosis of chronic (adult) periodontitis andwho were 21 years or older. Studies examining bothintrabony and furcation defects were reviewed, butexamined separately.
All studies which included some form of the place-ment of a physical barrier membrane, designed toselectively exclude unwanted tissue from repopulatingthe periodontal wound, either as test or control inter-vention, were considered for inclusion.
Exclusion Criteria: Studies with experimental designproblems; histologic or microbiological investigations;or those with outcome measurements, study popula-tions, or study duration not consistent with the inclu-sion criteria were excluded.
ComparisonsThe following comparisons were made:
1. GTR procedures versus open flap debridement(OFD).
2. GTR procedures using a barrier plus some formof augmentation, usually a particulate bone graft, ver-sus GTR procedures using a barrier alone.
3. GTR procedures using an expanded polytetra-fluoroethylene (ePTFE) barrier versus GTR proceduresusing a bioabsorbable barrier type.
4. GTR procedures using one surgical protocol ver-sus GTR procedures using a different surgical proto-col, but the same barrier material type, based upon theflap closure technique employed.
5. GTR procedures using one postoperative recallcare regimen versus GTR procedures using a differentpostoperative recall care regimen.
OutcomesShort-term: The following clinical parameters wereevaluated by recording changes in the outcome vari-able from the time of surgery to the end of the evalu-ation period:
1. Clinical attachment level gain (CAL), measuredin both a vertical (VPAL) and horizontal (HPAL) direc-tion for furcation-defect studies.
2. Probing depth reduction (PD), measured in botha vertical (VPD) and horizontal (HPD) direction forfurcation-defect studies.
3. Gingival recession (REC) increase.4. Bone levels: assessed radiographically (X-rays)
and/or at a re-entry; (Re-entry) for intrabony-defectstudies and HOPA (horizontal) and vertical (VOPA) forfurcation-defect studies.
5. Oral hygiene efficacy and compliance utilizing full-mouth bleeding scores (FMBS) or stated oral hygieneindex.
8011.qxd 12/30/03 3:33 PM Page 267

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
268
6. Complications related to surgical treatment (alsoa patient-centered outcome): exposure of barrier (ifapplicable), abscess formation, recession, morbidityfactor of pain.
Long-term: Long-term measurements included:1) tooth retention; 2) FMBS; and 3) disease recurrence.
Patient-centered: Patient-centered outcomes were:1) complications related to surgical treatment; 2) easeof maintenance-residual PD, defined as sites with lessthan 4 mm; and 3) esthetics, defined as REC in ante-rior teeth.
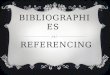
Data Collection and AnalysisThe study selection process is summarized in Figure 1.This search strategy resulted in the initial screening of
1,543 publications. These publications were entered intoa publication database manager. The abstracts of thesepublications were then obtained and reviewed. If abstracts
Figure 1.Study screening process.
Table 1.
Studies Failing to Meet Inclusion Criteria
Reference Rationale for Exclusion
Yukna10 1992; Eickholz, et al.11 2001 Data presentation errors
Windisch et al.12 2002; Teparat et al.13 1998; Dubrez et al.14 1996; Dowell et al.15 1995 Experimental design problem
Vuddhakanok et al.16 1993 Histologic investigation
Smith MacDonald et al.17 1998; Wang et al.18 1997; Chen et al.19 1997; De Sanctis et al.20 1996; MicrobiologicalMombelli et al.21 1996; Simion et al.22 1995; Frandsen et al.23 1994; Nowzari & Slots24 1994;Demolon et al.25 1993; Tempro & Nalbandian26 1993; Grevstad & Leknes27 1993; Minabe28 1991
Calongne et al.29 2001; Cortellini & Tonetti30 2001; Murphy et al.31 2000; Cortellini et al.32 1999; Case series or inadequateAguirre-Zorzano et al.33 1999; Eickholz & Hausmann34 1999; Tatakis & Trombelli35 1999; Peter et al.36 surgical controls1998; Eickholz et al.37 1998; Eickholz & Hausmann38 1998; Christgau et al.39 1997; Machtei et al.40 1995;Murphy41 1995; Froum & Tarnow42 1995; Müller & Eger43 1997; Trombelli & Scabbia44 1997;Eickholz & Hausmann45 1997; Trombelli et al.46 1997; Falk et al.47 1997; Cortellini et al.48 1996; De Sanctis et al.49
1996; Murphy50 1996; Piattelli et al.51 1996; Tonetti et al.52 1996; Nowzari et al.53 1996; Yukna & Yukna54 1996;Becker et al.55 1996; Machtei et al.56 1996; Cortellini et al.57 1996; Müller et al.58 1995; Novaes et al.59 1995;Drummond et al.60 1995; Cortellini et al.61 1995; Weigel et al.62 1995; Murphy63 1995; Anderegg et al.64 1995;Polson et al.65 1995; Cortellini et al.66 1995; Tonetti et al.67 1995; Laurell et al.68 1994; Cortellini et al.69 1994;Schallhorn & McClain70 1994; Trombelli et al.71 1994; Rosenberg & Cutler72 1994; Machtei et al.73 1994;Florès-de-Jacoby et al.74 1994; Tonetti et al.75 1993; Polson et al.76 1993; Tonetti et al.77 1993; Cortellini et al.78
1993; McClain & Schallhorn79 1993; Galgut80 1993; Mullally et al.81 1993; Al-Arrayed et al.82 1993;Selvig et al.83 1992; Gottlow et al.84 1992; Paul et al.85 1992; Stahl & Froum86 1991; Stahl & Froum3 1991;Galgut87 1990; Stahl et al.1 1990; Schallhorn & McClain5 1988; Gottlow et al.2 1986; Selvig et al.88 1993;Garrett et al.89 1988; Polson et al.90 1995; Eickholz et al.91 1996; Pontoriero et al.92 1989
Sbordone et al.93 2000; Wenzel et al.94 1992; Pontoriero et al.95 1987; Iversen et al.96 1996 Outcome measurements not consistent with this systematic review
Eickholz et al.97 2000; Karapataki et al.98,99 2000; Dörfer et al.100 2000; Trejo et al.101 1998; Chaves et al.102 Study population not1996; Sirirat et al.103 1996; Sander et al.104 1994; Stein et al.105 1993 consistent with this
systematic review (chronic periodontitis)
Sculean et al.106 2001; Christgau et al.107 1995; Twohey et al.108 1992 Study duration not consistent with this systemic review
8011.qxd 12/30/03 3:33 PM Page 268

Ann Periodontol Murphy, Gunsolley
269
were not available, the full-text publications were re-viewed for appropriateness for inclusion. On basis oftitle and abstract review, the full-text publications of 192studies were obtained and evaluated for inclusion inaccordance with the protocol of this systematic review.The 103 studies excluded for failing to meet inclusioncriteria are summarized in Table 1.1-3,5,10-108 Thedatasets of studies that provided only standard errorvalues were modified by estimating the standard devi-ation values.
The selection process resulted in the inclusion of 89publications for this review.4,6,109-195 Some of thesestudies had multiple arms that were suitable for analy-sis.109,110,119,132,133,138,140,142,145,147,157,167,182 A sub-set of studies initially failed to present either standarddeviation or standard error values. These studies wereassigned a standard deviation value derived from theaverage standard deviation for the same test or controlgroup of all studies containing standard deviation values.Table 2 summarizes intrabony-defect studies that wereincluded using these assumed values.109-114 Table 3summarizes furcation-defect studies that were includedusing these assumed values.115-126 This process of stan-dard deviation value assignment resulted in the inclu-sion of an additional 18 studies for analysis.109-126
Due to the large number of publications, a relationaldatabase program was used to enter the descriptive vari-ables of the evaluated studies. Using a database formtemplate, a data abstraction form was created. Eighty-two descriptive variables and 2 surgical technique andpostoperative care rankings were gathered for each studyreviewed. Five descriptive groupings for each study weredefined: Study design, treatment protocol, subject char-
acteristics, clinical outcomes, and patient-centered out-comes. The methodological quality of the study wasassessed, examining protocol characteristics such asrandomization methods, therapist and examiner con-cealment or masking, split-mouth or parallel design, andlimitations on number of test or control sites per patient.
In addition to the criteria listed in the data abstrac-tion form, 2 procedural rankings were developed.Advanced flap management techniques are frequentlyutilized to enhance primary closure over the physicalbarrier.32,48,66,127-129 The effect of these techniqueswas examined through the development of a rankingsystem. The flap closure ranking was assigned to eachstudy as using the following criteria:
Grade 1. No attempt to cover barrier with flap or a“standard technique” wherein gingival flaps are adaptedas best possible with standard incision design and inter-rupted sutures.
Grade 2. Periosteal fenestration or split-thicknessdissection used to facilitate passive flap adaptation; inter-rupted sutures. Some form of papillae retention is used.
Grade 3. Papillae retention with some form of mat-tress suturing or specifically designed flap incision andclosure techniques such as the modified papillaepreservation technique (MPPT)129 or the simplifiedpapillae preservation technique (SPPT).32
The effect of increasing frequency of postoperativecare visit upon clinical outcomes was examined by rank-ing each study’s supportive recall program as follows:
Grade 1. No weekly care stated in protocol or woundstabilization protocol for 6 weeks or 2 or less interventionsfor the first month; longer than monthly intervals for theremainder period or 3 or more interventions for the first
Table 2.
Intrabony-Defect Studies Selected for Inclusion, Using Modified Standard Deviation Values
Intervention
Reference Design Test Control Study Ranking
Pontoriero et al.109 1999 (4-arm study) RCT EMD OFD 1B
PLA OFDPLA/PGA OFD
ePTFE OFDSculean et al.110 1999 (2-arm study) RCT EMD PLA/PGA 1B
EMD + EDTA PLA/PGAal-Arrayed et al.111 1995 RCT Hum coll OFD 3B
Orsini et al.112 2001 CHT Ca sulfate + autogeneous bone Bov coll + autogenous bone 3BQuteish & Dolby113 1992 CHT Hum coll (human) OFD 3B
Bratthall et al.114 1998 RCT PLA/PGA OFD 2B
Abbreviations: Bov coll = bovine collagen; Ca = calcium; EMD = enamel matrix proteins; ePTFE = expanded polytetrafluoroethylene; Hum coll = humancollagen; OFD = open flap debridement; PLA/PGA = polylactic/ polyglycolic acid.
8011.qxd 12/30/03 3:33 PM Page 269

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
270
month, longer than a monthlyinterval but less than or equal toa 3-month interval for the remain-der period.
Grade 2. At least bi-weeklyfor the first 6 weeks, then everymonth thereafter.
Grade 3. Weekly for the first2 months, then bi-weekly ormonthly thereafter.
The accumulated data wereexported from the relationaldatabase to the statistical ana-lysis software. Weighted treat-ment outcomes were calculatedand expressed as weighted meandifferences. Multiple treatmentoutcomes were analyzed. Forintrabony-defect studies, CAL,PD, and REC were the primaryoutcome measures. For furcation-defect studies, VPAL, VPD, REC,VOPA, and HOPA were the pri-mary outcome measures. Hardtissue gain was also studied byexamining re-entry and x-rayoutcome measures. The statisti-cal significance of discrepanciesin the estimates of treatmentoutcomes or heterogeneity was
Table 3.
Furcation-Defect Studies Selected for Inclusion, Using Modified Standard Deviation Values
Intervention
Reference Design Test Control Study Ranking
Caton et al.115 1994 RCT PLA 910 OFD 1B
Garrett et al.116 1997 RCT PLA ePTFE 1BHugoson et al.117 1995 RCT PLA ePTFE 1B
Mehlbauer et al.118 2000 RCT PLA + PLA 910 (double barrier) + DFDBA PLA + DFDBA 1BMellonig et al.119 1994 RCT ePTFE OFD 2B
Mellonig et al. 119 1994 RCT ePTFE OFD 2BPontoriero & Lindhe120 1995* RCT ePTFE, Class II OFD 2B
Pontoriero & Lindhe121 1995* RCT ePTFE, Class III OFD 2BVan Swol et al.122 1993 RCT Bov coll OFD 2B
Vernino et al.123 1998 RCT PLA PLA 2BDemolon et al.124 1994 RCT ePTFE + amoxicillin + clavulanatic acid ePTFE 2B/3B
Garrett et al.125 1990 CHT Dura mater + DFDBA + citric acid + CPF DFDBA + citric acid + CPF 3BWallace et al.126 1994 RCT ePTFE + DFDBA ePTFE 3B
* SD and SE only shown graphically.Abbreviations: CPF = coronally positioned flap; ePTFE = expanded polytetrafluoroethylene; OFD = open flap debridement; PLA = polylactice acid; PLA/PGA =polylactic/polyglycolic acid; PLA 910 = polyglactin 910.
Table 4.
Intrabony-Defect Studies* that Provided Standard Deviation or Error Values
Intervention
Reference Design Test Control
Bichara et al.130 1999 RCT, split-mouth PLA + naproxen PLA500 mg bid
Cortellini131 1998 RCT, split-mouth PLA OFDCortellini et al.132 1995 RCT, parallel Cover of NFGT with CT CPF over NFGT
Cortellini et al.133 1996 RCT, parallel ePTFE OFDCortellini et al.133 1996 PLA OFD
Cortellini et al.132 1995 RCT, parallel ePTFE-TR OFDCortellini et al.127 2001 RCT, parallel PLA OFD
Gouldin et al.135 1996 RCT, split-mouth ePTFE + DFDBA ePTFEGuillemin et al.136 1993 RCT, split-mouth ePTFE + DFDBA ePTFE
Joly et al.137 2002 RCT, split-mouth PLA/PGA OFD
Kim et al.138 1996 RCT, parallel Ca carbonate + ePTFE Ca carbonateKim et al.138 1996
ePTFE OFDLekovic et al.139 2001 RCT, split-mouth Bov coll EMD + BPBM OFD
Sculean et al.140 2001 RCT, parallel PLA OFDSculean et al.140 2001 PLA + EMD EMD
8011.qxd 12/30/03 3:33 PM Page 270

Ann Periodontol Murphy, Gunsolley
assessed by means of Cochran’s test for heterogeneityusing fixed- and random-effects modeling. Regressionanalysis was performed to examine the relationship ofthe flap closure technique, postoperative recall care fre-quency, and timing of barrier removal upon the out-come measures.
Ranking of StudiesOnly studies assessed to be of evidence levels lB through3B as defined by the Oxford Centre for Evidence-basedMedicine Levels of Evidence (http://cebm.jr2.ox.ac.uk/docs/levels.html) were selected for analysis. Durationof the study was not a criterion for exclusion.
DESCRIPTION OF STUDIESIntrabony DefectsTable 4 summarizes the intrabony-defect studiesselected for inclusion. Fifty-two arms from 44 studiesqualified for inclusion.6,114,130-170 Only 4 studies werecohort (CHT) designed,166,168-170 the remainder wereRCTs. Of these RCTs, 20 studies were of a split-mouthdesign. Only 20 studies used some form of conceal-ment. Eighteen studies had a length of study under 12months, but none less than 6 months. The ages of par-ticipants ranged from 21 to 84 years. Smokers were
excluded in only 2 studies, but 13 studies made someform of smoker-data subset available. There was ainconsistent definition of a smoker. Seventeen studiesused an advanced form of flap closure technique cor-relating to Grade 3. Eleven studies employed a recallcare frequency of Grade 3.
Furcation DefectsTable 5 (page 274) summarizes the furcation-defectstudies selected for inclusion.4,167,171-194 Of the quali-fying studies, only one was a CHT.193 Of the remainingRCTs, 22 were a split-mouth design. Only 6 studiesemployed examiners masked to therapy and only 2studies used therapists masked to the treatment choicebefore the barrier placement. Sixteen studies were lessthan 12 months duration, but none were less than 6months. The ages of the participants ranged from 21to 76 years. Smokers were excluded in only 2 studiesand 4 studies provided smoker subset data. Ten of thestudies described recall care frequencies of Grade 3.
MAIN RESULTSLong-Term ResultsLong-term outcome variables such as tooth loss requirethe use of long-term studies. This systematic review failed
to identify any studies meetingthe inclusion criteria which eval-uated patient outcomes for morethan 5 years. Therefore, no state-ments can be made regardingthe efficacy of periodontal ther-apy using physical barriersenhancing tooth retention.
Providing patients with a peri-odontium that is easier to main-tain is indirectly related to prob-ing depth reduction and ismanifested in post-treatmentgingival bleeding indices. As willbe discussed in detail, reductionin PD and gain in CAL as sur-rogate variables were uniformlyenhanced in GTR procedures ascompared to OFD controls. Thebleeding index utilized variedgreatly among the includedstudies, as did the evaluationinterval, making comparisonslimited. In furcation-defect stud-ies, the incidence of furcationclosure was not evaluated dueto the disparity in the definitionof what constituted completeclosure of the furcation as wellas diagnosis of the grade of thefurcation.
271
Table 4. (continued)
Intrabony-Defect Studies* that Provided Standard Deviation or Error Values
StudyDuration Augmentation
N Study PopulationStudy
(months) Material Test Control Outcomes Ranking
9 24 24 CAL, PD, REC, re-entry 1B
12 23 23 CAL, PD, REC 1B12 14 14 VPAL, PD, REC 1B
12 12 12 CAL, PD, REC 1B12 12 12 CAL, PD, REC
12 15 15 CAL, PD, REC 1B12 55 54 CAL, PD, REC 1B
6 DFDBA 26 26 CAL, PD, REC, re-entry 1B6 DFDBA 15 15 CAL, PD, REC, re-entry 1B
8 TET roots 10 10 CAL, PD, REC, x-rays, 1Bre-entry
6 CA carbonate 14 13 CAL, PD, REC 1B
6 19 18 CAL, PD, REC 1B6 EMD + BPBM 18 18 CAL, PD, REC, re-entry 1B
12 14 14 CAL, PD, REC 1B12 EMD 14 14 CAL, PD, REC 1B(continued)
8011.qxd 12/30/03 3:33 PM Page 271

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
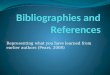
Intrabony-Defect StudiesBarrier versus open flap debride-ment therapy. Considering allbarrier types, meta-analysis ofincluded studies demonstratedthat GTR procedures resulted ina greater gain in clinical attach-ment (CAL) when compared toOFD controls (Fig. 2, page 277;and Tables 6, page 278; and 10,page 284) at a significance levelof P <0.0001. Removing studiesin which standard deviation val-ues were assumed did not affectthis outcome. Subgroup analy-sis of the barrier type, whethercollagen-derived, ePTFE, or apolymeric bioabsorbable barrier,demonstrated that the addedbenefit of the physical barrierremains constant independent ofthe barrier type employed. Het-erogeneity among the ePTFEand polymeric groups was highlysignificant (P <0.05). This het-erogeneity became nonsignifi-cant when the 3 most efficaciousstudies within each group whereexcluded.132,133,137 When thesestudies were excluded, the treat-ment effects of using a physicalbarrier remained highly signifi-cant (P >0.0001). The differencein gain of CAL between the testbarrier types collagen, poly-meric, and ePTFE and an OFDcontrol was 0.95 ± 0.47 mm,0.92 ± 0.18, and 1.61 ± 0.25 mm,respectively.
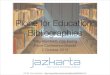
Similar findings were demon-strated with PD reduction for allbarrier types at a significancelevel of P <0.0001 (Fig. 3, page279; Tables 7, page 280; and 10,page 284). Removing studies inwhich assumed standard devia-tion values were utilized did notaffect this outcome. Subgroupanalysis of the barrier type,whether collagen-derived, ePTFE,or a polymeric bioabsorbable bar-rier, demonstrated that the addedbenefit of the physical barrierremains constant independent ofthe barrier type employed. Het-erogeneity among the groupings
272
Table 4. (continued)
Intrabony-Defect Studies* that Provided Standard Deviation or Error Values
Intervention
Reference Design Test Control
Tonetti et al.141 1998 RCT, parallel PLA/PGA- OFDTonetti et al.142 1996 RCT, parallel ePTFE-TR OFDTonetti et al.142 1996
ePTFE OFDTrejo et al.143 2000 RCT, parallel PLA + DFDBA PLA
Yoshinari et al.144 2001 RCT, parallel ePFTFE + minocycline ePTFEointment
Zucchelli et al.145 2002 RCT, parallel EMD ePTFEZucchelli et al.145 2002 RCT; split-mouth ePTFE-TR OFD
parallelZucchelli et al.146 1999 RCT, parallel ePTFE-TR + ePTFE-TR
metronidazole gel
Zybutz et al.147 2000 RCT, split-mouth PLA OFDZybutz et al.147 2000 ePTFE OFD
Blumenthal & Steinberg148 RCT, parallel Bov coll + DFDBA OFD1990
Camargo et al.149 2000 RCT, split-mouth Por coll + BPBM OFD
Mattson et al.150 1999 RCT, parallel Bov coll PLA/PGABenqué151 1997 CHT Bov coll (rapidly Bov coll (adult
progressive periodontitis)periodontitis)
Batista et al.152 1999 RCT, split-mouth Cellulose + HA CelluloseBratthall et al.114 1998 RCT, split-mouth PLA/PGA OFD
Chen et al.153 1995 RCT, split-mouth Bov coll + DFDBA Bov collChristgau et al.154 RCT, split-mouth PLA PLA 910
1998
Christgau et al.155 RCT, split-mouth PLA 910 ePTFE1997
Handelsman et al.6 1991 RCT ePTFE + citric acid ePTFE
Kersten et al.156 1992 RCT, split-mouth ePTFE + citric acid ePTFEKiliç et al.157 1997 RCT, parallel ePTFE OFDKiliç et al.157 1997
ePTFE + HA HAKim et al.158 1998 RCT, parallel Calcium sulfate + DFDBA OFD
Mayfield et al.159 1998 RCT, parallel PLA OFDMellado et al.160 1995 RCT, split-mouth ePTFE + DFDBA ePTFE
Paolantonio161 2002 RCT, parallel Pericardium + BPBM PericardiumPaolantonio et al.162 RCT, split-mouth Rubber dam ePTFE
1998
Weltman et al.163 1997 RCT, parallel PLA ePTFEZarkesh et al.164 1999 RCT, parallel ePTFE + TET ePTFE
8011.qxd 12/30/03 3:33 PM Page 272

Ann Periodontol Murphy, Gunsolley
of all barriers combined and thepolymeric barriers was significantP <0.01. Again, when the 3 mostefficacious studies were removedfrom analysis, the heterogeneitybecame nonsignificant while thetreatment effect remained highlysignificant P <0.0001. The differ-ence in PD reduction betweenthe test barrier types collagen,polymeric, and ePTFE andan OFD control was 1.06 ±0.37 mm, 0.89 ± 0.14 and 1.41 ±0.20 mm, respectively.
Differences between test andcontrol groups for the amountof post-treatment recession(REC) were not significant, butusually were larger in the testgroup (Table 8, page 281; Fig.4, page 282). Both ePTFE andbioabsorbable barriers resultedin a similar amount of mild gin-gival recession. However, stud-ies that utilized some formof advanced flap managementresulted in a decrease in post-treatment recession as com-pared to OFD controls.132,133
ePTFE versus bioabsorb-able barriers. Three studiesdirectly compared the efficacyof a bioabsorbable barrier toePTFE for CAL gain. Weltmanet al.163 evaluated a polylacticacid (PLA) barrier, whereasEickholz et al.167 and Christgauet al.155 evaluated a polyglactin-910 (PLA 910) barrier (Fig. 5,page 282). Meta-analysis ofthese selected studies failed todemonstrate a significant dif-ference between ePTFE and theaforementioned polymeric bar-riers (P = 0.623). Heterogeneitywas significant at the P = 0.03level. In a similar manner to theCAL outcome, no differencesbetween ePTFE and thebioabsorbable barriers wereevident when examining PDreduction as an outcome vari-able (P = 0.272) (Fig. 6, page282) in these 3 studies.Likewise, no differences in theoutcome measure REC were
273
Table 4. (continued)
Intrabony-Defect Studies* that Provided Standard Deviation or Error Values
Study Duration Augmentation
N Study PopulationStudy
(months) Material Test Control Outcomes Ranking
12 69 67 CAL, PD, REC 1B12 15 15 CAL, PD, REC 1B
12 15 15 CAL, PD, REC 1B12 DFDBA 16 16 CAL, PD, REC, re-entry 1B
6 20 20 CAL, PD, REC 1B
12 30 30 CAL, PD, REC 1B12 30 30 CAL, PD, REC 1B
12 26 26 CAL, PD, REC 1B
12 15 15 CAL, PD, REC, re-entry 1B12 14 14 CAL, PD, REC, re-entry 1B
12 DFDBA 15 15 CAL, PD, REC, re-entry 1B-2A
6 EMD + BPBM 22 22 CAL, PD, REC, re-entry 1B-2B
6 11 12 CAL, PD, REC, re-entry 1B-2B6 16 52 CAL, PD, REC 2A-3B
6 Bovine-derived HA 13 13 CAL, PD, REC, re-entry 2B12 11 11 CAL, PD, REC 2B
6 DFDBA 7 8 CAL, PD, REC 2B12 25 25 CAL, PD, REC, x-rays 2B
12 10 10 CAL, PD, REC 2B
9 9 9 CAL, PD, REC, re-entry 2B
12 14 12 CAL, PD, REC 2B6 HA + type I bov coll 10 10 CAL, PD, REC, x-rays 2B
6 HA + type I bov coll 10 10 CAL, PD, REC, x-rays12 Calcium sulfate + 13 13 CAL, PD, REC 2B
DFDBA (matrix is also aug)
12 10 11 CAL, PD, REC, re-entry 2BDFDBA 11 11 CAL, re-entry 2B
12 BPBM 17 17 CAL, PD, REC, re-entry 2B12 22 22 CAL, PD, REC, x-rays 2B
12 16 14 CAL, PD, REC, re-entry 2B12 ePTFE + TET 11 11 CAL, re-entry 2B
(continued)
8011.qxd 12/30/03 3:33 PM Page 273

detected in studies directly com-paring ePTFE to a bioabsorbablebarrier (Fig. 7, page 283).
Barrier versus barrier plusaugmentation material. Sevenstudies examined the effect ofthe addition of an augmenta-tion material under the physi-cal barrier (Fig. 8, page283).135,136,143,152,153,160,161
All studies used a form of partic-ulate bone graft, with demineral-ized freeze-dried bone allograft(DFDBA) selected in 5 of the7 studies. The control interven-tion was the barrier alone whilethe test intervention used thesame barrier in addition to a par-ticulate graft material. Meta-analysis of the selected studiesdid not reveal any difference inCAL gain between test and con-trol groups (P = 0.774). Hetero-geneity was significant (P
GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
274
Table 4. (continued)
Intrabony-Defect Studies* that Provided Standard Deviation or Error Values
Intervention
Reference Design Test Control
Chung et al.165 1990 RCT, split-mouth Bov coll OFDBenqué166 1997 CHT Bov coll + HA (rapidly Bov coll + HA
progressive (adult periodontitis)periodontitis)
Eickholz et al.167 1998 RCT, split-mouth PLA 910 ePTFENygaard-Østby et al.168 CHT ePTFE OFD
1996
Parashis et al.169 1998 CHT PLA DFDBARatka-Krüger et al.170 CHT PLA OFD
2000
* Sorted by study ranking.Abbreviations: AP = adult periodontitis; Bov coll = bovine collagen; BPBM = bovine porous bone mineral; Ca =calcium; CPF = coronally positioned flaps; DFDBA = demineralized freeze-dried bone allograft; EMD = enamelmatrix proteins; ePTFE = expanded polytetrafluoroethylene; HA = hydroxyapatite; NFGT = newly-formedgranulation tissue; OFD = open flap debridement; PLA = polylactic acid; PLA/PGA = polylactic/polyglycolicacid; PLA 910 = polyglactin 910; Por coll = porcine collagen; RPP = rapidly progressive periodontitis; TET =tetracycline; TR = titanium-reinforced.
Table 5.
Furcation-Defect Studies that Provided Standard Deviation or Error Values*
FurcationIntervention
Reference Design Class Test Control
Bouchard et al.171 1997 RCT, parallel II PLA/PGA ePTFE
Lekovic et al.172 1989 RCT, split-mouth II ePTFE OFDMetzler et al.173 1991 RCT, split-mouth II ePTFE OFD
Vest et al.174 1999 RCT II PLA + DFDBA + antibiotic regimen PLA + DFDBAWang et al.175 1994 RCT, split-mouth II Bov coll OFD
Anderegg et al.176 1991 RCT, split-mouth II ePTFE + DFDBA ePTFEBlumenthal177 1993 RCT II Bov coll ePTFE
dos Anjos et al.178 1998 RCT, split-mouth II Cellulose ePTFEFlanary et al.179 1991 RCT, split-mouth II Por coll OFD
Lekovic et al.180 1991 RCT, split-mouth II Periosteal graft as GTR OFDMachtei et al.181 1993 RCT, split-mouth II ePTFE + TET root condition ePTFE
Avera et al.182 1998 RCT, split-mouth II Periosteal membrane as GTR CRFAvera et al.182 1998 RCT, split-mouth II ePTFE OFD
Black et al.183 1994 RCT, split-mouth II Bov coll ePTFEBouchard et al.184 1993 RCT, split-mouth II ePTFE + citric acid CTG + citric acid
Caffesse et al.4 1990 RCT II ePTFE OFDDe Leonardis et al.185 1999 RCT, split-mouth II PLA + DFDBA PLA
8011.qxd 12/30/03 3:33 PM Page 274

<0.03). One study demon-strated a statistically significantnegative effect of the use ofDFDBA in addition to PLA (P =0.007).143 Six studies exam-ined PD reduction and meta-analysis of these studies alsodid not reveal any differencesbetween test and control inter-ventions (P = 0.468) (Fig. 9,page 283).135,136,143,152,153,161
Subgroup analysis of the typesof barriers used also failed toshow any differences.
Hard tissue changes. Themeta-analysis comparing bar-rier alone to OFD using re-entryassessment was based upon5 study arms from 4 studiesand 3 barrier types (Table 9,page 284).147,159,165,168 Onlyone of these studies favoredOFD.168 None of the studiesdemonstrated a loss or lack ofbone volume gain in the GTR
Ann Periodontol Murphy, Gunsolley
275
Table 4. (continued)
Intrabony-Defect Studies* that Provided Standard Deviation or Error Values
Study Duration Augmentation
N Study PopulationStudy
(months) Material Test Control Outcomes Ranking
12 10 10 CAL, re-entry 2B-3B6 HA 14 43 CAL, PD, REC 3B
24 10 10 CAL, PD, REC, x-rays 3B6 15 13 CAL, PD, REC, re-entry 3B
12 12 CAL, PD, REC, x-rays 3B12 23 21 CAL, PD, REC 3B
Table 5. (continued)
Furcation-Defect Studies* that Provided Standard Deviation or Error Values
Study Augmentation N sites
Study Duration (months) Material Test Control Outcomes Ranking
12 15 15 VPAL, VPD, HPD, REC 1B
6 12 12 VPAL, VPD, VOPA, HOPA, REC 1B6 17 17 VPAL, VPD, VOPA, HOPA, REC 1B
9 DFDBA 12 12 VPAL, VPD, HPD, VOPA, HOPA, REC 1B12 12 12 VPAL, VPD, VOPA, HOPA, REC 1B
6 DFDBA 15 15 VPAL, VPD, VOPA, HOPA, REC 1B-2B12 VPAL, VPD, VOPA, HOPA, REC 1B-2B
6 15 15 VPAL, VPD, VOPA, HOPA, REC 1B-2B6 19 19 VPAL, VPD, VOPA, HOPA, REC 1B-2B
6 15 15 VPAL, VPD, VOPA, HOPA, REC 1B-2B12 18 18 VPAL, HPAL, VPD 1B-2B
6 14 14 VPAL, VPD, VOPA, HOPA, REC 2B9 8 8 VPAL, VPD, VOPA, HOPA, REC 2B
6 13 13 VPAL, VPD, HPD, REC 2B12 12 12 VPAL, VPD, HPD, VOPA, HOPA 2B
12 9 4 VPAL, VPD 2B12 DFDBA 12 12 VPAL, VPD, HPD, REC 2B(continued)
8011.qxd 12/30/03 3:33 PM Page 275

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
276
group, while one study revealed a lack of bone volumegain in the OFD control group.165 There is a lack ofstandardization among studies examining the changein bone levels using a radiological assessment. Therewas only one study included in this systematic reviewthat demonstrated a difference in gain of bone heightof 0.90 mm, favoring GTR over OFD.157
Furcation StudiesBarrier versus open flap debridement therapy. Con-sidering all barrier types, meta-analysis of includedstudies demonstrated that GTR procedures resulted ina greater gain in vertical probing attachment (VPAL)when compared to OFD controls (Fig. 10, page 285;Tables 11, page 285; and 15, page 289) at a signifi-cance level of P <0.0001. Heterogeneity was significant(P <0.001). However, when the 2 most efficacious stud-ies were removed,182,189 the heterogeneity wasremoved and the treatment effect remained significant.Eleven studies using ePTFE barriers demonstrated adifference between test and control interventions ofweighted mean gains in VPAL of 1.39 ± 0.36 mm (P<0.0001). The single study evaluating a polymeric bar-rier115 demonstrated a gain in VPAL of 2.50 ± 0.85mm. Collagen barriers demonstrated a marginal gainof 0.10 ± 0.60 mm.
Sensitivity analysis on the effect of furcation loca-tion (maxillary versus mandibular; proximal versusfacial or lingual) failed to show a difference between
groupings. However, 2 studies that contributed 4 armsof data,120,121 contained data subsets regarding theeffect of furcation location. These studies included adiagnosis of the horizontal component of the furcationnot preoperatively, but rather after surgical debride-ment. Therefore, inclusion of these studies must bereviewed with caution. When these same studies andothers with modified standard deviation values wereexcluded from the analysis, a similar efficacy was dis-played comparing GTR to OFD.
A meta-analysis examining the outcome variable ofvertical probing depth reduction (VPD) demonstratedthat GTR results in greater VPD reduction as comparedto OFD at a significance level of P <0.0001. The hetero-geneity was significant <0.05 for the ePTFE and com-bined groupings. For the ePTFE group, when the mostefficacious study was removed from analysis,182 theheterogeneity was nonsignificant, while the effectremain significant. However, for the combined group-ing, heterogeneity remained due to the strongly posi-tive influence of polymeric barrier study115 (Fig. 11,page 286; Tables 12, page 286; and 15, page 289).Studies evaluating the gain in VOPA with barriers ascompared with OFD are summarized in Table 13 (page287). Collagen barrier usage usually resulted in greatergains in VOPA. However, statistical analysis was notperformed to confirm this trend.
A meta-analysis comparing GTR to OFD for the re-entry outcome variable horizontal open probing attach-
Table 5. (continued)
Furcation-Defect Studies* that Provided Standard Deviation or Error Values
FurcationIntervention
Reference Design Class Test Control
Lekovic et al.186 1990 RCT II ePTFE + porous HA ePTFELuepke et al.187 1997 RCT, split-mouth II PLA + DFDBA PLA
Parashis & Mitsis188 1993 RCT, split-mouth II ePTFE + TET ePTFEPontoriero et al.189 1988 RCT, split-mouth II ePTFE OFD
Scott et al.190 1997 RCT, split-mouth II DLB + DFDBA ePTFE + DFDBASimonpietri-C et al.191 2000 RCT, split-mouth II Cellulose + anorganic bovine bone Cellulose
Andersson et al.192 1994 RCT, split-mouth II ePTFE CPFEickholz et al.167 1998 RCT, split-mouth III PLA 910 ePTFE
Eickholz et al.167 1998 RCT, split-mouth II PLA 910 ePTFEGarrett et al.193 1994 CHT III ePTFE + DFDBA DFDBA + CPF
Yamaoka et al.194 1996 RCT, split-mouth II Demineralized ilium cortical strip ePTFE
* Sorted by study ranking.Abbreviations: Bov coll = bovine collagen; CTG = connective tissue graft; CPF = coronally positioned graft; DLB = demineralized laminar bone; ePTFE =expanded polytetrafluoroethylene; HA = hydroxyapatite; OFD = open flap debridement; PLA = polylactic acid; PLA 910 = polyglactin 910; Por coll = porcinecollagen; TET = tetracycline.
8011.qxd 12/30/03 3:33 PM Page 276

Ann Periodontol Murphy, Gunsolley
277
ment level gain (HOPA) was examined and found to besignificant in favor of GTR when all barrier types wereconsidered collectively (P <0.01) (Fig. 12, page 287;Tables 14, page 288; and 15, page 289). However, the
heterogeneity was highly significant (P <0.0001) for thecombined, ePTFE, and other groupings. The strength ofthis heterogeneity suggests that these studies shouldnot be combined for meta-analysis. The amount of post-
Table 5. (continued)
Furcation-Defect Studies* that Provided Standard Deviation or Error Values
Study Augmentation N sites
Study Duration (months) Material Test Control Outcomes Ranking
6 Porous HA 15 15 VPAL, VPD, VOPA, HOPA, REC 2B6 DFDBA 15 15 VPAL, VPD, HPD, VOPA, HOPA, REC 2B
6 9 9 VPAL, HPAL, VPD 2B6 VPAL, HOPA 2B
6 DFDBA 12 12 VPAL, VOPA, HOPA, REC 2B6 Anorganic 15 15 VPAL, VPD, VOPA, HOPA, REC 2B
bovine bone
12 9 9 VPAL, REC 2B-3B24 5 5 VPAL, VPD 3B
24 9 9 VPAL, VPD 3B12 DFDBA 14 12 VPAL, VOPA 3B
12 15 15 VPAL, VPD, HPD, VOPA, HOPA, REC 3B
Figure 2.Meta-analysis of intrabony-defect studies examining open flap debridement versus GTR with barrier, using CAL gain as an outcome variable.Abbreviations: Bov coll = bovine collagen; ePTFE = expanded polytetrafluoroethylene; Hum coll = human collagen; PLA = polylactic acid; PLA/PGA =polylactic/ polyglycolic acid;TR = titanium-reinforced.
8011.qxd 12/30/03 3:33 PM Page 277

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
treatment recession induced by the use of the physicalbarrier was also not significant when compared to OFDcontrols (Fig. 13, page 289).
ePTFE versus bioabsorbable barriers. Examiningthe outcome variables of VPAL and VPD, 8 study armsfrom 7 studies directly compared the use of ePTFE toa bioabsorbable barrier in the treatment of furcationdefects.116,117,167,171,177,178,183 When examining the
combined and polymeric barrier groupings, a statisticaldifference in favor of bioabsorbable barrier types overePTFE barriers could be detected (Figs. 14, page 289;and 15, page 290; Table 17, page 290) for VPAL out-come measures (P = 0.004 and P = 0.018, respec-tively), but not for VPD (P = 0.152). Only 2 stud-ies177,178 compared ePTFE versus bioabsorbablebarrier types while examining the re-entry outcome
278
Table 6.
Intrabony-Defect Studies* that Provided Standard Deviation or Error Values and that UsedCAL as an Outcome Variable when Comparing Membrane Only to OFD
Test Control
N Sites Outcome Outcome Outcome Outcome Difference Difference Reference Treated Intervention (mm) SD (mm) Intervention (mm) SD (mm) (mm) SD (mm)
CollagenChung et al.165 10 Bov coll 0.56 0.56 OFD −0.71 0.90 1.27 0.73
1990Blumenthal & 15 Bov coll 1.17 0.38 OFD 0.75 0.76 0.42 0.40
Steinberg148 1990
ePTFECortellini et al.133 12 ePTFE 5.20 1.40 OFD 2.30 0.80 2.90 1.10
1996Kim et al.138 19 ePTFE 4.00 2.10 OFD 2.00 1.70 2.00 1.90
1996Tonetti et al.142 15 ePTFE 4.10 1.90 OFD 2.50 0.80 1.60 1.35
1996Zybutz et al.147 2000 14 ePTFE 2.40 0.80 OFD 1.80 2.20 0.60 1.50Kiliç et al.157 1997 10 ePTFE 3.72 1.96 OFD 2.10 2.02 1.62 1.99Nygaard-Østby 15 ePTFE 2.40 2.00 OFD 2.20 1.20 0.20 1.60
et al.168 1996Cortellini et al.132 15 ePTFE-TR 5.30 2.20 OFD 2.50 0.80 2.80 1.50
1995Tonetti et al.142 1996 15 ePTFE-TR 5.30 2.20 OFD 2.50 0.80 2.80 1.50
PolymersRatka-Kruger et al.170 23 PLA 3.13 2.34 OFD 3.33 2.70 −0.20 2.52
2000Cortellini et al.131 23 PLA 3.00 1.70 OFD 1.60 1.80 1.40 1.75
1998Zybutz et al.147 2000 15 PLA 2.40 1.90 OFD 1.30 1.90 1.10 1.90Mayfield et al.159 10 PLA 1.50 1.90 OFD 1.30 1.70 0.20 1.80
1998Cortellini et al.134 55 PLA 3.50 2.10 OFD 2.60 1.80 0.90 1.95
2001Cortellini et al.133 12 PLA/PGA 4.60 1.20 OFD 2.30 0.80 2.30 1.00
1996Sculean et al.140 2001 14 PLA/PGA 3.10 1.50 OFD 1.70 1.10 1.40 1.30Bratthall et al.114 11 PLA/PGA 2.00 0.20 OFD 1.90 0.20 0.10 0.20
1998Joly et al.137 2002 10 PLA/PGA 2.37 0.37 OFD 1.65 0.35 0.72 0.36Tonetti et al.141 1998 69 PLA/PGA 3.04 1.64 OFD 2.18 1.46 0.86 1.55
* Sorted by test intervention.Abbreviations: Bov coll = bovine collagen; ePTFE = expanded polytetrafluoroethylene; OFD = open flap debridement; PLA = polylactic acid; PLA/PGA =polylactic/polyglycolic acid; TR = titanium-reinforced.
8011.qxd 12/30/03 3:33 PM Page 278

Ann Periodontol Murphy, Gunsolley
variable HOPA. Insufficient data were available for com-parisons regarding this outcome variable.
Barrier versus barrier plus augmentation material.Using the outcome variable of VPAL, 6 studies exam-ined the effect of the addition of an augmenta-tion material under the physical barrier (Fig. 16, page291 and Table 16, page 290).126,176,185-187,191 Collec-tively reviewing all barriers, VPAL was significantlyenhanced by the addition of a particulate bone graft (P= 0.039). The heterogeneity was not significant. As asubgroup, ePTFE plus a particulate graft resulted in asignificantly greater gain in VPAL as compared toePTFE alone (P <0.05). Polymeric or cellulose barriertreatments were not enhanced by the use of a graft.VPD reduction was also enhanced by the addition of aparticulate graft (P = 0.004) when all barriers were col-lectively reviewed (Fig. 17, page 291). Heterogeneitywas not significant. Again, the ePTFE grouping demon-strated a significant advantage (P <0.05).
Meta-analysis of the re-entry outcome variableHOPA demonstrated an advantage to the use ofaugmentation material in addition to the GTR barrier(Fig. 18, page 291) (P <0.05), but the highly signifi-cant heterogeneity (P <0.0001) suggests that thesestudies should not be combined for meta-analysis.
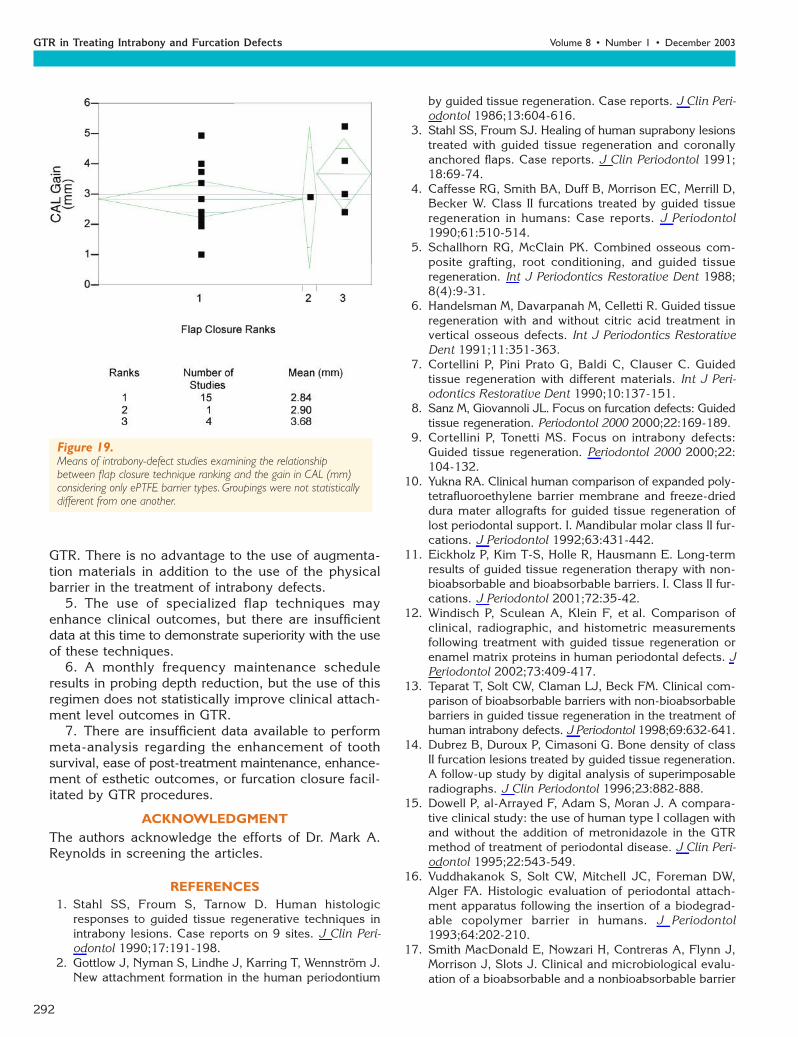
Possible Prognostic FactorsFlap closure technique ranking. Most reviewed studiesutilized a “standard” flap closure technique. Regressionanalysis examined the differences among groups sortedby flap closure ranking. Examining intrabony defectsand considering all barrier types, no significant differ-
ences between the rankings could be detected. However,when considering only ePTFE barriers in intrabony-defect studies, the mean gain in CAL utilizing a spe-cialized flap closure technique (Grade 3) was 3.76 mmas compared to 2.90 mm and 2.84 mm for Grades 2and 1, respectively. But these differences were not sta-tistically different (Fig. 19, page 292).
Flap closure technique Grade 3 was not used forany of the furcation-defect studies examined. Withthe exception of horizontal probing depth reduction(HPD), regression analysis of furcation studies failed todetect a difference in any outcome variable. HPD reduc-tion was enhanced when a passively adapted, coronallyrepositioned flap technique (Grade 2) was employed(Fig. 20, page 293). HPD for Grade 1 was 1.38 ± 0.14(SE) mm and 2.71 ± 0.22 (SE) mm for Grade 2. Thisdifference was not translated to other clinical outcomemeasures with statistical significance.
Frequency of postoperative recall care frequency.Studies that utilized a more frequent recall interval,especially in the time period after 3 months, showed atendency for greater gains in attachment levels (CAL,VPAL, HPAL, HOPA). However, regression analysis uti-lizing the recall care ranking failed to detect a statisti-cal difference between these groups for all outcomevariables with the exception of PD reduction in intra-bony-defect studies (Fig. 21, page 293). PD reductionwas enhanced with a Grade 3 recall ranking, resultingin a PD reduction of 4.97 mm, as compared to 3.73mm for Grade 2 and 3.52 mm for Grade 1 (P = 0.004).
Timing of barrier removal. Accurate documentationof the time of barrier removal for non-absorbable bar-
279
Figure 3.Meta-analysis of intrabony-defect studies examining open flap debridement versus GTR with barrier, using PD reduction as an outcome variable.Abbreviations: Bov coll = bovine collagen; ePTFE = expanded polytetrafluoroethylene; Hum coll = human collagen; PLA = polylactic acid; PLA/PGA =polylactic/polyglycolic acid;TR = titanium-reinforced.
8011.qxd 12/30/03 3:33 PM Page 279

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
riers was difficult as most studies described a range oftimes. The most commonly used time range was 4 to6 weeks. Therefore, differences in the effect of barrierremoval at the 4- and 6-week time intervals could notbe discerned from this dataset. Only 2 studies allowedthe barriers to remain for 8 weeks.172,188 These fur-cation defect studies reported an enhancement in VPAL
gain as compared with other furcation studies, butwithout any statistical significance.
Smoking. Eighteen studies provided some des-cription of the number of smokers in the test andcontrol populations. Comparisons between smokerand non-smoker groups were not possible as no stud-ies insured an even distribution of these populations
280
Table 7.
Intrabony-Defect Studies* that Provided Standard Deviation or Error Values and that UsedPD as an Outcome Variable when Comparing Membrane only to OFD
Test Control
N Sites Outcome Outcome Outcome Outcome Difference Difference Reference Treated Intervention (mm) SD (mm) Intervention (mm) SD (mm) (mm) SD (mm)
ePTFECortellini et al.133 12 ePTFE 5.90 1.00 OFD 4.30 1.40 1.60 1.20
1996Kim et al.138 19 ePTFE 4.80 1.80 OFD 3.30 1.60 1.50 1.70
1996Tonetti et al.142 15 ePTFE 5.50 2.60 OFD 4.60 1.20 0.90 1.90
1996Zybutz et al.147 14 ePTFE 3.10 1.20 OFD 2.50 1.90 0.60 1.55
2000Kiliç et al.157 10 ePTFE 5.83 2.84 OFD 3.17 0.98 2.66 1.91
1997Nygaard-Østby 15 ePTFE 3.80 1.20 OFD 2.90 1.10 0.90 1.15
et al.168 1996Cortellini 15 ePTFE-TR 6.30 1.40 OFD 4.60 1.30 1.70 1.35
et al.132 1995Tonetti et al.142 15 ePTFE-TR 6.30 2.50 OFD 4.60 1.20 1.70 1.85
1996
PolymersRatka-Kruger 23 PLA 3.71 1.92 OFD 3.66 2.67 0.05 2.30
et al.170 2000Cortellini et al.131 23 PLA 4.30 2.30 OFD 3.00 1.50 1.30 1.90
1998Zybutz et al.147 15 PLA 3.30 2.10 OFD 2.20 1.70 1.10 1.90
2000Mayfield et al.159 10 PLA 2.90 1.80 OFD 2.50 1.90 0.40 1.85
1998Cortellini et al.134 55 PLA 4.40 2.40 OFD 3.60 2.10 0.80 2.25
2001Tonetti et al.141 69 PLA/PGA 4.03 1.81 OFD 3.09 1.67 0.94 1.74
1998Cortellini et al.133 12 PLA/PGA 6.60 1.60 OFD 4.30 1.40 2.30 1.50
1996Sculean et al.140 14 PLA/PGA 4.20 1.90 OFD 3.70 1.40 0.50 1.65
2001Bratthall et al.114 11 PLA/PGA 3.60 0.20 OFD 2.90 0.20 0.70 0.20
1998Joly et al.137 10 PLA/PGA 2.64 0.42 OFD 1.84 0.36 0.80 0.39
2002
* Sorted by test intervention.Abbreviations: ePTFE = expanded polytetrafluoroethylene; OFD = open flap debridement; PLA = polylactic acid; PLA/PGA = polylactic/polyglycolic acid; TR =titanium-reinforced.
8011.qxd 12/30/03 3:33 PM Page 280

Ann Periodontol Murphy, Gunsolley
among the test and control interventions. Of thesestudies, most found a negative association betweensmoking and clinical outcomes. The statistical sig-nificance is unknown. Only 5 studies excludedsmoker patients.
Other outcomes. Patient-centered outcomes, suchas surgical complications and esthetically unacceptableresults, were not consistently reported. Only 13 studies
made mention of the incidence of postoperative abscessformation or some description of patient discomfort. Ofthe 13 studies examining the incidence of abscess for-mation, only 4 studies described any occurrence ratefor control groups. Likewise, only 4 described occur-rences for the test groups during the healing period.When reported, the incidence of abscess formation was15% or less.
281
Table 8.
Intrabony-Defect Studies* that Provided Standard Deviation or Error Values and that UseREC as an Outcome Variable When Comparing Membrane Only to OFD
Test Control
N Sites Outcome Outcome Outcome Outcome Difference Difference Reference Treated Intervention (mm) SD (mm) Intervention (mm) SD (mm) (mm) SD (mm)
CollagenCamargo et al.149 22 Bov coll + 1.11 1.40 OFD 1.36 1.40 −0.25 1.40
2000 BPBM
ePTFECortellini et al.133 12 ePTFE 1.20 1.30 OFD 2.00 1.60 −0.80 1.45
1996Kim et al.138 19 ePTFE 0.90 1.20 OFD 1.20 1.40 −0.30 1.30
1996Zybutz et al.147 14 ePTFE 0.80 0.90 OFD 0.00 1.30 0.80 1.10
2000Kiliç et al.157 10 ePTFE 2.12 0.86 OFD 1.05 0.55 1.07 0.71
1997Nygaard-Østby 15 ePTFE 1.70 1.50 OFD 0.70 0.90 1.00 1.20
et al.168 1996Cortellini et al.132 15 ePTFE-TR 0.90 1.60 OFD 2.10 1.60 −1.20 1.60
1995
PolymersRatka-Kruger 23 PLA 0.71 1.25 OFD 0.33 1.07 0.38 1.16
et al.170 2000Zybutz et al.147 15 PLA 0.70 0.90 OFD 0.00 1.10 0.70 1.00
2000Mayfield et al.159 10 PLA 1.40 0.90 OFD 1.20 1.00 0.20 0.95
1998Cortellini et al.134 55 PLA 0.90 1.00 OFD 0.90 1.30 0.00 1.15
2001Cortellini et al.133 12 PLA/PGA 2.00 1.40 OFD 2.00 1.60 0.00 1.50
1996Sculean et al.140 14 PLA/PGA 1.10 1.40 OFD 1.70 1.10 −0.60 1.25
2001Bratthall et al.114 11 PLA/PGA 2.30 0.20 OFD 1.60 0.20 0.70 0.20
1998Tonetti et al.141 69 PLA/PGA 1.00 1.40 OFD 1.01 1.18 −0.01 1.29
1998Joly et al.137 10 PLA/PGA 1.60 0.21 OFD 0.67 0.09 0.93 0.15
2002
* Sorted by test intervention.Abbreviations: Bov coll = bovine collagen; BPBM = bovine porous bone mineral; ePTFE = expanded polytetrafluoroethylene; OFD = open flap debridement;PLA = polylactic acid; PLA/PGA = polylactic/polyglycolic acid; TR = titanium-reinforced.
8011.qxd 12/30/03 3:33 PM Page 281

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
Long-term patient-centered outcomes, such as toothloss and ease of maintenance, were not reported in thestudies selected for inclusion in the current systematicreview.
DISCUSSIONThe purpose of this systematic review (SR) was toanswer the focused question, “In patients with peri-odontal osseous defects, what is the effect of physical
282
Figure 4.Meta-analysis of intrabony-defect studies examining open flap debridement versus GTR with barrier, using increase in gingival REC as an outcomevariable.Abbreviations: ePTFE = expanded polytetrafluoroethylene; PLA = polylactic acid.
Figure 5.Meta-analysis of intrabony-defect studies that compare ePTFE barrier to a bioabsorbable barrier, using CAL gain as an outcome variable.Abbreviations: ePTFE = expanded polytetrafluoroethylene; PLA = polylactic acid; PLA 910 = polyglactin 910.
Figure 6.Meta-analysis of intrabony-defect studies that compare ePTFE barrier to a bioabsorbable barrier, using PD reduction as an outcome variable.Abbreviations: ePTFE = expanded polytetrafluoroethylene; PLA = polylactic acid; PLA 910 = polyglactin 910.
8011.qxd 12/30/03 3:33 PM Page 282

Ann Periodontol Murphy, Gunsolley
barriers compared with surgical controls on clinical,radiographic, adverse and patient-centered outcomes?”This systematic review also aimed to expand upon 2previously systematic reviews of GTR as a regenerativetherapy.196,197 These reviews limited their scope toRCTs of intrabony defects or furcation defects, respect-ively. Our review aimed to examine GTR studies withthese defect types separately and collectively, in an
attempt to better understand some of the heterogene-ity described in these earlier systematic reviews.
The current SR also differed in that the reviewedstudies were not limited to RCTs. Despite this lack oflimitation, only a few additional cohort studies satis-fied the inclusion criteria. Our SR also included stud-ies of 6 months or greater. Needleman et al.196 did notinclude studies of less than one year duration. When
283
Figure 7.Meta-analysis of intrabony-defect studies that compare an expanded polytetrafluoroethlylene (ePTFE) barrier to a bioabsorbable barrier, using RECincrease as an outcome variable.
Figure 8.Meta-analysis of intrabony-defect studies directly comparing the use of a barrier alone with the use of a barrier plus augmentation, using CAL gain asan outcome variable.Abbreviations: BOV coll = bovine collagen; BPBM = bovine porous bone mineral; DFDBA = demineralized freeze-dried boneallograft; ePTFE = expanded polytetrafluoroethylene; HA = hydroxyapatite; PLA = polylactic acid.
Figure 9.Meta-analysis of intrabony-defect studies directly comparing the use of a barrier alone with the use of a barrier plus augmentation, using PD reductionas an outcome variable.Abbreviations: Bov coll = bovine collagen; BPBM = bovine porous bone mineral; DFDBA = demineralized freeze-dried boneallograft; ePTFE = expanded polytetrafluoroethylene; HA = hydroxyapatite; PLA = polylactic acid.
8011.qxd 12/30/03 3:33 PM Page 283

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
appropriate, we also included studies that combinedaugmentation materials and barriers in the GTRprocess. While acknowledging that while clinical attach-ment levels (CAL or VPAL) are surrogate variables,but considered the most reliable clinical measure ofregeneration, this SR examined 10 primary outcomemeasures, including attachment levels in both verti-cal and horizontal directions, probing depths, recession,and re-entry measurements. While this expansion ofprimary outcome measures increased the complexityof the analysis, our meta-analysis demonstrated thatnot all outcome variables followed the trends outlinedby attachment level gains.
Incomplete data representation and description ofmethods prevented the inclusion of many studies.
Most studies failed to describethe methodology of patientselection, randomization, ther-apist and examiner maskingand allocation concealment.Most significant of these prob-lems was the failure to describestandard deviation (SD) orstandard error values (SE).Without these values, meta-analysis is not possible. Jepsenet al.197 estimated these valuesfrom split-mouth studies de-rived from the literature. Thisuse of estimated values of stan-
dard deviations from unrelated studies may or maynot be valid. Our review also included such studiesthat did not present standard deviations or standarderror values, and their possible influence on the ana-lysis was noted.
Meta-analysis of the studies examining the effect ofGTR compared to OFD procedures, using the outcomevariable CAL and VPAL, demonstrated that GTR wasstrongly favored in the treatment of both intrabony andfurcation defects (P <0.0001). This finding was morerobust than previously reported and is probably relatedto the greater number of studies included for analysisin this SR. When PD or VPD were considered, similarrobust findings favoring GTR were demonstrated.HOPA, a horizontal re-entry outcome measure, was also
284
Table 10.
Summary of the Effect of the Use of a Physical Barrier asCompared with OFD in the Treatment of Intrabony Defects*
Barrier CAL SD PD SD
Collagen 0.95 ±0.47 1.06 ±0.37
Polymer 0.92 ±0.18 0.89 ±0.14
Expanded 1.61 ±0.25 1.41 ±0.20polytetrafluoroethylene
* Differences between CAL gain and PD reduction between barrier and OFD control (mm) [mean ± standarddeviation].
Table 9.
Intrabony-Defect Studies that Provided Standard Deviation or Error Values and that UsedRe-entry as an Outcome Variable when Comparing Membrane Only to OFD*
Test Control
N Sites Outcome Outcome Outcome Outcome Difference Difference Reference Treated Intervention (mm) SD (mm) Intervention (mm) SD (mm) (mm) SD (mm)
CollagenChung et al.165 10 Bov coll 1.16 0.94 OFD 0 0.78 1.16 0.86
1990
ePTFEZybutz et al.147 14 ePTFE 2.7 2.3 OFD 2.4 3 0.30 2.65
2000Nygaard-Østby 15 ePTFE 2 2 OFD 2.4 0.9 −0.40 1.45
et al.168 1996
PolymersZybutz et al.147 15 PLA 2.3 3 OFD 1.5 1.6 0.80 2.30
2000Mayfield et al.159 10 PLA 0.7 2.1 OFD 0.5 1.5 0.20 1.80
1998
* Studies expressing only a percent of defect fill were excluded.Abbreviations: Bov coll = bovine collagen; ePTFE = expanded polytetrafluoroethylene; OFD = open flap debridement; PLA = polylactic acid.
8011.qxd 12/30/03 3:33 PM Page 284

Ann Periodontol Murphy, Gunsolley
285
Figure 10.Meta-analysis of furcation-defect studies examining open flap debridement (OFD) versus GTR with barrier, using VPAL gain as an outcome variable.ePTFE = expanded polytetrafluoroethylene; Mand = mandibula; Max = maxilla.
Table 11.
Furcation-Defect Studies* that Provided Standard Deviation or Error Values and that UsedVPAL as an Outcome Variable when Comparing Membrane Only to OFD
Test Control
N Sites Outcome Outcome Outcome Difference DifferenceReference Treated Intervention (mm) SD (mm) Intervention (mm) SD (mm) (mm) SD (mm)
CollagenFlanary et al.179 19 Por coll 1.50 1.10 OFD 0.80 1.20 0.70 1.15
1991Wang et al.175 12 Bov coll 1.67 0.76 OFD 0.67 2.14 1.00 1.45
1994Lekovic et al.180 15 Periosteal graft 2.40 1.35 OFD −0.70 1.16 3.10 1.26
1991
ePTFELekovic et al.172 12 ePTFE 2.86 1.80 OFD −0.12 2.84 2.98 2.32
1989Metzler et al.173 17 ePTFE 1.00 0.90 OFD 0.20 0.60 0.80 0.75
1991Avera et al.182 8 ePTFE 1.50 0.46 OFD 0.13 0.48 1.37 0.47
1998Caffesse et al.4 9 ePTFE 1.80 1.30 OFD 0.60 1.90 1.20 1.60
1990Pontoriero 21 ePTFE 3.50 1.50 OFD 0.90 1.00 2.60 1.25
et al.189 1988Andersson 9 ePTFE 0.70 1.03 OFD 0.40 0.82 0.30 0.93
et al.192 1994
* Sorted by test intervention.Abbreviations: Bov coll = bovine collagen; ePTFE = expanded polytetrafluoroethylene; OFD = open flap debridement; Por coll = porcine collagen.
significantly greater for GTR as compared to OFDprocedures (P = 0.001), but the heterogeneity wassignificant.
The inclusion of a greater number of studies alsofacilitated subgroup or sensitivity analysis regarding thepossible effect of the type of barrier utilized. For intra-
8011.qxd 12/30/03 3:33 PM Page 285

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
bony defect studies, both ePTFE and polymeric barriersperformed with similar efficacy when compared toOFD. In intrabony studies that directly comparedePTFE to a bioabsorbable barrier, CAL was enhancedwith ePTFE, but not with statistical significance.
In the treatment of furcation defects using an OFDcontrol, there are relatively few studies which examined
the use of polymeric barriers alone. More furcation stud-ies directly compared ePTFE to a polymeric barrier.This is probably related to the fact that ePTFE becamethe perceived “gold standard” in regeneration, not OFD,due to the number of studies examining this material.When ePTFE is compared to a polymeric barrier in thetreatment of furcation defects, there was no significant
286
Figure 11.Meta-analysis of furcation-defect studies examining open flap debridement (OFD) versus GTR with barrier, using VPD reduction as an outcomevariable. ePTFE = expanded polytetrafluoroethylene; Mand = mandibula; Max = maxilla.
Table 12.
Furcation-Defect Studies* that Provided Standard Deviation or Error Values and that UsedVPD as an Outcome Variable When Comparing Membrane Only to OFD
Test Control
N Sites Outcome Outcome Outcome Difference Difference Reference Treated Intervention (mm) SD (mm) Intervention (mm) SD (mm) (mm) SD (mm)
CollagenLekovic et al.180 15 Periosteal 4.30 0.92 OFD 1.60 1.12 2.70 1.02
1991 graftLekovic et al.195 14 Periosteal 3.66 0.89 OFD 3.89 1.31 −0.23 1.10
1998 graftFlanary et al.179 19 Por coll 2.10 1.10 OFD 1.20 1.10 0.90 1.10
1991Wang et al.175 12 Bov coll 2.84 1.42 OFD 1.92 2.32 0.92 1.87
1994
ePTFELekovic et al.172 12 ePTFE 4.09 2.94 OFD 1.14 2.77 2.95 2.86
1989Metzler et al.173 17 ePTFE 1.70 0.80 OFD 0.90 0.80 0.80 0.80
1991Avera et al.182 8 ePTFE 2.88 0.48 OFD 1.38 0.65 1.50 0.57
1998Caffesse et al.4 9 ePTFE 2.80 1.00 OFD 1.60 0.90 1.20 0.95
1990
* Sorted by test intervention.Abbreviations: Bov coll = bovine collagen; ePTFE = expanded polytetrafluoroethylene; OFD = open flap debridement; Por coll = porcine collagen.
8011.qxd 12/30/03 3:33 PM Page 286

Ann Periodontol Murphy, Gunsolley
difference between observed changes in VPAL or VPDoutcome measures. Not enough studies examined HOPAin this context. In summary, both ePTFE and polymericbarriers performed in similar manner when used alonein GTR in the treatment of intrabony or furcation defects.
When augmentation of the barrier with a particu-late graft was examined, a dichotomy was seen inthe behavior of intrabony and furcation defects. Aug-mentation procedures did not enhance CAL or PDoutcomes when used in the treatment of intrabony
defects. This is in contrast to furcation defects whereinaugmentation enhanced VPAL and VPD outcomes(P <0.05 and P <0.005). HOPA were similarly influ-enced, but with heterogeneity among the studies. Sincedifficulty in maintaining the space under the barrier ismore likely to be a problem in a non-contained fur-cation defect, an augmentation material might demon-strate an advantage in furcation defects as opposed tointrabony defects.70,198 Unfortunately, this assumptioncannot be proven without descriptions of the bony con-
287
Figure 12.Forest plot of furcation-defect studies examining open flap debridement (OFD) versus GTR with barrier, using HOPA gain as an outcome variable.ePTFE = expanded polytetrafluoroethylene; Mand = mandibula; Max = maxilla.
Table 13.
Furcation-Defect Studies* that Provided Standard Deviation or Error Values and that UsedVOPA as an Outcome Variable When Comparing Membrane Only to OFD
Test Control
N Sites Outcome Outcome Outcome Outcome Difference DifferenceReference Treated Intervention (mm) SD (mm) Intervention (mm) (mm) (mm) (mm)
CollegenLekovic et al.180 15 Periosteal graft 2.00 0.54 OFD −1.27 1.33 3.27 0.94
1991Lekovic et al.195 14 Periosteal 1.93 0.56 OFD 0.20 0.97 1.73 0.77
1998 membrane as GTRFlanary et al.179 19 Por coll 1.00 1.20 OFD 0.60 1.10 0.40 1.15
1991Wang et al.175 12 Bov coll 2.83 1.42 OFD 1.50 0.39 1.33 0.91
1994
ePTFELekovic et al.172 12 ePTFE 0.21 1.66 OFD 0.24 1.59 −0.03 1.63
1989Metzler et al.173 17 ePTFE 1.50 1.30 OFD 0.60 0.80 0.90 1.05
1991Avera et al.182 8 ePTFE 0.00 0.10 OFD −0.69 0.25 0.69 0.18
1998
* Sorted by test intervention.Abbreviations: Bov coll = bovine collagen; ePTFE = expanded polytetrafluoroethylene; OFD = open flap debridement; Por coll = porcine collagen.
8011.qxd 12/30/03 3:33 PM Page 287

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
288
figurations of the defect. Very few studies contained anydescription of the bony defect morphology. Future stud-ies should examine what defect morphologies would bemore likely to benefit from the use of an augmentationmaterial in addition to the barrier in GTR procedures.
The effect of furcation defect location was examinedby Jepsen et al.197 in their SR on GTR for the treatmentof furcation defects. Their SR utilized GTR furcation stud-ies that our SR excluded for data presentation problems.Unfortunately, some of these studies excluded in the cur-rent SR are some of the very few that examined the role
of furcation location on the regenerative outcome inGTR.92,95 Therefore, our SR cannot provide evidenceabout this possible relationship.
The group of Cortellini, Tonetti, and PiniPrato9,32,127,129,132-134,141 and Murphy50 have exam-ined the use specialized flap techniques that facilitateprimary closure over the barrier. The implied purposeof these procedures is to enhance the regenerative out-come and decrease the frequency of complications byreducing the development of a pseudopocket in thespace lateral to the barrier. The current SR attempted
Table 14.
Furcation-Defect Studies* that Provided Standard Deviation or Error Values and that UsedHOPA as an Outcome Variable
Test Control
N Sites Outcome Outcome Outcome Outcome Difference DifferenceReference Treated Intervention (mm) SD (mm) Intervention (mm) (mm) (mm) (mm)
Augmentation material + barrier versus barrierAnderegg et al.176 15 ePTFE + 2.40 1.50 ePTFE 1.00 0.80 1.40 1.15
1991 DFDBALekovic et al.186 15 ePTFE + 1.60 0.81 ePTFE 0.13 0.34 1.47 0.58
1990 porousHA
Simonpietri-C et al.191 15 Cellulose + 3.27 1.39 Cellulose 2.47 0.99 0.80 1.192000 anorganic
bovinebone
Luepke et al.187 15 PLA + 2.10 1.12 PLA 1.80 1.26 0.30 1.191997 DFDBA
Barrier versus ePTFEBlumenthal177 12 Bov coll 2.50 0.67 ePTFE 1.83 1.03 0.67 0.85
1993dos Anjos et al.178 15 Cellulose 2.90 1.00 ePTFE 2.90 1.10 0.00 1.05
1998
Barrier versus OFDWang et al.175 12 Bov coll 2.04 1.48 OFD 1.08 2.11 0.96 1.80
1994Flanary et al.179 19 Por coll 1.50 0.80 OFD 0.80 0.80 0.70 0.80
1991Lekovic et al.180 15 Periosteal 1.60 0.63 OFD −0.20 0.56 1.80 0.60
1991 graftLekovic et al.195 14 Periosteal 1.60 0.79 OFD 0.13 3.37 1.47 2.08
1998 graft
ePTFE versus OFDAvera et al.182 8 ePTFE 1.19 0.16 OFD −0.69 0.23 1.88 0.20
1998Lekovic et al.172 12 ePTFE 0.18 1.84 OFD 0.14 1.17 0.04 1.51
1989Metzler et al.173 17 ePTFE 0.90 0.40 OFD 0.30 0.60 0.60 0.50
1991
* Sorted by test intervention.Abbreviations: Bov coll = bovine collagen; DFDBA = demineralized freeze-dried bone allograft; ePTFE = expanded polytetrafluoroethylene; HA =hydroxyapatite; OFD = open flap debridement; PLA = polylactic acid; Por coll = porcine collagen.
8011.qxd 12/30/03 3:33 PM Page 288

to correlate the incidence of complicationswith prognostic variables, but was unableto do so because of lack of data. There-fore, evidence-based statements cannotbe made regarding use of these proce-dures and the incidence of complications.However, retrospective studies employingthese techniques in a microsurgical envi-ronment have claimed a greater than 90%rate of flap coverage over the barrier at6 weeks.50,128 It is believed that if the bar-rier remains covered during the healingperiod, the rate of complications will bedecreased.9 This SR did provide limitedevidence that specialized flap proceduresresult in an increase in mean attachmentlevel gain for intrabony defects, but this
Ann Periodontol Murphy, Gunsolley
289
Figure 13.Meta-analysis of furcation-defect studies examining open flap debridement (OFD) versus GTR with barrier, using REC change as an outcome variable.ePTFE = expanded polytetrafluoroethylene.
Figure 14.Meta-analysis of furcation-defect studies that compare an expanded polytetrafluoroethylene (ePTFE) barrier to a bioabsorbable barrier, using VPALgain as an outcome variable Abbreviation: Mand = mandibula.
Table 15.
Difference in Weighted Means of All Furcation-DefectStudies Evaluated Comparing a Physical Barrier toOFD Controls and Using VPAL, VPD, and HOPA asOutcome Measures*
Barrier VPAL SD VPD SD HOPA SD
Collagen 0.10 ±0.60 −0.04 ±0.52 0.96 ±0.91
Other 1.76 ±0.65 1.69 ±0.57 1.18 ±0.54
Polymeres 2.50 ±0.85 2.30 ±0.74 Insufficient data
Expanded 1.39 ±0.36 1.01 ±0.31 0.99 ±0.31polytetrafluoroethylene
* In mm (mean ± standard deviation; SD).
8011.qxd 12/30/03 3:33 PM Page 289

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
finding is not statistically significant. It is of interestthat this advantage was seen only when ePTFE barri-ers were used and not bioabsorbable barriers. Like-wise, passive adaptation and coronal repositioning of
290
Figure 15.Meta-analysis of furcation-defect studies that compare an expanded polytetrafluoroethylene (ePTFE) barrier to a bioabsorbable barrier, using VPDreduction as an outcome variable.
the gingival flap in furcation GTR proce-dures statistically enhanced HPD reduc-tion, but not other outcome variables. Asmore clinical trials make use of these tech-niques, a better understanding of the effectof flap management on regenerative out-comes can be gained.
Needleman et al.196 appropriately ques-tioned whether the inclusion of studies witha very frequent recall program skewedresults in favor of the regenerative proce-dure. Indeed, our SR demonstrated that aprotocol that utilized a monthly mainte-nance schedule for the duration of thestudy enhanced the PD reduction for intra-bony defects only. No other outcomeswere enhanced. Therefore, the frequencyof the recall schedule cannot fully explainsome of the heterogeneity identified in pre-vious systematic reviews.
Despite the robust findings favoringGTR over OFD, the variability in outcomesmeasures that are clinically relevant con-tinues to be a problem with GTR proce-dures. For example, data subsets onsmokers were not consistently availabledespite the fact that findings from such apopulation could significantly alter results.Well-designed studies insure that patientsand prognostic variables are evenly dis-tributed over both test and control inter-ventions.131 Unfortunately, these protocolconsiderations were not common in thestudies included for this review.
REVIEWER’S CONCLUSIONS1. In the treatment of intrabony defects, GTR proce-dures compared to OFD controls result in significantlymore favorable gains in CAL and PD reduction.
Table 16.
Difference in Weighted Means of All Furcation-DefectStudies Evaluated Comparing a Physical Barrier Controlto the Same Barrier with an Augmentation Material,Using VPAL, VPD, and HOPA as Outcome Measures
Barrier VPAL SD VPD SD HOPA SD
Other −0.20 ±0.50 0.20 ±0.22 0.80 ±0.61
Polymers 0.39 ±0.37 0.51 ±0.16 0.30 ±0.61
Expanded 1.10 ±0.31 0.66 ±0.14 1.20 ±0.38polytetrafluoroethylene
* In mm (mean ± standard deviation; SD).
Table 17.
Difference in Weighted Means of All Furcation-DefectStudies Evaluated Comparing the Use of an ExpandedPolytetrafluoroethylene Physical Barrier Controlto Another Barrier, Using VPAL, VPD, and HOPA asOutcome Measures*
Membrane VPAL SD VPD SD HOPA SD
Collagen 0.54 ±0.10 0.37 ±0.24 Insufficientdata
Other 0.30 ±0.13 0.40 ±0.32
Polymeres 0.39 ±0.04 0.14 ±0.10
* In mm (mean ± standard deviation; SD).
8011.qxd 12/30/03 3:33 PM Page 290

Ann Periodontol Murphy, Gunsolley
2. In the treatment of furcation defects, GTR pro-cedures compared to OFD controls result in signifi-cantly more favorable gains in VPAL, reductions inVPD, and improvements in HOPA measurements.
3. In the treatment of intrabony defects, meta-analy-sis did not show any statistically significant superiorresults among the barrier types evaluated. However,the type of barrier utilized might account for some of
the heterogeneity of the data. In the treatment of fur-cation defects, the type of barrier employed did affectthe surrogate variable of VPAL, since VPAL wasenhanced only with the use of ePTFE and polymericbarriers.
4. The use of augmentation materials in addition tothe physical barrier enhances the regenerative out-come in the treatment of furcation defects treated with
291
Figure 16.Meta-analysis of furcation-defect studies directly comparing the use of a barrier alone with the use of a barrier plus augmentation, using VPAL gain asan outcome variable.Abbreviations: DFDBA = demineralized freeze-dried bone allograft; ePTFE = expanded polytetrafluoroethylene; HA =hydroxyapatite; Mand = mandibula.
Figure 17.Meta-analysis of furcation-defect studies directly comparing the use of a barrier alone with the use of a barrier plus augmentation, using VPD reductionas an outcome variable. Abbreviations: DFDBA = demineralized freeze-dried bone allograft; ePTFE = expanded polytetrafluoroethylene;HA = hydroxyapatite; Mand = mandibula.
Figure 18.Meta-analysis of furcation-defect studies directly comparing the use of a barrier alone with the use of a barrier plus augmentation, using HOPAreduction as an outcome variable. Abbreviations: DFDBA = demineralized freeze-dried bone allograft; ePTFE = expanded polytetrafluoroethylene;HA = hydroxyapatite; Mand = mandibula.
8011.qxd 12/30/03 3:33 PM Page 291
GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
GTR. There is no advantage to the use of augmenta-tion materials in addition to the use of the physicalbarrier in the treatment of intrabony defects.
5. The use of specialized flap techniques mayenhance clinical outcomes, but there are insufficientdata at this time to demonstrate superiority with the useof these techniques.
6. A monthly frequency maintenance scheduleresults in probing depth reduction, but the use of thisregimen does not statistically improve clinical attach-ment level outcomes in GTR.
7. There are insufficient data available to performmeta-analysis regarding the enhancement of toothsurvival, ease of post-treatment maintenance, enhance-ment of esthetic outcomes, or furcation closure facil-itated by GTR procedures.
ACKNOWLEDGMENTThe authors acknowledge the efforts of Dr. Mark A.Reynolds in screening the articles.
REFERENCES1. Stahl SS, Froum S, Tarnow D. Human histologic
responses to guided tissue regenerative techniques inintrabony lesions. Case reports on 9 sites. J Clin Peri-odontol 1990;17:191-198.
2. Gottlow J, Nyman S, Lindhe J, Karring T, Wennström J.New attachment formation in the human periodontium
by guided tissue regeneration. Case reports. J Clin Peri-odontol 1986;13:604-616.
3. Stahl SS, Froum SJ. Healing of human suprabony lesionstreated with guided tissue regeneration and coronallyanchored flaps. Case reports. J Clin Periodontol 1991;18:69-74.
4. Caffesse RG, Smith BA, Duff B, Morrison EC, Merrill D,Becker W. Class II furcations treated by guided tissueregeneration in humans: Case reports. J Periodontol1990;61:510-514.
5. Schallhorn RG, McClain PK. Combined osseous com-posite grafting, root conditioning, and guided tissueregeneration. Int J Periodontics Restorative Dent 1988;8(4):9-31.
6. Handelsman M, Davarpanah M, Celletti R. Guided tissueregeneration with and without citric acid treatment invertical osseous defects. Int J Periodontics RestorativeDent 1991;11:351-363.
7. Cortellini P, Pini Prato G, Baldi C, Clauser C. Guidedtissue regeneration with different materials. Int J Peri-odontics Restorative Dent 1990;10:137-151.
8. Sanz M, Giovannoli JL. Focus on furcation defects: Guidedtissue regeneration. Periodontol 2000 2000;22:169-189.
9. Cortellini P, Tonetti MS. Focus on intrabony defects:Guided tissue regeneration. Periodontol 2000 2000;22:104-132.
10. Yukna RA. Clinical human comparison of expanded poly-tetrafluoroethylene barrier membrane and freeze-drieddura mater allografts for guided tissue regeneration oflost periodontal support. I. Mandibular molar class II fur-cations. J Periodontol 1992;63:431-442.
11. Eickholz P, Kim T-S, Holle R, Hausmann E. Long-termresults of guided tissue regeneration therapy with non-bioabsorbable and bioabsorbable barriers. I. Class II fur-cations. J Periodontol 2001;72:35-42.
12. Windisch P, Sculean A, Klein F, et al. Comparison ofclinical, radiographic, and histometric measurementsfollowing treatment with guided tissue regeneration orenamel matrix proteins in human periodontal defects. JPeriodontol 2002;73:409-417.
13. Teparat T, Solt CW, Claman LJ, Beck FM. Clinical com-parison of bioabsorbable barriers with non-bioabsorbablebarriers in guided tissue regeneration in the treatment ofhuman intrabony defects. J Periodontol 1998;69:632-641.
14. Dubrez B, Duroux P, Cimasoni G. Bone density of classII furcation lesions treated by guided tissue regeneration.A follow-up study by digital analysis of superimposableradiographs. J Clin Periodontol 1996;23:882-888.
15. Dowell P, al-Arrayed F, Adam S, Moran J. A compara-tive clinical study: the use of human type I collagen withand without the addition of metronidazole in the GTRmethod of treatment of periodontal disease. J Clin Peri-odontol 1995;22:543-549.
16. Vuddhakanok S, Solt CW, Mitchell JC, Foreman DW,Alger FA. Histologic evaluation of periodontal attach-ment apparatus following the insertion of a biodegrad-able copolymer barrier in humans. J Periodontol1993;64:202-210.
17. Smith MacDonald E, Nowzari H, Contreras A, Flynn J,Morrison J, Slots J. Clinical and microbiological evalu-ation of a bioabsorbable and a nonbioabsorbable barrier
292
Figure 19.Means of intrabony-defect studies examining the relationshipbetween flap closure technique ranking and the gain in CAL (mm)considering only ePTFE barrier types. Groupings were not statisticallydifferent from one another.
8011.qxd 12/30/03 3:33 PM Page 292

Ann Periodontol Murphy, Gunsolley
293
Figure 20.Regression analysis of furcation-defect studies examining the relationship between flap closure technique ranking and the reduction in horizontalprobing depth reduction HPD (mm). Group1 and 2 are statistically different from one another.
Figure 21.Regression analysis of intrabony-defect studies examining the relationship between postoperative care protocol ranking and the reduction in probingdepth reduction PD (mm). Group 3 is statistically different from groups 1 and 2.
8011.qxd 12/30/03 3:33 PM Page 293

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
membrane in the treatment of periodontal intraosseouslesions. J Periodontol 1998;69:445-453.
18. Wang H-L, MacNeil RL, Thomas C, Shyr Y, Syed S. Theeffect of an absorbable collagen membrane on the subgin-gival microflora. Periodontal Clin Investig 1997;19:27-35.
19. Chen Y-T, Wang H-L, Lopatin DE, O’Neal R, MacNeil RL.Bacterial adherence to guided tissue regeneration barriermembranes exposed to the oral environment. J Peri-odontol 1997;68:172-179.
20. De Sanctis M, Zucchelli G, Clauser C. Bacterial colo-nization of barrier material and periodontal regenera-tion. J Clin Periodontol 1996;23:1039-1046.
21. Mombelli A, Zappa U, Brägger U, Lang NP. Systemicantimicrobial treatment and guided tissue regeneration.Clinical and microbiological effects in furcation defects.J Clin Periodontol 1996;23:386-396.
22. Simion M, Trisi P, Maglione M, Piattelli A. Bacterialpenetration in vitro through GTAM membrane with andwithout topical chlorhexidine application. A light andscanning electron microscopic study. J Clin Periodontol1995;22:321-331.
23. Frandsen EVG, Sander L, Arnbjerg D, Theilade E. Effectof local metronidazole application on periodontal heal-ing following guided tissue regeneration. Microbiologicalfindings. J Periodontol 1994;65:921-928.
24. Nowzari H, Slots J. Microorganisms in polytetrafluo-roethylene barrier membranes for guided tissue regen-eration. J Clin Periodontol 1994;21:203-210.
25. Demolon IA, Persson GR, Moncla BJ, Johnson RH,Ammons WF. Effects of antibiotic treatment on clinicalconditions and bacterial growth with guided tissue regen-eration. J Periodontol 1993;64:609-616.
26. Tempro PJ, Nalbandian J. Colonization of retrieved poly-tetrafluoroethylene membranes: Morphological and micro-biological observations. J Periodontol 1993;64:162-168.
27. Grevstad HJ, Leknes KN. Ultrastructure of plaque asso-ciated with polytetrafluoroethylene (PTFE) membranesused for guided tissue regeneration. J Clin Periodontol1993;20:193-198.
28. Minabe M. A critical review of the biologic rationale forguided tissue regeneration. J Periodontol 1991;62:171-179.
29. Calongne KB, Aichelmann-Reidy ME, Yukna RA, MayerET. Clinical comparison of microporous biocompatiblecomposite of PMMA, PHEMA and calcium hydroxidegrafts and expanded polytetrafluoroethylene barriermembranes in human mandibular molar Class II furca-tions. A case series. J Periodontol 2001;72:1451-1459.
30. Cortellini P, Tonetti MS. Evaluation of the effect of toothvitality on regenerative outcomes in infrabony defects.J Clin Periodontol 2001;28:672-679.
31. Murphy WL, Peters MC, Kohn DH, Mooney DJ. Sustainedrelease of vascular endothelial growth factor from min-eralized poly(lactide-co-glycolide) scaffolds for tissueengineering. Biomaterials 2000;21:2521-2527.
32. Cortellini P, Prato GP, Tonetti MS. The simplified papillapreservation flap. A novel surgical approach for the man-agement of soft tissues in regenerative procedures. IntJ Periodontics Restorative Dent 1999;19:589-599.
33. Aguirre-Zorzano LA, Estefanía-Cundín E, Gil-Lozano J,Martínez-Conde R, Núñez-Antón V, Santamaría-ZuazuaJ. Periodontal regeneration of intrabony defects using
bioabsorbable membranes: Determinants of the healingresponse. An observational clinical study. Int J Peri-odontics Restorative Dent 1999;19:363-371.
34. Eickholz P, Hausmann E. Evidence for healing of classII and class III furcations 24 months after guided tissueregeneration therapy: Digital subtraction and clinicalmeasurements. J Periodontol 1999;70:1490-1500.
35. Tatakis DN, Trombelli L. Adverse effects associated witha bioabsorbable guided tissue regeneration device in thetreatment of human gingival recession defects. A clini-copathologic case report. J Periodontol 1999;70:542-547.
36. Peter SJ, Miller MJ, Yasko AW, Yaszemski MJ, Mikos AG.Polymer concepts in tissue engineering. J Biomed MaterRes 1998;43:422-427.
37. Eickholz P, Lenhard M, Benn DK, Staehle HJ. Periodontalsurgery of vertical bony defects with or without syntheticbioabsorbable barriers. 12-month results. J Periodontol1998;69:1210-1217.
38. Eickholz P, Hausmann E. Evidence for healing ofinterproximal intrabony defects after conventional andregenerative therapy: Digital radiography and clinicalmeasurements. J Periodont Res 1998;33:156-165.
39. Christgau M, Bader N, Schmalz G, Hiller KA, Wenzel A.Postoperative exposure of bioabsorbable GTR mem-branes: Effect on healing results. Clin Oral Investig1997;1:109-118.
40. Machtei EE, Dunford R, Grossi SG, Genco RJ. Gingivalrecession and exposure of barrier membrane: Effect onguided tissue regeneration of class II furcation defects.Int J Periodontics Restorative Dent 1995;15:590-599.
41. Murphy KG. Postoperative healing complications asso-ciated with Gore-Tex Periodontal Material. Part II. Effectof complications on regeneration. Int J PeriodonticsRestorative Dent 1995;15:549-561.
42. Froum SJ, Tarnow D. Modified coronally positioned flapfor obtaining new attachment in Class 2 and 3 furcationdefects. Part I: Rationale and surgical technique. Int J Peri-odontics Restorative Dent 1995;15:463-473.
43. Müller H-P, Eger T. The overall significance of regener-ative procedures in the treatment of furcations. Quin-tessence Int 1997;28:321-328.
44. Trombelli L, Scabbia A. Healing response of gingivalrecession defects following guided tissue regenerationprocedures in smokers and non-smokers. J Clin Peri-odontol 1997;24:529-533.
45. Eickholz P, Hausmann E. Evidence for healing of classII and III furcations after GTR therapy: Digital subtrac-tion and clinical measurements. J Periodontol 1997;68:636-644.
46. Trombelli L, Kim C-K, Zimmerman GJ, Wikesjö UME.Retrospective analysis of factors related to clinical out-come of guided tissue regeneration procedures in intra-bony defects. J Clin Periodontol 1997;24:366-371.
47. Falk H, Laurell L, Ravald N, Teiwik A, Persson R. Guidedtissue regeneration therapy of 203 consecutively treatedintrabony defects using a bioabsorbable matrix barrier.Clinical and radiographic findings. J Periodontol 1997;68:571-581.
48. Cortellini P, Pini Prato G, Tonetti MS. The modified papillapreservation technique with resorbablebioabsorbablebarrier membranes in the treatment of intrabony defects.
294
8011.qxd 12/30/03 3:33 PM Page 294
Ann Periodontol Murphy, Gunsolley
Case reports. Int J Periodontics Restorative Dent 1996;16:547-559.
49. De Sanctis M, Zucchelli G, Clauser C. Bacterial colo-nization of bioabsorbable barrier material and periodontalregeneration. J Periodontol 1996;67:1193-1200.
50. Murphy KG. Interproximal tissue maintenance in GTRprocedures: Description of a surgical technique and1-year reentry results. Int J Periodontics Restorative Dent1996;16:463-477.
51. Piattelli A, Scarano A, Paolantonio M. Bone formationinside the material interstices of e-PTFE membranes:A light microscopical and histochemical study in man.Biomaterials 1996;17:1725-1731.
52. Tonetti MS, Pini Prato G, Stalpers G, Cortellini P. Guidedtissue regeneration of deep intrabony defects in strate-gically important prosthetic abutments. Int J Periodon-tics Restorative Dent 1996;16:378-387.
53. Nowzari H, MacDonald ES, Flynn J, London RM, MorrisonJL, Slots J. The dynamics of microbial colonization ofbarrier membranes for guided tissue regeneration. J Peri-odontol 1996;67:694-702.
54. Yukna CN, Yukna RA. Multi-center evaluation of bioab-sorbable collagen membrane for guided tissue regener-ation in human class II furcations. J Periodontol 1996;67:650-657.
55. Becker W, Becker BE, Mellonig J, et al. A prospectivemulti-center study evaluating periodontal regeneration forclass II furcation invasions and intrabony defects aftertreatment with a bioabsorbable barrier membrane: 1-yearresults. J Periodontol 1996;67:641-649.
56. Machtei EE, Grossi SG, Dunford R, Zambon JJ, GencoRJ. Long-term stability of class II furcation defects treatedwith barrier membranes. J Periodontol 1996;67:523-527.
57. Cortellini P, Pini Prato GP, Tonetti MS. Long-term stabilityof clinical attachment following guided tissue regenera-tion and conventional therapy. J Clin Periodontol 1996;23:106-111.
58. Müller H-P, Eger T, Lange DE. Management of furca-tion-involved teeth. A retrospective analysis. J Clin Peri-odontol 1995;22:911-917.
59. Novaes AB Jr, Gutierrez FG, Francischetto IF, Novaes AB.Bacterial colonization of the external and internal sulciand of cellulose membranes at time of retrieval. J Peri-odontol 1995;66:864-869.
60. Drummond BK, Holborow DW, Chandler NP. Guided tis-sue regeneration in managing an incisor with a labiallyfused supernumerary: Case report. Pediatr Dent 1995;17:368-371.
61. Cortellini P, Pini Prato GP, Tonetti MS. No detrimentaleffect of fibrin glue on the regeneration of intrabonydefects. A controlled clinical trial. J Clin Periodontol1995;22:697-702.
62. Weigel C, Brägger U, Hämmerle CHF, Mombelli A,Lang NP. Maintenance of new attachment 1 and 4 yearsfollowing guided tissue regeneration (GTR). J Clin Peri-odontol 1995;22:661-669.
63. Murphy KG. Postoperative healing complications asso-ciated with Gore-Tex Periodontal Material. Part I. Inci-dence and characterization. Int J Periodontics RestorativeDent 1995;15:363-375.
64. Anderegg CR, Metzler DG, Nicoll BK. Gingiva thick-
ness in guided tissue regeneration and associated reces-sion at facial furcation defects. J Periodontol 1995;66:397-402.
65. Polson AM, Garrett S, Stoller NH, et al. Guided tissueregeneration in human furcation defects after usinga biodegradable barrier: A multi-center feasibility study.J Periodontol 1995;66:377-385.
66. Cortellini P, Pini Prato G, Tonetti MS. Interproximal freegingival grafts after membrane removal in guided tis-sue regeneration treatment of intrabony defects. A ran-domized controlled clinical trial. J Periodontol 1995;66:488-493.
67. Tonetti MS, Pini-Prato G, Cortellini P. Effect of cigarettesmoking on periodontal healing following GTR in infrabonydefects. A preliminary retrospective study. J Clin Peri-odontol 1995;22:229-234.
68. Laurell L, Falk H, Fornell J, Johard G, Gottlow J. Clin-ical use of a bioabsorbable matrix barrier in guided tis-sue regeneration therapy. Case series. J Periodontol1994;65:967-75.
69. Cortellini P, Pini-Prato G, Tonetti M. Periodontal regen-eration of human infrabony defects (V). Effect of oralhygiene on long-term stability. J Clin Periodontol 1994;21:606-610.
70. Schallhorn RG, McClain PK. Clinical and radiographichealing pattern observations with combined regenerativetechniques. Int J Periodontics Restorative Dent 1994;14:391-403.
71. Trombelli L, Schincaglia G, Checchi L, Calura G. Com-bined guided tissue regeneration, root conditioning, andfibrin-fibronectin system application in the treatment ofgingival recession. A 15-case report. J Periodontol1994;65:796-803.
72. Rosenberg ES, Cutler SA. The effect of cigarette smok-ing on the long-term success of guided tissue regener-ation: A preliminary study. Ann R Australas Coll DentSurg 1994;12:89-93.
73. Machtei EE, Cho MI, Dunford R, Norderyd J, Zambon JJ,Genco RJ. Clinical, microbiological, and histological fac-tors which influence the success of regenerative peri-odontal therapy. J Periodontol 1994;65:154-161.
74. Florès-de-Jacoby L, Zimmermann A, Tsalikis L. Expe-riences with guided tissue regeneration in the treatmentof advanced periodontal disease. A clinical re-entrystudy, Part I. Vertical, horizontal and combined verticaland horizontal periodontal defects. J Clin Periodontol1994;21:113-117.
75. Tonetti MS, Pini-Prato G, Cortellini P. Periodontal regen-eration of human intrabony defects. IV. Determinants ofhealing response. J Periodontol 1993;64:934-940.
76. Polson AM, Southard GL, Dunn RL, Polson AP. Healingpatterns associated with an Atrisorb barrier in guidedtissue regeneration. Compendium Continuing Educ Dent1993;14:1162, 1164, 1166 passim; quiz 1172.
77. Tonetti MS, Pini Prato G, Williams RC, Cortellini P. Peri-odontal regeneration of human infrabony defects. III.Diagnostic strategies to detect bone gain. J Periodontol1993;64:269-277.
78. Cortellini P, Pini Prato G, Tonetti MS. Periodontalregeneration of human infrabony defects. II. Re-entryprocedures and bone measures. J Periodontol 1993;64:
295
8011.qxd 12/30/03 3:33 PM Page 295

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
261-268.79. McClain PK, Schallhorn RG. Long-term assessment of
combined osseous composite grafting, root conditioning,and guided tissue regeneration. Int J Periodontics Restora-tive Dent 1993;13:9-27.
80. Galgut PN. Polylactic acid used as a barrier membraneto enhance healing in human periodontal defects: A clin-ical study. J West Soc Periodontol 1993;41:37-42.
81. Mullally BH, Linden GJ, Napier SS. Candidal infectionas a complication of barrier membrane placement in adiabetic patient. J Ir Dent Assoc 1993;39:86-88.
82. Al-Arrayed F, Thomas S, Moran J. Effect of addition ofantimicrobial drugs to human collagen membrane. ClinMater 1993;12:169-179.
83. Selvig KA, Kersten BG, Chamberlain AD, Wikesjö UME,Nilvéus RE. Regenerative surgery of intrabony periodontaldefects using ePTFE barrier membranes: Scanning elec-tron microscopic evaluation of retrieved membranes ver-sus clinical healing. J Periodontol 1992;63:974-978.
84. Gottlow J, Nyman S, Karring T. Maintenance of newattachment gained through guided tissue regeneration.J Clin Periodontol 1992;19:315-317.
85. Paul BF, Mellonig JT, Towle HJ, Gray JL. Use of a col-lagen barrier to enhance healing in human periodontalfurcation defects. Int J Periodontics Restorative Dent1992;12:123-131.
86. Stahl SS, Froum S. Human intrabony lesion responsesto debridement, porous hydroxyapatite implants andteflon barrier membranes. 7 histologic case reports. JClin Periodontol 1991;18:605-610.
87. Galgut PN. Oxidized cellulose mesh. I. Biodegradablemembrane in periodontal surgery. Biomaterials 1990;11:561-564.
88. Selvig KA, Kersten BG, Wikesjö UME. Surgical treat-ment of intrabony periodontal defects using expandedpolytetrafluoroethylene barrier membranes: Influence ofdefect configuration on healing response. J Periodontol1993;64:730-733.
89. Garrett S, Loos B, Chamberlain D, Egelberg J. Treatmentof intraosseous periodontal defects with a combinedadjunctive therapy of citric acid conditioning, bone graft-ing, and placement of collagenous membranes. J ClinPeriodontol 1988;15:383-389.
90. Polson AM, Southard GL, Dunn RL, Polson AP, BillenJR, Laster LL. Initial study of guided tissue regenerationin class II furcation defects after use of a biodegradablebarrier. Int J Periodontics Restorative Dent 1995;15:42-55.
91. Eickholz P, Benn DK, Staehle HJ. Radiographic evalu-ation of bone regeneration following periodontal surgerywith or without expanded polytetrafluoroethylene barri-ers. J Periodontol 1996;67:379-385.
92. Pontoriero R, Lindhe J, Nyman S, Karring T, RosenbergE, Sanavi F. Guided tissue regeneration in the treatmentof furcation defects in mandibular molars. A clinicalstudy of degree III involvements. J Clin Periodontol 1989;16:170-174.
93. Sbordone L, Barone A, Di Genio M, Ramaglia L. Tetra-cycline fibres used to control bacterial infection duringguided tissue regeneration (GTR). Minerva Stomatol2000;49:27-34.
94. Wenzel A, Warrer K, Karring T. Digital subtraction radi-ography in assessing bone changes in periodontaldefects following guided tissue regeneration. J Clin Peri-odontol 1992;19:208-213.
95. Pontoriero R, Nyman S, Lindhe J, Rosenberg E, SanaviF. Guided tissue regeneration in the treatment offurcation defects in man. J Clin Periodontol 1987;14:618-620.
96. Iversen B, Albandar JM, Øydna J, Gjermo P. Bone den-sity changes after 1 year in periodontal lesions treatedsurgically with or without ePTFE membrane placement.J Clin Periodontol 1996;23:512-516.
97. Eickholz P, Kim TS, Steinbrenner H, Dörfer C, Holle R.Guided tissue regeneration with bioabsorbable barriers:Intrabony defects and class II furcations. J Periodontol2000;71:999-1008.
98. Karapataki S, Hugoson A, Falk H, Laurell L, KugelbergCF. Healing following GTR treatment of intrabonydefects distal to mandibular 2nd molars using bioab-sorbable and non-bioabsorbable barriers. J Clin Peri-odontol 2000;27:333-340.
99. Karapataki S, Hugoson A, Kugelberg CF. Healing fol-lowing GTR treatment of bone defects distal to mandibu-lar 2nd molars after surgical removal of impacted 3rdmolars. J Clin Periodontol 2000;27:325-332.
100. Dörfer CE, Kim T-S, Steinbrenner H, Holle R, Eickholz P.Regenerative periodontal surgery in interproximal intra-bony defects with biodegradable barriers. J Clin Peri-odontol 2000;27:162-168.
101. Trejo PM, Weltman R, Caffesse RG. Effects of expandedpolytetrafluoroethylene and polylactic acid barriers onhealthy sites. J Periodontol 1998;69:14-18.
102. Chaves ES, Geurs NC, Reddy MS, Jeffcoat MK. Clini-cal and radiographic digital imaging evaluation of aresorbablebioabsorbable membrane in the treatmentof periodontal bone defects. Int J Periodontics Restora-tive Dent 1996;16:443-453.
103. Sirirat M, Kasetsuwan J, Jeffcoat MK. Comparisonbetween 2 surgical techniques for the treatment of early-onset periodontitis. J Periodontol 1996;67:603-607.
104. Sander L, Frandsen EVG, Arnbjerg D, Warrer K, KarringT. Effect of local metronidazole application on peri-odontal healing following guided tissue regeneration.Clinical findings. J Periodontol 1994;65:914-920.
105. Stein MD, Salkin LM, Freedman AL. The effects ofguided tissue regeneration membrane placement onhealthy periodontal sites. J Periodontol 1993;64:57-59.
106. Sculean A, Donos N, Miliauskaite A, Arweiler N, BrecxM. Treatment of intrabony defects with enamel matrixproteins or bioabsorbable membranes. A 4-year follow-up split-mouth study. J Periodontol 2001;72:1695-1701.
107. Christgau M, Schmalz G, Reich E, Wenzel A. Clinicaland radiographical split-mouth-study on bioabsorbableversus non-bioabsorbable GTR-membranes. J Clin Peri-odontol 1995;22:306-315.
108. Twohey SM, Mellonig JT, Towle HJ, Gray JL. Use of asynthetic skin substitute as a physical barrier to enhancehealing in human periodontal furcation defects. Int J Peri-odontics Restorative Dent 1992;12:383-393.
109. Pontoriero R, Wennström J, Lindhe J. The use of bar-rier membranes and enamel matrix proteins in the treat-
296
8011.qxd 12/30/03 3:33 PM Page 296
Ann Periodontol Murphy, Gunsolley
ment of angular bone defects. A prospective controlledclinical study. J Clin Periodontol 1999;26:833-840.
110. Sculean A, Donos N, Blaes A, Lauermann M, Reich E,Brecx M. Comparison of enamel matrix proteins andbioabsorbable membranes in the treatment of intra-bony periodontal defects. A split-mouth study. J Peri-odontol 1999;70:255-262.
111. al-Arrayed F, Adam S, Moran J, Dowell P. Clinical trialof cross-linked human type I collagen as a barrier mate-rial in surgical periodontal treatment. J Clin Periodon-tol 1995;22:371-379.
112. Orsini M, Orsini G, Benlloch D, et al. Comparison of cal-cium sulfate and autogenous bone graft to bioab-sorbable membranes plus autogenous bone graft in thetreatment of intrabony periodontal defects: A split-mouth study. J Periodontol 2001;72:296-302.
113. Quteish D, Dolby AE. The use of irradiated-crosslinkedhuman collagen membrane in guided tissue regenera-tion. J Clin Periodontol 1992;19:476-484.
114. Bratthall G, Söderholm G, Neiderud AM, KullendorffB, Edwardsson S, Attström R. Guided tissue regener-ation in the treatment of human infrabony defects. Clin-ical, radiographical and microbiological results: A pilotstudy. J Clin Periodontol 1998;25:908-914.
115. Caton J, Greenstein G, Zappa U. Synthetic bioab-sorbable barrier for regeneration in human periodontaldefects. J Periodontol 1994;65:1037-1045.
116. Garrett S, Polson AM, Stoller NH, et al. Comparison ofa bioabsorbable GTR barrier to a non-absorbable barrierin treating human class II furcation defects. A multi-center parallel design randomized single-blind trial.J Periodontol 1997;68:667-675.
117. Hugoson A, Ravald N, Fornell J, Johard G, Teiwik A,Gottlow J. Treatment of class II furcation involvementsin humans with bioabsorbable and nonbioabsorbableguided tissue regeneration barriers. A randomized multi-center study. J Periodontol 1995;66:624-634.
118. Mehlbauer MJ, Greenwell H, Nouneh I, et al. Improvedclosure rate of Class III furcations using a layered GTRtechnique. Int J Periodontics Restorative Dent 2000;20:285-295.
119. Mellonig JT, Seamons BC, Gray JL, Towle HJ. Clinicalevaluation of guided tissue regeneration in the treatmentof grade II molar furcation invasions. Int J PeriodonticsRestorative Dent 1994;14:255-271.
120. Pontoriero R, Lindhe J. Guided tissue regeneration inthe treatment of degree II furcations in maxillary molars.J Clin Periodontol 1995;22:756-763.
121. Pontoriero R, Lindhe J. Guided tissue regeneration inthe treatment of degree III furcation defects in maxil-lary molars. J Clin Periodontol 1995;22:810-812.
122. Van Swol RL, Ellinger R, Pfeifer J, Barton NE, BlumenthalN. Collagen membrane barrier therapy to guide regen-eration in class II furcations in humans. J Periodontol1993;64:622-629.
123. Vernino AR, Ringeisen TA, Wang H-L, et al. Use ofbiodegradable polylactic acid barrier materials in thetreatment of grade II periodontal furcation defects inhumans–Part I: A multicenter investigative clinical study.Int J Periodontics Restorative Dent 1998;18:573-585.
124. Demolon IA, Persson GR, Ammons WF, Johnson RH.
Effects of antibiotic treatment on clinical conditions withguided tissue regeneration: One-year results. J Periodontol1994;65:713-717.
125. Garrett S, Martin M, Egelberg J. Treatment of peri-odontal furcation defects. Coronally positioned flapsversus dura mater membranes in class II defects. J ClinPeriodontol 1990;17:179-185.
126. Wallace SC, Gellin RG, Miller MC, Mishkin DJ. Guidedtissue regeneration with and without decalcified freeze-dried bone in mandibular class II furcation invasions.J Periodontol 1994;65:244-254.
127. Cortellini P, Tonetti MS, Lang NP, et al. The simpli-fied papilla preservation flap in the regenerative treat-ment of deep intrabony defects: Clinical outcomesand postoperative morbidity. J Periodontol 2001;72:1702-1712.
128. Cortellini P, Tonetti MS. Microsurgical approach to peri-odontal regeneration. Initial evaluation in a case cohort.J Periodontol 2001;72:559-569.
129. Cortellini P, Prato GP, Tonetti MS. The modified papillapreservation technique. A new surgical approach forinterproximal regenerative procedures. J Periodontol1995;66:261-266.
130. Bichara J, Greenwell H, Drisko C, et al. The effect ofpostsurgical naproxen and a bioabsorbable membraneon osseous healing in intrabony defects. J Periodontol1999;70:869-877.
131. Cortellini P, Carnevale G, Sanz M, Tonetti MS. Treatmentof deep and shallow intrabony defects. A multicenterrandomized controlled clinical trial. J Clin Periodontol1998;25:981-987.
132. Cortellini P, Pini Prato G, Tonetti MS. Periodontal regen-eration of human intrabony defects with titanium rein-forced membranes. A controlled clinical trial. J Periodontol1995;66:797-803.
133. Cortellini P, Pini Prato G, Tonetti MS. Periodontal regen-eration of human intrabony defects with bioabsorbablemembranes. A controlled clinical trial. J Periodontol1996;67:217-223.
134. Cortellini P, Tonetti MS. Microsurgical approach to peri-odontal regeneration. Initial evaluation in a case cohort.J Periodontol 2001;72:559-569.
135. Gouldin AG, Fayad S, Mellonig JT. Evaluation of guidedtissue regeneration in interproximal defects. (II). Mem-brane and bone versus membrane alone. J Clin Peri-odontol 1996;23:485-491.
136. Guillemin MR, Mellonig JT, Brunsvold MA. Healing inperiodontal defects treated by decalcified freeze-driedbone allografts in combination with ePTFE membranes(I). Clinical and scanning electron microscope analy-sis. J Clin Periodontol 1993;20:528-536.
137. Joly JC, CALioto DB, de Lima AFM, Mota LF, CaffesseR. Clinical and radiographic evaluation of periodontalintrabony defects treated with guided tissue regenera-tion. A pilot study. J Periodontol 2002;73:353-359.
138. Kim C-K, Choi E-J, Cho K-S, Chai J-K, Wikesjö UME.Periodontal repair in intrabony defects treated with acalcium carbonate implant and guided tissue regener-ation. J Periodontol 1996;67:1301-1306.
139. Lekovic V, Camargo PM, Weinlaender M, Kenney EB,Vasilic N. Combination use of bovine porous bone
297
8011.qxd 12/30/03 3:33 PM Page 297

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
mineral, enamel matrix proteins, and a bioabsorbablemembrane in intrabony periodontal defects in humans.J Periodontol 2001;72:583-589.
140. Sculean A, Windisch P, Chiantella GC, Donos N, BrecxM, Reich E. Treatment of intrabony defects with enamelmatrix proteins and guided tissue regeneration. Aprospective controlled clinical study. J Clin Periodontol2001;28:397-403.
141. Tonetti MS, Cortellini P, Suvan JE, et al. Generalizabilityof the added benefits of guided tissue regeneration inthe treatment of deep intrabony defects. Evaluation in amulti-center randomized controlled clinical trial. J Peri-odontol 1998;69:1183-1192.
142. Tonetti MS, Pini Prato G, Cortellini P. Factors affectingthe healing response of intrabony defects followingguided tissue regeneration and access flap surgery.J Clin Periodontol 1996;23:548-556.
143. Trejo PM, Weltman R, Caffesse R. Treatment ofintraosseous defects with bioabsorbable barriers aloneor in combination with decalcified freeze-dried boneallograft: A randomized clinical trial. J Periodontol 2000;71:1852-1861.
144. Yoshinari N, Tohya T, Kawase H, et al. Effect of repeatedlocal minocycline administration on periodontal healingfollowing guided tissue regeneration. J Periodontol2001;72:284-295.
145. Zucchelli G, Bernardi F, Montebugnoli L, De SanctisM. Enamel matrix proteins and guided tissue regener-ation with titanium-reinforced expanded polytetrafluo-roethylene membranes in the treatment of infrabonydefects: A comparative controlled clinical trial. J Peri-odontol 2002;73:3-12.
146. Zucchelli G, Sforza NM, Clauser C, Cesari C, De SanctisM. Topical and systemic antimicrobial therapy in guidedtissue regeneration. J Periodontol 1999;70:239-247.
147. Zybutz MD, Laurell L, Rapoport DA, Persson GR. Treat-ment of intrabony defects with bioabsorbable materi-als, non-bioabsorbable materials and flap debridement.J Clin Periodontol 2000;27:169-178.
148. Blumenthal N, Steinberg J. The use of collagen mem-brane barriers in conjunction with combined deminer-alized bone-collagen gel implants in human infrabonydefects. J Periodontol 1990;61:319-327.
149. Camargo PM, Lekovic V, Weinlaender M, et al. A con-trolled re-entry study on the effectiveness of bovineporous bone mineral used in combination with a col-lagen membrane of porcine origin in the treatment ofintrabony defects in humans. J Clin Periodontol 2000;27:889-896.
150. Mattson JS, Gallagher SJ, Jabro MH. The use of 2 bioab-sorbable barrier membranes in the treatment of inter-proximal intrabony periodontal defects. J Periodontol1999;70:510-517.
151. Benqué E, Zahedi S, Brocard D, Oscaby F, Justumus P,Brunel G. Guided tissue regeneration using a collagenmembrane in chronic adult and rapidly progressive peri-odontitis patients in the treatment of 3-wall intrabonydefects. J Clin Periodontol 1997;24:544-549.
152. Batista EL Jr, Novaes AB Jr, Simonpietri JJ, Batista FC.Use of bovine-derived anorganic bone associated withguided tissue regeneration in intrabony defects. Six-
month evaluation at re-entry. J Periodontol 1999;70:1000-1007.
153. Chen C-C, Wang H-L, Smith F, Glickman GN, Shyr Y,O’Neal RB. Evaluation of a collagen membrane withand without bone grafts in treating periodontal intrabonydefects. J Periodontol 1995;66:838-847.
154. Christgau M, Bader N, Schmalz G, Hiller K-A, WenzelA. GTR therapy of intrabony defects using 2 differentbioabsorbable membranes: 12-month results. J ClinPeriodontol 1998;25:499-509.
155. Christgau M, Schmalz G, Wenzel A, Hiller KA. Peri-odontal regeneration of intrabony defects with bioab-sorbable and non-bioabsorbable membranes: 30-monthresults. J Clin Periodontol 1997;24:17-27.
156. Kersten BG, Chamberlain ADH, Khorsandi S, WikesjöUME, Selvig KA, Nilvéus RE. Healing of the intrabonyperiodontal lesion following root conditioning with cit-ric acid and wound closure including an expandedPTFE membrane. J Periodontol 1992;63:876-882.
157. Kiliç AR, Efeoglu E, Yilmaz S. Guided tissue regener-ation in conjunction with hydroxyapatite-collagen graftsfor intrabony defects. A clinical and radiological eval-uation. J Clin Periodontol 1997;24:372-383.
158. Kim C-K, Chai J-K, Cho K-S, et al. Periodontal repairin intrabony defects treated with a calcium sulfateimplant and calcium sulfate barrier. J Periodontol 1998;69:1317-1324.
159. Mayfield L, Söderholm G, Hallström H, et al. Guidedtissue regeneration for the treatment of intraosseousdefects using a bioabsorbable membrane. A controlledclinical study. J Clin Periodontol 1998;25:585-595.
160. Mellado JR, Salkin LM, Freedman AL, Stein MD. Acomparative study of ePTFE periodontal membraneswith and without decalcified freeze-dried bone allograftsfor the regeneration of interproximal intraosseousdefects. J Periodontol 1995;66:751-755.
161. Paolantonio M. Combined periodontal regenerativetechnique in human intrabony defects by collagenmembranes and anorganic bovine bone. A controlledclinical study. J Periodontol 2002;73:158-166.
162. Paolantonio M, D’Archivio D, Di Placido G, et al.Expanded polytetrafluoroethylene and dental rubberdam barrier membranes in the treatment of periodon-tal intrabony defects. A comparative clinical trial. J ClinPeriodontol 1998;25:920-928.
163. Weltman R, Trejo PM, Morrison E, Caffesse R. Assess-ment of guided tissue regeneration procedures in intra-bony defects with bioabsorbable and non-bioabsorbablebarriers. J Periodontol 1997;68:582-590.
164. Zarkesh N, Nowzari H, Morrison J, Slots J. Tetracycline-coated polytetrafluoroethylene barrier membranes in thetreatment of intraosseous periodontal lesions. J Peri-odontol 1999;70:1008-1016.
165. Chung KM, Salkin LM, Stein MD, Freedman AL. Clin-ical evaluation of a biodegradable collagen membranein guided tissue regeneration. J Periodontol 1990;61:732-736.
166. Benqué E, Zahedi S, Brocard D, Oscaby F, Justumus P,Brunel G. Combined collagen membrane and hydrox-yapatite/collagen chondroitin-sulfate spacer placementin the treatment of 2-wall intrabony defects in chronic
298
8011.qxd 12/30/03 3:33 PM Page 298

Ann Periodontol Murphy, Gunsolley
adult and rapidly progressive periodontitis patients. J ClinPeriodontol 1997;24:550-556.
167. Eickholz P, Kim TS, Holle R. Regenerative periodontalsurgery with non-bioabsorbable and biodegradable bar-riers: Results after 24 months. J Clin Periodontol 1998;25:666-676.
168. Nygaard-Østby P, Tellefsen G, Sigurdsson TJ, ZimmermanGJ, Wikesjö UME. Periodontal healing following recon-structive surgery: Effect of guided tissue regeneration.J Clin Periodontol 1996;23:1073-1079.
169. Parashis A, Andronikaki-Faldami A, Tsiklakis K. Com-parison of 2 regenerative procedures–guided tis-sue regeneration and demineralized freeze-dried boneallograft–in the treatment of intrabony defects: A clin-ical and radiographic study. J Periodontol 1998;69:751-758.
170. Ratka-Krüger P, Neukranz E, Raetzke P. Guided tissueregeneration procedure with bioabsorbable membranesversus conventional flap surgery in the treatment ofinfrabony periodontal defects. J Clin Periodontol2000;27:120-127.
171. Bouchard P, Giovannoli JL, Mattout C, Davarpanah M,Etienne D. Clinical evaluation of a bioabsorbable regen-erative material in mandibular class II furcation therapy.J Clin Periodontol 1997;24:511-518.
172. Lekovic V, Kenney EB, Kovacevic K, Carranza FA Jr.Evaluation of guided tissue regeneration in class II fur-cation defects. A clinical re-entry study. J Periodontol1989;60:694-698.
173. Metzler DG, Seamons BC, Mellonig JT, Gher ME, GrayJL. Clinical evaluation of guided tissue regeneration inthe treatment of maxillary class II molar furcation inva-sions. J Periodontol 1991;62:353-360.
174. Vest TM, Greenwell H, Drisko C, et al. The effect of post-surgical antibiotics and a bioabsorbable membrane onregenerative healing in class II furcation defects. J Peri-odontol 1999;70:878-887.
175. Wang H-L, O’Neal RB, Thomas CL, Shyr Y, MacNeil RL.Evaluation of an absorbable collagen membrane intreating class II furcation defects. J Periodontol 1994;65:1029-1036.
176. Anderegg CR, Martin SJ, Gray JL, Mellonig JT, GherME. Clinical evaluation of the use of decalcified freeze-dried bone allograft with guided tissue regeneration inthe treatment of molar furcation invasions. J Periodontol1991;62:264-268.
177. Blumenthal NM. A clinical comparison of collagenmembranes with e-PTFE membranes in the treatmentof human mandibular buccal class II furcation defects.J Periodontol 1993;64:925-933.
178. dos Anjos B, Novaes AB Jr, Meffert R, Barboza EP.Clinical comparison of cellulose and expanded polyte-trafluoroethylene membranes in the treatment of classII furcations in mandibular molars with 6-month re-entry.J Periodontol 1998;69:454-459.
179. Flanary DB, Twohey SM, Gray JL, Mellonig JT, Gher ME.The use of a synthetic skin substitute as a physicalbarrier to enhance healing in human periodontal fur-cation defects: A follow-up report. J Periodontol 1991;62:684-689.
180. Lekovic V, Kenney EB, Carranza FA, Martignoni M. The
use of autogenous periosteal grafts as barriers for thetreatment of class II furcation involvements in lowermolars. J Periodontol 1991;62:775-780.
181. Machtei EE, Dunford RG, Norderyd OM, Zambon JJ,Genco RJ. Guided tissue regeneration and anti-infec-tive therapy in the treatment of class II furcation defects.J Periodontol 1993;64:968-973.
182. Avera JB, Camargo PM, Klokkevold PR, Kenney EB,Lekovic V. Guided tissue regeneration in Class II fur-cation involved maxillary molars: A controlled studyof 8 split-mouth cases. J Periodontol 1998;69:1020-1026.
183. Black BS, Gher ME, Sandifer JB, Fucini SE, RichardsonAC. Comparative study of collagen and expanded poly-tetrafluoroethylene membranes in the treatment ofhuman class II furcation defects. J Periodontol 1994;65:598-604.
184. Bouchard P, Ouhayoun J-P, Nilvéus RE. Expandedpolytetrafluoroethylene membranes and connective tis-sue grafts support bone regeneration for closingmandibular class II furcations. J Periodontol 1993;64:1193-1198.
185. De Leonardis D, Garg AK, Pedrazzoli V, Pecora GE.Clinical evaluation of the treatment of class II furcationinvolvements with bioabsorbable barriers alone or asso-ciated with demineralized freeze-dried bone allografts.J Periodontol 1999;70:8-12.
186. Lekovic V, Kenney EB, Carranza FA Jr, Danilovic V.Treatment of class II furcation defects using poroushydroxylapatite in conjunction with a polytetrafluo-roethylene membrane. J Periodontol 1990;61:575-578.
187. Luepke PG, Mellonig JT, Brunsvold MA. A clinical eval-uation of a bioabsorbable barrier with and withoutdecalcified freeze-dried bone allograft in the treatmentof molar furcations. J Clin Periodontol 1997;24:440-446.
188. Parashis AO, Mitsis FJ. Clinical evaluation of the effectof tetracycline root preparation on guided tissue regen-eration in the treatment of class II furcation defects. J Peri-odontol 1993;64:133-136.
189. Pontoriero R, Lindhe J, Nyman S, Karring T, RosenbergE, Sanavi F. Guided tissue regeneration in degree IIfurcation-involved mandibular molars. A clinical study.J Clin Periodontol 1988;15:247-254.
190. Scott TA, Towle HJ, Assad DA, Nicoll BK. Comparisonof bioabsorbable laminar bone membrane and non-bioabsorbable ePTFE membrane in mandibular furca-tions. J Periodontol 1997;68:679-686.
191. Simonpietri-C JJ, Novaes AB Jr, Batista EL Jr, Filho EJF.Guided tissue regeneration associated with bovine-derivedanorganic bone in mandibular class II furcation defects. 6-month results at re-entry. J Periodontol 2000;71:904-911.
192. Andersson B, Bratthall G, Kullendorff B, Gröndahl K,Rohlin M, Attström R. Treatment of furcation defects.Guided tissue regeneration versus coronally positionedflap in mandibular molars; a pilot study. J Clin Peri-odontol 1994;21:211-216.
193. Garrett S, Gantes B, Zimmerman G, Egelberg J. Treat-ment of mandibular class III periodontal furcation defects.Coronally positioned flaps with and without expandedpolytetrafluoroethylene membranes. J Periodontol 1994;
299
8011.qxd 12/30/03 3:33 PM Page 299

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
65:592-597.194. Yamaoka SB, Mellonig JT, Meffert RM, Arnold RM,
Nummikoski PV, Mealey BL. Clinical evaluation of dem-ineralized-unicortical-ilium-strips for guided tissueregeneration. J Periodontol 1996;67:803-815.
195. Lekovic V, Klokkevold PR, Camargo PM, Kenney EB,Nedic M, Weinlaender M. Evaluation of periosteal mem-branes and coronally positioned flaps in the treatmentof class II furcation defects: A comparative clinicalstudy in humans. J Periodontol 1998;69:1050-1055.
196. Needleman IG, Giedrys-Leeper E, Tucker RJ, WorthingtonHV. Guided tissue regeneration for periodontal infra-bonydefects. Cochrane Database Syst Rev 2001;(2):CD001724.
197. Jepsen S, Eberhard J, Herrera D, Needleman I. A sys-tematic review of guided tissue regeneration for peri-odontal furcation defects. What is the effect of guidedtissue regeneration compared with surgical debride-ment in the treatment of furcation defects? J Clin Peri-odontol 2002;29(Suppl. 3):103-116.
198. Schallhorn RG, McClain PK. Periodontal regenerationusing combined techniques. Periodontol 2000 1993;1:109-117.
Correspondence: Dr. Kevin G. Murphy, Suite 2, 4 W. Uni-versity Pkwy., Baltimore, MD 21218. E-mail: [email protected].
Accepted for publication October 5, 2003.
APPENDIX ACONSENSUS REPORT
Members of the Section read and studied the reviewtitled “Guided Tissue Regeneration for the Treatment ofPeriodontal Intrabony and Furcation Defects. A Sys-tematic Review” by Kevin G. Murphy and John C. Gun-solley. The focused PICO question addressed by this evi-dence-based systematic review is: “In patients withperiodontal osseous defects, what is the effect of phys-ical barriers compared with surgical controls on clinical,radiographic, adverse and patient-centered outcomes?”
INTRODUCTIONA survey of Section members established that therewere no conflicts of interest that would have an impactupon their deliberations or decisions. This Sectionfocused on evaluation of the evidence presented in thesystematic review and on challenging the evidence withthe personal knowledge and clinical experience of allthe members. The discussion focused on addressingthe PICO question and data provided by the currentsystematic review and prior systematic reviews.
The PICO question limited the scope of the system-atic review. The systematic review protocol includedonly high quality randomized controlled clinical trials(RCTs). A wide body of information that may haveexplored other aspects of this field was not included.Clinical experience and knowledge of the group iden-tified several areas that could not be captured by the
conclusions of the report and which might have animpact upon the clinical utilization of the informationdeveloped as a result of this workshop.
Clinical considerations such as tooth morphology,gingival characteristics, tooth mobility, strategic valueof the tooth, furcation defect location (maxillary ormandibular), furcation severity, the individuality of thedefect, intrabony defect type (number of walls), useof adjunctive anti-infective therapies, and patientoral hygiene status may affect clinical outcomes andtherefore treatment selection. These and other factors,in addition to the recommendations made below inresponse to question 5, may account for variability inthe response to therapy and require specific decisionmaking by clinicians on a case-by-case basis. Conse-quently one could anticipate a more favorable outcomethan reported in this meta-analysis when treatment isindividualized to a specific clinical condition.
1. Does the Section agree that the evidence-basedsystematic review is complete and accurate?The data review was complete and accurate within thecontext of the question posed. Because of the scopeof the subject and the breadth of the data available,the analysis and interpretation of the data collectedmay be expanded to include: furcation closure, mor-bidity, and long-term outcomes.
Furcation fill/closure. The optimum clinical resultfrom the application of GTR to furcation defects is com-plete furcation fill/closure. Data reported in the sys-tematic review that did not meet the stipulated criteriafor quantitative analyses, because of the lack of a con-sistently applied criterion for furcation fill/closure, indi-cated that complete closure was an infrequent event.
Morbidity. Adverse events and patient concerns areimportant considerations in assessing the risk/benefitratio of a procedure. Observational evidence seems toindicate that GTR with non-resorbable membranes isassociated with increased morbidity. Evidence withbioabsorbable membranes detected no differencebetween GTR and access flap control.
Long-Term Effects. Obtaining and maintainingimproved attachment levels and extending tooth sur-vival with GTR over extended periods of time areimportant. Data available for intrabony and furcationdefects1-6 but not included in the meta-analysis anddata that became available after the cut-off date7 indi-cate that clinical attachment levels and teeth can bemaintained for periods of 5 years or more with propermaintenance care.
2. Has any new information been generatedor discovered since the evidence-based searchcut-off date?New information has been generated since the January2002 search cut-off date, but the results have not alteredthe general conclusions of the review.
300
8011.qxd 12/30/03 3:33 PM Page 300
Ann Periodontol Murphy, Gunsolley
3. Does the Section agree with the interpretationsand conclusions of the reviewers?After assessment of the original evidence, the Sectionagrees with the following conclusions:
1. In the treatment of intrabony and furcationdefects, GTR is significantly more favorable when com-pared to open flap debridement procedures when theintrabony surrogate outcome variables of clinicalattachment level (CAL) and probing depth (PD), andthe furcation surrogate outcome variables (i.e., verti-cal attachment level [VPAL], vertical probing depth[VPD], horizontal probing attachment [HOPA]) areevaluated.
2. In the treatment of intrabony defects, the meta-analysis did not show any statistically significant supe-rior results among the barriers evaluated. However, thetype of barrier utilized can describe some of theheterogeneity of the data. In the treatment of furcationdefects, the type of barrier employed did affect thesurrogate variable VPAL, as VPAL was enhanced onlywith the use of ePTFE and polymeric barriers.
3. The use of augmentation materials in addition tothe physical barrier enhances the regenerative out-come in the treatment of furcation defects treated withGTR. There is no advantage to the use of augmenta-tion materials in addition to the use of the physicalbarrier in the treatment of intrabony defects.
4. The use of specialized flap techniques mayenhance clinical outcomes, but there is not sufficientdata at this time to demonstrate superiority with the useof these techniques.
5. A monthly frequency maintenance scheduleresults in probing depth reduction, but the use of thisregimen does not statistically improve clinical attach-ment level outcomes in GTR.
6. There are insufficient data available to performa meta-analysis regarding the enhancement of toothsurvival, ease of post-treatment maintenance, enhance-ment of esthetic outcomes, or furcation closure facil-itated by GTR procedures.
4. What further research needs to be done relative tothe focused questions of the evidence-based review?The members of the Section observed that the major-ity of published research is focused on surrogate clini-cal measures. Such research was critical in providing theevidence of efficacy. Relatively few studies so far havefocused on patient-centered outcomes. Data are neededwith relation to the benefit of periodontal regenerationin terms of tooth survival, improved function, esthetics,ease of maintenance, and patient comfort. The Sectionalso felt that there was an urgent need to identify the pos-sible sources of variability of results, such as patient- anddisease-based factors and defect morphology. Moreinformation is also needed to assist in selection of theappropriate treatment options for specific clinical situ-
ations. Research is needed to evaluate new technologies(e.g., tissue engineering, growth factors) used to mod-ify or in conjunction with physical barriers on clinical,histologic, and patient-centered outcomes.
5. How can the information from the evidence-based review be applied to patient management?A. Barrier membranes provide additional benefits overopen flap debridement in terms of improving clinicalattachment levels and reducing probing depths in intra-bony and furcation defects.
Level of Evidence:8 Strong.Rationale: Meta-analyses from this systematic
review utilizing over 50 Level I RCTs and 2 other sys-tematic reviews.
B. In intrabony defects the morbidity associated withthe use of bioabsorbable membranes is no greater thanthat with open flap debridement.
Level of Evidence: Strong.Rationale: Data from 1 large multi-center level I
RCT specifically designed to examine patient morbid-ity.
C. The use of bone replacement grafts in additionto the physical barrier enhances clinical outcomes infurcation defects.
Level of Evidence: Strong.Rationale: Meta-analyses from this systematic
review utilizing 6 level I RCTs.D. The use of a barrier alone provides similar results
to the combination of bone replacement graft plus bar-rier in intrabony defects.
Level of Evidence: Strong.Rationale: Meta-analyses from this systematic
review utilizing 6 level I RCTs. However, the Sectionfeels strongly that the randomized trials did not cap-ture the individuality of the anatomy of the defectsand, therefore, the combination may be appropriatein specific clinical situations.
E. Applications of barriers in intrabony defects maybe associated with increased recession of the gingivalmargin compared to open flap debridement.
Level of Evidence: Strong.Rationale: Meta-analyses from this systematic
review of 19 level I RCTs.F. There was no difference in gingival recession fol-
lowing the application of bioresorbable or non-resorbable barriers in intrabony defects.
Level of Evidence: Strong.Rationale: Meta-analyses from this systematic
review of 6 level I RCTs. However, the Section felt thatgingival recession as a postoperative complication maylead to adverse clinical outcomes.
G. Coronally advanced flaps to cover the barrier areassociated with better clinical outcomes in furcationdefects.
301
8011.qxd 12/30/03 3:33 PM Page 301

GTR in Treating Intrabony and Furcation Defects Volume 8 • Number 1 • December 2003
Level of Evidence: Strong.Rationale: Meta-analyses from this systematic
review of 4 level I RCTs.H. In GTR procedures for treating intrabony defects
papilla preservation flaps are probably associated withbetter clinical outcomes.
Level of Evidence: Moderate.Rationale: This systematic review of 6 RCTs and
additional level II studies.I. Intensive postoperative care protocols result in
shallower probing depths in the treatment of intrabonydefects.
Level of Evidence: Strong.Rationale: Meta-analyses from this systematic
review of 6 level I RCTs.J. There is incomplete evidence to indicate that
intensive postoperative care protocols after GTR pro-cedures enhance clinical outcomes other than reduc-tion in probing depths.
Level of Evidence: Incomplete.Rationale: Inadequate data on this topic from 6 level I
RCTs.
REFERENCES1. Gottlow J, Nyman J, Karring T. Maintenance of new
attachment gained through guided tissue regeneration.J Clin Periodontol 1992;19:315-317.
2. Cortellini P, Pini-Prato G, Tonetti M. Periodontal regener-ation of human infrabony defects (V). Effect of oral hygieneon long-term stability. J Clin Periodontol 1994;21:606-610.
3. Cortellini P, Pini Prato GP, Tonetti MS. Long-term stabilityof clinical attachment following guided tissue regenera-tion and conventional therapy. J Clin Periodontol 1996;23:106-111.
4. Weigel C, Brägger U, Hämmerle CHF, Mombelli A, LangNP. Maintenance of new attachment 1 and 4 years fol-lowing guided tissue regeneration (GTR). J Clin Periodontol1995;22:661-669.
5. Cortellini P, Stalpers G, Pini Prato G, Tonetti MS. Long-term clinical outcomes of abutments treated with guidedtissue regeneration. J Prosthet Dent 1999;81:305-311.
6. De Sanctis M, Zucchelli G. Interleukin-1 gene polymor-phisms and long-term stability following guided tissueregeneration therapy. J Periodontol 2000;71:606-613.
7. Cortellini P, Tonetti MS. Long-term tooth survival fol-lowing regenerative treatment of intrabony defects. J Peri-odontol 2004; accepted for publication.
8. Newman MG, Caton J, Gunsolley JC. The use of the evi-dence-based approach in a periodontal therapy contem-porary science workshop. Ann Periodontol 2003;8:1-11.
SECTION MEMBERSJames T. Mellonig, Kevin G. Murphy, Reviewer
Group Leader Edward P. AllenMaurizio Tonetti, Chair Kenneth W. BueltmannDonald S. Clem, III, Pierpaolo Cortellini
Secretary J. Gary MaynardMichael MacNeil Robert G. SchallhornMichael K. McGuire Henry H. TakeiThomas Oates Raymond A. Yukna
302
8011.qxd 12/30/03 3:33 PM Page 302