Embed Size (px)
Citation preview

GUIDELINES FOR DESIGNING KITCHEN APPLIANCES
FOR THE ELDERLY Except where reference is made to the work of others, the work described in this thesis is my own or was done in collaboration with my advisory committee. This thesis does not
include proprietary or classified information.
_________________________________ Susan Richelle Raven
Certificate of Approval: ________________________ ________________________ Christopher Arnold Tin Man Lau, Chair Assistant Professor Professor Industrial Design Industrial Design ________________________ ________________________ Shea Tillman Stephen L. McFarland Assistant Professor Acting Dean Industrial Design Graduate School

GUIDELINES FOR DESIGNING KITCHEN APPLIANCES
FOR THE ELDERLY
Susan Richelle Raven
A Thesis
Submitted to
the Graduate Faculty of
Auburn University
in Partial Fulfillment of the
Requirements for the
Degree of
Master of Industrial Design
Auburn, Alabama August 7, 2006

iii
GUIDELINES FOR DESIGNING KITCHEN APPLIANCES
FOR THE ELDERLY
Susan Richelle Raven
Permission is granted to Auburn University to make copies of this thesis at its discretion, upon request of individuals or institutions and at their expense. The author reserves all
publication rights.
________________________ Signature of Author
________________________ Date of Graduation

iv
VITA
Susan Raven, daughter of Richard and Eleanor Raven, was born on October 22,
1981, in Lansing, Michigan. She graduated from Shaw High School in Columbus,
Georgia in 1999. In the same year, she entered Auburn University and received a
Bachelor of Mechanical Engineering in August 2003. In May 2005, she graduated with a
Bachelor of Science in Environmental Design from Auburn University. She started her
graduate career in May 2005 at Auburn University pursuing a Masters in Industrial
Design.

v
THESIS ABSTRACT
GUIDELINES FOR DESIGNING KITCHEN APPLIANCES
FOR THE ELDERLY
Susan Richelle Raven
Master of Industrial Design, August 7, 2006 (B.S., Auburn University, 2005)
(B.M.E., Auburn University, 2003)
106 Typed Pages
Directed by Tin Man Lau
The number of elderly people in the United States is growing due to the baby
boom. The life span of kitchen appliances is also growing due to new technologies that
are developed. Since the elderly will be using their kitchen appliances longer than
before, their appliances should be designed with their needs in mind.
The guidelines created in this study give specific dimensions and shapes for
features such as knobs, buttons, switches, and handles. The luminance level of lights,
frequency and decibel of sounds, and color and size of graphics are also given. To create
these guidelines, existing control standards and the aging process of humans were
analyzed.
The guidelines were applied to the design of a microwave oven.

vi
Style manual or journal used American Psychological Association Computer software used Microsoft Word, Adobe Illustrator, Adobe Photoshop

vii
TABLE OF CONTENTS
LIST OF TABLES............................................................................................................. ix LIST OF FIGURES ............................................................................................................ x I. INTRODUCTION........................................................................................................... 1
a. Problem Statement ...................................................................................................... 1 b. Need for Study ............................................................................................................ 1 c. Literature Review........................................................................................................ 2 d. Definition of Terms.................................................................................................... 8 e. Assumptions............................................................................................................... 9 f. Scope and Limits ...................................................................................................... 10 g. Anticipated Outcomes.............................................................................................. 11
II. CHARACTERISTICS OF ELDERLY ........................................................................ 12
a. Physical Changes ...................................................................................................... 12 b. Psychological Changes ............................................................................................. 16 c. Reaction Towards Technology ................................................................................. 19
III. DEVELOPMENT OF DESIGN GUIDELINES ........................................................ 20
a. Controls ..................................................................................................................... 20 i. Layout .................................................................................................................... 20 ii. Force ..................................................................................................................... 22 iii. Round Knobs ....................................................................................................... 22 iv. Pointer Knobs ...................................................................................................... 26 v. Press buttons ......................................................................................................... 27 vi. Toggle Switches................................................................................................... 30 vii. Contact Switches ................................................................................................ 32 viii. Rocker Switches ................................................................................................ 33 ix. Toaster Lever ....................................................................................................... 34 x. Feedback ............................................................................................................... 35
1. Lights ................................................................................................................ 36 2. Sounds............................................................................................................... 37
b. Handles ..................................................................................................................... 43 c. Displays..................................................................................................................... 46
i. Graphics ................................................................................................................. 46 ii. Lettering................................................................................................................ 56 iii. Colors................................................................................................................... 58

viii
iv. Digital Displays ................................................................................................... 60 d. Technology and Form of appliances......................................................................... 61
IV. GUIDELINES FOR DESIGNING KITCHEN APPLIANCES FOR ELDERLY ..... 64
a. Controls ..................................................................................................................... 64 i. Round Knobs ......................................................................................................... 64 ii. Pointer Knobs ....................................................................................................... 65 iii. Press Buttons ....................................................................................................... 66 iv. Toggle Switches................................................................................................... 67 v. Contact Switches................................................................................................... 68 vi. Rocker Switches .................................................................................................. 69 vii. Toaster Lever ...................................................................................................... 70 viii. Feeback.............................................................................................................. 71
1. Lights ................................................................................................................ 71 2. Sounds............................................................................................................... 72
b. Handles ..................................................................................................................... 72 c. Displays..................................................................................................................... 73
i. Graphics ................................................................................................................. 73 ii. Lettering................................................................................................................ 73 iii. Colors................................................................................................................... 73 iv. Digital Displays ................................................................................................... 74
d. Technology and Form of Appliances........................................................................ 75 V. APPLICATION OF GUIDELINES............................................................................ 76
a. Idea Sketches............................................................................................................. 76 b. Preliminary Models................................................................................................... 82 c. Final Model .............................................................................................................. 85 d. Summary of Project ................................................................................................. 91
VI. CONCLUSIONS ....................................................................................................... 92 VI. REFERENCES .......................................................................................................... 93

ix
LIST OF TABLES
Table 1: Index Finger Width............................................................................................. 29
Table 2: Hand Length of Elderly ...................................................................................... 31
Table 3: Hand Breadth ...................................................................................................... 35
Table 4: Intensity Level of Sounds ................................................................................... 37
Table 5: Classifications of Hearing Impairment............................................................... 39
Table 6: Preferred Listening Level of Speech Sounds by Age......................................... 40
Table 7: Hearing Loss in a Population 0-100 years old.................................................... 42
Table 8: Minimum Character Height When Viewed in Close Proximity......................... 53
Table 9: Visual Acuity vs. Age......................................................................................... 55

x
LIST OF FIGURES
Figure 1: DIP Range of Motion ........................................................................................ 23
Figure 2: PIP Range of Motion......................................................................................... 23
Figure 3: MCP Range of Motion ...................................................................................... 24
Figure 4: Hand Strength: Adults vs. Elderly..................................................................... 25
Figure 5: Ulnar Drift ......................................................................................................... 27
Figure 6: Normal and Elderly Range of Motion in Hand Joints....................................... 45
Figure 7: Existing Graphics on Kitchen Appliances......................................................... 48
Figure 8: Stroke Width, Height, and Width...................................................................... 57
Figure 9: Form of Appliances for Elderly......................................................................... 62
Figure 10: Round Knob Dimensions ................................................................................ 64
Figure 11: Pointer Knob Dimensions ............................................................................... 65
Figure 12: Press Buttons Dimensions ............................................................................... 66
Figure 13: Toggle Switch Dimensions ............................................................................. 67
Figure 14: Contact Switch Dimensions ............................................................................ 68
Figure 15: Rocker Switch Dimensions ............................................................................. 69
Figure 16: Toaster Lever Dimensions............................................................................... 70
Figure 17: Light Dimensions ............................................................................................ 71
Figure 18: Handle Dimensions ......................................................................................... 72
Figure 19: Graphic Dimensions ........................................................................................ 73

xi
Figure 20: Letter Dimensions ........................................................................................... 73
Figure 21: Digital Display Dimensions ............................................................................ 74

1
I. INTRODUCTION
a. Problem Statement
Along with the growing number of elderly people in the United States, due to the
baby boom, the life span of kitchen appliances is also improving because of advances in
technology. Therefore, people will have the same appliances for several years. As
people grow older it will be more difficult for them to use their current appliances
because they were not designed with the aging process of people in mind.
Since most kitchens have several different brands of appliances, there are many
inconsistencies when it comes to their features. With the creation of guidelines, the
inconsistency in the kitchen is eliminated. The guidelines provide specific criteria to
consider when designing, such as type of handle, size of knobs, buttons, graphics, and
colors that are adaptable to aging users.
b. Need for Study
By the year 2030, there will be approximately 70 million people in the United
States over the age 65 (Saxon & Etten, 2002). Due to the increase in the elderly
population and the longer lives of kitchen appliances, newly designed products need to
adapt to their user as they age. The guidelines show designers the existing specifications
on appliances along with the modification needed for the elderly.

2
On July 1, 2004 the annual estimate of housing units in the United States was
122,671,734 (United States Census Bureau, 2004). There are numerous kitchen
appliance manufacturers in the United States that produce several types of appliances,
and they each have their own design style. Since most kitchens contain several different
brands of appliances their features are inconsistent. The guidelines, when used, allow
kitchen appliances to be compatible with each other and are appropriate for the targeted
user. The guidelines also save designers time as they do not have to do much research to
determine what is functional for the targeted user.
c. Literature Review
The number of elderly people in the United States is growing rapidly. The United
States Census Bureau projected that the older population, 65 and over, will double from
36 million in 2003 to 72 million in 2030. By 2050, the older population is estimated to
be 86.7 million. American Housing Survey (AHS) stated, in 2001, there were 21.8
million homes in the United States where the householder was 65 or older. According to
Census 2000, 27.8% of people 65 and over live alone in the United States. Because there
is such a large number of elderly couples and elderly people living alone, products in
their homes should be designed with their needs in mind.
As a person ages, there are many physical changes that occur. Saxon and Etten
(2002) discuss several physical and physiological changes in their book. As people grow
older all of their senses become affected; these changes begin in the middle of their lives
and grow gradually with age. There is an inconsistency in the rate at which people age;
each person is different.

3
Saxon and Etten (2002) state that with age the lens of the eye becomes thicker,
denser, and less elastic, therefore they become more yellow. The “yellowing filter effect”
alters a person’s color vision, which makes is difficult to differentiate between darker
colors, such as green and blue. Cataracts, which are a common age related disorder,
cause visual loss due to the gradual increase of opacity in the lens. To compensate for the
changes in the eye, products designed for the elderly should use bright colors and larger
print.
Hearing loss can begin in the fourth decade and it gradually worsens with age.
Over half of the people over 65 and 90% of people over 80 have some hearing loss.
Hearing loss usually begins with high frequencies, and then later can affect the middle
and low frequencies. Because many elderly people can not hear high frequencies, alarms
and timers on products should use a low frequency.
Osteoporosis, which affects many older adults, causes the bones to become
porous, fragile, and brittle. Arthritis is the deterioration of articular cartilage, which
exposes the ends of the bones at the joints and results in pain and stiffness. This type of
pain restricts range of motion and worsens with the movement of joints. Products
designed for the elderly should pay close attention to the size of handles and twisting
controls.
Elderly people need stronger stimuli to activate their sensory receptors. Since the
elderly are slower in receiving information through sensory receptors, they need more
time to perform simple tasks, to process sensory information, and to respond.
Isle, Denno, and Metz (1992) discuss the changes that the eye goes through as it
ages. The lenses of the eyes become less able to change shape and bend light passing

4
through them, which is reduced by as much as one-third. It also becomes more difficult
to shift focus from far to near objects. The elderly become incapable of focusing on an
object at a close distance. Because of the aging eye, light should be increased along with
the size of graphics and lettering.
Tilley (2002) states things to consider when designing products for the elderly.
Larger visual details should be used for the elderly. The eye’s reaction time and
disability glare doubles with age. Lights need to be brighter and illumination should be
increased 20% for the elderly. An elderly person’s hand strength is reduced by 16-40%.
All of these criteria should be considered when designing any product for the elderly.
Burdman (1986) discusses the three major psychological concerns among the
older population which are depression, dementia, and alcohol and drug related disorders.
Depression can be caused by a physical illness or sensory deprivation. People with
dementia are deprived the use of part of the brain that is associated with intellectual skills
and activities. Alcoholism is a progressive illness which can develop over several years.
Designers should consider these disorders to ensure their product has simple functions
and is safe to use.
Historically, manufacturers of consumer products have made product design
decisions without considering the needs, wants and expectations of the full range of
consumers (DellaContrada, 2006). Since physical and psychological changes occur as a
person ages, products should be designed to compensate for those changes.
There are a few products that have been designed with consideration to the
elderly. Designers have developed cooking utensils especially for elderly people with
arthritis, for example a knife with thicker handle so it is easier for the user to grip (Jayson

5
& Dixon, 1974). A wide variety of tools with “easy grip” handles are available to meet
the needs of individuals who are affected by arthritis (Kelsheimer & Hawkins, 2000).
Oxo’s Good Grip produces kitchen utensils that have chunky, comfortable handles
(Jeavans, 2005). The idea came about when Sam Farber noticed his wife, who suffered
from arthritis, was struggling with her metal potato peeler (Jeavans, 2005).
TKO manufactures a turning knob operator, which is a turning device for people
with hand disabilities or arthritis. The knob operator fits over existing knobs, faucets,
valves, and keys and has a T-shaped handle for easy grip. Comfortable spoon and fork
holders are available for people with arthritis. The plastic holder slips onto existing
silverware to give a larger handle which is easier to grip.
The Rehabilitation Engineering Research Center on Technology Transfer at the
University at Buffalo helps corporations produce consumer products that are more usable
and accessible to all, including persons with disabilities and the elderly, such as
automatic jar openers and a remote control for washers and dryers (DellaContrada, 2006).
Black & Decker produces the Automatic Lids off jar opener and Whirlpool will introduce
a new interactive device for washers and dryers that will enable remote operation and
interaction of those appliances (DellaContrada, 2006).
Several products have been created for the kitchen specifically for the elderly,
which makes it easier for them to accomplish necessary tasks. However, kitchen
appliances designed with the elderly in mind were not mentioned. They are a major part
of the kitchen and their design should be changed to accommodate the changes that occur
in the aging process.
6
Other things are done in the kitchen to help the elderly work efficiently; for
example, raising the oven and dishwasher six inches off the floor can make it easier to
transfer food or dishes to the countertop and cuts down on bending (Winfield, 1999).
Non-glare, matte finish countertops with contrasting color edging can help people with
diminishing eyesight distinguish where the counter ends (Winfield, 1999). Counter
heights can be varied and the installation of pull-out work spaces can provide easier
access for the elderly (Hardwood Manufacturers Association, 2001).
Although there are tips for how a kitchen should be designed, several different
kinds of utensils, and gadgets to accommodate the elderly, there are no kitchen
appliances designed specifically for them. Since kitchen appliances are the most used
thing in the kitchen, they should be designed with consider for the elderly. It is as if
kitchen designers are using existing products and adapting them to the elderly, when they
should be designing the products specifically for the elderly from the beginning.
The Human Factors Design Handbook by Woodson (1992) discusses a wide
range of controls including resistance needed to activate along with visual and auditory
displays. The criterion given is general and can be used for any product; it is not
specifically for kitchen appliances. Basic dimensions of the body of males and females
70 and over in the 5th, 50th, and 95th percentile are given. The only dimensions that are
relevant to determine control specifications are the tables containing information about
the hands. These dimensions alone are not enough to determine control specifications for
the elderly; more specific information is needed. Even though Woodson has given this
information about males and females over 70, it is not at all mentioned in the control
specifications.

7
Woodson also discusses the strength of humans in relation to control operation.
Many forces are listed for different types of movements and controls. However, nothing
is said about what the force should be if the operator is elderly. Some of the forces are
classified by 5th, 50th, and 95th percentile, with this type of table it is not known who or
what age group is in which percentile.
The Human Factors Design Handbook (Woodson, 1992) suggests when beginning
the design process, the designer should find out who will be using the product, how they
feel about its adequacy and ease with which the job can be done. This is contradictory of
the information discussed above; Woodson gives human factors criteria that only focus
on the “average” user, the information does not include the elderly.
Honeywell Inc. (1992) has produced Human Factors Guidelines for the Elderly
and People with Disabilities. In arriving at the guidelines, specific changes that occur in
the aging process are discussed, along with a wide range of physical, perceptual, and
cognitive impairments, including blindness, paralysis, complete hearing loss, and severe
mental retardation. Specific percentages of loss are given, which aid in arriving at the
appropriate specification for the elderly. Many types of controls are given with
appropriate specifications for the elderly; however, no development of the guidelines
could be found. They are just listed without reason supporting those specifications.
Reasoning or existing specifications should be given along with the guidelines so one can
see the need for the change. It is very difficult to make guidelines that include everyone
from the blind to the mentally retarded because they have completely different needs.
The guidelines should focus on the normal aging process of a human to satisfy the
majority of the population.

8
Design guidelines for kitchen appliances for the elderly need to be developed;
they would be based on the aging process of humans and existing feature specifications.
Generally, when products are made more accessible to people with limitations, they are
usually easier for more able-bodied people to use. Some benefits include lower fatique,
increased speed, and lower error rates (Vanderheiden, 1990).
d. Definition of Terms
1. alcoholism – a diseased condition caused by the excessive or continuous use of
alcoholic liquors.
2. arthritis – inflammation or degenerative changes in body joints.
3. audition – the sense of hearing.
4. cataract – is a cloudy or opaque lens severe enough to interfere with light rays passing
through the lenses and causing impaired vision.
5. cerumen – the wax or yellow matter secreted by the glands of the external ear.
6. compression – pressed together, make more compact by or as by pressure.
7. concave – hollow and curved like a section of the inner surface of a spherical body.
8. dementia - a syndrome of progressive and global decline in cognitive capabilities,
severe enough to substantially interfere with the individual’s well being and social
function (age related disorder).
9. depression – low spirits, gloominess, dejection, sadness.
10. electroencephalogram (EEG) – records brainwave patterns from the continuous tiny
electrical signals coming from the brain. The EEG machine then magnifies the size of

9
these signals, without affecting the brain, so that the information can be recorded on
paper or computer.
11. gustation – the sense of taste.
12. kinesthetic – the sensation of position, movement, tension, etc. of parts of the body,
perceived through nerve end organs in muscles, tendons, and joints.
13. olfaction – the sense of smell.
14. ossicle – a small bone or bonelike structure; especially, any of the three small bones
in the tympanic cavity of the ear.
15. osteoporosis – gradual progressive change causing a rate of bone resorption greater
than bone formation with the result that bone mass is reduced; bones become porous
and more fragile but the chemical composition of the bone remains normal.
16. pinna - in anatomy, the external ear; auricle.
17. presbycusis – the gradual loss of acute hearing with advancing age.
18. pupil – the contractile circular opening, apparently black, in the center of the iris of
the eye.
19. purchase – grip.
20. shear – shearing stress
21. suicide – the act of killing oneself intentionally.
22. tactile – having the sense of touch.
23. vestibular – balance.
24. yellow filter effect – yellowing of the lenses.
e. Assumptions

10
• Kitchen appliances are not designed to adapt to people as they age.
• Existing specifications of kitchen appliance features are not adequate for elderly
users.
• Kitchen appliance features are inconsistent from brand to brand.
• Adults and elderly people have multiple appliances of multiple brands in their
kitchens.
• Elderly people are only affected by the “normal aging process”.
• Overhead lighting of elderly peoples’ kitchens has not been enhanced; it is the
same amount as adults’ kitchen.
f. Scope and Limits
Scope
• Aging process of humans: physically, psychologically, and acceptance of
technology.
• Existing control, handle, display, and form specifications on kitchen appliances.
• Define new control, handle, display, and form specifications for the elderly using
the changes that occur as a person ages.
Limits
• People in United States
• Adults age: 16-64 years old
• Elderly age: 65-79 years old

11
g. Anticipated Outcomes
Guidelines will be created for elderly users using existing feature specifics along
with the aging process of humans. Research findings will be used to determine specifics
for features such as handles, knobs, buttons, text, color, and graphics. The guidelines will
outline the cross section, diameter, and length of handles. Knobs will be defined by their
shape, diameter, and depth. Buttons will be specified by their shape and size. The height
and color of text will be given along with the size and color of graphics.
It is expected that although features will be similar for the adult and elderly users
adaptations will be needed for the elderly user such as larger graphics, brighter lights,
louder sound, more color contrast, and less resistance.

12
II. CHARACTERISTICS OF ELDERLY
a. Physical Changes
As people age, their sensory systems are affected: vision, hearing, taste, smell,
touch, balance, and muscle sense (Saxon and Etten, 2002). Sensory changes begin in the
fourth and fifth decade with a gradual reduction in sharpness, but they do not appreciably
limit behavior until about the seventh and eighth decade (Saxon and Etten, 2002). The
measurement of the decrease in functionality of a given sensory system cannot enable
one to predict an older person’s unique behavior capabilities or limitations associated
with the particular sensory loss (Saxon and Etten, 2002). There is significant variation
among individuals in the rate of aging. The amount of loss is highly variable from one
organ system to another within a given individual (Saxon and Etten, 2002). Humans can
adapt and compensate for gradual changes (Saxon and Etten, 2002). Some sensory
systems are more important in everyday functioning than others, for example, vision is
more important than the sense of smell (Saxon and Etten, 2002). As a person ages it
takes stronger stimuli to activate their sensory receptors; lights need to be brighter,
sounds louder, and smells stronger (Saxon and Etten, 2002).
Eyes
The lenses of the eyes have two important functions in vision, refraction and
accommodation, both of which are affected by aging (Saxon and Etten, 2002).
Refraction requires crystalline clear lenses, while accommodation requires the lenses to

13
be elastic and able to change shape (Saxon and Etten, 2002). The lens of the eye
becomes less able to change its shape and bend the light rays passing through it (Caldwell
and Hegner, 1986). The decrease in the refractive power of the lens in shifting focus
from far to near objects reduces from a peak of 14 diopters at 8 years old to less than 2
diopters at age 50 (Isle, Denno, and Metz, 1992). When a person reaches 60 years old
their lens is incapable of focusing on an object at close distance (Isle et al, 1992). The
pupil size increases as a person ages, which reduces the amount of light that enters by as
much as one-third; therefore, this reduces the abilitly to detect details (Isle et al, 1992).
The lenses grow with age by adding layers (Saxon and Etten, 2002). Between the ages of
20 and 80 the width of the lenses increases by 50% (Saxon and Etten, 2002). As a result,
they become thicker, denser, and less elastic (Saxon and Etten, 2002). As the lenses
become denser, they also become more yellow, impairing their refractive ability (Saxon
and Etten, 2002). Yellowing of the lenses or the “yellow filter effect” produces changes
in color vision, although many older adults remain unaware that color discrimination has
altered (Saxon and Etten, 2002). Older people with distorted color perception are often
able to differentiate between bright colors such as reds and yellows better than between
darker colors such as blues and greens (Saxon and Etten, 2002). Color blindness tends to
increase, especially among men (Caldwell and Hegner, 1986). Peripheral vision is
reduced, especially in dim light (Caldwell and Hegner, 1986). Additionally, the eye’s
reaction time and disability glare doubles with aging (Tilley, 2002). Cataracts, the most
common age related disorder of the eye, affect approximately 90% of those people over
70 and are the single most important cause of blindness in old age (Saxon and Etten,
2002). A cataract is a cloudy or opaque lens that interferes with light rays passing though

14
the lens and causes impaired vision (Saxon and Etten, 2002). Visual loss is due to a
gradually increasing opacity of the lens (Caldwell and Hegner, 1986). The lens is
originally a clear crystalline body enclosed in a capsule which changes its shape in order
to bend the light rays to focus on the retina (Caldwell and Hegner, 1986). If the lens is
opaque, light cannot pass through it; therefore, vision is lost (Caldwell and Hegner,
1986). For older adults, lights need to be brighter and illumination should be increased
20% (Tilley, 2002).
Hearing
Changes in a person’s hearing usually begin in their fourth decade and progress
gradually with age (Saxon and Etten, 2002). Approximately 60% of people over 65 and
perhaps as many as 90% of people over age 80 have some hearing impairment (Saxon
and Etten, 2002). Presbycusis is the most common cause of hearing loss in the older
population and is caused by physiologic aging. It usually results in high frequency
hearing loss and should not be diagnosed until all other possibilities are eliminated.
Hearing loss often goes undetected and untreated in older adults. In our culture, men
tend to have hearing loss earlier than women, partly because men generally have been
exposed to more prolonged occupational noise than women (Saxon and Etten, 2002). As
a person ages there are specific changes that occur in their ears. The pinna in the outer
ear loses some flexibility and becomes longer and wider (Saxon and Etten, 2002). Hairs
in the external ear canal become stiffer and the drying and thinning of tissues in the
external ear canal contribute to a likelihood of cerumen accumulation with age (Saxon
and Etten, 2002). Cerumen is ear wax that is produced in the later years and is of thicker
consistency and is not always easily removed (Saxon and Etten, 2002). Cerumen in the

15
external ear canal is responsible for a substantial amount of hearing impairment (Saxon
and Etten, 2002). Changes in the membranes of the middle ear and the ossicles impair
transmission of sound vibrations but do not impair hearing significantly (Saxon and
Etten, 2002). With age, auditory loss generally affects perception of high frequencies
first. Later, age related changes may involve middle and low frequency ranges as well
(Saxon and Etten, 2002).
Bones and Joints
Osteoporosis is the most common metabolic bone disease in older adults (Saxon
and Etten, 2002). It is a gradual, progressive change causing a rate of bone resorption
greater than bone formation with the result that bone mass is reduced (Saxon and Etten,
2002). The bone becomes porous and more fragile, but the chemical composition of the
bone remains normal (Saxon and Etten, 2002). The porous bones eventually become
fragile and brittle (Saxon and Etten, 2002).
Arthritis is an inflammation or degenerative change in body joints (Saxon and
Etten, 2002). Three common types of arthritis are osteoarthritis, rheumatoid, and gout
(Saxon and Etten, 2002). Osteoarthritis is the most common and leading cause of
disability in those over 65 (Saxon and Etten, 2002). 85% of people over 65 have
osteoarthritis (Steven, 1987). Osteoarthritis involves the progressive loss of articular
cartilage, exposing the ends of the bones at the joints and resulting in pain and stiffness
(Saxon and Etten, 2002). This pain restricts range of motion in the fingers and worsens
with movement of the joints. To help relieve the pain, people with arthritis will often
keep their fingers bent. While this temporarily relieves discomfort, holding a joint in the
16
same position for too long can cause permanent loss of mobility and hinder daily
activities.
In a normal adult, range of motion for the distal interphalangeal joint (DIP), the
outer most joint on the finger, is extension = 0 degrees and flexion = 80 degrees (Eaton,
1997). The range of motion for the proximal interphalangeal joint (PIP), the middle joint
on the finger, is extension = 0 degrees and flexion = 100 degrees (Eaton, 1997). The
range of motion for the metacarpophalangeal joint (MCP), the knuckle joint, is
hypertension = 0 to -45 degrees and flexion = 90 degrees (Eaton, 1997). The range of
motion in the fingers of someone with arthritis is severely limited; it ranges from 17 to 40
degrees for each joint (Bieber, Weiland, and Volenec-Dowling, 1986). The extension
deficit average in people with arthritis is about 47 degrees (Swanson, 2005).
People with arthritis have difficulty performing every day tasks, such as opening
jars, buttoning shirts, and tying shoes. An elderly person’s hand strength is reduced by
16-40%. The loss of strength, manual dexterity and decrease of range of motion due to
bone disease should be taken into account when designing any product.
b. Psychological Changes
With age, nervous system activities are slowed (Saxon and Etten, 2002). Older
adults are usually slower in receiving information through sensory receptors, slower in
transmitting, processing, and interpreting information and somewhat slower in acting
upon it (Saxon and Etten, 2002). Increased time is needed for an older person to perform
simple tasks and to process sensory information and to respond (Saxon and Etten, 2002).
Action does not respond as rapidly to the will, and it requires greater motor impulse to

17
perform the act while greater mental concentration is required to obtain and hold sensory
impressions (Nascher, 1979). Responding to multiple or complicated stimuli is more
difficult (Saxon and Etten, 2002). It is slightly more difficult for older adults to learn
new motor skills than younger people. Elderly people also need more trials to achieve
the same degree of learning as a younger person (Stokes, 1992). Learning still occurs at
an old age, it is just slower and more difficult. There is no serious decline in sensory
information until after 70 (Caldwell and Hegner, 1986). After this time many elderly
need more time to process sensory information and to respond (Caldwell and Hegner,
1986). Sensory receptors, in general, are less reactive, and stronger stimulation is needed
to elicit a response.
Sleep patterns change with age (Saxon and Etten, 2002). Although older adults
spend more time in bed trying to sleep, their total sleep time is less than in younger years,
and the time it takes to fall asleep increases (Saxon and Etten, 2002). Frequent rest
periods are mandatory (Caldwell and Hegner, 1986). They tire more easily and have
little vitality (Caldwell and Hegner, 1986). Sleep deprivation and decreased nervous
system response result in a decrease of cognitive function in the elderly which can limit
their ability to use appliances.
Depression, dementia, and alcohol and drug related disorders are three major
concerns among the older population (Burdman, 1986). Women ages 65-84 are more
likely than men to have severe depression symptoms. Among people 85 and older, men
and women have a similar prevalence of severe depressive symptoms, accounting for as
high as 23%. The rate of depression increases with age.
18
Depression may be caused by a variety of factors that often represent a loss of
some type to the individual (Burdman, 1986). Physical illnesses such as strokes,
respiratory infections, cancers, heart disease, and arthritis are among many disorders that
can induce depression (Burdman, 1986). Another source of depression in older people is
sensory deprivation (Burdman, 1986). Hearing or visual loss may cause older people to
withdraw from interaction with others (Burdman, 1986). Closely related to depression is
a high risk for alcoholism which is known to increase with age (Burdman, 1986).
Alcoholism is usually a progressive illness developed over a period of five to
twenty years (Burdman, 1986). Alcohol and other drug related problems among the
elderly are increasing as the number of older people multiplies (Burdman, 1986).
Dementia is an age related disease of the brain that results in the progressive loss
of mental faculties, beginning with the memory, learning, attention, and judgment
(Burdman, 1986). People affected by dementia are deprived of the use of parts of the
brain associated with a range of intellectual skills and activities (Burdman, 1986). It is
estimated that 5% of the United States population age 65 and over is severely demented,
10% may be mildly to moderately impaired, and 85% is without the illness (Burdman,
1986). Older people with moderate or severe memory impairment ranged from about 4%
among the 65-74 year olds to 36% among people 85 and older (Tepper and Cassidy,
2004). When designing appliances, consideration needs to be given to simple function
and safety.

19
c. Reaction Towards Technology
Many older people are less exposed to new technology than a younger generation,
which can make them feel intimidated (Eisma et al, 2003). As elderly grow closer to the
end of their lives, they begin to have no desire to try new things (Day). They also feel
that they have no need for new technologies around the house. People who are
accustomed to older technologies may not be aware of the new technologies available
(Eisma et al, 2003). Older people’s opinions about new technology are often based on a
limited number of experiences or stories that they have heard from friends or relatives
(Eisma et al, 2003).
20
III. DEVELOPMENT OF DESIGN GUIDELINES
There are many different interactive components on kitchen appliances that
require different uses of the body, such as eyes sight, hearing, and gripping. As people
age their senses and function ability reduces. Therefore, products for the elderly need to
have larger text, louder sounds, and decreased resistance. This section reviews existing
specifications for components found on kitchen appliances. Using this information and
analyzing the aging process of humans, design guidelines for the elderly are created.
a. Controls
i. Layout
Controls should be placed so they are easy for the elderly to use. We are
conditioned for a top to bottom and left to right scanning (Wildbur, 1989). Thus, the
simplest way to group controls is in a continuous line either vertically or horizontally
(Wildbur, 1989). Sequential operations should flow smoothly by placing controls in
close proximity (Corlett and Clark, 1995). The grouping of five controls in a horizontal
arrangement is ideal as the eye can easily make the choice between the one in the center,
which acts as a datum, and those to the left and right (Wildbur, 1989). Beyond five
controls, errors of selection increase rapidly (Wildbur, 1989). In terms of vertical
stacking, two or three rows are the most that should be used, giving a matrix of 10-15
units (Wildbur, 1989). Arrange controls of similar function together (Wildbur, 1989).
21
Where there is no natural sequence of operations or where some of the controls will be
used infrequently, group the controls into areas or zones designated by use or function or
define them by color or background (Wildbur, 1989). Each control should have only one
function and the number of controls must be kept to a minimum (Peterson, 1998).
Controls should be easy to read and operate, with high contrast and redundant cuing or
cues that are audible, tactile and visual (Peterson, 1998). Sufficient clearance should be
provided between adjacent controls so that critical controls can be easily grasped and
manipulated (Woodson, 1992). Arrange related controls in same area, sequence of use—
left to right, top to bottom, most frequently used in the most convenient place, emergency
controls—where the operator does not have to search or reach for control (Woodson,
1992). The size and shape of handles, knobs, and buttons should be compatible with the
size of the operator’s hand (Woodson, 1992). The shape of a control should also be
compatible with the kind of grip or motion required to operate the control interface
(Woodson, 1992). The control should be chosen as though it were an extension of the
operator’s limb (Woodson, 1992). Create displays that are easy to read and interpret, as
opposed to displays that are merely attractive and/or startling to look at. Avoid
decorative displays, it hurts readability and interpretation. The more complex the
display, the more time it takes to read and interpret the information provided by the
display, and the more apt the operator is to misinterpret the information or fail to use it
correctly. Some key issues for labels are legibility, size in relation to viewing distance,
illumination, clarity of meaning, and location.

22
ii. Force
Force is exerted more effectively when the hand and handle are in compression
rather than shear (Pheasant, 1996). It is better to exert a force perpendicular to the axis of
a cylindrical handle than along the axis (Pheasant, 1996). If controls are used for a short
amount of time, their resistance should be high (Ivergard, 1989). If controls are used for
a long period of time they should have a low resistance (Ivergard, 1989). The resistance
should increase gradually and then disappear when the button is activated (Ivergard,
1989). Controls that require dual motion, such as pressing down and turning, are difficult
for many people to use (Ivergard, 1989). Controls must have enough resistance to
prevent their activation by mistake and be designed to handle misuse (Ivergard, 1989). In
an emergency situation very high forces are often applied and the control must be able to
withstand these (Ivergard, 1989).
iii. Round Knobs
Round knobs can be found on ovens and toasters. A circular knob implies that the
knob turns continuously and makes it easier for the operator to reposition his or her
fingers for multi-turn manipulation (Woodson, 1992). If knobs have to be very small in
diameter, they should be deeper and have serrations (Woodson, 1992). If a precise knob
rotation is required, the knob should be large enough so that all the user’s fingers and the
thumb can be placed on the knob rim and/or surround the knob edges if considerable
torque is required (Woodson, 1992).

23
For adult users, the minimum dimensions of a round control knob are 0.25”
diameter and 0.75” depth (Woodson, 1992). This size knob should include serrations and
should have 2-4 in-oz of resistance (Woodson, 1992). The preferred minimum round
knob diameter is 0.5” diameter and 0.5” deep with serrations (Woodson, 1992). Four in-
oz of resistance is the maximum for this size knob (Woodson, 1992). As the diameter of
the knob increases the resistance also increases because the knob will be easier to grip
(Woodson, 1992).
Since most elderly people have arthritis, the range of motion in their hands
becomes limited as well as their hand strength. Figures 1, 2, and 3 illustrate the
difference in range of motion of the finger joints for normal adults and elderly adults.
Figure 1: DIP Range of Motion

24
Figure 2: PIP Range of Motion
Figure 3: MCP Range of Motion

25
Figure 4: Hand Strength: Adults vs. Elderly
Figure 4 shows the difference in hand strength for adults and elderly.
Due to the limited range of motion and the hand strength of the elderly, the
diameter of round knobs should be increased along with a decrease in resistance. Round
knobs for the elderly should be serrated and have a diameter of 1”-2” and a depth of 0.5”-
0.75”. Since hand strength of the elderly reduces 16-40% (Tilley, 2002), the resistance
for these knobs should be no more than 3 to 6 in-oz.

26
iv. Pointer Knobs
Pointer knobs can be found on ranges, ovens, coffee makers, and toaster ovens. A
pointer knob implies that it is a positioning control that can be positioned in discrete
increments (Woodson, 1992). Knobs with indents let the operator “feel” that the knob is
properly positioned (Woodson, 1992). A pointer knob with a sloped point allows for a
better view of the pointer tip, therefore fewer mistakes would be made (Woodson, 1992).
Pointers should move right, up, or clockwise to indicate a value increase (Woodson,
1992). Knobs with moving pointers should be used over knobs with moving scales
because they are easier to read (Ivergard, 1989).
For adult users, the length of the pointer knob is between 1”-2”. The width is
between 0.25” and 0.5” and the height is 0.5” (Woodson, 1992). The torque required to
turn a pointer knob is 10 to 45 in-oz (Woodson, 1992).
Figures 1 through 3, which show joint range of motion, Figure 4, which illustrates
hand strength of adults and elderly, and Figure 5, which illustrates the average ulnar drift
for an elderly person with arthritis, are considered in the development of the new
specifications for pointer knobs. Having an ulnar drift and limited range of motion
makes it difficult to grip a pointer knob; therefore, the width of the pointer should be
enlarged to 0.5”-0.75”. The length of the pointer should be between 2”-3”; this length
allows more fingers to grip the knob. The height of the knob should be 0.75” to ensure
enough contact with the control. The resistance needed to turn this size pointer knob
should be between 6 in-oz and 27 in-oz.

27
Figure 5: Ulnar Drift
Bieber, Weiland, Volenec-Dowling, 1986.
v. Press buttons
Press buttons are suitable for starting and stopping or for switching on or off and
are found on ovens, blenders, and coffee makers (Ivergard, 1989). In order to indicate

28
the button has been activated, some kind of feedback should be emitted, either a sound or
light (Ivergard, 1989). Press buttons should be designed so that the fingers will not slide
off them (Ivergard, 1989). The surface should be made concave or have some form of
increased friction (Ivergard, 1989). A press buttons is an effective emergency control
device for shutting off machines in a hurry (Woodson, 1992). In this type of application
the button should be larger so the operator does not have to very accurate when pressing
the button (Woodson, 1992).
For normal users, the smallest diameter for a press button should be no less than
0.25” (Woodson, 1992). If the press button is 0.75” or larger in diameter, it should have
a concave top (Woodson, 1992). When press buttons are placed in a row horizontally or
vertically, the distance between them should be 0.1875” (Woodson, 1992). The average
resistance for a press button is between 10 and 20 in-oz (Woodson, 1992).
Table 1, which displays the index finger width for men and women in the 5th, 50th,
and 95th percentile, is considered when arriving at the correct press button diameter for
the elderly. The diameter should be between 0.5” and 0.75” for elderly users because the
majority of the users’ index finger will fit on the button. This size press button should be
concave, so the user’s finger will not slide off. The distance between press buttons
should be increased to 0.25” to ensure the correct placement of the finger on the button.
Since the hand strength of an elderly person is reduced, the resistance needed to activate a
press button should be between 6 and 12 in-oz.

29
Table 1: Index Finger Width
Tilley, 2002.

30
vi. Toggle Switches
Toggle switches make good controls as they provide feedback of the movements
made. A two position toggle switch is better than one with three positions because of the
limited distance between positions (Woodson, 1992). The maximum range of movement
for a toggle switch is 60 degrees. There are different types of toggle switches; the most
common has a spherical end and tapers down as it gets closer to the product (Woodson,
1992). One has a skinny cylindrical rod to toggle; another has a round ball on the end
and a cylindrical rod connecting it to the product (Woodson, 1992). The last toggle
switch has a flat top and bottom, which allows for better grip on the switch (Woodson,
1992). If a number of toggle switches are used they should be placed in a horizontal row
(Woodson, 1992). Toggle switches can become dangerous if they are too long
(Woodson, 1992).
For normal users, the most common type of toggle switch is used. The minimum
length of the switch is 0.5” while the maximum is 2” (Woodson, 1992). The tip of the
switch can range from 0.125” to 1” in diameter (Woodson, 1992). If toggle switches are
lined up horizontally, the minimum distance between them is 0.75” while 2” is optimum
(Woodson, 1992). The resistance required to control a switch is 10 in-oz for a small
switch and 40 in-oz for a large switch (Woodson, 1992).
A toggle switch that has a flat top and bottom should be used for elderly users
because their fingers will be less likely to slip off the switch. To determine the length of
the switch, Table 2 was used, which shows the hand length for elderly men and women in
the 5th, 50th, and 95th.

31
Table 2: Hand Length of Elderly
Tilley, 2002.

32
The index distal phalanx is 8.6% of the hand length in men and women (Davidoff
and Freivalds, 1993). Using that and the hand lengths shown above, the average index
distal phalanx is between 0.49” and 0.65”. Therefore, the flat end of the toggle switch
should be 0.5” to 0.625” long and 0.375” wide. The width of the toggle switch is more
than half the index finger width in all but one percentile from Table 1. Since it is not
necessary to grip the toggle switch to operate it, the height of the flat switch should be
0.125”. Toggle switches lined up horizontally should be separated by at least 1” to
ensure the wrong switch is not hit by mistake. Toggle switches designed for the elderly
should have 9 to 12 in-oz of resistance.
vii. Contact Switches
Contact switches, which are used on microwaves, dishwashers and ovens, give no
3-dimensional feedback (Woodson, 1992). This type of switch should not be used for
critical functions (Woodson, 1992). If this type of switch is used, clear visual or auditory
feedback should be provided (Woodson, 1992). Clear graphic delineation of switch
boundaries and graphic distinction between switches and purely visual displays should be
used (Woodson, 1992). Contact switches are very useful where frequent cleaning is
necessary (Woodson, 1992).
For normal users, the standard size of a rectangular contact switch ranges from
0.5” x 0.5” to 0.625” x 0.75”. A rectangular contact switch that ranges from 0.5” x 1” to
0.75” x 1.25” is used for “Start” and “Cancel” buttons. Circular contact switches are also
used, which are 0.5” in diameter. These types of switches require 1 to 5 in-oz of force to
operate (Woodson, 1992).

33
The index distal phalanx length calculated above and the index finger width from
Table 1 are used in obtaining the size of the contact switches for the elderly. The height
of the switch should be 0.625”, and the width should be 0.875”. This size will
accommodate the length and width of the index distal phalanx. The size of the “Start”
and “Cancel” buttons should be at least 0.625” in height, and the length should be
between 1” and 1.25”. If a circular contact switch is used, the minimum diameter should
be 0.625”, which accommodates the length of the index distal phalanx. The resistance
needed to operate these types of switches should be reduced to 3 in-oz. Because there is
no 3-dimensional feedback with this type of switch, a light or sound should be associated
with the activation of a switch.
viii. Rocker Switches
Rocker switches can be found on coffee makers, ovens, blenders, and mixers.
They are a good substitute for toggle switches because they provide a good physical
indication of the switch position (Woodson, 1992). Since toggle switches protrude out,
things can easily be snagged on them (Woodson, 1992). 30 degrees of travel by the
switch is recommended (Isle, 1992). Rocker switches should snap into position with an
audible click (Woodson, 1992).
The majority of rocker switches found on kitchen appliances are oval, and their
height ranges from 0.5” to 1”while their width ranges from 0.625” to 1.5”. The circular
switches ranged from 0.5” to 0.625” in diameter. The square shaped rocker switches
found were 0.375” x 0.5”. Some rocker switches had red of green lights to indicate when

34
the switch had been activated. The force needed to activate a rocker switch is 10-40 in-
oz (Isle, 1992).
An oval shaped rocker switch should be used for the elderly. A circular rocker
switch does not give enough room for the user’s finger to fit on the switch. The square
rocker switch has hot spots on the corners of the switch, which are not comfortable to its
users. Table 1, which gives the finger width of men and women, was used to determine
the size of oval rocker switches. Rocker switches for the elderly should range between
0.5” to 0.625” in height and 1” to 1.25” in length. To ensure the grip the surfaces should
be concave. Having an activation light would cause less confusion during operation. A
rocker switch designed for the elderly should have a resistance between 6 and 16 in-oz.
ix. Toaster Lever
Toaster levers are what the user pushes down to begin toasting. On existing
toasters, the levers ranged from 0.875” to 3.125” wide and 0.75” to 1.25” deep.
Toaster levers designed for elderly should be large enough so that a couple of
their fingers will fit on the lever. This will ensure control over the lever and will reduce
slippage. To arrive at the proper width of the lever, Table 3, which shows the hand
breadth for men, women, and elderly men, was used. Table 3 says that the hand breadth
of a 95th% elderly man is 3.6”. The lever does not need to accommodate all fingers; a
lever that can fit two to three fingers is sufficient. The width of the lever should be at
least 2” and get larger if desired. To arrive at the depth of the lever the index distal
phalanx length was used, which was calculated from Table 2. The index distal phalanx
ranges between 0.49” and 0.65”; therefore, the depth of the lever should be around 0.75”.

35
This distance ensures that the 95th% elderly man’s fingers will fit on the lever with extra
room between the fingers and the toaster.
Table 3: Hand Breadth
Tilley, 2002.
x. Feedback
Controls must give feedback, a light or sound, so that the operator knows when it
has been activated, even when it has been done by mistake (Ivergard, 1989). The control

36
interface should provide feedback so the operator knows at all times what his or her input
is accomplishing.
1. Lights
To determine the brightness of lights on appliances for elderly users, many things
are considered, such as the deterioration of their eye sight and the luminance level needed
in kitchens. For adult users, the luminance level of a light on an appliance should be at
least 10% greater than the surrounding luminance (Woodson, 1992). The maintained
average illumination level in a kitchen is 300 lux, while the food preparation areas have
an average of 500 lux (Oregon). Since most appliances are on the counter in the food
preparation area, 500 lux will be used as the surrounding luminance level. For adults the
luminance level of a light on an appliance should be 550 lux. Since the illumination for
the elderly should be increased 20%, the luminance level of a light on an appliance
should be 650 lux. The majority of lights on appliances that are associated with a control
movement are red; however, some are yellow and green. The light color should remain
the same on appliances designed for the elderly; changing it may cause confusion. The
majority of lights found on appliances are circular and have a diameter of 0.125”. Some
circular lights have a diameter as high as 0.25”, but none went below 0.125” in diameter.
Oval shaped lights are also used on appliances; they average 0.5” wide by 0.125” to 0.25”
high. The diameter of circular lights for elderly users should be increased to at least
0.1875”, to ensure visibility. The size of the oval shaped lights can remain the same as
they are for adult users because they are already large enough.
37
2. Sounds
Sounds in a kitchen are found on microwaves, ranges, wall ovens and
dishwashers. Audible tones are heard after buttons are activated and when a timer
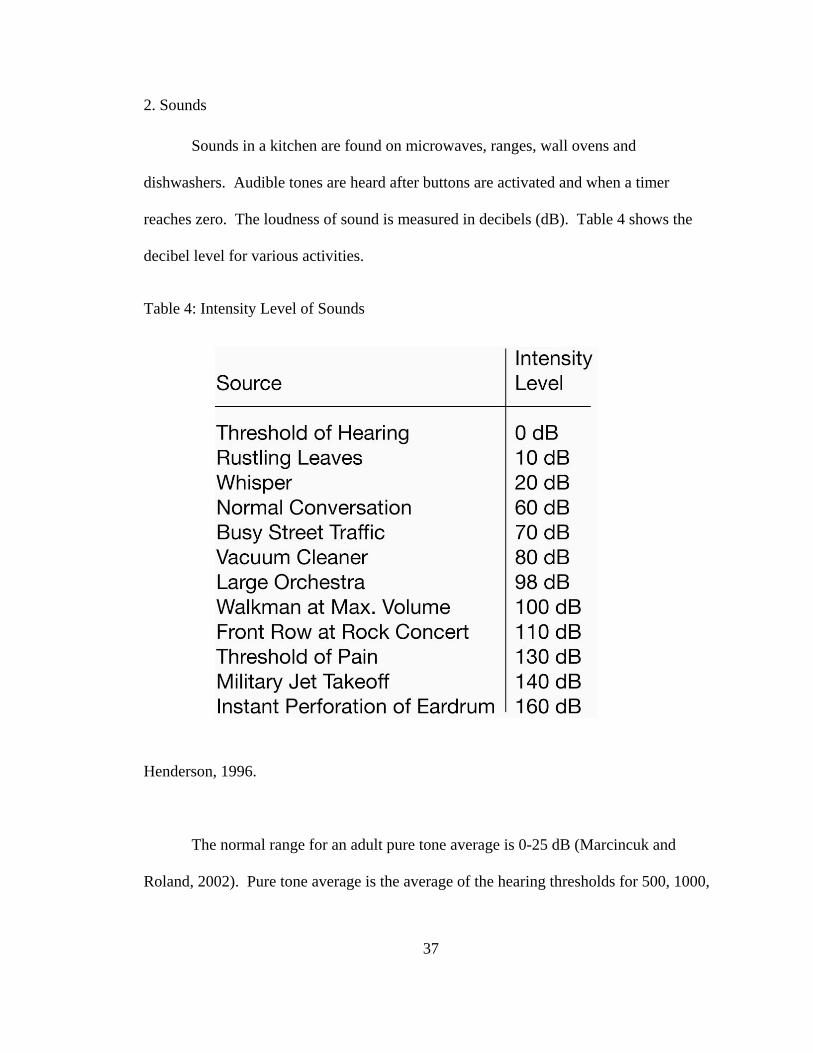
reaches zero. The loudness of sound is measured in decibels (dB). Table 4 shows the
decibel level for various activities.
Table 4: Intensity Level of Sounds
Henderson, 1996.
The normal range for an adult pure tone average is 0-25 dB (Marcincuk and
Roland, 2002). Pure tone average is the average of the hearing thresholds for 500, 1000,

38
and 2000 Hz, which are the most important frequencies of speech (Marcincuk and
Roland, 2002).
The frequency, the pitch of a sound, is measured in Hertz (Hz). A low frequency
can be heard from a bass drum or tuba and ranges from 125-750 Hz (Burmark and
Fournier, 2003). A high frequency can be heard in a bird chirping or a flute playing. A
low frequency sound must have a higher decibel level in order to “sound” as loud as a
higher frequency sound. A young person can hear frequencies in a range from 0-20,000
Hz (The Hyperacusis Network). By the time that person reaches forty years old, that
range has been decreased to 0-12,000 Hz (The Hyperacusis Network). Many elderly
people can only hear up to 8,000 Hz (The Hyperacusis Network). As people age it
becomes harder for them to hear higher frequencies (Poulson, 1996). If an elderly
person’s hearing threshold shifts by 40 dB it does not mean that their suprathreshold also
shifts (Isle, Denno, and Metz, 1992). The decibel level that they can hear comfortably is
limited (Isle, Denno, and Metz, 1992). Table 5 shows classifications of hearing loss
based on decibels (Davis, 1978). Table 6 shows the preferred listening level of speech
for people ages 15 – 85 (Coren, 1994).

39
Table 5: Classifications of Hearing Impairment
Davis, 1978.

40
Table 6: Preferred Listening Level of Speech Sounds by Age
Coren, 1994.

41
For normal users, auditory tones have a frequency of 30-3,000 Hz; the ear is most
sensitive at this range (Tiresias, 2006). This frequency of audible tone does not cause
alarm, but attracts attention (Woodson, 1992). Standard auditory tones range from 62-80
dB. Using the sound level preferred for 15 year olds from Table 6, which is 54 dB, there
is an 8 to 26 dB increase for auditory tones above the preferred listening level.
Studies were found giving an estimation of hearing loss for elderly people. A
study was conducted by A. J. Duquesnoy (1983) with elderly people that had moderate,
nearly symmetrical pure-tone hearing losses with an average loss at 500, 1000, and 2000
Hz of between 9 and 40 dB. Another study was conducted by S. Arlinger (1990) with
elderly people with presbycusis and their pure-tone hearing loss ranged from 11 to 70 dB
with an average of 40 dB. Table 7, illustrates the hearing loss in decibels and frequency
in people 0 to 100 years old.

42
Table 7: Hearing Loss in a Population 0-100 years old
Isle, Denno, Metz, 1992.
43
Using the studies by Duquesnoy (1983) and Arlinger (1990) and Table 7, 40dB is
used as the threshold of hearing for the elderly. Referring to Table 6, the preferred
listening level for the elderly at the age of 85 is 85 dB. Using the same auditory tone
increase for adults, the tone should be 8-26 dB above the preferred listening level, which
would be 93-111 dB. Using Table 4, 111 dB would feel like the person was at a rock
concert, which would be damaging to their ears. Therefore, the decibel range for
auditory tones for the elderly should be between 93 and 98 dB. Since elderly people can
not hear high frequencies as well as low ones, the frequency of auditory tones on kitchen
appliances should be below 900 Hz (Poulson, 1996).
b. Handles
Handles should not include sharp edges or other surface features which cause
pressure hot spots when gripped, such as finger shaping, edges of flat or raised surfaces
for application of labels, and ‘pinch points’ between moving parts (Pheasant, 1996). A
rectangular cross section will give greater purchase but will be less comfortable than a
round or oval shaped handle (Pheasant, 1996). If a rectangular handle is used the edges
should be rounded where the two planes meet to a minimum radius of 1”(Pheasant,
1996). In a circular handle the diameter must be large enough so that the user’s hand and
finger surface contact is maximized, but not so large that a firm grip cannot be
maintained (Woodson, 1992).
For normal users, three types of handle cross sections were found on kitchen
appliances: rectangular, oval, and round. The rectangular handles ranged from 1.125” to

44
1.5” in width, 0.5” to 1.125” in depth, and had a clearance, distance from handle to the
product, of 1.125” to 1.5”. The oval shaped handles had a width of 1” to 1.5”, had a
depth of 0.5” to 1”, and had a clearance of 1.125” to 1.5”. The round handles had a
diameter of 1” to 1.25” and a clearance of 1” to 1.5”. The counter top appliances had a
handle length that ranged from 3.25” to 4.25”.
Since elderly lose 16-40% of their hand strength (Tilley, 2002), a round or oval
handle should be used because it provides maximum grip strength and greater flexibility
for the operator if his or her orientation with respect to the handle must be changed
(Woodson, 1992). Handles with a circular cross section will be comfortable to grip since
there will be no possibility of hot spots, but they may not provide adequate purchase
(Pheasant, 1996). For elderly users, an oval shaped handle should be used on kitchen
appliances because they provide maximum grip strength, flexibility, no hot spots, and
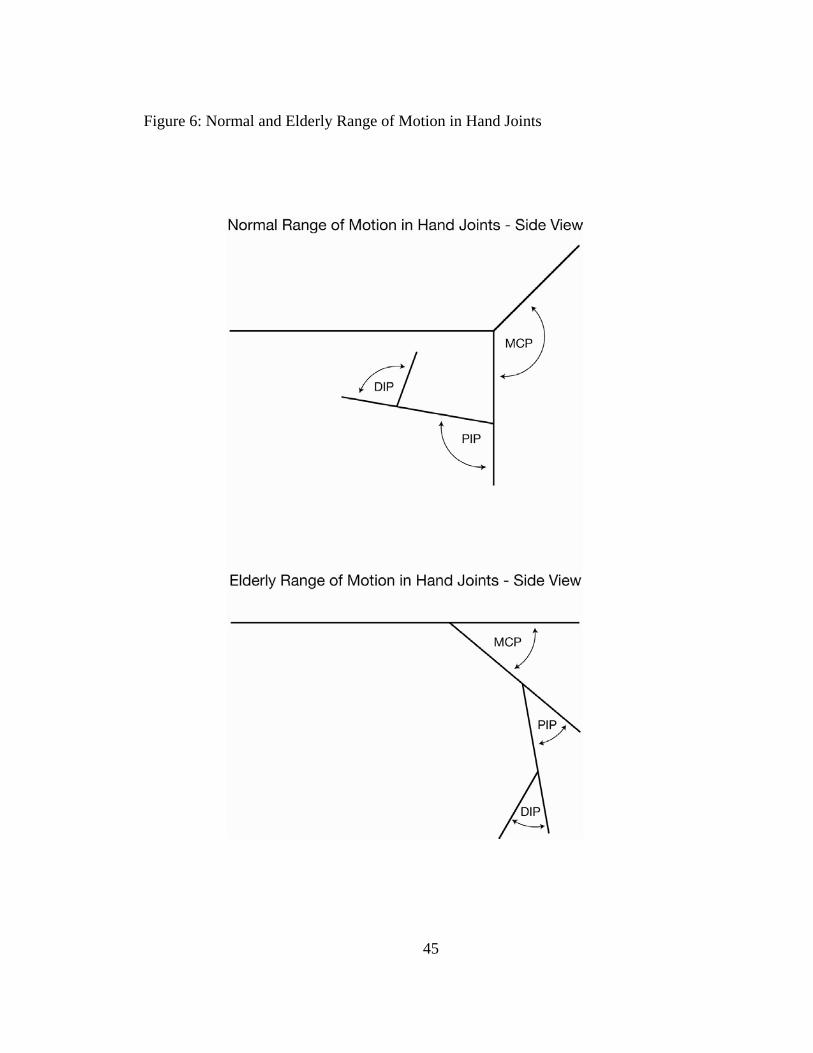
adequate purchase. To arrive at the appropriate size of oval handle, Figure 6 which
illustrates the maximum finger joint movement in an elderly person is considered.
45
Figure 6: Normal and Elderly Range of Motion in Hand Joints

46
Due to the limited range of motion of finger joints in the elderly, handles should
be larger. With handles being larger, the elderly users would not have to move their
finger joints as much and would experience less pain than if the handle was smaller.
Oval handles should be between 1.5” and 1.75” wide and between 1” and 1.25” deep.
This size ensures maximum contact between the hand and handle. Due to the limited
range of motion in the finger joints of the elderly seen in Figure 6, the clearance between
the handle and the appliance needs to be increased as well. Since it is difficult for elderly
people to open their hand all the way, the clearance should accommodate that. Therefore
the clearance should be between 1.5” and 2”. Using the information in Table 3, which
gives the hand breadth for men, women, and elderly men, the handle length for counter
top appliances, should be between 4.125” and 4.625”. This length considers the hand
breadth of the 95th percentile elderly men and adds 0.25” to 0.5” to each side to ensure
enough clearance for the hand.
c. Displays
i. Graphics
When operating any appliance or machine, the graphics and controls are the basic
interface with the user (Wildbur, 1989). The graphics identify, inform, and supply
feedback about the state of the operation by means of a system of words and symbols
(Wildbur, 1989). Interface graphics normally take three forms: verbal, symbolic, and
pictogrammic (Wildbur, 1989). Both words and pictograms are used to identify controls
and functions (Wildbur, 1989). Words are used to amplify directions and give warnings
47
and symbols such as arrows and arcs, to show direction of movement, increases or
decreases and sequence of operations (Wildbur, 1989). Symbols can be designed to fit
standard format such as a square or circle and therefore are more consistent in shape and
proportion (Wildbur, 1989). Because symbols carry a heavy load of identity information,
they are often reduced to the bare essentials of shape, line, tone, and other design
structures (Crow, 1986). Graphics should be capable of lasting the estimated life of the
product or appliance taking into account the working environment and frequency of use
(Wildbur, 1989). There are products in which the graphics have peeled off or worn away
leaving in doubt the function of the control settings and in some cases safety margins
(Wildbur, 1989). Printing directly onto the product material by ink or foil is an option,
while embossing or relief moulding, etching and anodizing are other common techniques
(Wildbur, 1989).
Figure 7 illustrates existing graphics found on kitchen appliances. The graphics
are either acceptable or unacceptable based on their design and amount of use on
appliances.

48
Figure 7: Existing Graphics on Kitchen Appliances

49

50

51

52
Since elderly people can not detect details as well as normal adults (Isle et al,
1992), the acceptable graphics are simple and do not have extra or unnecessary shapes.
The acceptable graphics are commonly used on appliances and easy to understand. The
acceptable graphics should be used for both normal and elderly people; the only
difference should the size of the graphic.
For normal users the height of graphics on appliances range from 0.1875” to
0.25”. Table 8 illustrates the increase of numeral and letter height along with the increase
of the viewing distance. Using Table 8, graphics at a height of 0.1875” to 0.25” can be
viewed from a distance of 15” to 40”.

53
Table 8: Minimum Character Height When Viewed in Close Proximity
Woodson, 1992.

54
A person with “normal” vision has a visual acuity of 20/20 (Montgomery, 1998).
As the second number increases, the closer a person must stand to see the same object
that the “normal” person saw (Montgomery, 1998). For instance, a person with 20/20
visual acuity can stand 30 feet away, while a person with 20/40 visual acuity must stand
15 feet away to see the same object (Montgomery, 1998). As shown in Table 9, the
visual acuity of one’s eyes decreases with age. Approximately one-third of people over
80 have vision of 20/50 (Isle et al, 1992), which means they have to stand 12 feet away
from the object (Montgomery, 1998). Using the distance of 30 feet for “normal” vision
and 12 feet for elderly vision, there is a 60% loss in vision for the elderly. Applying that
loss to the existing graphic size, the height of graphics for the elderly should be between
0.3” and 0.4”.

55
Table 9: Visual Acuity vs. Age
Timiras, 2003.

56
ii. Lettering
Two common types of fonts are serif and san serif. Serif types are defined by the
presence of a finishing stroke at the end of major stem and hairline strokes (Crow, 1986).
San serif types do not have serifs of any kind (Crow, 1986). Their variety comes from
stroke thickness variation and weight differences (Crow, 1986). The kind of typefaces
used for signs, labels, and other printed forms also make a difference in whether or not a
message can be easily understood (Gay, 1986). Typefaces should be avoided if they have
uneven stroke widths, extended serifs, include internal patterns or stripes, italics,
stenciled, appear like handwritten script, shadowed or look 3D, old English script, and
distorted to look tall, thin, wide or fat (Woodson, 1992). Some standard type styles that
are acceptable include Folio Book, News Gothic, Trade Gothic, Futura Medium, and
Spartan Medium (Woodson, 1992). Maximum contrast should be used for lettering
(Woodson, 1992).
Avoid clutter and illegibility that result when characters are crowded together
(Woodson, 1992). For individual letters, the optimum height to width ratio is 1:0.7
(Corlett and Clark, 1995). The stroke width to height ratio for black characters on a
white background is 1:6 and for white characters on a black background is 1:8 (Corlett
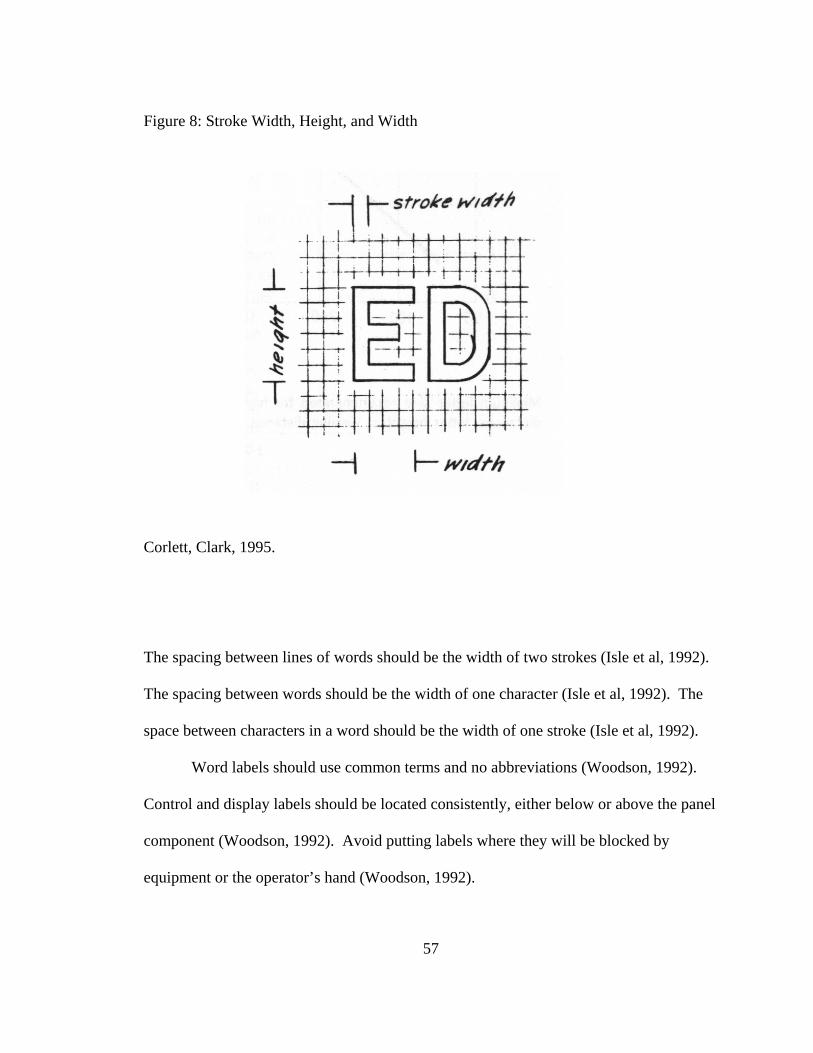
and Clark, 1995). This ratio is illustrated in Figure 8.
57
Figure 8: Stroke Width, Height, and Width
Corlett, Clark, 1995.
The spacing between lines of words should be the width of two strokes (Isle et al, 1992).
The spacing between words should be the width of one character (Isle et al, 1992). The
space between characters in a word should be the width of one stroke (Isle et al, 1992).
Word labels should use common terms and no abbreviations (Woodson, 1992).
Control and display labels should be located consistently, either below or above the panel
component (Woodson, 1992). Avoid putting labels where they will be blocked by
equipment or the operator’s hand (Woodson, 1992).

58
On existing kitchen appliances, the height of letters range from 0.09375” to
0.125”. Title case and uppercase was used approximately the same amount, while
lowercase was used rarely. The exact fonts used is unknown, however they were all san
serifs.
The size of characters should be increased for the elderly because of their loss of
visual acuity. To find the height of the lettering, Table 9 was considered and a 60% loss
of visual acuity in the elderly will be used, this percentage was calculated in the previous
section. To make up for that loss, the letter height for the elderly should be increased to
0.15” to 0.2”. Helvetica should be used as the typeface (Isle et al, 1992). Woodson
(1992) feels that all capital letters should be used for short labels and signs. While
Wildbur (1989) thinks lower case lettering is the first choice because many descriptions
giving the function of a control consist of a single word, and the use of all lower case will
give a more harmonious look to the panel than starting each word with a capital letter.
For elderly users, lettering on kitchen appliances should be in title case because it is
easier to read than all capital letters and all lower case letters. Title case words provide a
greater variety of shapes unlike capital letters which are a similar block shape (Bellevue,
2004).
iii. Colors
To ensure adequate legibility there must be adequate visual contrast between
alphanumeric characters and the background against which they are viewed (Woodson,
1992). Saturated colors should be used as opposed to pale colors when colors have
special significance (Woodson, 1992). If raised letters are used there must be additional

59
coloring to make the letters contrast with the background (Woodson, 1992). Do not
assume that a raised letter that is the same color as the basic background will be readable
just because it is raised (Woodson, 1992). Utilize size and/or color coding to help the
observer differentiate between levels of importance on your panel (Gay, 1986). Color
coding may also help put across clear visual messages; for example, red means stop;
green means go or on, and yellow means caution (Woodson, 1992). No more than five
colors should be used on a visual display (Galer, 1987).
On existing kitchen appliances most control panels are either white characters on
a black background or black characters on a white background. Some appliances have a
stainless steel background with black characters. Red, yellow, and green are usually
found on kitchen appliances, to signify stop, caution, and start.
A high contrast control panel will simplify use for a person with visual
impairments (Peterson, 1998). Instrument faces are more easily seen if the markings are
black on a light colored face (Peterson, 1998). Applying this to the elderly, the control
panel should have a white background with black lettering. Using black and white will
create more contrast than using just a light color for the background. Due to the increase
of glare in the elderly, a stainless steel background on a control panel should not be used.
Bright colors, such as red and yellow, should be used over dark colors, such as blue and
green, because as a person ages their color perception changes and they can not
differentiate between dark colors as well as bright ones. Red and yellow can still be used
on kitchen appliances for the elderly. If the color green is used it should be brighter than
it is on existing appliances. A standard green is around C-80, M-0, Y-100, K-0. For the
elderly, the green should be around C-50, M-0, Y-70, K-0. This CMYK is significantly

60
brighter than the standard green. The brighter the green, the easier it will be for an
elderly person to see.
iv. Digital Displays
Electronically generated characters are formed with either a dot matrix or line
segments. There are four sizes of dot matrixes, 5x7 matrix, which is the minimum size
accepted, 7x9 matrix, which is preferred, 8x11 matrix, which is the minimum size
preferred if the symbols are rotated, and 15x21 matrix, which is preferred if the symbols
rotate (Woodson, 1992). Lowercase letters should not be used in a matrix, because they
can be hard to distinguish from one another (Woodson, 1992). Dot matrixes are easier to
read because they produce curved lines (Woodson, 1992). Segmented displays are found
more on kitchen appliances than dot matrixes. Segmented displays either use a liquid
crystal display (LCD) or light emitting diodes (LED). The color of an LED is determined
by its wavelength (Marktech). For example the color green has a frequency of 560 – 569
nm, and red has a frequency of 628 – 639 nm (Marktech).
Most kitchen appliances feature digital displays with segmented characters; the
majority of them are LED, but there are a few LCD. The LED digital displays can be
found in red, yellow, and green. The average height of the characters is 0.5”.
For the elderly, a dot matrix which is 7 x 9 should be used. The height of the
characters should be 0.5” tall, which is the same as existing digital displays. There is no
need to increase the height because the maximum letter height calculated above was 0.2”.
Since the elderly can differentiate between bright colors better than dark ones, the digital
display characters should be red or yellow.

61
d. Technology and Form of appliances
New technologies that manufacturers are producing today help families save time
in the kitchen. For instance, TMIO makes an oven that refrigerates food and will begin
cooking when the user accesses the oven through the internet or by phone. Whirlpool
also makes a refrigerated range, which keeps your food cool until it is time to start
cooking. LG makes a refrigerator that has a television built into the door, which includes
FM radio, stereo speakers, and cable-ready TV tuner. LG also has a refrigerator with a
built in computer and barcode scanner that keeps track of the groceries and can send e-
mails to the users letting them know if they are out of milk.
Since elderly people spend a lot more time at home and are not as busy as young
families, kitchen appliances designed specifically for them should not include
unnecessary new technologies. The technology used in appliances for the elderly should
be similar to what they are used to; if something new and different is integrated into their
appliances it may be rejected. The form and shape of appliances for the elderly should
also be similar to what they are used to; all of the appliances should be recognizable.
Figure 9 gives some examples of unacceptable and acceptable forms and shapes for
several kitchen appliances.

62
Figure 9: Form of Appliances for Elderly

63

64
IV. GUIDELINES FOR DESIGNING KITCHEN APPLIANCES FOR ELDERLY a. Controls
i. Round Knobs
Adults – Minimum diameter is 0.25” and depth is 0.75” with serrations, 2 - 4 in-
oz resistance. Preferred diameter is 0.5” and depth is 0.5” with serrations, 4 in-oz
resistance.
Elderly – Diameter 1” - 2” and depth of 0.5” – 0.75” with serrations, 3 - 6 in-oz
resistance.
Figure 10: Round Knob Dimensions
Image from Woodson, 1992

65
ii. Pointer Knobs
Adults – Length is 1”-2”, Width is 0.25” – 0.5”, Height is 0.5”, 10 - 45 in-oz
resistance.
Elderly – Length is 2” - 3”, Width is 0.5” – 0.75”, Height is 0.75”, 6 – 27 in-oz
resistance.
Figure 11: Pointer Knob Dimensions
Image from Woodson, 1992
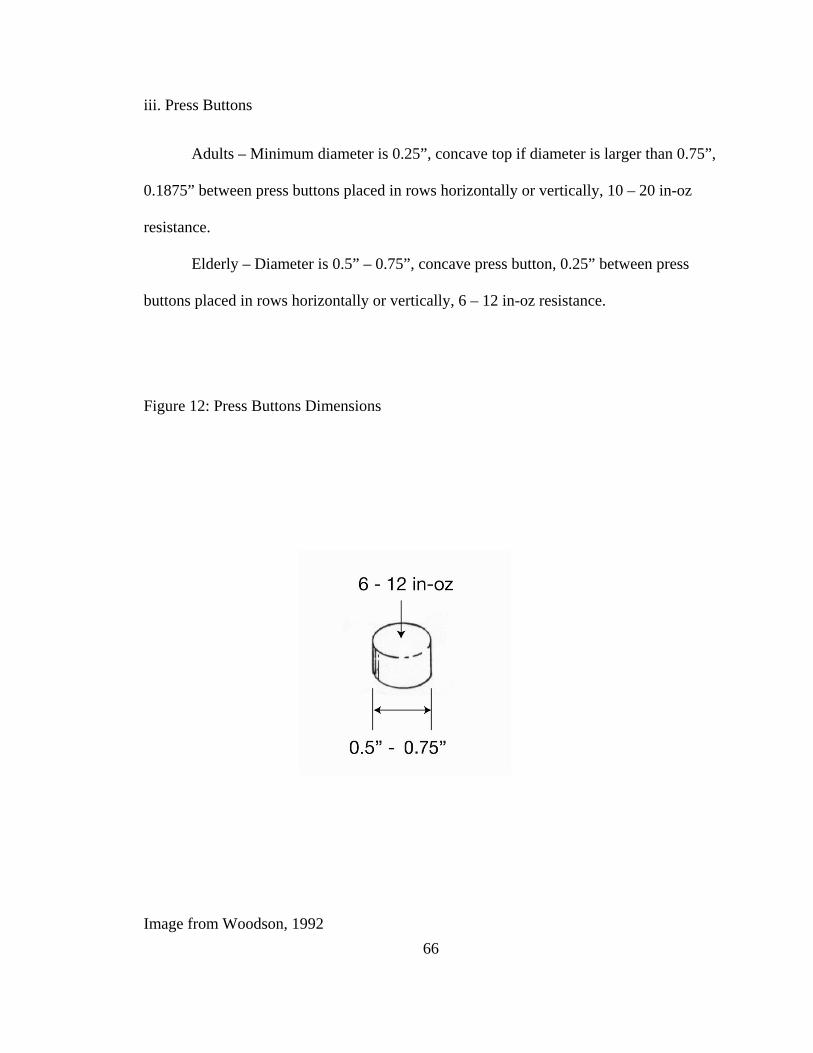
66
iii. Press Buttons
Adults – Minimum diameter is 0.25”, concave top if diameter is larger than 0.75”,
0.1875” between press buttons placed in rows horizontally or vertically, 10 – 20 in-oz
resistance.
Elderly – Diameter is 0.5” – 0.75”, concave press button, 0.25” between press
buttons placed in rows horizontally or vertically, 6 – 12 in-oz resistance.
Figure 12: Press Buttons Dimensions
Image from Woodson, 1992
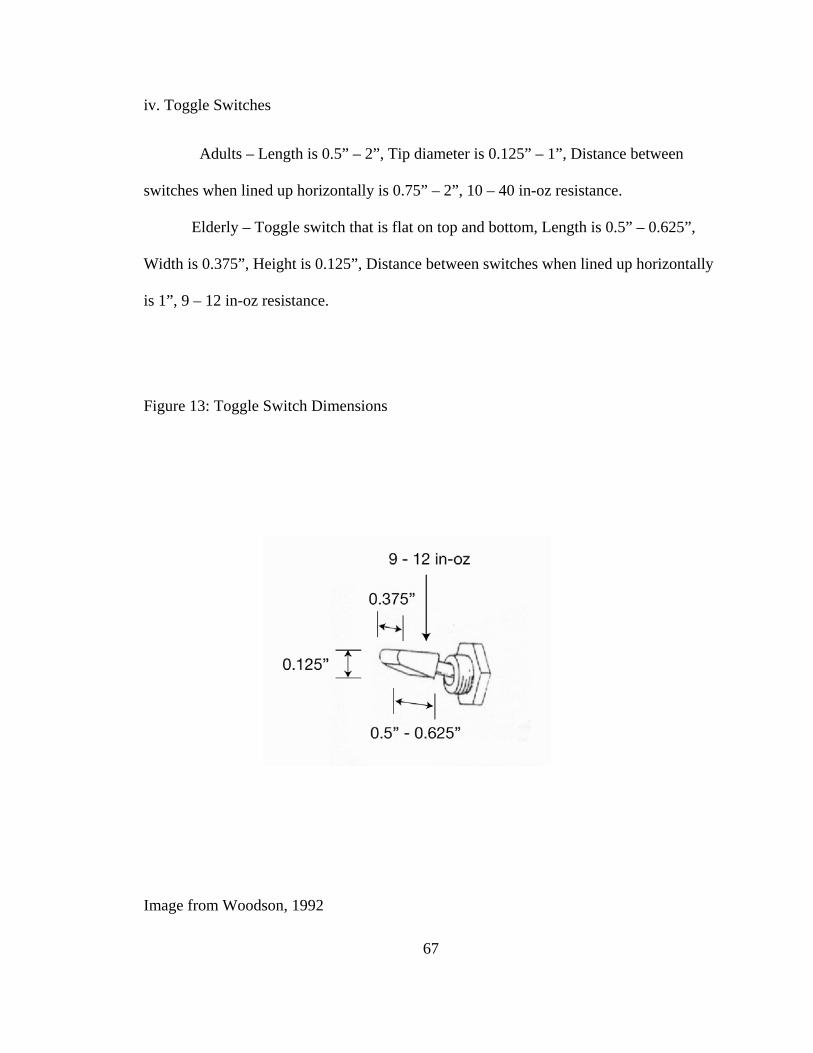
67
iv. Toggle Switches
Adults – Length is 0.5” – 2”, Tip diameter is 0.125” – 1”, Distance between
switches when lined up horizontally is 0.75” – 2”, 10 – 40 in-oz resistance.
Elderly – Toggle switch that is flat on top and bottom, Length is 0.5” – 0.625”,
Width is 0.375”, Height is 0.125”, Distance between switches when lined up horizontally
is 1”, 9 – 12 in-oz resistance.
Figure 13: Toggle Switch Dimensions
Image from Woodson, 1992

68
v. Contact Switches
Adults – Square or rectangular switches: Height is 0.5” – 0.625”, Width is 0.5” –
0.75”, Circular switches: 0.5” diameter, 1 – 5 in-oz resistance.
Elderly – Square or rectangular switches: Height is 0.625”, Width is 1” – 1.25”,
Circular switches: 0.625” diameter, 3 in-oz resistance.
Figure 14: Contact Switch Dimensions
Image from Woodson, 1992

69
vi. Rocker Switches
Adults – Oval switches: height is 0.5” – 1, width is 0.625” – 1.5”, Circular
switches: 0.5” – 0.625” diameter, Square switches: 0.375” x 0.5”, 10 – 40 in-oz
resistance.
Elderly – Oval switch: height is 0.5” – 0.625”, width is 1” – 1.25”, concave
surface and activation light, 6 – 16 in-oz resistance.
Figure 15: Rocker Switch Dimensions

70
vii. Toaster Lever
Adults – Width is 0.875” – 3.125”, Depth is 0.75” – 1.25”.
Elderly – Width is at least 2”, Depth is 0.75”.
Figure 16: Toaster Lever Dimensions

71
viii. Feeback
1. Lights
Adults – Luminance level is 550 lux, Circular lights: diameter is 0.125” – 0.25”,
Oval lights: width is 0.5”, height is 0.125” – 0.25”.
Elderly – Luminance level is 650 lux, Circular lights: diameter is 0.1875”, Oval
lights: width is 0.5”, height is 0.125” – 0.25”.
Figure 17: Light Dimensions

72
2. Sounds Adults – 62 – 80 dB. Frequency is 30 – 3,000 Hz.
Elderly – 93 – 98 dB, Frequecy is below 900 Hz.
b. Handles
Adults – Rectangular handles: Width is 1.125” – 1.5”, Depth is 0.5” – 1.125”,
Clearance is 1.125” – 1.5”, Oval handles: Width is 1” – 1.5”, Depth is 0.5” – 1”,
Clearance is 1.125” – 1.5”, Round handles: Diameter is 1” – 1.25”, Clearance is 1” –
1.5”, Handle Length is 3.25” – 4.25”.
Elderly – Oval handles: Width is 1.5” – 1.75”, Depth is 1” – 1.25”, Clearance is
1.5” – 2”, Handle Length is 4.125” – 4.625”.
Figure 18: Handle Dimensions
Image from www.fixturesetc.com

73
c. Displays
i. Graphics
Adults – Height is 0.1875” – 0.25”.
Elderly – Height is 0.3” – 0.4”. Refer to Figure 7 for acceptable graphics.
Figure 19: Graphic Dimensions
ii. Lettering
Adults – Height of letters is 0.09375” – 0.125”, San serif typeface, Title case and
uppercase are used.
Elderly – Height of letters is 0.15” – 0.2”, Helvetica typeface, Title case.
Figure 20: Letter Dimensions
iii. Colors
Adults – Either white characters on black background, black characters on white
background, or black characters on stainless steel background. Red, yellow, and green.

74
Elderly – Black lettering on white background, Red and yellow can be used. If
green is used it should be brighter than a standard green.
iv. Digital Displays
Adults – Majority are LED, some are LCD, LED are red, yellow, and green,
Height is 0.5”.
Elderly – Dot matrix 7 x 9, Height is 0.5”, LED are red or yellow.
Figure 21: Digital Display Dimensions

75
d. Technology and Form of Appliances
Elderly – Appliances should be recognizable and use technology that is similar to
those commonly available.

76
V. APPLICATION OF GUIDELINES
a. Idea Sketches
A microwave was designed using the guidelines that were created in this thesis.
Shown below are some idea sketches of microwaves.
Concept A - The door on this microwave opens downward, which allows the user
to pull their food onto the door after cooking. The control panel is at a 45 degree angle
and placed on the top of the microwave so it is easier to see.

77
Concept B – The door on this microwave swings to the left similar to a
conventional microwave. The control panel is placed on the top of the microwave and
angled.

78
Concept C – The control panel is place on the top of the microwave door and the
door opens downward.

79
Concept D – The control panel is placed on the top of the microwave and angled,
while the door opens downward.

80
Concept E – The control panel is angled and placed at the top. The door swings
to the left like conventional microwaves.

81
Concept F – The control panel is placed on the door, the most important controls
are at the top of the microwave. The door swings to the left like a conventional
microwave.

82
b. Preliminary Models
Models were made of three of the concepts. The models were made from blue
Styrofoam.
Concept A

83
Concept C

84
Concept F

85
c. Final Model
Concept F was chosen as the final design because it is a more conventional than
concept A and C. Refer to section III. Development of Design Guidelines d. Technology
and Form of Appliance for more explanation.

86
Control Dimensions

87
Detail shot of round knob.
Detail shot of press buttons.

88
Detail shot of contact switches and clock.
Detail shot of round knob and handle.

89

90

91
d. Summary of Project
The microwave measures 12” in height, 16” in depth, and 18” wide, and the door
hinges on the left side. Contact switches are used for the numbers, Timer, Clock, Start,
and Cancel. The dimensions for the contact switches come from section IV. a. v., which
explains that rectangular switches should have a height of 0.625” and a width of 1”-
1.25”. A round knob is used for Cook Time, Defrost, Power Level, and Keep Warm.
The dimensions of the round knob come from section IV. a. i., which states that the
diameter should be between 1” and 2”, while the depth should be between 0.5” and 0.75”.
Press buttons are used for the preset foods such as Pizza and Potatoes. Section IV. a. iii.
states that the diameter of a press button should be between 0.5” and 0.625”. The handle
length is 11”, while the viewing window measures 4” high by 10” wide. The handle
dimensions are stated in section IV. b., which say that the oval handle should have a
width between 1.5” and 1.75”, a depth of 1” to 1.25”, and a clearance of 1.5” to 2”. The
turntable inside is 12 ¾” in diameter. The internal components of the microwave would
be housed on the left side. The internal dimensions of the microwave are 10” high, 14 ½”
deep, and 14” wide.
92
VI. CONCLUSIONS
The intention of the thesis was to develop guidelines for designers to use when
they are designing kitchen appliances for the elderly population. Existing control
standards on appliances are given along with physical and psychological characteristics
of the elderly. The guidelines were formed by analyzing a specific characteristic of the
elderly and the appliance standard used currently. The guidelines created can be applied
to any kitchen appliance. All guidelines should be used when designing; if one or more
are left out the user may have trouble operating that component of the appliance. Even
though the guidelines are specific about each component, many different designs can be
created.
In the thesis, the guidelines were applied to the design of a microwave oven. The
final design is not the only possible solution; it simply illustrates how the guidelines are
used.
93
VI. REFERENCES
Aldrich-Ruenzel, N., & Fennell, J. (1991). Designer’s Guide to Typography. New York: Watson-Guptill Publications. Belleve Linux Users Group. (2004). The Linux Information Project. Seattle, Washington: www.bellevuelinux.org. Bieber, E. J., Weiland, A. J., & Volenec-Dowling, S. (1986). Silicone-rubber implant arthroplasty of the metacarpophalangeal joints. Wheeless’ Textbook of Orthopaedics, 68(2), 206-9. Burdman, G. M. (1986). Healthful Aging. New Jersey: Prentice Hall, Inc. Burmark, L. & Fournier, L. (2003). Enlighten Up! An Educator’s Guide to Stress-Free Living. Association for Supervision and Curriculum Development. Caldwell, E., & Hegner, B. R. (1986). Geriatrics: A study of maturity. Albany, New York: Delmar Publishers, Inc. Conacher, G. (1986). Kitchen sense for disabled people. London: Croom Helm. Corlett, E. N., & Clard, T. S. (1995). The ergonomics of work spaces and machines. London: Taylor and Francis. Coren, S. (1994). Most Comfortable Listening Level as a Function of Age. Ergonomics, 37(7), 1269-1274. Crow, W. C. (1986). Communication Graphics. Englewood Cliffs, New Jersey: Prentice Hall. Davidoff, N. A., & Freivalds, A. (1993). A graphical model of the human hand using CATIA. International Journal of Industrial Engineers, 12,255-264. Davis, H. (1978). Abnormal Hearing and Deafness. New York: Holt, Rhinehart, and Winston. Day, Thomas. About Medical Care for the Elderly. http://www.longtermcarelink.net/eldercare_medical_careissues.htm.

94
DellaContrada, J. (2006). Fortune 500 Program Designs Next Generation Products: MBA Students Work with Center on Market Research, Product Design. University of Buffalo. Duquesnoy, A.J. (1983). Effect of a Single Interfering Noise or Speech Source Upon the Binaural Sentence Intelligibility of Aged Persons. The Journal of the Acoustical Society of America, 74(3): 739-743. Eaton, Charles. (1997). The Electronic Textbook of Hand Surgery. www.eatonhand.com. Eisma, R., Dickinson, A., Goodman, J., Mival, O., Syme, A., & Tiwari, L. (2003). Mutual Insiration in the Development of New Technology for Older People. London. Fuller, R. B. (1972). Symbol Sourcebook. New York: Van Nostrand Reinhold Company. Gambert, S. R. (1987). Handbook of Geriatrics. New York: Plenum Publishing Corporation. Gay, K. (1986). Ergonomics: making products and places fit people. Hillside, New Jersey: Enslow Publishers, Inc. The Hyperacusis Network. www.hyperacusis.net/hyperacusis/supplement/default.asp. Hardwood Manufacturers Association. (2001). Hardwoods Add Style, Practicality to Universal Design. Henderson, Tom. (1996). The Physics Classroom. www.glenbrook.k12.il.us/GBSSCI/PHYS/CLASS/sound/u11l2b.html. Isle, B., Denno, S., Metz, S.V. (1992). Human Factors Design Guidelines for the Elderly and People with Disabilities. Minneapolis, MN: Honeywell, Inc. Ivergard, T. (1989). Handbook of Control Room Design and Ergonomics. London: Taylor and Francis. Jayson, M. I. V., & Dixon, A. St. J. (1974). Understanding Arthritis and Rheumatism. New York: Pantheon Books. Jeavans, C. (2005). A Design for (Long) Life. BBC News. Johnstone, B. R. (2001). Proximal interphalangeal joint surface replacement anthroplasty. Hand Surgery: An International Journal Devoted to Hand and Upper Limb

95
Surgery and Related Research; Journal of the Asia-Pacific Federation of Societies for Surgery of the Hand, 6(1), 1-11. Kelsheimer, H. & Hawkins, S. (2000). Older Adult Women Find Food Preparation Easier with Specialized Kitchen Tools. Journal of the American Dietic Association, 100, 950-952. Kirby, S. D. (1999). Safe, Comfortable Housing for the Elderly. Oklahoma State University Extension Service. Marcincuk, M.C. & Roland, P.S. (2002). Geriatric Hearing Loss: Understanding the Causes and Providing Appropriate Treatment. Geriatrics Advisor. Marktech Optolelectronics. Segmented Displays. Latham, New York: www.marktechopto.com. Montgomery, T. (1998). Anatomy, Physiology, & Pathology of the Human Eye. www.tedmontgomery.com. Nascher, I. L. (1979). Geriatrics: the diseases of old age and their treatment. New York: Arno Press. Oregon: Resources for Seniors and People with Disabilities. Minimum Maitained Average Illuminance. File://G:/Thesis/articles/lighting.shtml.htm. Peterson, L.K., & Cullen, C. D. (2000). Global Graphics: Color. Gloucester, Massachusetts: Rockport Publishers. Peterson, M. J. (1981). Universal Kitchen and Bathroom Planning: Design that adapts to people. New York: McGraw-Hill. Pheasant, S. (1996). Bodyspace: Anthropometry, Ergonomics, and the design of work. London: Taylor and Francis Publishers. Poulson, David. (1996). Hearing Impairment. Brussels-Luxembourg: www.stakes.fi/include/1-8-3-2.htm. Saxon, S. V., & Etten, M. J. (2002). Physical Change and Aging: A guide for the helping professions. New York: The Tiresias Press, Inc. Sutherland, R., & Karg, B. (2003). Graphic Designer’s Color Handbook. Gloucester, Massachusetts: Rockport Publishers. Tepper, L. M., & Cassidy, T. M. (2004). Multidisciplinary Perspectives on Aging. New York: Springer Publishing Company.
96
Tilley, A. R. (2002). The measure of man and woman: revised edition: human factors in design. New York: John Wiley and Sons, Inc. Timires, P. S. (1988). Physiological Basis of Geriatrics. New York: MacMillan Publishing Company. United States Census Bureau. (2004). Annual Percent Change of Housing Unit Estimates for the United States and States, and State Rankings: July 1, 2003 to July 1, 2004. www.census.gov/popest/housing/tables/HU-EST2004-03.xls United States Census Bureau (2005). 65+ in the United States: 2005. www.census.gov/population/www/socdemo/age.html. Vanderheiden, G. C. (1990). Thirty-something Million: Should They be Exceptions?. Human Factors, 32(4), 383-396. Walker, R. H., Craig-Lees, M., Hecker, R., & Francis, H. (2002). Technology-Enabled Service Delivery: An investigation of reasons affecting customer adoption and rejection. International Journal of Service Industry Management, 13(1), 91-106. Wildbur, P. (1989). Information Graphics. New York: Van Nostrand Reinhold Company. Winfield, B. (1999). Product Advice: The Kitchen That Could. www.improvenet.com. Woodson, W. E. (1992). Human Factors Design Handbook. New York: McGraw-Hill. Wright Medical Technology, Inc. (2005). Swanson Finger Joint.