Embed Size (px)
Citation preview
Health Promotion and Education (HPE)Department of Noncummunicable Diseases
and Mental Health
Guidelines for DevelopingBehavioural Change Interventions
in the Context of Avian Influenza

© World Health Organization 2008
All rights reserved. Requests for publications, or for permission to reproduce or translate WHOpublications—whether for sale or for noncommercial distribution can be obtained from Publishingand Sales, World Health Organization, Regional Office for South-East Asia, Indraprastha Estate,Mahatma Gandhi Marg, New Delhi-110 002, India (fax: +91-11-23370197; e-mail: [email protected]).
The designations employed and the presentation of the material in this publication do not imply theexpression of any opinion whatsoever on the part of the World Health Organization concerning thelegal status of any country, territory, city or area or of its authorities, or concerning the delimitation ofits frontiers or boundaries. Dotted lines on maps represent approximate border lines for which theremay not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that theyare endorsed or recommended by the World Health Organization in preference to others of a similarnature that are not mentioned. Errors and omissions excepted, the names of proprietary products aredistinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify theinformation contained in this publication. However, the published material is being distributedwithout warranty of any kind, either expressed or implied. The responsibility for the interpretationand use of the material lies with the reader. In no event shall the World Health Organization be liablefor damages arising from its use.
This publication contains the collective views of an international group of experts and does notnecessarily represent the decisions or the stated policy of the World Health Organization.
Printed in India, June 2008
WHO Library Cataloguing-in-Publication data
World Health Organization, Regional Office for South-East Asia.Guidelines for developing behavioural change interventions in the context of Avian Influenza.
1. Influenza, Human - prevention and control. 2. Behavior Therapy. 3. Communication.4. Guidelines. ISBN 978-92-9022-325-2 (NLM classification: WC 515)

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza iii
Contents
Acknowledgements .............................................................................................. iv
About the guidelines .............................................................................................. v
Preface ................................................................................................................. vii
1. Background..................................................................................................... 1
2. What are behavioural change interventions? ................................................... 3
3. Development and management of behavioural change interventions .............. 5
Phase 1: BCI Preparation ........................................................................................ 5
Phase 2: Implementation of BCI ............................................................................. 9
Phase 3: Monitoring, evaluation and research ........................................................ 17
4. Conclusion ....................................................................................................20
Bibliography ........................................................................................................ 21

Acknowledgements
The Behavioural Change Intervention (BCI) Guidelines were produced under theoverall direction of Health Promotion and Education (HPE) Unit, Department ofNoncommunicable Diseases and Mental Health (NMH) with financial support fromthe Communicable Diseases Surveillance (CSR) Unit, Department of CommunicableDiseases (CDS). HPE is grateful to the WHO staff members at regional and countrylevel for their contribution to the development of the guidelines in various ways. HPEis also indebted to the external reviewers for their valuable input, namely: Dr SarojJha (India), Professor O. Amienyi (Arkansas State University, USA), and Ms AnnaCharlotta Adelstal (Sweden).
Last but not least, the lessons drawn from countries affected by AI, specificallythe decisions and actions taken by governments, local and international organizations,and the communities significantly shaped the content of the BCI Guidelines. HPE isgrateful for the collective action in producing the BCI Guidelines.

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza v
About the guidelines
These guidelines for developing Behaviour Change Interventions (BCI) related to avianinfluenza (AI) are intended for all those involved in AI prevention and control at theplanning, implementation, evaluation and policy levels. More specifically, the guidelinesare intended to be a resource for programme managers and/or facilitators of activitiesthat seek to address the sociocultural and behavioural aspects of AI at the national,provincial, district and community levels, using multisectoral approaches. The guidelinesfocus on the following three development phases in logical sequence:
(1) Preparation phase
During this phase, information is gathered through a situational analysis, akey activity which establishes predisposing, enabling and reinforcing factorsrelated to basic information, cultural issues, services available, capacity, policiesand regulations related to AI. Planning of activities is guided by findingsfrom the situational analysis.
(2) Implementation phase
During this phase, activities planned are implemented through incorporatingthe relevant BCI elements in an integrated manner;
(3) Research, monitoring and evaluation phase
This phase is intended to generate new information and establish the evidenceof the effectiveness of the behavioural change intervention.
In defining the above three phases, the guidelines also provide a comprehensiveunderstanding of the processes that are essential for behavioural change interventionwith respect to AI. It seeks to alert and equip those involved in the multisectoraldevelopment and management of AI prevention and control activities towardsbehaviouralal change to:
• Be mindful of the need for a detailed planning process, which includes asituational analysis in order to determine the predisposing, enabling andreinforcing factors likely to hinder or promote the success of behaviouralchange interventions;
• Identify and develop consensus on essential elements of BCI that are relevantto the AI situation being addressed, which includes communication, capacitybuilding, partnerships and resource mobilization among others;
• Recognize that while communication processes are the main strategy for AIcontrol and prevention, communication alone has limited impact on

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenzavi
behavioural change, particularly those practices established over a long timesuch as the coexistence between humans and poultry. In order to reverseor halt negative behaviourals associated with AI transmission, there is a needfor implementing multifaceted activities that include communication as apre-requisite for achieving desired results;
• Involve communities, civil society groups and the private sector throughoutthe process of developing, monitoring and evaluation of behavioural changeinterventions.
Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza vii
Preface
These guidelines for Behavioural Change Interventions (BCI) have been developedfor health promotion programme managers, facilitators and trainers to build thecapacities of health and non-health professionals working with government,nongovernmental organizations, the private sector and community-based groups topromote, enable and support individuals and communities to achieve desired healthoutcomes through behavioural change interventions. The guidelines have beendeveloped as a tool for halting or reducing the transmission of avian influenza (AI)from poultry to humans. However, the principles and strategies of BCI as described inthe document could well be applied within most other prevention and controlprogrammes that are disease specific, population or settings-based.
Several key elements that are essential to effect desired behavioural change arehighlighted in the BCI Guidelines. While each situation would dictate which element(s)should be prioritized, it is evident that communication for behavioural change, policycoherence and advocacy (governance issues), capacity building, an understanding ofprevailing attitudes and culture and monitoring and evaluation are likely to remain atthe core of any BCI seeking to address public health concerns.
These guidelines should help in better planning, implementation, monitoringand evaluation of behavioural change interventions that are likely to yield positivelifestyle changes among individuals, communities and organizations in the South-EastAsia Region.
Dr Samlee Plianbangchang, M.D., Dr.P.H.Regional Director

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza 1
The outbreak of avian influenza (AI) in poultry and wild bird populations (H5N1)aswell as confirmed human cases in some countries of the South-East Asia Region havealerted public health authorities to initiate urgent interventions to prevent thetransmission of AI from poultry to humans.
The past pandemics of AI reported in 1918, 1957 and 1968 which resulted in43 million human deaths worldwide are a strong reminder to convince governmentsthat history must not be allowed to repeat itself. In addition to loss of human lives, thepandemics resulted in major economic losses globally.
Currently, the threat of an AI pandemic appears high. To date, AI has beendetected among poultry in countries of WHO’s Western Pacific, South-East Asia, EasternMediterranean, Europe and Africa Regions. AI has resulted in human deaths inIndonesia, Thailand, the People’s Republic of China and in Viet Nam.
WHO and other partners are making concerted efforts to reduce humanexposure to avian flu virus through promoting a set of simple yet valuable measuresthat will not only improve and enhance biosecurity at critical stages of the food supplychain (production, transportation, marketing and consumption) but will also ensurethat the potential transmission of AI virus from animals to humans is considerablyreduced1. This will also include prevention activities at potential sources of infection,surveillance and use of epidemiological data on outbreaks, as well as provision ofpharmaceuticals and personal protective gear.
These are wide ignorance and misconceptions about AI and its potential threatto human life. While there is urgent need for education and communicationprogrammes, it must be appreciated that human behavioural is complex and will notchange overnight. Poultry is considered as a part of family’s assets, both as a source ofincome as well as food. It would thus require more than just providing facts andfigures and verbal persuasion to convince communities to give up rearing chickens intheir backyards.
It is well known that disease outbreaks and other forms of disasters are oftenaccompanied by fear and panic among the general population. Avian influenza appearsto cause extreme forms of anxiety because of its high potential to be fatal, with noknown cure and with its etiology still not fully understood. Public information andeducation programmes including the mass media, print, radio and television have
Background
1Manual for improving biosecurity in food supply chain: Focus on live animal markets. WHO/SEARO, 2006.
1

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza2
often been aggressive in reporting new cases and deaths in both humans and poultryand overemphasizing the limited availability of medicines (osel tamivir) and difficultiesin breaking the interrelationship between humans and animals particularly poultry inaffected countries. Such approaches may, in fact, lead to an opposite effect, by fuelingirrational fears and creating immense anxiety among people in countries experiencingoutbreaks and even in those where there are no outbreaks.
While health communication remains a critical element of BCI, the mere provisionof knowledge is not sufficient if communities lack basic systems that facilitate theadoption of healthy behavioural. BCI thus entails a process of changing conditions,promoting structures and policies that support healthy lifestyles. In the context ofavian influenza, BCI is inherently linked to the availability and accessibility of healthservices, a clean environment and a healthy marketplace, in addition to knowledgegain.

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza 3
Behavioural Change Interventions (BCI) is a package of well-defined multiple strategiesdesigned to address human behaviour in complex settings.
BCI strategies are especially relevant in the field of health for promoting andstrengthening policies and structures that support healthy lifestyles. BCI must be seendifferently from either health education (HE) or communication for behavioural change(CBC).
BCI incorporates CBC and health education concepts within the health promotionframework. BCI goes beyond just educating or communicating with individuals andcommunities to encompass a range of actions to advocate for and establish interventionsthat will not only enable but will also reinforce desired behavioural change. BCI basesits strategies on the growing acceptance of the fact that human behaviour is complexand is influenced by a number of interrelated determinants including political,legislation, socioeconomic conditions, cultural diversities, the availability ornonavailability of services and the opportunities to think, learn and take decisions toimprove the quality of life.
Health education has been an integral part of most national health programmesover the past several decades. It is based on the premise that only ignorance or lack ofinformation prevents people from adopting healthy behaviour. Health educationmethods largely consist of providing information and persuasion tactics through atop-down approach. This “trickle down” model has failed to address a crucial issue,specifically, “why do people continue to indulge in harmful practices despite beingtold and being aware of the harmful effects”? Health education has clearlydemonstrated that making information available brings about knowledge gain, whichalso improves understanding. Ultimately, it is clear that access to information resultsin knowledge gain and understanding; however, this does not bring about the desiredbehavior change.
In this context, communications for behaviour change (CBC) evolved to changethe paternalistic approach and to make communications a horizontal process in whichboth senders and receivers of information took on interchangeable roles, throughfocus group discussions and other methods. Communication changed its focus from“persuasion” to “participatory communication” where information is created and sharedbetween participants to reach a mutual understanding and collective decision-making.
In recognizing that there are no single approaches or strategies that can breakthe chain of transmission of the avian flu virus from poultry to humans, BCI seeks to
What are behavioural change interventions?2

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza4
examine and address predisposing, enabling and reinforcing factors associated withbehavioural change which also includes, in addition to addressing cultural values andbeliefs, government policies and legislations, partnership building, resource mobilizationand generating evidence of the effectiveness of BCI through research, monitoring andevaluation among others.
Communication for behavioural change stands high on the list of BCI strategies.However, it is also recognized that communication cannot be a stand-alone interventionwhen addressing a public health concern such as reducing transmission of avianinfluenza from poultry to humans because of the strong sociocultural influences ofthe behaviours being targeted. For instance, families and communities in South-EastAsia have kept poultry (chickens, ducks and birds) from time immemorial, as part ofhousehold assets or for commercial purposes. This long historical interrelationshipbetween humans and poultry (including migratory birds) cannot be ignored whendeveloping measures to halt or eliminate the spread of AI.
Communication for behavioural change activities therefore needs to be reinforcedby other BCI elements including healthy policy, creating an enabling environment,providing easy access to health services, imparting skills, capacity building, social andcommunity mobilization and partnerships. Advocacy plays an important role in BCIto influence policy and decision-makers and initiate social action to create a supportiveenvironment for BCI, as, for example, in ensuring political commitment and stakeholderparticipation in developing healthy food markets.
BCI also encourages dialogue and exchange of views among concerned partieswithin the framework of a functional partnership, involving those with interests inhuman health and economic benefits from poultry. Ultimately, BCI aims to supportprogramme managers to identify and address factors likely to promote or hinderbehavioural change such as culture, historical continuity, language, gender, governanceand capacity building, as well as to offer practical solutions addressing specific needsof intended beneficiaries, including fears or concerns.
Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza 5
The development and management of BCI is in three distinct but interrelated phases:preparation, implementation and monitoring and evaluation.
Programme planners and managers can decide whether to implement BCI as apilot, demonstration or institutionalized project.
Phase 1: BCI Preparation
Conducting BCI situation analysis
Scientific inquiry is considered the most reliable of all the methods of conducting asituational analysis2. This will include information on national policies and organizationalstructures, and available epidemiological and behavioural data. The informationderived from a situational analysis is a valuable tool for planning programmes andpolicy decision-making.
A situation analysis for developing BCI helps to:
• Determine what policies, legislation and regulations exist in the country tosupport behavioural change and what is needed;
• Identify community assets that exist and those that do not exist to promoteBCI, including political will and leadership, expertise, infrastructure andhuman and financial resources;
• Establish what information, skills and other prerequisites the public possessesvis-à-vis the gaps that have to be filled, for desired behavioural outcometowards AI prevention and control.
– Baseline AI related knowledge, perceptions, attitude, behaviour, culturalbeliefs or community felt needs for AI prevention;
– communication channels available to reach target groups;
– source credibility and barriers for people seeking AI information; and
– behaviours targeted for change.
• Determine factors likely to enable, reinforce or hinder BCI for AI preventionand control, e.g. :
Development and management ofbehavioural change interventions
3
2Amienyi, O.P. Communicating national integration: Empowering development in African countries, Ashgate,2005.

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza6
– Political commitment and leadership;
– social mobilization and advocacy;
– cultural values and beliefs;
– partnership, alliances and networks for BCI implementation;
– resource mobilization;
– gathering evidence on the effectiveness of BCI through research;
– monitoring and evaluation;
– any other factors likely to promote or hinder behavioural change forAI prevention and control.
The situation analysis should be conducted by a multidisciplinary team withexpertise in both qualitative and quantitative research methodologies.
Establishing BCI goal and objectives
A “ goal” is a broad intent of the desired outcome.
The goal of BCI is to reduce transmission of AI to humans in any setting.
“Objectives” are clear and specifically stated desired outcomes.
A statement of objectives must be “SMART”, namely :
• Specific — for the target audience in the context of their knowledge, skills,attitudes, behaviour, beliefs and perceptions, among others.
• Measurable — for assessing behavioural impact.
• Achievable — attainable under the conditions set.
• Relevant — be related to or contribute to the activity.
• Time-bound — with results expected within a given time.
Specific BCI objectives for the prevention and control of AI are to build nationalcapabilities to:
• Advocate for policies, legislation and regulation that help to create an enablingenvironment to prevent and control AI;
• disseminate appropriate age, gender and culture-specific AI prevention andcontrol information to target populations;
• facilitate communication among individuals and communities in order toverbally and non-verbally express opinions, desires and fears related to AI;
• promote and facilitate positive health-seeking behaviours including earlydiagnosis, compliance with medical advice including treatment and any otherhealth recommendations if AI infection is suspected;
Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza 7
• promote participation of all sectors in AI prevention and control activities;
• integrate BCI activities in pre-pandemic preparedness plans across sectors atall administrative levels – national, provincial and district;
• plan, implement, monitor and evaluate integrated behavioural changeinterventions using various players including communities, civil society groups,the private sector and all other relevant government ministries in addition tohealth;
• establish a monitoring system that includes formal and informal mechanismsto receive ongoing feedback from communities on the appropriateness ofthe BCI strategies being adopted and its effectiveness; and
• utilize findings from BCI evaluation and research in making programme andpolicy changes.
Identifying settings and target audience
The settings approach demands that individuals not be treated in isolation from thelarger social units in which they live, work and play3. In order to reduce exposure ofhumans to avian flu, BCI should target individuals working in settings that put them indirect contact with poultry or birds, namely poultry farmers, cullers, poultry tradersand market attendants. There is also a need to target men, women and children whoare not in regular direct contact with poultry but could be exposed because of visits tothe poultry market or recreation parks. Ultimately, the likelihood that one could bein contact with birds or poultry, qualifies that individual to be a target for riskcommunication. Schools provide ideal locations for implementing BCI, not only amongstudents but also among teachers and parents.
In general, the settings or localities for targeting BCI to reduce human exposureto avian flu should include, but are not limited to:
• Poultry farms (large, small and backyard)
• Wet markets/Poultry markets
• Poultry meat processing factories
• Slaughterhouses
• Schools
• Workplaces
• Households and communities (including chicken fights as a culturalrecreation)
3Poland et al. Setting for Health promotion: Theory and practice. Sage Publications, 2000.

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza8
Establishing BCI stimulus
Communication is a major element of BCI. However, it needs to be implemented asan integrated strategy and not as a stand-alone intervention. In establishingcommunication for behavioural change, the stimulus or source of communication isconsidered as a critical element for achieving the desired change. In other words, togain acceptance and ownership, establishing the credibility of the source ofcommunication is essential.
A further stimulus is the recognition that behavioural change interventions mustmove away from the traditional top-down, one-way processes where the problem,goal, objectives and solutions are conceptualized by people outside the targetcommunity or social system without involving communities that are the intendedbeneficiaries.
Community members must become part of decision-making to make BCI moreeffective. It is well known that early adopters can be effective change agents apartfrom becoming a very credible source of information.
Communication for behavioural change to reduce transmission of avian influenzafrom poultry to humans in various settings should therefore preferably use healthand non-health professionals only as facilitators or catalysts, and allow the individuals,families and communities being targeted to provide input throughout the processincluding identification of content, channels, timing and language, among otheractivities. This is referred to as the “grassroots” approach2.
Conducting Audience Analysis
Once the objectives of BCI have been identified, there is the need to studyepidemiological data, and map and analyse the target audience in relation to:
• Who is the target group – age, gender, economic status, location, education,occupation, language, preferred channels of communication etc.;
• what does the target audience already know about avian influenzatransmission, prevention and control;
• what are the current sociocultural and behavioural characteristics of thetarget group as related to AI;
• whose behaviour needs to change to bring about desired health or socialoutcome;
• what are the predisposing, enabling and reinforcing factors likely to promoteor hinder achievement of desired behavioural change outcomes; and
2Amienyi, O.P. Communicating national integration: Empowering development in African countries, AshgatePubishing, 2005.

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza 9
• what reinforcing factors (policy, structure, political commitment, legislationsetc.) are needed by the affected and service providers to bring about desiredresults.
Conducting communication diagnosis
BCI revolves around communication to achieve desired behavioural change. It mustbe recognized that communities are not necessarily harmonious and therefore it isessential that appropriate assessment is made on each community or group beforeidentifying the most appropriate messages and channels of communication.
Communication messages, viewed as information, are usually conveyed throughinterpersonal channels and the mass media. Interpersonal communication whichincludes group media is intended to reach a specific group with a particular message.The medium used includes but is not limited to discussions, videos, films, drama,song or games. Group media promotes face-to-face interpersonal communicationwith small groups. As opposed to this, the mass media channel is aimed at reachinglarge population groups in different places rapidly. This medium uses television, radio,posters and billboards among others. As a prerequisite for success, the strengths andlimitations of each medium of communication should be established by the programmeplanner or facilitator in order to utilize the approach likely to deliver the desiredresults for behavioural change.
Phase 2: Implementation of BCI
Implementation of BCI includes the following seven elements:
Element 1. Communication for behaviour change (CBC)
Communication for behaviour change is a critical element for the success of behaviouralchange interventions.
What you need to know about communications:
• Communication takes place all the time;
• communication is a vehicle for behavioural change through informationdissemination, attitude and skill-building using appropriate communicationchannels;
• communication is a two-way process involving the transmission of ideas,feelings and attitudes between sender and receiver, both verbally andnonverbally;
• feedback is essential for effective communication. This helps to improveand refine the communication process.

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza10
The challenge about information-seeking behaviour is that often theinformation you have is what you do not need; and what you need, youdo not have. The challenge is getting what you need, when you need it.
The communication loop in Figure 1 encompasses the following:
• Who (sender)
• What (message)
• How (channel)
• To whom (receiver)
• With what effect (response)
“Sender” is the source of communication.
“Encoding” is the process of putting thought into symbolic form.
“Message” is the set of symbols that the sender transmits.
“Channel” refers to how the message moves (interpersonal, mass media etc).
“Receiver” also called the audience, is the party that messages are addressed to.
“Decoding” is the process by which the receiver assigns meanings to the symbolstransmitted by the sender.
Sender (1)
Feedback loop(5)
Feedback loop(4)
Barriers (6)
Message (2)
and channel
Receiver(3)EncodingDecoding
Figure 1: Basic communication style(Verbal and Nonverbal Communication)
Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza 11
“Feedback” is part of the receiver’s response that the receiver communicatesback to the sender.
Barriers to communication
Barriers to communication can operate at various levels—sender, receiver, messageand channel levels. For example,
At sender level:
• Flawed audience and communication analysis;
• ignorance regarding receiver’s prevailing knowledge, attitudes and practices;
• lack of clear communication objectives;
• top-down communication planning that does not invite community inputsand audience participation;
• disregard for social norms including language and culture;
• lack of clear communication objectives;
• insensitivity to feedback.
At receiver level:
• Distrust of source;
• selective perceptions or misperceptions.
At message and channel levels:
• Lack of clarity and reason;
• distracting noises;
• distortion of messages;
• prohibitive cost of mass media.
At organizational level:
• Lack of institutional support, including financial, policy and/or strategy relatedto BCI;
• lack of trained personnel;
• absence of process, outcome or impact assessment.
Facilitating desired behavioural change through communication
For communication to facilitate desired behavioural change, specific requisites shouldbe considered as stated below:
• The intended beneficiaries should regard the source of information as beingcredible.

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza12
• The sender should be willing to communicate and enjoy the trust of thereceiver.
• The sender should be a good listener, be non-judgmental, be aware of theprevailing attitudes and culture related to AI and value the feedback received.
• The sender should communicate solutions only after a problem or questionhas been raised.
• Messages should be delivered in a manner deemed appropriate in terms ofcontent, language, timing, medium and setting.They must be clear, non-conflicting, accurate and sensitive to gender and prevailing culture.
• Messages may need to be prioritized especially when high-risk populationsare being addressed. For instance, CBC will be important in AI-affectedareas to inform the general public including children to keep away fromchickens, ducks and other birds (even as pets), their wastes or feathers; tokeep themselves clean by washing with soap and water whenever they havetouched poultry or poultry faeces and to seek prompt medical attention ifill. Professional cullers on the other hand will, in addition, need to useprotective gear, to properly dispose of diseased bird carcasses and faecesand keep themselves and their work environment scrupulously clean.
• Appropriate messages also need to be addressed to the general public andlocal health authorities.
• The contextual environment in which communication takes place shouldsupport behavioural change. In that regard, BCI requires policies, legislation,advocacy, partnership, resources and capacity building, among other steps,in order to reinforce communication for behavioural change activities.
• Channels selected to convey messages, whether mass media or interpersonal,should be appropriate for the intended audience.
• Research, monitoring and evaluation, not only regarding the effectivenessof communication but the overall BCI, is essential in order to effectivelyinfluence behavioural change and policy decision-making.
• Finally, transparency and accountability should be assured throughout theprocess of communication.
Channels of communication
The two major channels of communication are interpersonal communication (groupmedia) and mass media. The interpersonal channel is a powerful channel to establishpersonal relationships and group consciousness when communicating with individualsand groups in various settings. It is crucial in helping people to make decisions andcomply with intervention activities. Group media facilitates groups, especially themarginalized, to speak to one another and articulate their thoughts and feelings.
Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza 13
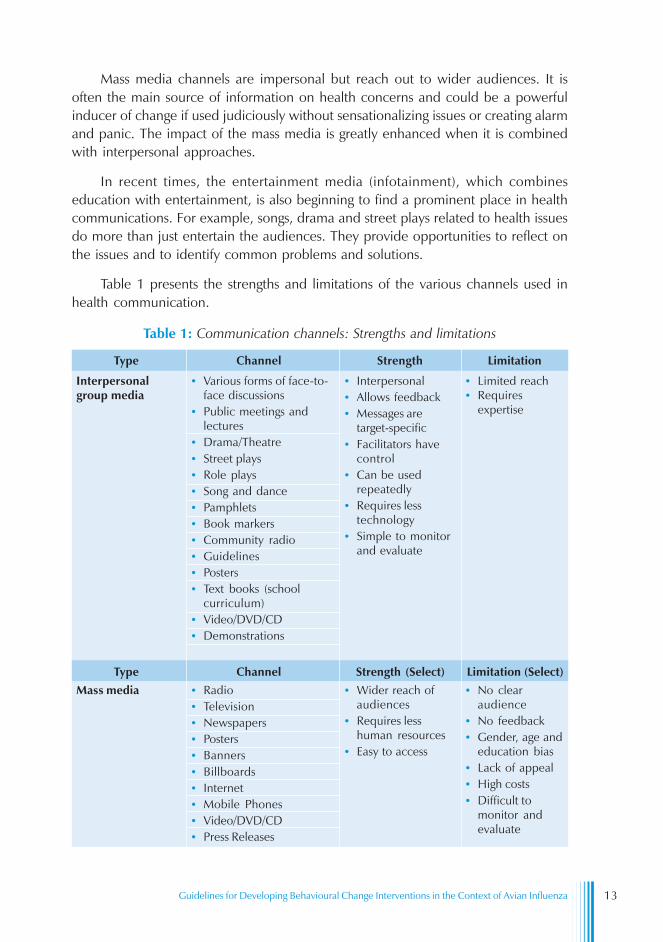
Mass media channels are impersonal but reach out to wider audiences. It isoften the main source of information on health concerns and could be a powerfulinducer of change if used judiciously without sensationalizing issues or creating alarmand panic. The impact of the mass media is greatly enhanced when it is combinedwith interpersonal approaches.
In recent times, the entertainment media (infotainment), which combineseducation with entertainment, is also beginning to find a prominent place in healthcommunications. For example, songs, drama and street plays related to health issuesdo more than just entertain the audiences. They provide opportunities to reflect onthe issues and to identify common problems and solutions.
Table 1 presents the strengths and limitations of the various channels used inhealth communication.
Table 1: Communication channels: Strengths and limitations
• Various forms of face-to-face discussions
• Public meetings andlectures
• Drama/Theatre• Street plays• Role plays• Song and dance• Pamphlets• Book markers• Community radio• Guidelines• Posters• Text books (school
curriculum)• Video/DVD/CD• Demonstrations
• Interpersonal• Allows feedback• Messages are
target-specific• Facilitators have
control• Can be used
repeatedly• Requires less
technology• Simple to monitor
and evaluate
• Limited reach• Requires
expertise
Interpersonalgroup media
• Wider reach ofaudiences
• Requires lesshuman resources
• Easy to access
• No clearaudience
• No feedback• Gender, age and
education bias• Lack of appeal• High costs• Difficult to
monitor andevaluate
• Radio• Television• Newspapers• Posters• Banners• Billboards• Internet• Mobile Phones• Video/DVD/CD• Press Releases
Type Channel Strength Limitation
Type Channel Strength (Select) Limitation (Select)Mass media

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza14
Making communication effective: What you can do
(1) Establish trust and credibility as a communicator.
(2) Demonstrate willingness to communicate.
(3) Use information from the audience analysis study to decide on whatmessages to convey, the preferred language, presentation format and thecommunication channels to be used.
(4) Be inclusive – build a functional partnership with all concerned parties.
(5) Ensure the participation of intended beneficiaries throughout the processof developing risk communication, including designing content, choosingthe medium and monitoring feedback.
(6) Sit down with the affected community and engage them in a dialogue.Listen carefully to their concerns and fears. Respond to these openly andhonestly without exaggerating the negative (or positive) impact of avianflu. Sitting and listening is a sign of empathy for those affected.
(7) Respect cultural values, beliefs and attitudes, particularly those associatedwith health and disease, by addressing the negative values and believes ina sensitive manner and reinforcing the positive ones.
(8) In conveying messages avoid ambiguity and always use multiple channelsfor communicating. By using only a single channel, you will lose theeffectiveness and power that the synergies of multiple media can produce.
(9) Avoid inducing undue anxiety or fear. Present facts as they are known todate and avoid sounding like a salesperson or alarmist, regardless of howdeadly avian flu is thought to be.
(10) If the target group is poultry farmers, establish if there is a historical linkwith avian flu and how it had been managed in the past. The avian flu of1957 and 1968 could provide some leads regarding how communitiesresponded.
(11) In the case of grieving poultry farmers following losses through culling,acknowledge losses but do not promise compensation until it has beensanctioned and communicated in writing.
(12) Recommend protective measures such as the use of disinfectants andprotective clothing and provide details on where they could be accessed.
(13) Always follow set guidelines for using protective gear against possibleexposure to avian influenza. Avoid use of protective gear when visiting wetmarkets or poultry farms where deaths in poultry or avian influenzaoutbreak among poultry has not been reported as this is likely to increasefear among the locals. Overprotection by outsiders could create mistrustbetween intended beneficiaries and service providers. In the event of visiting

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza 15
areas known to be high risk, always make certain the local people who areaccompanying you during the tour are also adequately protected.
(14) Give authoritative guidance regarding early diagnosis and medical care inthe event of the appearance of avian flu signs and symptoms.
(15) Advocate widely to ensure that risk communication to reduce humanexposure from avian flu is integrated into the government policy on diseasepandemics.
(16) Those responsible for coordinating and managing behaviour changeintervention activities at community level should guarantee that beneficiarieshave a right to be heard and to have access to information and protectivedevices.
Word of caution:
• Communication is not a solution for every human need or desireincluding behavioural change.
• Simply giving information does not guarantee behavioural change,irrespective of the source or accuracy of the information.
• All acts of information dissemination must be supported by othercomplementary actions such as community empowerment, policies andparticipation of various players including communities, civil society groupsand the private sector among others. For instance, if the cause of theproblem or its contributing factor as revealed by the situation analysis ispolitical, economic, cultural or any other, there is a need to find solutionsrelated to the identifiable causes.
• What has been communicated cannot be recalled easily. Hence, thereis a need to plan carefully on what is to be communicated.
• Interventions do not conclude when public information campaigns end.Sustainability of the programme must be ensured.
Element 2. Governance: Policy coherence and political commitment
BCI requires the support and commitment of all concerned parties, specifically thedifferent government ministries that are involved in AI control and prevention. Theseministries include agriculture, animal husbandry, health, information and trade. Thepolitical commitment should be in the form of putting in place policies, legislation andregulations and providing financial and technical resources that support, promoteand protect communities from contracting AI, as well as enforcement. It is essential toassess to what extent media policies, laws and regulations in a particular countrycould prohibit or promote free dissemination of information.

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza16
At the South-East Asia Regional Conference of the Ministries of Health,Agriculture and Livestock held in New Delhi in July 2006, the jointMinisterial statement to combat avian influenza articulated acommitment to “improve risk communication in raising public awarenessand empowering communities to take positive action on prevention andcontrol of avian influenza taking into account relevant socio-behavioural,cultural, and economic factors”
Element 3. Planning and implementation
Good planning that recognizes the need to be sensitive to gender, age and to social,political and economic factors is the first step for the successful implementation of BCI.
When planning, care must also be taken to recognize that culture plays a significantrole in determining ways of thinking, believing, and behaving, which may lead toboth positive and negative health behaviours4. If BCI is to have a positive impact onthe target population to relinquish the negative practices associated with AI transmission,cultural values and beliefs related to the co-existence of humans and poultry need tobe fully assessed and understood by AI programme managers. In other words, culturecould either impede or promote the implementation of an effective BCI intervention.However, no single approach or strategy can break the transmission chain.
Element 4. Capacity building
BCI requires concerted efforts in building national capability to plan, implement andmanage activities associated with AI prevention and control. Training in BCI strategyand techniques should be made available to both health and non-health professionalsas well as community leaders and civil society groups working on AI prevention andcontrol at national, provincial (state) and district levels.
Element 5. Social and community mobilization
Social and Community Mobilization as a process of bringing together variousstakeholders including communities to identify and to decide on the action to betaken is a critical element of BCI. In the context of AI, it is aimed to raise people’sawareness about the disease, demand AI-related services and assist in its delivery forsustainability and self reliance.
Element 6. Partnerships, alliances and networks
Participation of various players including communities, civil society groups, the privatesector, media and development partners including WHO and other UN agencies is a
4Airhihenbuwa, C.O. Health and culture: Beyond the western paradigm. Sage Publications, 1955.

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza 17
prerequisite for successful implementation of BCI. The role of partnership is to bringin additional technical and financial resources and increase social responsibility amongpartners and acceptance by communities.
Element 7. Resource mobilization
BCI requires human, financial and infrastructural resources in order to execute activitiessuccessfully. In order to mobilize resources, all activities related with BCI need to beproperly planned, monitored and evaluated. In addition to requesting the governmentto allocate a substantial budget to fight AI, a private–-public sector partnership isencouraged to raise financial and technical support. Ultimately, accountability of allresources allocated to AI prevention and control should be an integral part ofprogramme monitoring and evaluation.
Phase 3: Monitoring, evaluation and research
Monitoring
“Monitoring” is the systematic tracking of the progress of activities that are implementedto ensure that the stated objectives of BCI are met.
Monitoring should form an integral part of all BCI activities to ensure that theprogramme is on track and that deadlines are met. Monitoring also helps in identifyingbottlenecks to allow for corrective action.
Designing appropriate monitoring indicators and establishing a system of feedbackshould be developed at the planning stage of BCI activities. Most monitoring activitiesare carried out through examination of records and reports, supervisory visits andinterviews. Workers could also provide important feedback about the progress of theintervention through regular face-to-face contact with the beneficiaries.
Evaluation
“Evaluation” assesses whether the programme has met its set objectives, its outcomeand impact. Evaluation is fundamental not merely to influence programme and policydirection related to AI prevention and control but also to help all those involved inimplementing BCI, including target communities, to assess the outcome of theprogramme. Just as in monitoring, appropriate evaluation indicators need to bedeveloped to measure each of the BCI elements for outcome and impact. Theminimum acceptable indicator for behavioural change is reported knowledge gain.While evaluation would involve both internal and external experts, communities shouldalso be encouraged to participate in the process. This would provide them with bothskills and a sense of ownership.
Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza18
A well-planned evaluation activity involves formative, process, outcome and impactevaluation that would incorporate all of the BCI elements.
The following example relates to the evaluation of the CBC element of BCI.
Formative: To be conducted before and/or during BCI implementation to assess
– What people think about avian flu interventions
– What messages work(ed) with what audience
– Which of the communication media were found effective
Process: To assess what was accomplished
– Number of people, including children, reached both in high-risk and low- risk situations
– Number of materials produced, trainings conducted, meetingsheld, etc.
– Number of advocacy actions – using group and mass mediatechniques
Outcome: to examine the effect of BCI activities on knowledge, attitudes, beliefsand Values and changes in behaviour, policies, infrastructure andstrategies, to determine
– Any measurable change in perceptions, knowledge, beliefs,attitudes and behaviours associated with AI prevention andcontrol as a result of BCI activities
– Changes in health practices related to BCI
Impact: Measures long-term effects of BCI at community levels. The mainpurpose of impact evaluation is to measure the long-term effects ofBCI on AI prevention and control. Principally, the expected long-term effect is to achieve desired behavioural changes. Nevertheless,human health behaviours are determined by a variety of causesincluding social, cultural, psychological, economic, environmental andgeographical factors. Since these changes occur over a long time, itbecomes difficult to attribute all changes to a specific intervention.The impact evaluation results should be compared against the statedgoal of BCI and should be conducted by qualified individuals withexpertise drawn from stakeholders, target groups and externalconsultants.
In summary, impact evaluation seeks to determine whether changes in attitudesand beliefs produced desired behavioural change and if there were any policy changesresulting from the intervention.

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza 19
Research
Research plays a vital role in influencing policy, intervention strategies, service delivery,communication and advocacy. In the context of BCI for prevention and control of AI,both qualitative and quantitative research methods should be used with a strongfocus on behavioural research and priorities set through a participatory process,mobilizing all those involved in effecting behavioural change. Research objectives mustbe clearly defined and realistically set and high standards maintained to ensure reliablefindings.
Sociocultural and behavioural theories and models that attempt to explain humanbehaviour related to risk-taking, information-seeking, acquisition and utilization, shouldbe applied to fully understand AI transmission and prevention.
Finally, research findings must be disseminated widely and promptly to all stake-holders and the follow-up actions that may be needed carried out without delay.

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza20
Human behaviour is influenced by multiple factors acquired over a long period oftime and hence cannot be changed overnight. Access to information alone does notguarantee behavioural change. This is illustrated by the following analysis which statesthat, “hearing is not knowing; and knowing is not understanding; and understandingis not doing or acting”. Thus, for BCI in AI control and prevention to yield the desiredresults, BCI activities should be implemented in all its phases using an intersectoralapproach which encourages the participation of other players including communitiesand civil society groups as well as beneficiaries. There should be policies, legislationand regulations in place in order to create an environment conducive to AI preventionand control.
Concerted efforts are required to:
(1) Plan AI prevention and control programmes that have clear objectives andimplementation strategies that includes BCI.
(2) Build capacities at country level for intersectoral planning, implementationand evaluation of all AI prevention and control activities, using bothquantitative and qualitative approaches. The findings should be used toimprove behavioural change interventions not only for AI prevention andcontrol but also for other health programmes that seek to address relatedrisk behaviours, preventive behaviours, illness behaviours and compliantbehaviours associated with cultural values, perceptions, belief, and attitudes;
Reinforce desired behavioural changes through continued behavioural changeinterventions, namely, capacity building, policy implementation and enforcement,resource mobilization and participation of various players including government,nongovernmental organizations, civil society groups and the target population.
Conclusion4

Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza 21
Bibliography
(1) World Health Organization, Regional Office for South-East Asia. Public healthinterventions for prevention and control of avian influenza – a manual forimproving biosecurity in the food supply chain: focusing on live animal markets.New Delhi: WHO, 2006.
(2) Amienyi OP. Communicating national integration: empowering development inAfrican countries. Ashgate, 2005.
(3) Poland et al. Setting for health promotion: linking theory and practice. NewDelhi: Sage Publications, 2000.
(4) Airhihenbuwa CO. Health and culture: beyond the western paradigm. California:Sage Publications, 1995.
(5) WHO Global Influenza Programme. WHO global influenza preparedness plan:the role of WHO and recommendations for national measures before and duringpandemics. Geneva : World Health Organization, 2005.
(6) World Health Organization, Regional Office for South-East Asia. Regionalinfluenza preparedness plan (2006-2008). New Delhi, WHO/SEARO, 2006.Document SEA-CD-148.
(7) World Health Organization, Regional Office for South-East Asia. Avian influenzacontrol and pandemic preparedness in Asia: report of the conference of ministersof health, agriculture/livestock.. New Delhi: WHO/SEARO, 2006. DocumentSEA-CD-157.
(8) World Health Organization, Regional Office for South-East Asia. A guide forconducting table-top exercises for national influenza pandemic preparedness.New Delhi: WHO/SEARO, 2006. Document SEA-CD-156.
(9) United Nations Children’s Fund. Behaviour change communication inemergencies: a toolkit.Kathmandu: Regional Office for South Asia (UNICEFROSA), 2006.
(10) Communication for Social Change Consortium. New York. Website:www.communicationforsocialchange.org



















![LEV II V xj .ppt [Kompatibilitetsl ge] - SwedeAmp · 2019. 12. 3. · Interventions that promote behavioural change among health professionals. Interventions that have no or little](https://img.pdfslide.net/doc/110x75/610d7efea039cf5f2733bf55/lev-ii-v-xj-ppt-kompatibilitetsl-ge-swedeamp-2019-12-3-interventions-that.jpg)










