Embed Size (px)
Citation preview

10/27/2013
1
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
Guidelines of Leads extraction An update
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
“The advent of implantable devices has produced the subsequent need for removal of these devices. Malfunction, erosion, pocket infection, endocarditis, and other unique device-related issues are common reasons for removal…..” M. Smith, C.J. Love. Extraction of Transvenous Pacing and ICD Leads. PACE 2008; 31:736–752
Introduction
3.25 mln PM
180.000 ICD
400.000-500.000 nuovi impianti/anno
A. Curnis, L.Bontempi, M. Cerini et al. Complicanze infettive nel paziente portatore di dispositivi: l’estrazione di elettrocateteri. G Ital Cardiol 2010; 11 (10 Suppl 1): 42S-47S
200
420
600
300
Today:
(nu
ovi
im
pia
nti
/m
ilio
ne d
i ab
itan
ti) Complication
In contrast to the relative frequency of lead
failure, either as a result of implantation
error or deterioration of the lead materials,
primary malfunction of the pulse generator
is rare. Infection is another complication of
implanted devices; it is reported to occur from 0.13 up to 19% of the PM patients and from 2 to 7% of the ICD patients. M.G. Bongiorni, G. Giannola, G. Arena et al. Pacing and implantable cardioverter defibrillator transvenous lead extraction. Ital Heart J 2005; 6 (3): 261-266
10/27/2013
2
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
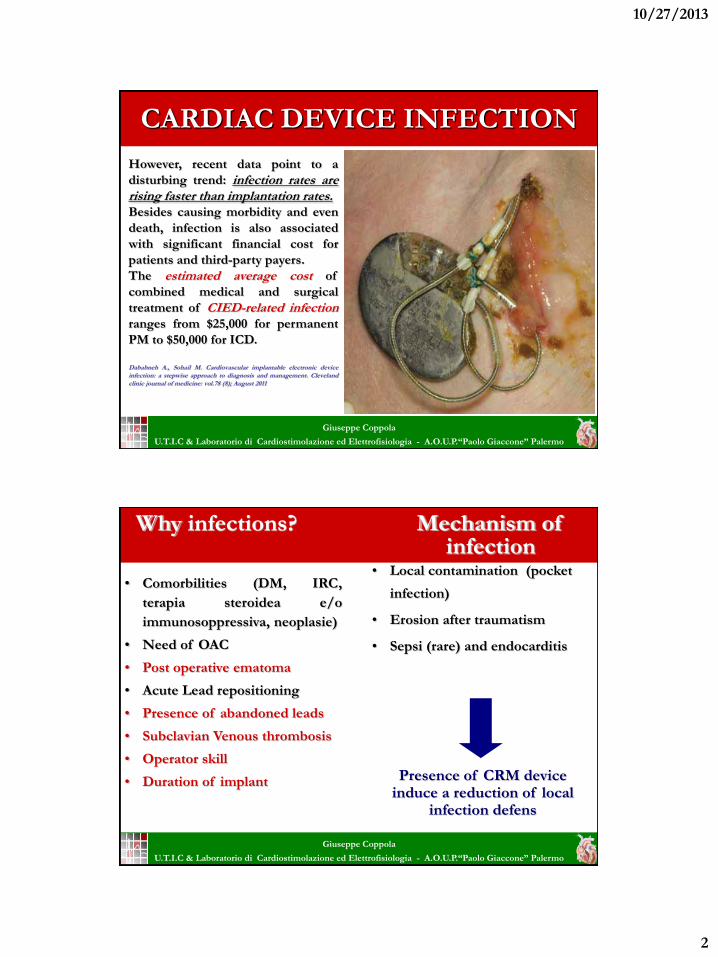
CARDIAC DEVICE INFECTION
However, recent data point to a
disturbing trend: infection rates are rising faster than implantation rates. Besides causing morbidity and even
death, infection is also associated
with significant financial cost for
patients and third-party payers.
The estimated average cost of
combined medical and surgical
treatment of CIED-related infection
ranges from $25,000 for permanent
PM to $50,000 for ICD.
Dababneh A., Sohail M. Cardiovascular implantable electronic device infection: a stepwise approach to diagnosis and management. Cleveland clinic journal of medicine: vol.78 (8); August 2011
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
• Comorbilities (DM, IRC,
terapia steroidea e/o
immunosoppressiva, neoplasie)
• Need of OAC
• Post operative ematoma
• Acute Lead repositioning
• Presence of abandoned leads
• Subclavian Venous thrombosis
• Operator skill
• Duration of implant
Why infections?
• Local contamination (pocket
infection)
• Erosion after traumatism
• Sepsi (rare) and endocarditis
Mechanism of infection
Presence of CRM device induce a reduction of local
infection defens

10/27/2013
3
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
MICROBIOLOGY OF DEVICE INFECTION
Site of infection Microorganismo isolato
Device or leads Stafilococco Epidermidis *
(senza coinvolgimento IV) Stafilococco Aureus *
Corinebatteri
Escherichia coli
Proteus
Enterobatteri
Batteriemia o endocardite Stafilococco Aureus *
Stafilococco Epidermidis *
Pseudomonas Aeruginosa
Klebsiella
Proteus
Serratia Marcescens
* = Batteri più comunemente involti (72-95%)
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
Indications for lead Extraction are evolving!
The need for lead extraction is rapidly increasing
due to:
New indication for device treatment
Higher lead prevalence due to increased life expectancy
CIED modes requiring more lead for patient
Upgrading from device systems becoming more frequent
Lead Recalls
Lead Infections
Maytin M and Epstein LM. Cardiology, 2009;6(2):51-3

10/27/2013
4
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
Laser sheath for tunnelled
dialysis catheters
extraction: a case report. Curnis A., Bontempi L., Coppola G. et al.
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
The Byrd Classification (1990) Systemic Infection Mandatory
Local Infection Necessary
Malfunction Discretionary
Indications for lead Extraction are evolving!
PACE 2000
HRS 2009

10/27/2013
5
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
DEFINITION (procedura)
Lead Removal: Removal of a pacing or defibrillator lead using any
technique.
Lead Explant: A lead removal using simple traction techniques (no locking
stylet, telescoping sheaths or femoral extraction tools).
Lead Extraction: Removal of a lead that has been implanted for more than
1 year (less for ICD), or a lead regardless of duration of implant requiring the
assistance of specialized equipment that is not included as part of the typical
implant package, and/or removal of a lead from a route other than via the
implant vein.
Heart Rhythm, Vol 6, No 7, July 2009
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
HRS 2009 Indications
INFECTION
CHRONIC PAIN
THROMBOSIS OR VENOUS STENOSIS
FUNCTIONAL LEADS
NON-FUNCTIONAL LEADS

10/27/2013
6
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
INFECTIONS – Class I
1) Complete device and lead removal is recommended in all patients with
definite CIED systemic infection, as evidenced by valvular endocarditis lead
endocarditis or sepsis. (LOE: B)
2) Complete device and lead removal is
recommended in all patients with CIED
pocket infection as evidenced by pocket
abscess, device erosion, skin adherence, or
chronic draining sinus without clinically
evident involvement of the transvenous
portion of the lead system. (LOE: B)
3) Complete device and lead removal is recommended in all patients with
valvular endocarditis without definite involvement of the lead(s) and/or
device. (LOE: B) 4) Complete device and lead removal is recommended in patients with occult
gram+ bacteremia (not contaminant). (LOE: B)
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
INFECTIONS – Class II a
Complete device and lead removal is reasonable in patients with persistent
occult gram-negative bacteremia. (LOE: B)
INFECTIONS – Class III 1) CIED removal is not indicated for a superficial or incisional infection
without involvement of the device and/or leads. (Level of evidence: C)
2) CIED removal is not indicated to treat chronic bacteremia due to a source
other than the CIED, when long term suppressive antibiotics are required.
(LOE: C)
Device and/or lead removal is reasonable in patients with severe chronic pain, at
the device or lead insertion site, that causes significant discomfort for the
patient, is not manageable by medical or surgical techniques and for which there
is no acceptable alternative. (LOE: C)
CHRONIC PAIN – Class II a

10/27/2013
7
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
THROMBOSIS/VENOUS STENOSIS – Class I
1) Lead removal is recommended in patients with clinically significant
thromboembolic events associated with thrombus on a lead or a lead
fragment. (LOE: C)
2) Lead removal is recommended in patients with bilateral subclavian V or SVC
occlusion precluding implantation of a needed transvenous lead. (LOE: C)
3) Lead removal is recommended in patients with planned stent deployment in
a vein already containing a transvenous lead, to avoid entrapment of the lead.
(LOE: C)
4) Lead removal is recommended in patients with SVC stenosis or occlusion
with limiting symptoms. (LOE: C)
5) Lead removal is recommended in patients with ipsilateral venous occlusion
preventing access to the venous circulation for required placement of an
additional lead when there is a contraindication for using the contralateral
side (e.g. contralateral AV fistula, shunt or vascular access port, mastectomy).
(LOE: C)
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
THROMBOSIS/VENOUS STENOSIS – Class I
Lead removal is reasonable in
patients with ipsilateral venous
occlusion preventing access to the
venous circulation for required
placement of an additional lead,
when there is no contraindication
for using the contralateral side.
(LOE: C)
OCCLUSION of the vein
with the need to add 1 or
more leads

10/27/2013
8
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
FUNCTIONAL and NON FUNCTIONAL LEADS: Class I
1) Lead removal is recommended in
patients with life threatening arrhythmias
secondary to retained leads. (LOE: B)
2) Lead removal is recommended in patients
with leads that, due to their design or their
failure, may pose an immediate threat to the
patients if left in place (Telectronics
ACCUFIX J wire fracture with protrusion).
(LOE: B)
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
FUNCTIONAL and NON FUNCTIONAL LEADS: Class I
3) Lead removal is
recommended in patients
with leads that interfere with
the operation of implanted
cardiac devices. (LOE: B)
4) Lead removal is
recommended in patients
with leads that interfere with
the treatment of a
malignancy (radiation or
reconstructive surgery).
(LOE: C) Inappropriate shocks

10/27/2013
9
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
FUNCTIONAL and NON FUNCTIONAL LEADS: Class II a
1) Lead removal is reasonable in patients
with functioning leads that due to their
design or their failure pose a threat to the
patient, that is not immediate or
imminent if left in place. (e.g.
Telectronics ACCUFIX without
protrusion). (LOE: C)
2) Lead removal is reasonable in patients if
a CIED implantation would require 4 or
more leads on one side or 5 or more leads
through the SVC. (LOE: C)
3) Lead removal is reasonable for patients that require specific imaging
techniques (e.g. MRI) and can not be imaged due to the presence of the CIED
system for whom there is no other available imaging alternative for the
diagnosis. (LOE: C)
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
FUNCTIONAL LEADS: Class II b
1) Lead removal may be considered in patients with an abandoned functional
lead that poses a risk of interference with the operation of the active CIED
system. (LOE: C)
2) Lead removal may be considered in patients with functioning leads that due
to their design or their failure pose a potential future threat to the patient if
left in place. (e.g. Telectronics ACCUFIX without protrusion). (LOE: C)
3) Lead removal may be considered in patients with leads that are functional
but not being used. (i.e. RV pacing lead after upgrade to ICD) (LOE: C)
4) Lead removal may be considered in patients who require specific imaging
techniques (e.g. MRI) that can not be imaged due to the presence of the
CIED system for which there is no other available imaging alternative for the
diagnosis. (LOE: C)
5) Lead removal may be considered in patients in order to permit the
implantation of an MRI conditional CIED system. (LOE: C)

10/27/2013
10
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
NON FUNCTIONAL LEADS: Class II b
1) Lead removal may be considered at the time of an indicated CIED procedure,
in patients with non-functional leads, if contraindications are absent. (LOE C)
2) Lead removal may be considered in order to permit the implantation of an
MRI conditional CIED system. (LOE: C)
FUNCTIONAL and NON FUNCTIONAL LEADS: Class III
1) Lead removal is not indicated in patients with redundant leads if patients
have a life expectancy of less than one year. (LOE: C) 2) Lead removal is not indicated in patients with known anomalous placement
of leads through structures other than normal venous and cardiac structures,
(e.g. subclavian artery, aorta, pleura, atrial or ventricular wall or mediastinum)
or through a systemic venous atrium or systemic ventricle. Additional
techniques including surgical backup may be used if the clinical scenario is
compelling. (Level of evidence: C)
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
Undesired LV pacing!! A. Curnis, L. Bontempi1, G. Coppola et al. G Ital Cardiol 2011;12(11):724-725
PFO

10/27/2013
11
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
BE CAREFUL!!!
“Recommendations for lead extraction apply only to those patients in whom the benefits of lead removal outweigh the risks when assessed, based on individualized patient factors and operator specific experience and outcomes.”
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo
…NON FA SCIENZA, SENZA LO RITENERE,
AVERE INTESO….

10/27/2013
12
Giuseppe Coppola
U.T.I.C & Laboratorio di Cardiostimolazione ed Elettrofisiologia - A.O.U.P.“Paolo Giaccone” Palermo





























