Embed Size (px)
Citation preview

1
Guidelines on the Management of COVID-19 in Obstetrics
Addendum to the first revision dated 3rd February 2021
30th August 2021 The maternal and fetal implications of COVID-19 infection among pregnant mothers in Malaysia remains significant. 3,396 mothers have been confirmed to be positive between March till June 2021 and the incidence continues to rise. Although almost 1% of pregnant mothers were tested positive in Malaysia, between 3.0 to 5.5% required ICU admissions. This means that about 1 in 20 pregnant mothers will require intensive care and ventilation if infected with SARS-CoV-2. As of 9th August 2021, there has been a total of 70 maternal deaths due to COVID-19 infection in Malaysia.
Phase 2 of the National COVID-19 Immunisation Programme was initiated in June 2021 and pregnant mothers were identified and prioritized as a vulnerable group. 146,759 pregnant mothers have been vaccinated in Malaysia as of 8th of August 2021.
This update is in keeping with the evidence from medical literature, which has emerged since the last edition, to ensure pregnant mothers in Malaysia continue to receive optimal care in COVID-19.
Updates
i) Importance of a consultant led multi-professional approach in managing COVID-19 pregnant mothers which includes physicians, senior obstetrician, infectious disease specialist, intensivist, respiratory physicians, rehab physicians and psychiatrist.
ii) Home surveillance of COVID-19 pregnant mothers iii) Safety of X-ray, CTPA and high-resolution CT scans in pregnancy iv) VTE risk assessment of COVID-19 mothers and update on
thromboprophylaxis v) Steroids for COVID-19 mothers and steroids for fetal lung maturity vi) Safety of Tocilizumab in pregnancy vii) Prone positioning of pregnant mothers viii) When to deliver and surgical modifications ix) Fetal optimization x) Post-COVID patients xi) Mental health xii) Pregnant frontliners
Annex 23a

2
1) General advice for pregnant mothers
It is important that all pregnant mothers, their household and close contacts adhere to the MOH recommendations on physical distancing, wearing a double mask, face shield and maintaining hand hygiene.
If anyone in the household or close contacts are confirmed to be positive for COVID-19, it is important for them to self-isolate from others, especially pregnant mothers. If pregnant mothers are symptomatic or have significant contact, it is important to be tested, diagnosed early and appropriately risk stratified.
Routine supplementation of Vitamin C or Vitamin D to prevent COVID-19 infection is not recommended, although it has been used in patients who have been confirmed positive. No other additional supplements have been proven to be beneficial. 2) Home monitoring of COVID-19 pregnant mothers
While it is preferable that pregnant mothers are monitored as in-patient, this is not always possible due to resource limitations. The option of home quarantine can be considered if the following criteria are fulfilled:
Evidence-based, multi-professional approach is essential and shared decision-making is central to the management of COVID-19 mothers. Life-saving interventions should not be withheld in pregnancy and breastfeeding.
Although vaccination reduces the incidence of hospital admissions and deaths, it does not prevent infections. Physical distancing, double masking, use of face shield and hand hygiene remains imperative.
All newly-diagnosed pregnant mothers with COVID-19 should be risk stratified to identify the most appropriate monitoring facility. All women who are planned for home quarantine should be given advice on red flag signs, able to utilize the Home Assessment Tool and know when to seek help.
Annex 23a

3
Patients who fulfill the criteria for home quarantine should be tagged and provided with Home Assessment Tool (Appendix 1). If there are any urgent obstetric issues that develop within this isolation period, these patients should be managed as per MOH guidelines and retrieval should be arranged by the nearest health care facility to a COVID / Hybrid Hospitals. Patient and caregivers will be given advice on:
• Category 1 or Category 2 < 22 weeks of gestation • No medical co-morbidities • BMI < 35 kg/m2 • Age < 40 years old • No per vaginal bleeding / hyperemesis gravidarum • Adequate understanding and adherence to protocol • Able to contact nearest healthcare facility • Contactable at all times • If possible to avoid the following persons in the house o Adults over the age of 60 years
o Immunocompromised o Adult with co-morbidities o Young children < 12 years
• Compliance to home assessment tool • Consider monitoring these mothers at a dedicated PKRC if feasible which with
easy access to tertiary hospitals • Basic infection prevention control measures such as hygiene and cough
etiquette • Self-monitoring: symptoms / temperature / oxygen saturation / pulse rate • Continuation of prenatal vitamins • To contact nearest health care facility if urgent obstetric issue • RED FLAGS and importance of seeking immediate attention
Annex 23a

4
• Separate room with adequate ventilation
• Separate bathroom • If possible, avoid if there are adults over the age of 60
years/immunocompromised/adults with multiple comorbidities/young children < 12 years old
• Do not share utensils with family members house occupants • Do not eat meals together • Do not share the same bathroom. If needed, to clean bathroom with
household detergent and water
Caregivers/cleaners need to always wear face mask and face shield when handling contaminated items or waste and dirty laundry • Contaminated items or waste should be separately disposed in a
plastic bag by patient followed by a second bagging by the care giver • Dirty laundry should be washed separately and to wear gloves during
cleaning
• Be contactable at all times • Able to seek medical attention immediately to the nearest health care
facility
Annex 23a

5
3) Safety of imaging in pregnancy
Gestational age (weeks)
Effects of <50mGy
Effects of 50-100mGy
Effects of >100mGy
Estimated threshold dose
0-2 None None None 50-100mGy
3-4 None Probably none Possible miscarriage
50-100mGy
5-10 None Uncertain Possible congenital anomalies, IUGR
200-250mGy
11-17 None Uncertain Risk of diminished IQ, microcephaly
60-310mGy 25 IQ point loss per
1000mGy
> 18 weeks None None
TYPE OF EXAMINATION FETAL RADIATION DOSE (mGy)
Very low dose examination (<0.1mGy)
Chest X-ray (two views) 0.0005 - 0.01
Low to moderate dose examination (0.1–10 mGy)
Chest CT or CT pulmonary angiography (CTPA) 0.01 - 0.66
High resolution CT thorax Low dose protocol Ultra-low dose protocol
1.6 ± 0.3 1.1 ± 0.3
Low-dose perfusion scintigraphy 0.1 - 0.5
Pulmonary digital subtraction angiography (DSA) 0.5
Higher dose examination (10–50 mGy)
Abdominal CT 1.3 - 35
Pelvic CT 10.50
• Imaging is an important adjunct to facilitate diagnosis and guide management.
• Fetal radiation dose of <50mGy is considered safe and does not causes any harm.
• Ultra-low-dose HRCT can be reliably used during the COVID-19 pandemic to reduce the hazards from radiation exposure. Its sensitivity exceeds 90%.
Annex 23a

6
4) Thromboprophylaxis among COVID-19 positive mothers
Normal physiological changes in pregnancy result in alteration of maternal blood volume and reduced fibrinolysis. This hypercoagulable state coupled with the microthrombotic nature of COVID-19, makes pregnant mothers susceptible to venous thromboembolism (VTE).
All pregnant women should have an individualized risk stratification for VTE by using the VTE risk scoring table at COVID-19 Assessment Centres (CAC), regardless if she requires home quarantine or admission to a health facility (see Appendix 2). This is consistent with the MOH “VTE in Pregnancy and Puerperium” guidelines published in 2018.
In healthcare facilities without diagnostic imaging services, where the suspicion is high for a thromboembolic event, the patient should be treated with therapeutic doses of LMWH while awaiting further management. Thrombocytopenia is observed in 6.6% of pregnant women with COVID-19 infection but only a small subset is severe enough to cause concern with routine thromboprophylaxis.
Category of disease
Quarantine Centre
VTE score
LMWH Duration of thromboprophylaxis
Category 1 & 2
Home Quarantine / CAC / PKRC
1 LMWH if VTE score is >3
Based on VTE score
Category 1 - 3
Hospital admission
3 Prophylactic dose of LMWH
Start on admission and continue for a minimum of 10
days following discharge
Category 3 +
High risk factors*
Hospital admission
>3 Consider High prophylactic
doses
Start on admission and continue for a minimum of 10
days following discharge**
Category 4 & 5
Irrespective of risk factor and VTE score
Consider treatment dose of LMWH
Start on admission and continue for 10-21 days
following discharge
*High risk factors: Cardiac disease, active SLE, BMI > 35kg/m2,diabetic nephropathy, nephrotic syndrome **Long COVID: Patient may require thromboprophylaxis > 10 days post-discharge
• VTE risk assessment should be done for all pregnant women routinely at the CAC.
• Interval VTE assessment is required during in-patient care. In the event of deterioration, treatment should be escalated, with a low threshold to exclude pulmonary embolism.
• Anticoagulation therapy during labour and delivery should be managed as per standard obstetric protocol.
• If anticoagulation was initiated prior to the diagnosis of COVID-19, it should be continued.
Annex 23a

7
Dosing regimens for Enoxaparin
BODY WEIGHT PROPHYLACTIC DOSE LMWH
HIGH PROPHYLACTIC
DOSE LMWH
TREATMENT DOSE LMWH
<50 kg 20mg OD 40mg OD 40mg BD
50- 69 kg 40mg OD 60mg OD 60mg BD
70-89 kg 40mg OD 80mg OD 80mg BD
90-109 kg 60mg OD 100mg OD 100mg BD
110-124kg 60mg OD 120mg OD 120mg BD
125-130 kg 60mg OD Liaise with haematologist
Liaise with haematologist
131-170 kg 80mg OD
>170 kg 100mg OD
CONSIDER DEFERRING OR WITHHOLDING THROMBOPROPHYLAXIS IF: • Delivery is expected within the next 12-24 hours • Anticipated bleeding • Disseminated intravascular coagulation • Thrombocytopenia <100K • Severe septicemia
Annex 23a

8
5) Corticosteroids for COVID-19 in pregnancy
Pregnant women with medical comorbid may have been on steroids prior to SARS-Cov-2 infection and this should not be ceased abruptly, especially if women have been on long term steroids. In RECOVERY, a multicenter, open-label trial in the United Kingdom, hospitalized patients with COVID-19 were randomized to receive either dexamethasone plus standard of care or standard of care alone (control arm). In the subgroup of participants who did not require supplemental oxygen at enrollment, no survival benefit was observed for dexamethasone; 17.8% of participants in the dexamethasone arm and 14% in the control arm died within 28 days of enrollment (rate ratio 1.19; 95% CI, 0.91–1.55). In this trial, low-dose dexamethasone (6 milligrams) reduced mortality by up to one-third among COVID-19 patients on mechanical ventilation and one-fifth among those who received supplemental oxygen. Pregnant women in this trial received either oral prednisolone or intravenous hydrocortisone. Unlike dexamethasone, prednisolone and hydrocortisone are extensively metabolized in the placenta with minimal transfer to the fetus. While the neonatal benefits of fluorinated antenatal corticosteroids are well-established when administered to women at risk of imminent preterm birth, exposure to repetitive doses of steroids is associated with adverse neonatal outcomes.
Furthermore, the WHO REACT meta-analysis, which included data from the RECOVERY trial, suggested that the benefit of glucocorticoid was a class effect. However, it did not specifically recommend any steroid regimen for pregnant women with COVID-19. The Royal College of Obstetricians and Gynaecologists (RCOG) suggest that corticosteroid therapy should be considered for 10 days or up to discharge, whichever is sooner, for women who are unwell with COVID-19 and requiring oxygen supplementation or ventilatory support. The following steroid regimen was proposed:
• Pregnant women who require steroids for other medical conditions, including inhalational steroids, may continue their use.
• If steroids are indicated for obstetric reasons in addition to COVID-19 infection, dexamethasone is appropriate.
• If steroids are not required for obstetric reasons, oral prednisolone or hydrocortisone can be considered.
Annex 23a

9
Type of steroid Plasma half-life (min)
Biological half- life (hours)
Glucocorticoid potency
Mineralo-corticoid potency
Placental transfer
(%)
Maternal-fetal ratio
Hydrocortisone 90 Short acting (8-12)
1 1 15 6.7 : 1
Prednisolone 200 Intermediate acting (12-36)
4 0.8 10-12.5
8-10 : 1
Methyl- prednisolone
180 Intermediate acting (12-36)
5 0.5 44 2.24 : 1
Dexamethasone 200-300 Long acting (36-54)
20-30 0 50 2 : 1
Betamethasone 300 Long acting (36-54)
20-30 0 33 3 : 1
If steroids are indicated for obstetric reasons (fetal lung maturity)
If steroids are not indicated for obstetric reasons (fetal lung maturity)
IM dexamethasone 6mg 12 hourly for 4 doses then oral prednisolone 40 mg OD or IV hydrocortisone 80mg BD
Oral prednisolone 40mg OD or IV hydrocortisone 80mg BD
For 10 days or until discharge, whichever is sooner
For 10 days or until discharge, whichever is sooner
6) Safety of tocilizumab in pregnancy
The REMAP-CAP trial was an essential trial which showed improved outcomes and survival among critically ills patients being given interleukin 6 receptor antagonist, namely tocilizumab and sarilumab. It remains a targeted therapy among patients with clinical evidence of a cytokine storm.
The UK teratology information service guidelines on the use of tocilizumab in pregnancy recommends no evidence related to tocilizumab with regards to teratogenicity and fetal toxicity. It was widely being used among patients with rheumatoid arthritis in pregnancy. The global safety database for the use of tocilizumab in pregnancy showed no association with teratogenicity even if used on the first trimester.
However, in resource-limited settings where access to tocilizumab may be limited or not available, the alternative option of Baricitinib can be used if deemed essential as the pregnant mother should not be denied a lifesaving medication or intervention.
Tocilizumab is safe in pregnancy. If unavailable, consider Baricitinib as an alternative.
Annex 23a
10
7) Prone positing of pregnant mothers
The benefits of prone positioning among selected group of COVID-19 mothers has been established and remains a standard of care. Pregnancy is not an absolute contraindication for this positioning and delivery should not be performed solely to facilitate prone positioning.
A. Prone positing of an awake mother
https://www.youtube.com/watch?v=7orutHYuXFQ
B. Prone positioning of an intubated mother
https://www.youtube.com/watch?v=SOgwakxeyXE
Pregnant mother can be nursed in a prone position, with certain modifications, without the immediate need for delivery.
Annex 23a

11
8) Medications which should not be used in the treatment of COVID-19
The following medications have been shown to be ineffective in improving outcomes in COVID-19 and should not be used solely for its management:
• Hydroxychloroquine
• Lopinavir or ritonavir
• Remdesivir
9) Delivery in ill obstetric patients
Generally, timing of delivery should be determined by obstetric indications rather than the diagnosis of COVID-19. However, in ill pregnant women, such decisions are complex, involves many clinical variables yet may have to be made within a short period of time. Therefore, it is recommended that these decisions are multidisciplinary, involving the consultant obstetrician, anaesthetist, infectious disease physician and paediatrician, amongst others, in addition to the patient’s family. Appendix 3 shows the process flow chart of intrapartum care of COVID-19 mothers. It is also recognized that severely ill women beyond the age of viability with increasing ventilatory requirements may benefit from early delivery. These include women with severe hypoxemia unresponsive to incremental increases in positive end expiratory pressure (PEEP), prone positioning and/or deep sedation with chemical paralysis.
Care in high-dependency unit (HDU) or intensive care unit (ICU) alone is not an indication for delivery.
Antenatal mothers who have recovered from COVID-19 earlier in pregnancy would require no alteration in their timing of delivery
• The decision for delivery in pregnant women with COVID-19 is complex and should involve consultants across various specialties, namely obstetricians, intensivist, anaesthetist, infectious diseases specialist and paediatrician.
• Expedient delivery may be indicated in women with increasing ventilatory requirements especially if the managing team perceives that the cardiorespiratory benefits following delivery is far beneficial to the mother as compared to the benefits of prolonging the pregnancy.
• Resuscitative hysterotomy (Perimortem caesarean section) should be considered in maternal collapse due to COVID-19.
Annex 23a
12
10) Surgical considerations during caesarean section
To avoid potential delays in managing surgical complications, including massive obstetric haemorrhage, the senior-most personnel available should perform surgeries in pregnant women with COVID-19. Operating under less than optimal conditions due to these circumstances can make it difficult for less experienced personnel. Consideration has to be given to the time taken for donning of personal protective equipment (PPE) when calling for additional help.
Although there is concern with the prothrombotic state in COVID-19 in addition to the risks conferred by pregnancy itself, tranexamic acid and carboprost use is not contraindicated to arrest bleeding. It may be reasonable to avoid routine prophylactic use of tranexamic acid.
Intraperitoneal and subrectus drains may be considered, especially in women on higher than prophylactic dose of heparin and when associated with severe thrombocytopenia. Meticulous haemostasis is essential to reduce the likelihood of postoperative haematoma and additional surgery for wound closure.
Protamine sulphate may be considered where bleeding is due to anticoagulation use. A maximum dose of 50mg protamine sulphate can be used.
• The senior-most personnel should perform the operation to avoid delays in managing complications due to the additional time incurred by donning of PPEs.
• Tranexamic acid and carboprost can be used to arrest bleeding
• Meticulous haemostasis is essential to reduce postoperative bleeding
• Consider intraperitoneal / subrectus drains and protamine sulphate where appropriate
Annex 23a

13
11) Fetal optimization
Antenatal steroids Clinical considerations for the use of corticosteroids for fetal lung maturity and treatment of COVID-19 patients requiring oxygen has been explained in the previous section.
Magnesium sulphate Magnesium sulfate therapy is recommended for neuroprotection of the neonate, and should be offered to women up to 31+6 weeks of gestation. The dose is similar to those given for prevention of eclampsia and should ideally be administered for at least 4 hours preceding delivery.
Delayed cord clamping can be performed as usual during delivery There is a theoretical concern that a partially detached placenta in women with infectious diseases could expose the baby to maternal blood leading to microtransfusion to the baby. However, findings from 405 women with SARS-CoV-2 infection who were enrolled in a prospective observational study where 231 newborns (57.3%) had early cord clamping (ECC) and 172 newborns (42.7%) had delayed cord clamping (DCC) were reassuring. 1.7% of newborns had a positive nasopharyngeal PCR in the first 12 hours postpartum; 2 (1.7%) ECC vs 3 (3.6%) DCC. This was in spite of a higher proportion of women in the ECC cohort who had skin-to-skin contact and breastfeeding immediately in the postpartum period.
12) Management of post-COVID patients
Patients who had Category 1 or 2 disease should ideally be assessed within 14 days following discharge in the nearest health clinic to ensure they remain well. A holistic approach looking for possible complications of long or post-COVID syndrome, namely fatigue, pain, fever, cardiovascular, respiratory and psychological implications should be systematically assessed. If there are concerns, they should be referred to the nearest specialist O&G clinic for an early review. A VTE risk assessment is also essential.
Pregnant mothers who recovered from COVID-19 should be assessed within 14 days post discharge. Category 1 & 2 mothers can be assessed at the health clinic while category 3,4 or 5 should be reviewed in the O&G specialist clinic.
Consider the use of magnesium sulphate infusion of at least 4 hours for fetal neuroprotection for women up to 31+6 weeks of gestation. Delayed cord clamping is not a contraindication.
Annex 23a
14
Patients who recovered from category 3, 4 or 5 should ideally be reviewed in the O&G specialist clinic within 14 days from discharge. Although there are no specific fetal implications, assessing for complications such as thromboembolism, organizing pneumonia, secondary infections or breathlessness are part of a holistic approach to detection of long-COVID syndrome (refer Appendix 4: Flow chart for Follow up of long COVID-19 patients).
13) Mental health and COVID-19
• Mental health screening should be performed on each encounter, with the aid of the Whooley’s questionnaire.
• Perinatal mental health team should be involved in the joint management of women with mental health conditions.
• All healthcare professionals should be able to recognise and respond to perinatal mental health problems.
Annex 23a

15
The COVID-19 pandemic has had a major impact on pregnant women who are vulnerable to the risk of severe COVID-19 infection, coping with preterm birth and mental health conditions such anxiety, self-isolation, depression, dissociative conditions and domestic violence. Women should be advised on
Women should be assessed and onward referral to the perinatal mental health team performed where indicated
14) Pregnant healthcare professionals and frontliners
Appreciating the significance and occupational hazards of pregnant healthcare frontliners who serve beyond their call of duty, it is advisable that our frontliners are protected and not directly involved in the management of COVID-19 patients beyond 22 weeks of pregnancy, despite being fully vaccinated. The rationale for this consensus is based on the risk of developing severe COVID-19 infection in the late second and third trimester. This however, should be based on available local resources and the extent of the pandemic.
If feasible, pregnant healthcare professionals and frontliners beyond 22 weeks of pregnancy should not directly be involved in the management of COVID-19 patients.
• Maintaining a healthy lifestyle, proper diet and regular exercise • Availability of online support groups for pregnant mothers • Availability of mental health helplines • Practice relaxation techniques (breathing exercises) • RED flag signs and to seek help immediately if present • Connect with family members and loved ones
RED FLAGS • Suicidal ideation • Poor sleep quality • Poor appetite • Harm to baby • Psychotic symptoms
Annex 23a
16
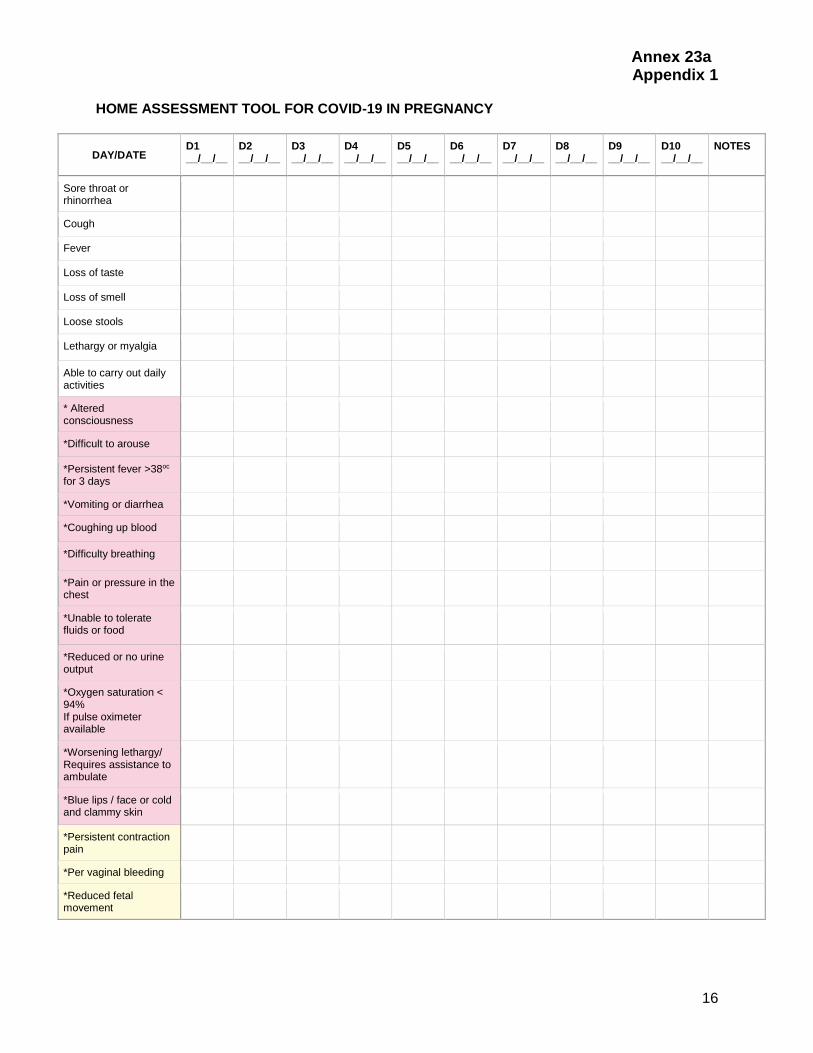
Appendix 1 HOME ASSESSMENT TOOL FOR COVID-19 IN PREGNANCY
DAY/DATE D1 __/__/__
D2 __/__/__
D3 __/__/__
D4 __/__/__
D5 __/__/__
D6 __/__/__
D7 __/__/__
D8 __/__/__
D9 __/__/__
D10 __/__/__
NOTES
Sore throat or rhinorrhea
Cough
Fever
Loss of taste
Loss of smell
Loose stools
Lethargy or myalgia
Able to carry out daily activities
* Altered consciousness
*Difficult to arouse
*Persistent fever >38oc
for 3 days
*Vomiting or diarrhea
*Coughing up blood
*Difficulty breathing
*Pain or pressure in the chest
*Unable to tolerate fluids or food
*Reduced or no urine output
*Oxygen saturation < 94% If pulse oximeter available
*Worsening lethargy/ Requires assistance to ambulate
*Blue lips / face or cold and clammy skin
*Persistent contraction pain
*Per vaginal bleeding
*Reduced fetal movement
Annex 23a

17
Appendix 2 VTE risk assessment
Annex 23a

18
Appendix 3 Flow chart for intrapartum care of COVID-19 mothers
Annex 23a

19
Appendix 4 Flow chart for follow up of long COVID-19 patients
Annex 23a
20
References 1. MOH guidelines on COVID-19 Vaccination among pregnant and breastfeeding mothers 2. UKTIS. Use of tocilizumab in pregnancy 3. Jiménez-Lozano, I., Caro-Teller, J.M., Fernández-Hidalgo, N., Miarons, M., Frick, M.A.,
Batllori Badia, E., Serrano, B., Parramon-Teixidó, C.J., Camba-Longueira, F., Moral-Pumarega, M.T., San Juan-Garrido, R., Cabañas Poy, M.J., Suy, A. and Gorgas Torner, M.Q. (2021), Safety of tocilizumab in COVID-19 pregnant women and their newborn: A retrospective study. J Clin Pharm Ther, 46: 1062-1070. https://doi.org/10.1111/jcpt.13394
4. Hoeltzenbein M, Beck E, Rajwanshi R, Gøtestam Skorpen C, Berber E, Schaefer C, Østensen M. Tocilizumab use in pregnancy: Analysis of a global safety database including data from clinical trials and post-marketing data. Semin Arthritis Rheum. 2016 Oct;46(2):238-245. doi: 10.1016/j.semarthrit.2016.05.004. Epub 2016 May 25. PMID: 27346577.
5. Tolcher MC, McKinney JR, Eppes CS, Muigai D, Shamshirsaz A, Guntupalli KK, Nates JL. Prone Positioning for Pregnant Women With Hypoxemia Due to Coronavirus Disease 2019 (COVID-19). Obstet Gynecol. 2020 Aug;136(2):259-261. doi: 10.1097/AOG.0000000000004012. PMID: 32516274.
6. TOG 2019 :imaging in pregnancy 7. World Health Organization. Guideline: Delayed umbilical cord clamping for improved
maternal and infant health and nutrition outcomes. 2014. Available from https://apps.who.int/iris/bitstream/handle/10665/148793/9789241508209_eng.pdf [Accessed 12th August 2021]
8. Mejía Jiménez I, Salvador López R, García Rosas E, et al. Umbilical cord clamping and skin-to-skin contact in deliveries from women positive for SARS-CoV-2: a prospective observational study. BJOG : an International Journal of Obstetrics and Gynaecology. 2021 Apr;128(5):908-915. DOI: 10.1111/1471-0528.16597. PMID: 33187026; PMCID: PMC7753553.
9. World Health Organization. Guideline: Delayed umbilical cord clamping for improved maternal and infant health and nutrition outcomes. 2014. Available from https://apps.who.int/iris/bitstream/handle/10665/148793/9789241508209_eng.pdf [Accessed 12th August 2021]
10. Mejía Jiménez I, Salvador López R, García Rosas E, et al. Umbilical cord clamping and skin-to-skin contact in deliveries from women positive for SARS-CoV-2: a prospective observational study. BJOG : an International Journal of Obstetrics and Gynaecology. 2021 Apr;128(5):908-915. DOI: 10.1111/1471-0528.16597. PMID: 33187026; PMCID: PMC7753553.
11. TOG 2019 Maternal,fetal and neonatal outcomes associated with long term use of coriticosteroids during pregnancy AlSaad D et al
12. RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with Covid-19. N Engl J Med. 2021 Feb 25;384(8):693-704
13. RCOG. Coronavirus (COVID-19) Infection in Pregnancy. Version 13 14. WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group
Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19: A Meta-analysis. JAMA. 2020 Oct 6;324(13):1330-1341
15. Dept of Health and Wellbeing. South Australian Neonatal Medication Guidelines Protamine sulfate 50mg/5mL ampoule
Annex 23a
21
Contributors, Authors and Editors
1) Dr Voon Hian Yan
Maternal Fetal Medicine Specialist, Hospital Umum Sarawak. Kuching
2) Dr Muniswaran Ganeshan
Maternal Fetal Medicine Specialist, Hospital Tunku Azizah, Kuala Lumpur
3) Dr Gayathri Mariappa
Maternal Fetal Medicine Fellow, Hospital Tunku Azizah, Kuala Lumpur
4) Dr Nurul Wahidah bt Abdul Rashid, Obstetrician & Gynaecologist, Hospital Tunku Azizah, Kuala Lumpur
5) Dr Rahmah Rashidah Bt Hashim Hospital Tunku Azizah, Kuala Lumpur
6) Dr Ravichandran Jeganathan,
National Head of O&G Services, Maternal Fetal Medicine Specialist, Senior Consultant and Head of Department, Hospital Sultanah Aminah, Johor Bahru.
7) Dr Harris Suharjono Senior Consultant and Head of Department, Hospital Umum Sarawak, Kuching, Sarawak
Annex 23a





























