Embed Size (px)
Citation preview

New Guidelines & the Latest in Research for TPN in ICU/Surgical
Patients - practical implications
Prof. Hon. Mette M. BergerLausanne University Hospital
Switzerland

Disclosures - Mette M BergerGrants: Baxter, Fresenius Kabi
Lecturer: Baxter, BBraun, DSM, Fresenius Kabi, Nestlé, Nutricia
Advisory board: Baxter, Fresenius Kabi
Bonds ..: none
Member of ICU Guidelines working groups of ESPEN & ESICM

Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill PatientSociety of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.)McClave – Taylor et al JPEN 2016
• Assess patients on admission to the intensive care unit (ICU) for nutrition risk, and calculate both energy and protein requirements to determine goals of nutrition therapy.
• Initiate enteral nutrition (EN) within 24−48 hours following the onset of critical illness and admission to the ICU, and increase to goals over the first week of ICU stay.
• Take steps as needed to reduce risk of aspiration or improve tolerance to gastric feeding (use prokinetic agent, continuous infusion, chlorhexidine mouthwash, elevate the head of bed, and divert level of feeding in the gastrointestinal tract).
• Implement enteral feeding protocols with institution‐specific strategies to promote delivery of EN.
• Do not use gastric residual volumes as part of routine care to monitor ICU patients receiving EN.
• Start parenteral nutrition early when EN is not feasible or sufficient in high‐risk or poorly nourished patients.
Table 2. Bundle Statements


1 - ASSESSMENTGLOBAL STATUS – NRSINTESTINAL TRACT

NRS nutritional risk screeningKondrup et al ClNu 2003
Points
A. BMI kg/m2
A. % Eating
A. Weightloss 3 m
B.Severity
C.Age
Total
0 > 20 Normal >75%
<5% No disease <70
1 18.5-20 50-75 % 5-10% Hip # >702 <18.5
(<20 if >70y)25-50 % >10% Major surgery
BPN3 <25 % ICU
APACHE>10
ICU cut-off: > 5 points
« Worst A » + B +C
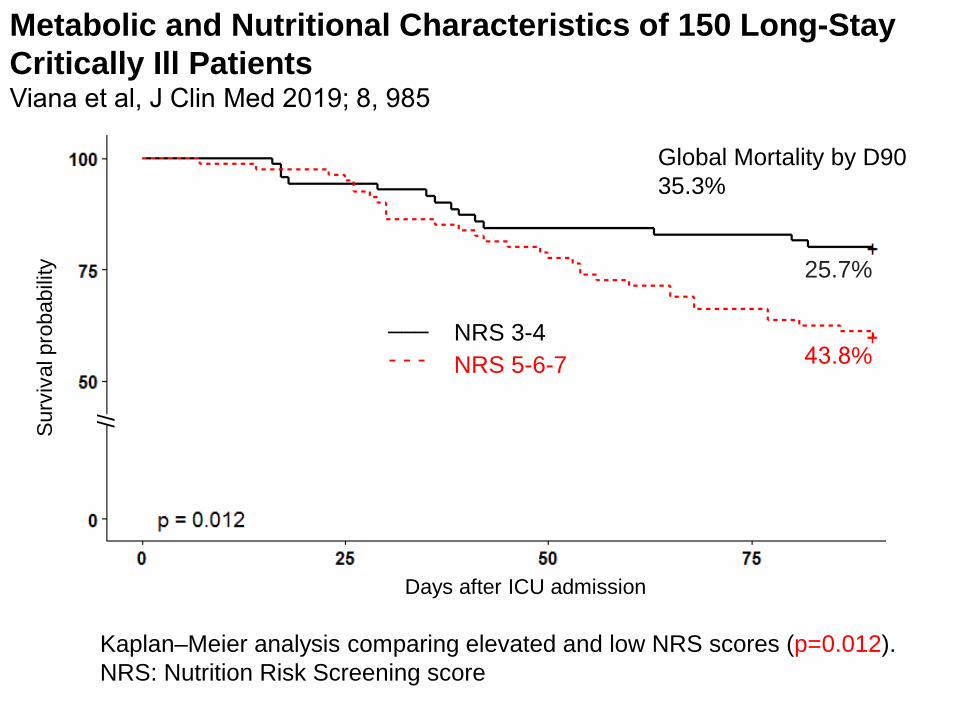
Metabolic and Nutritional Characteristics of 150 Long-StayCritically Ill PatientsViana et al, J Clin Med 2019; 8, 985
Surv
ival
pro
babi
lity
Days after ICU admission
//
NRS 3-4___
NRS 5-6-7- - -
Kaplan–Meier analysis comparing elevated and low NRS scores (p=0.012). NRS: Nutrition Risk Screening score
Global Mortality by D9035.3%
25.7%
43.8%

2 - TIMINGMETABOLIC & INTESTINAL ASPECTS

Singer et al, Clin Nutr 2019.38:48;

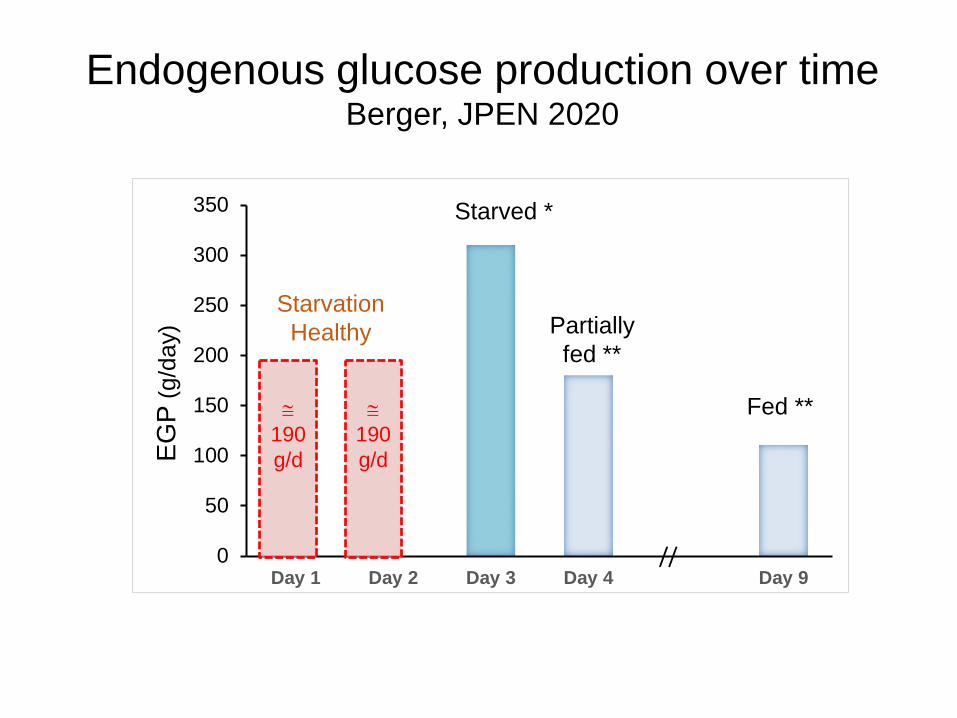
Effects of isoenergetic glucose based or lipid based PN on Glucose metabolism, DNL and respiratory gas exchanges in critically ill patientsTappy et al CCM 1998; 26:860 Substrate oxidation in critically ill patients after a 3-day starvation
Resting metabolic rate 1824 kcal/ day 116% of predicted
Glycemia 7.3 mmol/LEndogenous glucose production 310 g/ day – 3.1 mg/kg/min
1230 kcal/dayNet glucose oxidation 8% (512 kcal/ day)Net fat oxidation 46% (840 kcal /day)Net protein oxidation 26% (470 kcal/ dayNet protein balance ‐117 g/ day
N=16, age 40 yrs, 69.3 kg, predominantly trauma patients
0
50
100
150
200
250
300
350
Day 1 Day 2 Day 3 Day 4 Day 9
EGP
(g/d
ay)
Starved *
Partially fed **
Fed **
Endogenous glucose production over timeBerger, JPEN 2020
//
≅190 g/d
≅190 g/d
StarvationHealthy
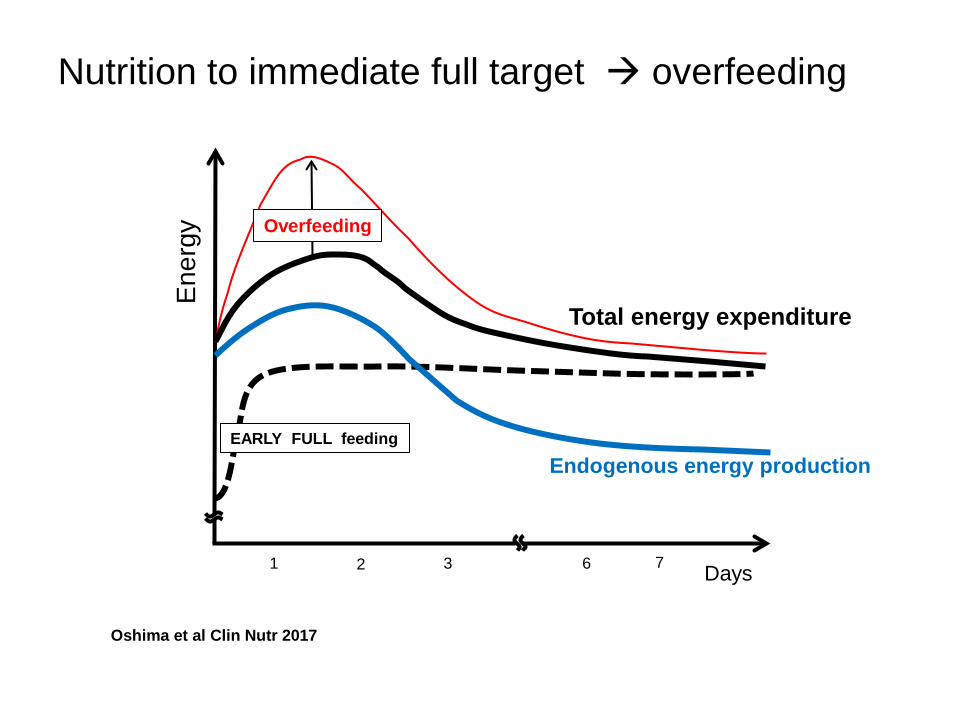
EARLY FULL feeding
Ener
gy Overfeeding
1 Days6 72 3
Oshima et al Clin Nutr 2017
Nutrition to immediate full target overfeeding
Total energy expenditure
Endogenous energy production

How to cover energy?
• Assess Energy Expenditure using indirect calorimetry or VCO2 x 8.2
• Administer about isocaloric nutrition rather than hypocaloric nutrition to be progressively implemented (70%) in the early phase of acute illness.
• To be followed by 80-100% in the stable phase• Using EEN if possible.• If not, start PN from day 3 (earlier in depleted patients)
Singer et al, ClNu 2019
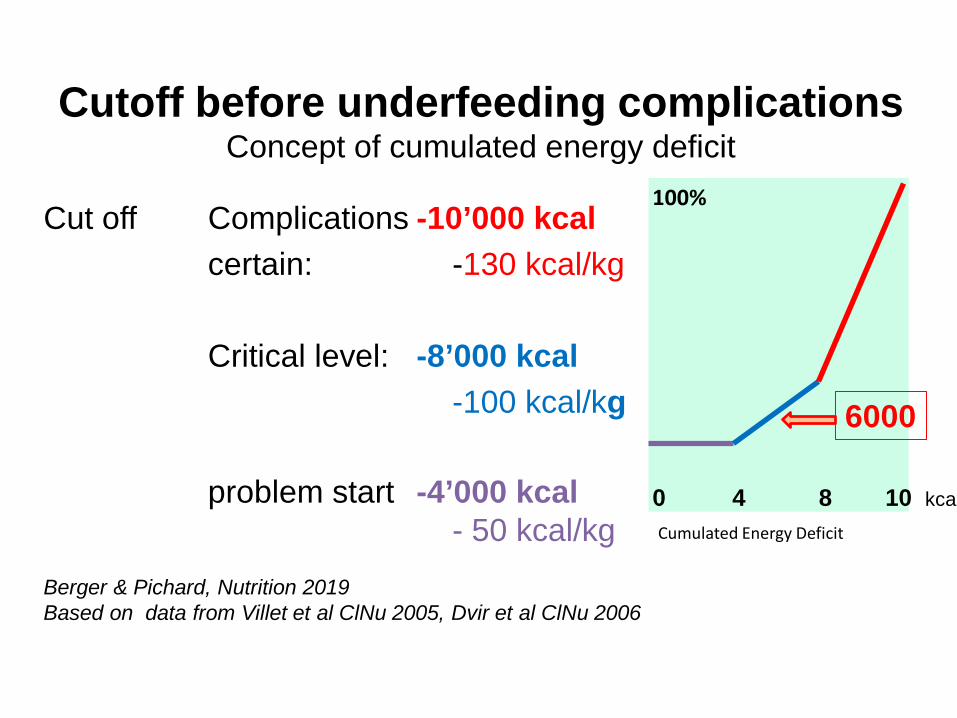
Cutoff before underfeeding complications Concept of cumulated energy deficit
Cut off Complications -10’000 kcalcertain: -130 kcal/kg
Critical level: -8’000 kcal-100 kcal/kg
problem start -4’000 kcal- 50 kcal/kg
Berger & Pichard, Nutrition 2019Based on data from Villet et al ClNu 2005, Dvir et al ClNu 2006
Cumulated Energy Deficit
0 4 8 10 kcal
100%
6000

3 - ROUTEDOES THE ROUTE MATTER?
Not as much as previously claimed more balanced PN composition

When should nutrition therapy be initiated ?Which route should be used?
Recommendation 5• If oral intake is not possible, early EN (within 48 hours) shall be performed/initiated in critically ill adult patients rather than early PN
•Grade of recommendation: A – strong consensus (100 % agreement)
Singer et al, Madrid 2018

Recommendations 1 + 21. We suggest using EEN in critically ill adult
patients (Grade 2C).1a. We suggest using EEN rather than early PN (Grade 2C).1b. We suggest using EEN rather than delaying EN (Grade 2C).
Reintam et al, Intensive Care Med (2017) 43:380–398
2. We suggest using Early EN in patients with shock receiving vasopressors or inotropes when shock is controlled with fluids and named medications (Grade 2D).Comment: EN should not be started if shock is uncontrolled and haemodynamic and tissue perfusion goals are not reached
N=24 international authors

Advantages of Enteral• Maintains mucosal structure & integrity• Maintains GI motility if early• Maintains GI immunity (IgA)• Feeds the microbiome• Limits exacerbation of inflammation• ⇓ bacterial proliferation• ⇓ Translocation (bacteria / toxins)• ⇓ line sepsis• ⇓ metabolic complications -hyperglycemia• ⇓ Feeding solutions are cheaper
But to benefit EN, you need a feeding protocol SOP …. and great nurses

GIdisordersin the ICU Stomach
Pylorus
Small bowel
Colon
Splanchnic ischemia- shock of any origin- vascular disease- Ischemia/reperfusion- cardiopulmonary bypass- compartment syndrome
↓ gastric motility & Pyloric closure :- catecholamines- mechanical ventilation-↑ intracranial pressure- sedatives, opiates
Paralytic ileus- opiates, sedatives, clonidine- excessive fluid resuscitation- retroperitoneal bleeding- severe abdominal sepsis
↓ motilityOgilvie syndrome
Diarrhea
Esop
hagu
s
Antiperistaltism

We suggest DELAYING EN
General recommendations – to delay EN• uncontrolled shock• uncontrolled hypoxemia and acidosis• uncontrolled upper GI bleeding• bowel obstruction
expert opinion = Grade 2D
15. Overt bowel ischaemia16. High-output fistula without distal feeding access18.b. Abdominal compartment syndrome21. Gastric aspirate > 500 ml/6 h
Early enteral nutrition in critically ill patients: ESICM clinical practice guidelines. Reintam et al, ICM 2017

• Recommendation 6In case of contraindications to oral and EN, PN should be implemented within 3-7 days.Grade of recommendation: B –consensus (89 % agreement)
• Recommendation 7Early and progressive PN can be provided instead of no nutrition in case of contraindications for EN in severely malnourished patients. Grade of Recommendation: 0 –strong consensus (95 % agreement)
Singer et al, Madrid 2018

Always assess/consider GI tract first
Which route?
SupplementalPN
ParenteralNutrition
ENTERALDuodenal/
Jejunal Tube

N Engl J Med. 2014 Oct 30;371(18):1673-84
Septic shock patientsN= 2410EN: greater risk of digestive severe complications
more vomiting (34 vs 20% p<0·0001)more diarrhoea (36 vs 33% p=0·009)
bowel ischaemia (2% vs <1% p=0·007), acute colonic pseudo-obstruction (1% vs <1% p=0·04)
CALORIESMechanically ventilated patientsN=2400PN: less hypoglycemia (3.7% vs.
6.2%, P = 0.006) less vomiting (8.4% vs16.2% P<0.001)

4 - COMPOSITION AMINO ACIDS LIPIDS GLUCOSE

Evolution of PNBerger, Clin Nutr 2014
1930
.//.
1960
1970
1980
1990
2000
2010
2020

0,5 1,0 1,5 2,0 2,5 3,0
ASPEN/SCCM 2009BMI < 30
BMI > 30
SFAR/SRLF BMI
> 40
American Burn Association
Protein intake according to the guidelines
ESICM1998
2001
2009
2014
g/kg/d
Healthy
ASPEN/SCMM2016
2019 ESPEN
ESPEN

Ishibashi et al, CCM 1998;26:1529-35
Change in Total Body ProteinIn trauma & sepsis
Courtesy J Wernerman
Optimal protein requirement during the first 2 weeks after the onset of critical illness.

Protein RequirementsFerrie et al, JPEN 2016
119 ICU patientsPN solutions with AA at 0.8 g/kg or 1.2 g/kgThe higher level of amino acids was associated with small improvements in a number of different measures, supporting guideline recommendations for ICU patient

Glutamine – “Conditional Deficiency”
Newsholme P., J. Nutr. 131: 2515S–2522S, 2001
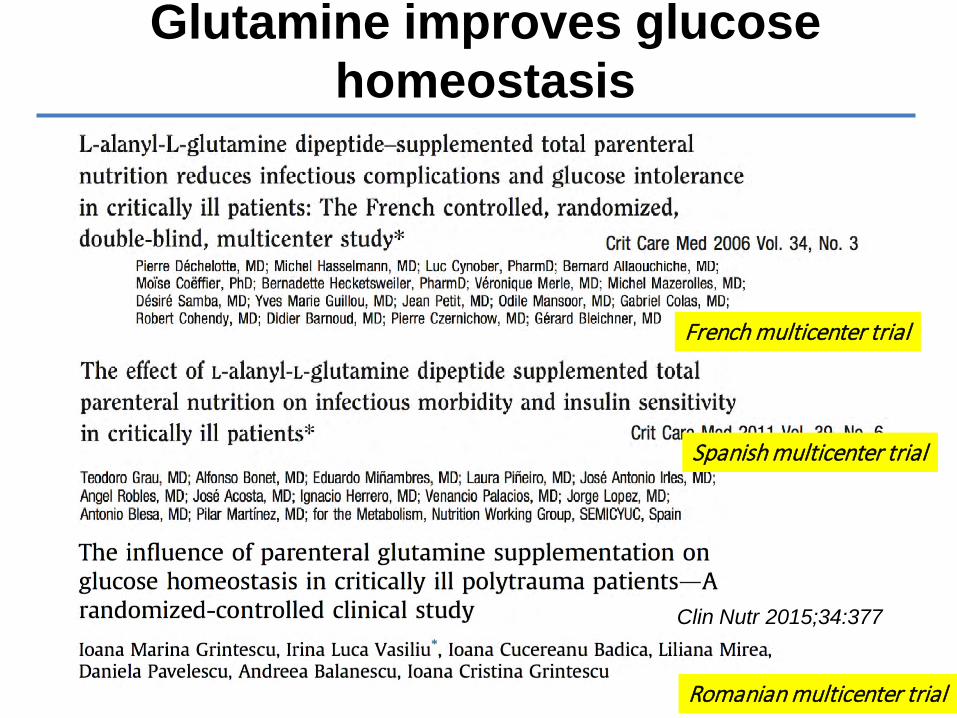
Glutamine improves glucose homeostasis
Romanian multicenter trial
Spanish multicenter trial
French multicenter trial
Clin Nutr 2015;34:377
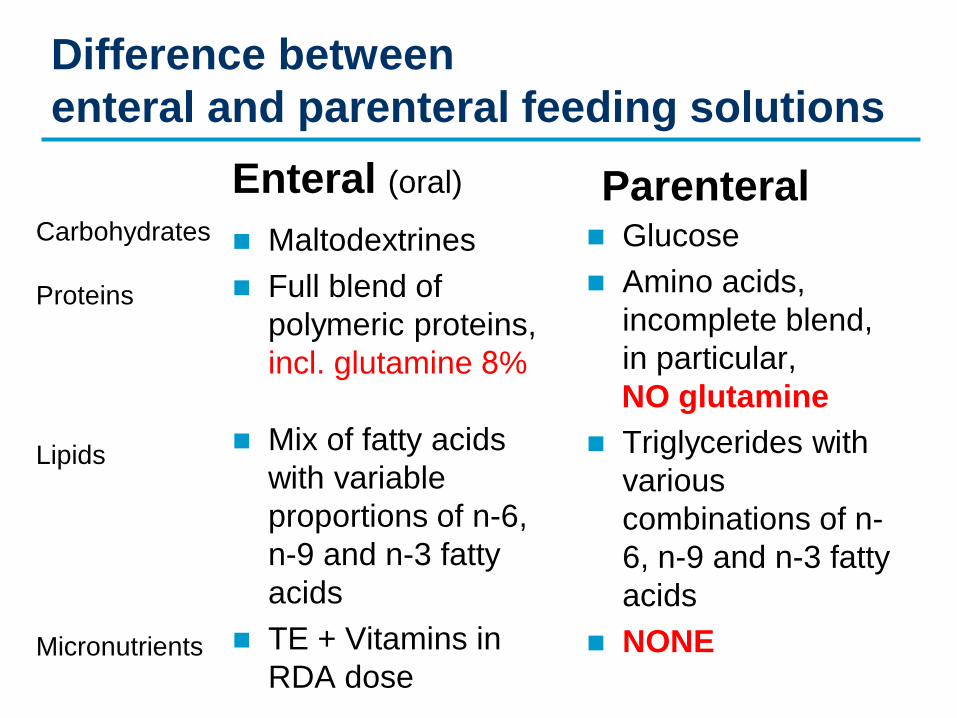
Difference between enteral and parenteral feeding solutions
Enteral (oral)
Maltodextrines Full blend of
polymeric proteins, incl. glutamine 8%
Mix of fatty acids with variable proportions of n-6, n-9 and n-3 fatty acids
TE + Vitamins in RDA dose
Parenteral Glucose Amino acids,
incomplete blend, in particular, NO glutamine
Triglycerides with various combinations of n-6, n-9 and n-3 fatty acids
NONE
Carbohydrates
Proteins
Lipids
Micronutrients

Amino acids: beware of unbalanced PN solutions
Fürst & Stehle New Horizons 1994

Stehle P et al., Clin Nutr ESPEN 17 (2017) 75-85
This meta-analysis clearly confirms that when critically ill patients are supplemented with parenteral GLN dipeptide according to clinical guidelines as part of a balanced nutrition regimen, it significantly reduces hospital mortality, infectious complication rates, and hospital LOS.
15 RCTs (16 publications) including 842 critically ill patients. None had renal and/or hepatic failure. Average study quality (Jadadscore) > predefined cut-off of 3.0 (3.8 points)
Intervention : parenteral GLN dipeptides in combination with supplemental or total PN for at least 3 days while the control treatment consisted of isoenergetic and iso-N supplements

CompositionCommercialPN

Should we use additional enteral / parenteral glutamine (GLN) in the ICU?
Recommendation 26• In patients with burns > 20% body surface area, additional
enteral doses of glutamine (0.3-0.5 g/kg/d) should be administered for 10-15 days as soon as EN is commenced.
• Grade : B – strong consensus (95 % agreement)Recommendation 28• In ICU patients except burn and trauma patients, additional
enteral glutamine should not be administered.• Grade : B – strong consensus (92.31 % agreement)Recommendation 29• In unstable and complex ICU patients, particularly in those
suffering from liver and renal failure, parenteral glutamine-dipeptide shall not be administered.
• Grade : A – strong consensus (92.31 % agreement)
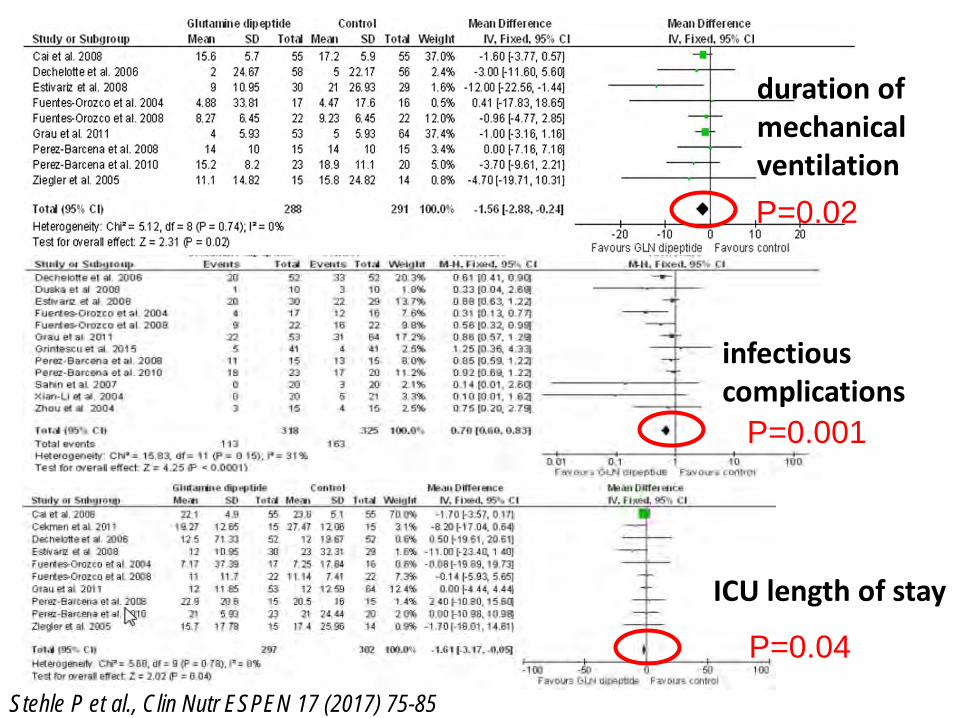
ICU length of stay
infectious complications
duration of mechanical ventilation
Stehle P et al., Clin Nutr ESPEN 17 (2017) 75-85
P=0.02
P=0.001
P=0.04

Length of stay in hospital
Hospital mortality
P=0.01
P=0.03
Stehle P et al., Clin Nutr ESPEN 17 (2017) 75-85

Essential Fatty Acid Requirements and Intravenous Lipid EmulsionsGramlich et al JPEN 2019
Fatty acid structures and biosynthetic pathways

Essential Fatty Acid Deficiency in Human Adults During PN
Hamilton et al NCP 2006
pivotal paper in 19753 case studies of patients receiving prolonged fat-
free PN at home skin lesions + abnormal plasma fatty acid profiles
The skin lesions and biochemical evidence of essential fatty acid deficiency (EFAD) resolved when Intralipid was administered. Until this time, EFAD was documented only in animals and infants but not in adults.

Essential fatty acid deficiency
Courtesy Stanley Dudrick & Stanislaw Klek

Essential Fatty Acid Requirements and Intravenous Lipid Emulsions
Gramlich et al JPEN 2019
Linoleic acid (LA) and α-linolenic acid (ALA) must be supplied to the human body and are therefore considered essential fatty acids. This narrative review discusses the signs, symptoms, diagnosis, prevention, and treatment of essential fatty acid deficiency (EFAD).
Although rare, EFAD is diagnosed by an elevated triene:tetraene (T:T) ratio, which reflects increased metabolism of oleic acid to Mead acid in the absence of adequate LA and ALA

Fats - any side-effects?• Altered pulmonary hemodynamics (PHT) and
oxygenation• Hepatobiliary disorders associated with PN -
PNALD: steatosis, cholestasis, gallbladder sludge/stones …
• Fat Overload Syndrome in infants (> 3 g/kg/d)• Hypertriglyceridemia & pancreatitis• Decreased insulin sensitivity• Administration of IV fat resistance to
anticoagulation in patients on anti-vit K (warfarin)• Immune effects & risk of infection• Microbial growth in IV fat emulsions

Biological and Clinical Aspects of an Olive Oil-Based Lipid Emulsion-A Review
Cai, Calder et al, Nutrients 2018; 10: 776
Olive oil-based ILE appears to support the innate immune system, is associated withfewer infections, induces less lipid peroxidation, and is not associated with increased hepatobiliary or lipid disturbances. These data would suggest that olive oil-based ILE is a valuable option in various PN-requiring patient populations.
Infection rates in adult surgical patients (N = 458)Jia et al Nutr. J. 2015, 14, 119
Adhesion of LPS-induced leukocytes in a rat model. Demirer et al 2016

Infla
mm
atio
n
Hyper
Hypo
HYPERINFLAMMATION
Excess inflammatory eicosanoids,
cytokines, ROS, adhesion molecules;
NFkB activation
IMMUNOSUPPRESSIONExcess anti-inflammatory Cytokines;Suppressed HLA expression & antigen presentation;Suppressed T cell function
INSULT
POOROUTCOME
ω-3 PUFAs

0
1 2 3 4 5 6
SIRSCARS
eico
sano
ids
HLA
-DR
TNF,
IL-1
, 6 e
tc.
phys
iolo
gic
rang
e of
infla
mm
atio
nov
erw
helm
ing
infla
mm
atio
nim
mun
e-pa
raly
sis
IL-4, 10, 13, etc.
self destructiontissue injury
breakdownof host defense
shock
ω-6 fatty acids
ω-3 PUFAs

Influence of n-3 PUFAs enriched lipid emulsions on nosocomial infections and clinical outcome in critically ill patients: ICU lipids studyGrau-Carmona et al, CCM 2015; 43: 31.
Time free of infection for patients givenparenteral nutrition with different lipid emulsions
Inlcusion: 159 medical and surgical ICU patientsMain results: The number of patients with nosocomial infections was significantly reduced in the fish oil-receiving group (21.0% vs 37.2%, p = 0.035) and the predicted time free of infection was prolonged (21 ± 2 vs 16 ± 2 d, p = 0.03). No significant differences were detected for ICU, hospital, and 6-month mortality.

Should we use enteral / parenteral EPA/DHA? Recommendation 30• High doses of omega-3-enriched EN formula
should not be given by bolus administration. • Grade : B – strong consensus (91 % agreement)Recommendation 31• EN enriched with omega-3 fatty acids within
nutritional doses can (should) be administered. • Grade : 0 – strong consensus (95 % agreement)Recommendation 32• High dose omega-3-enriched enteral formulas
should not be given on a routine basis. • Grade : B – consensus (90 % agreement)
Singer et al, Clin Nutr 2019;38:48-79
ICU2019

Choosing the lipid: A key consideration in PNIndustry proposes AIO with different levels of SFAs, PUFAs, and MUFAs
Wanten GJA, Calder PC. Am J Clin Nutr. 2007;85(5):1171-1184. Driscoll DF. Nutr Clin Pract. 2006;21(4):381-386.
Intralipid®
20%
Lipofundin®
MCT/LCT 20%
Structolipid®
20%
Omegaven®
10%
ClinOleic®
20%
Lipoplus®
20%
SMOFlipid®
20%Oil source
% FA
100% soy 50% coconut 50% soy
36% coconut 64% soy
100% fish 80% olive 20% soy
50% coconut40% soy10% fish
30% soy30% coconut
25% olive15% fish
SFA 15.0 59.4 46.3 21.2 14.5 49.0 36.9
MUFA 24.0 11.0 14.0 24.3 63.7 14.1 32.7
PUFA 61.1 33.8 40.0 42.3 22.0 36.9 30.3
ω-3 8.0 4.5 5.0 35.2 2.8 10.5 8.3ω-6 53.1 29.3 35.0 7.1 19.2 26.5 22.0ω-9 24.0 11.0 14.0 15.1 62.3 13.9 31.2

Intravenous Fish Oil in Critically Ill and Surgical Patients - Historical Remarks and Critical Appraisal
Kreymann et al, Clin Nutr 2018;37:1075
Effect of different fish oil admixtures or fish oil-supplemented emulsions on infection rates in critically ill patients

Effect of different fish oil admixtures or fish oil-supplemented emulsions on infection rates in surgical patients with malignancies
Intravenous Fish Oil in Critically Ill and Surgical Patients - Historical Remarks and Critical Appraisal
Kreymann et al, Clin Nutr 2018, 37(3):1075

ω-3 Fatty-Acid Enriched PN in Hospitalized Patients: Systematic Review With Meta-Analysis & Trial Sequential Analysis
Pradelli et al JPEN 2019
Provision of ω-3-enriched lipid emulsions should be preferred over standard lipid emulsions in patients with an indication for PN.
Publications after duplicates removed (n = 2992) Included in meta-analyses (n = 49)
Fig. 2. Infection ratesN= 2154Z = 5.26 P < 0.00001

ω-3 Fatty-Acid Enriched PN in Hospitalized Patients: Systematic Review With Meta-Analysis & Trial Sequential Analysis
Pradelli et al JPEN 2019
Fig.3. 30-day mortality Z = 1.44P = 0.15
Fig.4. LICUZ = 2.49 P = 0.01

Fig.5. LOSN= 2182Z = 5.35 P < 0.00001
ω-3 Fatty-Acid Enriched PN in Hospitalized Patients: Systematic Review With Meta-Analysis & Trial Sequential Analysis
Pradelli et al JPEN 2019
Fig.6. SepsisN=1141Z = 3.52P = 0.0004
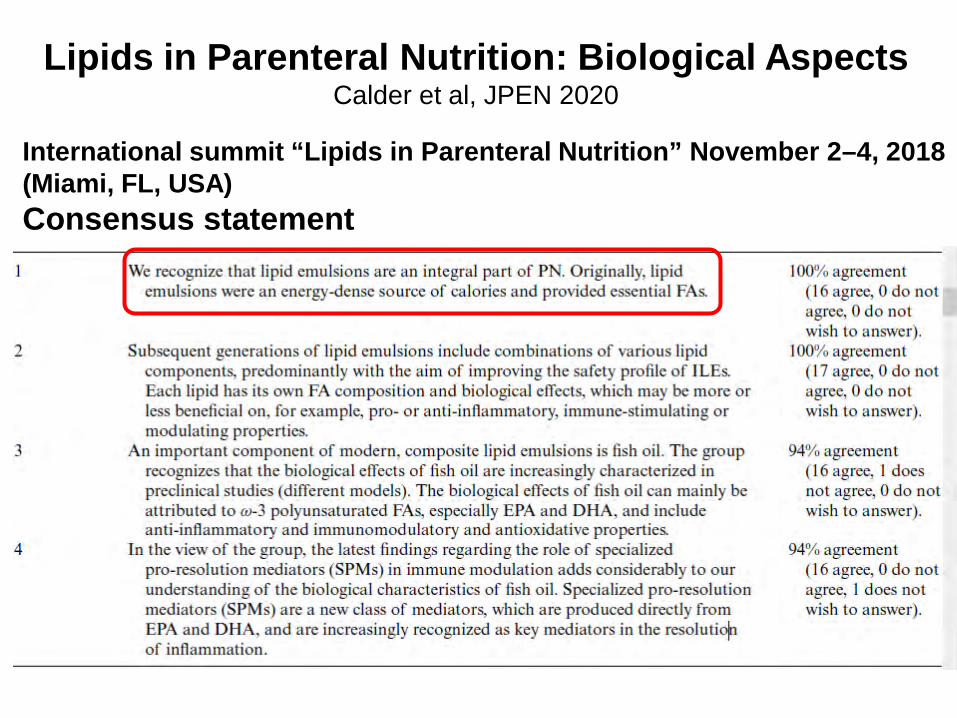
Lipids in Parenteral Nutrition: Biological AspectsCalder et al, JPEN 2020
International summit “Lipids in Parenteral Nutrition” November 2–4, 2018 (Miami, FL, USA)Consensus statement

Summary of the Anti-Inflammatory Actions Attributed To Marine ω-3 PUFA
EPA and DHA are direct precursors of potent Specialized pro-resolving lipidmediators (SPMs): resolvins, protectins, and maresins
Lipids in Parenteral Nutrition: Biological AspectsCalder et al, JPEN 2020

TOTAL energy expenditure
Σ Endogenous production + exogenous supply
Endogenous production
1
Progressiveearly EN
Days72 3
Supplemental PN ?
Time (hrs) 24 48 72
Ener
gy
Indirect calorimetry
Proposed Feeding strategy in the ICU
Adapted from Oshima et al, Clin Nutr 2017;36:651
High+ protein High E + protein
43% of patients stay
> 72 hrs in SMIA
Goals 1st week: 20 kcal/kg + protein 1.2-1.3 g/kg

SPN - Combined EN +PN strategyHeidegger et al, Lancet 2013; 381: 385
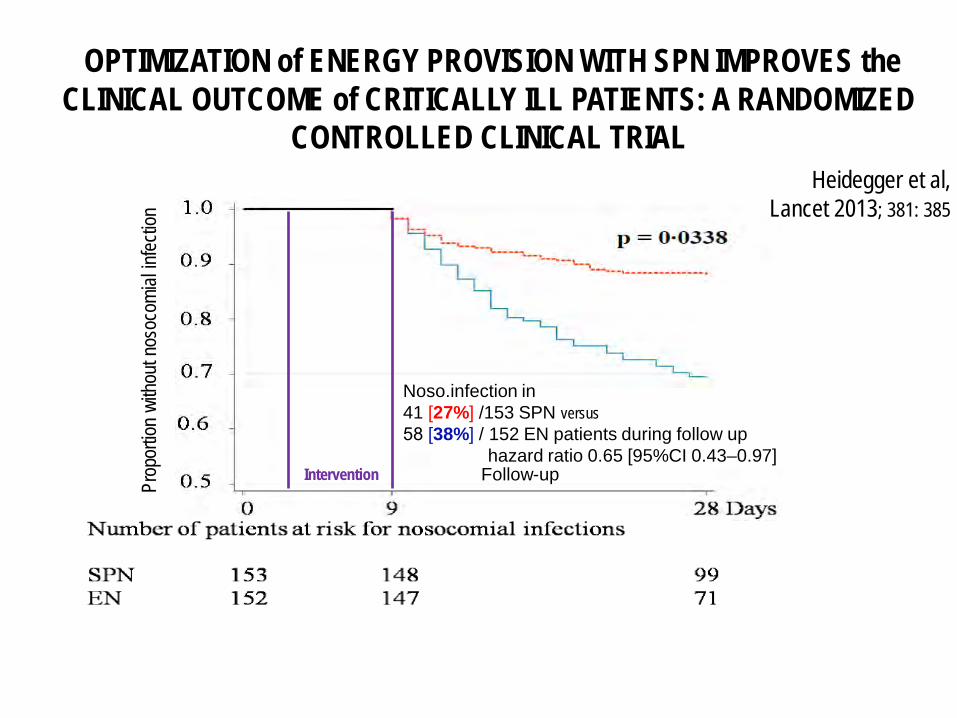
OPTIMIZATION of ENERGY PROVISION WITH SPN IMPROVES the CLINICAL OUTCOME of CRITICALLY ILL PATIENTS: A RANDOMIZED
CONTROLLED CLINICAL TRIAL Heidegger et al,
Lancet 2013; 381: 385
Noso.infection in 41 [27%] /153 SPN versus58 [38%] / 152 EN patients during follow up
hazard ratio 0.65 [95%CI 0.43–0.97]Intervention Follow-upPr
opor
tion
witho
ut no
soco
mial
infec
tion

pg/m
L
E N S P N -D 1 00
5
1 0
1 5
2 0
P H A , d o s e 1 :1 , P o s t /P r e r e s p o n s e s , E N /S P N
nb o
f sub
ject
s
R
N R
Fisher's exact test 0.2138
r a t io p o s t /p re > 1 .2
TNF-α
(pg/m
L)
D 4 D 1 0 D 4 D 1 01 0
1 0 0
1 0 0 0
1 0 0 0 0
0.0923 0.0186
E N S P N
B
Supplemental Parenteral Nutrition 2Berger et al – Clin Nutr 2019

Supplemental parenteral nutrition in intensive care patients: A cost saving strategyPradelli et al Clin Nutr 2017
Tornado diagram depicting the results of the one-way deterministic sensitivity analysis
Swiss SPN Study (N = 305; ClinicalTrials.gov: NCT00802503 // Lancet 2013
The risk of nosocomial infection was by 10% for each 1000 kcal in cumulative energy deficit

Guidelines & Research in TPN Conclusions
• While enteral nutrition should remain the first option, ICU patients do no always tolerate it
• Malnutrition may result from prolonged failed EN attempts
• Parenteral nutrition is lifesaving• Main indication is GI failure, followed by low EN • The recent better balanced PN solutions
particularly regarding lipid emulsions improve outcome
• PN solutions still incomplete as to amino acids. • Modulation of inflammation, and ↓ infection is a
very important result of the addition of w-3 PUFA

Thank you!http://lavieestleplusgranddesguru.over-blog.com/2015/10/les-pensees-un-banc-de-poissons.html





























