Embed Size (px)
Citation preview
Guslihan Dasa TjiptaGuslihan Dasa TjiptaDivision of Perinatology
Department of Child Health Medical SchoolUniversity of Sumatera Utara
1
y

Predisposing FactorsPredisposing FactorsMaternal factors:
Primigra idaPrimigravida Cephalopelvic disproportion,
small maternal stature maternal pelvic anomalies
Prolonged or rapid labor DystociaDystocia Oligohydramnios
2

Predisposing factorsPredisposing factorsF t l f tFetal factors:
Abnormal presentation Breech, face
VLBW or extreme prematurity p yFetal macrosomia Large fetal headLarge fetal head Fetal anomalies
3

Predisposing FactorsPredisposing Factors
Ob t t i l I t tiObstetrical Interventions:Use of mid-cavity forceps or vacuum extraction Versions and extractions
4

Types of InjuryTypes of Injury
Soft tissue injuriesHead and Skull Face Musculoskeletal injuriesMusculoskeletal injuries Intra-abdominal injuries Peripheral nerve injuries
5

Soft Tissue InjuriesSoft Tissue Injuries
E th & Ab iErythema & Abrasions- Forceps, Dystocia
Petechiae-head/neck/chest/back- Cord around neck /breech- thrombocytopeniay p
Ecchymosesbreech/prematurity
6
-breech/prematurity

7

Soft Tissue InjuriesSoft Tissue InjuriesLacerations
l b tt k thi hscalp, buttocks, thighs(Fetal scalp electrodes, surgeons knife!)Infection a risk, but most heal uneventfullyManagement:
careful cleaning, application of antibiotic ointment and observationointment, and observation Bring edges together using Steri-Strips Lacerations occasionally require suturing
8
y q g
Soft Tissue InjuriesSoft Tissue InjuriesSubcutaneous fat Necrosis (SFN)
N t ll d t t d t bi thNot usually detected at birthIrregular, hard, non-pitting, subcutaneous plaques with overlying dusky red-purple p q y g y p pdiscoloration on the extremities, face, trunk, or buttocks May be caused by pressure during deliveryMay be caused by pressure during deliveryHypothermia/ischemia/asphyxiaappear @ 6-10 dayspp @ yresolve @ 6-8 wk/atrophySometimes calcifies
9

10

Soft Tissue InjuriesSoft Tissue Injuries
SFN: TreatmentSFN: TreatmentTreat symptomatic hypercalcemia
i laggressivelyincreased fluid intakelow calcium/ vit. D dietfurosemide -calcium-wasting diureticSteroids-inhibit metabolism of vit. DBiphosphonates-reduce bone resorption
11
Injuries to the HeadjCaput Succedaneum
most frequently observed lesionmost frequently observed lesionpressure on the scalp against cervixsubcutaneous extraperiosteal accumulation ofsubcutaneous, extraperiosteal accumulation of blood/serumpresenting part involvedpresenting part involvedoverlying bruising/Petechiaecrosses suture linescrosses suture linesresolves within days
12

Injuries to the HeadInjuries to the HeadCephalhematomap
0.4%-2.5% of all live birthssub-periosteal hemorrhage from rupture of blood p g pvessels between the skull and the periosteumbuffeting of fetal head against the pelvisg g pno extension across suture linesmost commonly parietal, may occasionally be y p , y yobserved over the occipital bone
13

Injuries to the HeadInjuries to the Head
CephalhematomaCephalhematomaincreases in size with time 15% bilateral18% associated skull fractureForcepsVacuumVacuum
14

Injuries to the Headj
Subgaleal HemorrhageSubgaleal HemorrhageDiagnosis is generally clinical:
fluctuant boggy mass developing over the scalp ggy p g p(especially over the occiput) develops gradually 12-72 hours after deliveryhematoma spreads across the whole calvarium Usually insidious and may not be recognized for hhoursswelling may obscure the fontanelle and cross suture lines (distinguishing it from
15
suture lines (distinguishing it from cephalhematoma)

Injuries to the HeadInjuries to the Head
Subgaleal HemorrhageSubgaleal HemorrhageRx if signs of substantial volume loss:
compression wrap restore blood volumerestore blood volumesurgical drainage25% mortality25% mortality
16

17

Caput Succedaneum
Cephalhematoma
Subgaleal hemorrhage with skull fractureSubgaleal hemorrhage with skull fracture
18

SkinEpicranial aponeuroses
Caput CephalhematomaSubgaleal hemorrhageaponeuroses
Periosteumextradural hemorrhage
Skull
DDura
Lesion External swelling ↑ after birth
Crosses suture lines
↑↑↑acute blood losslines loss
Caput succedaneum Soft, pitting No Yes NoCephalhematoma Firm tense Yes No No
19
Cephalhematoma Firm, tense Yes No No
Subgaleal hematoma Firm, fluctuant Yes Yes Yes

Injuries to the HeadInjuries to the Head
Skull FracturesSkull FracturesUncommon because of compressible skull & opensuturesForceps/Prolonged laborLinear/DepressedUsually asymptomaticAssociated intracranial hemorrhage may produce
symptoms
20

21
Injuries to the HeadInjuries to the HeadSkull FracturesRx – conservative
- elevation of depressed fractureelevation of depressed fracture- Thumb pressure- Hand pumpHand pump- Vacuum extractor
Surgical elevationSurgical elevationHealing within a few months
22

Injuries to the HeadInjuries to the HeadIntracranial hemorrhage
- Subdural/Subarachnoid/IVH- Subdural/Subarachnoid/IVH- Usually asymptomatic
F /V- Forceps/Vacuum- Prolonged labor
U ll i t d ith f t- Usually associated with fracture
23

Injuries to the HeadInjuries to the Head
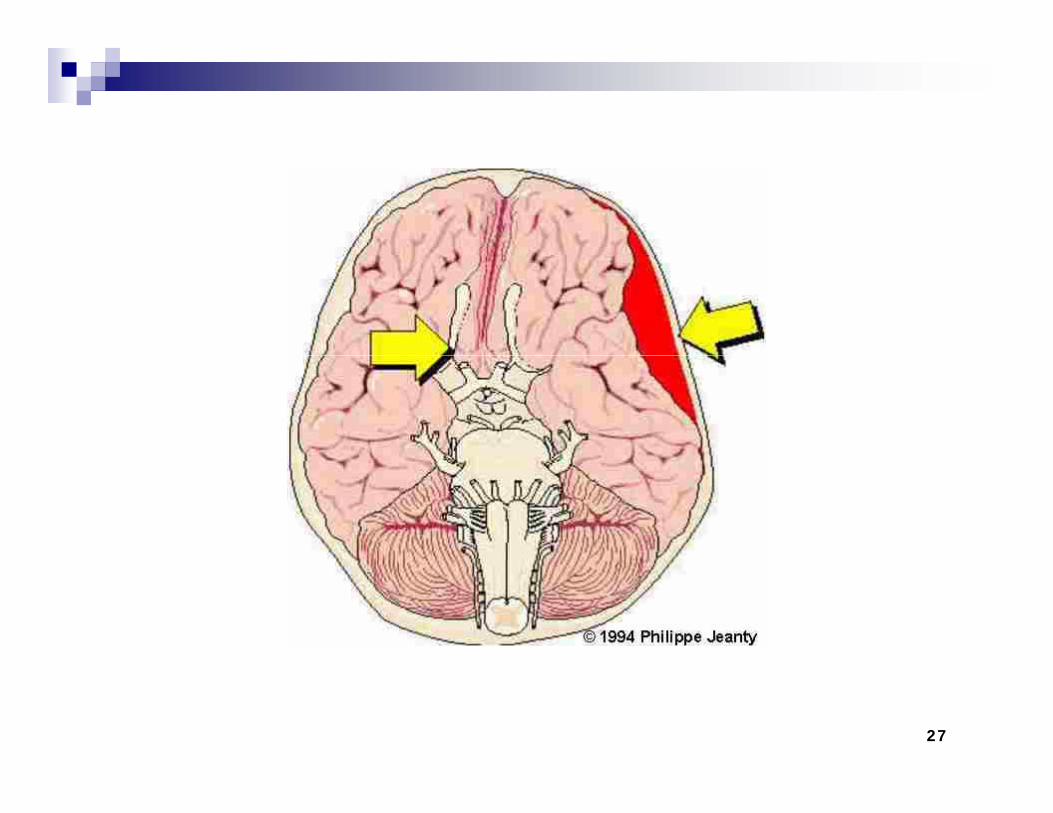
Subarachnoid hemorrhagef t th li d-more frequent than realized
-usually asymptomatic-may cause seizures (day 2-3)-bloody CSF- CT/MRI
24

25

Injuries to the Head
Subdural Hematoma- may be silent for several daysmay be silent for several days-↑head circumference- poor feeding /vomiting /lethargypoo eed g / o t g / et a gy- altered consciousness/seizures - DX- CT/MRI- RX- Subdural taps/surgical drainage
26
27

Injuries to the HeadInjuries to the Head
Fractures of Facial bonesFractures of Facial bones-nasal fracture/dislocation-deviated nasal septum-maxillary fracture-mandibular fracture
28

EYE INJURIESEYE INJURIES
Eye Lidsedema/ecchymoses/lacerationSubconjuntival hemorrhageOrbital fracture/hemorrhageE t O l M l i jExtra Ocular Muscle injuryCorneal AbrasionIntra Ocular hemorrhageIntra Ocular hemorrhage
29

Injuries to the Ear
EcchymosesAbrasionAvulsionHematoma
30
Neck and Shoulder injuriesjFractured Clavicle
-most frequently fractured bone-difficult delivery-shoulder dystocia-breech -Crepitus or deformity at the site-↓movement/moro on affected side-↓movement/moro on affected side-associated brachial plexus palsy
31

Neck and Shoulder injuriesNeck and Shoulder injuriesFractured ClavicleDX- X-rayDX- X-rayRX- conservative
immobilizationreduce painreduce painpain subsides in 7-10 days
good prognosis
32

N k d Sh ld i j iNeck and Shoulder injuries
Fracture of the Humerussecond most common fracturedifficult delivery/tractiondifficult delivery/tractionshoulder dystociabreech
deformity
33

Neck and Shoulder injuries
Fractured Humerus: ManagementFractured Humerus: Management Splinting/immobilization in adductionClosed reduction and casting when displacedClosed reduction and casting when displacedWatch for evidence of radial nerve injuryC ll f ti d l tCallus formation occurs, and complete recovery expected in 2-4 weeksIn 8 10 days the callus formation is sufficientIn 8-10 days, the callus formation is sufficient to discontinue immobilization
34

Intra abdominal Organ InjuryIntra-abdominal Organ Injury
UncommonUncommonsometimes overlooked as a cause of death in the newbornthe newbornHemorrhage is the most serious acute complicationcomplicationliver is the most commonly damaged internal organg
35

Nerve PalsiesFacial NerveEtiology
Compression Of peripheral nerve-forceps-prolonged labor-in-utero compressionCNS Injury-temporal bone fracture-tissue destruction
36
Nerve PalsiesNerve Palsies
Facial NerveFacial NerveClinical Manifestation
Paralysis apparent day 1-2Unilateral/bilateralAffected side smooth/droopingAmplified by crying
37

Nerve PalsiesNerve PalsiesFacial Nerve: central nerve injury
t i f i ith iasymmetric facies with cryingmouth is drawn towards the normal sidewrinkles are deeper on the normal sidewrinkles are deeper on the normal sidemovement of the forehead and eyelid is unaffectedthe paralyzed side is smooth with a swollen appearanceabsent nasolabial fold on affected sideabsent nasolabial fold on affected sidecorner of the mouth droops on affected sideno evidence of trauma is present on the face
38
p

Nerve PalsiesNerve Palsies
F i l NFacial Nerve: peripheral nerve injuryasymmetric facies with cryingUnable to close eye on affected sidemay be evidence of forceps markmay be evidence of forceps mark
39

40

Nerve PalsiesNerve PalsiesFacial Nerve Palsy: prognosisFacial Nerve Palsy: prognosis
85% recover in 1 week90% recovery in 1 year90% recovery in 1 yearSurgery if no resolution in 1 yrPalsy due to trauma usually resolves orPalsy due to trauma usually resolves or improvespalsy that persists is often due to absence of thepalsy that persists is often due to absence of the nerve
41

Nerve PalsiesNerve Palsies
B hi l Pl i jBrachial Plexus injuryTypes of InjuryTypes of Injury
StretchRuptureRuptureAvulsion
42

Nerve PalsiesNerve Palsies
Brachial Plexus injuryT f I jTypes of Injury
Stretch- 90-100% recovery in 1 yearRupture-needs surgical repairAvulsion-needs surgical repairg
43
Nerve Palsies
Brachial Plexus injuryBrachial Plexus injuryWeakness or total paralysis of muscles innervated by the brachial plexus C-5 to C-8innervated by the brachial plexus C 5 to C 8 and T1Erb's Palsy C5-C7- proximal muscle weaknessy pKlumpke’s Palsy C8 and T1- weakness in the intrinsic muscles of the hand
44

45
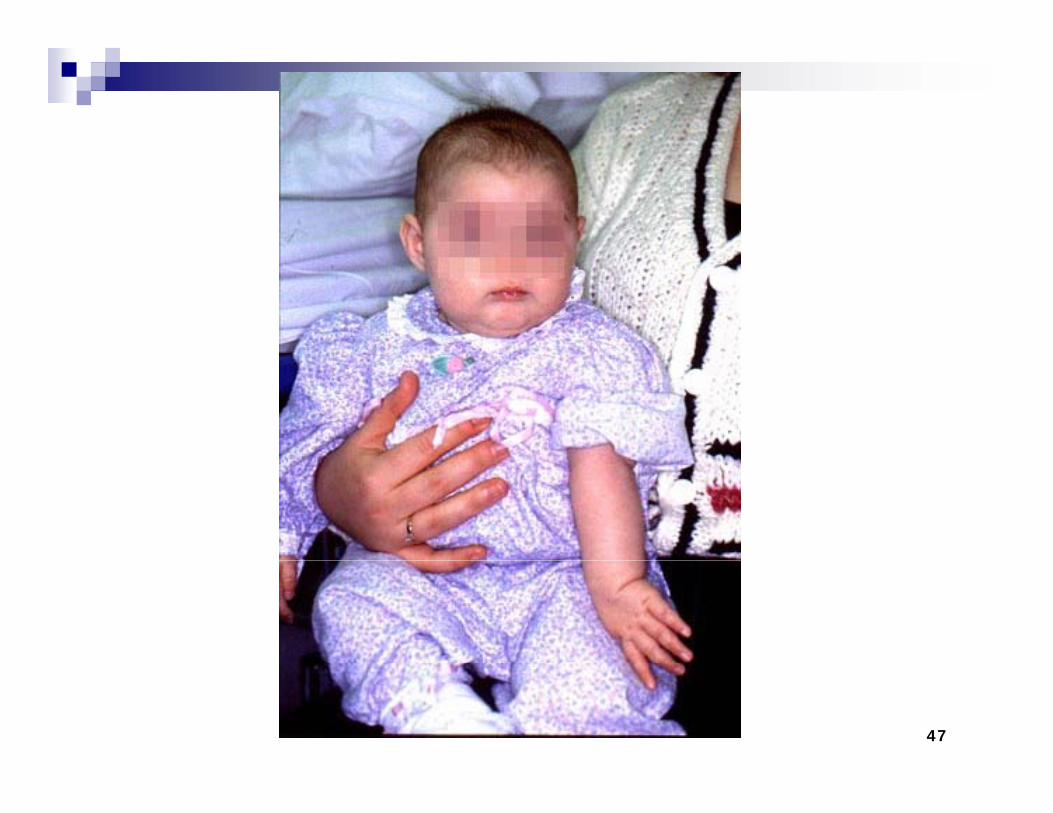
Nerve PalsiesBrachial Plexus injuryNeurological FeaturesNeurological FeaturesErb's Palsy (C5-C6)The involved extremity lies:
in adductionin pronation and internally rotated M bi d di l fl b tMoro, biceps and radial reflexes are absent Grasp reflex is usually present2-5% ipsilateral phrenic nerve paresis2 5% ipsilateral phrenic nerve paresisThe "waiter's tip" posture
46
47

Nerve PalsiesNerve PalsiesBrachial Plexus InjuryNeurological FeaturesKlumpke’s Palsy (C7-8 T1)Klumpke s Palsy (C7-8, T1)
weakness of the intrinsic muscles of the handhandgrasp reflex is absent
48
Nerve PalsiesNerve PalsiesBrachial Plexus InjuryNeurological FeaturesTotal Plexus PalsyTotal Plexus Palsy
Erb's Palsy + absent grasp reflex S l th E b'Sensory loss worse than Erb's
49
Nerve PalsiesNerve Palsies
Brachial PlexusBrachial PlexusPrognosisg
Depends on severity and extent of lesionlesion88% resolved by 4 months92% b 12 th92% by 12 months 93% by 48 months
50

Nerve PalsiesNerve Palsies
Brachial PlexusBrachial PlexusPrognosisg
Depends on severity and extent of lesionlesion88% resolved by 4 months92% b 12 th92% by 12 months 93% by 48 months
51

Nerve PalsiesNerve PalsiesBrachial PlexusManagement
Prevention of contracturesPrevention of contracturesimmobilize limb gently across the abdomen for first week and thenabdomen for first week and then start passive range of motion exercises at all jointsall joints supportive wrist splints
52
Nerve PalsiesNerve Palsies
Brachial PlexusBrachial PlexusManagement g
Electrotherapy-controversial Surgical exploration if no significantSurgical exploration-if no significant functional recovery by 3 monthsE l ti ft 6 th i f littlExploration after 6 months is of little benefit
53
Nerve PalsiesLaryngeal nerve injury
The infant presents with a hoarse cry orThe infant presents with a hoarse cry or respiratory stridor most often unilateral nerve paralysisSwallowing may be affected if the superior branch is involved Bilateral paralysis may be caused by trauma toBilateral paralysis may be caused by trauma to both laryngeal nerves or, more commonly, by a CNS injury such as hypoxia or hemorrhage involving the brain steminvolving the brain stemPatients with bilateral paralysis often present with severe respiratory distress or asphyxia
54

Nerve PalsiesLaryngeal nerve injury& Prognosis:& Prognosis:
Paralysis often resolves in 4-6 wk, although full recovery may take 6-12 monthsrecovery may take 6 12 months
TreatmentsymptomaticsymptomaticSmall frequent feeds, once infant is stable Minimize the risk of aspirationMinimize the risk of aspirationInfants with bilateral involvement may require gavage feeding and tracheotomy
55
gavage feeding and tracheotomy
56