Embed Size (px)
Citation preview
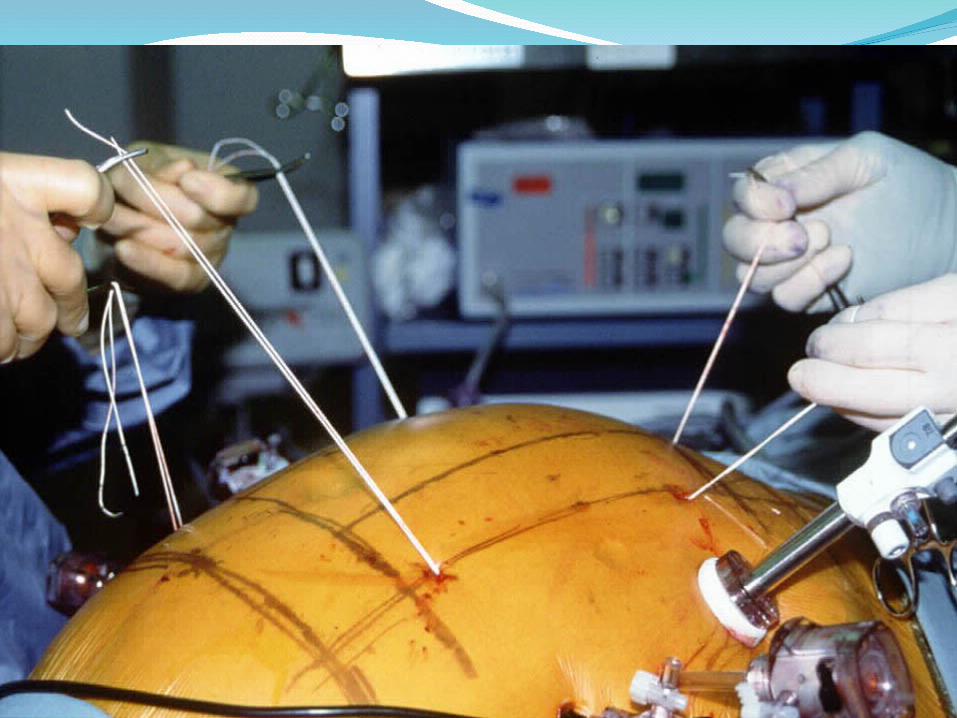
Guy Voeller, MD, FACSProfessor of Surgery, University of TennesseePast President, The American Hernia Society



SUTURE FIXATION• Van’t Riet 2002• Pig model using PPM• Used sutures vs tacks (1-5/7cm mesh)• Tensile strength
67N vs 28N for single fixation(p<0.001)
115N vs 42N for double(p<0.001) 150N vs 82N for 5 fixation points(p<0.05)
SUTURE FIXATION• Increasing fixation > 3 per 7cm did not
improve TS (every 1.8cm)• The TS is up to 2.5 times greater when
sutures are used instead of tacks• Sutures are preferable for LVH repair
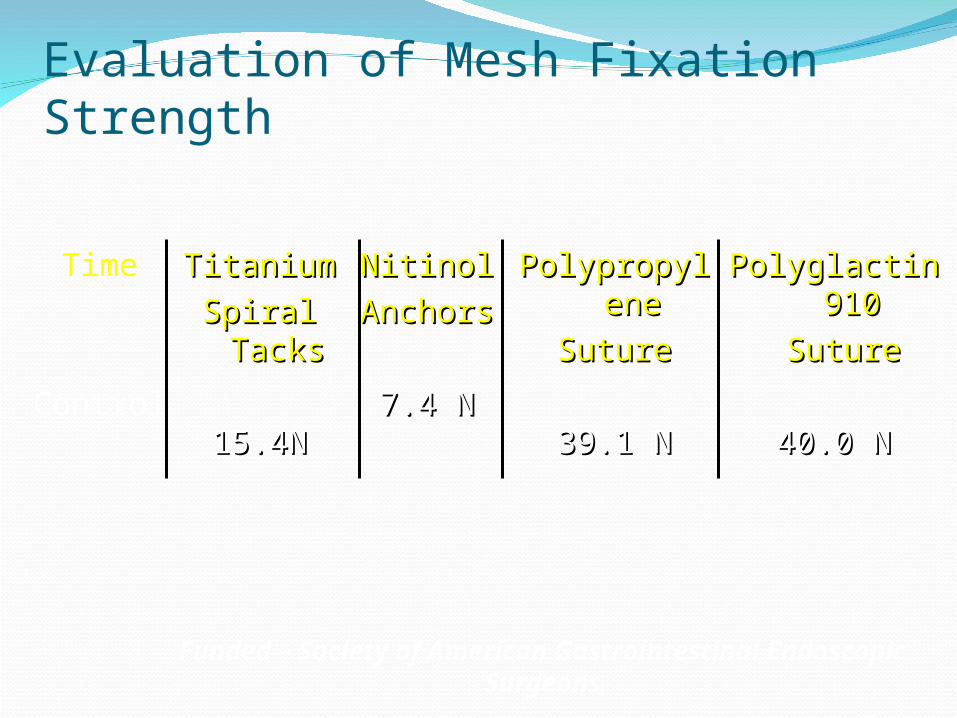
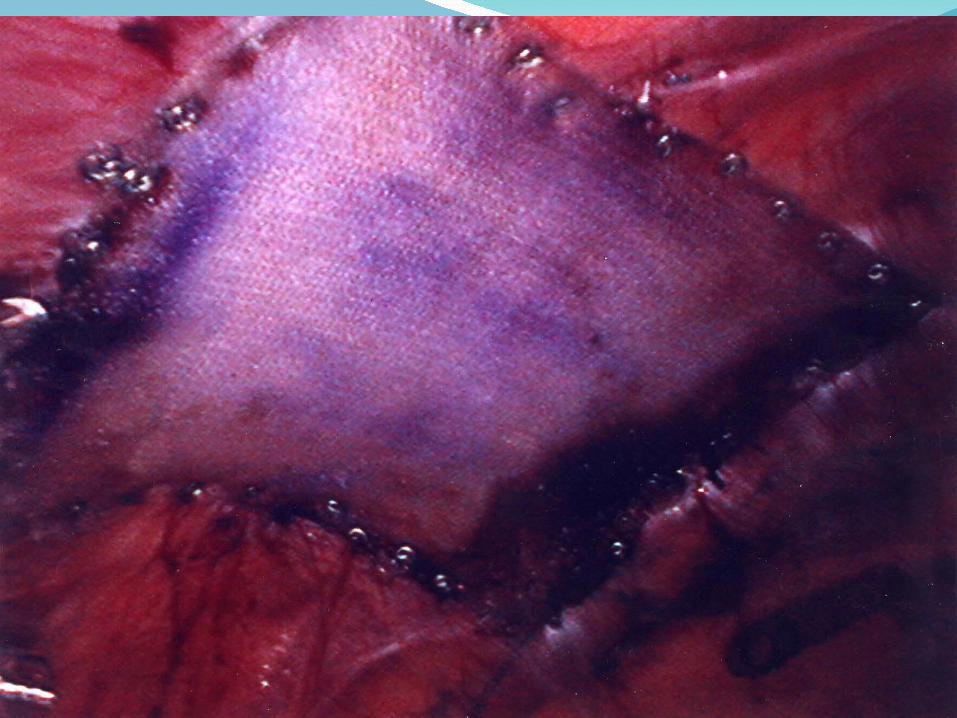
Evaluation of Mesh Fixation Strength
Time
Control
TitaniumTitanium
Spiral TacksSpiral Tacks
15.4N15.4N
NitinolNitinol
AnchorsAnchors
7.4 N7.4 N
PolypropylePolypropylenene
SutureSuture
39.1 N39.1 N
Polyglactin Polyglactin 910910
SutureSuture
40.0 N40.0 N
Funded – Society of American Gastrointestinal Endoscopic Surgeons
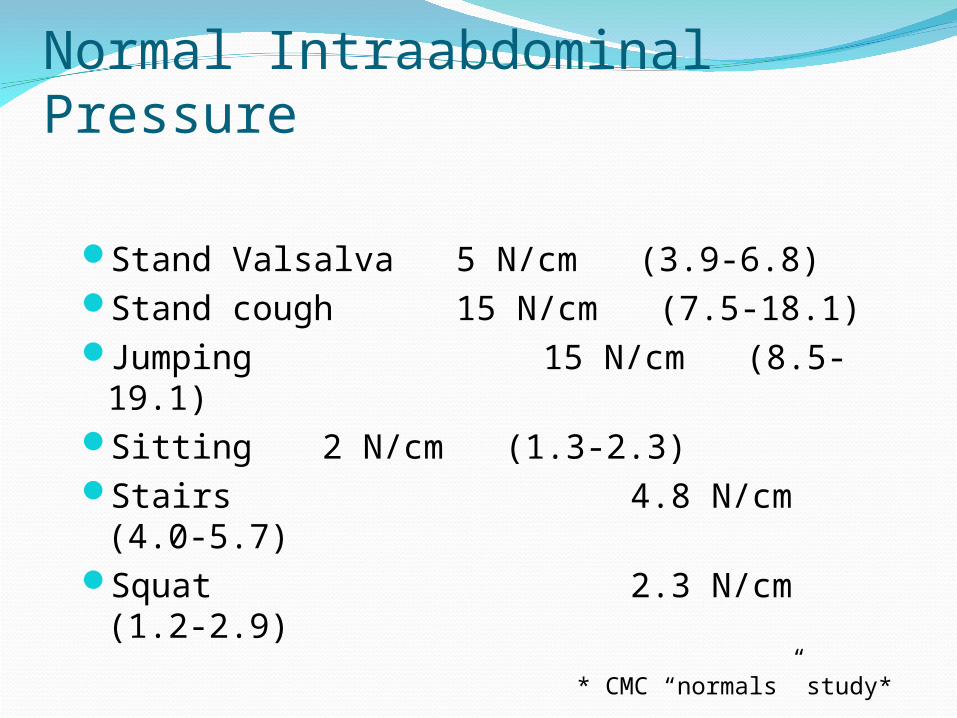
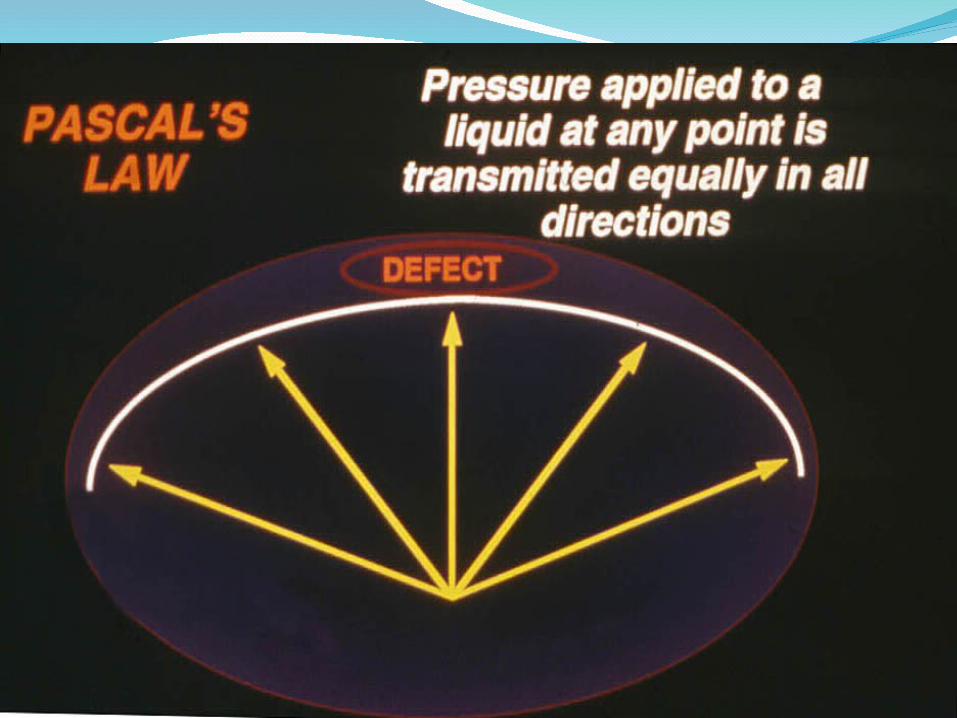
Normal Intraabdominal Pressure
Stand Valsalva 5 N/cm (3.9-6.8)
Stand cough 15 N/cm (7.5-18.1)Jumping 15 N/cm (8.5-19.1)Sitting 2 N/cm (1.3-2.3)Stairs 4.8 N/cm (4.0-5.7)Squat 2.3 N/cm (1.2-2.9)
* CMC “normals” study*

PIONEERSLeBlanc (Louisiana)
Toy and Smoot (Delaware)
Gagner , Park and Pomp (Canada)
Franklin (Texas) and Ramshaw (Atlanta)
Voeller and Mangiante (Memphis)
LeBlancSurg Laparosc Endosc 1993
5 cases; ePTFE
5 trocars
Staples only; no sutures
Extension of his IPOM technique
Toy and SmootExtension of their IPOM for inguinal
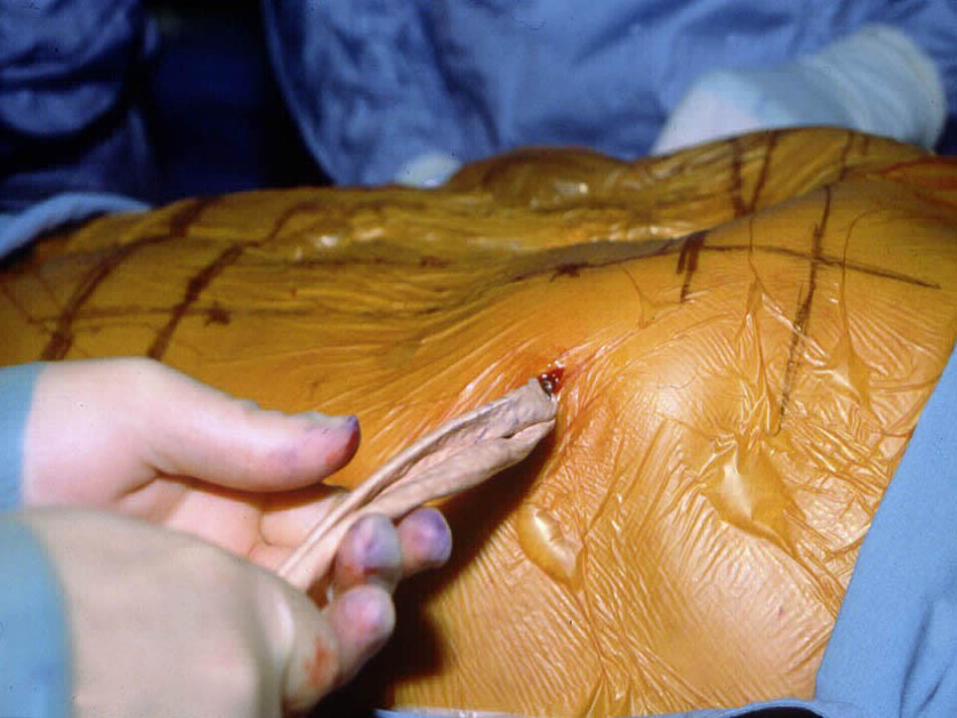
Developed mesh spreader
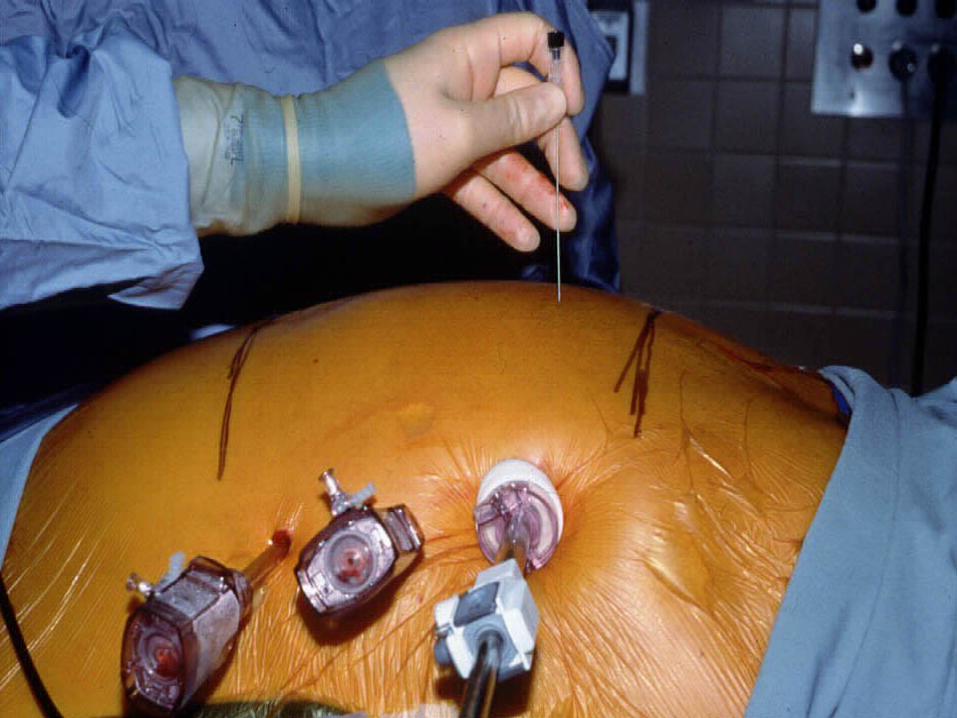
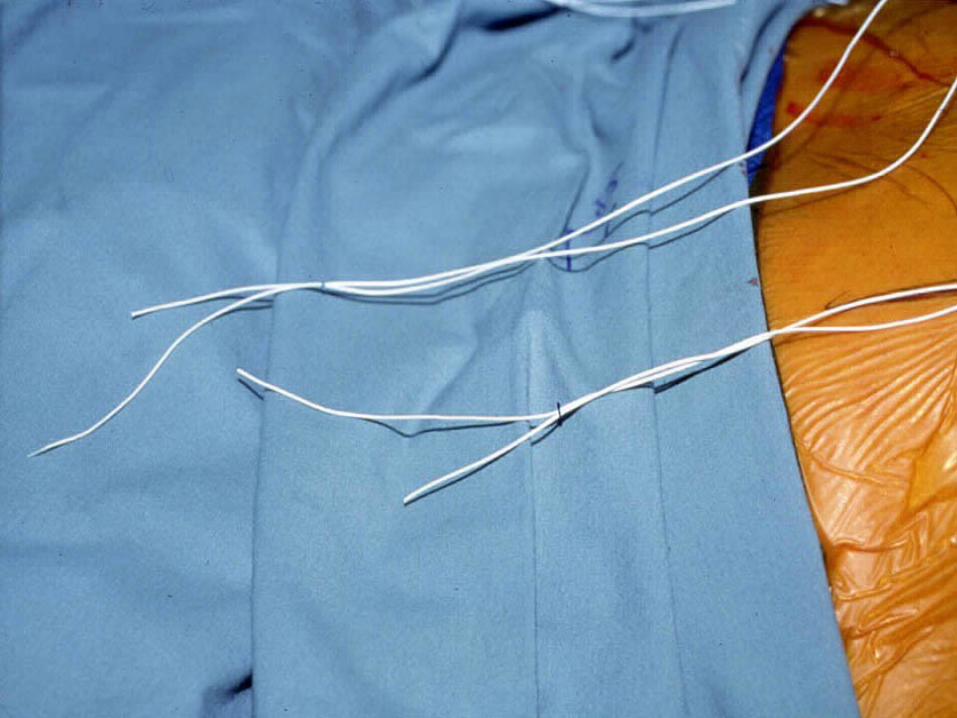
Developed suture passer
Used ePTFE
FranklinSurg Laparosc Endosc 1998176 patients from 1991-1998ePTFE and PPM; sutures and staplesFirst to try to close defect if possibleF/U 1-84 months1.1% recurrenceNo mention of % f/u
Voeller and MangianteFirst case in 1993 with staples onlyRecurred 6 months laterMangiante taught Rives repair by George
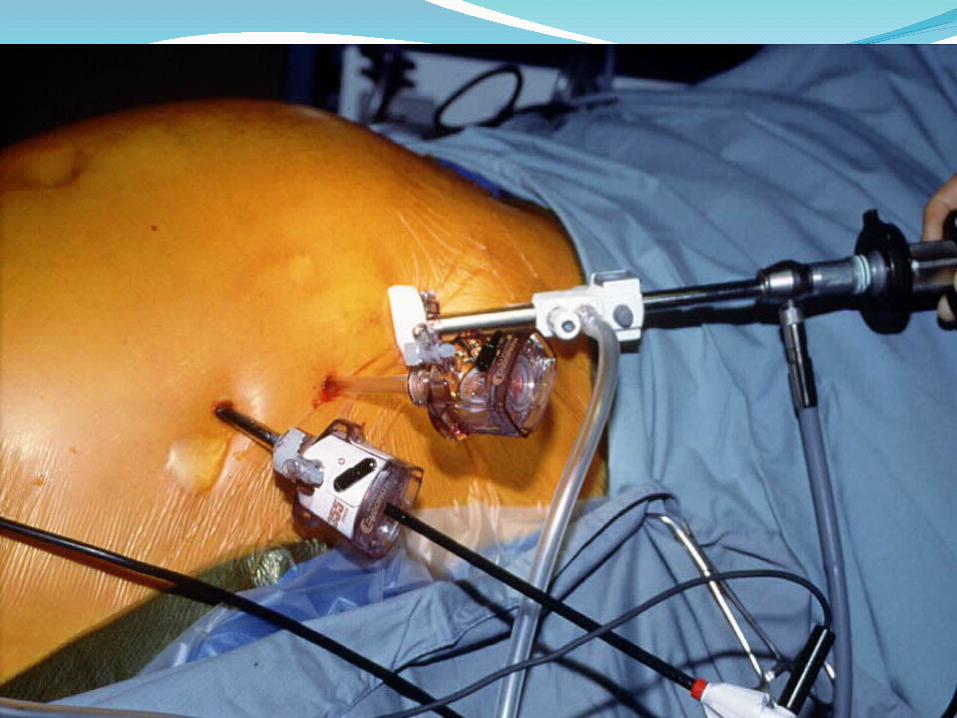
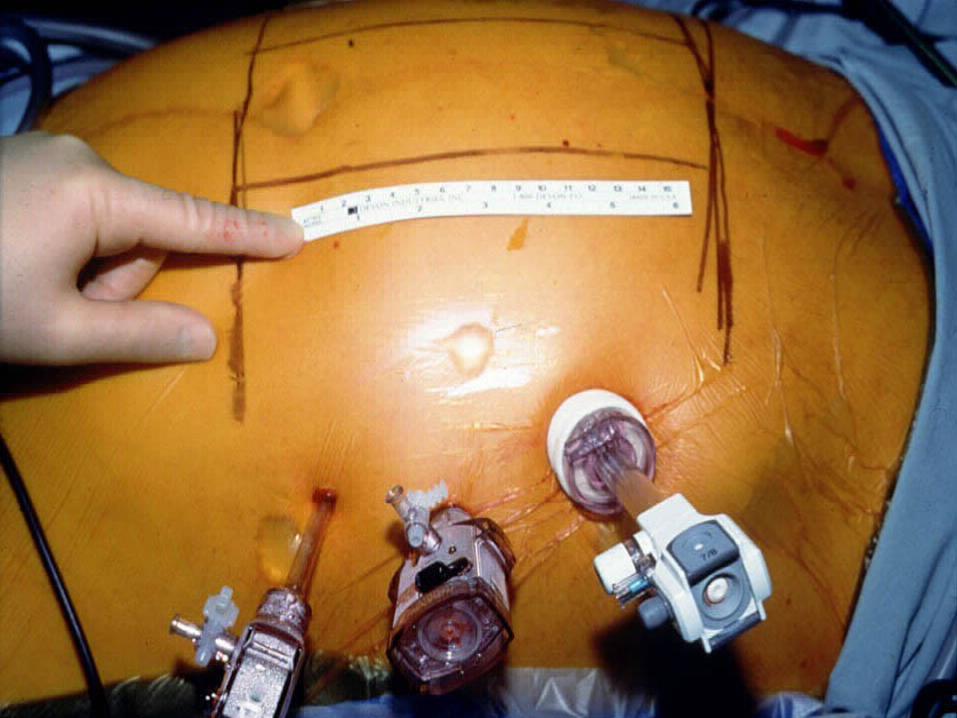
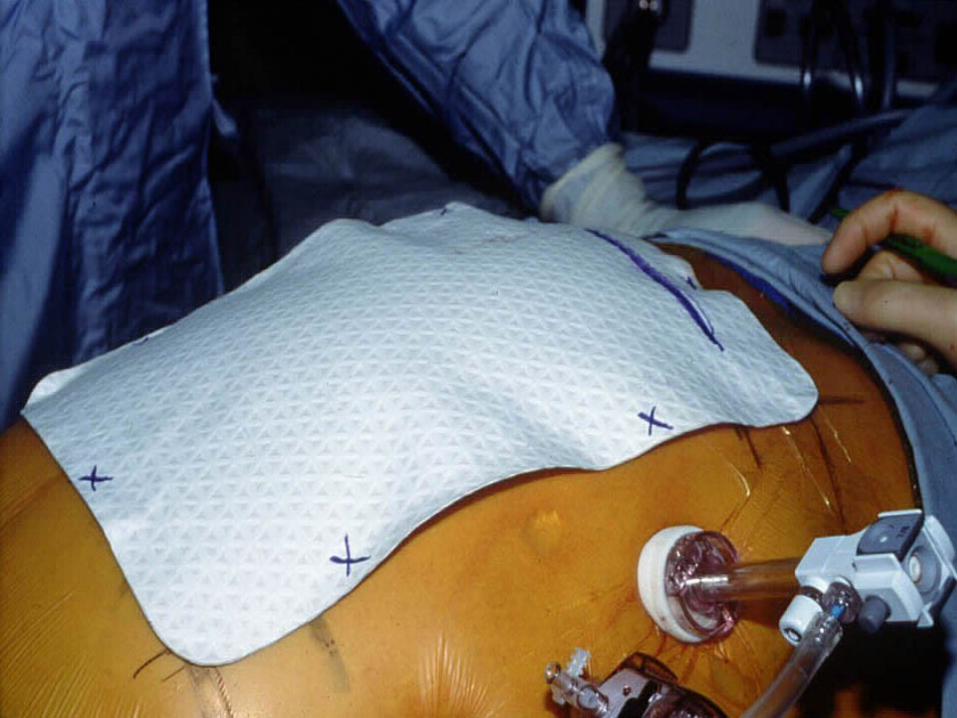
WantzRealized mimic Rives was criticalFirst to use 5mm tacking deviceFirst to do with all 5mm portsIntroduced Ioban® as part of procedureFirst course in the world in 1995 in Memphis
Park, Gagner and Pomp1996 Surg Laparosc Endosc
30 cases
ePTFE and PPM; sutures
One recurrence at 18 mo f/u
Minimal morbidity
Prospective, Multicenter Study of Laparoscopic Ventral Hernioplasty. Preliminary ResultsToy, Bailey, Carey, Chappius, Gagner, Josephs,
Mangiante, Park, Pomp, Smoot, Uddo, VoellerSurg Endosc 1998Hernias > 4 cm2- ePTFE; sutures and staples
(tacks)144 patients over first 2 yearsMean OR time was 120 minMean f/u was 355 days with 95% f/u4.2% RR; D/C at mean of 2.3 daysReturn to normal activity at 15 days
RAMSHAWAm Surg 1999Retrospective study of lap vs open3 year period, 1995-1998Mean f/u was 21 months36 recurrences in open and 2 in the lap groupComplications much less
VOELLERACS 1999Heniford, Park, Ramshaw, Voeller407 repairsF/U 2-5 yearsRR 3.4% majority due to mesh removal for
infection
PARKAmerican Surgical AssociationPublished AOS 2003Heniford, Park , Ramshaw, Voeller850 patients13% morbidityMean f/u was 20 months4.7% RR
ConclusionsLAP has fewer wound problemsLAP has fewer mesh infectionsLAP has quicker return to activityLAP and OPEN same recurrence rateQOL is same after LAP and OPENLAP does not reconstruct abdominal wallNeed a study to see if lack of reconstruction
matters
Abdominal Wall FunctionRectus muscles act as stays to stabilize
Linea alba is a larger area than a “line”
Lateral muscles insert on midline via rectus sheath
Length of muscle fibers are short in upper, long in the middle and nonexistent in lower
Incisional HerniaMore than a hole in the abdominal wall
Different from groin, epigastric or umbilical hernias
Rives called it “eventration disease”
Extent of eventration dictates for the most part what I do for incisional hernia
Eventration DiseaseRespiratory insufficiency
Abdominal wall moves in and out during both inspiration and expiration
Bowels are pushed out on inspiration and eventually the bowels lose their right of domain
Back muscles are not counterbalanced by abdomen
Eventration Disease (cont.)Postural changes occur i.e. lordosis
Lateral abd. muscles retract
Muscles become fatty and fibrotic
Lateral retraction makes defect larger
Last changes are dermatologic - skin ischemia, ulcers
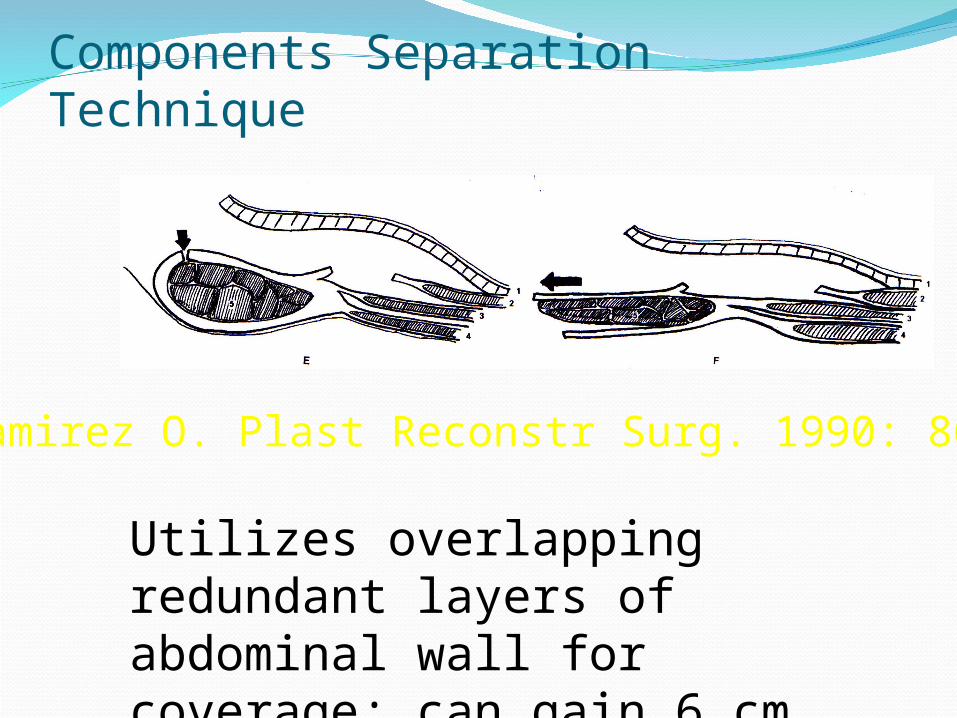
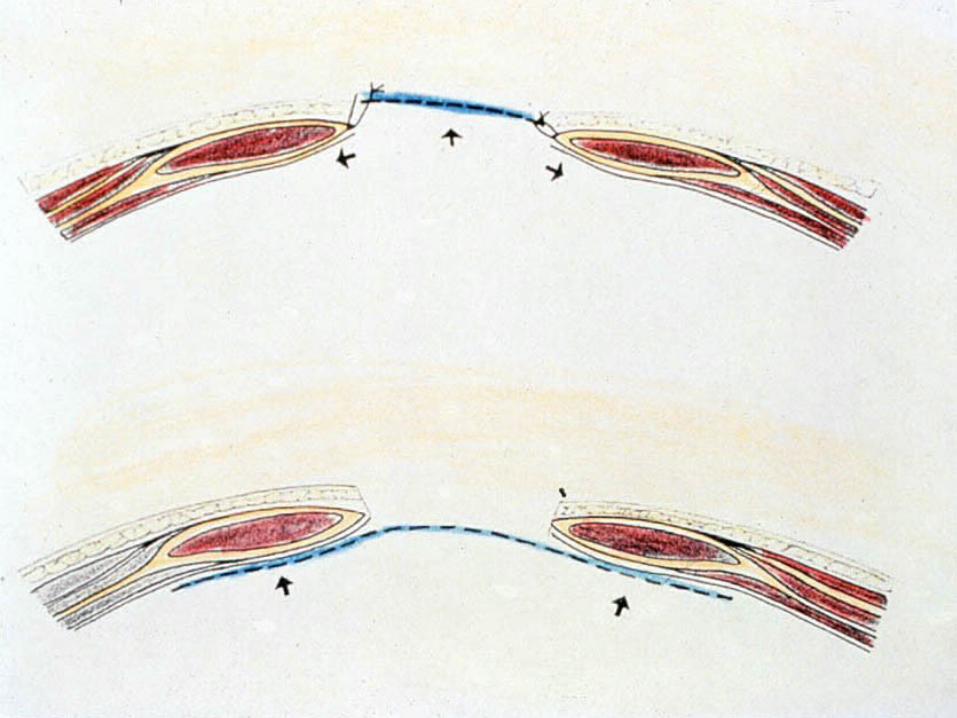
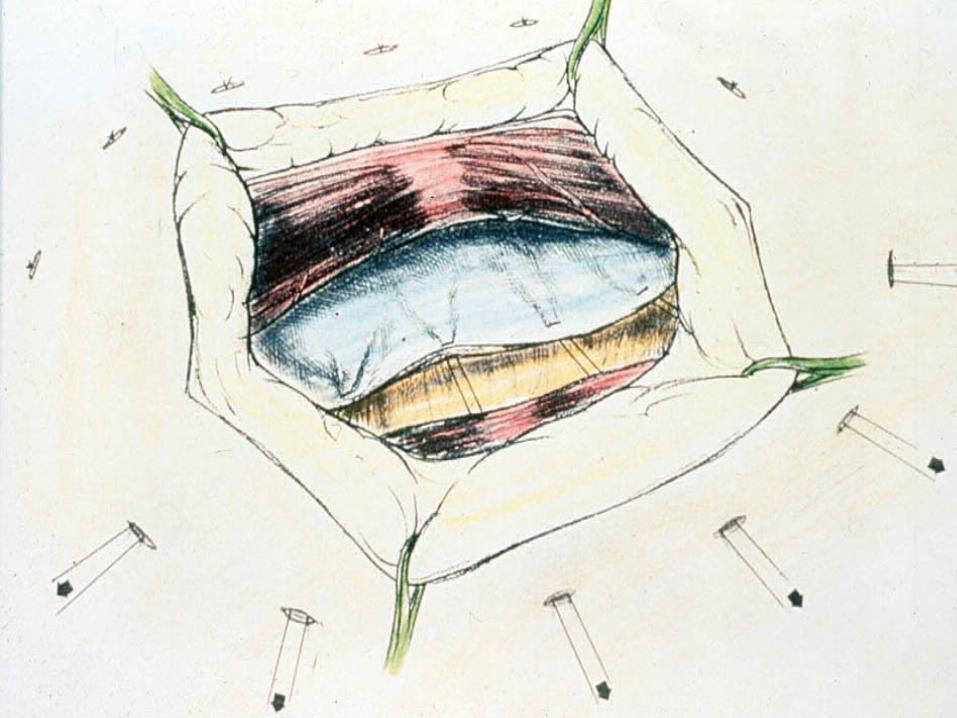
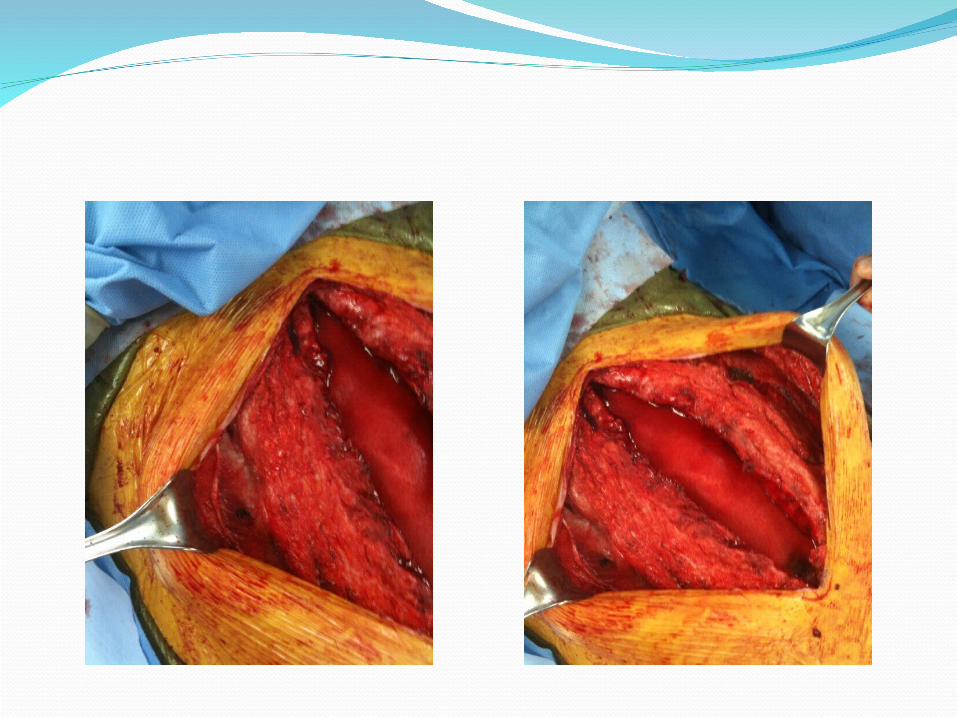
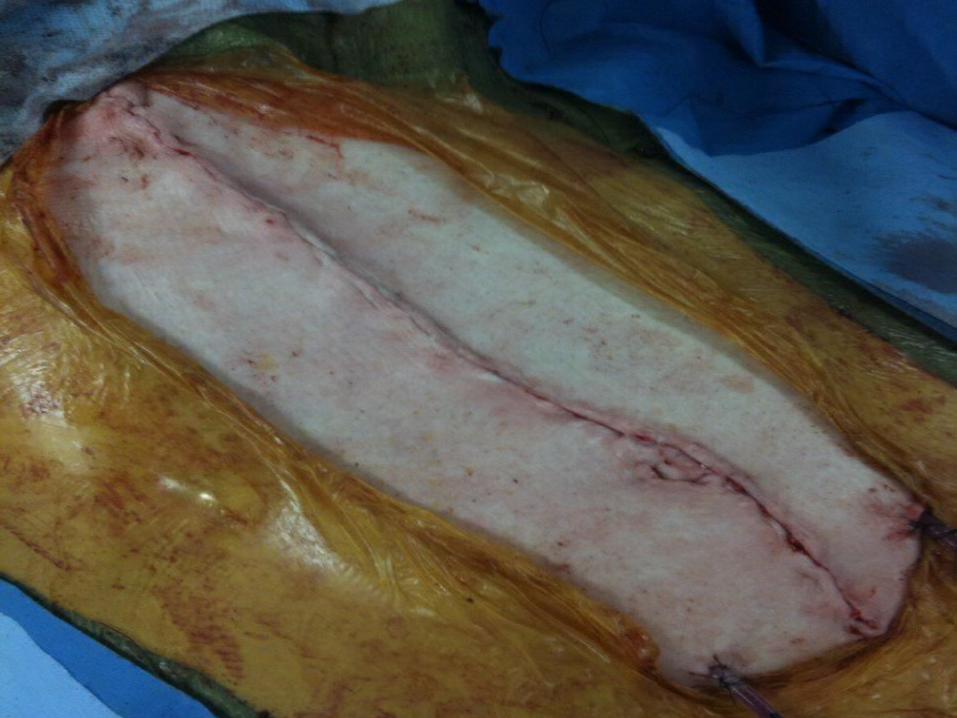
Components Separation Technique
Ramirez O. Plast Reconstr Surg. 1990: 86:519)
Utilizes overlapping redundant layers of abdominal wall for coverage; can gain 6 cm laterally from each side
COMPONENTS SEPARATION• Bleichrodt the Netherlands JACS 2003• 43 patients with ventral hernias• Mean f/u of 15 months in 38 patients• 17 with complications• 12 of 38 (32%) with recurrence• Best in contaminated situation where mesh
should not be used

MIS Components SeparationFirst group to do was Lowe PRS 2000
Maas and Bleichrodt used hernia balloon
Rosen popularizing in USA
Combine MIS CS with closure of the defect laparoscopically to “reconstruct” the abd. wall
FutureSILSNotesSelf-Adhering meshMeshes impregnated with agents to fight
infectionMeshes impregnated with agents to decrease
painAbdominal wall transplant
ADHESIVELadurner, Eur J Med Res 2008
Cyanoacrylat glue vs tacks vs sutures
Animal model of LVIH
Glue equal to tacks in tensile strength
NOTESFong, Endoscopy 2007Transcolonic5 pigs2 x 3 cm pieces of meshUsed magnetsTransfascial suturesAll meshes intact and no infection at sacrifice
NOTESSurg Endosc, Miedema 2009Transgastric; 5 pigs13 x 15 cm Surgisis with sutures deliveredSacrificed at 2 weeksOR time 215 minCulture positive abscesses present in 3 of 5
meshesAdhesions varied from 2-100%
NOTESJacobsenHernia 200938 y.o. femalePainful recurrent umbilical herniaRepaired transvaginally
NOTESLomanto 20095 pigsMesh placed and fixed transvaginally; fibrin
glueSacrificed at 2 weeksAll meshes in placeOne subQ abscess
Self-Adhering MeshChampault Hernia 2009LW PPM; Adhesix® (Cousin Biotech, France)Coated with glue on one sideImplanted laparoscopically in pigsRemoval at 1 day, 1 week and 1 month post-
opExcellent integrationNo migration or shrinkage

Thank youThank you