Embed Size (px)
Citation preview
Gynecologic Oncology-Gynecologic Oncology-The Times They Are The Times They Are
A’Changin A’Changin
Ronald D. Alvarez, MDRonald D. Alvarez, MD
University of Alabama at BirminghamUniversity of Alabama at BirminghamDivision of Gynecologic OncologyDivision of Gynecologic Oncology

DisclosuresDisclosures
Grant supportGrant support
– Morphoteck Morphoteck
– Pfizer Pfizer
– MerrimackMerrimack
Florida Society of Florida Society of Gynecologic OncologyGynecologic Oncology
Organized 1993Organized 1993 Founders meeting 1994 Founders meeting 1994
(Holloway,Chair) (Holloway,Chair) Invited speaker at 1Invited speaker at 1stst, and , and
1010thth meetings (one with a meetings (one with a hurricane) hurricane)
Invited for 19Invited for 19thth meeting meeting (Penalver, Chair)(Penalver, Chair)
Many longterm Many longterm connections and friendsconnections and friends

Lecture OutlineLecture Outline
Thoughts on change Thoughts on change Changes in gynecologic oncologyChanges in gynecologic oncology Drivers of change Drivers of change Adapting to changeAdapting to change

Lecture OutlineLecture Outline
Thoughts on change Thoughts on change Changes in gynecologic oncologyChanges in gynecologic oncology Drivers of change Drivers of change Adapting to changeAdapting to change

There is nothing There is nothing permanent except permanent except change.change.- - Heraclitus, c. 500 BC Heraclitus, c. 500 BC

Rapid Pace of ChangeRapid Pace of Change
Agricultural revolution Agricultural revolution 8000 yrs8000 yrs Industrial revolution Industrial revolution 120 yrs 120 yrs Light bulb Light bulb 90 yrs 90 yrs Moon landing Moon landing 22 yrs 22 yrs World wide web World wide web 9 yrs 9 yrs Human genome sequencedHuman genome sequenced

Principles of Principles of Transformational ChangeTransformational Change
Something old Something old passes awaypasses away
Something new Something new comes to becomes to be
Something stays Something stays the samethe same
Aristotle, 350 BC

Why Is Change So Threatening?Why Is Change So Threatening?
We all have a worldviewWe all have a worldview It is shaped by beliefs, It is shaped by beliefs,
values, experiencevalues, experience Change often Change often
challenges and challenges and misaligns our misaligns our worldview worldview
How Is Change Best Implemented?How Is Change Best Implemented?
Positive vision of Positive vision of abundanceabundance
Create a readiness for Create a readiness for changechange
Implement small Implement small changes that changes that stakeholders can ownstakeholders can own
Help stakeholders Help stakeholders change worldviewchange worldview
Win
Win Win
WIN
Win
Win

Lecture OutlineLecture Outline
Thoughts on change Thoughts on change Changes in gynecologic oncologyChanges in gynecologic oncology Drivers of change Drivers of change Adapting to changeAdapting to change

Personal PerspectivePersonal Perspective Born – 1957Born – 1957 High school – 1975High school – 1975 College and married – 1979College and married – 1979 Medical school – 1983 Medical school – 1983 Children -1984, 1987, 1992Children -1984, 1987, 1992 Residency -1987Residency -1987 Fellowship -1990Fellowship -1990 Division Director – 2003Division Director – 2003 First grandchild, SGO President - 2012First grandchild, SGO President - 2012
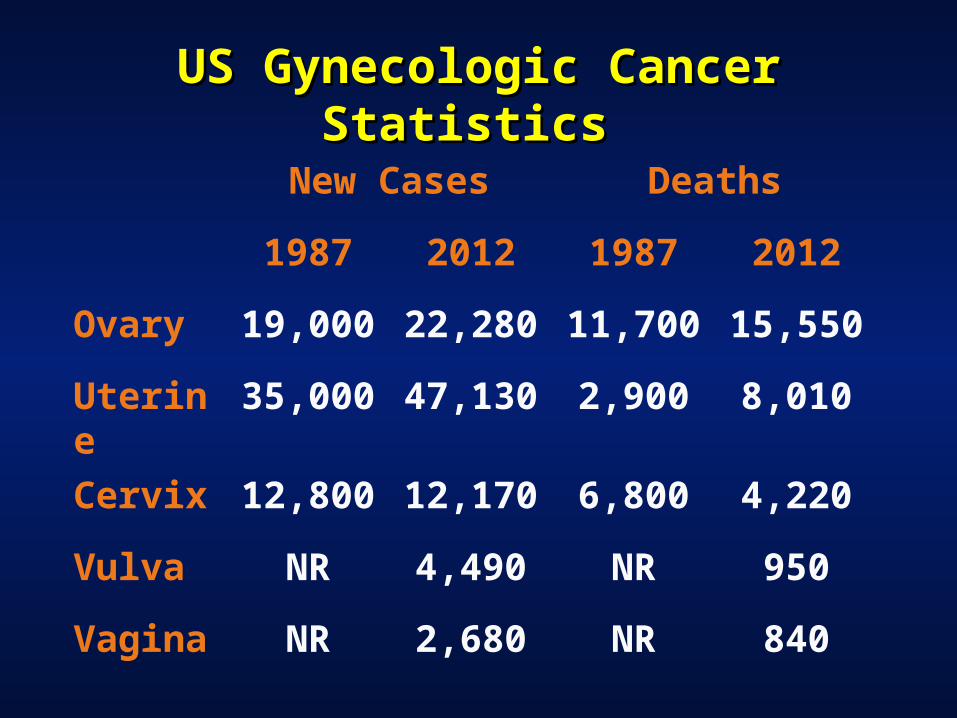
US Gynecologic Cancer Statistics US Gynecologic Cancer Statistics
New Cases Deaths
1987 2012 1987 2012
Ovary 19,000 22,280 11,700 15,550
Uterine 35,000 47,130 2,900 8,010
Cervix 12,800 12,170 6,800 4,220
Vulva NR 4,490 NR 950
Vagina NR 2,680 NR 840

Ovarian Cancer - 1987Ovarian Cancer - 1987
Risk groups not identifiedRisk groups not identified Known as the Known as the ““silentsilent”” cancer cancer Surgical debulking often suboptimalSurgical debulking often suboptimal Limited chemotherapy optionsLimited chemotherapy options Short median survivalShort median survival
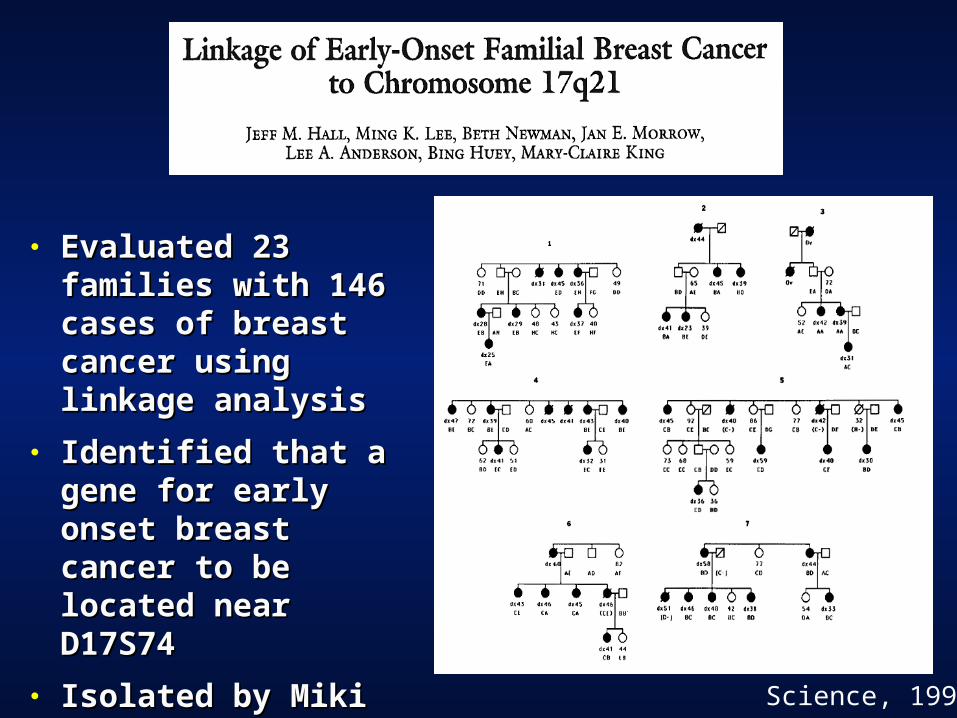
Science, 1990
● Evaluated 23 families Evaluated 23 families with 146 cases of with 146 cases of breast cancer using breast cancer using linkage analysislinkage analysis
● Identified that a gene Identified that a gene for early onset breast for early onset breast cancer to be located cancer to be located near D17S74near D17S74
● Isolated by Miki et al in Isolated by Miki et al in 1994 Science paper1994 Science paper

Hereditary Ovarian Cancer – Beyond Hereditary Ovarian Cancer – Beyond the Usual Suspectsthe Usual Suspects
Swisher, 2012
Screening for Ovarian CancerScreening for Ovarian Cancer
PLCO Trial (Partridge et al, 2009)PLCO Trial (Partridge et al, 2009)– Evaluated annual CA125 and TVU vs. Evaluated annual CA125 and TVU vs.
observation in general population observation in general population – 20:1 surgery:cancer ratio20:1 surgery:cancer ratio– Most late stage/no reduction in mortalityMost late stage/no reduction in mortality
UKCTOCSUKCTOCS– Evaluating yearly CA125 vs. yearly TVU Evaluating yearly CA125 vs. yearly TVU
vs. observation in general populationvs. observation in general population– Results due 2014Results due 2014
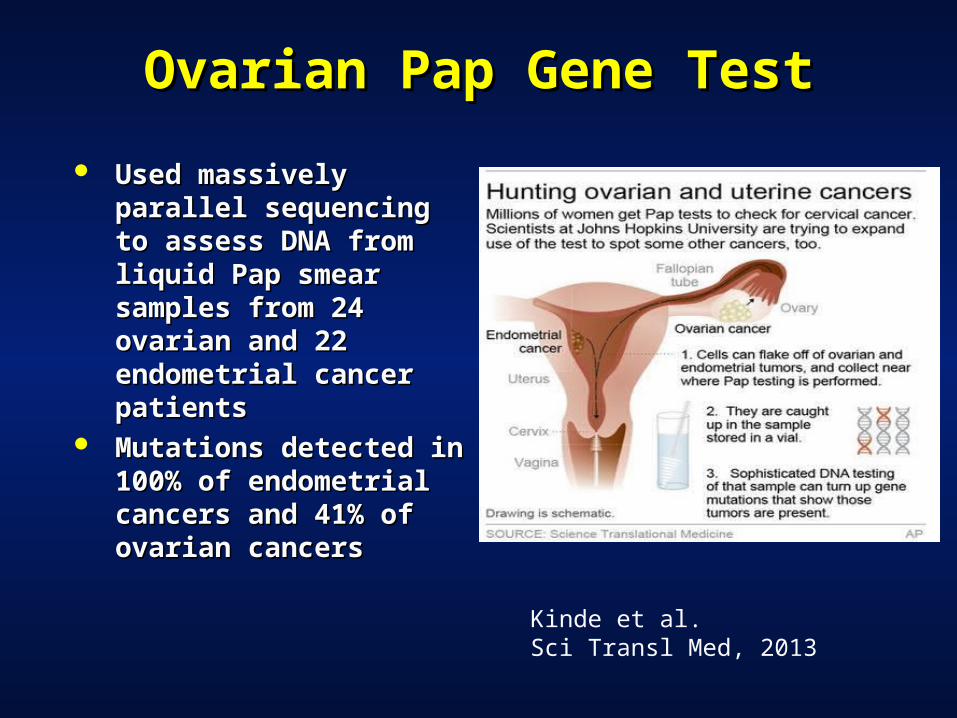
Ovarian Pap Gene TestOvarian Pap Gene Test
Used massively Used massively parallel sequencing to parallel sequencing to assess DNA from liquid assess DNA from liquid Pap smear samples Pap smear samples from 24 ovarian and 22 from 24 ovarian and 22 endometrial cancer endometrial cancer patientspatients
Mutations detected in Mutations detected in 100% of endometrial 100% of endometrial cancers and 41% of cancers and 41% of ovarian cancersovarian cancers
Kinde et al. Sci Transl Med, 2013

Ovarian Cancer is not a Ovarian Cancer is not a ““SilentSilent”” Cancer Cancer
Symptoms Symptoms – BloatingBloating– Pelvic or abdominal painPelvic or abdominal pain– Difficulty eating or feeling full quicklyDifficulty eating or feeling full quickly– Urinary symptoms (urgency or Urinary symptoms (urgency or
frequency)frequency) Workup – Pelvic exam, sonar, CA125Workup – Pelvic exam, sonar, CA125

Achieving Maximum Debulking in Achieving Maximum Debulking in Ovarian CancerOvarian Cancer
• Debulking TAH BSODebulking TAH BSO
• OmentectomyOmentectomy
• Colon resectionColon resection
• Small bowel resectionSmall bowel resection
• SplenectomySplenectomy
• Hepatic resectionHepatic resection
• Diaphragm strippingDiaphragm stripping
• Peritoneal strippingPeritoneal stripping
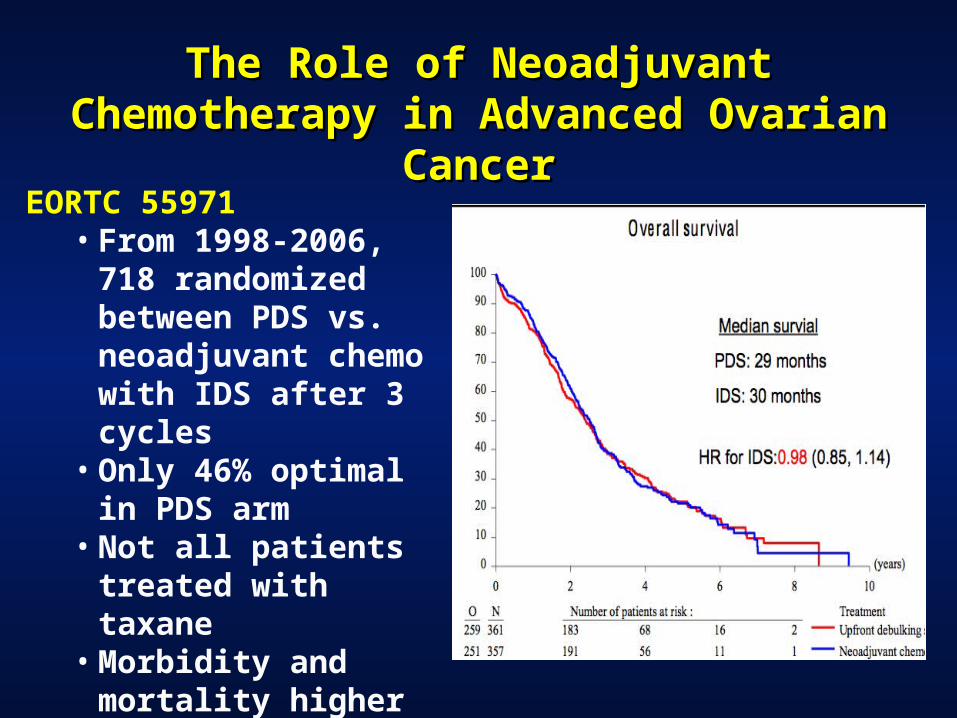
The Role of Neoadjuvant Chemotherapy in The Role of Neoadjuvant Chemotherapy in Advanced Ovarian CancerAdvanced Ovarian Cancer
EORTC 55971• From 1998-2006, 718
randomized between PDS vs. neoadjuvant chemo with IDS after 3 cycles
• Only 46% optimal in PDS arm
• Not all patients treated with taxane
• Morbidity and mortality higher in the PDS arm
New Chemotherapy Approaches New Chemotherapy Approaches in Ovarian Cancer in Ovarian Cancer
Taxane based regimensTaxane based regimens
Intraperitoneal chemotherapyIntraperitoneal chemotherapy
Dose dense taxanesDose dense taxanes
Consolidation chemotherapyConsolidation chemotherapy
Anti-angiogenic therapyAnti-angiogenic therapy
PARP inhibitorsPARP inhibitors

TCGA Project – Molecular TCGA Project – Molecular Characterization of HGSCCharacterization of HGSC
Serous 82%
Carcinosarcoma 6%
Clear cell 6%
Endometrioid 3%
Mixed 3%
BRCA1 Germline
8%BRCA2
Germline6%
BRCA1 Somatic
3%
BRCA2 Somatic
3%
BRCA1 Methylation
11%
EMSY Amplification
6%PTEN Loss
5%Other HRD7%
CCNE1 Amplification
15%
MMR Germline
2%
RB1 deletion3%
PIK3CA Amplification
4%
KRAS Amplification
3%
NF1 Deletion3% Other
21%
CGARN, Nature 2011

PACLITAXEL
CISPLATIN
AGGRESSIVESURGERY,
COMBINATIONCHEMOTHERAPY
Su
rviv
al (
mo)
Progress in Ovarian Cancer Progress in Ovarian Cancer
PACLITAXELCARBO
IP THERAPY

Endometrial Cancer - ThenEndometrial Cancer - Then
No known risk groupsNo known risk groups Poor understanding of biologyPoor understanding of biology Surgical staging rare Surgical staging rare All patients treated with radiationAll patients treated with radiation Limited use of adjuvant systemic Limited use of adjuvant systemic
therapytherapy

HNPCC and Endometrial CancerHNPCC and Endometrial Cancer
2-3% of all endometrial cancers2-3% of all endometrial cancers Due to mutations in MMR genes Due to mutations in MMR genes
– MLH1, MSH2, MSH6,EPCAM, PMS2MLH1, MSH2, MSH6,EPCAM, PMS2 Identifying patients at riskIdentifying patients at risk
– Colorectal/endometrial cancer age < 50Colorectal/endometrial cancer age < 50– MSI high histology (i.e., mucinous, signet ring, TIL)MSI high histology (i.e., mucinous, signet ring, TIL)– Abnormal MSI/IHC tumor test Abnormal MSI/IHC tumor test – 2 or more family members with HNPCC related 2 or more family members with HNPCC related
cancer, one age <50cancer, one age <50– 3 or more family members with HNPCC related 3 or more family members with HNPCC related
cancer, any agecancer, any age
Modern Surgical Management of Modern Surgical Management of Endometrial CancerEndometrial Cancer
MIS has improved surgical MIS has improved surgical outcomesoutcomes
Robotic surgery more Robotic surgery more feasible for obese patientsfeasible for obese patients
Surgical staging still Surgical staging still controversial controversial
Debulking employed more Debulking employed more with advanced stage with advanced stage cancercancer

Uterine Cancer - Uterine Cancer - Adjuvant TreatmentAdjuvant Treatment
Low risk early stage Low risk early stage – No benefit of radiationNo benefit of radiation
Intermediate risk early stageIntermediate risk early stage– Vaginal brachytherapyVaginal brachytherapy– Chemotherapy/radiationChemotherapy/radiation
High risk advanced stage/RecurrentHigh risk advanced stage/Recurrent– Chemotherapy Chemotherapy ++ radiation radiation

Advances in Endometrial CancerAdvances in Endometrial Cancer
Evolving Evolving understanding of understanding of pathogenesispathogenesis
TCGA elucidating TCGA elucidating biologybiology
Targeted therapeuticsTargeted therapeutics– AntiangiogenesisAntiangiogenesis– mTOR inhibitorsmTOR inhibitors

Cervical Cancer - 1987Cervical Cancer - 1987
Evolving understanding of Evolving understanding of etiology/natural historyetiology/natural history
Annual Pap standard of careAnnual Pap standard of care CKC, cryo, laser used for CINCKC, cryo, laser used for CIN Radical hysterectomyRadical hysterectomy Radiation alone usedRadiation alone used

New 2013 Cervical Cancer New 2013 Cervical Cancer Screening GuidelinesScreening Guidelines
Age < 21 – No screeningAge < 21 – No screening Age 21-29 – Cytology alone q Age 21-29 – Cytology alone q
3 yrs 3 yrs Age 30-65 – Cytology/HPV Age 30-65 – Cytology/HPV
testing q 5 yrs testing q 5 yrs Age > 65 – No screening with Age > 65 – No screening with
negative prior screeningnegative prior screening After hysterectomy – No After hysterectomy – No
screening unless history of screening unless history of CIN 2/3 or cervical caCIN 2/3 or cervical ca
Cervical Cancer VaccinesCervical Cancer Vaccines
All VLP basedAll VLP based– Merck - Gardasil - 16/18/6/11Merck - Gardasil - 16/18/6/11– GSK - Cervarix - 16/18 - ASO4GSK - Cervarix - 16/18 - ASO4
EfficacyEfficacy– Enhances HPV Ab responseEnhances HPV Ab response– Decreases CIN 2/3Decreases CIN 2/3– Duration of protection at Duration of protection at
least 5 yrs least 5 yrs

Modern Surgical ManagementModern Surgical Management of Cervical Cancer of Cervical Cancer
PET CT allows for PET CT allows for better preop better preop assessment assessment
MIS has improved MIS has improved surgical outcomessurgical outcomes
Fertility sparing Fertility sparing procedures – CKC, procedures – CKC, radical trachelectomyradical trachelectomy
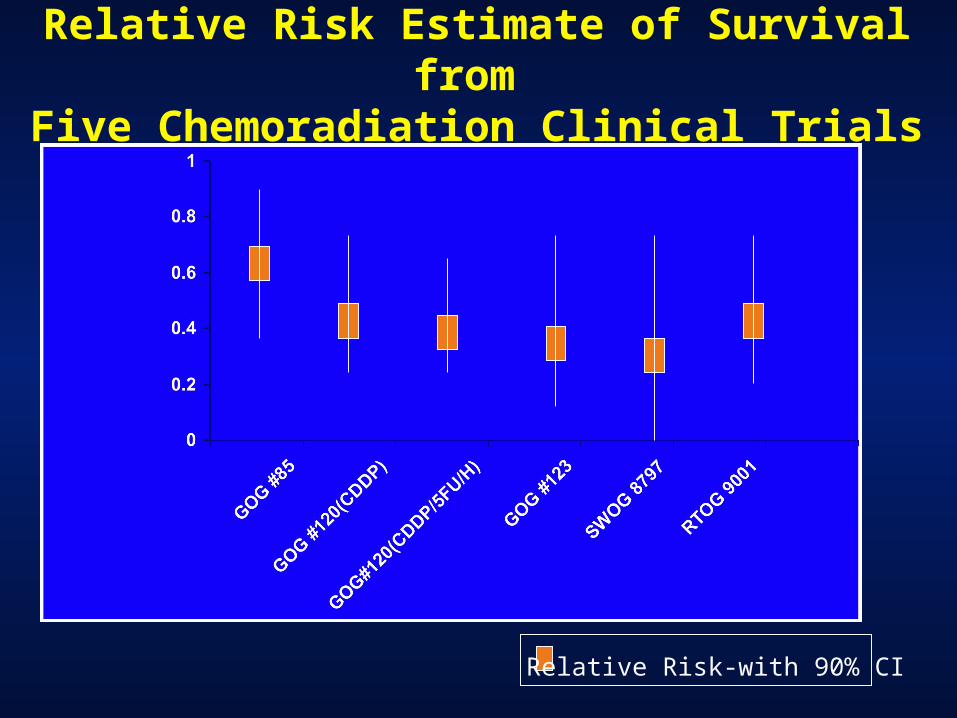
Relative Risk Estimate of Survival from Five Chemoradiation Clinical Trials
Relative Risk-with 90% CI
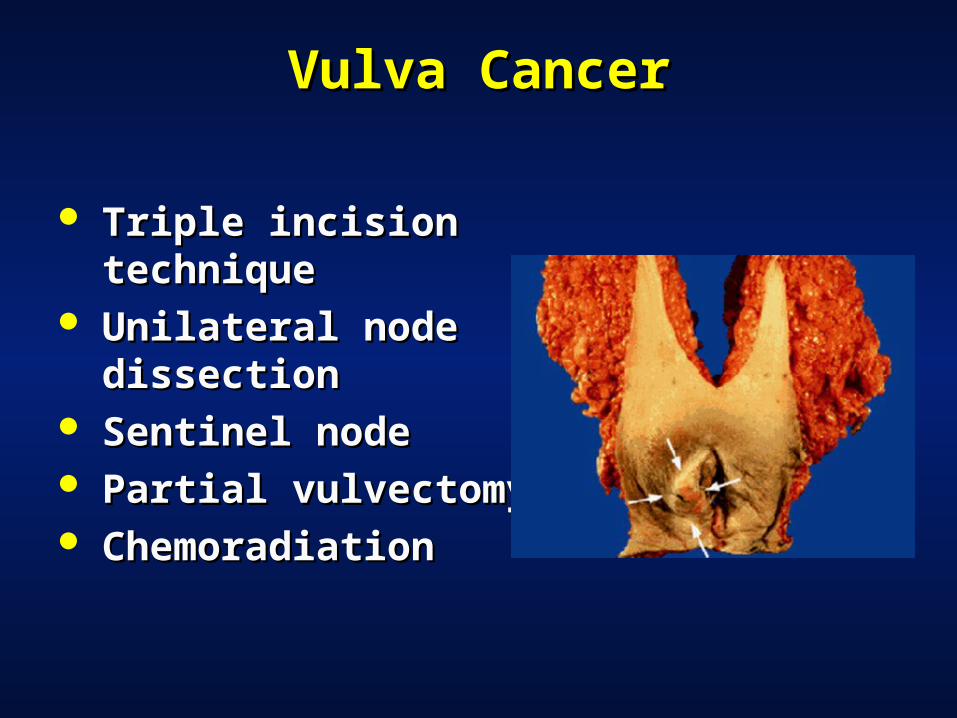
Vulva CancerVulva Cancer
Triple incision Triple incision techniquetechnique
Unilateral node Unilateral node dissectiondissection
Sentinel nodeSentinel node Partial vulvectomyPartial vulvectomy ChemoradiationChemoradiation

Lecture OutlineLecture Outline
Thoughts on change Thoughts on change Changes in gynecologic oncologyChanges in gynecologic oncology Drivers of change Drivers of change
– Scientific discovery and Scientific discovery and innovationinnovation
Adapting to changeAdapting to change

The Genomic RevolutionThe Genomic Revolution

Clinical and Surgical InnovationClinical and Surgical Innovation
Enhanced imaging Enhanced imaging technologytechnology
Minimally invasive Minimally invasive surgerysurgery
Targeted Targeted therapeuticstherapeutics
Improved Improved supportive caresupportive care

Lecture OutlineLecture Outline
Thoughts on change Thoughts on change Changes in gynecologic oncologyChanges in gynecologic oncology Drivers of change Drivers of change
– Changing demographicsChanging demographics Adapting to changeAdapting to change

The US Population is GrowingThe US Population is Growing

The US Population is Getting OlderThe US Population is Getting Older

The Number of Patients with a The Number of Patients with a Gyn Cancer will IncreaseGyn Cancer will Increase
2010 2030
All 1.6 mil 2.3 mil
Cervix 13,000 17,000
Uterine 44,000 58,000
Ovarian 24,000 33,000
Smith et alJCO, 2009

We are More Culturally DiverseWe are More Culturally Diverse
50% nonwhite in 50% nonwhite in 20502050
Latino and Asian Latino and Asian populations will populations will tripletriple
More multiracialMore multiracial More immigrationMore immigration

We Have Disparities in Gyn CancerWe Have Disparities in Gyn Cancer
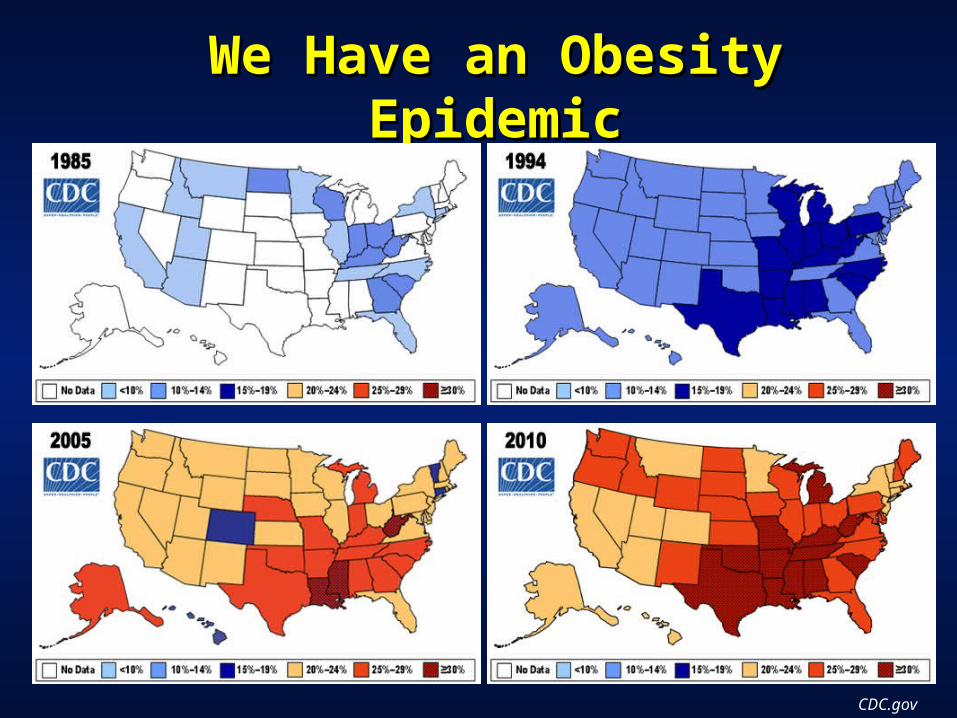
We Have an Obesity We Have an Obesity EpidemicEpidemic
CDC.gov

Lecture OutlineLecture Outline
Thoughts on change Thoughts on change Changes in gynecologic oncologyChanges in gynecologic oncology Drivers of change Drivers of change
– Government relatedGovernment related Adapting to changeAdapting to change

Cost of Health Care in USCost of Health Care in US
0
1000
2000
3000
4000
5000
6000
7000
8000
19
80
19
81
19
82
19
83
19
84
19
85
19
86
19
87
19
88
19
89
19
90
19
91
19
92
19
93
19
94
19
95
19
96
19
97
19
98
19
99
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
United StatesNorwaySwitzerlandCanadaNetherlandsGermanyFranceDenmarkAustraliaSwedenUnited KingdomNew Zealand
0
2
4
6
8
10
12
14
16
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
United StatesFranceSwitzerlandGermanyCanadaNetherlandsNew ZealandDenmarkSwedenUnited KingdomNorwayAustralia
Total expenditures on health as % of GDPAverage spending on health per capita
The U.S. spends 2.4x the average of all developed countries and 60% more per capita
than the next highest spenders
Health Care Reform in USHealth Care Reform in US
PPACA – signed 3/23/10PPACA – signed 3/23/10 Upheld by Supreme Upheld by Supreme
Court, Presidential Court, Presidential Election 2012Election 2012
Major goals Major goals – increase the number of increase the number of
insuredinsured
– Improve qualityImprove quality
– control rising health control rising health
care care costscosts
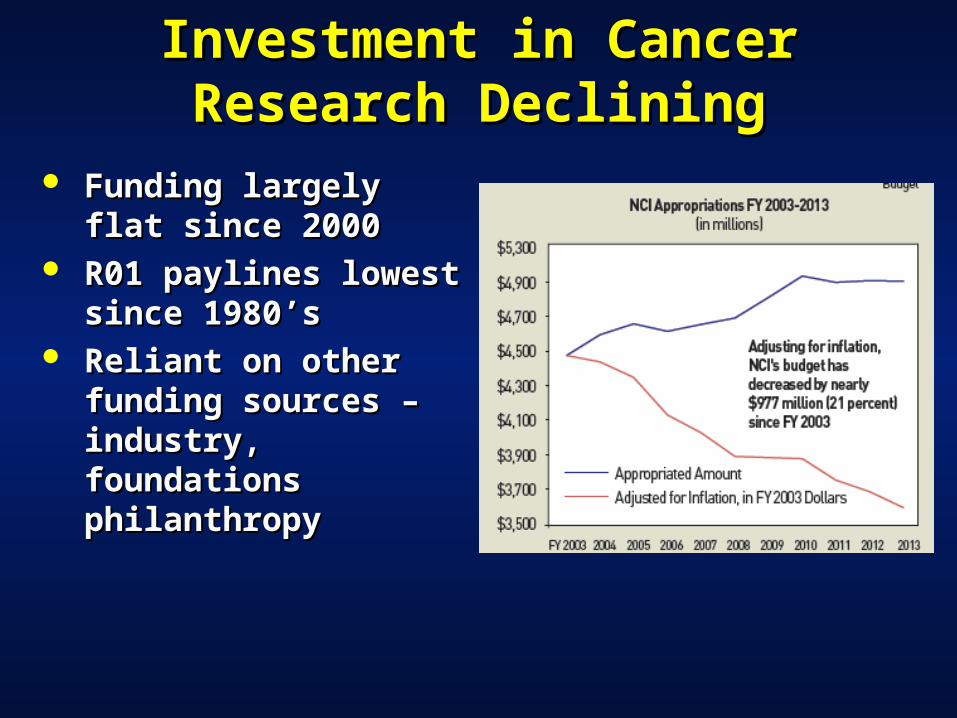
Investment in Cancer Research Investment in Cancer Research DecliningDeclining
Funding largely flat Funding largely flat since 2000since 2000
R01 paylines lowest R01 paylines lowest since 1980’ssince 1980’s
Reliant on other Reliant on other funding sources – funding sources – industry, foundations industry, foundations philanthropyphilanthropy

NCI Cooperative Group Trials NCI Cooperative Group Trials Program is ReorganizingProgram is Reorganizing
IOM advocates changeIOM advocates change NCI develops NCTNNCI develops NCTN Funding 4 adult and 1 pediatric Funding 4 adult and 1 pediatric
operation centersoperation centers Funding 40 lead academic sitesFunding 40 lead academic sites
Lecture OutlineLecture Outline
Thoughts on change Thoughts on change Changes in gynecologic oncologyChanges in gynecologic oncology Drivers of change Drivers of change Adapting to changeAdapting to change
What and How We Learn What and How We Learn Will Be DifferentWill Be Different
Commit to life long learning Commit to life long learning Define and teach the skills Define and teach the skills
our trainees will need in the our trainees will need in the future future
Ensure continuing education Ensure continuing education and proficiency post trainingand proficiency post training
Innovative IT educational Innovative IT educational strategies strategies

We Must Revolutionize We Must Revolutionize How We Practice How We Practice
Current health care system promotes Current health care system promotes fragmented, poorer quality, high cost fragmented, poorer quality, high cost carecare
The Practice SummitThe Practice Summit− How should high quality, cost effective How should high quality, cost effective
gynecologic cancer care be delivered? gynecologic cancer care be delivered? − How should high quality gynecologic How should high quality gynecologic
cancer care be defined? cancer care be defined? − How should the delivery of high quality How should the delivery of high quality
gynecologic cancer care be fairly gynecologic cancer care be fairly compensated? compensated?
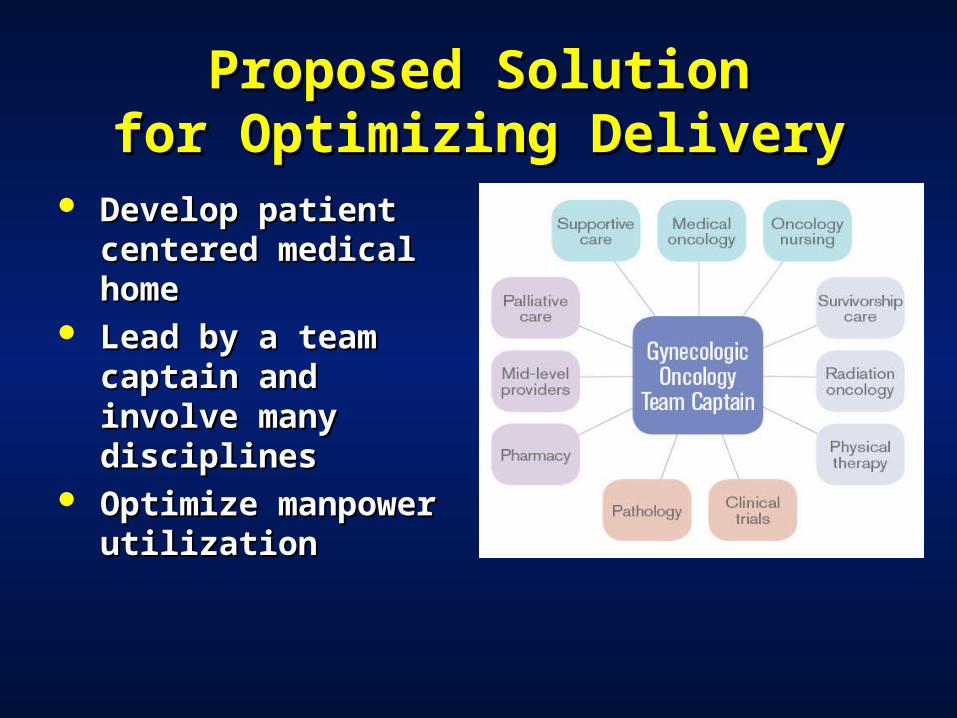
Proposed SolutionProposed Solutionfor Optimizing Deliveryfor Optimizing Delivery
Develop patient Develop patient centered medical centered medical homehome
Lead by a team Lead by a team captain and involve captain and involve many disciplinesmany disciplines
Optimize Optimize manpower manpower utilizationutilization

Proposed SolutionsProposed Solutionsfor Optimizing Qualityfor Optimizing Quality
Create uniform access to Create uniform access to best-qualified providersbest-qualified providers Better define standards for Better define standards for high-quality gynecologichigh-quality gynecologic cancer carecancer care Expand access to clinical Expand access to clinical
trialstrials Hold providers accountable Hold providers accountable
for delivering higher quality for delivering higher quality gynecologic cancer caregynecologic cancer care

Proposed SolutionsProposed Solutionsto Optimizing Payment to Optimizing Payment
SystemsSystems Test episode of care Test episode of care reimbursement reimbursement systems systems
Incentivize hospitals Incentivize hospitals to become centers of to become centers of excellenceexcellence
Fairly value surgery Fairly value surgery for complicated for complicated benign gynecology benign gynecology and obstetric patientsand obstetric patients

We Must Advocate for We Must Advocate for Research in Gynecologic Research in Gynecologic
CancerCancer Enhance research training Enhance research training Set gyn cancer research Set gyn cancer research
priorities and build research priorities and build research teamsteams
Seek funding for research in Seek funding for research in prevention and high mortality prevention and high mortality gynecologic cancersgynecologic cancers
Advocate for robust clinical Advocate for robust clinical trials program and expand trials program and expand access to clinical trialsaccess to clinical trials

My Gene Therapy My Gene Therapy Scientific CollaboratorsScientific Collaborators
Hopkins/UAB Cervical SPORE
UAB Ovarian SPORE

Change Must Start with Change Must Start with the Individualthe Individual
Commit to life long learning Commit to life long learning and expand your skill setsand expand your skill sets
Work smarter and critically Work smarter and critically evaluate what you are doing evaluate what you are doing
Work collaborativelyWork collaboratively Take risks – get out of your Take risks – get out of your
comfort zonecomfort zone

When you're finished changing,
you're finished.-- Benjamin Franklin

Thanks for your attention - Thanks for your attention - Questions?Questions?
Ronald D. Alvarez, MDRonald D. Alvarez, MD
University of Alabama at BirminghamUniversity of Alabama at BirminghamDivision of Gynecologic OncologyDivision of Gynecologic Oncology





























