Embed Size (px)
Citation preview
TRANSVAGINAL ULTRASOUND
Gynecology Mini-Lectures for Students
TechniqueTransvaginal Ultrasound
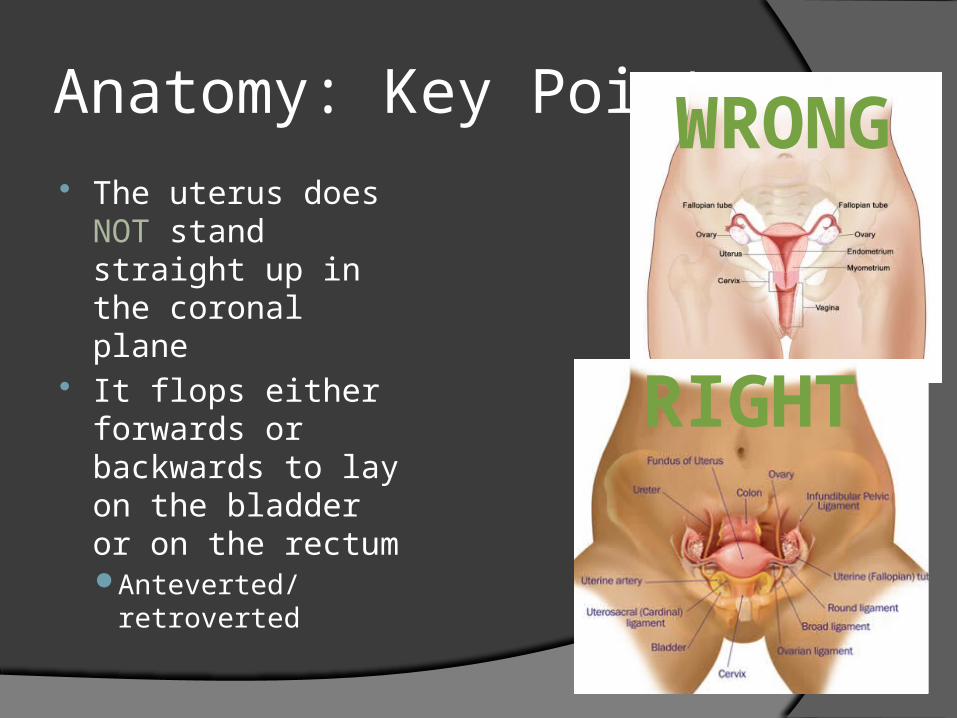
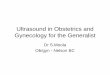
Anatomy: Key Points The uterus does
NOT stand straight up in the coronal plane
It flops either forwards or backwards to lay on the bladder or on the rectumAnteverted/
retroverted
WRONG
RIGHT
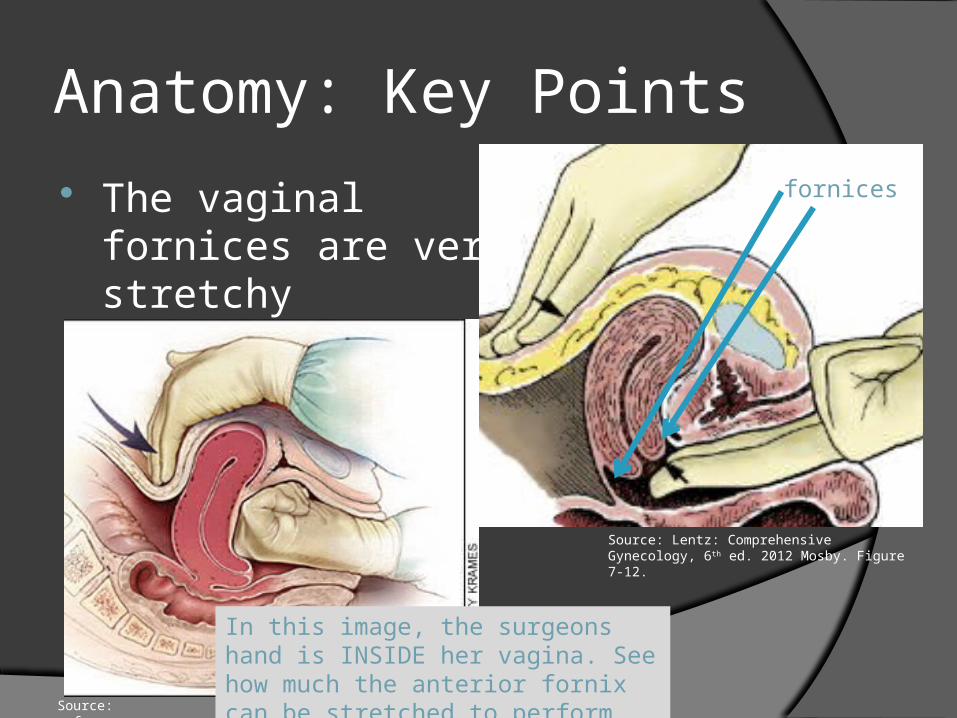
Anatomy: Key Points
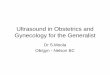
The vaginal fornices are very stretchy
Source: Lentz: Comprehensive Gynecology, 6th ed. 2012 Mosby. Figure 7-12.
In this image, the surgeons hand is INSIDE her vagina. See how much the anterior fornix can be stretched to perform bimanual massage of the uterusSource: aafp.org
fornices
Anatomy: Key Points
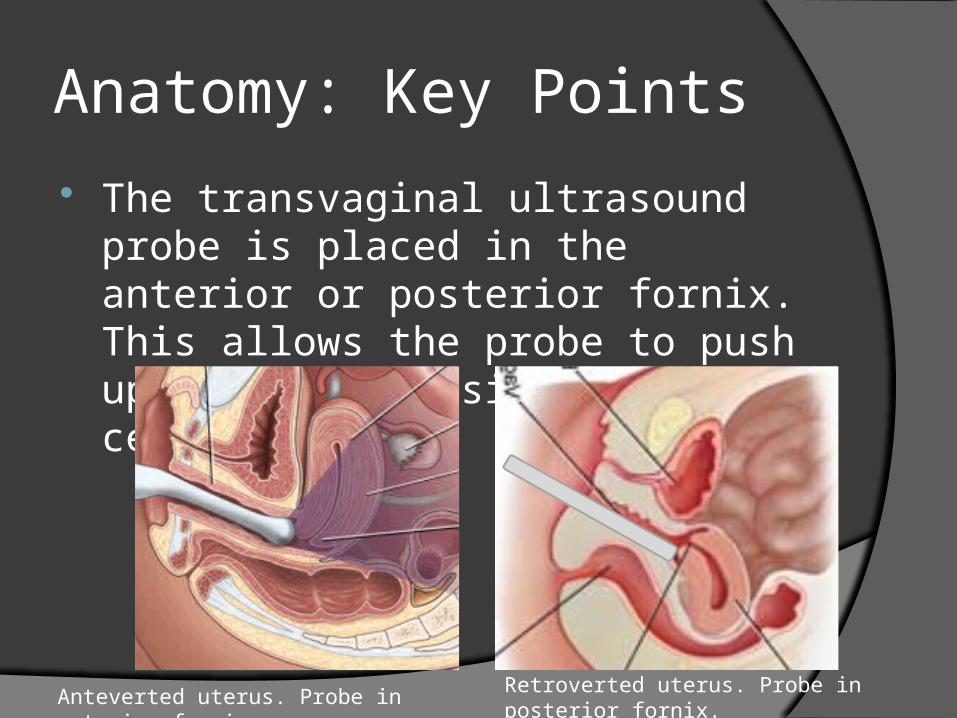
The transvaginal ultrasound probe is placed in the anterior or posterior fornix. This allows the probe to push up against the side of the cervix.
Anteverted uterus. Probe in anterior fornix. Retroverted uterus. Probe in posterior fornix.
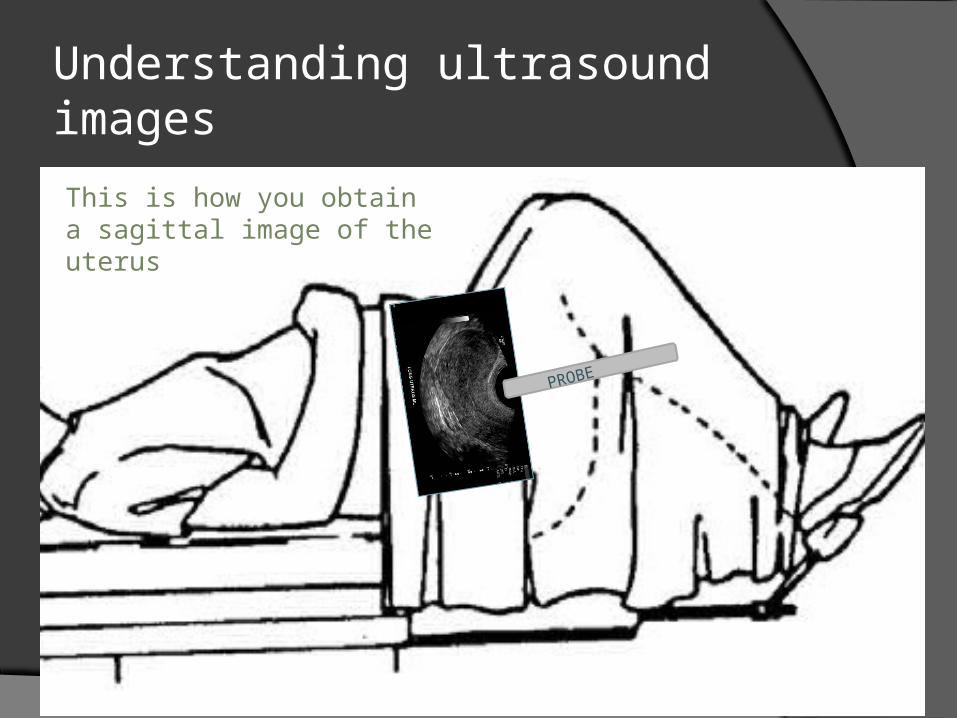
Understanding ultrasound imagesThis is how you obtain a sagittal image of the uterus
PROBE
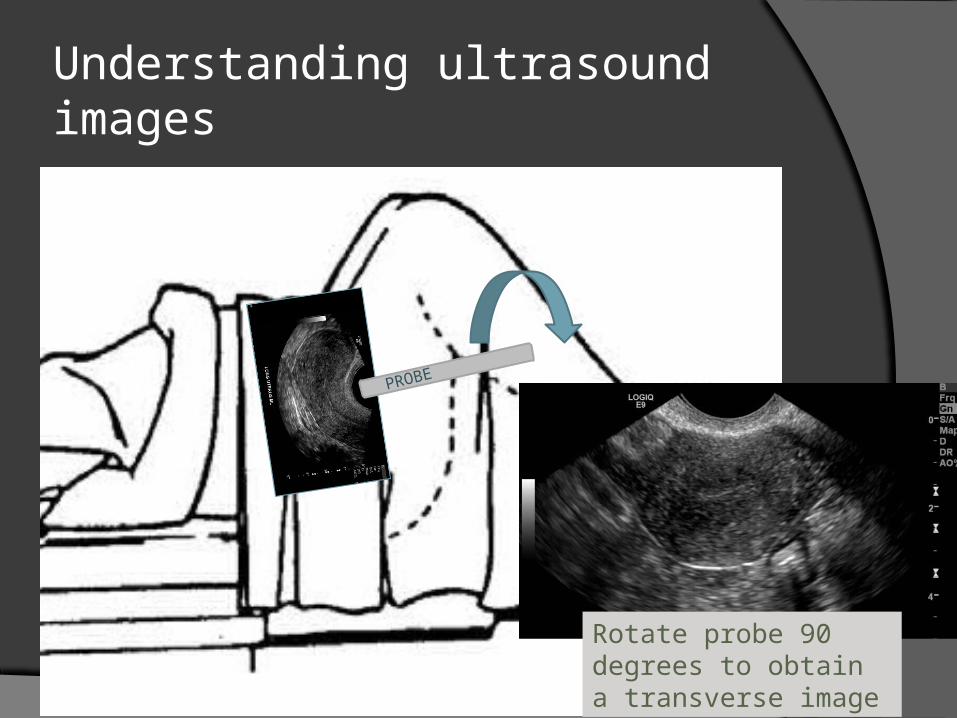
Understanding ultrasound images
Rotate probe 90 degrees to obtain a transverse image
PROBE

Understanding ultrasound images
As you can see from this image, it is impossible to obtain a “head-on” or “coronal” view of the uterus using normal transvaginal ultrasound. The probe would have to be outside the vagina.
vagina
PROBE

Understanding ultrasound images The “head-on” or “coronal” view of the
uterus can only be obtained by creating a 3D reconstruction of the sagittal and transverse images

AdvantagesTransvaginal Ultrasound
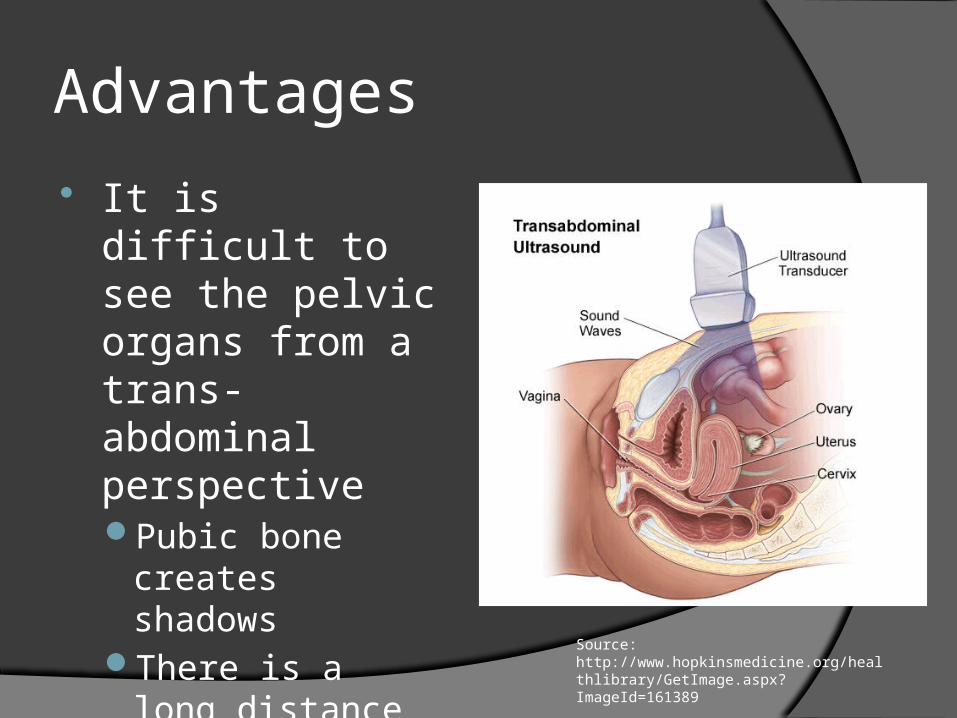
Advantages
It is difficult to see the pelvic organs from a trans-abdominal perspectivePubic bone creates
shadowsThere is a long
distance between probe and organs
Source: http://www.hopkinsmedicine.org/healthlibrary/GetImage.aspx?ImageId=161389
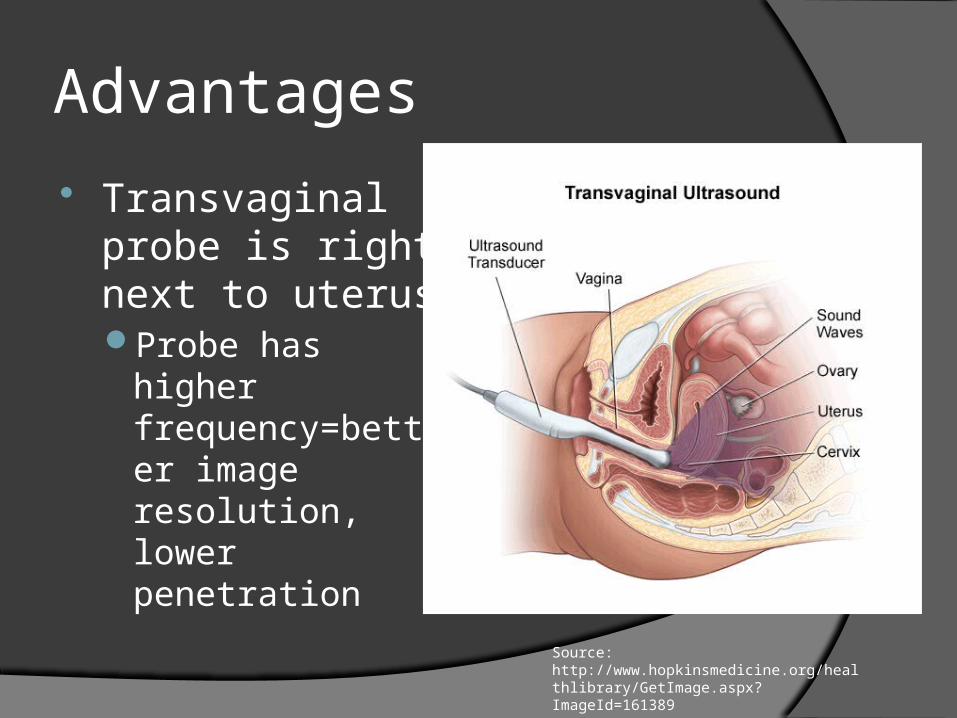
Advantages
Transvaginal probe is right next to uterusProbe has higher
frequency=better image resolution, lower penetration
Source: http://www.hopkinsmedicine.org/healthlibrary/GetImage.aspx?ImageId=161389
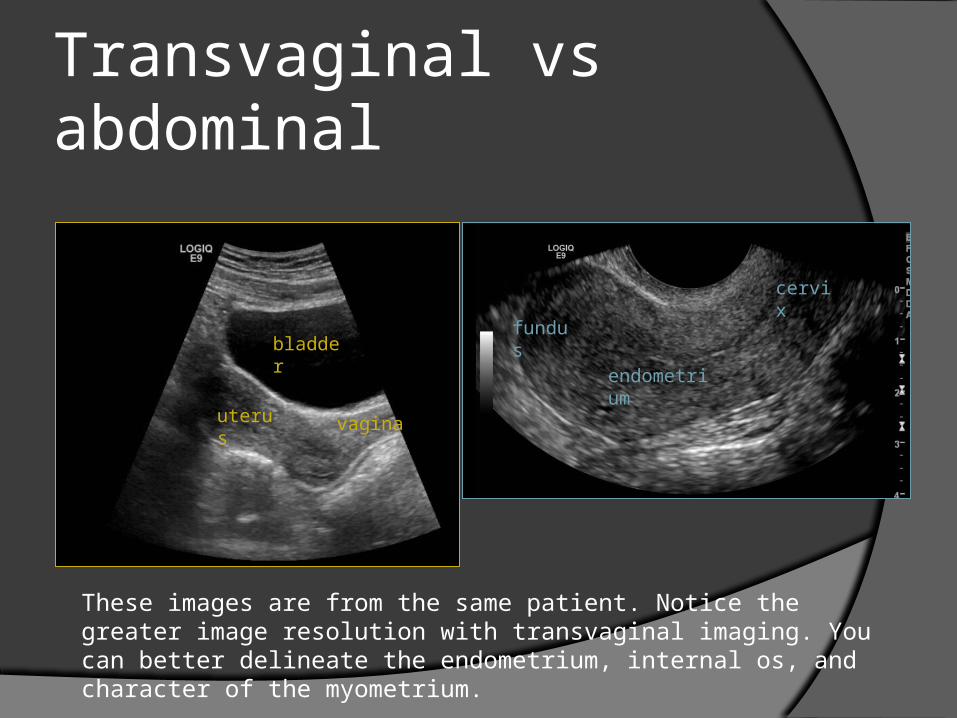
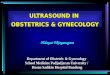
Transvaginal vs abdominal
These images are from the same patient. Notice the greater image resolution with transvaginal imaging. You can better delineate the endometrium, internal os, and character of the myometrium.
uterus
bladder
vagina
fundus
endometrium
cervix
ProcedureTransvaginal Ultrasound
Procedure
Patient should empty her bladder Patient lays in lithotomy position Gel placed on ultrasound probe
Improves transmission of ultrasound waves Sterile probe cover placed on probe Gel placed over probe cover Patient or sonographer inserts probe Images obtained

Procedure The components of a typical gynecologic
sonographic examination include:Uterine size, shape, and orientationEvaluation of endometrium, myometrium, and cervixIdentification and morphology of ovaries, if possibleAssessment of the uterus and adnexa for masses,
cysts, hydrosalpinges, fluid collectionsEvaluation of the cul-de-sac for free fluid or massesNormal fallopian tubes usually cannot be seen during
pelvic sonography
Source: UpToDate, “Ultrasound examination in obstetrics and gynecology.”
Color flow
Doppler color flow mapping uses different colors to depict the direction of flow on a real-time color image
Useful to determine:Presence of flow
○ Rule out ovarian torsionVascularity of a mass
○ Characterize the massVascularity of the endometrium/myometrium
○ Distinguish benign versus malignant conditions
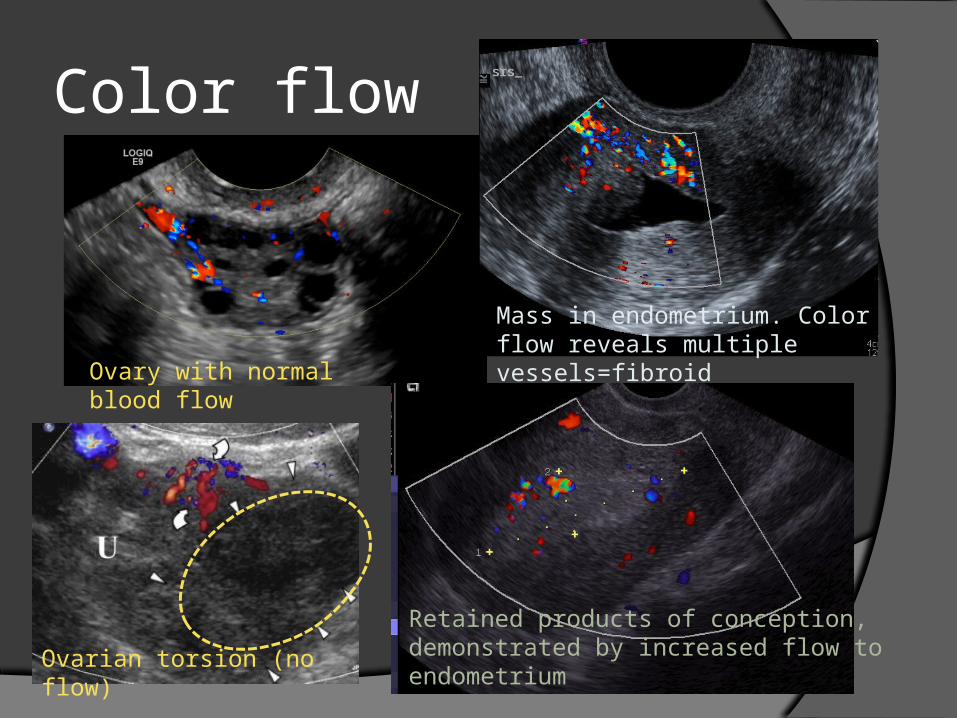
Color flow
Ovary with normal blood flow
Ovarian torsion (no flow)
Mass in endometrium. Color flow reveals multiple vessels=fibroid
Retained products of conception, demonstrated by increased flow to endometrium
IndicationsTransvaginal Ultrasound
Indications Gynecologic ultrasound examination has multiple uses,
including but not limited to:Evaluation of the menstrual cycle (endometrial thickness,
follicular development)Monitoring natural or stimulated follicular development during
infertility therapyLocalization of an intrauterine deviceEvaluation of abnormal uterine bleedingAssessment of a pelvic mass (eg, adenomyosis, fibroid,
cancer, cysts)Evaluation for sequelae of pelvic infection (eg, abscess,
hydrosalpinx)Evaluation of congenital uterine anomaliesScreening for malignancySource: UpToDate, “Ultrasound examination in obstetrics and gynecology.”