Embed Size (px)
Citation preview

Hem philiaTODAY
N e w s l e t t e r o f t h e C a n a d i a n H e m o p h i l i a S o c i e t y • W i n t e r 2 0 0 1 • V o l 3 6 N o 1
Hem philiaTODAY
I N S I D E
Until a few years ago, von Willebrand Disease (vWD),and in particular its impact on women,was littlerecognized – even among those in the bleedingdisorders community. For the next three years, withthe generous support of Aventis Behring, CHS isundertaking a major campaign aimed at increasingawareness about von Willebrand Disease amonghealth care providers and the general public. Thecampaign will kick off on April 17, InternationalHemophilia Day, with a major media blitz and localawareness activities to be presented by chapters andclinics across the country. Hopefully, as a result of ourefforts over the next three years, there will no longerbe a reason for persons to have to endure thesymptoms of untreated vWD.
This special issue of Hemophilia Today will featurea variety of topics relating to von Willebrand Diseaseincluding articles of a medical nature as well aspersonal stories of individuals from our communitywho are living with vWD.
How can I control myheavy periods?
Why do I bleedso much at thedentist?
Why do I bruise
so easily?
Why do I getso many
nosebleeds?
von Willebrand Disease…the most common bleeding disorder
you CAN stop the bleeding…
CHS launches national von Willebrand Disease Awareness Campaign
The CHS would like to express its appreciationto Aventis Behring for making this educationalprogram possible.
EDITOR’S KEYBOARD 2
PRESIDENT’S MESSAGE 3
NEWS UPDATE 4
MEDICAL NEWSVon Willebrand Disease: Diagnosis and Management of the Most Common Inherited Bleeding Disorder 5
PROFILEDr. David Lillicrap 8
THE BLOOD FACTOROctosim® Spray Available, Not Widely Used 9
THE FEMALE FACTORWomen with Bleeding Disorders in Emergency Departments 10
VWD RESOURCES 13
FAMILIES IN TOUCHA Family Profile 14New Interactive CD-ROM for Parents
YOUTH FILE 16Living with vWD
CHS HONOURS PAST AND PRESENT AWARD RECIPIENTS 18
THE GLOBAL PERSPECTIVE 20
w w w . h e m o p h i l i a . c a
(Please send any comments raised by this, or any other Editorial to the Editor,Hemophilia Today, 1409B 4th Street N.W., Calgary, AB T2M 2Y8.Or fax your comments to (403) 282-0786)
WINTER 2001 • VOL 36 • NO 1
Hemophilia Today625 President-Kennedy Avenue, Suite 1210
Montreal, Quebec H3A 1K2. www.hemophilia.ca
Phone: (514) 848-0503Fax: (514) 848-9661
Toll Free 1(800) 668-2686
Hemophilia Today is the official publication of the Canadian Hemophilia Society (CHS) and
is issued three times yearly.
The Canadian Hemophilia Society exists to improve the quality of life for all persons
with hemophilia and other inherited bleeding disorders and to find a cure.
The purpose of Hemophilia Todayis to inform the hemophilia and bleedingdisorders community about current news
and relevant issues. Publications and speakersmay freely use the information containedherein, provided a credit line including the
volume number of the issue is given. Opinions expressed are those of writers only
and do not necessarily reflect the views of the CHS.
EDITORBarry Isaac, Ph.D.
PRESIDENTErma Chapman, Ph.D.
EXECUTIVE DIRECTORDaniel Lapointe
EDITORIAL COMMITTEEClare Cecchini
Barry Isaac, Ph.D.David Page
Patricia Stewart
CONTRIBUTING WRITERSJean-Daniel Beaubien
Frank BottHeather CarlsonClare Cecchini
Karen CreightonErma Chapman, Ph.D.
Céline CyrWilliam Dutot
Barry Isaac, Ph.D.François LarocheDr. David Lillicrap
David PageRenee Paper, RNPatricia Stewart
Matt StrmicDesirée Sutton
Ania Szado
PRODUCTION COORDINATORClare Cecchini
PRODUCTION ASSISTANT AND FRENCH VERSION COORDINATOR
Hélène Bourgaize
GRAPHIC DESIGNPaul Rosenbaum
TRANSLATORSVivien Kairy
Marie PréfontaineNormand Latulippe
Marc-André Robitaille
PRINTINGBowne of Montreal
EDITOR’SKEYBOARD
Barry Isaac, Ph.D. Hem philiaTODAY
H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
Notes of a Personal Nature
This issue of Hemophilia Today deals almost exclusively with von WillebrandDisease (vWD), the nearly invisible member of the hemophilia family. It isnearly invisible because it is often mistaken for some other malady, or the
patient might feel that the bleeding episodes are not severe enough to warrantmedical attention, and so it lies hidden, sometimes for decades, sometimes forgenerations. With this issue of Hemophilia Today, and through the undertaking of amajor national awareness campaign, the CHS hopes to bring vWD into the light andthus bring a new focus on its nature and treatment. All of us at Hemophilia Today,and all of our members who have taken the time to write the articles in this issue,hope that our efforts will be fruitful and that the information now in your hands will help in bringing all those who suffer from vWD to a new understanding of theirdisorder and to new and better treatment. But your Editor has another matter that he wishes to speak about here.
It is seldom that the editorial column really does have personal opinion, even thoughthat is what it is meant to contain. More often your Editor speaks about the contentof the issue and the important issues that face the CHS from day to day.But this column is about personal matters. Last November your Editor was therecipient of the Frank Schnabel Award and he attended the Annual CHS AwardsBanquet, held in one of the prettiest resorts imaginable, the Briars on Lake Simcoe in Ontario. Upon receiving the award, your Editor gave what may have been one ofthe shortest “thank you” speeches on record. If truth be known, your Editor wasovercome with emotion and barely even able to say a minimal “thanks”. For that he apologizes deeply.
For the record, the Editor would like to repeat what he did say and expand his thanksto all members of the CHS. Two individuals have always stood at your Editor’s side ashe has tried to do the tasks for which he volunteered: Joan Isaac and Clare Cecchini.Joan has supported your Editor for more than 34 years, and Clare must often feel thatit has been that long for her as well. Whatever your Editor might have done for theCHS over the years, he owes a huge debt to Clare, who has the patience of Job and aboundless heart. Others, too, have been helpful and supportive over the years, HélèneBourgaize, Robert St-Pierre, Pierre Latreille, Lindee David and Bob Shearer. Hélèneand Robert are the only ones still with the CHS office staff, and one of the manythings your Editor sincerely misses because he is no longer on the CHS Executive isworking directly with them. They are wonderful people, generous in nature and wisefar beyond their years. Your Editor still misses Pierre Latreille, a man of wise andquiet counsel, who passed away at a shockingly early age.
But most of all it has been the work and aid of literally dozens of volunteers fromevery province in the nation to which your Editor feels indebted. He is constantly inwonder at the courage and determination you all show in your daily lives and the wayyou manage your hemophilia. It is this courage, this determination, this ability tolaugh in the face of constant threats that often gives your Editor the means to get onin his own life and tasks. People like you give our Editor strength to accomplish thetasks for which he was awarded the Frank Schnabel Award. Thank you all for being sosupportive, kind and helping over the years. And thank you for letting your Editor sayhere what he could not at the Awards Banquet owing to a surplus of emotion.

PRESIDENT’SMESSAGE Erma Chapman, Ph.D.
H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
n writing this last message toyou as President of the CanadianHemophilia Society, I looked to
my first message (Fall 1998) forinspiration. While the issues that wereof interest to us then bear an amazingsimilarity to those of today, the way weoperate as an organization has changedover the past three years.
Compensation for all Canadiansinfected with HCV through theblood system remains a priority forthe CHS. At the time that I amwriting my message, I have reasonto hope that an equitable solutionwill be found in the near future.
Canadian Blood Services andHéma-Québec have focused onsafety as the blood serviceinstitutions in this country. Whilewe have at times struggled with ourpartnerships with theseorganizations, we continue tomaintain an open dialogue towardsthe shared goal of a safe andefficacious blood system in thiscountry. Our position as awatchdog of the blood system wasreinforced at our January 2000strategic planning meeting. As Inoted in my first message to you,however, we can never againcompletely trust.
Care and treatment of people withbleeding disorders have remained ourfocus. Beginning with the “WinnipegII” meeting of April 1998, we haveworked with the Association ofHemophilia Clinic Directors of Canada(AHCDC) and Canadian Association ofHemophilia Nurses to establishstandards of care across the country.A clinic in Saskatchewan appearsimminent, and strides have been madein other areas to enhance clinicalservices. We have dealt with thepresence of CJD, and welcomed theintroduction of second-generation
recombinant products. Volunteers andstaff members have developed programinitiatives in the areas of inhibitormanagement, a CD-ROM format forinformation designed to assist parentsof newly-diagnosed children, improvedaccess to appropriate care in emergencyrooms, and services for women with
bleeding disorders.Currently, a majorinitiative is underwayto ensure theappropriate diagnosisand treatment of vonWillebrand Disease.
The opportunityto work with theWorld Federation ofHemophilia inplanning for theWorld Congress ofHemophilia inMontreal wasunique. Our CHSvolunteers wereamong the stars ofthe Congress lastsummer. The youthexperience was notonly successful forthe Congress, but hasrevitalized youth
initiatives within the CHS. As well, theCHS has been able to establish a fundfor international projects thanks to therevenue from the Congress. The CHSwas also represented in the planning ofthe first global forum on the use ofhemophilia products, held in Montrealduring April 2000.
Research is the hope of every personwith a bleeding disorder for a betterlife, and will remain a priority for theCHS. A positive and productiveworking relationship with theHemophilia Research Million DollarClub has helped to generate anincreased funding base for research
towards a cure, and the promise of evengreater research revenue over the nextthree years. This past year, the CareUntil Cure research fund wasintroduced along with the AventisBehring – CHS-AHCDC Fellowship inHemophilia. In addition, we have hadincreased opportunities to participatein priority-setting and researchinitiatives with the AHCDC, HealthCanada and the Laboratory Centre forDisease Control.
A new vision for resourcedevelopment within our organizationopens opportunities for morediversified funding sources, as well as opportunities for volunteerdevelopment. A Chief DevelopmentOfficer has been added to our staffingcomplement. Over the next month, staffpositions will be added in Saskatchewanand in the Maritime Region.
Much of the success of the pastthree years can be attributed toteamwork within the CHS. We haveforged a new way of working together,between volunteers and staff members,and among national, chapter andregional levels of the organization. Wehave developed a shared strategic visionfor people with bleeding disorders andtheir families, and have ensured thatorganizational structures are in place tosupport the realization of our dreams.
During my time as President, I havehad the chance to work with threeremarkable executive directors. LindeeDavid’s knowledge of bleedingdisorders and blood systems wasmatched by her passion for justice, hercaring for others and her hearty laugh.Pierre Latreille’s quiet reassuranceprovided me with the direction andconfidence to fulfill my leadershipresponsibility; I still grieve his passingand miss his gentle guidance. DanielLapointe brought a wealth of non-profit management knowledge, skillsand experience to the position. Hispassion for excellence, belief incollaboration, and ability to developeffective partnerships are qualities I willcontinue to treasure.
It has been a privilege to meet andshare with so many members across thecountry. And it has been an honour toserve as President of such a dedicatedgroup of volunteers and staff.
Thank you, and farewell,Erma Chapman, Ph.D.
Final thoughts…Much of the success of the past three years can be attributed toteamwork within the CHS. We have forged a new way of working together, between volunteers and staff members, and among national,chapter and regional levels of the organization.
I
Careand
treatmentof people
withbleedingdisorders
haveremainedour focus.
SHARE IDEAS, TAKE ACTIONA three-track program that will include :
BASIC AND CLINICAL SCIENCEPUBLIC HEALTH
SOCIAL SCIENCE AND COMMUNITY
Organized by the Canadian Hemophilia Society,
in partnership with :Canadian Association for the Study of the Liver
Hepatitis C Society of CanadaCanadian Liver Foundation
Canadian Public Health AssociationCanadian Centre on Substance Abuse
Prisoners with HIV/AIDS Support Action NetworkHepatitis C Division, Health Canada
This conference has been made possiblethrough the exceptional support of
For information or registration :1ST CANADIAN CONFERENCE ON HEPATITIS C
CONFERENCE SECRETARIATTelephone : 1-866-420-1684
Fax : (514) 848-9661E-Mail : [email protected] Web Site : www.hepc1conf.ca
NEWSUPDATE
H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
◗ First Care Until Cure ResearchGrants Awarded
CHS and Genetics Institute are pleased toannounce the first recipients of the newlyestablished research program aimed atimproving the qualityof life of personsliving withhemophilia oranother inheritedbleeding disorder.Congratulations to thefollowing recipients:
Recipient: Dr. Georges-Étienne RivardNames of Co-investgators: Dr. Rochelle Winikoff
Dr. Patrick St-LouisDr. Claire Infante-Rivard
Project Title: Von Willebrand Factor and PhysicalExercise
Recipient: Dr. Jenny HeathcoteNames of Co-investgators: Dr. Jerome Teitel
Dr. Ignatious FongProject Title: Therapy for Patients with Congenital
Coagulation Disorders with Hepatitis Cwith or without HIV co-infection
Recipient: Dr. Manuel CarcaoNames of Co-investgators: Dr. Brian Feldman
Dr. Victor BlanchetteDr. Paul OhDr. Paul BabynDr. Douglas Hedden
Project Title: A Prospective, Randomized Trial toCompare Two Regimes of Prophylaxisin Older Boys with Severe Hemophilia A
Applications for the second year of theCare Until Cure Research Program willbe available in May. For further infor-mation please contact the National Office.
◗ CHS Scholarship & BursaryProgram
Applications for the 2001 CHS Scholarshipand Bursary Program are now available atchapters, clinics and national, provincial,and regional offices. The deadline forsubmitting applications this year is April30, 2001. Recipients will be notified in May.
◗ Three Canadian Winners inNational Art Contest
Three of the winners in the Aventis Behring2001 Calendar Contest were from theCanadian bleeding disorders community.Annette Kavelaars-Burrows of London,Ontario was awarded First Prize for herartistic depiction of living with a bleedingdisorder. Christine Czipf of Thunder Bay,Ontario was awarded Grand Prize for herartistic photograph depicting the journey ofher two daughters Olivia and Jacklyn asthey move down the path of life. AndTimothy Glazebrook, age 6, of Greenwood,Nova Scotia was awarded First Prize for hisartistic depiction of nature’s beauty.Contratulations to the recipients.
◗ RCMP Investigation intoDestruction of Documents
The RCMP announced on February 26,2001 that no charges would be laidregarding the destruction of CanadianBlood Committee documents. TheRCMP confirmed that audio recordingsand verbatim transcripts of the now-defunct federal-provincial governmentcommittee’s meetings from 1982 to 1989had been destroyed, but announced thatthey could not determine if this was donewith criminal intent. CHS remainsoptimistic that the RCMP will uncover thetruth in the larger investigation regardingpotential criminal wrong doing that led tothe contamination of Canada’s bloodsupply.
◗ Manitoba Government ExtendsCompensation
On January 19th the ManitobaGovernment announced their decision tooffer compensation to hepatitis C victimswho were infected through bloodproducts received either before 1986 orafter 1990. Manitoba joins Ontario andQuebec in announcing financial assistanceto victims in their province who were leftout of the 1986-1990 Hepatitis CCompensation Agreement. Manitoba and Quebec are providing a lump sumpayment of $10,000 and Ontario isproviding $25,000 to all individualsinfected with hepatitis C prior to 1986 orafter 1990. CHS continues its efforts toconvince the federal government and theseven remaining provinces to follow theleadership shown by Ontario, Quebec andManitoba and compensate all victims ofthis tragedy.
◗ Canadian Red Cross SocietySettlement Denied
On February 20, 2001 Justice Winklerdenied approval of the proposedCRC settlement. The CHS believes thatthis recent event illustrates once morehow the extension of the 1986-1990Hepatitis C Compensation Package to allvictims of tainted blood remains the bestway to respond to the needs andexpectations of those victims who are stillwaiting for compensation. CHS hasreason to hope that the federalgovernment may reconsider its positionand accept to extend the 1986-1990package to those infected outside of thisperiod in light of recent evidence showingthat approximately 5,000 victims arepresently excluded, a number considerablylower than previous projections.
11STCANADIAN CONFERENCEON HEPATITIS C
M a y 1 - M a y 4 , 2 0 0 1H I L T O N M O N T R É A L B O N A V E N T U R E
NOTICE
The Annual General Meeting of the CanadianHemophilia Society will convene as follows:
Saturday, May 26th 2001 at 9:00 a.m.at the Sheraton Hotel in Halifax, Nova Scotia
1. To acknowledge the designated Directors ofeach Chapter;
2. To acknowledge the Elected Directors at Largefor 2001-2002;
3. To receive the audited financial statements of theCanadian Hemophilia Society for the year endedDecember 31, 2000;
4. To appoint an auditor for the ensuing year;5. To approve the proposed revised by-laws
(Copies of the proposed revised by-laws areavailable at the CHS Office. To obtain a copy prior to the AGM please call 1-800-668-2686;
6. To transact such other business as may properlycome before this Annual General Meeting of themembers of the Canadian Hemophilia Society.
Ron MacLeodSecretary

H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
MEDICALNEWS
Von WillebrandDisease: Diagnosisand Management ofthe Most CommonInherited BleedingDisorder
Dr. David LillicrapProfessor, Departments of Pathology andMedicine, Queen’s University
Seventy five years ago, Dr. Erik vonWillebrand first described aninherited bleeding disorder that
manifests as excessive bleeding frommucous membranes and into the skinin a large family in the Aaland Islands in Scandinavia. The index case in his studies, a 14 year old girl, subsequentlydied as a result of excessive bleedingassociated with menstruation. The con-dition described by Dr. von Willebrandnow bears his name and is recognizedas the most common inherited bleedingdisorder known in humans.
Introduction to von Willebrand Disease
Over the past decade, with theincreasing realization that vonWillebrand Disease (vWD) was not arare condition, but in fact a very com-mon, usually mild, bleeding disorder,interest in the diagnosis and improvedclinical management of the conditionhas increased significantly.Furthermore, recognition that themajor health problem associated withvWD is heavy bleeding associated withmenstruation, has also begun to affectthe practice of gynecologists and familyphysicians who see large numbers ofwomen with this concern.
The primary abnormality in vWD
involves the deficiency or abnormalfunction of a large protein, vonWillebrand Factor (vWF), that is pro-duced by the lining cells of blood vessels(endothelial cells) and by the parentcells of blood platelets (megakary-ocytes). Von Willebrand Factor isrequired for two essential componentsof the normal blood clotting process.The protein acts as an adhesive bridgeto bind blood platelets to the site ofblood vessel damage and secondly,serves as a carrier for Factor VIII in theblood. Without normal levels of vWF,Factor VIII is rapidly cleared from theblood, resulting in a significant second-ary deficiency of this critical blood clot-ting factor.
Studies performed in Europe andNorth America indicate that as many as1% of the population may have clinicalsigns, and laboratory test results areconsistent with a diagnosis of vWD. Inmany of these subjects, the clinical evi-dence of bleeding may be subtle andamount to no more than a tendency tobruise easily or to experience recurrentnose bleeds. Nevertheless, even thoughtheir tendency to bleed spontaneouslymay be minor, these individuals may beprone to a significantly greater risk ofexcessive post-operative and post-trau-matic bleeding. Despite the fact that weare now fairly confident about the highprevalence of this condition, we need tounderstand a great deal more about whythe disorder is so common.
The Diagnosis of von Willebrand Disease
A diagnosis of vWD requires consid-eration of three factors: a personal history of excessive bleeding, a familyhistory of excessive bleeding and labo-ratory test results of blood clotting thatare consistent with vWD.
In the vast majority of vWD cases,the spontaneous bleeding tendency islimited to excessive blood loss into theskin (easy bruising and prolongedbleeding from cuts) or from mucusmembranes (nose bleeds, bleeding fromthe bowel and menstrual bleeding).However, in a rare, severe form of thedisorder (Type 3 vWD), spontaneous
bleeding also occurs into muscles andjoints as is seen in severe hemophilia.Excessive and prolonged bleeding is alsofrequent after dental work and otherforms of surgery. For a physician tomake a diagnosis of vWD, it is extreme-ly important for them to be able toobtain a detailed bleeding history fromwhich they can evaluate the extent ofthe bleeding problem. A history of nosebleeds or bruising is not uncommon inthe general population, and only adetailed assessment will identifywhether the extent of bleeding warrantsthe type of laboratory evaluationrequired to make a diagnosis of vWD.
CLINICAL SIGNS AND SYMPTOMS OF VON WILLEBRAND DISEASE
• Easy bruising• Frequent and prolonged nose bleeds• Prolonged bleeding from cuts• Heavy menstrual bleeding• Prolonged and excessive bleeding
following dental work and surgery
Von Willebrand Disease is an inher-ited disorder and, as such, there shouldbe other people within the patient’sclose family with the condition. As thegene that directs production of vonWillebrand Factor is located on chro-mosome 12, and everyone receives twochromosome 12s, one from each parent,this bleeding disorder, in contrast tohemophilia, manifests in equal numbersof males and females.
Most forms of vWD have a so-calleddominant mode of inheritance, wherebyonly one (of two) copies of the vonWillebrand Factor gene needs to beabnormal to lead to the clinical mani-festations of the disease. Thus, for manypeople with vWD, one of their parentswill have signs of excessive bleeding andthere may be other siblings with a simi-lar history. However, one of the factorsthat complicates our understanding ofthis condition is a phenomenonreferred to as incomplete penetrance.This circumstance results in many people that have inherited the vWDgene not showing any clinical manifes-tations and thus a family history for thecondition is hidden.
The condition described by Dr. Erik von Willebrand now bears his name and is recognized as the most common inherited bleeding disorder known in humans

H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
Laboratory Tests forvon Willebrand Disease
Once there is a clinical suspicion ofvWD from the clinical and family histo-ry, a standard set of laboratory investi-gations should be ordered to confirm orrule out the diagnosis. These laboratorytests range from a basic blood count,from which the physician can assess thepatient’s hemoglobin and platelet count,to relatively sophisticated studies of thestructure of von Willebrand Factor(vWF) in the blood. The most importantof these studies are measurements of theclotting Factor VIII level (Factor VIII iscarried in the blood by vWF), a meas-urement of the amount of the vWF pro-tein in the blood (the vWF antigen:vWF:Ag) and a determination of thefunctional activity of the vWF (the risto-cetin co-factor: vWF:RCo). In most typesof vWD, these laboratory tests will showa significant reduction in vWF andFactor VIII from that seen in the bloodof normal subjects.
LABORATORY TESTS FORVON WILLEBRAND DISEASE
• Von Willebrand Antigen (VWF:Ag)Measures the amount of vWF proteinin the blood.
• Von Willebrand Factor RistocetinCo-factor (VWF:RCo)Measures the function of the vWF
• Factor VIII clotting activity (FVIII:C)Measures the amount of factor VIIIbeing carried by vWF
• Von Willebrand Factor MultimerAnalysisDetermines the structure of vWF in the blood. Usually abnormal in Type 2 vWD
These tests can all be performed on asingle blood sample, but, because sever-al of the tests are time consuming andcomplex, most laboratories collect sam-ples to perform the tests in batches acouple of times each month. The resultsof these tests will show one of severaloutcomes. They may show unequivocalevidence of vWD and the diagnosis isthus confirmed. However, even if theseinitial tests are positive, the physicianwill need to sub-type the disorder intoone of the three major categories ofvWD, types 1-3. This will require some
additional laboratory tests (such as thevWF multimer analysis) that can usual-ly be performed on the same bloodsample that was used for the initialdiagnosis, and again, these tests usuallytake at least a couple of weeks to com-plete. Sub-typing of vWD is necessaryto develop the most effective plan forprevention and treatment of bleeding invWD because we know that the thera-peutic responses of the sub-types varysignificantly for certain forms of treat-ment.
SUB-TYPES OF VON WILLEBRAND DISEASE
Type 1 vWD~ 85% of all cases.
Mild/moderate reduction in vWF and Factor VIII levels.
Type 2 vWD~ 15% of all cases.
Production of functionally abnormalvWF.
Type 3 vWD~ 50 cases in Canada.
Total absence of vWF from the blood.Severe clinical disease.
Asecond potential outcome fromthe initial set of laboratory studies is that the test results are
“borderline” or normal. In this instance,the physician will need to re-evaluatethe clinical bleeding history and, if thisstill appears to be excessive, they willvery likely ask for a repeat set of tests tobe performed. Unfortunately, this cir-cumstance is not unusual in attemptingto make the diagnosis of vWD. Theblood levels of vWF and Factor VIII arewell known to fluctuate over time, andunless testing has been repeated at leasttwice (and some physicians will ask forthree sets of tests) the diagnosis of vWDcannot be ruled out with confidence insomeone with a significant bleeding his-tory. Even after several sets of tests,some individuals still show “borderline”values for vWF and Factor VIII. Thesepeople may be told that they probablyhave vWD and that at the current timeno additional studies can clarify this sit-uation. These observations emphasizethat the major problems in dealing withvWD are the initial consideration of thecondition as a diagnostic possibilityand, probably most difficult of all, con-firming the diagnosis.
The Prevention and Treatment ofBleeding in von Willebrand
Disease
In contrast to the challenges in making the diagnosis of vWD, the treat-ment of this condition is effective andrelatively straightforward. Apart fromthe very few individuals with the severetype 3 form of the disorder, mostpatients with vWD do not require regu-lar treatments with transfusions. For thepast 20 years the mainstay of treatmentin most vWD patients has been the useof the drug Desmopressin (chemicalabbreviation DDAVP). This drug iseffective in the prevention or treatmentof bleeding in approximately 80% ofpatients with vWD. Desmopressinworks by inducing the release of vWFfrom stores of the protein that aremaintained in the cells in which it isproduced. In most patients, a treatmentof Desmopressin will increase the bloodlevel of vWF (and Factor VIII) by 3 to5-fold over the baseline values, at onehour after administration. The drug is
usually given by intravenous or sub-cutaneous injection, but a new concen-trated form of Desmopressin, adminis-tered as an intranasal spray, has alsorecently been introduced. The adminis-tration of Desmopressin is sometimesaccompanied by mild side effects thatmay include some facial flushing andsmall transient changes to the pulse andblood pressure. In contrast, the seriousside effect of seizure induction, isextremely rare and can be effectivelyprevented by limiting fluid intake in the24 hours after Desmopressin treatment.These issues are routinely discussedwith patients by their physician or nurseco-ordinator at the time of drug admin-istration. Desmopressin is a safe andvery effective treatment for the preven-tion of bleeding at the time of dentalwork, minor surgery and for minor ormoderate bleeding episodes. It can also
In contrast to the challenges
in making the diagnosis of
vWD, the treatment of this
condition is effective and
relatively straightforward.
H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
to investigate the underly-ing genetic changes in thecommon type 1 form ofvWD. Over the next year,patients with type 1 vWDwill be approached by clin-ics to invite their participa-tion in this study, in whichthe vWF gene will be ana-lyzed in over 100 familieswith this form of the disor-der. It is hoped that thisstudy, in conjunction witha similar research project
ongoing in 7 European countries, willimprove the complex and often unre-solved diagnostic strategies currently inuse for this subtype of vWD.
Canadian Type 1 von WillebrandDisease Research Project
Funded for 3 years from the CanadianInstitutes of Health Research
Objective: To determine the geneticchanges associated with Type 1 vWD and,in doing so, to improve the diagnostic efficiency for this disorder
Study Plan: To perform coagulation andgenetic testing on 150 families withproven Type 1 vWD
If you have Type 1 vWD and are interested in participating in this project, please speak to the staff atyour local Hemophilia Clinic.
Concluding Remarks
There is now uniform agreementthat vWD represents the commonestinherited bleeding disorder in humans.Although in most instances the disorderdoes not result in major spontaneousbleeding, it does produce long-termproblems in menstruating women andcan result in significant and prolongedbleeding after dental work and surgery.Confirming the diagnosis of vWDremains a difficult challenge in manycases, but once the diagnosis has beendocumented there are several safe andvery effective means of preventing andtreating bleeding. Future research willhopefully further enhance the choice oftreatment options for vWD and alsoprovide a more effective means ofestablishing the diagnosis.
– Raises vWF and Factor VIII levels by 3 to 5-fold in ~80% of patients
– Plasma-derived vWF concentrate for treatment of major bleeding
– Useful in treating heavy menstrual bleeding and for prevention of bleedingwith dental work and minor surgery
• Desmopressin (DDAVP)
• Humate-P
• Hormones (oral contraceptive) and clot stabilizing drugs (Cyklokapron and Amicar)
Treatment Options for von Willebrand Disease
be used to reduce heavy bleeding associ-ated with menses.
For the treatment of more seriousbleeding episodes and in patients thatrespond inadequately to Desmopressin,a von Willebrand Factor concentrate,derived from plasma, is available fortransfusion. The most frequently usedconcentrate for this purpose is Humate-P, which has been shown in studies,both in Canada and elsewhere, to besafe (no evidence of virus transmission)and very effective at replacing vWFfunction in the clotting process.
Overall, vWD produces more long-term problems in menstruating womenthan any other patient group. Studiescompleted recently in both Europe andNorth America have indicated that 10-20% of women with excessive menstrual bleeding have vWD andwould clearly benefit from the treat-ment of this disorder. In this clinical situation, many health care centers arenow beginning to initiate programs thatprovide combined hematologic andgynecologic expertise. This will enablewomen with a diagnosis of vWD toreceive the best advice concerning theuse of hormone treatments (forms ofthe oral contraceptive) and clot stabiliz-ing drugs (e.g. Cyklokapron andAmicar) that are among the most effec-tive methods of treating this problem.
Von Willebrand Disease Projects in Canada
There are several ongoing efforts inCanada that relate directly to the diagnosis and treatment of vWD.
CHS National Awareness Campaign
The Canadian Hemophilia Society isin the first year of a three year project toraise public and physician awareness
about vWD. This project will involveextensive media communications and avariety of targeted educational eventsthat will re-introduce the current concepts of vWD diagnosis and management to gynecologists and family physicians.
CHS has established an advisorycommittee composed of physicians,nurses and consumers to provide guid-ance into the planning and implemen-tation of the project.
CHS has hired a part-time publicrelations consultant, Natalie Byk, tocoordinate the awareness campaign.
Association of Hemophilia ClinicDirectors of Canada Sub-committees
• AHCDC Women’s BleedingDisorders Scientific Sub-committee
• AHCDC von Willebrand DiseaseScientific Sub-committee
The hemophilia physician’s group,the Association of Hemophilia ClinicDirectors of Canada (AHCDC), nowhas two scientific sub-committees thatare dealing with issues concerningvWD. A recently formed “Women’sBleeding Disorders” sub-committee(Chairperson, Dr. Christine Demers)will be addressing vWD problems thatare exclusive to women, while the pre-existing vWD sub-committee(Chairperson, Dr. David Lillicrap) isinvolved in several long-term studies ofvWD. These projects include the main-tenance of a Canadian vWD Registry inwhich anonymous, encrypted data hasbeen collated on over 800 vWD patientsbeing followed by CanadianHemophilia Clinics. The other majorproject that this Group is embarking onis a three year study funded by theCanadian Institutes of Health Research
H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
hemophilia, combined with the discov-ery of the factor VIII gene in 1984 allmade for a serendipitous moment inDr. Lillicrap’s life. “I was terribly lucky,”he says, to have been in the right placeat the right time, working with the rightpeople. One cannot help but wonder ifthis really was luck, or was it, like somany other “lucky” events, the result ofhard work and intense curiosity.
Dr. Lillicrap’s current research inter-ests in the genetics of von
Willebrand Disease have naturallygrown out of his work in clinical andresearch medicine. But his work doesnot stop there, as he is also working ongenetic therapy for factor VIII hemo-philiacs. He feels that this may be avail-able on a small scale in five or six yearsbecause the factor VIII gene is “middleaged,” its genetic structure having beenknown for some 15 years. Factor VIIIhas been around quite a while as amodel for a genetic disease, andadvances in its therapeutic use shouldnot be long in arriving. “We’re busy,” hesays enthusiastically, remarking that it isan “exciting time” to be working inthese fields and on these projects. Thetherapy will consist of injections of adead virus that will carry the factor VIIIgenetic material and allow it to be pro-duced in the patient’s body and thusprovide the missing clotting factor. ButDr. Lillicrap advises that the first factorto be made available through gene ther-apy in all likelihood will be factor IXsimply because of its relatively smallsize. Dr. Lillicrap has been and isuniquely and fortunately situated forresearch into both factors as Dr. Giles’animal colony afforded “an extremelyvaluable model,” he says.
When asked what has been thegreatest advance in care for
hemophiliacs, Dr. Lillicrap quicklyreplies, “the genetic revolution.” Boththe diagnosis and treatment of the disorder have been made more effectiveand safe by developments in genetictherapy and research. It is now easier todiagnose the disease and to treat it withgenetically recombinant clotting agents,which are far safer than simple humanclotting agents, all as a result of thegenetic revolution. But “the icing on thecake,” says Dr. Lillicrap, will be genetherapy for hemophilia. In fact, it willbe easier to “sell the human genomeproject,” says Dr. Lillicrap, once aneffective genetic therapy is developedfor hemophilia. That project, now in itslate stages, is a map of the entire humangenetic content, a description of thecomplete human genetic picture. Oncethis project is complete, it should bepossible to provide genetic therapy forany disease the human organism has.That is the current research thought onthe subject.
Beyond these steps, Dr. Lillicrap feelsthat the future holds some answers toquestions that currently puzzleresearchers, questions such as, why doestype I von Willebrand Disease occur? He also suggests that some advances intreatment, such as a “super factor VIII”and an increase in the half life of clot-ting factors, will be available “withintwo to three years.” Advances such asthe “super factor VIII” will result fromusing types of the molecule other thanthe normal one, once again a product ofthe genetic revolution.
Dr. Lillicrap’s enthusiasm andwarmth makes anything seem possible,and we are once again most fortunatethat he, like so many other care giversand researchers, has chosen Canada ashis home, a home for both his familyand his research interests.
by Barry M. Isaac, Ph.D.
Born in the United Kingdom, Dr.David Lillicrap received his med-ical education at St. Mary’s
Hospital Medical School, University ofLondon, the very place where Dr.Fleming discovered the “miracle” drug,penicillin. But his interest in medicinewas sparked years earlier by an aunt,Muriel Roffey, who was a Nursing Sisterand who served as Dr. Lillicrap’s rolemodel. He says that, like her, he “waslucky; I never wanted to do anythingelse” than medicine, and this was rein-forced each year when he and his familywould make a Christmas visit to hisaunt at the hospital where she worked.This early interest was married to adesire to know the puzzles as to how thehuman organism works: “I was alwayscurious – wanted to know the answers.”And Canada was the eventual luckynation to benefit from his curiosity anddesire to know how the human genomeworked.
Dr. Lillicrap moved first toEdmonton and the University ofAlberta in 1978, but then moved toQueen’s University, Kingston, Ontario,in 1980. Dr. Lillicrap has lived inKingston since then with his wife, Mary,and 3 children – Tim, (19) Kate, (18,)and Anna (16).
He says that he moved to Queen’s to“avoid” the subject of blood clot-
ting, but that he came under the wingof Dr. Alan Giles, already doing ground-breaking work with his colony of hemo-philiac dogs. His interest in Hematologyhad grown since medical school wherehe discovered that it was a fascinatingblend of clinical and laboratory sci-ences, offering challenges in bothpatient care and laboratory research inunique ways. So Dr. Giles’ interest inhemophilia, the colony of hemophiliacanimals, Dr. Lillicrap’s interest in factorVIII, first realized when he worked withDrs. Arthur Bloom and Ian Peake on
ProfileDr. David Lillicrap
Dr. Lillicrap’s current researchinterests in the genetics of vonWillebrand Disease have naturallygrown out of his work in clinicaland research medicine.
H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
BLOODFACTOR
Octostim® Nasal Spray comes in aspray pump bottle with 25 doses. Asingle treatment usually involves 1dose sprayed into each nostril. Thetreatment has been proven effective ina number of situations including
minor surgery, dentalwork, menorrhagia,nosebleeds, bleedingin the mouth, musclebleeds and jointbleeds. Because it isso easy to administer,people quickly learnhow to use the prod-uct at home. Thismeans many fewertrips to hospital or tothe doctor.Octostim® NasalSpray is regularly pre-scribed by physiciansacross Canada’s net-work of HemophiliaTreatment Centres.
Octostim® NasalSpray can be used forchildren as young as1 year of age.
The drug is notwithout side effects.It causes the body to
retain water. Consequently, peopletaking desmopressin are advised todecrease their intake of fluids. This isespecially important for young chil-dren and older people. Other sideeffects can include flushing,headaches and sleepiness. People witha history of high blood pressure orthrombosis (blood clots) may not beable to take desmopressin.
One reason why Octostim® NasalSpray has not achieved wide accept-ance is the cost. One spray pump bot-tle of 25 doses, or 12 treatments, costsalmost $400. Some provinces cover
the cost of the drug for people receiv-ing social assistance. Also, people withprivate drug insurance plans can get alarge percentage of the bill paid.However, this leaves many peopleacross the country with no coverage.Some cannot afford the high cost.
Tom Alloway, CHS Vice-president,told Hemophilia Today, “One of thepriorities for the CHS is services forpeople with vWD. This includesaffordable treatment for everybodyright across the country.”
The Canadian Hemophilia Societyhas adopted the position that desmo-pressin is a blood alternative andshould be made available in the sameway as factor concentrates – free ofcharge to the user, distributed byCanadian Blood Services and Héma-Québec, and paid for by theprovinces. Indeed, the alternatives tousing desmopressin are even morecostly – plasma-derived factor con-centrates costing hundreds of dollarsper infusion and frequent hospitalvisits. A failure to treat vWD leads toincreased absenteeism from work andthe possibility of serious complica-tions from bleeding. The CHS posi-tion is supported by the CanadianBlood Services mission statementwhich says: “Canadian Blood Servicesoperates Canada’s blood supply in amanner that gains the trust, commit-ment and confidence of all Canadiansby providing a safe, secure, cost-effec-tive, affordable and accessible supplyof quality blood, blood products andtheir alternatives.”
For more information on vonWillebrand Disease, see All Aboutvon Willebrand Disease, publishedby the CHS or visit the CHS websiteat www.hemophilia.ca
Octostim®Spray Available, Not Widely UsedEffective treatment for Type 1 von Willebrand Disease and mild hemophilia A
David Page, Chairperson, CHS Blood Safety CommitteeTHE
Anew treatment for Type 1 vonWillebrand Disease (vWD)and mild hemophilia A has
been available in Canada since late1998 but is not yet widely used.Octostim® Nasal Spray, manufacturedby Ferring Pharmaceu-ticals, is the brand namefor desmopressin acetatedelivered through a con-venient nasal spray, idealfor home use.
Other forms of desmo-pressin acetate have beenlicensed in Canada since1993. These includeDDAVP® Injection andOctostim® Injection. Asthe names imply, boththese products wereadministered by injection,either intravenously orsubcutaneously. None ofthese products are madefrom blood.
All three forms ofdesmopressin act byreleasing von WillebrandFactor (vWF) stored with-in the body. VonWillebrand Factor is oneof the proteins necessaryin blood clotting. In Type 1 vonWillebrand Disease, characterized bylow levels of vWF, the vWF levels aretemporarily raised high enough tostop bleeding. In mild hemophilia A,the increased amount of vWF carriesadditional quantities of factor VIII,the protein lacking in this condition,to the site of bleeding. Desmopressinis of no value in Type 2B or Type 3vWD, nor is it useful to treat severehemophilia A. However, some peoplewith Type 2A vWD do receive somebenefit.
Tom Alloway,CHS Vice-president, toldHemophiliaToday, “One of the prioritiesfor the CHS isservices forpeople withvWD. Thisincludesaffordabletreatment foreverybody rightacross thecountry.”

H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
In this issue, the Female Factor deals withthe way women live with vWD. The firstarticle is written by Renee Paper, a womanwho was diagnosed with vWD in hertwenties. She has been working for manyyears advocating for better vWD diagnosisand treatment. Ms. Paper works in Nevadaas an ER nurse and is President of theNevada Hemophilia Society. The secondarticle presents the viewpoint of a youngwoman, Céline Cyr, who, although she had some major problems, also was notdiagnosed until she was in her mid-twenties. The experiences of these twowomen shows the need for information onvWD both for the general public and formedical practitioners.
Like Mixing Oil and Water? Women with BleedingDisorders in EmergencyDepartments.By Renee Paper, RN, CCRN
Reprint of an article which appeared in the July 1998, Vol 3 Issue 3 ofHEMAWARE, published by NationalHemophilia Foundation.
When I was asked to write this,I thought about the irony ofhaving to write such a
specialized article. The fact that such anarticle is even needed is a sad example ofthe care many women with bleedingdisorders have reported receiving inemergency departments (ERs) throughoutthe country. Accounts such as “thephysician didn’t believe a woman couldhave a bleeding disorder” or “the doctorhad never heard of von WillebrandDisease” are all too common. In fact,reports about mistreatment at the handsof ER personnel throughout the countrywhen managing males with hemophiliacontinue to abound, so one is notsurprised to hear that women withbleeding disorders face the samemismanagement. For a woman, however,the issue of gender bias enters the picture.
Despite the facts that von Willebrand
Disease (vWD) is the most commonbleeding disorder, at least 100 times morecommon than hemophilia, and that itaffects males and females, hemophilia stillhas the most name recognition among notonly the general public, but the healthcarecommunity as well. Since hemophilia is asex-linked recessive disorder affectingmainly males, most physiciansautomatically think of hemophilia whenthey hear about a patienthaving an inheritedbleeding disorder. Thosewithout knowledge orexpertise in vWD mayeven assume a male withvWD actually has a formof hemophilia and that afemale with “alleged”vWD is lying. Add tothat a woman whopresents with some ofthe rarer coagulationdisorders, or even thesymptomatic carrierstate, and her chances ofbeing believed andreceiving appropriatemanagement willprobably decreaseaccordingly. After all,many hematologists donot readily acknowledgethe symptomatic carrierstate (which is actuallyno different clinicallyfrom mild hemophilia),so why expect cliniciansless versed in coagulationdisorders to do so?
Obviously, such behaviour andignorance are unacceptable, but the cold,grim reality is that they still persist. Sowhat can a woman with a bleedingdisorder do to increase her chances ofadequate and appropriate management atthe hands of ER personnel? The followingare some steps I propose every woman orcaregiver of a girl with a bleeding disorderthink about prior to having to utilize ERservices.
Be realistic about your expectations forcare in the ER
Why are you seeking ER care? Is it forthe usual emergent conditions such asbroken bones, lacerations, or burns are
you looking to the ER personnel to figureout why you keep having excessivemenstrual bleeding and prescribe therapyto stop it? Such complaints are moreappropriately handled by yourhematologist in consultation with yourgynecologist. ER personnel are notspecialized in either. ER personnel aretruly “jacks of all trades, but masters offew.” The reason for this is they see and
treat such an incrediblywide array of illnessesand injuries that they arelikely to have trueexpertise only in thosethey see frequently, suchas heart attacks, strokes,asthma, trauma,diabetes, fractures andlacerations. Assuming oreven desiring that ERpersonnel have expertisein managing bleedingdisorders is probablyunfair and unrealistic.They cannot possiblyknow everything aboutevery disorder. ERpersonnel increasinglyare looking to patientswith rare chronicdisorders for guidanceon how to manage them.For instance, if you needto go to the ER to have awound sutured, theymay look to you to guidethem on how to stop orprevent the bleeding that
may be associated with the injury or itstreatment. They expect you to haveknowledge of how to treat such bleedingepisodes. And you should.
Look for alternatives whenever possible
Hemophilia, vWD, and relatedbleeding disorders are chronic, lifelongdisorders, just like diabetes. Peopleaffected by these disorders should learnearly on how to manage them on a day-to-day basis. Do not become dependenton ERs to do so. Diabetics do not go tothe ER for their daily insulin injection,and also, people with bleeding disordersshould not count on ERs to manage theirclotting factor or DDAVP infusion needs.If you need frequent infusions of clotting
This section is related specifically to women with bleeding disorders and their families. All articles arereviewed by physicians to ensure medical accuracy. If you have any questions, comments or ideas,
feel free to contact me, Patricia Stewart, at the following addresses:Phone & Fax: 418-884-2208 or e-mail: [email protected] or simply put pen to paper and mail to:
389, R.R. # 4, La Durantaye, Quebec G0R 1W0
FEMALEFACTOR
THE
by Patricia Stewart
Hemophilia,vWD, and relatedbleedingdisorders arechronic, lifelongdisorders, justlike diabetes.People affectedby thesedisorders shouldlearn early onhow to managethem on a day-to-day basis.

H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
factor or DDAVP, either learn how to dothem yourself, have a family memberlearn, or employ the services of a homehealth company that can send a nurse toyour home to perform the infusion. Thissolution is quicker, cheaper, and lessstressful than the ER. It returns somecontrol back to the patient and theirfamily and ultimately causes lessdisruption in their lives. Also, if you useDDAVP and have never tried the highpotency nasal spray formula calledStimate, ask your physician about it. Mostpeople who respond to the intravenous(IV) form respond adequately to the nasalspray form too. Your physician will giveyou a test dose to measure your response,and, if adequate, you may be able to avoidthe need for IV infusions.
Be prepared to educate the ER staffabout your disorder and its management
Most people with bleeding disorderswho have had to utilize an ER can recountthe infamous question by an ERphysician, “so how long have you hadhemophilia?” That is your first warningsign that you are in trouble. If thephysician does not know that hemophiliaand von Willebrand Disease are inheriteddisorders and that you were born with it,do not expect him or her to know how totreat it. Know enough about your disorderand its treatment to be able to explain itto the personnel. Make it short and sweet.ERs are busy places, and the ER staff willnot have time to listen to the basics ofhemostasis and the differences betweenintermediate purity and recombinantfactor concentrates. Just tell them whatthey need to know to care for you. Have aletter or wallet card from your physicianoutlining your treatment regimen,including dosage, so they can administerthe necessary treatment without delay.Make sure the letter includes yourphysician’s name and number if the ERphysician needs to contact him or her.Be sure to wear a Medic Alert bracelet thatlists your disorder for those situations inwhich you may be unable to speak. Thetreating physician can call the number onthe back of the bracelet and get yourindividualized treatment recommen-dations provided by you when youobtained the bracelet and which you haveperiodically updated.
Bring your own factor or DDAVP
If your treatment requires infusion offactor concentrate or DDAVP, it is best tobring it with you to avoid delays in
obtaining it. If you do not have factorwith you, know where to obtain it in yourcommunity. If you are travelling to ruralareas, it is best to carry factor with youbecause it may be completely unobtain-able in a reasonable period of time insmall rural communities. Know how tomix and administer the product. Again,this may be the first time those personnelhave given clotting factor concentrates;the more you help them, the moreefficient the procedure will be. Be sure the
letter from your physician tells them toround off the dosages for factor VIII or IXin order to utilize the entire vial contents,or the personnel are likely to draw up onlythe dose ordered and dispose of the rest.In almost all cases, it is cheaper if youprovide your own product from home, ashospitals routinely mark up the prices ofmedicines to exorbitant levels to offset thecosts of operating facilities 24 per day.Sure, some ERs will not want you to bring
Continued on page 12
One Woman’s StoryCéline Cyr, Montreal, Quebec
Growing up, I was always covered inbruises, big and small. I love being active,so I never deprived myself of sports andgot plenty of bruises. Luckily I neversuffered a serious injury.
I have always had heavy periods andhave always had to be less active at thattime. I had no choice because the bleeding was always too heavy for me to doanything, and I was always afraid my clothes would get stained, especially inpublic. My periods became heavier and heavier, and a few times I wasbleeding so much that I had to go to the emergency room. I was evenhospitalized for a hemorrhage (a period that did not end). When the doctorfound no cause, such as miscarriage or fibroids he ordered blood tests andreferred me to a hematologist.
I was 25 when I was diagnosed with Type 1 Von Willebrand Disease. I hadalready spent 2 years trying to find out what was causing my problem and ittook me another 2 years, after the diagnosis, to find a doctor who really knewabout the disease.
When I was diagnosed, my first reaction was “What is vWD, how did I getit and what should I do?” Then I wondered “Is there a cure?” My way ofdealing with it was to get lots of information from books, the Internet and mydoctors. I found out everything about the illness and I also got to know myselfbetter, which is what enables me to live with it today. Nobody else in myfamily has vWD.
After I was diagnosed, the bleeding was brought under control, and I am now more careful about what sports I take part in. On days when thebleeding is heavy, I stay home from work and watch a movie or immersemyself in a book.
I am now on birth control pills all the time, to stop me from menstruating.I have a period about every 2 months and when the bleeding is excessive, Itake cyklokapron and inject myself with DDAVP under the skin. This greatlyreduces my problems.
Although I have not yet decided whether I want to have children, I knowthat vWD will be a big factor in my decision. I have one chance in two ofpassing it on, and if I do I know I will feel guilty.
The disease also has a big psychological impact. One lives in constant dread ofbeing covered in blood in public or even just waking up in the morning in ablood-soaked bed. Even now, and in spite of the treatment, the fear is still there.

in your own product. They are likely totell you it is against policy. Always ask tosee a copy of such a policy. They rarelyexist. If you know how to administer yourown product and just need them toperform the venipuncture, then after theyperform the “stick” go ahead and infuseyourself or your family member. Theycannot stop you from medicating yourselfor family member. You do not lose yourrights just because you are in an ER. Thebest thing to do, however, is to infusebefore you leave home. For example, ifyou need to use an ER for sutures, infuseyourself at home first so when you arrivein the ER you are a “non-hemophiliac.”You have managed that which you are ableto and are now utilizing the ER for thatwhich you cannot do, namely suturing.
Stay informed and in charge
Be careful about consenting to invasiveprocedures unless you fully understandthem, are sure of their necessity, and pre-treat ahead of time. For example, if the ERphysician recommends an arterial bloodgas (ABG) because you are complaining ofa cough and shortness of breath, ask ifthere are any alternatives. An ABGinvolves drawing a blood specimen froman artery, usually in the wrist. Thisprocedure can cause excessive bleedingand hematoma formation in persons withblood clotting abnormalities. A lessinvasive test is the pulse oximetry, whereinthey attach a monitoring device to yourindex finger which tells them thepercentage of oxygen saturation in yourbloodstream. It does not involve anyneedles and often gives the physicianenough information so that the moreinvasive ABG is not needed. Again, I amnot expecting you to know thealternatives, just to ask if there are any,and fully understand the risks and benefitsof a procedure before you consent to it. Ifultimately you feel the procedure iswarranted, be sure to pre-treat if thelikelihood for bleeding post-procedureexists. An example of procedures that willusually require pre-treatment includelumbar puncture (spinal tap), naso-gastrictube insertion (if at all possible ask for thetube to be inserted orally instead ofnasally), angiogram, chest tube insertion,and peritoneal lavage (a good alternativeto this is a CAT scan which will revealbleeding in the abdomen without havingto insert a needle into it). The insertion ofa peripheral (arms or legs) intravenousline usually does not require pre-
treatment, but the insertion of a centralline into the chest or groin does becausethe risk of bleeding with that procedure ishigher. Obviously, if you are in need ofany of these procedures, you are probablyseriously ill or injured, and making suchdecisions under those circumstances isdifficult at best. If at any time you areunsure of what to do, insist that yourhematologist or the nearest HTC beconsulted prior to proceeding.
Do not consent to unnecessary testing
This includes unnecessary bloodtesting. It always amazes me to hear aboutpeople with known hemophilia allowingan ER physician to order coagulationscreening studies on them such as a PTand PTT. What did they expect to find?These tests will only confirm the fact thatthe person has some sort of bleedingdisorder; it will not confirm the type!What was the purpose of such a test? Theperson already told the physician he hadhemophilia. Sometimes even the doctor isnot sure when asked why he or sheordered the test. There is no benefit toperforming such tests. They prolong thevisit and raise the cost. Refuse them. Thesame goes for X-rays of routine jointbleeds. In the absence of some sort oftraumatic event preceding the bleed, thereis little information the ER physician willgarner from X-rays of the joint.
Remember you can catch more flies with honey than vinegar
Always treat ER personnel with thesame respect and dignity with which youwish to be treated. Behaving in athreatening or adversarial manner will nothelp the situation; it will only worsen it.You are in a crisis, and these professionalsare there to help. You will need tounderstand and accept the fact that theywill not have the expertise in managingbleeding disorders that you may desire.What they do possess, however, is theknowledge and skill to help you in a trueemergency. Go in prepared to help explainthe bleeding disorder and its treatment sothat they can proceed to deliver thenecessary care.
ER visits need not be horrible,frightening, powerless experiences. Thepower truly does rest with the patients ifthey will just assume that role. Butremember, if you can avoid the ER in thefirst place, that is always best.
H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
WEAR AMOUSTACHE
Occasionally I do the walrusthing. You know, long whitemoustache hanging down –
at least, half a moustache. It comes right out of my nostril. It is, in fact, aKleenex. Okay, you caught me: it’s toiletpaper. A big wad of toilet paper,jammed right up my nose and hangingdown, getting in the way of lip-relatedactivities. This is called doing the walrusthing. It’s also called having a nose-bleed.
My brother did it. I do it. It’s disgust-ing – but it’s also brazen, which is, Ithink, a good thing to be in the face of amorale-zapping medical condition. I do,by the way, know better. A nosebleed ismeant to be faced patiently, sitting down,a cold cloth pressed firmly to the activearea. I subject my daughter to the squeezetreatment, and it works – for her.
Personally, I can’t wait. I bleed slowlyand persistently. And impatiently. Facedby gushing, I’ll give it a good squeeze.I’ll sit pretending the fingers on mynose are my mom’s, reminiscing aboutdegrees of pressure and how nice it feltto have her hand resting on my cheek.But the results are so indefinite – itseems the blood never completely stops.There’s always a stubborn trickle: toobig to ignore, but enough to make methink the grand squeeze is overkill. Cuethe walrus.
Did I say it’s disgusting? It is! It’s oneof those things that makes you appreci-ate marriage. My husband is used tome. It also helps to work at home. Mycomputer is used to me, too.
But it’s one of the ways I cope: getup, get on with it. Laugh about it. Thereare worse things to be than ridiculous.Even disgusting isn’t necessarily bad. It’sall in the attitude.
The nose-squeeze is good; it has itsplace, and it’s an important one. So weall squeeze. But I suspect there’s also anarmy of secret moustache-wearers outthere, can’t-hold-em-down walruses,dangling toilet paper in the privacy oftheir own homes. At least, I hope thereare. I can’t be the only one.
Can I?
Ania Szado, Toronto, Ontario
Continued from page 11
H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
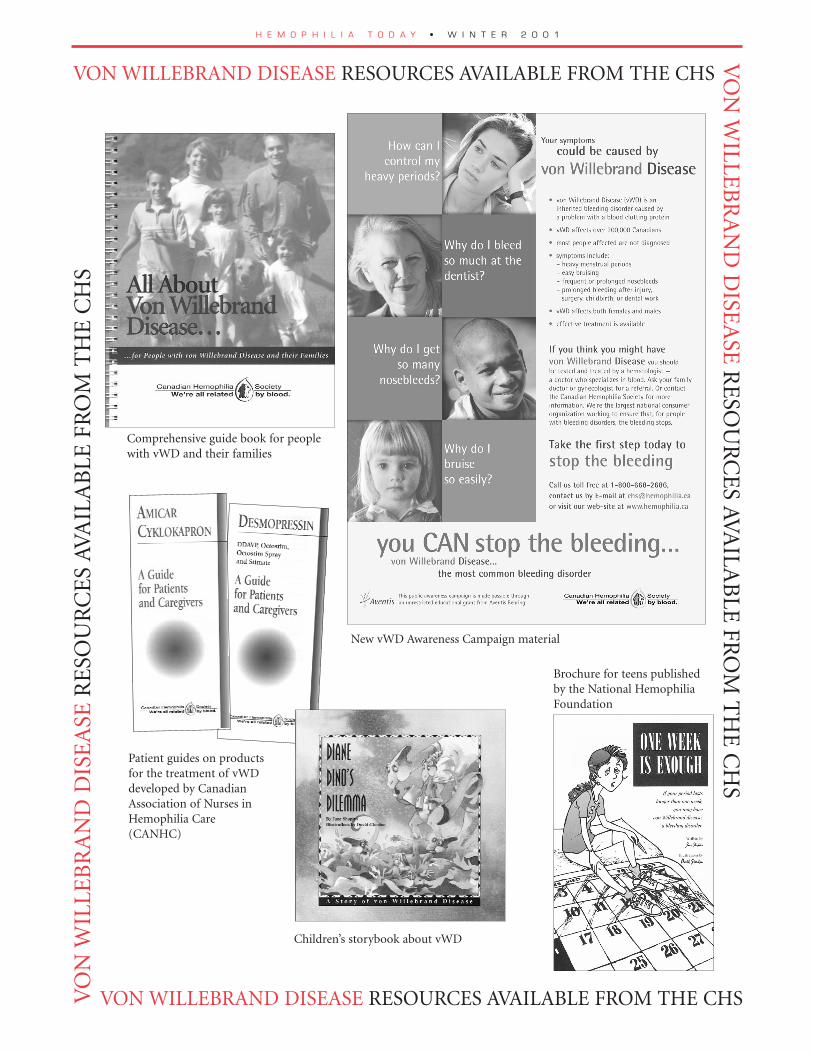
VON WILLEBRAND DISEASE RESOURCES AVAILABLE FROM THE CHSV
ON
WILLE
BR
AN
D D
ISEA
SE R
ESO
UR
CE
S AVA
ILAB
LE FR
OM
TH
E C
HS
VO
N W
ILLE
BR
AN
D D
ISE
ASE
RE
SOU
RC
ES
AVA
ILA
BLE
FR
OM
TH
E C
HS
VON WILLEBRAND DISEASE RESOURCES AVAILABLE FROM THE CHS
Comprehensive guide book for peoplewith vWD and their families
Patient guides on productsfor the treatment of vWDdeveloped by CanadianAssociation of Nurses inHemophilia Care(CANHC)
New vWD Awareness Campaign material
Children’s storybook about vWD
Brochure for teens publishedby the National HemophiliaFoundation

HEMOPHILIA & YOUR CHILD –
Bayer, in collaboration with CHS,Presents A New Interactive CD-ROM for Parents
H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
families inTOUCH
In the Spring of 1992, my husbandTed and I discovered our fraternalnine month old triplets each had
hemophilia. That day will forever moreremain our personal definition of“overwhelmed”. I also remember the lackof educational materials available to helpus cope and to understand more abouthemophilia. Literature for children andparents, teaching videos, and supportgroups were not in abundance. Focus onnew parents and young children was yetto come – even Hemophilia In Perspective,had not yet been published. So manygreat resources have been developed andmade available over the years and it keepsgetting better.
The plethora of available materials onhemophilia is a great accomplishment, asthe needs have been identified, andresources have been utilized to producegreat educational materials for childrenwith hemophilia and their families.A new and exciting tool for parents isbeing launched entitled, Hemophilia &Your Child. It is an interactive,educational CD-ROM , which wasdeveloped by a group of hemophilianurses, physiotherapists, physicians,parents and Bayer, in collaboration withthe Canadian Hemophilia Society. It wascreated to address the immediateconcerns of raising children withhemophilia and to help parents take anactive role in the management of theirchild’s hemophilia.
This free educational CD-ROM will beavailable in April 2001 through your localclinic or the Canadian HemophiliaSociety. As one of the parents who haveworked on this project, I hope it helpsmany families.
ProvidingSupport toFamilies
continued on page 15
Developed by Digital Rain, a newmedia company with expertise in com-puter oriented patient education tools,the CD-ROM was designed so that theprogram has no specific beginning or end.The viewers explore the program, choosinglinks to topics of immediate interest whileprogressing at their own rate.
There is a main menu with eight majortopic headings such as Growing Up withHemophilia, Living Safely, andUnderstanding and Assessing Bleeds. Eachsection provides acarefully chosencollection of sub-topics that are hot-linked so thatwhen the viewersclick on a link,they can jump todifferent types ofrelated infor-mation, such as theGlossary andResource Section.Simple animationand video footageof parents dis-cussing their expe-riences help to illustrate certain topics.Although targeted primarily to parents,there is also a section for children withHemophilia-related puzzles and games.
“Given Canada’s dispersed population,it is often difficult for families to attendclinic programs. In such cases, an effectivelearning resource is an interactive programthat will make accessing information easy.Hemophilia & Your Child is portable andcan be used in any computer with a CD-ROM drive – at home, work, at the libraryor school,” said Rena Battistella, MarketManager, Hemostasis, Bayer. “A tremen-dous amount of work went into develop-ing Hemophilia & Your Child, and theBayer team wants to extend a heart-feltthank you to everyone who was involved.”
This free educational CD-ROM will beavailable in April 2001 through your localhemophilia clinic or the CanadianHemophilia Society.
“Caring for a childwith hemophilia isa team effortinvolving the nursecoordinator, thehematologist,parents and mostimportantly – the child. We areall workingtogether to helpgive the patient thebest quality of life.”
As parents, we want our children tobe healthy and happy at all times.The reality is – every child encoun-
ters challenges. It’s all part of growing up.That’s why children need parents to helpand support them through difficult times.
As parents of a child with hemophilia,you’ll face many difficult challenges. Theinitial diagnosis can cause tremendousanxiety as you worry about your child’sfuture and the risks of everyday life. Asyour child grows, you must constantlyadjust and allow them the freedom andindependence to mature, while ensuringtheir safety and well being.
“Fortunately, the anxieties, worries andfrustration can be alleviated through edu-cation about how to manage the bleedingdisorder,” said Erma Chapman, President,Canadian Hemophilia Society. “By beingsupportive and informed, parents can helptheir child – in fact, the whole family – dealwith hemophilia in a healthy and positiveway. Knowledge helps you to feel somecontrol, the kind of control you need toenjoy family life on a day-to-day basis.”
There are many formal resources avail-able to parents, including the hemophiliaclinic team, The Canadian HemophiliaSociety, parent support groups and books.A new and exciting tool for parents is theinteractive Hemophilia & Your Child CD-ROM, which was developed by a group ofhemophilia nurses, physiotherapists, physi-cians, parents and Bayer, in collaborationwith the Canadian Hemophilia Society.
Hemophilia & Your Child is an interac-tive, educational CD-ROM designed topromote effective parenting skills. It wascreated to address the immediate concernsof raising children with hemophilia and tohelp parents take an active role in the man-agement of their child’s hemophilia.
“Caring for a child with hemophilia is ateam effort involving the nurse coordina-tor, the hematologist, parents and mostimportantly – the child. We are all workingtogether to help give the patient the bestquality of life,” said Nora Schwetz, BleedingDisorders Nurse Coordinator, WinnipegHealth Sciences Centre. Hemophilia & YourChild will certainly be a worthwhile tool tohelp parents learn more about their child’shemophilia. We are extremely appreciativeto Bayer for their ongoing support andfunding of education programs inCanada.”

H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
Ican easily understand how parents ofchildren with von Willebrand Disease havestruggled with the lack of understanding
about this condition and the lack of availableresources to support them. Historically, littlehad been done to gather families and childrentogether to discuss their experiences andconcerns. That changed when a mother of 2children with von Willebrand Disease decidedto get involved with her local hemophiliachapter, where she subsequently tabled heridea to have a workshop for families about vonWillebrand Disease. The first von Willebrand’sworkshop was held in Hamilton in 1997. Formany it was the first time they met other familiesdealing with von Willebrand Disease.
Caroline Mulder-Sutton is the mom whobecame involved at CWOR (Central WestOntario Region). She continues to support herchapter, is a Board member at CWOR andremains involved in many continuing projects forfamilies and children with vonWillebrand Diseaseand hemophilia.
I spoke to Caroline about Desiree’s article. She and Alan are very proud of Desiree’sinitiative and what she wants to share. For theSutton family, living life is a key lesson and notletting the bleeding disorder live your life foryou is something they want both their childrento accept.
I asked Caroline what has helped her copeso positively with the added challenges ofparenting children with bleeding disorders.Caroline works part time, so making sure theschools are well informed is key; a cell phonegives her peace of mind and freedom to nothave to be with the kids or at home. She andAlan have helped the kids choose activitiesthat make sense for each of them, and in herown words,
“You get tired of saying no, so we havetaught the kids that they have to takeresponsibility for their own actions and theirown bodies. We have made sure they know allabout first aid and the appropriate responsesfor injuries they incur. We have tried to teachthem how to cope with their bleeding disorderand to make sure they lead normal lives. I alsothink I have learned so much by beinginvolved at CWOR and with the CHS vonWillebrand Advisory Committee. How wecope with things teaches our kids to cope too.”
Congratulations Desiree. Thank you forsharing your article with us. Congratulationsto Mom and Dad also. It seems your effortsare paying off! Perhaps Brendan will write tous some day too with his thoughts on havinga bleeding disorder?
Take care and keep in touch.
Karen [email protected]
The following article is written byDesiree Sutton. Desiree is 12 yearsold and is a grade 7 student. Sheand her brother Brendan who is 9,both have von Willebrand Disease.They live in Cambridge with theirmom, Caroline and father Alan,who also has Type 1 vWD.
Having a bleeding disorder can be fun. A bleeding disorder can not be
seen unless you are bleeding. You might bleed for a couple of minutes, or for
a day. If you know what to do, and the right way to do it, then nobody needs
to know about it, or even care too much about it. It’s a part of you, and me
for that matter. You can look at the disorder in two ways, the many things
you can’t do, or the many things you could do. You might not be able to do
boxing or things like that, but you might play an instrument or take up
hiking or canoeing. You can find something that interests you and devote
your time to it.
The first thing you should do when you start school and have gym is tell
the teacher about it. The sooner you get it over with, the better. I should
know. If the teacher fusses over you, just tell him or her it is no big deal.
Unless, of course, it is a big deal to you and to them. You because you didn’t
tell them. Them, because if you told them, they might have prevented the
injury from happening to you.
Another thing that might help with your disorder is to not be afraid of
blood. The colour of blood, the sight of blood, the taste or even feel of blood.
You name it (if you can find anymore senses other than hearing, but I don’t
think you can hear blood. Can you?) Most people might not think this has
anything to do with a bleeding disorder, other than you get to see more of it
than other people.
Don’t hold yourself back too often, or you might miss a lot of the things
that make life worth living. What’s a little scrape or two if it meant that you
get to be with your friends. Also, don’t over extend yourself. Know where
your boundaries are and if you don’t know where they are, find out. You
might find something about yourself you never knew before. I’m finding new
things every week. I tried playing the flute at school and ended up in the
band. I’m a ‘fish out of water’, in the summer. You almost have to drag me
out of the pool. In the winter, I go skating. My real talent seems to be in the
water, not on it, even if it is frozen. I keep on asking for pads to go on my
butt for all the times I fall down. I heard somewhere that you learn
something new every day. You might not think so, but look back at what you
learned at school. You would not even be able to read this if you didn’t go to
school. You hopefully didn’t even have to put too much effort into reading,
you just do it, you weren’t born able to read, you had to learn it. I hope you
learned something reading my thoughts, because I certainly did, writing
about them. Thanks for reading my thoughts.
Desiree Sutton
H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
YOUTHFILE
The Guys’s Perspective
Jean-Daniel Beaubien19 years old – Type 2A vWDMontreal, Que.
Jean-Daniel was diagnosed withType 2A vWD as a baby. His moth-
er and sister also have it. Since he hasalways lived with the knowledge thathe has this disease, he simply accepts it.
He played a lot of sports whenyoung. Of course he had more bruisesthen every other kid, and when he’dget hit in the face with a hockey stick,he’d often end up in the hospital, buthe’d go back out and do it all overagain...
As a child, there wasn’t any syn-thetic treatment and the blood-basedcoagulants were available but the riskof HIV was too scary. So he wouldeither tough it out or go to the hospi-tal where they would pack his nose.They would fill his nose up to thesinuses with cotton bands (lubricatedwith Vaseline). “It’s horrible, one ofthe most painful procedures I ever gotin my life” says Jean-Daniel. Today heuses DDAVP nasal spray.
“ I rarely think about the fact thatI have vWD and it has never causedme a life-threatening problem. Mostof the time when I think about it, it’sbecause I’m already bleeding. I snow-board regularly; I train at a gym and
physical education classes. His interestsinclude curling, swimming (“if onlythere was a swimming pool around “)and he enjoys art.
He says his friends know that he hasa bleeding disorder because it’s so evi-dent. He explains what vWD is tothem. William has learned to live withType 3-vWD and places his own limitson his activities, but feels that it doesn’ttake over his life. He just deals with itand goes on with everyday living.
Matt Strmic12 years old – Type 3 vWDBoulton, Ontario
Matt was diagnosed with hemo-philia at the age of two when he
fell and bit his tongue and it wouldn’tstop bleeding. Both his parents werethen tested and, 3 months later, thediagnosis was changed to Type 3 vonWillebrand Disease. His sister has amild form.
He wasn’t a very adventurous kidand preferred playing with toys. Hesays this was probably lucky for himand his parents. He had few problemsuntil he was six when he had a gastricbleed, a frightening experience. It wasthen that he began to realize thatsomething was wrong.
His everyday life is affected onlywhen he can’t join his friends in cer-tain activities. And at times he has toexplain all his bruises. However, thisdoesn’t stop Matt from taking part inmany sports. But his passion is swim-ming. Matt would rather swim thando anything else. He feels that it hashelped limit his bleeding episodesbecause it develops muscles whichhelp cushion the joints. He joined theVaughan Aquatic Club 5 years agoand now swims almost daily. He hasclose provincial times in the 100mand 200m backstroke and regularlyparticipates in swim meets. Hiscoaches know about his condition
basically do anything Iwant. I always wanted totake boxing classes, but Idecided I’d be better offnot to.”
His friends are allaware of his bleedingproblem, although only afew have ever seen himbleed. “ I’ve had the samefriends for maybe 13-14years now. I guess they’resurprised sometimes
when I start bleeding in front ofthem, they aren’t used to that kind ofbleeding. But”, he says, “we still haveno problems punching each other’sarm until it hurts...”
Jean-Daniel adds: “Perhaps the onlything I’d like to add is this. When I waslittle, the doctors told me I should neverski, play football, etc, etc... Skiing turnedout to be the most fun I ever had in mylife, perhaps. Unless you have a reallyserious case of vWD or hemophilia,go out, and try things, even if they sayyou shouldn’t… just be a bit morecareful I guess.
William Dutot17 years old – Type 3 vWDPort-aux-Basques, Nfld.
As a baby, William had problemswith teething, actually drooling
blood and he had so many bruises thatthere were rumours that he was beingabused. He was diagnosed with Type3, the severe form of vWD, when hewas about nine months old. Hismother has been diagnosed with amilder type of vWD.
His earliest memories are of beingall “banged up” just by running aroundthe house. William has always livedwith the knowledge that he has vWD.He has accepted the limits that thistype of vWD puts on him and avoidsrough contact sports. He also skips
Living with vWD
Jean-Daniel flyinghigh at Club Med circus school
H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
and are very encouraging. However,Matt had a big disappointment lastJune when a hip bleed prevented himfrom participating in a meet wherehis team won the gold. But one of theolder boys sent him a medal that he’dwon. That’s true friendship!
Matt attributes his success to aclose family and supportive friends. Ithelps him get through difficult times.His mother is his medical advocate,his father “is in charge of the fundepartment”, while his sister, Katie,comforts him when he’s hurt, is thefirst one with the ice pack ready andalways cheers him on.
“Our family has a kind of philoso-phy or attitude which I feel has reallyhelped me to keep positive aboutthings. We accept things we cannotchange and learn to adapt to situa-tions supporting each other every stepof the way.”
A Young Woman’sPerspective
Heather Carlson24 years old - Type 1 vWDToronto, Ontario
Iwas diagnosed at the age of 17. Myyounger brother had some other
medical issues and one of his doctorshad recognised a problem with bruisingand suggested that he be tested for ableeding disorder. When testing resultedin a diagnosis of vWD, the doctor sug-gested that my mother should be testeddue to her history of bleeding problems.She didn’t even consider the possibilityof my having vWD as well. We were justchatting about her upcoming appoint-ment to be tested and what symptomsshe had when I suggested that I showedall the same symptoms. I accompaniedher to her appointment and shortlyafter we were both diagnosed with vWDType 1. I think the word relieved is thebest to describe my reaction. All of asudden things made sense.
Prior to being diagnosed I had had ableeding problem when my tonsils wereremoved and when baby teeth fell out.And I have always had problems withmy periods being very heavy andpainful. In fact shortly after I startedmenstruating my family doctor sent me
to a gynecologist and Iwas put on birth con-trol pills in order tolessen the duration andpain involved. At thattime I would be offschool for 2-3 days eachmonth. I continue tohave problems withperiods like mid-monthspotting, 2-3 week peri-ods a couple of timesand the most embar-rassing for a young girl,bleeding through cloth-ing at times. I learnedearly to wear dark colours at that timeof the month.
I now use DDAVP and Octostim andI do my injections myself at home. Imust admit I avoided learning how todo this for quite some time. My motheris a nurse so it was easier to get her to doit. The nurse co-ordinator at the hemo-philia clinic finally talked me into learn-ing to inject myself. I use alittle needle that goes justunder the skin and I injecta fairly small amount ofliquid. All the hemophiliacsI know are quite jealous ofthe ease of my injections. Idon’t need them oftenenough to get really com-fortable giving them, butafter a few times I wasmore relaxed about it.
Von WillebrandDisease doesn’t reallyaffect my every-day lifenow. I just have to be a lit-tle careful. My biggestissue now is that I’m aklutz. I’m famous for hit-ting my head or walkinginto things. Anyone whoknows me can attest tothis. I have to be careful toice any good bumps to my head and payattention if I get any headaches. If Ithink I’m really going to bruise I’ll takean injection. Some times if I cut myselfit doesn’t want to stop seeping a littlebit of blood. I’ll hold pressure on it alittle longer than the average person.For me I’m just being a little more care-ful when I hurt myself.
Most of my friends know about mydiagnosis but only because I’ve chosento tell them. In my case, and like most
persons with vWD, if I didn’t tell peoplethey would never know.
I guess the reason I was so willing toshare my story is to let other youngwomen with vWD know that there areothers out there like them. And, girls,I‘m beginning to feel a little out-num-bered by all of these hemo guys. Now
don’t get me wrong, guys;you’re all great, and someof you are my dearestfriends. But I would liketo see more young womenwith von Willebrandinvolved in the Society. Inmy 4 years as a memberI’ve been involved inweekend retreats, canoetrips and I was fortunateenough to go to Montrealfor the World Federationof Hemophilia Congress.At the youth pre-congressmeeting, only one othervWD female was present,Anna from Sweden. Shebecame a friend and Ihope to see her at the nextconference in Spain 2002.Come on, girls; we can’tcontinue to let the guys
have all the fun.I would like to hear from any other
young women with vWD. You can con-tact me at the address below:
Heather Carlson552 Birchmount Road, # 704Scarborough, ONM1K 1P4
or forward your comments to KarttikShah, editor of the Youth File [email protected]
I guess thereason I wasso willing toshare my storyis to let otheryoung womenwith vWDknow thatthere are others outthere likethem.
Heather Carlson and Karttik Shah

H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
By Frank Bott,Past Chair, National Awards Committee
The Briars on Lake Simcoe was the setting for the annualCHS Awards Banquet on November 25th, 2000. FrankBott, retiring Chair of the National Awards Committee,
was Master of Ceremonies. President Erma Chapmanannounced the appointment of Barry Isaac as the new chair ofthe committee. Frank Bott introduced the previous year’scommittee – Barry Isaac, Normand Landry, Patricia Stewart,Eric Stolte, and Pam Wilton. He also acknowledged the excel-lent work of Clare Cecchini, the staff resource person duringthe five years he had been committee chairperson.
The Chapter RecognitionAward was presented toSheila Comerford andPatricia Stewart of theQuebec Chapter by ErmaChapman, in recognitionof their fundraising whichresulted in a 50% increasein revenues. Successfulfundraising initiatives
included a Corporate Campaign, a golf tournament, a lottery,and sale of Christmas colouring books.
The Chapter/Region ofthe Year Award was pre-sented by Erma Chapmanto Pam Wilton and MikeMcCarthy of theSouthwestern OntarioRegion for its outstandingefforts, in collaborationwith the clinic team, to
ensure the maintenance of the comprehensive care programduring its transfer to another institution. The ProgramCouncil continued to be an effective mechanism to facilitatecollaboration between consumers and health care providers.
The Award of Appreciation went to NoraSchwetz, nurse-coordinator in Winnipegwho has, over and above her professionaldedication and devotion, contributed vol-unteer hours to education, family camp,and group facilitation. As well, she hasbeen Co-Chair of the CHS Nursing Groupand helped to develop educationalresources for patients. She has also been
active on the international scene. The award was presented toher by the President of the Manitoba Chapter, Frank Figler.
The Dr. Cecil Harris Award waspresented by Dr. Sue Robinson,Chair of the Medical and ScientificAdvisory committee to Dr. DavidLillicrap of Kingston, recognizing15 years of devoted work toimprove the quality of life for per-sons with hemophilia. Dr. Lillicraphas an international reputation asa researcher in the area of genetherapy. He is one of Canada’s
leading authorities on von Willebrand Disease and serves asChair of the AHCDC sub-committee on vWD and is a valuedmember of the CHS vWD Advisory committee. In 1997 hecreated the Canadian registry for patients with von WillebrandDisease. He has served for many years on the CHS Medicaland Scientific Committee.
The Chapter LeadershipAward was given to twosisters, Lois Bedard andJoyce Rosenthal, who werevery much a team in thefounding and early devel-opment of the OntarioChapter, including settingup the structure of thefirst provincial chapter,and early educational and
advocacy efforts on behalf of persons with bleeding disorders.As well, they were both actively involved in the national organ-ization, Lois at one point being on the national ExecutiveCommittee, and Joyce as the first national Executive Directorof the CHS when the office was in Toronto. Erma Chapmanand Tom Alloway, representing Hemophilia Ontario, jointlymade the presentation.
The recipient of this year’sFrank Schnabel Award wasBarry Isaac of Calgary.Frank Bott made the pres-entation, citing Barry’sachievements over at least30 years, including hisinfluential involvement inupgrading and developingcomprehensive care in
Calgary; years of serving at regional, chapter, and national lev-els of the CHS; his valuable advisory role in HIV and hepatitisC compensation, the Krever Inquiry, and blood safety issues.For the past ten years he has been editor of Hemophilia Today.He has been a member of the National Awards committeesince its inception, developed the criteria for the CHSScholarship and Bursary Program, and is the current chair ofthe Scholarship Review Committee.
CHS HONOURS PAST AND PRESENT AWARD RECIPIENTS

H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
The nomination package for theyear 2000 National Awards hasbeen sent out to chapters and
clinics or may be obtained by calling theNational Office. This year a new award,in memory of Pierre Latreille, is beingintroduced to recognize CHS staff.
Please consider nominating an individ-ual from one of the following cate-gories. The National Awards are:
CHAPTER / REGION OF THE YEARAWARD
The award is designed to recognise achapter or region that has demonstratedexcellence over all, during the past year.It is awarded to that chapter which hasshown outstanding efforts in a varietyof areas such as advocacy, fundraising,patient services, education, or chapter/regional development.
Previous RecipientManitoba Chapter
CHAPTER RECOGNITION AWARD
This award is designed to recognisechapters that have demonstrated anachievement over the preceding year ina specific area such as fund-raising,patient services, education, or chapter/regional development.
Previous Recipients:
B.C. Chapter CWOR Hemophilia Ontario Manitoba Chapter Newfoundland Labrador Chapter Nova Scotia Chapter PEI Chapter Quebec Chapter Saskatchewan Chapter
TCOR
AWARD OF APPRECIATION
This award honours an individual whohas demonstrated outstanding service tothe care of persons with hemophilia orrelated bleeding disorders.
Previous Recipients:
Ann Harrington, Nurse Co-ordinatorJane Neil, PhysiotherapistLois Lindner, Nurse Co-ordinatorMuriel Girard, Nurse Co-ordinatorJack McDonald, Ph.D., Social WorkerBrenda Blair, Nurse Co-ordinatorLorraine Bernier, Nurse Co-ordinator
DR. CECIL HARRIS AWARD
This award honours distinguished con-tributions in the areas of hemophilia-related research or the advancement ofthe care of patients with hemophilia orrelated bleeding disorders. It is namedafter the late Dr. Cecil Harris, in recog-nition of his contribution as one of thepioneers in the care and treatment ofhemophiliacs in Canada.
Previous Recipients:
Dr. Irwin Walker Dr. Georges-Étienne Rivard Dr. Martin Inwood Dr. Kenneth Shumak Dr. Man-Chiu Poon Dr. Kaiser Ali
CORPORATE LEADERSHIP AWARD
This award honours outstanding corpo-rate leadership which fosters commit-ment to the spirit of voluntarism onbehalf of hemophilia on a national level.
Previous Recipient:Bayer Inc.
CHAPTER LEADERSHIP AWARD
This award is given to an individualwho has merited special national recog-nition for having provided exceptionalleadership and devotion to a specificCHS Chapter over many years and foroutstanding efforts to further thegrowth and development of the chapter.
Previous Recipient:Normand Landry, New Brunswick
HONOURARY LIFE MEMBERSHIPAWARD
This award is given to an individualwho has demonstrated exceptional lead-ership and devotion to the CHS overmany years. The recipient has meritedspecial recognition for continuingefforts, particularly at the CHS Boardlevel, to further the growth and devel-opment of the mission and objectives ofthe CHS and the development of publicrecognition of the CHS and its goals atthe National and Chapter level.
Previous Recipients:
James Kreppner Durhane Wong-Rieger, Ph.D.Pierre Fournier David Page Jack McDonald, Ph.D.Elaine Woloschuk Joyce Rosenthal
Kenneth E. PoyserDr. Martin InwoodPat HarrisDr. C.E.C. HarrisRonald George, Ph.D.Leni GeorgeFrank L. Schnabel
FRANK SCHNABEL AWARD
This award was initiated to honour theoutstanding service of Frank Schnabel,the founder of the CanadianHemophilia Society, for his valued rolein the growth and development of theCHS, the education of and care ofhemophiliacs, and the education of thepublic regarding hemophilia needs. Theaward is presented in his name to hon-our a volunteer who, over a number ofyears, has rendered distinguished servic-es and noteworthy contributions to themission and objectives of the CanadianHemophilia Society.
Previous Recipients:
Erma Chapman, Ph.D.John Plater Ken Little Durhane Wong-Rieger, Ph.D.Frank Bott David Page Peter Wachter
PIERRE LATREILLE AWARD
This new award for excellence will begiven to a staff member of the CHSworking at either the national, chapteror regional level who demonstrates thequalities that were shown by the dearlyappreciated CHS staff member forwhom it is named, Pierre Latreille.Pierre worked as Finance Manager forthe Society from September 1991 toOctober 1999 and served as actingExecutive Director from November1998 to July 1999. He passed away onOctober 29th, 1999 in the CHS officewhile at work at his many duties.
SPECIAL AWARDS OFAPPRECIATION
Special awards in recognition of out-standing contributions to the CanadianHemophilia Society have been awardedover the years to the following persons:
Previous Recipients:
Robert GibsonGeorge Moody, MPP, Nova ScotiaPaul Ramsey, MPP, BCRussel Williams, MNA, QuebecBonnie Tough Kathy PodroberakEd Kubin
NOMINATIONS FOR YEAR 2000 NATIONAL AWARDS

H E M O P H I L I A T O D A Y • W I N T E R 2 0 0 1
Over the past several years there hasbeen an increasing sense that the CHSneeds to step up to the challenge ofwhat it means to be part of a globalcommunity. There are countries wherethe average life expectancy of a personwith hemophilia is under 25 years Still,over 75% of people with hemophiliaaround the world die from bleeding.Being so well resourced, we must helpthose in our world-wide bleeding disor-der community whose resources areseverely low.
To keep our readers informed aboutinternational issues we are introducing anew column, The Global Perspective,which will feature topics of interestabout the global community. This firstissue will include an article about thenewly established CHS InternationalProjects Committee and a report on theQuebec Chapter’s recent visit toSenegal. Please forward any commentsor suggestions for future topics to me at
Having helped to host the WFH’sWorld Congress last summer, anagreement was struck that will
give the CHS somewhere around$150,000. It was decided to put thosefunds to use outside our borders. Toenable that, and to give longer term direc-tion to our global responsibilities, theCHS struck what has come to be calledthe International Projects Committee thatI have the priviledge of chairing. It’s excit-ing to think of the difference we can makeas we help, both organizationally andmedically, people with bleeding disordersin needy countries.
François Laroche, Vice-PresidentCanadian Hemophilia Society,Quebec Chapter
From November 12 to 20, 2000, theCanadian Hemophilia Society -Quebec Chapter (SCHQ) undertook
a field trip to Dakar to formalize itsTwinning Agreement with l’Associationsénégalaise des hémophiles (ASH).
I had the opportunity of heading thismission. Accompanying me were ClaudineAmesse, Hemophilia Nurse Coordinator,Sainte Justine Hospital in Montreal, andLouis Gibeau, representing the WorldFederation of Hemophilia (WFH).
Our trip corresponded with one of themain objectives of the WFH, namely topromote the advancement of hemophiliaassociations in developing countries. Thisin turn will enable a network to be forgedbetween the associations, leading to bilat-eral cooperation and productive culturalexchange.
SCHQ first made contact with ASHduring the International Congress of theWFH in Dublin in 1996. More intensivediscussions took place at the 1998Congress in The Hague and in Canada, atthe Montreal Congress, in 2000.
Why did we choose ASH? Because
QUEBEC FORMALIZES TWINNINGAGREEMENT WITH SENEGAL
Our first goal is to figure out how bestto distribute the funds we’ve been given.Already requests have come both fromCanadian chapters who are working withother countries as well as from othercountries themselves. Exactly what ourpriorities are and how we can strategicallycontribute to long term improvement inbleeding disorder care will be the commit-tee’s first challenge. We’re eager to begin toput funds in the hands of worthy initia-tives as soon as possible. We’ll look for-ward to keeping you abreast of futuredevelopments as we get going.
Quebec and Canada have always hadextensive cultural and commercial rela-tions with Senegal. In addition, ASHseemed to be a solid organization run bydynamic people dedicated to improvingthe quality of life for hemophiliacs. Lastbut not least, synergy and a feeling of trustsoon built up between everyone involved,especially the president, Ms. Anta Sar.
We spent a busy week with friendlypeople who made us feel very welcome.Our colleagues in Senegal did everything tomake things easier and treated us as VIPs.
Among the highlights of our programwere a tour of the national transfusion cen-tre, a meeting with ASH administratorsand members during Hemophilia Day, avisit to the Canadian embassy in Dakar, ameeting with the director of the office ofthe Minister of Health, interviews with theSenegalese press and electronic media, atour of Dakar’s three hospitals, a shortexcursion outside the capital and, ofcourse, the signing of the TwinningAgreement.
The goals of the partnership are: to dis-seminate the operational model of theSCHQ and the hemophilia treatment cen-tres, including their development, possibil-ities and limitations; to support ASH inraising the awareness of Senegalese deci-
sion-makers in order to ensure hemophili-acs receive adequate treatment from healthprofessionals with expertise in this type oftreatment; and to organize bilateralexchanges conducive to developing ourmutual skills and knowledge.
It was agreed that the TwinningAgreement would be signed for two yearsand then re-evaluated. For this type ofproject to succeed, both parties need tohave the same expectations and common,realistic goals.
This field trip taught the SCHQ a lotabout life and customs in Senegal. It gaveus the chance to make friends with won-derfully warm, welcoming people who areeasy to work with. Our partnership prom-ises to be extremely productive for the people of Senegal and Quebec.
My thanks go to WFH representativeLouis Gibeau for his sound advice and sup-port, which were indispensable on such amission abroad.
I also salute the contribution ofClaudine Amesse, Nurse Coordinator ofthe hemophilia clinic at Sainte JustineHospital. In projects like this, being able torely on the support and expertise of ahemophilia treatment centre is paramount.
Finally, I acknowledge the tireless dedi-cation of ASH president Anta Sar; herkindness and generosity during our stayknew no bounds. Thank you, Anta, wehope to meet again soon.
THEGLOBALPERSPECTIVE
By Eric Stolte,Chair, International Projects Committee
CHS INTERNATIONAL PROJECTS COMMITTEE