Embed Size (px)
Citation preview
8/12/2019 Ha Tace for Mmlm 2008
http://slidepdf.com/reader/full/ha-tace-for-mmlm-2008 1/6
AJR:190, January 2008 99
tastasis does occur, chemotherapeutic op-
tions are limited.
Hepatic arterial chemoembolization for the
management of hepatic metastasis of melano-
ma was first reported in 1988 [2]. Chemoem-
bolization achieves greater drug concentra-
tion within the tumor than does systemic che-
motherapy while decreasing systemic toxicitysuch as myelosuppression [5]. A retrospec-
tive analysis [6] showed that hepatic arterial
chemoembolization with a cisplatin-based
regimen was the only technique resulting in
improved survival compared with other treat-
ments, including systemic chemotherapy and
chemotherapy through a surgically implanted
arterial port. However, reports of outcomes
remain extremely limited. The primary goal
of hepatic arterial chemoembolization is to
Hepatic Arterial
Chemoembolizationfor Management ofMetastatic Melanoma
Karun V. Sharma1
Jennifer E. Gould1,2
J. William Harbour2, 3
Gerald P. Linet te2, 4
Thomas K. Pilgram1
Pouya N. Dayani3
Daniel B. Brown1,2,5
Sharma KV, Gould JE, Harbour JW, et al.
1Mallinckrodt Institute of Radiology, Washington
University School of Medicine.
2Siteman Comprehensive Cancer Center, Washington
University School of Medicine, St. Louis, MO.
3Department of Ophthalmology, Washington University
School of Medicine, St. Louis, MO.
4Division of Oncology, Department of Medicine,
Washington University School of Medicine, St. Louis, MO.
5Present address: Division of Cardiovascular and
Interventional Radiology, Thomas Jefferson University
Hospital, Suite 4200 Gibson Bldg., 111 S 11th St.,
Philadelphia, PA 19107. Address correspondence to
D. B. Brown.
Itervetio Rioogy • Origi Reerch
AJR 2008; 190:99–104
0361–803X/08/1901–99
© American Roentgen Ray Society
The overall incidence of liver-
dominant metastatic melanoma
is low, particularly in compari-
son with that of other primary
tumors, such as colon and breast cancer. Oc-
ular melanoma is the most common intraoc-
ular malignant tumor in adults [1–3]. Despite
undergoing apparently definitive manage-ment of the primary tumor with either enu-
cleation or plaque radiation therapy, many
patients eventually have a relapse, and dis-
tant metastatic lesions develop, most com-
monly in the liver. Once hepatic metastasis
occurs, the prognosis is extremely poor; the
mean survival period is approximately 4
months despite salvage chemotherapy [3, 4].
Cutaneous melanoma rarely results in liver-
dominant metastasis. When this type of me-
Keywords: hepatic arterial chemoembolization, liver,metastatic disease, metastasis, ocular melanoma
DOI:10.2214/AJR.07.2675
Received June 5, 200 7; accepted after revision
August 7, 2007.
OBJECTIVE. Hepatic arterial chemoembolization is an accepted therapy for stage 4 mela-
noma with liver-dominant metastasis. However, the reports of outcomes are limited. We present
our outcomes with hepatic arterial chemoembolization for metastasis of stage 4 melanoma.
MaTERIals and METHOds. Twenty patients with liver-dominant metastasis of
ocular or cutaneous melanoma were treated with hepatic arter ial chemoembolization. Overall
survival and progression-free survival rates were calculated from the first treatment. Patients
with intrahepatic tumor progression were treated with additional hepatic arterial chemoembo-lization. Both overall survival and progression-free survival were analyzed with the Kaplan-
Meier method. Tumor pattern on angiography was characterized as either nodular or infiltrative
on the basis of angiographic appearance.
REsUlTs. The 20 patients underwent 46 hepatic arterial chemoembolization sessions
(mean, 2.4 sessions; range, 1–5). The mean and median overall survival times were 334 ± 71
and 271 days, respectively. There were no deaths within 30 days of treatment. Thirteen of
the 20 patients had progression of disease. The mean and median progression-free survival
times for these patients were 231 ± 42 and 185 days, respectively. Patients with lesions that
had a nodular angiographic appearance had longer progression-free survival than patients
with lesions that had an infiltrative appearance (mean progression-free survival time, 249
vs 63 days). Patients with lesions that had a nodular angiographic appearance also survived
significantly longer than those with lesions that had an infiltrative angiographic pattern (mean
overall survival time, 621 vs 114 days; p = 0.0002).
COnClUsIOn. Hepatic arterial chemoembolization for liver-dominant metastasis ofstage 4 melanoma is a safe treatment that results in longer survival than has occurred among
historical controls. Patients with lesions that have a nodular tumor appearance on angiogra-
phy survive significantly longer than patients with lesions that have an infiltrative appearance
on angiography.
Sharma et al.Hepatic Arterial Chemoembolization of MelanomaInterventional RadiologyOriginal Research
8/12/2019 Ha Tace for Mmlm 2008
http://slidepdf.com/reader/full/ha-tace-for-mmlm-2008 2/6
100 AJR:190, January 2008
shrm et .
arrest progression of disease. A common
finding in existing studies is that a large num-
ber of patients experience disease progres-
sion despite treatment with hepatic arterial
chemoembolization, the reported response
rates being less than 50% [6, 7]. To date there
has been no method, to our knowledge, of pre-
dicting which patients will respond to therapy.The reported survival times among patients
who do respond to treatment range from 14 to
22 months [6, 7]. In this study, we evaluated
our institutional experience with a multidrug
hepatic arterial chemoembolization regimen
of cisplatin, doxorubicin, and mitomycin C
in the treatment of patients with liver-domi-
nant metastasis of melanoma. The principle
outcome investigated was overall survival in
a contemporary cohort. A secondary mea-
sure was angiographic findings, which sug-
gest there are two distinct forms of hepatic
metastatic disease that respond differently to
hepatic arterial chemoembolization and are
predictive of outcome.
Materials and Methods
This study was approved by our institutional
review board. All patients underwent cross-sec-
tional imaging with contrast-enhanced CT, PET/
CT, or both within 1 month before treatment.
Informed consent was obtained from all pa-
tients. On the day of treatment, laboratory data,
including complete blood cell count, complete
metabolic panel, and prothrombin time, were ob-
tained. Standard preprocedural medications (8
mg ondansetron, 10 mg dexamethasone, and 500mg metronidazole) were administered.
Local anesthesia was obtained with 1% buff-
ered lidocaine, and sedation was achieved with IV
midazolam and fentanyl. The Seldinger technique
was used to access the common femoral artery.
Superior mesenteric angiography was performed
though the portal venous phase to evaluate for
portal vein patency and flow direction and vari-
ant arterial anatomic features. Celiac artery an-
giography was followed by subselection of the
right or left hepatic artery with a microcatheter.
After confirmation of the appropriate position,
chemoembolization was performed with a mix-
ture of 50 mg cisplatin, 50 mg doxorubicin, and 10
mg mitomycin C dissolved in sterile contrast ma-
terial (ioversol, Optiray 350, Mallinckrodt Medi-
cal) and emulsified with ethiodized oil (Ethiodol,
Savage Laboratories). After infusion of the che-
motherapeutic agents under fluoroscopic monitor-
ing, embolization was performed with either ab-
sorbable gelatin sponge (Gelfoam, Upjohn) slurry
or 300–500 mm polyvinyl a lcohol (PVA) par ticles
mixed in contrast material until near stasis of flow
in tumor-feeding branches was achieved. Use of
PVA was reserved for cases in which feeding ar ter-
ies were severely pruned from previous treatment.
The decision to use PVA was made by the pr imary
operator at the time of the procedure. Use of PVA
did not limit further hepatic arterial chemoem-
bolization. Aliquots of 1–3-mL of 1% lidocaine
were intermittently administered intraarterially
during infusion of the chemotherapeutic mixture
[8]. Up to one lobe was treated per hepatic arterial
chemoembolization session; the contralateral lobe
was treated 4–6 weeks after the first procedure.
After the procedure, patients received main-
tenance IV antiemetics and antibiotics (8 mg on-
dansetron every 8 hours and 500 mg metronidazole
every 12 hours) until discharge from the hospital.
Pain control was achieved with hydromorphone hy-
drochloride delivered through a patient-controlled
anesthesia device. Patients were discharged from
the hospital when oral intake was adequate and
pain well controlled without IV narcotics. Follow-
up cross-sectional imaging (contrast-enhanced CT
or PET/CT) was performed approximately 4–6
weeks after treatment of all tumor-bearing branch-
es to evaluate response and determine the need
for additional hepatic arterial chemoembolization
treatments. If residual hepatic disease was pres-
ent or if there was evidence of intrahepatic disease
progression, additional chemoembolization proce-
dures were performed with repeated imaging after
repeated treatment of tumor-bearing vessels. Dis-
ease progression, response, and stability were de-
fined according to the Response Evaluation Criteria
in Solid Tumors [9]. Complications were evaluated
with the National Cancer Institute Common Toxic-
ity Criteria for Adverse Events (CTC) version 3.0,
which is the accepted measurement tool for toxic-
ity in oncologic studies [10]. Survival rates and
time to disease progression from the time of first
chemoembolization were calculated with Kaplan-
Meier analysis.
Results
Patient Characteristics and Survival
Between February 2004 and February 2007,
20 patients (14 men, six women; mean age, 62
years; range 31–81 years) underwent 46 hepatic
arterial chemoembolization procedures. Sev-
enteen patients had ocular and three had cuta-
neous melanoma. All patients except one pre-
1.0
0.9
P r o p o r t i o n o
f P a t i e n t s
S u r v i v i n g
Survival Period (d)
1,200
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
1,0009008007006005004003002001000
0.0
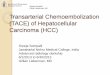
Fig. 1—Graph shows resultsof Kaplan-Meier analysis ofoverall survival for entiregroup after hepatic arterialchemoembolization. Calcu-lated mean and median sur-vival times were 33 4 ± 71 and272 days, respectively.
1.0
0.9
P r o p o r t i o n
o f P a t i e n
t s
S u r v i v i n g
Time to Progression (d)
900
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
8007006005004003002001000
0.0
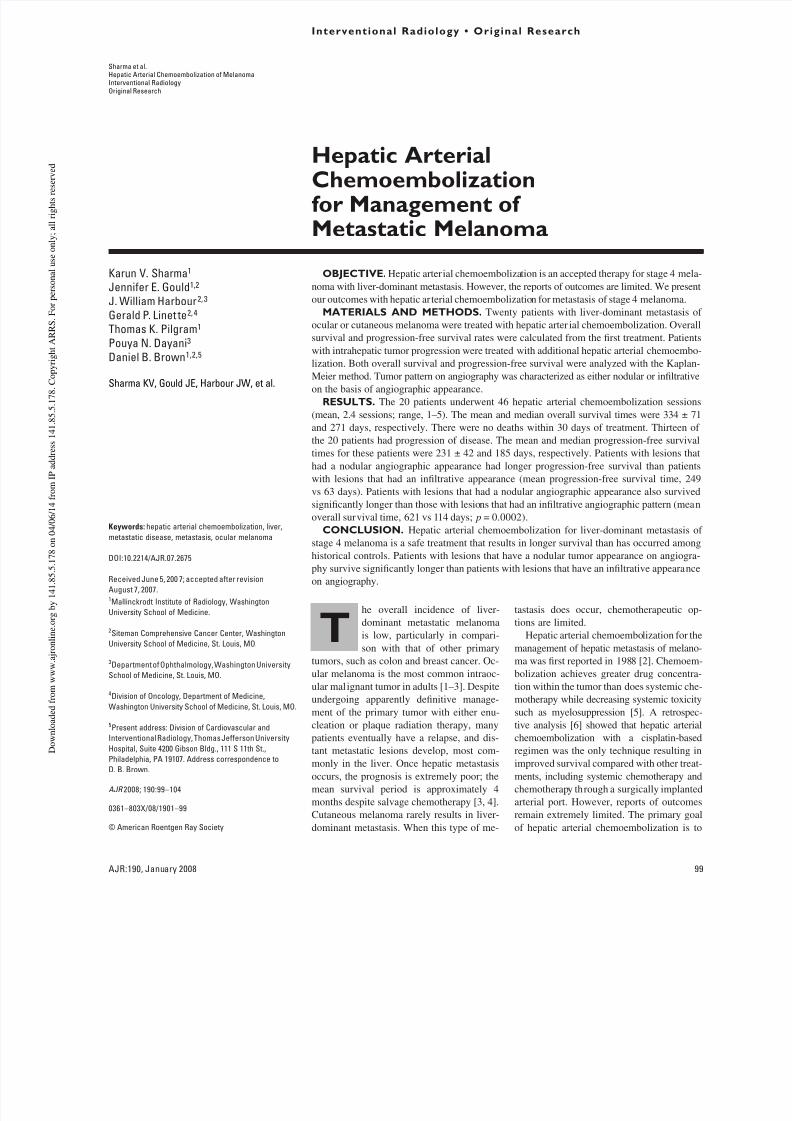
Fig. 2—Graph shows resultsof Kaplan-Meier analysis of
time to progression for entiregroup after hepatic arterialchemoembolization. Calcu-lated mean and median times
to progression were 231 ± 42and 185 days, respectively.
8/12/2019 Ha Tace for Mmlm 2008
http://slidepdf.com/reader/full/ha-tace-for-mmlm-2008 3/6
AJR:190 , January 200 8 101
Hepatic Arterial Chemoembolization of Melanoma
sented with bilobar disease with more than 10
tumors measurable on imaging. Most of the pa-
tients had too many tumors to count. The pa-
tient who was the exception had a solitary 8-cm
tumor in the right lobe of the liver and was
judged not a candidate for resection. One to five
hepatic arterial chemoembolization treatments
were performed per patient (mean, 2.4 treat-ments per patient). There were no deaths within
30 days of treatment and no complications ac-
cording to CTC version 3.0 criteria. Kaplan-
Meier analysis showed the mean and median
overall survival times for the group were
334 ± 71 and 271 days, respectively (range,
36–1,185 days) (Fig. 1). Six patients were alive
at the time of this writing, a median survival
time of 311 days (range, 141–1,185 days).
According to the Response Evaluation
Criteria in Solid Tumors, there were no com-
plete or partial responses. At initial follow-up,
13 (65%) of the patients had stable disease
and seven (35%) had progression. All seven
patients with progression at initial follow-up
died within 109 days. Of the 13 patients with
stable disease on initial imaging, six eventu-
ally had disease progression, for a total of 13
patients with progression of disease. The
mean and median progression-free survival
times for this group of patients were 231 ± 42and 185 days, respectively (Fig. 2).
Angiographic Appearance
Review of angiographic images showed
two distinct appearances of hepatic metastatic
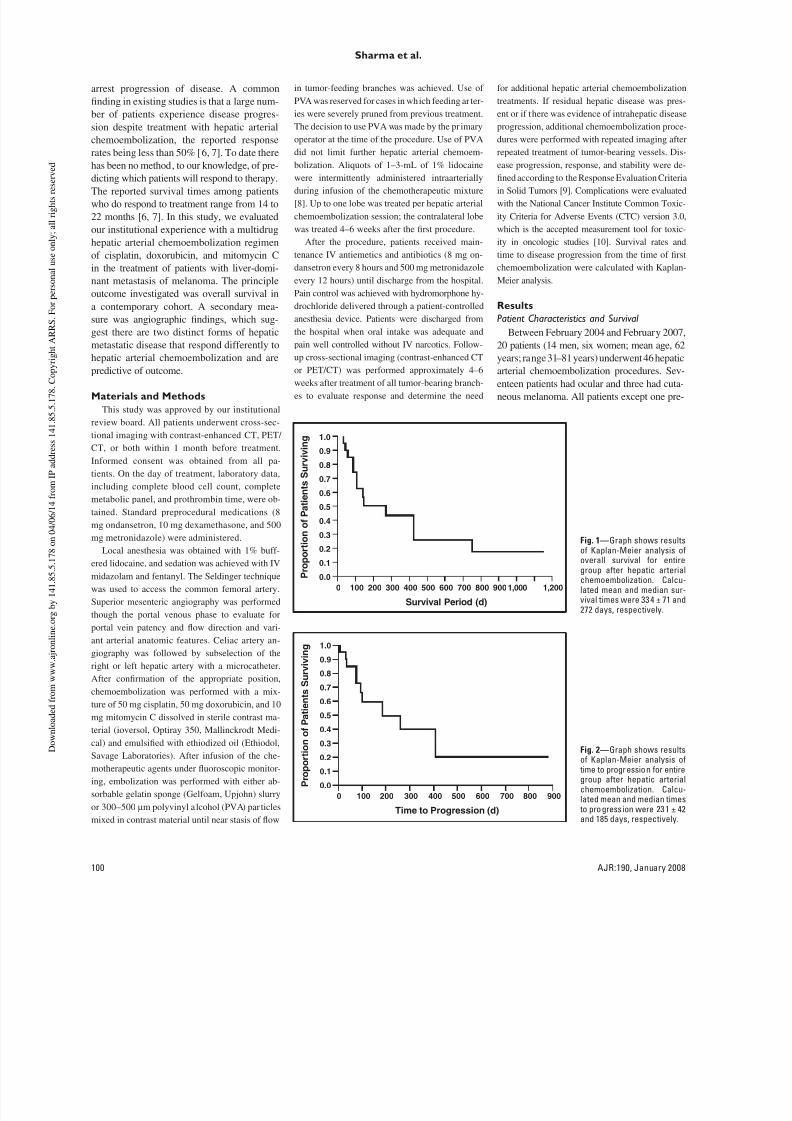
lesions. In one subset of patients (n = 8),
large nodular well-defined tumor masses
were present (Fig. 3). In the other subset of
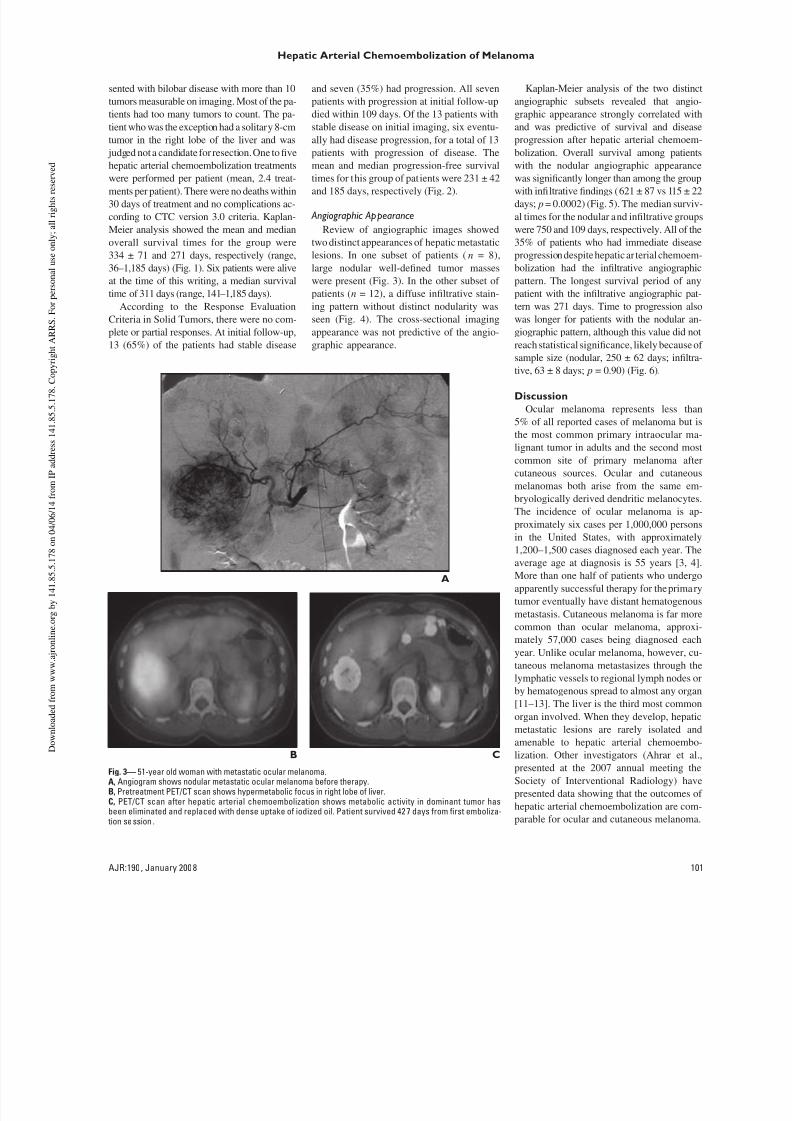
patients (n = 12), a diffuse infiltrative stain-
ing pattern without distinct nodularity was
seen (Fig. 4). The cross-sectional imaging
appearance was not predictive of the angio-
graphic appearance.
Kaplan-Meier analysis of the two distinct
angiographic subsets revealed that angio-
graphic appearance strongly correlated with
and was predictive of survival and disease
progression after hepatic arterial chemoem-
bolization. Overall survival among patients
with the nodular angiographic appearance
was significantly longer than among the groupwith infiltrative findings (621 ± 87 vs 115 ± 22
days; p = 0.0002) (Fig. 5). The median surviv-
al times for the nodular and infiltrative groups
were 750 and 109 days, respectively. All of the
35% of patients who had immediate disease
progression despite hepatic ar terial chemoem-
bolization had the infiltrative angiographic
pattern. The longest survival period of any
patient with the infiltrative angiographic pat-
tern was 271 days. Time to progression also
was longer for patients with the nodular an-
giographic pattern, although this value did not
reach statistical significance, likely because of
sample size (nodular, 250 ± 62 days; infiltra-
tive, 63 ± 8 days; p = 0.90) (Fig. 6).
dicuio
Ocular melanoma represents less than
5% of all reported cases of melanoma but is
the most common primary intraocular ma-
lignant tumor in adults and the second most
common site of primary melanoma after
cutaneous sources. Ocular and cutaneous
melanomas both arise from the same em-
bryologically derived dendritic melanocytes.
The incidence of ocular melanoma is ap-
proximately six cases per 1,000,000 personsin the United States, with approximately
1,200–1,500 cases diagnosed each year. The
average age at diagnosis is 55 years [3, 4].
More than one half of patients who undergo
apparently successful therapy for the primary
tumor eventually have distant hematogenous
metastasis. Cutaneous melanoma is far more
common than ocular melanoma, approxi-
mately 57,000 cases being diagnosed each
year. Unlike ocular melanoma, however, cu-
taneous melanoma metastasizes through the
lymphatic vessels to regional lymph nodes or
by hematogenous spread to almost any organ
[11–13]. The liver is the third most commonorgan involved. When they develop, hepatic
metastatic lesions are rarely isolated and
amenable to hepatic arterial chemoembo-
lization. Other investigators (Ahrar et al.,
presented at the 2007 annual meeting the
Society of Interventional Radiology) have
presented data showing that the outcomes of
hepatic arterial chemoembolization are com-
parable for ocular and cutaneous melanoma.
A
B C
Fig. 3— 51-year old woman with metastatic ocular melanoma.A, Angiogram shows nodular metastatic ocular melanoma before therapy.B, Pretreatment PET/CT scan shows hypermetabolic focus in right lobe of liver.C, PET/CT scan after hepatic arterial chemoembolization shows metabolic activity in dominant tumor hasbeen eliminated and replaced with dense uptake of iodized oil. Patient survived 42 7 days from first emboliza-
tion session .
8/12/2019 Ha Tace for Mmlm 2008
http://slidepdf.com/reader/full/ha-tace-for-mmlm-2008 4/6
102 AJR:19 0, January 200 8
shrm et .
Ocular melanoma has a high affinity for
metastasizing to the liver, which is usually
the first site of extraocular disease and is
involved in approximately 90% of patients.
In more than one half of patients with meta-
static disease, the liver may be the only or-
gan involved [14, 15]. The presence of he-
matogenous metastasis in the liver is a major
determinant of clinical course and patient
survival. Despite advances in the diagnosis
and management of primary uveal melano-ma, hepatic metastasis remains refractory to
standard oncologic therapies. Once hepatic
metastasis is diagnosed, the mean survival
time without treatment is only 2–3 months.
Treatment with systemic chemotherapy is
of limited value, the reported mean survival
time being approximately 4 months [16–18].
Surgical resection is rarely an option. Al-
though one study [19] showed an overall sur-
vival period of 27 months, less than 10% of
patients with hepatic metastasis in that study
were candidates for surgical resection.
In 1988, Mavligit et al. [2] first reported
management of ocular melanoma with he-patic arterial chemoembolization and cis-
platin and PVA particles. Those authors re-
ported a 46% radiologic response rate and
an 11-month median survival time for 30
patients with metastatic ocular melanoma. In
1995, the same group [6] reported their in-
stitutional experience comparing hepatic ar-
terial chemoembolization, systemic chemo-
therapy, and hepatic arterial chemotherapeu-
A B
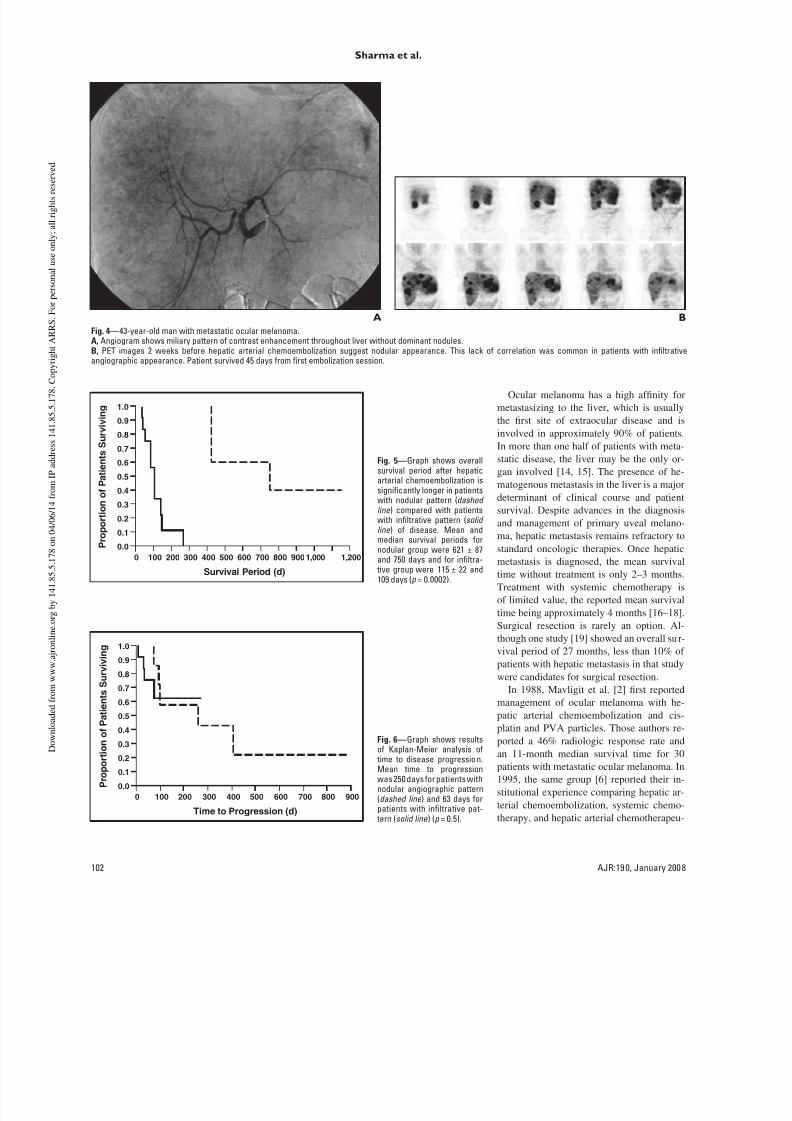
Fig. 4—43-year-old man with metastatic ocular melanoma.A, Angiogram shows miliary pattern of contrast enhancement throughout liver without dominant nodules.
B, PET images 2 weeks before hepatic arterial chemoembolization suggest nodular appearance. This lack of correlation was common in patients with infiltrativeangiographic appearance. Patient survived 45 days from first embolization session.
1.0
0.9
P r o p o
r t i o n
o f P a t i e n t s
S u r v i v i n g
Survival Period (d)
1,200
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
1,0009008007006005004003002001000
0.0
Fig. 5—Graph shows overallsurvival period after hepaticarterial chemoembolization issignificantly longer in patientswith nodular pattern (dashedline ) compared with patientswith infiltrative pattern (solidline ) of disease. Mean andmedian survival periods fornodular group were 621 ± 87and 750 days and for infiltra-
tive group were 115 ± 22 and109 days (p = 0.0002).
1.0
0.9
P r o p o r t i o n
o f P a t i e n
t s
S u r v i v i n g
Time to Progression (d)
900
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
8007006005004003002001000
0.0
Fig. 6—Graph shows resultsof Kaplan-Meier analysis of
time to disease progression.Mean time to progressionwas 250 days for patients withnodular angiographic pattern(dashed line ) and 63 days forpatients with infiltrative pat-
tern (solid line ) (p = 0.5).

8/12/2019 Ha Tace for Mmlm 2008
http://slidepdf.com/reader/full/ha-tace-for-mmlm-2008 5/6
AJR:190 , January 200 8 103
Hepatic Arterial Chemoembolization of Melanoma
tic infusion through a surgically implanted
port in the treatment of patients with meta-
static ocular melanoma. Only hepatic arterial
chemoembolization with the cisplatin-based
regimen produced a meaningful response
rate. Responders survived a median of 14.5
months; patients who underwent systemic
therapy survived 5 months. Not all patientsresponded to chemoembolization; that sub-
set survived a median of 5 months. This out-
come is similar to that among our group of
patients who did not respond to therapy.
Improved survival among patients with
metastatic uveal melanoma managed with
hepatic arterial chemoembolization and car-
mustine has been reported [7]. The overall
median survival time in that study was 5.2
months. However, patients with a radio-
graphic response had a median survival time
of nearly 22 months. Another treatment op-
tion attempted is direct hepatic arterial che-
motherapeutic infusion through a surgically
implanted port. Using fotemustine, Leyvraz
et al. [20] reported a response rate of 40%
and a median overall survival time of 14
months. Feldman et al. [21] and Grover and
Alexander [22] evaluated isolated hepatic
perfusion by infusing melphalan and captur-
ing the effluent from the hepatic vein. This
treatment led to a radiologic response in ap-
proximately 60% of patients and resulted in a
median survival period of 12 months. There
is much room for improvement in maximiz-
ing the percentage of patients who respond
and delaying the time to disease progressionand treatment failure. Other catheter-direct-
ed techniques, such as use of 90Y have not
been described but may be of value.
The results of the cur rent study show over-
all mean and median survival times of 271
and 334 ± 71 days among patients with liver-
dominant metastatic melanoma managed
with cisplatin–doxorubicin–mitomycin he-
patic arterial chemoembolization. We found
that compared with the findings in studies
of single-drug regimens, the multidrug regi-
men is extremely well tolerated without ad-
ditional toxicity. The survival period of our
group of patients is consistent with previ-ously reported median survival times of 5
and 11 months with carmustine and cisplatin
therapy, respectively.
An important finding of our study is rec-
ognition of two distinct angiographic pat-
terns of metastatic melanoma that appear to
be predictive of patient response and overall
survival after hepatic arterial chemoembo-
lization treatment. Patients with the nodu-
lar angiographic pattern were found to have
a favorable response to hepatic arterial
chemoembolization treatment, evidenced
by a median survival time of more than 2
years. Patients with the infiltrative angio-
graphic pattern, however, typically did not
have a favorable response to hepatic arterial
chemoembolization treatment, evidenced bya median survival time of only 115 days. We
believe that the strong correlation between
the observed angiographic pattern and sur-
vival benefit after hepatic arterial chemoem-
bolization may be valuable prognostic infor-
mation that can be used to help counsel and
guide the care of individual patients. Unfor-
tunately, the observed angiographic pattern
was not accurately predicted with pretreat-
ment contrast-enhanced CT or PET/CT.
Although it is possible that the nodular
pattern may represent an earlier pattern of
disease that eventually transforms into in-
filtrative disease, this evolution was not ob-
served in our cohort. The nodular and infil-
trative angiographic patterns may be related
to underlying differences in tumor genetics
that confer different biologic behavioral and
growth patterns that result in the observed
morphologic features. This hypothesis is
supported by results of gene expression pro-
file experiments showing that primary uveal
melanomas cluster into two distinct molecu-
lar classes. Results of this molecular classi-
fication into distinct low-grade (class 1) and
high-grade (class 2) groups are strongly pre-
dictive of metastatic death of patients withocular melanoma [4, 23–25]. It is tempting
to speculate that the differences in molecu-
lar class may be related to the differences in
angiographic pattern and response to hepatic
arterial chemoembolization treatment. To
further investigate this possibility, we are
obtaining hepatic arterial chemoemboliza-
tion before hepatic biopsy specimens for
gene profile analysis.
Deficiencies of this study were those in-
herent to a retrospective design and those re-
lated to small sample size. Our sample size,
however, was similar to those in other stud-
ies of hepatic arterial chemoembolization [2,7]. Given the size of the study group, we use
these findings as a way to counsel patients,
not to make decisions about whether therapy
should be offered. Our treatment group did
include two types of melanoma, but Ahrar et
al. (presented at the 2007 annual meeting the
Society of Interventional Radiology) found
similar survival data among patients with dif-
fering melanotic sources. The number of pa-
tients with cutaneous melanoma in our group
was too small for statistical comparison with
those with ocular melanoma. However, the
patients with cutaneous melanoma were not
outliers in median survival. The only two pa-
tients who survived more than 1,000 days in
our group had ocular melanoma.
Ocular melanoma is a rare tumor, and oncehepatic metastasis is diagnosed, patients are
faced with an extremely poor prognosis. He-
patic arterial chemoembolization of hepatic
metastatic lesions of melanoma was first re-
ported in the late 1980s and has been found
to be a safe, well-tolerated treatment option.
Unlike the well-reported outcome of hepatic
arterial chemoembolization for hepatocellu-
lar carcinoma, there is a relative lack of infor-
mation in the medical literature on outcome
after hepatic arterial chemoembolization
therapy for metastasis of hepatic melanoma.
In this study, we found improved survival
among patients with metastatic melanoma
managed with cisplatin–doxorubicin–mito-
mycin C hepatic arterial chemoembolization
compared with survival of historical controls
treated with systemic chemotherapy and sug-
gest that this outcome can be predicted on
the basis of angiographic pattern.
References
Harbour JW. Eye cancer: unique insights into onco-1.
genesis—the Cogan Lecture. Invest Ophthalmol
Vis Sci 2006; 47:1736–1745
Mavligit GM, Charnsangavej C, Carrasco CH, Patt2.
YZ, Benjamin RS, Wallace S. Regression of ocularmelanoma metastatic to the liver after hepatic arte-
rial chemoembolization with cisplatin and polyvi-
nyl sponge. JAMA 1988; 260:974–976
Singh AD, Topham A. Incidence of uveal melano-3.
ma in the United States: 1973–1997. Ophthalmolo-
gy 2003; 110:956–961
Singh AD, Borden EC. Metastatic uveal melanoma.4.
Ophthalmol Clin North Am 2005; 18:143–150
Stuart K. Chemoembolization in the management5.
of liver tumors. Oncologist 2003; 8:425–437
Bedikian AY, Legha SS, Mavligit G, et al. Treat-6.
ment of uveal melanoma metastatic to the liver: a
review of the M. D. Anderson Cancer Center expe-
rience and prognostic factors. Cancer 1995;
76:1665–1670
Patel K, Sullivan K, Berd D, et al. Chemoemboliza-7.
tion of the hepatic artery with BCNU for metastatic
uveal melanoma: results of a phase II study. Mela-
noma Res 2005; 15:297–304
Hartnell GG, Gates J, Stuart K, Underhill J, Brophy8.
DP. Hepatic chemoembolization: effect of intraarte-
rial lidocaine on pain and postprocedure recovery.
Cardiovasc Intervent Radiol 1999; 22:293–297

8/12/2019 Ha Tace for Mmlm 2008
http://slidepdf.com/reader/full/ha-tace-for-mmlm-2008 6/6
104 AJR:19 0, January 200 8
shrm et .
Therasse P, Arbuck SG, Eisenhauer EA, et al. New9.
guidelines to evaluate the response to treatment in
solid tumors. J Natl Cancer Inst 2000 ; 92:205–216
Trotti A, Colevas AD, Setser A, et al. CTCAE10.
v3.0: development of a comprehensive grading
system for the adverse effects of cancer treatment.
Semin Radiat Oncol 2003; 13:176–181
Balch CM. Surgical margins for melanoma: is 211.
cm too much? ANZ J Surg 2002; 72:251–252
Demierre MF. Epidemiology and prevention of12.
cutaneous melanoma. Curr Treat Options Oncol
2006; 7:181–186
Giblin AV, Thomas JM. Incidence, mortality and13.
survival in cutaneous melanoma. J Plast Reconstr
Aesthet Surg 2007; 60:32–40
Lorigan JG, Wallace S, Mavligit GM. The preva-14.
lence and location of metastases from ocular
melanoma: imaging study in 110 patients. AJR
1991; 157:1279–1281
Becker JC, Terheyden P, Kampgen E, et al. Treat-15.
ment of disseminated ocular melanoma with se-
quential fotemustine, interferon alpha, and inter-
leukin 2. Br J Cancer 2002; 87:840–845
Diener-West M, Hawkins BS, Markowitz JA,16.
Schachat AP. A review of mortality from choroidal
melanoma. Part II. A meta-analysis of 5-year mor-
tality rates following enucleation, 1966 through
1988. Arch Ophthalmol 1992; 110:245–250
Gragoudas ES, Egan KM, Seddon JM, et al. Sur-17.
vival of patients with metastases f rom uveal mela-
noma. Ophthalmology 1991; 98:383–389
Shields JA, Shields CL, De Potter P, Singh AD.18.
Diagnosis and treatment of uveal melanoma.
Semin Oncol 1996; 23:763–767
Aoyama T, Mastrangelo MJ, Berd D, et al. Pro-19.
tracted survival after resection of metastatic uveal
melanoma. Cancer 2000; 89:1561–1568
Leyvraz S, Spataro V, Bauer J, et al. Treatment of ocu-20.
lar melanoma metastatic to the liver by hepatic arterial
chemotherapy. J Clin Oncol 1997; 15:2589–2595
Feldman ED, Pingpank JF, Alexander HR Jr. Re-21.
gional treatment options for patients with ocular
melanoma metastatic to the l iver. Ann Surg Oncol
2004; 11:290–297
Grover A, Alexander HR Jr. The past decade of22.
experience with isolated hepatic perfusion. On-
cologist 2004; 9:653–664
Onken MD, Ehlers JP, Worley LA, Makita J, Yoko-23.
ta Y, Harbour JW. Functional gene expression anal-
ysis uncovers phenotypic switch in aggressive uveal
melanomas. Cancer Res 2006; 66:4602–4609
Onken MD, Worley LA, Davila RM, Char DH,24.
Harbour JW. Prognostic testing in uveal melano-
ma by transcriptomic profiling of fine needle bi-
opsy specimens. J Mol Diagn 2006; 8:567–573
Tschentscher F, Husing J, Holter T, et al. Tumor25.
classification based on gene expression profiling
shows that uveal melanomas with and without
monosomy 3 represent two distinct entities. Can-
cer Res 2003; 63:2578–2584