Embed Size (px)
Citation preview
Haematology for Clinical Finals
Paul Greaves: Consultant Haematologist, BHRUT, Romford
21 cases, 88 MCQs, and a framework to guide your cramming
The whole of haematology in 2 hours...In 21 cases, 88 MCQs and a framework to hang your cramming on...
Haematology is 5 things:
1. Clotting2. Transfusion3. Cancer4. Red cell5. Dire emergencies you must never mess up
CLOTTING is 5 things
1. PT, APTT and two ways to make a clot2. How to use heparin, warfarin and NOACs3. What to do with a bleeding patient taking anticoags4. Bleeding tendency5. Clotting tendency
TRANSFUSION is 5 things
1. Red cells: ABO, Rh and K2. Plasma3. Platelets (and thrombocytopenia)4. Tranexamic Acid5. Cryo, Fibrinogen, The stuff in a locked cupboard
➢ octaplex, novoseven, factor concentrates
CANCER (Leukaemia, Lymphoma, Myeloma, MPD) is 5 things1. Presentation
➢ lumps, organomegaly, bone marrow failure, infection
2. Diagnostics ➢ scans, bone marrow, biopsy, blood film, flow, cytogenetics
3. Treatment ➢ chemo, radio, targeted antibodies, targeted molecules
4. Supportive care➢ antiemetics, mouth-care, antimicrobials, bisphosphonates,
psychosocial
5. Emergencies➢ sepsis, tumour lysis, leukostasis, cord compression

RED CELL is 5 things
1. Haematinics2. Haemoglobin/opathy3. Haemolysis4. Haemochromatosis5.
5 things to NEVER MESS UP
1. Massive Transfusion and transfusion reactions2. Sepsis, Tumour Lysis & Hypercalcemia3. Cord Compression4. Sickle Chest crisis5. Dangerous thrombocytopenias
Never MissTumour lysis syndrome: Hyperphos, hypocalc, Oliguria
Prevent with allopurinol, rasburicase and generous IV fluidsCord Compression: Back pain, known malignancy (or suspected), neurology
Suspect with low index of suspicionSteroids (unless a new diagnosis), image, radiotherapy, neurosurgery
Thrombotic Thrombocytopenic PurpuraAnaemia, jaundice, thrombocytopenia, fever, renal fx, NeurologicalIV lines and straight to pheresis centre for PLEX +/- chemotherapy
Acute transfusion reactionUnwell on a transfusion -> STOP it, ?adrenaline neededcheck BAG, BAND, BLOOD; involve HDU, Hydrate, inform lab, send samples,
Never Miss: the dangerous thrombocytopeniasAlways ask for a blood film and check medication historyAre they bleeding? Or may they have a clot?Could they have a bone marrow failure or immunological syndrome?� Pregnancy-Associated
○ Liver function? Proteinuria? Hypertension?○ Think HELLP / Eclampsia spectrum
� Heparin Induced Thrombocytopenia & Thrombosis (HITT)� Thrombotic Thrombocytopenic Purpura (TTP)
○ Anaemia, jaundice, thrombocytopenia, fever, renal fx, Neurological○ IV lines and straight to pheresis centre for PLEX +/- chemotherapy
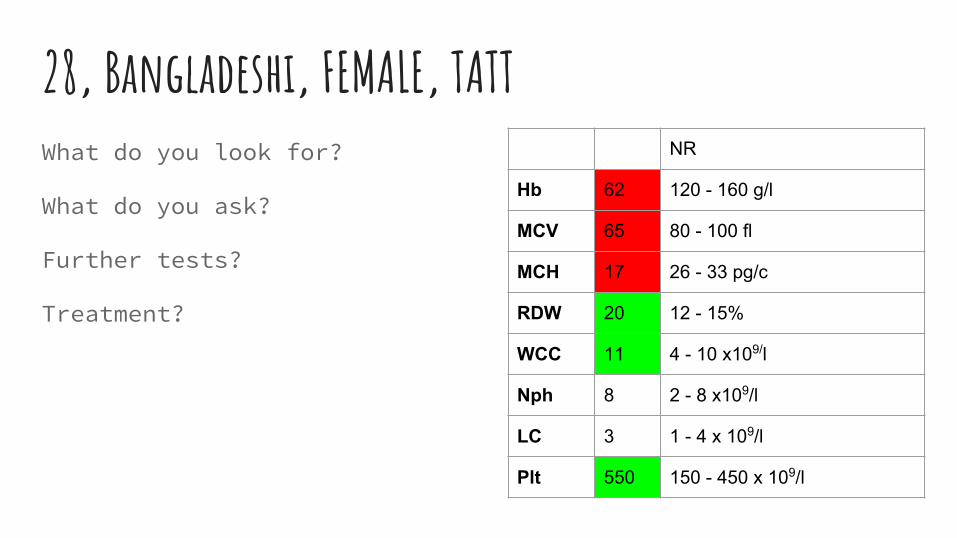
28, Bangladeshi, FEMALE, TATTWhat do you look for?
What do you ask?
Further tests?
Treatment?
NR
Hb 62 120 - 160 g/l
MCV 65 80 - 100 fl
MCH 17 26 - 33 pg/c
RDW 20 12 - 15%
WCC 11 4 - 10 x109/l
Nph 8 2 - 8 x109/l
LC 3 1 - 4 x 109/l
Plt 550 150 - 450 x 109/l
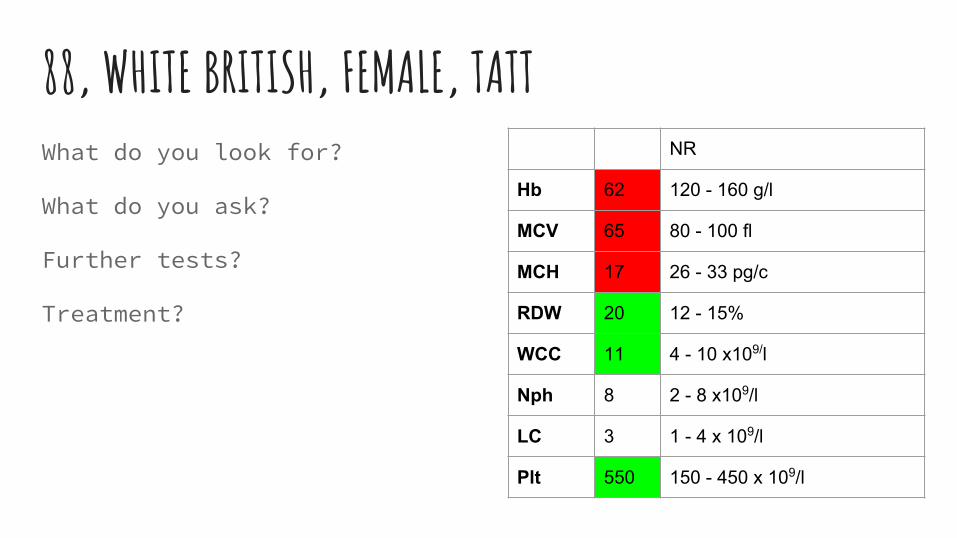
88, WHITE BRITISH, FEMALE, TATTWhat do you look for?
What do you ask?
Further tests?
Treatment?
NR
Hb 62 120 - 160 g/l
MCV 65 80 - 100 fl
MCH 17 26 - 33 pg/c
RDW 20 12 - 15%
WCC 11 4 - 10 x109/l
Nph 8 2 - 8 x109/l
LC 3 1 - 4 x 109/l
Plt 550 150 - 450 x 109/l
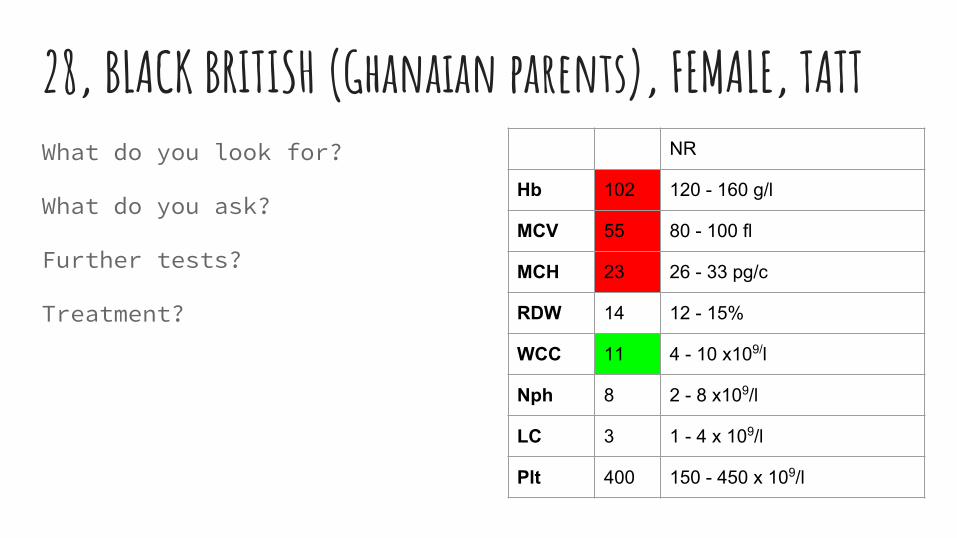
28, BLACK BRITISH (Ghanaian parents), FEMALE, TATTWhat do you look for?
What do you ask?
Further tests?
Treatment?
NR
Hb 102 120 - 160 g/l
MCV 55 80 - 100 fl
MCH 23 26 - 33 pg/c
RDW 14 12 - 15%
WCC 11 4 - 10 x109/l
Nph 8 2 - 8 x109/l
LC 3 1 - 4 x 109/l
Plt 400 150 - 450 x 109/l
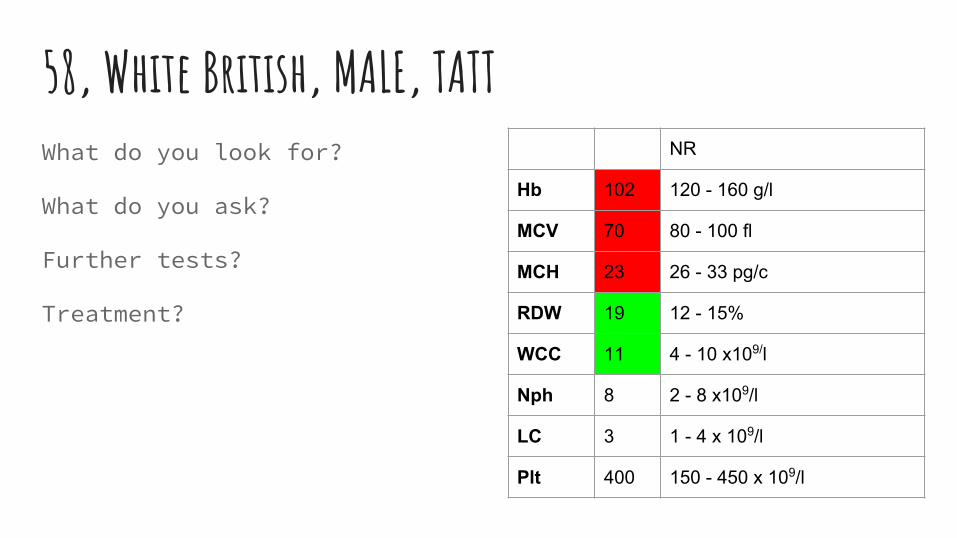
58, White British, MALE, TATTWhat do you look for?
What do you ask?
Further tests?
Treatment?
NR
Hb 102 120 - 160 g/l
MCV 70 80 - 100 fl
MCH 23 26 - 33 pg/c
RDW 19 12 - 15%
WCC 11 4 - 10 x109/l
Nph 8 2 - 8 x109/l
LC 3 1 - 4 x 109/l
Plt 400 150 - 450 x 109/l
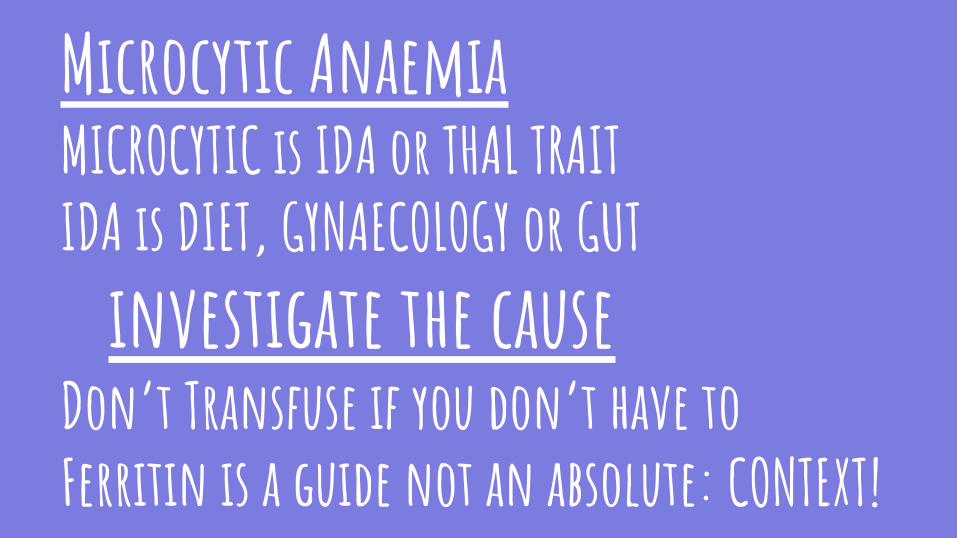
Microcytic AnaemiaMICROCYTIC is IDA or THAL TRAITIDA is DIET, GYNAECOLOGY or GUT
investigate the causeDon’t Transfuse if you don’t have toFerritin is a guide not an absolute: CONTEXT!
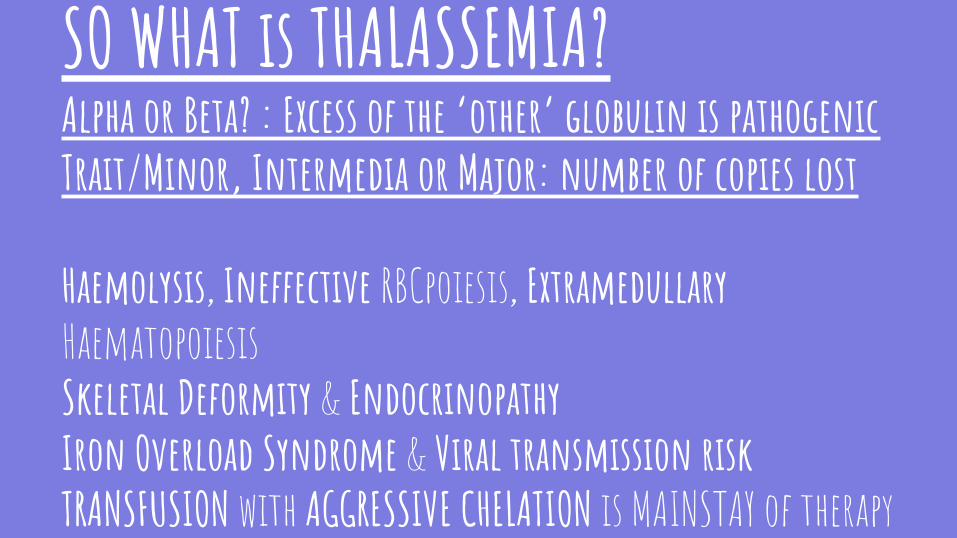
SO WHAT is THALASSEMIA?Alpha or Beta? : Excess of the ‘other’ globulin is pathogenicTrait/Minor, Intermedia or Major: number of copies lost
Haemolysis, Ineffective RBCpoiesis, Extramedullary HaematopoiesisSkeletal Deformity & EndocrinopathyIron Overload Syndrome & Viral transmission riskTRANSFUSION with AGGRESSIVE CHELATION is MAINSTAY of therapy
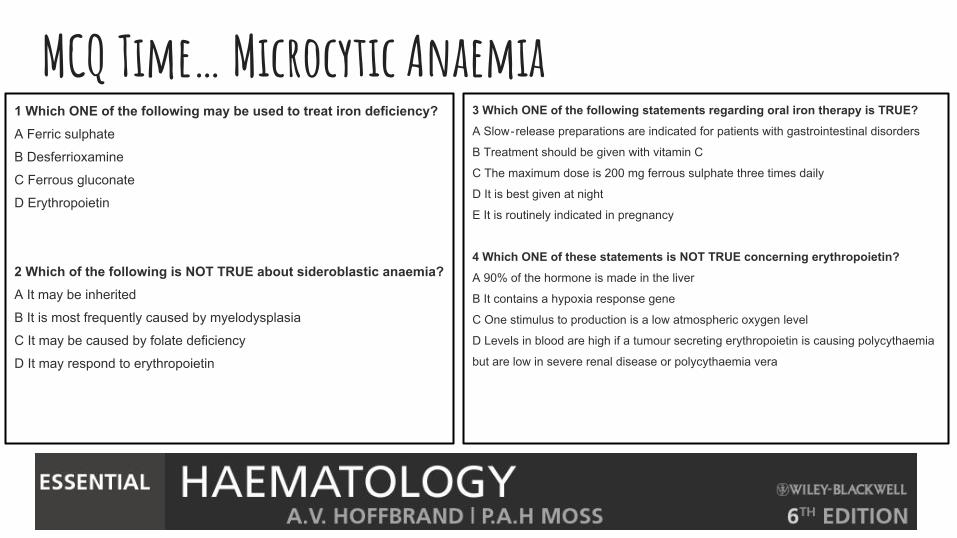
MCQ Time… Microcytic Anaemia1 Which ONE of the following may be used to treat iron deficiency?A Ferric sulphate
B Desferrioxamine
C Ferrous gluconate
D Erythropoietin
2 Which of the following is NOT TRUE about sideroblastic anaemia?A It may be inherited
B It is most frequently caused by myelodysplasia
C It may be caused by folate deficiency
D It may respond to erythropoietin
3 Which ONE of the following statements regarding oral iron therapy is TRUE?
A Slow‐release preparations are indicated for patients with gastrointestinal disorders
B Treatment should be given with vitamin C
C The maximum dose is 200 mg ferrous sulphate three times daily
D It is best given at night
E It is routinely indicated in pregnancy
4 Which ONE of these statements is NOT TRUE concerning erythropoietin?
A 90% of the hormone is made in the liver
B It contains a hypoxia response gene
C One stimulus to production is a low atmospheric oxygen level
D Levels in blood are high if a tumour secreting erythropoietin is causing polycythaemia
but are low in severe renal disease or polycythaemia vera
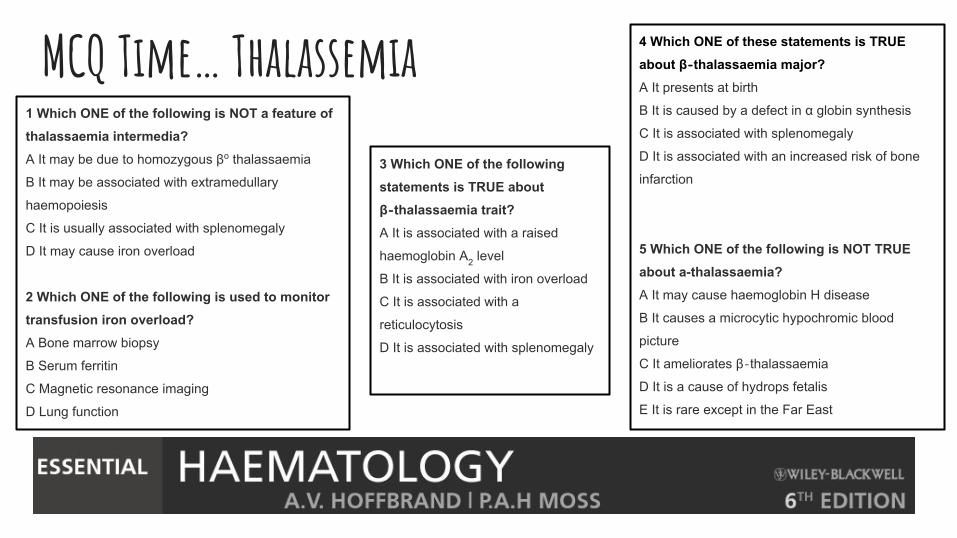
MCQ Time… Thalassemia1 Which ONE of the following is NOT a feature of thalassaemia intermedia?A It may be due to homozygous βo thalassaemia
B It may be associated with extramedullary
haemopoiesis
C It is usually associated with splenomegaly
D It may cause iron overload
2 Which ONE of the following is used to monitor transfusion iron overload?A Bone marrow biopsy
B Serum ferritin
C Magnetic resonance imaging
D Lung function
4 Which ONE of these statements is TRUE about β‐thalassaemia major?A It presents at birth
B It is caused by a defect in α globin synthesis
C It is associated with splenomegaly
D It is associated with an increased risk of bone
infarction
5 Which ONE of the following is NOT TRUE about a-thalassaemia?A It may cause haemoglobin H disease
B It causes a microcytic hypochromic blood
picture
C It ameliorates β‐thalassaemia
D It is a cause of hydrops fetalis
E It is rare except in the Far East
3 Which ONE of the following statements is TRUE about β‐thalassaemia trait?A It is associated with a raised
haemoglobin A2 level
B It is associated with iron overload
C It is associated with a
reticulocytosis
D It is associated with splenomegaly
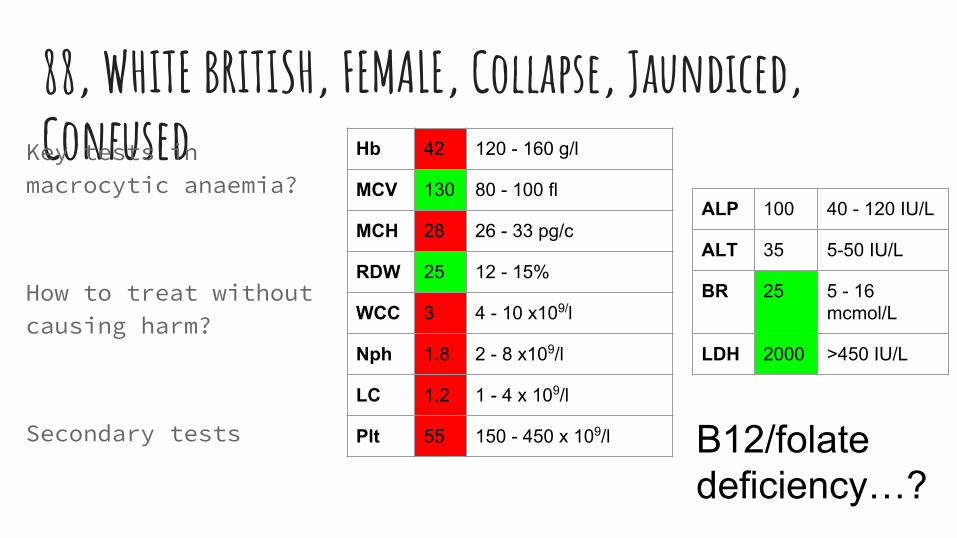
88, WHITE BRITISH, FEMALE, Collapse, Jaundiced, ConfusedKey tests in
macrocytic anaemia?
How to treat without causing harm?
Secondary tests
Hb 42 120 - 160 g/l
MCV 130 80 - 100 fl
MCH 28 26 - 33 pg/c
RDW 25 12 - 15%
WCC 3 4 - 10 x109/l
Nph 1.8 2 - 8 x109/l
LC 1.2 1 - 4 x 109/l
Plt 55 150 - 450 x 109/l B12/folate deficiency…?
ALP 100 40 - 120 IU/L
ALT 35 5-50 IU/L
BR 25 5 - 16 mcmol/L
LDH 2000 >450 IU/L
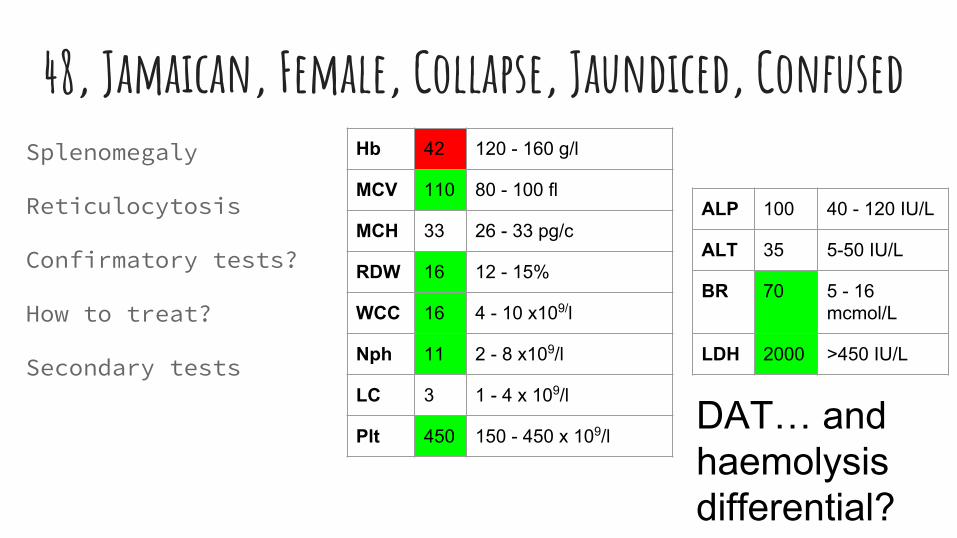
48, Jamaican, Female, Collapse, Jaundiced, ConfusedSplenomegaly
Reticulocytosis
Confirmatory tests?
How to treat?
Secondary tests
Hb 42 120 - 160 g/l
MCV 110 80 - 100 fl
MCH 33 26 - 33 pg/c
RDW 16 12 - 15%
WCC 16 4 - 10 x109/l
Nph 11 2 - 8 x109/l
LC 3 1 - 4 x 109/l
Plt 450 150 - 450 x 109/l
ALP 100 40 - 120 IU/L
ALT 35 5-50 IU/L
BR 70 5 - 16 mcmol/L
LDH 2000 >450 IU/L
DAT… and haemolysis differential?
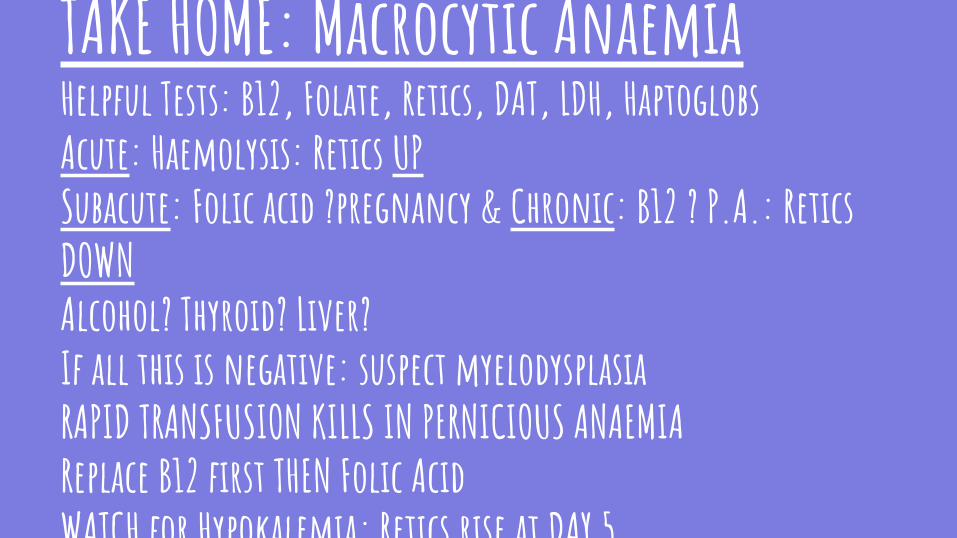
TAKE HOME: Macrocytic AnaemiaHelpful Tests: B12, Folate, Retics, DAT, LDH, HaptoglobsAcute: Haemolysis: Retics UPSubacute: Folic acid ?pregnancy & Chronic: B12 ? P.A.: Retics DOWNAlcohol? Thyroid? Liver?If all this is negative: suspect myelodysplasiaRAPID TRANSFUSION KILLS IN PERNICIOUS ANAEMIAReplace B12 first THEN Folic AcidWATCH for Hypokalemia; Retics rise at DAY 5
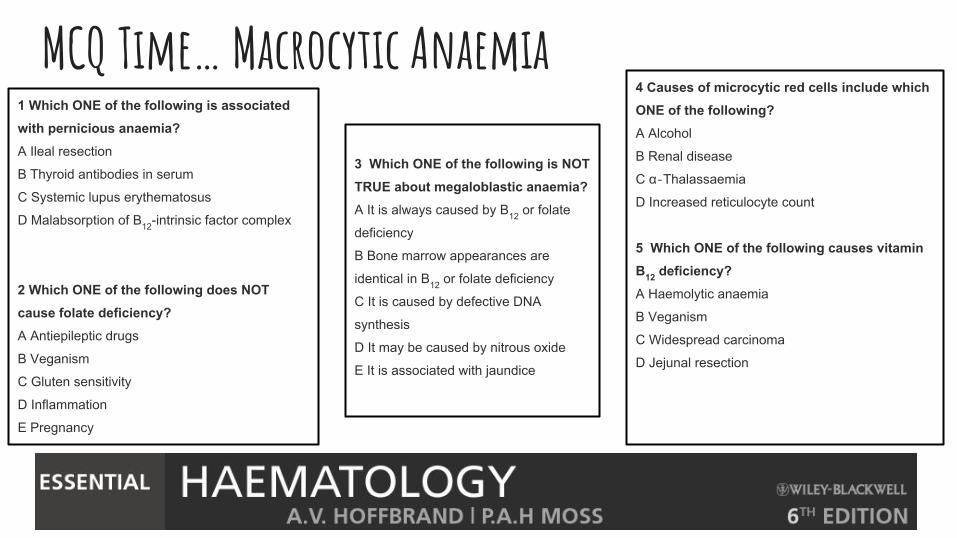
1 Which ONE of the following is associated with pernicious anaemia?A Ileal resection
B Thyroid antibodies in serum
C Systemic lupus erythematosus
D Malabsorption of B12-intrinsic factor complex
2 Which ONE of the following does NOT cause folate deficiency?A Antiepileptic drugs
B Veganism
C Gluten sensitivity
D Inflammation
E Pregnancy
MCQ Time… Macrocytic Anaemia4 Causes of microcytic red cells include which ONE of the following?A Alcohol
B Renal disease
C α‐Thalassaemia
D Increased reticulocyte count
5 Which ONE of the following causes vitamin B12 deficiency?A Haemolytic anaemia
B Veganism
C Widespread carcinoma
D Jejunal resection
3 Which ONE of the following is NOT TRUE about megaloblastic anaemia?A It is always caused by B12 or folate
deficiency
B Bone marrow appearances are
identical in B12 or folate deficiency
C It is caused by defective DNA
synthesis
D It may be caused by nitrous oxide
E It is associated with jaundice
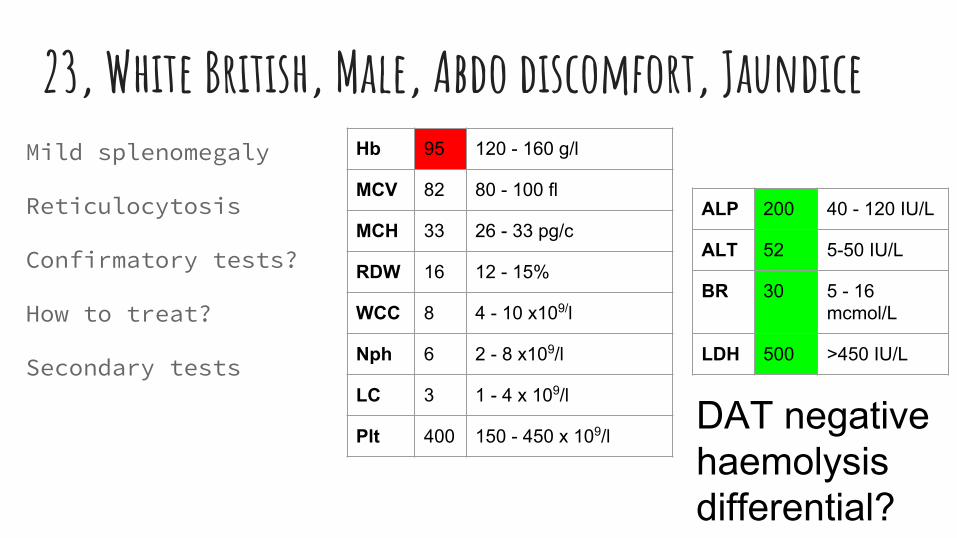
23, White British, Male, Abdo discomfort, JaundiceMild splenomegaly
Reticulocytosis
Confirmatory tests?
How to treat?
Secondary tests
Hb 95 120 - 160 g/l
MCV 82 80 - 100 fl
MCH 33 26 - 33 pg/c
RDW 16 12 - 15%
WCC 8 4 - 10 x109/l
Nph 6 2 - 8 x109/l
LC 3 1 - 4 x 109/l
Plt 400 150 - 450 x 109/l
ALP 200 40 - 120 IU/L
ALT 52 5-50 IU/L
BR 30 5 - 16 mcmol/L
LDH 500 >450 IU/L
DAT negative haemolysis differential?
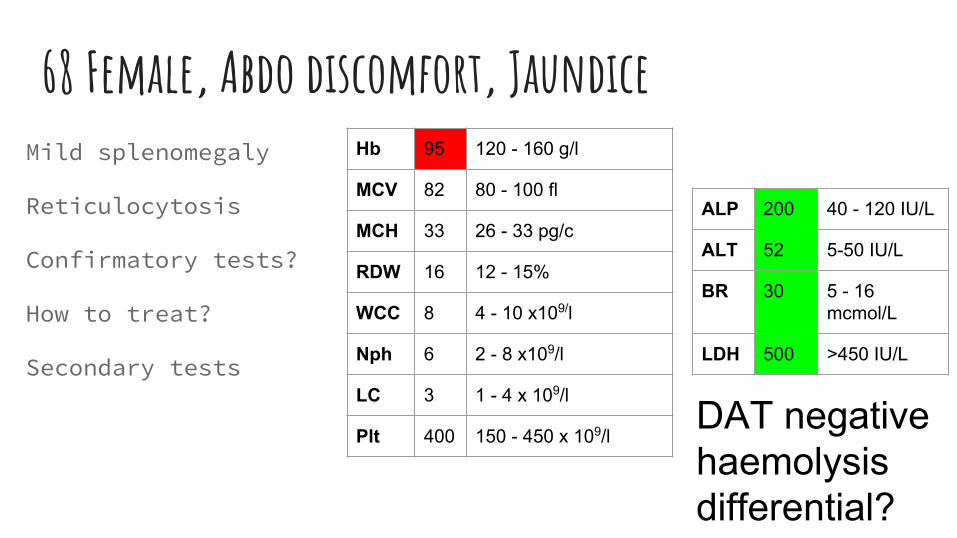
68 Female, Abdo discomfort, JaundiceMild splenomegaly
Reticulocytosis
Confirmatory tests?
How to treat?
Secondary tests
Hb 95 120 - 160 g/l
MCV 82 80 - 100 fl
MCH 33 26 - 33 pg/c
RDW 16 12 - 15%
WCC 8 4 - 10 x109/l
Nph 6 2 - 8 x109/l
LC 3 1 - 4 x 109/l
Plt 400 150 - 450 x 109/l
ALP 200 40 - 120 IU/L
ALT 52 5-50 IU/L
BR 30 5 - 16 mcmol/L
LDH 500 >450 IU/L
DAT negative haemolysis differential?
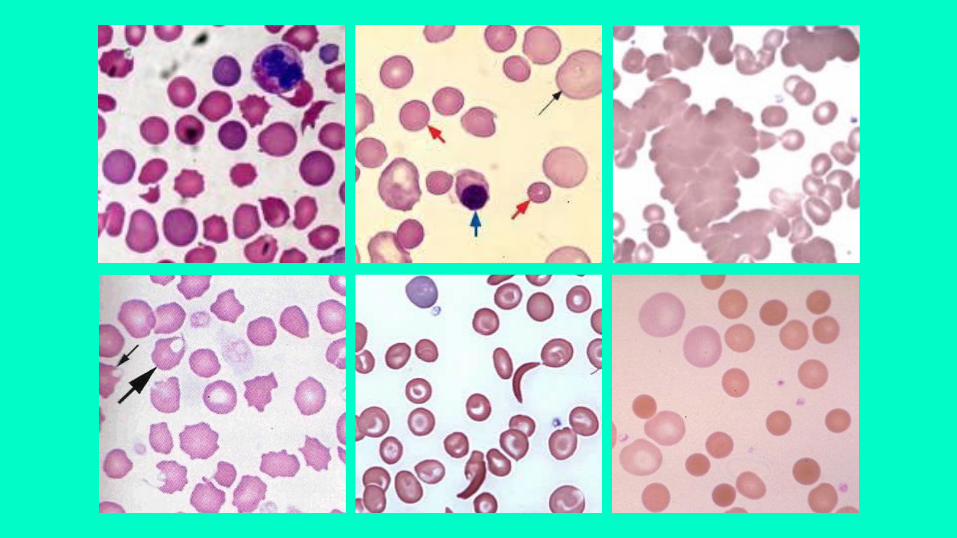
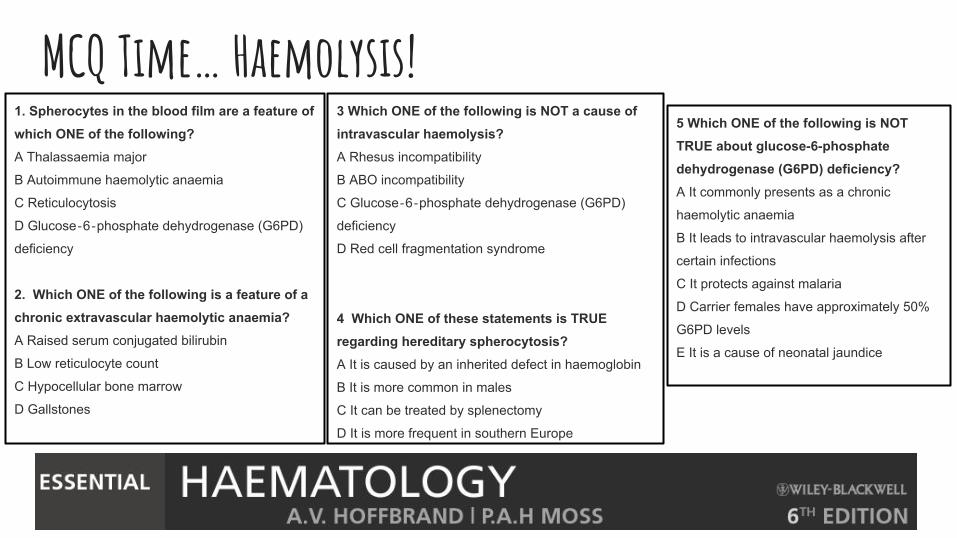
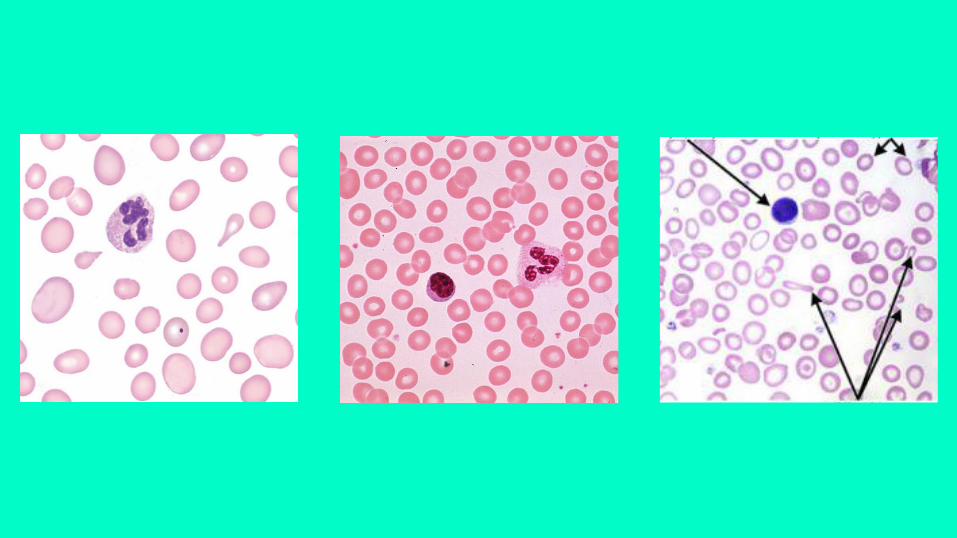
MCQ Time… Haemolysis!1. Spherocytes in the blood film are a feature of which ONE of the following?A Thalassaemia major
B Autoimmune haemolytic anaemia
C Reticulocytosis
D Glucose‐6‐phosphate dehydrogenase (G6PD)
deficiency
2. Which ONE of the following is a feature of a chronic extravascular haemolytic anaemia?A Raised serum conjugated bilirubin
B Low reticulocyte count
C Hypocellular bone marrow
D Gallstones
3 Which ONE of the following is NOT a cause of intravascular haemolysis?A Rhesus incompatibility
B ABO incompatibility
C Glucose‐6‐phosphate dehydrogenase (G6PD)
deficiency
D Red cell fragmentation syndrome
4 Which ONE of these statements is TRUE regarding hereditary spherocytosis?A It is caused by an inherited defect in haemoglobin
B It is more common in males
C It can be treated by splenectomy
D It is more frequent in southern Europe
5 Which ONE of the following is NOT TRUE about glucose-6-phosphate dehydrogenase (G6PD) deficiency?A It commonly presents as a chronic
haemolytic anaemia
B It leads to intravascular haemolysis after
certain infections
C It protects against malaria
D Carrier females have approximately 50%
G6PD levels
E It is a cause of neonatal jaundice
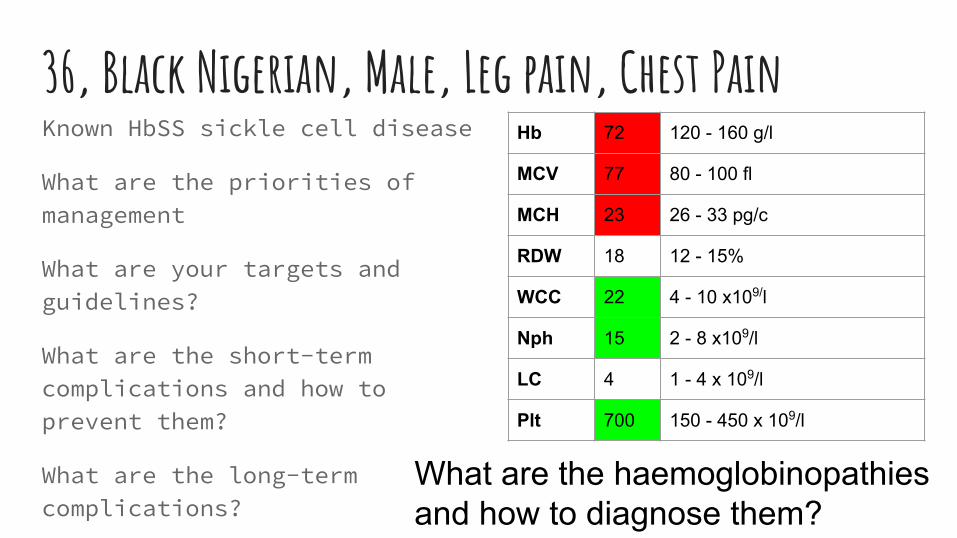
36, Black Nigerian, Male, Leg pain, Chest PainKnown HbSS sickle cell disease
What are the priorities of management
What are your targets and guidelines?
What are the short-term complications and how to prevent them?
What are the long-term complications?
Hb 72 120 - 160 g/l
MCV 77 80 - 100 fl
MCH 23 26 - 33 pg/c
RDW 18 12 - 15%
WCC 22 4 - 10 x109/l
Nph 15 2 - 8 x109/l
LC 4 1 - 4 x 109/l
Plt 700 150 - 450 x 109/l
What are the haemoglobinopathies and how to diagnose them?
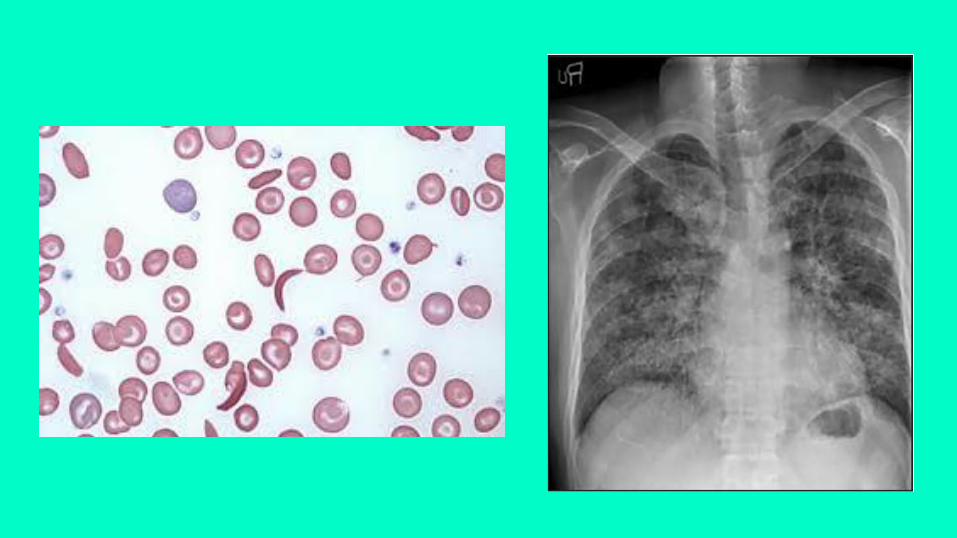
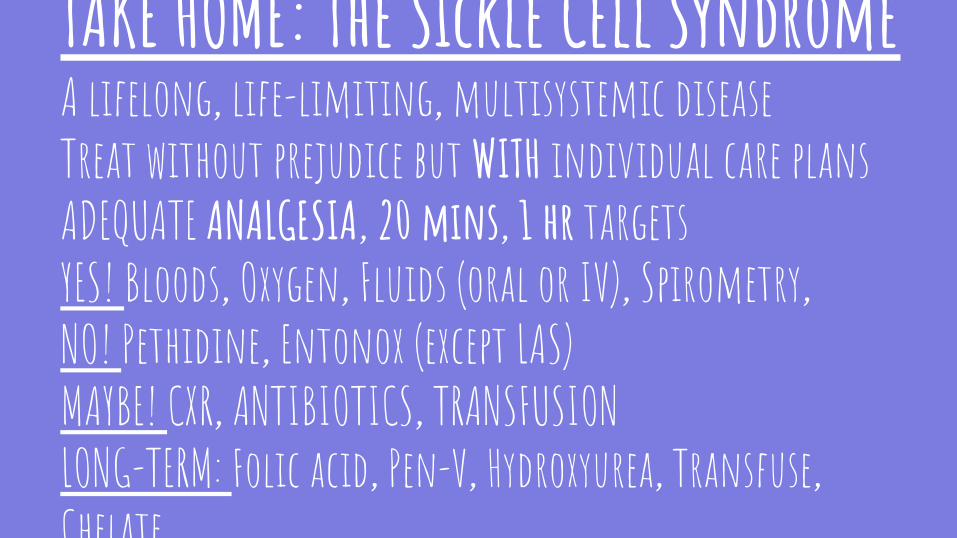
TAKE HOME: The Sickle Cell SyndromeA lifelong, life-limiting, multisystemic diseaseTreat without prejudice but WITH individual care plansADEQUATE ANALGESIA, 20 mins, 1 hr targetsYES! Bloods, Oxygen, Fluids (oral or IV), Spirometry, NO! Pethidine, Entonox (except LAS)MAYBE! CXR, ANTIBIOTICS, TRANSFUSIONLONG-TERM: Folic acid, Pen-V, Hydroxyurea, Transfuse, Chelate
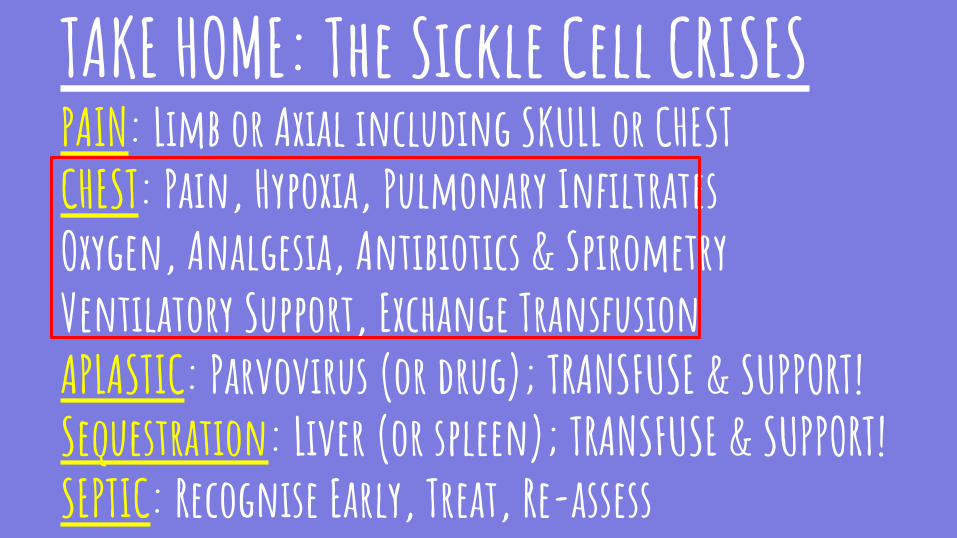
TAKE HOME: The Sickle Cell CRISESPAIN: Limb or Axial including SKULL or CHESTCHEST: Pain, Hypoxia, Pulmonary InfiltratesOxygen, Analgesia, Antibiotics & SpirometryVentilatory Support, Exchange TransfusionAPLASTIC: Parvovirus (or drug); TRANSFUSE & SUPPORT!Sequestration: Liver (or spleen); TRANSFUSE & SUPPORT!SEPTIC: Recognise Early, Treat, Re-assess
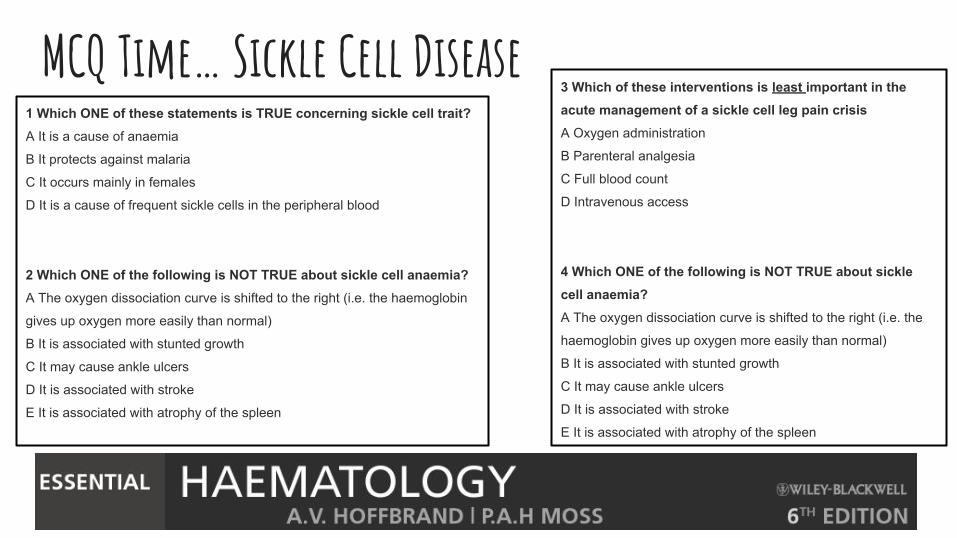
1 Which ONE of these statements is TRUE concerning sickle cell trait?A It is a cause of anaemia
B It protects against malaria
C It occurs mainly in females
D It is a cause of frequent sickle cells in the peripheral blood
2 Which ONE of the following is NOT TRUE about sickle cell anaemia?A The oxygen dissociation curve is shifted to the right (i.e. the haemoglobin
gives up oxygen more easily than normal)
B It is associated with stunted growth
C It may cause ankle ulcers
D It is associated with stroke
E It is associated with atrophy of the spleen
MCQ Time… Sickle Cell Disease3 Which of these interventions is least important in the acute management of a sickle cell leg pain crisisA Oxygen administration
B Parenteral analgesia
C Full blood count
D Intravenous access
4 Which ONE of the following is NOT TRUE about sickle cell anaemia?A The oxygen dissociation curve is shifted to the right (i.e. the
haemoglobin gives up oxygen more easily than normal)
B It is associated with stunted growth
C It may cause ankle ulcers
D It is associated with stroke
E It is associated with atrophy of the spleen
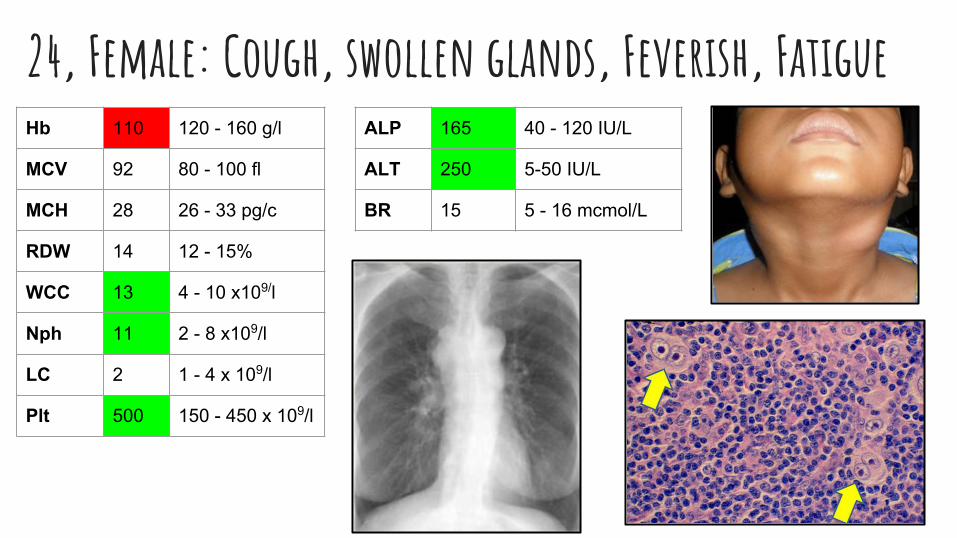
24, Female: Cough, swollen glands, Feverish, FatigueHb 110 120 - 160 g/l
MCV 92 80 - 100 fl
MCH 28 26 - 33 pg/c
RDW 14 12 - 15%
WCC 13 4 - 10 x109/l
Nph 11 2 - 8 x109/l
LC 2 1 - 4 x 109/l
Plt 500 150 - 450 x 109/l
ALP 165 40 - 120 IU/L
ALT 250 5-50 IU/L
BR 15 5 - 16 mcmol/L
EVERYONE needs:a biopsy - Lymph node, bone marrowFBC: Marrow failure often a complicationChemistry: Tumor lysis, Calcium, Liver infiltration, Fitness for treatmentHIV and Hepatitis status checkAutoimmune and thyroid
Staging / Prognostication:IMAGING: LYMPHOMA: CT and ‘functional’ PET-CTMyeloma: Skeletal survey, MRI spineMolecular: Immunophenotyping defines cell typeCytogenetics determines prognosis
Haematological Malignancy
SUPPORTIVE CARE: Antimicrobials, BMFx, Analgesia, Mouthcare, Antiemetics, Anti-TLSx
Non-Hodgkin: CommonUSUALLY B CELL, High Grade or Low Grade
High Grade = DLBCLLow Grade = Follicular lymphomaLow grade + IgM paraprotein =
LPCLymphomaSometimes T cell (10%) = RASHES and BAD NEWSBURKITT’s - rare super-highgrade, EBV3 types: Sporadic (elderly); Endemic (Africa, jaw, kids); HIV / immunosuppression associatedTargeted antibody: RITUXIMAB (CD20)
TAKE HOME: Lymphomas
Hodgkin: Rare (NLPHL RARER)Teens and twenties PLUS elderlyReed Sternberg cells; 30% EBV+Histological subtypes x4 (usu NS or MC)Targeted antibody: Brentuximab (CD30)Staged and treated the same!Biopsy, CT or PET-CT: Anne Arbor stageChemotherapy mainstayRadiotherapy for localisedBM Transplant for relapse
MCQ Time… Lymphoma1 Which ONE of these is most useful in the staging of Hodgkin's lymphoma?A Clinical examination
B Erythrocyte sedimentation rate and
lactic dehydrogenase
C Bone marrow trephine
D CT scan
2 What percentage of patients are cured of Hodgkin's lymphoma?A 55
B 65
C 75
D 85
3 Which ONE of these is NOT TRUE concerning positron emission tomography (PET) scanning in Hodgkin's lymphoma?A The radiolabel emits β‐particles
B The images reflect tissue metabolic activity
C Predicts disease response if performed after only 1 course of
treatment
D Often upstages Stage I/II disease to stage III/IV
4 A 65-year-old woman has had a swelling in the neck for 9 months. She is otherwise well with a normal FBC. Most likely diagnosis?A Diffuse large B‐cell lymphoma
B Follicular lymphoma
C Sézary syndrome
D Toxoplasmosis
5 A 60‐year‐old man presents with headaches and anaemia. Investigations reveal an IgM paraprotein of 30 g/L. What is the most likely diagnosis?A Burkitt's lymphoma
B Follicular lymphoma
C Mycosis fungoides
D Lymphoplasmacytic lymphoma
6 A 6‐year‐old boy in Kenya develops swelling of the jaw. The mass responds rapidly to chemotherapy. What is the most likely diagnosis?A Burkitt's lymphoma
B Follicular lymphoma
C Mycosis fungoides
D Lymphoblastic lymphoma
MCQ Time… Malignancy Supportive 11 Which ONE of these is NOT TRUE concerning central venous catheters used in patients with haematological malignancies?
A They are associated with increased
risk of Gram‐positive septicaemia
B They can be used to take blood
and administer intravenous drugs
C Chest X‐ray can be used to check
the position of the catheter
D It is usually placed in the inferior
vena cava
2 Which ONE of these is TRUE concerning blood product support for patients undergoing treatment for haematological malignancy?A If a patient has recently received
fludarabine chemotherapy, any blood
products should be irradiated before
administration
B Platelet counts should generally be
maintained above 20.109/L
C The haemoglobin concentration should be
kept within the normal range for age and
gender
D Human albumin is useful for the
management of bleeding disorders
3 Which ONE of these is TRUE regarding fertility in relation to treatment for malignancy?
A Initial chemotherapy for Hodgkin's lymphoma does not usually
make women infertile
B Total body irradiation, which is used as conditioning for bone
marrow transplantation, does not permanently impair fertility
C It is easier to freeze oocytes rather than fertilized embryos
D Sperm donation is rarely a priority in young men who require
chemotherapy
4 Which ONE of these drugs is most valuable as an antiemetic drug?
A Methotrexate
B Ondansetron
C Piriton
D Tranexamic acid
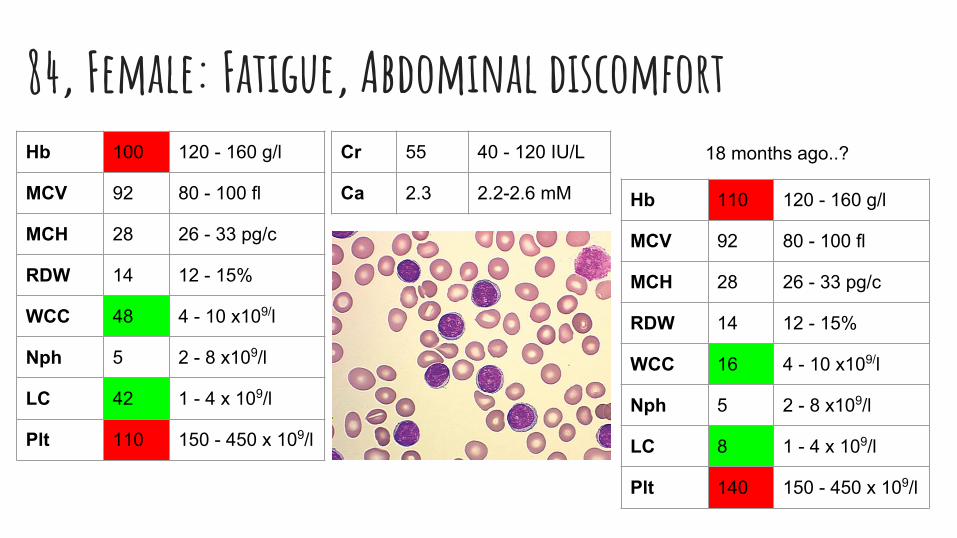
84, Female: Fatigue, Abdominal discomfortHb 100 120 - 160 g/l
MCV 92 80 - 100 fl
MCH 28 26 - 33 pg/c
RDW 14 12 - 15%
WCC 48 4 - 10 x109/l
Nph 5 2 - 8 x109/l
LC 42 1 - 4 x 109/l
Plt 110 150 - 450 x 109/l
Cr 55 40 - 120 IU/L
Ca 2.3 2.2-2.6 mM Hb 110 120 - 160 g/l
MCV 92 80 - 100 fl
MCH 28 26 - 33 pg/c
RDW 14 12 - 15%
WCC 16 4 - 10 x109/l
Nph 5 2 - 8 x109/l
LC 8 1 - 4 x 109/l
Plt 140 150 - 450 x 109/l
18 months ago..?
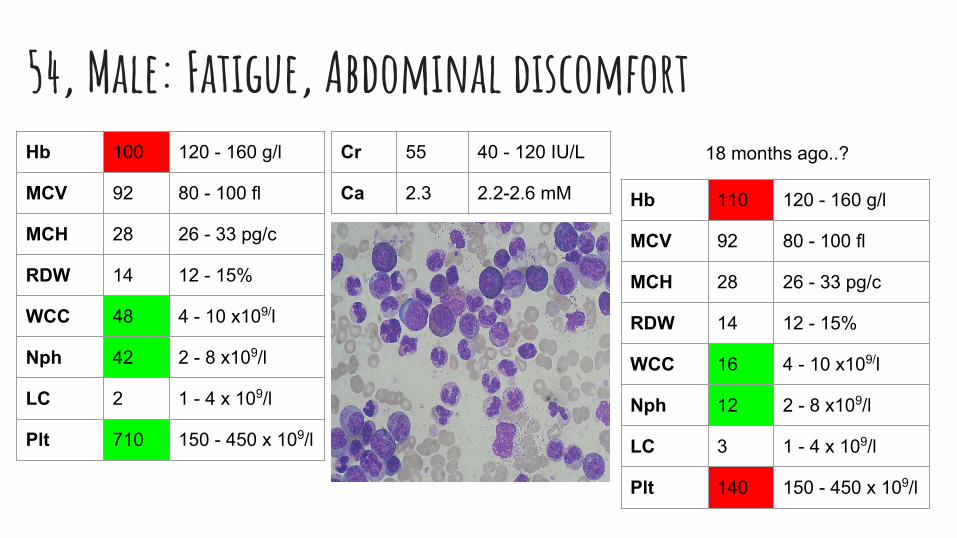
54, Male: Fatigue, Abdominal discomfortHb 100 120 - 160 g/l
MCV 92 80 - 100 fl
MCH 28 26 - 33 pg/c
RDW 14 12 - 15%
WCC 48 4 - 10 x109/l
Nph 42 2 - 8 x109/l
LC 2 1 - 4 x 109/l
Plt 710 150 - 450 x 109/l
Cr 55 40 - 120 IU/L
Ca 2.3 2.2-2.6 mM Hb 110 120 - 160 g/l
MCV 92 80 - 100 fl
MCH 28 26 - 33 pg/c
RDW 14 12 - 15%
WCC 16 4 - 10 x109/l
Nph 12 2 - 8 x109/l
LC 3 1 - 4 x 109/l
Plt 140 150 - 450 x 109/l
18 months ago..?
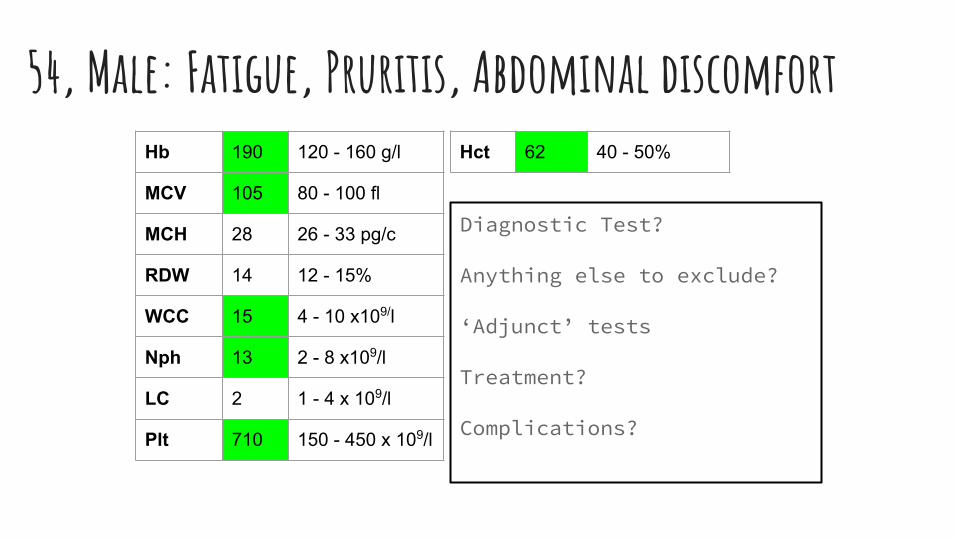
54, Male: Fatigue, Pruritis, Abdominal discomfortHb 190 120 - 160 g/l
MCV 105 80 - 100 fl
MCH 28 26 - 33 pg/c
RDW 14 12 - 15%
WCC 15 4 - 10 x109/l
Nph 13 2 - 8 x109/l
LC 2 1 - 4 x 109/l
Plt 710 150 - 450 x 109/l
Hct 62 40 - 50%
Diagnostic Test?
Anything else to exclude?
‘Adjunct’ tests
Treatment?
Complications?
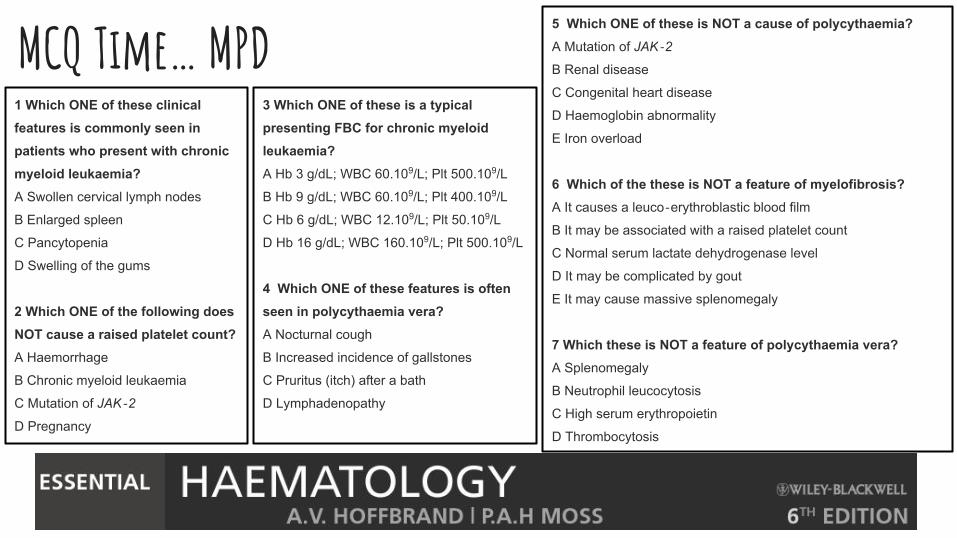
MCQ Time… MPD1 Which ONE of these clinical features is commonly seen in patients who present with chronic myeloid leukaemia?A Swollen cervical lymph nodes
B Enlarged spleen
C Pancytopenia
D Swelling of the gums
2 Which ONE of the following does NOT cause a raised platelet count?A Haemorrhage
B Chronic myeloid leukaemia
C Mutation of JAK‐2
D Pregnancy
5 Which ONE of these is NOT a cause of polycythaemia?A Mutation of JAK‐2
B Renal disease
C Congenital heart disease
D Haemoglobin abnormality
E Iron overload
6 Which of the these is NOT a feature of myelofibrosis?A It causes a leuco‐erythroblastic blood film
B It may be associated with a raised platelet count
C Normal serum lactate dehydrogenase level
D It may be complicated by gout
E It may cause massive splenomegaly
7 Which these is NOT a feature of polycythaemia vera?A Splenomegaly
B Neutrophil leucocytosis
C High serum erythropoietin
D Thrombocytosis
3 Which ONE of these is a typical presenting FBC for chronic myeloid leukaemia?A Hb 3 g/dL; WBC 60.109/L; Plt 500.109/L
B Hb 9 g/dL; WBC 60.109/L; Plt 400.109/L
C Hb 6 g/dL; WBC 12.109/L; Plt 50.109/L
D Hb 16 g/dL; WBC 160.109/L; Plt 500.109/L
4 Which ONE of these features is often seen in polycythaemia vera?A Nocturnal cough
B Increased incidence of gallstones
C Pruritus (itch) after a bath
D Lymphadenopathy
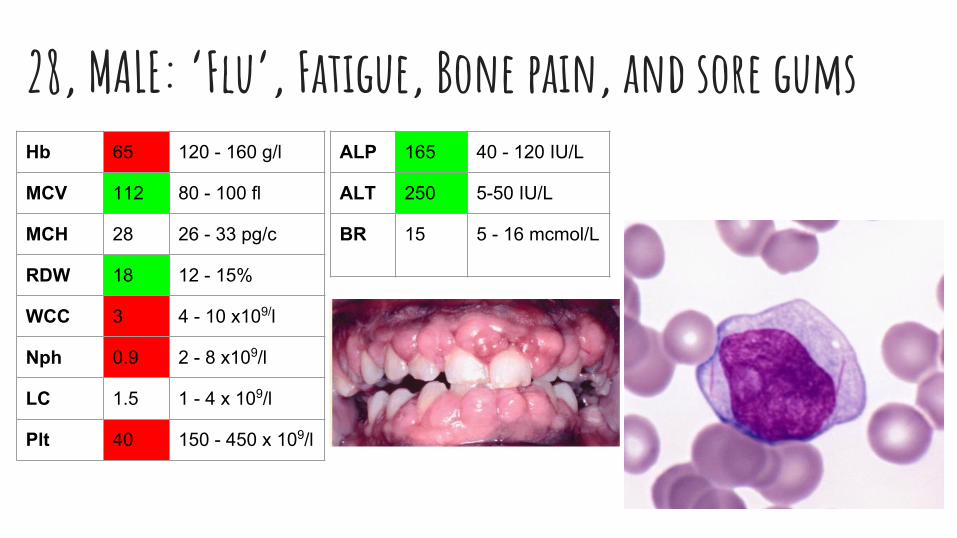
28, MALE: ‘Flu’, Fatigue, Bone pain, and sore gumsHb 65 120 - 160 g/l
MCV 112 80 - 100 fl
MCH 28 26 - 33 pg/c
RDW 18 12 - 15%
WCC 3 4 - 10 x109/l
Nph 0.9 2 - 8 x109/l
LC 1.5 1 - 4 x 109/l
Plt 40 150 - 450 x 109/l
ALP 165 40 - 120 IU/L
ALT 250 5-50 IU/L
BR 15 5 - 16 mcmol/L
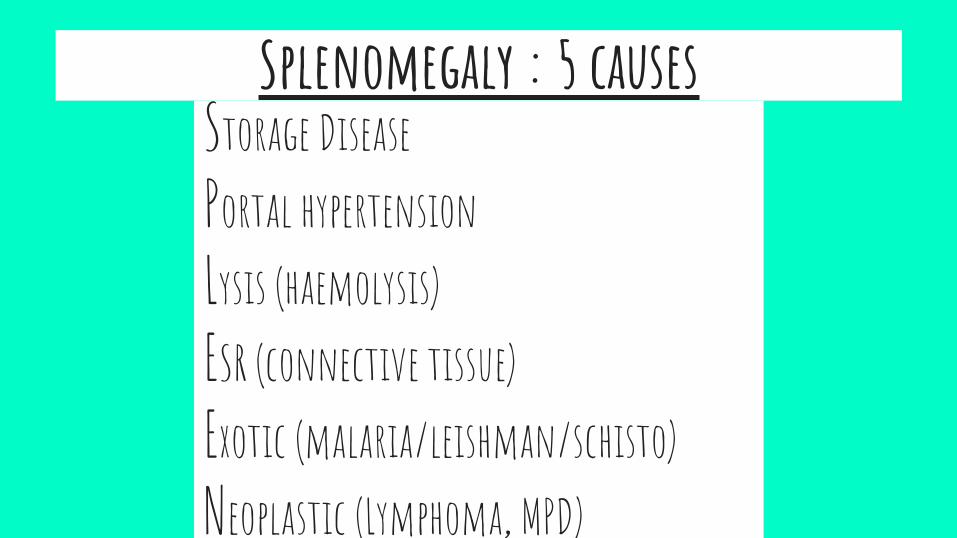
1. Myeloid Malignancy2. Chronic Haemolysis3. Storage Disease4. Portal hypertension5. Systemic disease: Infection /
Connective tissue
Splenomegaly : 5 causesStorage DiseasePortal hypertensionLysis (haemolysis)ESR (connective tissue)Exotic (malaria/leishman/schisto)Neoplastic (Lymphoma, MPD)
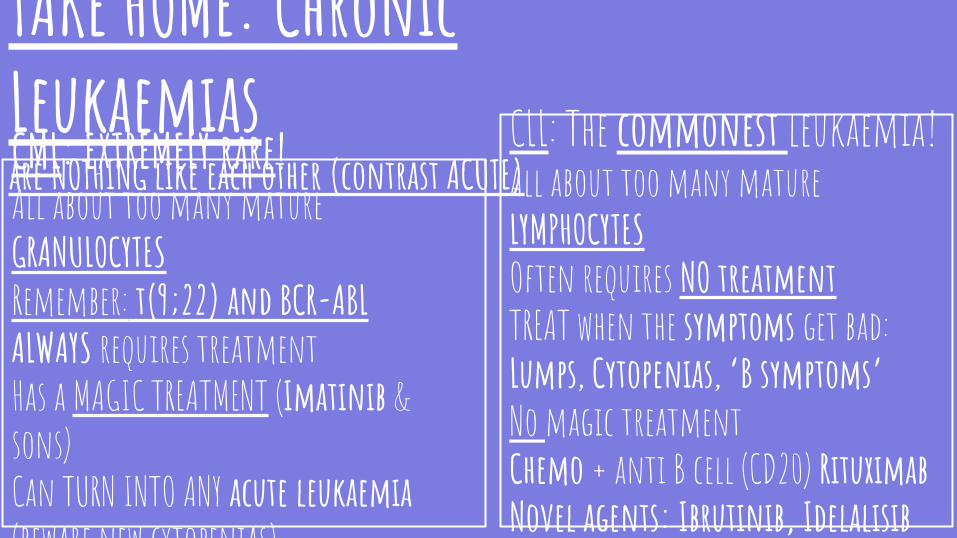
CLL: The commonest leukaemia!All about too many mature LYMPHOCYTES Often requires NO treatmentTREAT when the symptoms get bad: Lumps, Cytopenias, ‘B symptoms’No magic treatmentChemo + anti B cell (CD20) RituximabNovel agents: Ibrutinib, Idelalisib
CML: EXTREMELY rare!All about too many mature GRANULOCYTESRemember: t(9;22) and BCR-ABLALWAYS requires treatmentHas a MAGIC TREATMENT (Imatinib & sons)Can TURN INTO ANY acute leukaemia (beware new cytopenias)
TAKE HOME: Chronic Leukaemiasare NOTHING like each other (contrast ACUTE)
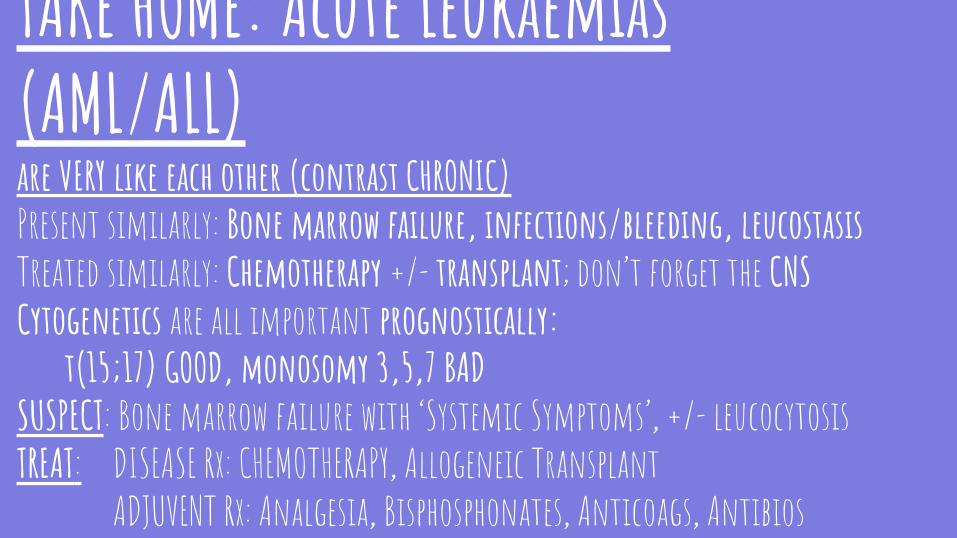
TAKE HOME: Acute Leukaemias (AML/ALL)are VERY like each other (contrast CHRONIC)Present similarly: Bone marrow failure, infections/bleeding, leucostasis Treated similarly: Chemotherapy +/- transplant; don’t forget the CNSCytogenetics are all important prognostically:
t(15;17) GOOD, monosomy 3,5,7 BADSUSPECT: Bone marrow failure with ‘Systemic Symptoms’, +/- leucocytosisTREAT: DISEASE Rx: CHEMOTHERAPY, Allogeneic Transplant
ADJUVENT Rx: Analgesia, Bisphosphonates, Anticoags, AntibiosBEWARE!: Leucostasis, Tumor Lysis, Coagulopathy
MCQ Time… Leukaemia1 Which ONE of these statements is most accurate concerning the approximate long-term cure rate for acute myeloid leukaemia?A It is 30% at all ages
B It is 60% in those aged <60 years and 30% thereafter
C It is 60% in those aged <60 years and 10% thereafter
D It is 30% in those aged <60 years and 10% thereafter
2 Which ONE of these is used in treatment of relapsed acute myeloid leukaemia?A Arsenic
B Digoxin
C Cyanide
D Atropa belladonna
3 Which ONE of the following is NOT TRUE about acute myeloid leukaemia?
A It may cause pancytopenia
B It has a cure rate of >80% in some
subtypes
C Allogeneic stem cell transplantation is
needed in all patients less than 50 years
old with an HLA‐matched donor
D It may follow myelodysplasia
E It may cause swelling of the gums
4 Which ONE of these is the MOST LIKELY blood count in a patient who presents with acute myeloid leukaemia?A Hb 14 g/dL; white blood cell count (WBC)
270.109/L; platelets 100.109/L
B Hb 9 g/dL; WBC 2.109/L; platelets 140.109/L
C Hb 9 g/dL; WBC 27.109/L; platelets 10.109/L
D Hb 14 g/dL; WBC 270.109/L; platelets
1000.109/L
5 Which ONE of these genetic abnormalities defines a patient with acute myeloid leukaemia as having an unfavourable prognosis?A t(8;21) translocation
B Normal karyotype
C Translocation of NPM gene
D Deletion of chromosome 7
Aplastic Anaemia:Sometimes curable Disease of Mid-AgeAutoimmune mechanismDoes not evolve to AML Treatment:Immunosuppression (ATG/CSA) + BMT
TAKE HOME: Bone Marrow Failure SyndromesEXCLUDE CONGENITAL and secondary causes: Nutritional/Viral/Toxin/Radiation
Myelodysplastic syndrome:Generally incurable Disease of the elderlyNeoplastic / malignant mechanismFrequently evolves to AMLTreatment:Hypomethylators, Growth factors, chemo + BMTSometimes Immunosuppression or Lenalidomide
Support with blood products and antimicrobial prophylaxis
MCQ Time… Bone Marrow Failure1 Which ONE of these is the most likely clinical picture in a patient with myelodysplastic syndrome associated with isolated del(5q)?
A A man with Hb 13 g/dL and a
platelet count of 600 × 109/L
B A woman with Hb 10 g/dL and
platelet count of 600 × 109/L
C A woman with Hb 13 g/dL and
platelet count 100 × 109/L
2 What is the most likely treatment for a 75-year-old patient with refractory anaemia and haemoglobin 9 g/dL?A Azacytidine
B Stem cell transplantation
C Lenolidamide
D Trial of erythropoietin
3 In which patients with myelodysplastic syndrome is ciclosporin most effective?A Low risk disease, hypocellular bone marrow
B Low risk disease, hypercellular bone marrow
C High risk disease, hypocellular bone marrow
D High risk disease, hypercellular bone marrow
4 Which of the following does NOT cause pancytopenia?A Iron deficiency
B Folate deficiency
C Aplastic anaemia
D Acute myeloid leukaemia
E Cyclophosphamide
5 Which ONE of these is NOT a feature of the blood count and bone marrow in patients with aplastic anaemia?A Abnormal ‘blast’ cells on the blood film
B Hypoplastic bone marrow with replacement by fat
C Normal appearance of neutrophils on the blood film
D Normochromic normocytic anaemia
6 Which of these is NOT associated with red cell aplasia?A A raised reticulocyte count
B Parvovirus infection
C Thymoma
D Chronic lymphocytic leukaemia
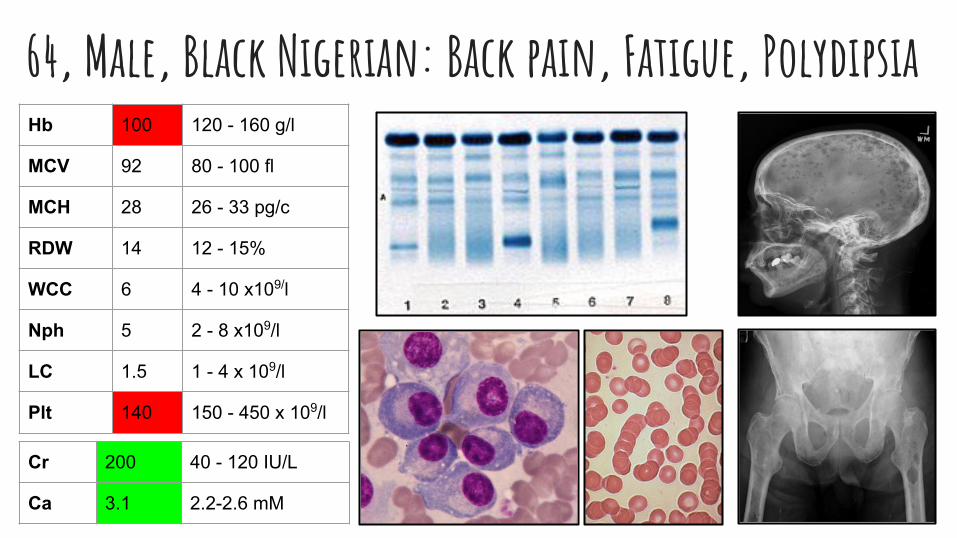
64, Male, Black Nigerian: Back pain, Fatigue, Polydipsia
Cr 200 40 - 120 IU/L
Ca 3.1 2.2-2.6 mM
Hb 100 120 - 160 g/l
MCV 92 80 - 100 fl
MCH 28 26 - 33 pg/c
RDW 14 12 - 15%
WCC 6 4 - 10 x109/l
Nph 5 2 - 8 x109/l
LC 1.5 1 - 4 x 109/l
Plt 140 150 - 450 x 109/l
TAKE HOME: MYELOMAMULTISYSTEMIC MALIGNANCY: CRAB criteria (+ infections)
Calcium, Renal, Anaemia, Bone (+Infection, Thrombus, Amyloid)SUSPECT: Anaemia, bone pain, fatigue, high globulins, HypercalcemiaTREAT:
DISEASE Rx: Chemo/RT, novel agents: velcade & Imids, auto BMTADJUVENT Rx: Analgesia, Bisphosphonates, Anticoags, Antibios
BEWARE!: Cord Compression, Pathological #, Renal Failure, Infection, Hyperviscosity
MCQ Time… Myeloma1 Which ONE of these is NOT associated with paraproteinaemia?A Chronic lymphocytic leukaemia
B Lymphoplasmacytic lymphoma
C Primary amyloidosis
D Chronic myeloid leukaemia
2 Which ONE of these is a relatively common complication in multiple myeloma?A Acute renal failure
B Cardiomyopathy
C Diarrhoea
D Pulmonary fibrosis
3 Which ONE of these clinical cases is an example of smouldering myeloma?A Bone marrow plasma cells >10%, no paraproteinand lytic bone lesions
B Bone marrow plasma cells >10%, abnormal serum free light chain ratio and
hypercalcaemia
C Plasma cells <1%, paraprotein in blood and osteoporosis
D Plasma cells >10%, paraprotein 30 g/L in blood and no tissue damage
4 Which ONE of these treatment strategies is most likely to be used for a 64-year-old man who is diagnosed with multiple myeloma?A Approximately four courses of chemotherapy followed by collection of autologous
stem cells and transplant after melphalan conditioning
B Monthly courses of oral melphalan with prednisolone until the paraprotein level
reaches a plateau, then thalidomide maintenance
C High dose chemotherapy followed by a related donor stem cell transplant
D Monthly courses of R‐CHOP chemotherapy
5 Which ONE of these is NOT a typical clinical feature of systemic amyloidosis?A Macroglossia
B Peripheral neuropathy
C Cardiomyopathy
D Liver cirrhosis
6 Which ONE of these is a side-effect of treatment with thalidomide?A Hyperactivity
B Bleeding
C Myopathy
D Constipation
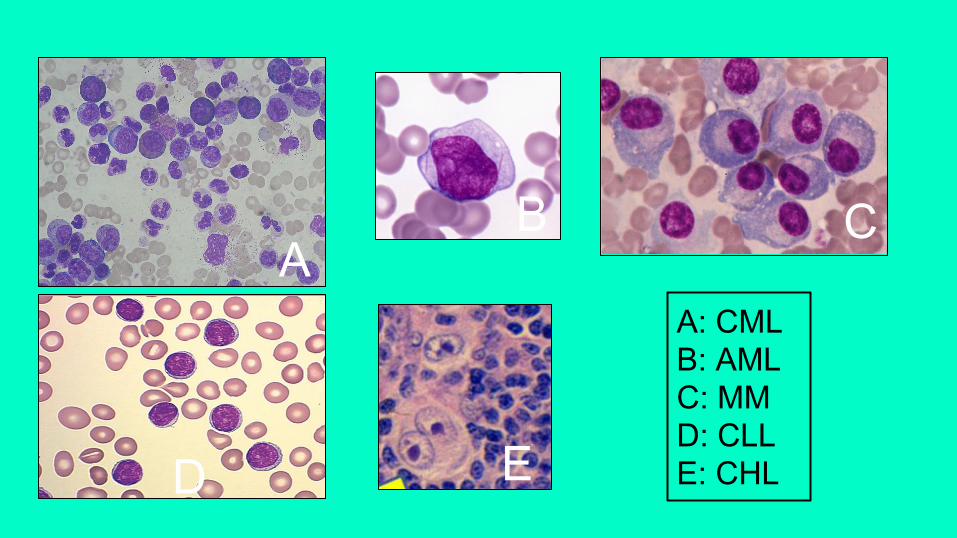
D E
B C
A: CMLB: AMLC: MMD: CLLE: CHL
A
MCQ Time… Spleen1 Which ONE of these is a major function of the spleen?
A Removal of the nucleus
from red cells released from
the bone marrow
B Production of neutrophils
for release into the circulation
C Storage of blood cells
which can be released at
times of physiological stress
D Generation of humoral
(antibody) immune response
to encapsulated bacteria
2 Which is NOT associated with hyposplenism?A Coeliac disease
B Inflammatory bowel disease
C Sickle cell anaemia
D Chronic myeloid leukaemia
3 Which ONE of these statements is TRUE concerning management patients who have had a splenectomy?A Lifelong prophylactic phenoxymethylpenicillin
recommended
B Patients should be advised not to travel abroad
C Patients should be monitored for reactivation of herpes
viruses such as Epstein-Barr virus and cytomegalovirus
D Inactivated vaccines such as influenza are not useful in
these patients
4 Infection risk with which ONE of these organisms is NOT increased after splenectomy?A Neisseria meningitides
B Clostridium difficile
C Haemophilus influenzae type B
D Streptococcus pneumoniae
5 Which ONE of these is a common complication within the first 2 weeks after a splenectomy?A A rise in the platelet count up to 1000 × 109/L
B Monocytosis
C Hepatic encephalopathy
D Disseminated intravascular coagulation
6 Before splenectomy, which vaccines is NOT given?A BCG
B Neisseria meningitides
C Haemophilus influenzae
D Streptococcus pneumoniae
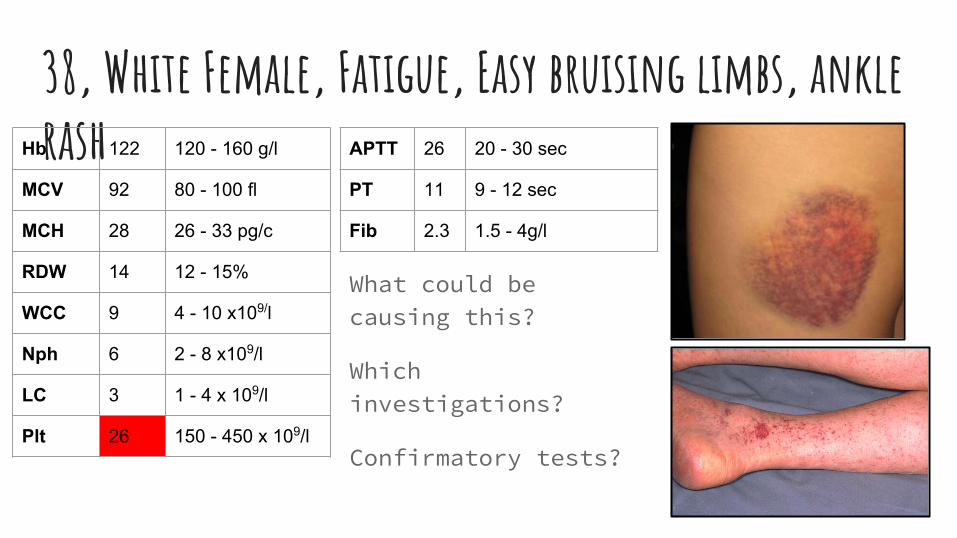
38, White Female, Fatigue, Easy bruising limbs, ankle rash
What could be causing this?
Which investigations?
Confirmatory tests?
Hb 122 120 - 160 g/l
MCV 92 80 - 100 fl
MCH 28 26 - 33 pg/c
RDW 14 12 - 15%
WCC 9 4 - 10 x109/l
Nph 6 2 - 8 x109/l
LC 3 1 - 4 x 109/l
Plt 26 150 - 450 x 109/l
APTT 26 20 - 30 sec
PT 11 9 - 12 sec
Fib 2.3 1.5 - 4g/l
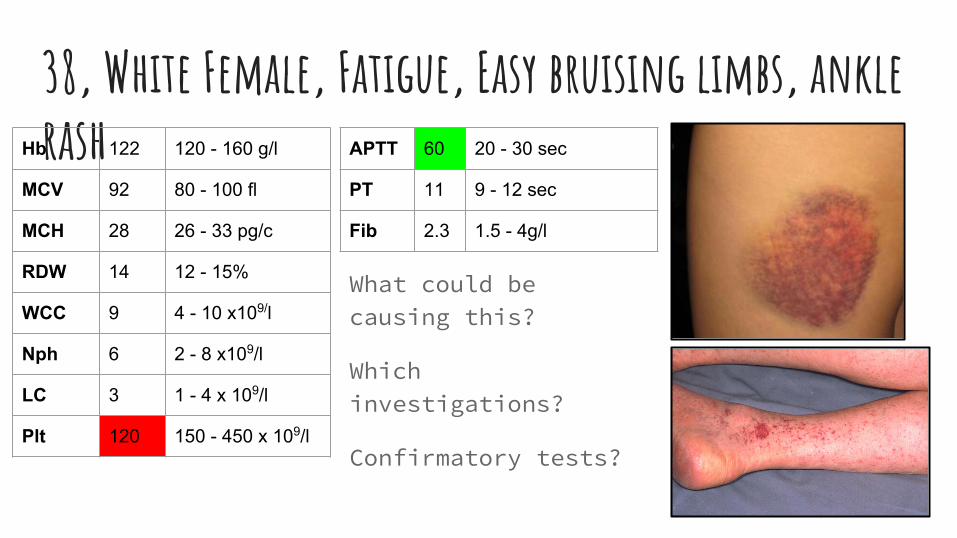
38, White Female, Fatigue, Easy bruising limbs, ankle rash
What could be causing this?
Which investigations?
Confirmatory tests?
Hb 122 120 - 160 g/l
MCV 92 80 - 100 fl
MCH 28 26 - 33 pg/c
RDW 14 12 - 15%
WCC 9 4 - 10 x109/l
Nph 6 2 - 8 x109/l
LC 3 1 - 4 x 109/l
Plt 120 150 - 450 x 109/l
APTT 60 20 - 30 sec
PT 11 9 - 12 sec
Fib 2.3 1.5 - 4g/l
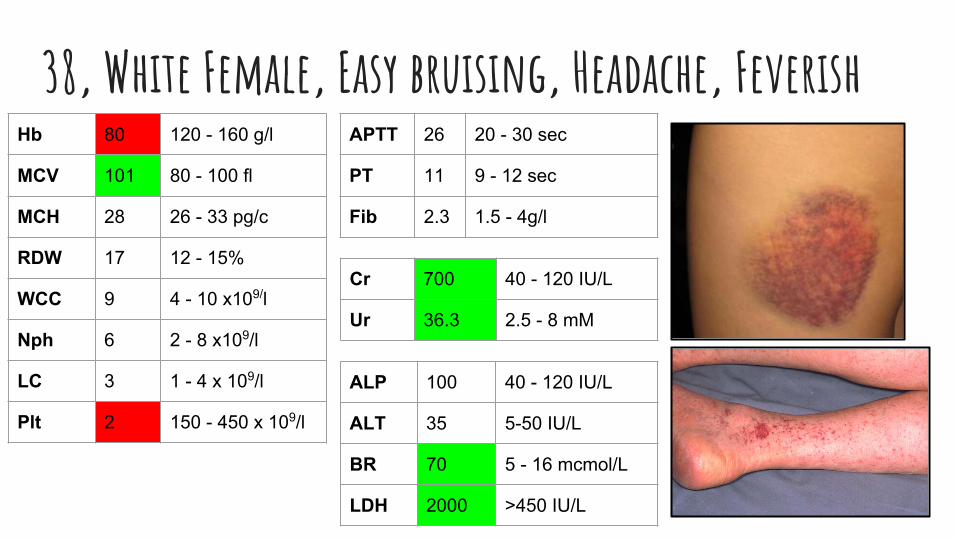
38, White Female, Easy bruising, Headache, FeverishHb 80 120 - 160 g/l
MCV 101 80 - 100 fl
MCH 28 26 - 33 pg/c
RDW 17 12 - 15%
WCC 9 4 - 10 x109/l
Nph 6 2 - 8 x109/l
LC 3 1 - 4 x 109/l
Plt 2 150 - 450 x 109/l
APTT 26 20 - 30 sec
PT 11 9 - 12 sec
Fib 2.3 1.5 - 4g/l
ALP 100 40 - 120 IU/L
ALT 35 5-50 IU/L
BR 70 5 - 16 mcmol/L
LDH 2000 >450 IU/L
Cr 700 40 - 120 IU/L
Ur 36.3 2.5 - 8 mM
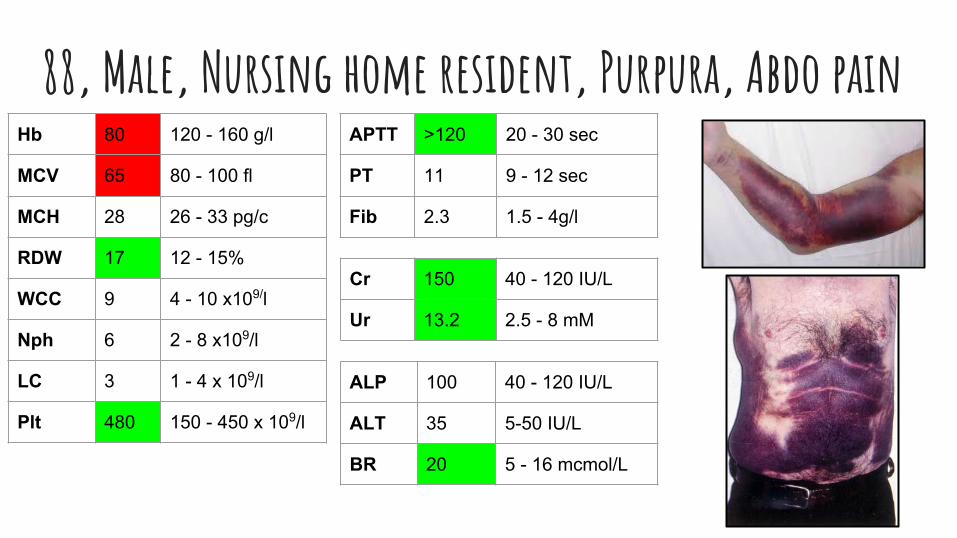
88, Male, Nursing home resident, Purpura, Abdo painHb 80 120 - 160 g/l
MCV 65 80 - 100 fl
MCH 28 26 - 33 pg/c
RDW 17 12 - 15%
WCC 9 4 - 10 x109/l
Nph 6 2 - 8 x109/l
LC 3 1 - 4 x 109/l
Plt 480 150 - 450 x 109/l
APTT >120 20 - 30 sec
PT 11 9 - 12 sec
Fib 2.3 1.5 - 4g/l
ALP 100 40 - 120 IU/L
ALT 35 5-50 IU/L
BR 20 5 - 16 mcmol/L
Cr 150 40 - 120 IU/L
Ur 13.2 2.5 - 8 mM
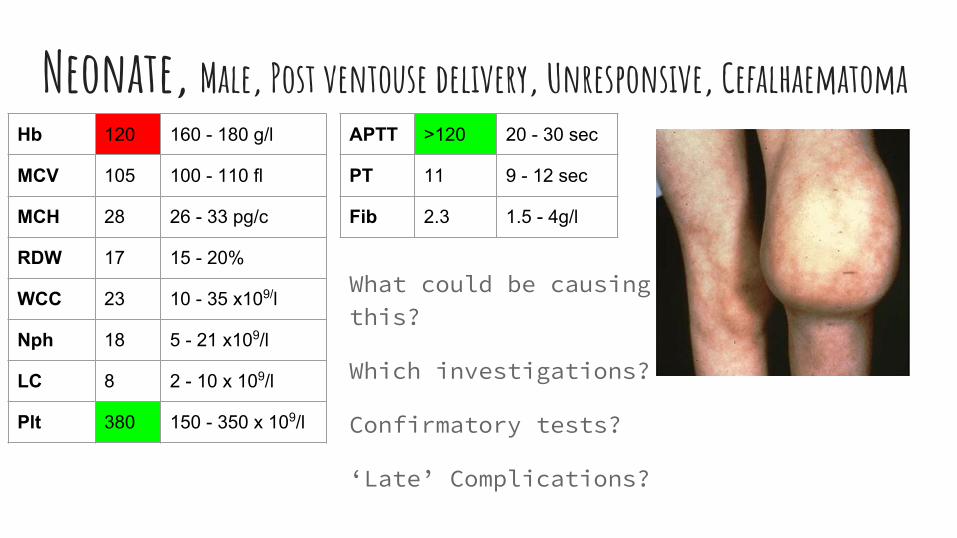
Neonate, Male, Post ventouse delivery, Unresponsive, CefalhaematomaHb 120 160 - 180 g/l
MCV 105 100 - 110 fl
MCH 28 26 - 33 pg/c
RDW 17 15 - 20%
WCC 23 10 - 35 x109/l
Nph 18 5 - 21 x109/l
LC 8 2 - 10 x 109/l
Plt 380 150 - 350 x 109/l
APTT >120 20 - 30 sec
PT 11 9 - 12 sec
Fib 2.3 1.5 - 4g/l
What could be causing this?
Which investigations?
Confirmatory tests?
‘Late’ Complications?
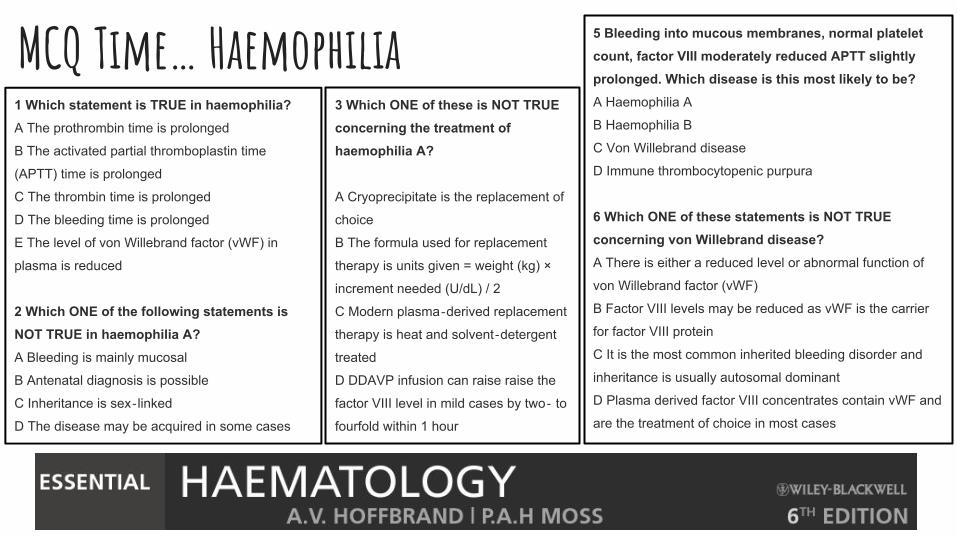
MCQ Time… Haemophilia 1 Which statement is TRUE in haemophilia?A The prothrombin time is prolonged
B The activated partial thromboplastin time
(APTT) time is prolonged
C The thrombin time is prolonged
D The bleeding time is prolonged
E The level of von Willebrand factor (vWF) in
plasma is reduced
2 Which ONE of the following statements is NOT TRUE in haemophilia A?A Bleeding is mainly mucosal
B Antenatal diagnosis is possible
C Inheritance is sex‐linked
D The disease may be acquired in some cases
3 Which ONE of these is NOT TRUE concerning the treatment of haemophilia A?
A Cryoprecipitate is the replacement of
choice
B The formula used for replacement
therapy is units given = weight (kg) ×
increment needed (U/dL) / 2
C Modern plasma‐derived replacement
therapy is heat and solvent‐detergent
treated
D DDAVP infusion can raise raise the
factor VIII level in mild cases by two‐ to
fourfold within 1 hour
5 Bleeding into mucous membranes, normal platelet count, factor VIII moderately reduced APTT slightly prolonged. Which disease is this most likely to be?A Haemophilia A
B Haemophilia B
C Von Willebrand disease
D Immune thrombocytopenic purpura
6 Which ONE of these statements is NOT TRUE concerning von Willebrand disease?A There is either a reduced level or abnormal function of
von Willebrand factor (vWF)
B Factor VIII levels may be reduced as vWF is the carrier
for factor VIII protein
C It is the most common inherited bleeding disorder and
inheritance is usually autosomal dominant
D Plasma derived factor VIII concentrates contain vWF and
are the treatment of choice in most cases
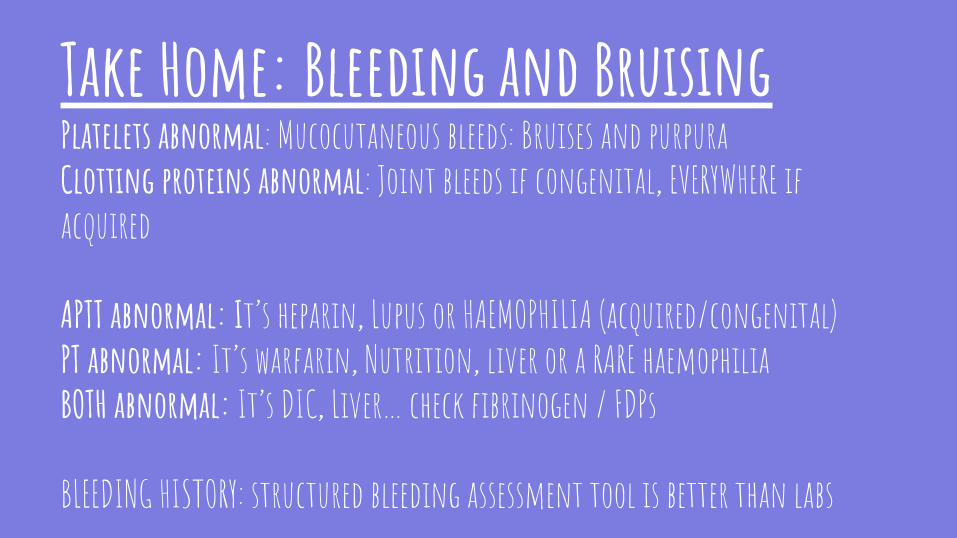
Take Home: Bleeding and BruisingPlatelets abnormal: Mucocutaneous bleeds: Bruises and purpuraClotting proteins abnormal: Joint bleeds if congenital, EVERYWHERE if acquired
APTT abnormal: It’s heparin, Lupus or HAEMOPHILIA (acquired/congenital)PT abnormal: It’s warfarin, Nutrition, liver or a RARE haemophiliaBOTH abnormal: It’s DIC, Liver… check fibrinogen / FDPs
BLEEDING HISTORY: structured bleeding assessment tool is better than labs
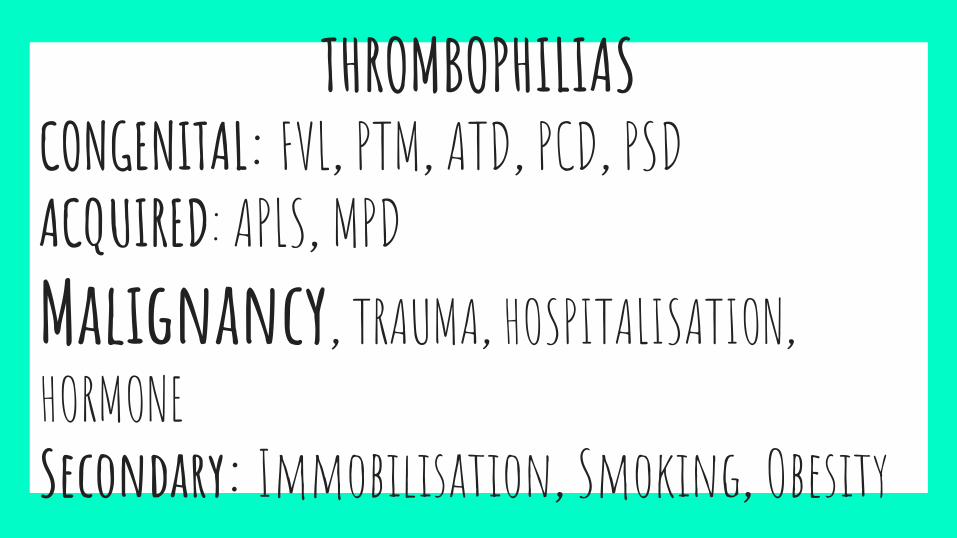
THROMBOPHILIASCONGENITAL: FVL, PTM, ATD, PCD, PSDACQUIRED: APLS, MPDMalignancy, TRAUMA, HOSPITALISATION, HORMONESecondary: Immobilisation, Smoking, Obesity
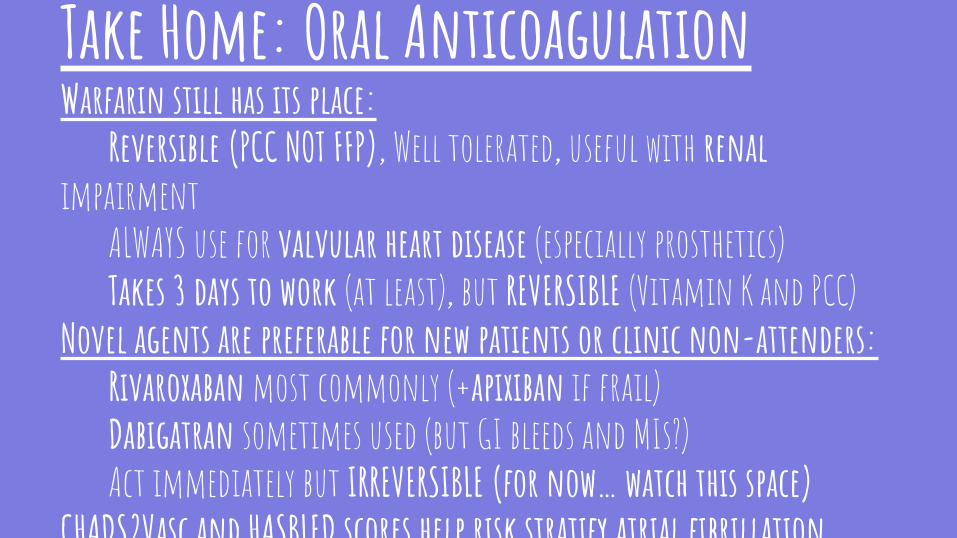
Take Home: Oral AnticoagulationWarfarin still has its place:
Reversible (PCC NOT FFP), Well tolerated, useful with renal impairment
ALWAYS use for valvular heart disease (especially prosthetics)Takes 3 days to work (at least), but REVERSIBLE (Vitamin K and PCC)
Novel agents are preferable for new patients or clinic non-attenders:Rivaroxaban most commonly (+apixiban if frail)Dabigatran sometimes used (but GI bleeds and MIs?)Act immediately but IRREVERSIBLE (for now… watch this space)
CHADS2Vasc and HASBLED scores help risk stratify atrial fibrillation
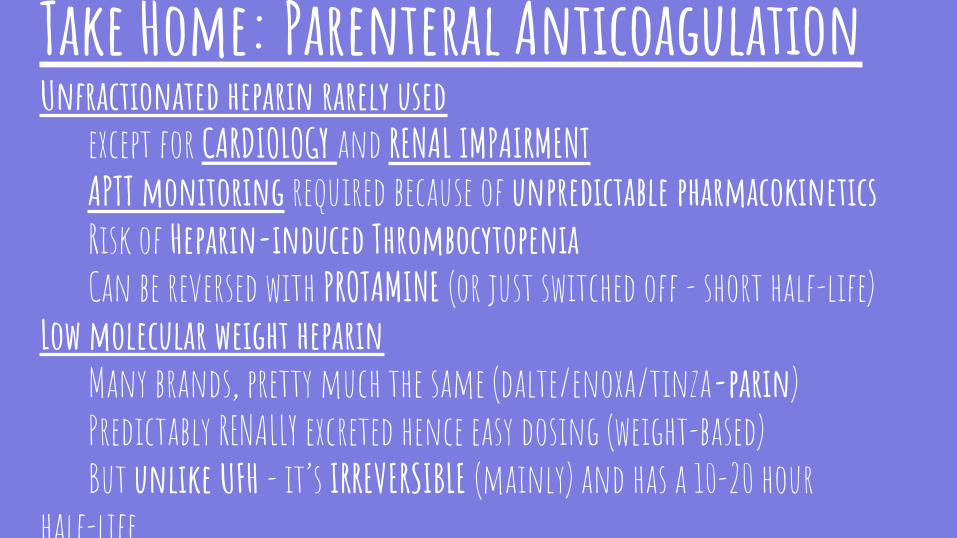
Take Home: Parenteral AnticoagulationUnfractionated heparin rarely used
except for CARDIOLOGY and RENAL IMPAIRMENTAPTT monitoring required because of unpredictable pharmacokineticsRisk of Heparin-induced ThrombocytopeniaCan be reversed with PROTAMINE (or just switched off - short half-life)
Low molecular weight heparinMany brands, pretty much the same (dalte/enoxa/tinza-parin)Predictably RENALLY excreted hence easy dosing (weight-based)But unlike UFH - it’s IRREVERSIBLE (mainly) and has a 10-20 hour
half-life
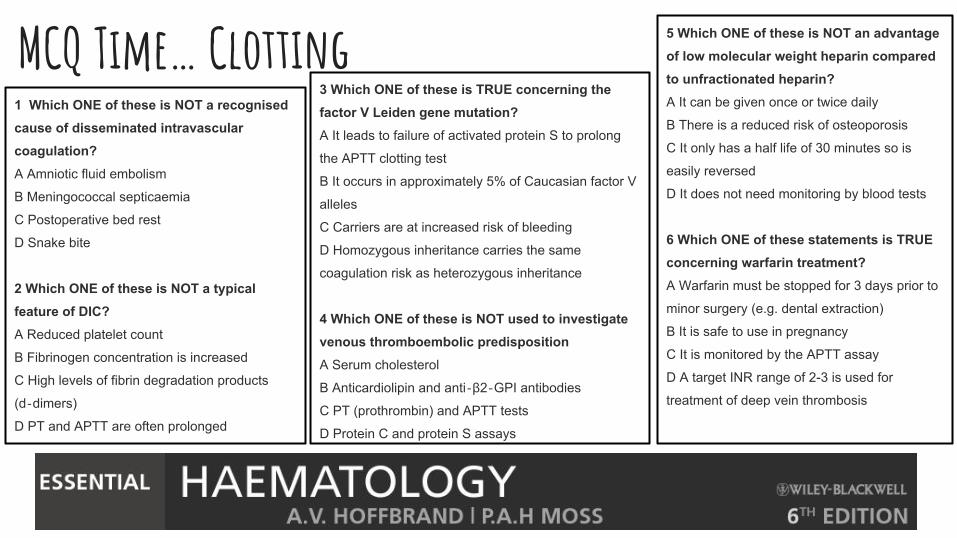
MCQ Time… Clotting1 Which ONE of these is NOT a recognised cause of disseminated intravascular coagulation?A Amniotic fluid embolism
B Meningococcal septicaemia
C Postoperative bed rest
D Snake bite
2 Which ONE of these is NOT a typical feature of DIC?A Reduced platelet count
B Fibrinogen concentration is increased
C High levels of fibrin degradation products
(d‐dimers)
D PT and APTT are often prolonged
3 Which ONE of these is TRUE concerning the factor V Leiden gene mutation?A It leads to failure of activated protein S to prolong
the APTT clotting test
B It occurs in approximately 5% of Caucasian factor V
alleles
C Carriers are at increased risk of bleeding
D Homozygous inheritance carries the same
coagulation risk as heterozygous inheritance
4 Which ONE of these is NOT used to investigate venous thromboembolic predispositionA Serum cholesterol
B Anticardiolipin and anti‐β2‐GPI antibodies
C PT (prothrombin) and APTT tests
D Protein C and protein S assays
5 Which ONE of these is NOT an advantage of low molecular weight heparin compared to unfractionated heparin?A It can be given once or twice daily
B There is a reduced risk of osteoporosis
C It only has a half life of 30 minutes so is
easily reversed
D It does not need monitoring by blood tests
6 Which ONE of these statements is TRUE concerning warfarin treatment?A Warfarin must be stopped for 3 days prior to
minor surgery (e.g. dental extraction)
B It is safe to use in pregnancy
C It is monitored by the APTT assay
D A target INR range of 2-3 is used for
treatment of deep vein thrombosis
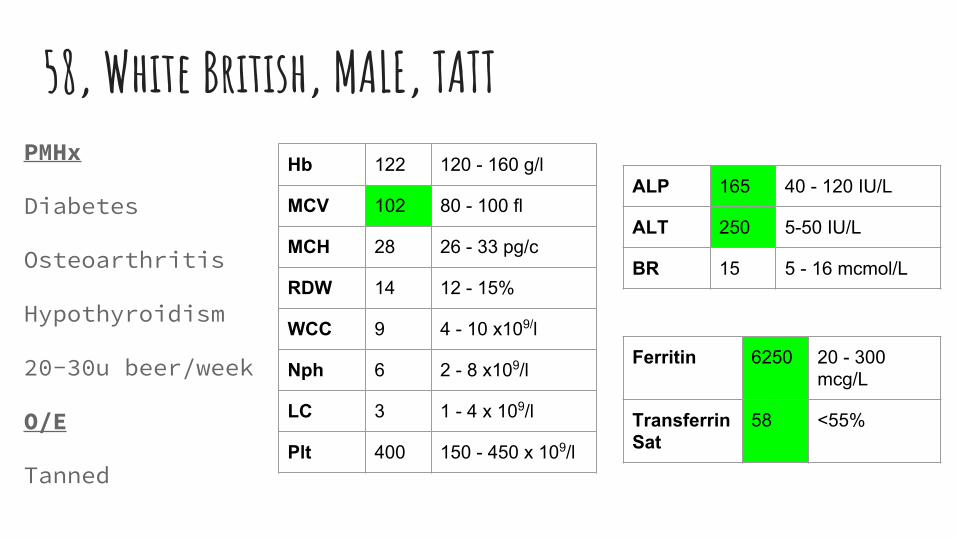
58, White British, MALE, TATTPMHx
Diabetes
Osteoarthritis
Hypothyroidism
20-30u beer/week
O/E
Tanned
Hb 122 120 - 160 g/l
MCV 102 80 - 100 fl
MCH 28 26 - 33 pg/c
RDW 14 12 - 15%
WCC 9 4 - 10 x109/l
Nph 6 2 - 8 x109/l
LC 3 1 - 4 x 109/l
Plt 400 150 - 450 x 109/l
ALP 165 40 - 120 IU/L
ALT 250 5-50 IU/L
BR 15 5 - 16 mcmol/L
Ferritin 6250 20 - 300 mcg/L
Transferrin Sat
58 <55%
58, White British, MALE, TATTHow to confirm the diagnosis?
How to treat now?
How to manage long-term?
Further work to be done?
HFEC282YH63DIron metabolism…?
Take Home: Iron OverloadHyperferritinemia = ACUTE PHASE, LIVER … or iron overloadGut is the main regulator through HEPCIDIN and HFETransfusional, Ineffective Erythropoiesis or H.H.Liver, Endocrine, Cardiac, Joint, SkinC282Y or H63D mutated HFE geneVENESECT if H.H.Iron Chelation if Ineffective Epoiesis/Transfusion
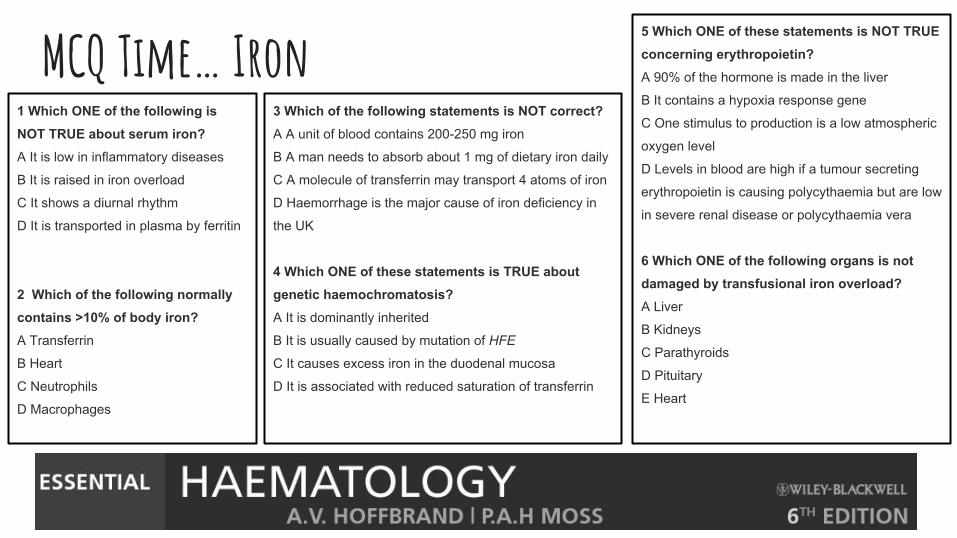
MCQ Time… Iron1 Which ONE of the following is NOT TRUE about serum iron?A It is low in inflammatory diseases
B It is raised in iron overload
C It shows a diurnal rhythm
D It is transported in plasma by ferritin
2 Which of the following normally contains >10% of body iron?A Transferrin
B Heart
C Neutrophils
D Macrophages
3 Which of the following statements is NOT correct?A A unit of blood contains 200-250 mg iron
B A man needs to absorb about 1 mg of dietary iron daily
C A molecule of transferrin may transport 4 atoms of iron
D Haemorrhage is the major cause of iron deficiency in
the UK
4 Which ONE of these statements is TRUE about genetic haemochromatosis?A It is dominantly inherited
B It is usually caused by mutation of HFE
C It causes excess iron in the duodenal mucosa
D It is associated with reduced saturation of transferrin
5 Which ONE of these statements is NOT TRUE concerning erythropoietin?A 90% of the hormone is made in the liver
B It contains a hypoxia response gene
C One stimulus to production is a low atmospheric
oxygen level
D Levels in blood are high if a tumour secreting
erythropoietin is causing polycythaemia but are low
in severe renal disease or polycythaemia vera
6 Which ONE of the following organs is not damaged by transfusional iron overload?A Liver
B Kidneys
C Parathyroids
D Pituitary
E Heart
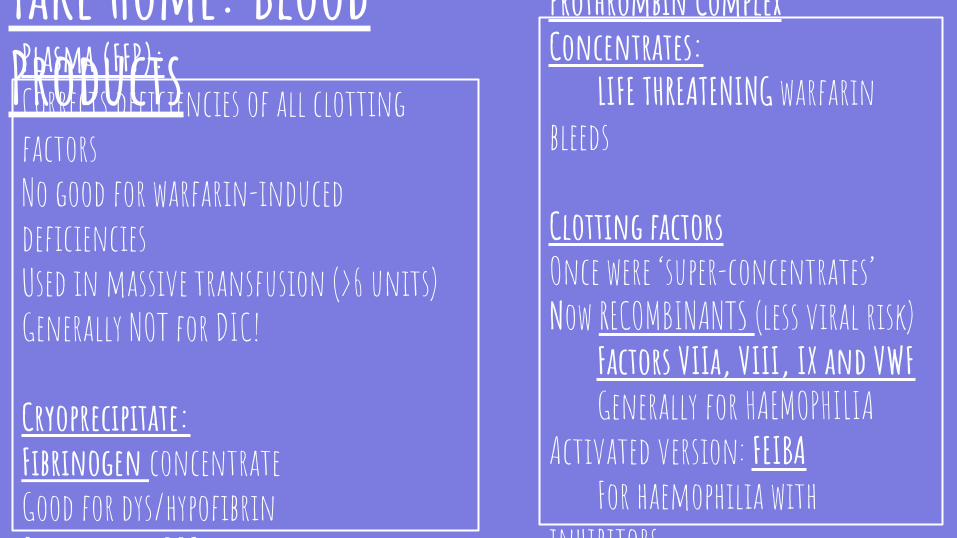
Plasma (FFP): Corrects deficiencies of all clotting factorsNo good for warfarin-induced deficienciesUsed in massive transfusion (>6 units) Generally NOT for DIC!
Cryoprecipitate:Fibrinogen concentrateGood for dys/hypofibrin Occasionally DIC and obstetric bleeds
Prothrombin Complex Concentrates:
LIFE THREATENING warfarin bleeds
Clotting factorsOnce were ‘super-concentrates’Now RECOMBINANTS (less viral risk)
Factors VIIa, VIII, IX and VWFGenerally for HAEMOPHILIA
Activated version: FEIBAFor haemophilia with
inhibitors
Take Home: Blood Products
MCQ Time… TRANSFUSION1 Which ONE of these infectious agents is NOT tested for in blood products?A Hepatitis C antibody
B Hepatitis B
C Gonorrhoea
D HIV
2 Which ONE of the following transfusions is likely to cause intravascular haemolysis?A Group O blood to group A recipient
B Group B blood to group O recipient
C Group O blood to group AB recipient
D Rh‐positive blood to a Rh‐negative
donor
3a. Which of the following is the most frequently reported transfusion related reaction leading to major morbidity A. Acute transfusion reactions
B. Haemolytic transfusion reactions
C. Infected blood product
D. Transfusion-related acute lung injury
E. Transfusion-associated circulatory overload
3b. Which most frequently leads to death?A. Acute transfusion reactions
B. Haemolytic transfusion reactions
C. Infected blood product
D. Transfusion-related acute lung injury
E. Transfusion-associated circulatory overload
4. In 2014, 700 ‘near misses’ of transfusing the incorrect blood product to a patient were reported in the UK. These are the top five reasons discovered by root cause analysis. Which was the commonest by far?
A Attachment of incorrect unit to patient IV line by
administering nurse
B Collection of incorrect unit from blood bank
C Data entry error by laboratory clerical staff
D Sampling/labelling error on initial cross match
sample
A young woman estimated to be in her mid 20s is admitted to resuscitation bay with clinical shock having sustained a RTA resulting in severe pelvic and chest trauma. Which blood product should she receive…?The same, but he is a young man…?
MCQ Time… Miscellaneous Haematology1 Which ONE of the following is NOT TRUE about neutropenia?A It may be caused by acute myeloid leukaemia
B It occurs in aplastic anaemia
C It is caused by aspirin
D It is associated with systemic lupus
erythematosus
E It is a cause of mouth ulcers
2 Which ONE of the following is NOT a cause of eosinophilia?A Steroid therapy
B Eczema
C Hookworm
D Hodgkin's lymphoma
2 Which ONE of the following infections can often cause lymphocytosis?A Haemophilus influenza
B Bordetella pertussis
C Tuberculosis
D Salmonella species
3 Which ONE of these statements is TRUE about T-lymphocytes?A They express CD5
B They synthesize immunoglobulin
C They recognize soluble antigens
D They activate the complement cascade
4 Which ONE is TRUE about B-lymphocytes?A They secrete surface immunoglobulin
B They are divided into helper and killer cells
C They are all short‐lived
D They are the atypical lymphocytes in infectious
mononucleosis
5 Which ONE of these statements is NOT TRUE concerning immunoglobulins?A Each immunoglobulin has one kappa and one
lambda chain
B IgM is the largest isotype
C There are four subclasses of IgG
D The normal serum level of IgG is 6-16 g/L
That was…Haematology for Clinical Finals
Paul Greaves: Consultant Haematologist, BHRUT, Romford
...any questions? (now or later: [email protected]