-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
1/18
Haemorrhoidal disease is a common presenting anorectal
condition. Although its treatment
dates several hundreds of years, there has been no consensus on
an optimal treatment
modality. Advances in the understanding of the pathophysiology
of haemorrhoids are aiding
clinicians in providing the most appropriate form of treatment.
Once more sinister
pathologies have been excluded management strategies are
tailored to the individual patient
depending on the severity of the disease. Clinical
classification systems are particularlyuseful as a measure of
severity. In many patients conservative measures may prove to
be
highly effective, but persistence and progression of symptoms
may necessitate more
interventional procedures. This article aims to define and
classify haemorrhoids, and review
the efficacy of current treatment modalities including the
latest techniues.
Introduction
The word !piles" is derived from the #atin word pila, meaning
ball. It has traditionally been
the layman$s term for haemorrhoids, for which treatment dates
bac% almost &''' years.
Although there are many well recognised precipitating factors
associated with haemorrhoids(such as low fibre inta%e, prolonged
straining and pregnancy) the precise aetiology remains
unclear, which is certainly reflected in the number of treatment
options available. This review
aims to define haemorrhoidal disease both anatomically and
clinically and further explain
how this affects subseuent management strategies. The efficacy
of the most popular
modalities of treatment is reviewed and a novel surgical
techniue is introduced.
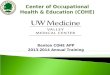
Anatomy and Pathophysiology
The concept of anal cushions being the precursors of
haemorrhoids was first introduced in
*+- and described in the classical , and ** o$cloc% positions
(*). These cushions lie
predominantly above the dentate line and are separated from the
sphincter complex by the
submucosal layer / a combination of blood vessels, muscular and
connective tissue0 related
to which is the inferior haemorrhoidal plexus which can become
engorged at the anal verge.
This is important in distinguishing prolapsing internal
haemorrhoids which are lined by an
insensate covering and whose nec% arises above the dentate line,
from external haemorrhoids
which arise below this line. The importance of anal cushions
lies in part in the maintenance
of faecal continence0 vascular filling is thought to be
responsible for approximately 1'2 of
resting anal pressure (1), and the cushions are able to provide
a conformable plug to maintain
complete closure of the anal canal. Theories of the aetiology of
haemorrhoids are thought by
some to be related to their vascularity and underlying
supportive structure. #ocal changes in
pressure are thought to cause venous dilatation in the anal
cushions and (along with avalveless venous system) lead to their
engorgement, seen in the increased prevalence of
haemorrhoids in pregnancy. The alternative connective tissue
theory suggests that the
underlying support provided by the collagenous fibres of the
submucosa degenerates over
time and ultimately leads to a caudal displacement of the anal
cushions (), perhaps
explaining the phenomenon of haemorrhoidal prolapse.
Figure 1 - Anatomy of the Anal Canal (4)
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
2/18
Classification
Improved understanding of local anatomy has led to helpful
clinical classifications for
haemorrhoids. The product of underlying pathophysiological and
anatomic changes, theyallow examination findings to be
standardi3ed, and therefore allow the most appropriate form
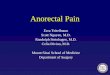
of treatment to be offered. One such classification is the
4oligher classification, which
describes & clinical entities (-). 4rade I describes a
normal appearance externally with
haemorrhoids which bleed but do not prolapse whereas in grade II
the haemorrhoids may
prolapse but reduce spontaneously. 4rade III and I5 describe
prolapsing haemorrhoids which
reuire manual digital reduction or remain prolapsed permanently,
repectively / figure 1.
However, with the increased availability of endoscopy,
haemorrhoids are being able to be
visuali3ed during colonoscopic or sigmoidoscopic examination
with a retroflexed scope /
figure . This has led to the development of endoscopic
classification systems which again
address and closely correlate to the patient$s symptoms (6).
Although this classification is limited by the assumption of
bleeding and prolapse being the
only symptoms attributed by haemorrhoids, it still has an
important place in the management
of the condition when used in con7unction with the wider
clinical picture.
Figure 2 oligher Classification of !aemorrhoids"
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
3/18
Figure # $etrofle%ed colonoscope sho&ing internal 'ie&
of haemorrhoids
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
4/18
he Clinical Picture
Haemorrhoids affect between &2 and 62 of the general
population (), however this figure
is indicative only of symptomatic haemorrhoids and may well be
an under8estimate. Hospital8
based proctoscopy studies have shown prevalence rates of up to
962 with the ma7ority of
patients being asymptomatic. (9) :ymptoms are widely variable,
but haemorrhoids are
responsible for the ma7ority of cases of rectal bleeding. The
most common symptoms after
bleeding include pain, mucous discharge and pruritus with or
without associated
haemorrhoidal prolapse (+). The colour of the bleeding is
attributed to the arterial oxygen
tension caused by arteriovenous communications within the anal
cushions (*'), while pruritis
and associated discomfort is thought to be due to prolapse of
the rectal mucosa leading to
deposition of mucus on the perianal s%in. The combination of
type and severity of symptoms
in addition to examination findings, allows the most appropriate
treatment modality to be
offered.
It is paramount not to attribute all cases of bright red rectal
bleeding to haemorrhoids0Conditions from anal fissure to colorectal
malignancy may all produce similar symptoms and
concurrent pathology must be excluded with investigation of the
proximal colon, which in
most cases is performed by sigmoidoscopic or colonoscopic
investigation. Also,
haemorrhoids are rarely responsible for anaemia (**).
he reatment adder
Classification systems, such as the one described above, allow
standardisation of the
condition and can also monitor progression. Once a patient has
been satisfactorily
investigated, the surgeon is in a position to offer the most
appropriate treatment. As
haemorrhoids are essentially a benign condition, treatment is
directed at alleviating symptoms
rather than to necessarily halt progression. ;ost surgeons have
traditionally adopted a step8
wise approach in treatment depending on the severity of symptoms
and clinical grading of the
haemorrhoids, with escalation if necessary. /
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
5/18
Conser'ati'e +anagement
Conservative management is usually reserved for the minimum of
symptoms and grade I orgrade II haemorrhoids. >y addressing some
of the precipitating factors, they may well
prevent the need for further intervention. It essentially
involves lifestyle modification and
dietary advice as well as medical treatment. :ome have suggested
that constipation may be a
precipitating factor in the development and progression of
haemorrhoids and the lower
incidence of the condition in populations with high dietary
fibre inta%e may add weight to
this theory (*1), although this is never been proven
definitively, and others have eually
proposed that haemorrhoids may actually lead to constipation
(*). Adeuate fluid and fibre
inta%e may reduce straining effort during defaecation, along
with laxatives, but may well also
prevent recurrence of haemorrhoids. A recent meta8analysis of
fibre supplementation showed
that the ris% of bleeding was lower with an increased fibre
inta%e, along with the rate of
recurrence (*&). #) and in7ection sclerotherapy, although
cyrotherapy and
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
6/18
photocoagulation are potential options.
Figure .on-conser'ati'e reatments
?># has been modified over the years from >laisdell$s
original description (*6) which
advocated the application of a single band alone. Currently,
surgeons may apply up to
bands at a time and can repeat this every 6 wee%s or so. The
techniue involves the direct
visualisation of the haemorrhoidal pedicle through a
proctoscope, with application of a band
around it using either forceps or a suction device. This results
in ischaemic necrosis of the
haemorrhoidal tissue which subseuently auto8amputates. It is
important to warn patients that
they may experience some bleeding after *'8*& days when the
banded tissue sloughs off.
:uccess rates of between 6+2 and +&2 have been shown (*)
with low complication rates,
although there have been potentially life8threatening
complications reported. =ith higher
success rates than other office procedures, it is still deemed
to be less efficient than
haemorrhoidectomy in the long term, albeit with less pain and
fewer complications.(*9)
?ecent evidence suggests that in fact most patients complain of
moderate or worse
discomfort after banding (*+).
In7ection sclerotherapy is a widely available techniue, the most
common sclerosant being
-2 phenol in almond oil, and is particularly useful for bleeding
piles. The sclerosant induces
an inflammatory reaction causing changes both in the
haemorrhoidal mass and affecting the
underlying architecture. Haemorrhoids are again identified by
proctoscopy and then in7ected
well above the dentate line. As long as the in7ections are
appropriately directed there is no
pain experienced by the patient. Although this is a seemingly
easy, reproducible procedure,there are as many reported problems
with it as advantages. High failure rates accompanied by
misplaced in7ections have led many surgeons to abandon this
office procedure.
There are certain contraindications for banding and in7ecting
piles such as patients being on
formal anticoagulant medication and coagulopathies, but there
are no guidelines discouraging
the use of a combination of procedures under these
circumstances. One large study has shown
that by using a combination of sclerotherapy, rubber band
ligation and infrared coagulation
over a period of 1 months on average, satisfaction rates of
around +'2 were achieved with
less than *'2 reuiring surgical intervention. (1')
Cyrotherapy appears to have fallen out of favour. =ith the use
of a specialised probe, thehaemorrhoidal mass is ablated, and can
be repeated over time. @otential problems include
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
7/18
ulceration and discharge as a conseuence of impaired healing
following application of the
cyro8probe. (1*)
@hotocoagulation reuires the use of specific infrared optical
euipment. The procedure is
similar to sclerotherapy in that direct visualisation of the
haemorrhoid with a procotscope is
reuired. Once the coagulator device is primed, the base of the
haemorrhoidal tissue istargeted and necrosis ensues. The subseuent
healing of the mucosa leads to shrin%age of the
piles and ulcer formation. It has been most commonly used for
internal haemorrhoids and has
been shown to be a superior techniue to sclerotherapy with fewer
complications (11).
*urgical ,ptions
/%cision !aemorrhoidectomy
Haemorrhoidectomy has remained the centre of all the surgical
procedures for symptomatic
haemorrhoids of high grade or those failing office procedures.
Although the exact details ofthe operation and its variants are
beyond the scope of this review, haemorrhoidectomy has
been shown to be the most effective treatment for haemorrhoids
(1). Originally described by
=hitehead in the late part of the *+th century, its
modification, the ;illigan8;organ
operation (1&) was later reserved for prolapsing
haemorrhoids of grade III and I5. This
involves excision of the internal and external components of
each haemorrhoid, leaving the
s%in open in a 8leaf clover pattern and allowing healing to
occur by secondary intention.
Over the years newer, more efficient surgical procedures have
been developed with the
operation being performed with either an open (as described
above) or closed techniue
where the haemorrhoid component is excised and the wounds closed
primarily (1-). The
theory behind the closed or oulder) haemorrhoidectomy are also
varieties of operation
which have the common theme of excising haemorrhoidal tissue,
the latter using a specialised
surgical instrument to minimise tissue trauma and confer faster
wound healing. At present the
#iga:ureT; haemorrhoidectomy has been shown to more efficacious
than conventional
haemorrhoidectomy (1).
Bnfortunately, complication rates have traditionally been higher
in surgery than office
procedures with post8operative pain being the most common,
though this is not necessarilythe case with newer techniues (19). A
number of trials have attributed this to be the main
factor preventing patients from an early return to normal life,
and have suggested time8frames
of between 1 and & wee%s before patients return to wor%
(1+8*). Other complications include
urinary retention, sepsis, incontinence and anal stenosis (1,
).
Figure 0 Photograph of +illigan-+organ !aemorrhoidectomy
(#4)
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
8/18
*tapled Anope%y
This procedure has recently gained a reputation for being the
4old8standard for prolapsed
haemorrhoids (grade III and I5) with encouraging results
regarding postoperative recovery
and comparable complication to traditional haemorrhoidectomy
(-).
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
9/18
3oppler-uided !aemorrhoidal Artery igation (3-
!A)
The newest treatment modality which is gaining considerable
popularity is oppler8guided
haemorrhoidal artery ligation. Although essentially a surgical
procedure, it is far lesstraumatic than traditional surgical
options and does not involve the excision of haemorrhoidal
tissue and their associated complications. This techniue was
first described more than
decade ago and involves the use of a specialised proctoscope
coupled with a oppler probe
(&-). It can be performed with or without general
anaesthesia depending on the patient and
clinical circumstances. It has been performed on grades II8I5,
but is thought to be most
useful for grades II and III. The procedure wor%s on the
principle that arterial flow through
local arteriovenous anastamoses maintains the haemorrhoidal
mass. #igating these vessels
ultimately leads to haemorrhoid shrin%age with conseuent
reduction and cessation of
bleeding.
Figure Cast of haemorrhoid &ith arterial supply displayed
(40)
Bsing the proctoscope to identify terminal branches of the
superior rectal artery and
haemorrhoidal artery, the vessels are subseuently ligated by
placing haemostatic sutures
(
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
10/18
An even newer techniue which aims to act on grade I5
haemorrhoids with rectal mucosaprolapse is the 48HA# recto8anal
repair (?A?). It uses the same method as 48HA# but
additionally applies a vertical running suture which retracts
the prolapsed mucosa. There are
no large series$ published on this treatment, however it could
be potentially a rival to stapled
anopexy.
he Future
The resurgence in the treatment of haemorrhoids has led to the
introduction of more efficient
variants of traditional techniues and novel surgical procedures
all aimed to increase efficacy,
reduce complications and promote better healing and higher
satisfaction. =ith greater
understanding of the anatomy and pathophysiology of the
condition, it may be possible to
limit treatment to a few interventions relating directly to an
appropriate classification system.
It is highly improbable that there will be one all8encompassing
optimal treatment modality
for haemorrhoids, as the condition represents a spectrum of
severity. However, the important
message is that whichever treatment is used, it must be safe and
efficient.
?D, @enninc%x
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
11/18
and in vitro study in man. Int E Colorectal is. *+9+F &0
**98*11.
/ Haas @A, 4. Dvaluation of anaemia caused by hemorrhoidal
bleeding. is
Colon ?ectum. *++&F 0 *''68.
*1 / >ur%itt @. 5aricose veins, deep vein thrombosis and
haemorrhoidsF Dpidemiology and
suggested aetiology. >;E. *+1Fii0 --68-6*.
* / Eohanson Elaisdell @C. Office ligation of internal
haemorrhoids. American E. of :urg. *+-9F +60
&'*8&'&.
* / >at #, ;el3er D, Goler ;, re3nic% . Complications of
rubber band ligation of
symptomatic internal haemorrhoids. iseases of Colon and ?ectum.
*++F 60 1981+'.
*9 / :hanmugam 5, Thaha ;A, ?abindranath G:, Campbell G#, :teele
?EC, #oudon ;A.
?ubber band ligation versus excisional haemorrhoidectomy for
haemorrhoids. Cochrane
atabase of :ystematic ?eviews 1''-. Issue *, Art oF
C''-'&.
*+ / =atson
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
12/18
operative treatment of haemorrhoids. #ancetF *+0 10
***+8**1&.
1- / occasanta @, Capretti @4, 5enturi ;, Cioffi B, e :imone ;,
:alamina 4, Contessini8
Avesani D, @eracchia A. ?andomised controlled trial between
stapled circumferential
mucosectomy and conventional circular hemorrhoidectomy in
advanced hemorrhoids with
external mucosal prolapse. Am E :urg. 1''*F *910 6&869.
1 / :enagore A, ;a3ier =@, #uchtefeld ;A, ;acGeigan E;, =engert
T. Treatment of
advanced hemorrhoidal diseaseF a prospective, randomised
comnparison of cold scalpel vs.
contact dFLA4 laser. is Colon ?ectum. *++F 60
*'&18*'&+.
/ evien C5, @u7ol E@. Total circular hemorrhoidectomy. Int :urg.
*+9+F &0 *-&8.
& / Appearance immediately after pile removal. Eeremy
#ivingstone$s :urgical @age, 1''.
JOnlineK Available at www.livingstone.demon.co.u%Mimg1+.7pg.
Accessed 'M'*M1''
- / :utherland #;, >urchard AG, ;atsuda G, :weeney E#,
>o%ey D#, Childs @A. A
systematic review of stapled hemorrhoidectomy. Arch :urg 1''1F
*0 *+-8*&'6.
6 / #ongo A. Treatment of hemorrhoidal disease by reduction of
mucosa and hemorrhoidal
prolapse with a circular stapling deviceF a new procedure.
@roceedings of the 6th =orld
Congress of Dndoscopic :urgery, Eune , *++9. ;undo33i Dditore,
*++9.
/ g G8H, Ho G8:, Ooi >:, Tang C#, Du G=. Dxperience of **
stapled
haemorrhoidectomy operations. >r E of :urg. 1''6F +0
11681'.
9 / ;ehigan >E, ;onson E?, Hartley ED. :tapling procedure for
haemorrhoids versus
;illigan8;organ haemorrhoidectomyF randomised controlled trial.
#ancet. 1'''F --0 918
9-.
+ / ?owsell ;, >ello ;, Hemingway ;. Circumferential
mucosectomy (stapledhaemorrhoidectomy) versus conventional
haemorrhoidectomyF randomised controlled trial.
#ancet. 1'''F --0 +89*.
&' / Ho LH, Cheong =G, Tsang C, et al. :tapled
hemorrhoidectomy / cost and
effectiveness. ?andomised controlled trial including
incontinence scoring, anorectal
manometry, and endoanal ultrasound assessments at up to months.
is Colon ?ectum.
1'''F &0 *6668*6-.
&* / Dsser :, Ghubchandani I, ?a%hmanine ;. :tapled
hemorrhoidectomy with local
anaesthesia can be performed safely and cost8efficiently. is
Colon ?ectum. 1''&F &0 **6&8
**6+.
&1 / ?ipetti 5, Caricato ;, Arullani A. ?ectal perforation,
retropneumoperitoneum, and
pneumomediastinum after stapling procedure for prolapsed
hemorrhoidsF report of a case andsubseuent considerations. is Colon
?ectum. 1''1F &-0 1698'.
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
13/18
& / ;aw A, Du G=, :eow8Choen , :hetty , #indsey I, ;ortensen
E, =arren >ritish Haemorrhoid Centre 1''. Cast of a haemorrhoid.
JOnlineK Available at
www.halocentre.comMwhatishalo.html. Accessed 'M'*M'
& /
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
14/18
Mandi di bak mandi dengan air hangat,biasanya dapat mengurangi
rasa sakit
di perianal.0al ini mungkin karena air hangat dapat merelaksasai
meksnisme
spinkter dan spasme.1ebuah literatur menyebutkan, kompres es
dapat
menguragi nyeri akibat thrombosis akut.1ebagian besar pasien
melihat adanya
perbaikan atau resolusi komplit dari gejala-gejala yang mereka
alam, dengan
tindakan konservasi! di atas. Pengobatan diarahkan hanya pada
gejala dan
bukan penampakan hemoroid.
"ika pasien mengeluhkan nyeri hebat, kemugkinan ia menderita
hemoroid
ekternal akibat thrombosis.2ni biasanya membaik dalam 3-)* hari,
tetapi jika
tetap terasa sakit da luar periode tersebut, bisa di lakukan
eksisi untuk
menghilangkan thrombus. Penggunaan dressing penekan, bisa
menjadi pilihan
pengobatan.
Pengobatan Farmakologis
Pengobatan !armakologis non spesi!ik meliputi laksati!,
analgesik,
antiin!lamasi dan obat-obatan topikal#mengandung anatesi local
dan
steroid$.1ementara obat-obatan spesi!ik untuk hemoroid #agen
phlebotropik$
yang ada saat ini adalah !lavonoid, mencakup micronised diosmin
dan
hesperidin dan hidrosomin. Obat-obatan ini secara signi!ikan
menurunkan gejala
dan mencegah terjadinya rekurensi.%ahkan sebuah studi
menemukan,
pemberian diosmin dan hesperidin sama e!ekti! dengan rubber band
ligation,
dengan e!ek samping yang lebih kecil.
Laksatif
4aksati! dalam bentuk serat dapat membantu menguragi gejala
hemoroid,
terutama perdarahan. 1ebuah tinjauan dilakukan P.&lonso dan
ka(an-ka(an
terhadap tujuan hasil penelitan melibatkan 35 pasien, yang
secara acak dibrri
serat atu non serat.Meta analisa ini menunjukan, laktasi! dalam
pengobatan
hemoroid simtomatik.
Diosmin-Hesperidin
Keduanya biasa di!omulasi sebagai micronized purified flavonoid
fraction
#MP66$ unik, yang mengandumg 7*8 diosmin dan )*8 hesperidin.
0esperidindiektrak dan genus citrusdengan spesies Rutaceae
aurantieae,suatu tipe jeruk
kecil yang biasa ditemukan di daratan 1panyol, &!rika tara
dan
9hina,sementara diosmin yang merupakan senya(a !lavonoid
diperoleh melalui
proses sintesa, mulai dari bahan baku.
Melalui mikronisasi, kedua bahan akti! tersebut mengalami
proses
penggilingan dengan teknologi tinggi. 1ebuahjet of air at
supersonic velocities
mampu mengurangi ukuran partikel standar dari 3:m, hingga kurang
dari
;:m.&kibatnya, penyerapan keduanya jadi lebih cepat dan
lebih baik, sehingga
bisa meningkatkan bioavailabilitas. 2mplikasinya tentu mengarah
pada e!ikasi
klinis yang lebih cepat dan superior.
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
15/18
Kedua senya(a tersebut memiliki mekanisme kerja yang unik.
4ayaknya
noradrenalin, obat ini mengakibatkan kontraksi vena,menurunkan
ekstravasasi
dari kapiler dan menghambat reaksi in!lamasi terhadap
prostaglandin terhadap
prostaglandin #P
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
16/18
%anyak obat bebas yang bisa di gunakan untuk mengobati hemoroid.
2ni
biasanya obat yang sama yang digunakan untuk mengatasi gejala
anal, seperti
gatal atau tidak nyaman. %eberapa penelitian menunjukkan,
obat-obatan ini
tidak berdampak pada hemoroid, hanya menurunkan gejala
hemoroid.
Produk-produk yang digunakan untuk pengobatan hemeroid tersedia
dalambentuk ointments, creams, gels, suppositories, !oams dan
pads.1aat digunakan
pada anal canal, produk-produk ini dimasukkan dengan jari atau
suatu pipa.
1ebelum dimasukkan, pipa harus diberi pelumas.
Protektan
Proktetan mencegah iritasi daerah perianal dengan membentuk
barier !isik
pada kulit, yang mencegah kontak kulit yang teriritasi dengan
cairan atau
kotoran yang berpotensi memperburuk kondisi.%arier tersebut
menurunkan
iritasi, rasa gatal, sakit dan rasa terbakar.
Protektan meliputi@
&luminium
9ococa buter
inc oide atau calamine #yang mengandung Ainc oide$ dalam
konsentrasi
sampai ;+8
Astrigents
&strigents menyebabkan koagulasi protein dalam sel kulit
perianal ataulapisan kanal anal. 0al ini menyebabkan kulit kering,
yang pada akhirnya
membantu mengurangi rasa terbakar, gatal dan sakit.
&strigents meliputi@
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
17/18
9alamine +-;+8
>inc oide +-;+8
Witch haAel )*-+*8
Antiseptik
&ntiseptik menghambat perkembangan bakteri dan organisme
lain. %elum jelas,
apakah antiseptik lebih e!ekti! dari sabun dan air.
9ontoh antiseptic meliputi@
%oric acid
0ydrastis
Phenol
%enAalkonium chloride
9etylpyridinium chloride
%enAenthorium choloride
Resorcinol
Keratolitis
Keratolitik adalah kimia yang menyababkan lapisan terluar kulit
atau jaringan
lain mengelupas.&lasan digunakan obat ini, agar obat-obatan
yang digunakan
pada anus dan daerah perianal dapat masuk ke jaringan yang lebih
dalam. 'ua
agen keratolitik yang disetujui 6'& adalah@
&lumunium chlorhydroy allantoinate *,;-;,*8
Resoncinol )-8
Anlgesik
Produk-produk analgesik, seperti produk anatesi, menguragi rasa
sakit, gatal
dan terbakar dengan menekan reseptor dari sara! rasa sakit.
9ontoh analgesik@
Menthol *,) B ),*8 #lebih besar dari ),*8 tidak dianjurkan$
9amphor *,) B 8 #lebih besar dari 8 tidak dianjurkan$
-
8/13/2019 Haemorrhoidal Disease is a Common Presenting Anorectal
CoHE,OROIDndition
18/18
"uniper tar ) B +8
Kortikosteroid
Kortikosteroid menentukan in!lamasi dan mengurangi rasa gatal.
"ika
digunakan berkepanjangan , bisa menyebabkan kerusakan permanen
pada kulit.














![[Alex] COHE LOTO [Instructor]](https://img.pdfslide.net/doc/110x75/56d6bed41a28ab301693c015/alex-cohe-loto-instructor.jpg)