Embed Size (px)
Citation preview

Wound Practice and Research 208
A systematic review of the literature addressing asepsis in wound management
ABSTRACTThere has been extensive ongoing debate on the application of aseptic technique in wound management over the previous decades and changes to the way in which theory is applied to clinical practice have occurred regularly. Clinicians often express confusion over the way various techniques should be applied, particularly when practising in clinical settings in which maintenance of strict asepsis is inherently difficult (for example, community-based wound management). Wound cleansing, use of open but unused
wound dressings and storage of wound management equipment are frequent issues on which clinicians request guidance. A systematic review using Joanna Briggs Institute methods was undertaken in order to establish the current state of the scientific literature on this topic and inform the development of recommendations for practice in this field. All levels of evidence were included in the review, including opinion papers. Findings from the 20 quantitative studies were reported in narrative summary and findings from 37 qualitative research papers were aggregated in a thematic synthesis. Although high-level evidence on wound cleansing solutions was identified, the review concluded that there is a paucity of scientific literature on most topics related to asepsis in wound care.
Keywords: Asepsis, wound cleansing, aseptic non-touch technique, handwashing, infection control.
INTRODUCTIONWound infection has a large impact on individuals and the health care system. Precise incidence rates are difficult to determine due to the many types of wounds and various methods of diagnosing and tracking wound infection. As many as 60% of chronic wounds have infection in the form of demonstrated presence of surface bacteria or invasive biofilm1,2. Rates of surgical site infection vary substantially based on surgical site3; however, recent estimates suggest 10–12% of all surgical wounds become clinically infected4. Infection rate in lacerations is cited at 5%5, and rate of biofilm in all acute wounds is approximately 6%2.
Facility-acquired wound infection is of particular concern given the increasing significance of antibiotic-resistant bacteria. Infection control procedures are first-line strategy to prevent infection spread6. Given the impact of wound infection and significance of infection control practices in reducing its incidence, it is important that clinicians understand the implementation of infection control procedures when managing wounds. Historically, there have been major changes to aseptic theory in wound management7-9. Surveys indicate clinicians experience confusion about how to implement aseptic technique and other infection control principles10,11.
Within Australia, the introduction of a standard on health care-associated infection12 and publication of a national
Haesler E, Thomas L, Morey P & Barker J
Haesler E et al. A systematic review of the literature addressing asepsis in wound management
Emily Haesler*PhD, BN, PostGradDipAdvNurs(Gerontics)Adjunct Associate ProfessorCurtin University, School of Nursing, Midwifery and Paramedicine, WA, AustraliaHonorary AssociateLa Trobe University, Australian Centre for Evidence Based Aged Care, Vic, AustraliaEmail: [email protected] +61 2 6244 2946
Lyn ThomasRN, NP, BHlthSci(Nurs), MNP Community and Aged Care Services,Greater Newcastle Sector, Hunter New England Local Health District, NSW, Australia
Pam MoreyMN, NP, STN, PhD(C)Nurse Practitioner, Advanced Wound Assessment Service, Silver ChainNurse Practitioner Course CoordinatorCurtin University, WA, Australia
Judith BarkerRN, NP, BHlthSc(Nurs), MNPNurse Practitioner — Wound ManagementAdjunct Associate Professor, University of Canberra, Synergy: Research Centre for Nursing and Midwifery Practice, CanberraCanberra Hospital, ACT Health, ACT, Australia
* Corresponding author

Volume 24 Number 4 – December 2016209
infection control policy13 led to a demand for updated wound management procedures. Wounds Australia established a working party to develop clinical guidance on procedures associated with prevention and control of wound infection. To inform the development of this document, a systematic review (SR) was undertaken.
AIMSThe objective of this review was to identify the contemporary evidence addressing topics associated with aseptic technique and infection control in wound management. Specific aims were to identify evidence related to cleaning considerations when performing a wound procedure, techniques for wound cleansing, environmental considerations in performing wound management and ways in which wound dressings can be handled and stored aseptically.
REVIEW METHODSThe review was undertaken using methods published by the Joanna Briggs Institute (JBI)14,15. An initial search was conducted in MEDLINE, CINAHL, EMBASE, Current Contents and the Cochrane library. All papers published in English up to October 2015 that related to topics outlined in the aims were eligible for inclusion. All research designs, qualitative research and opinion papers were eligible for inclusion; however, news items, letters and conference abstracts were excluded. Papers related to aseptic technique in the operating room, intravenous therapy or catheterisation were excluded. Search terms and MESH headings included: asepsis, non-touch technique, aseptic technique, steriliz/sation, disinfection, microbial and bacterial contamination, hospital, healthcare and community-acquired infection. These terms were used in combination with terms associated with wound care, wound dressings, equipment storage, cleansing, and equipment recycling. The working party reviewed the search strategy to ensure it captured the intended literature. On review of the evidence it was noted by the working party that significant changes in theory and practice have occurred in the field of aseptic technique. It was determined that inclusion would be limited to papers published between January 2000 to October 2015 in order that the review findings reflect contemporary knowledge. References cited in included manuscripts were also considered for inclusion.
All papers meeting inclusion criteria were critically appraised by two independent reviewers using the JBI suite of appraisal tools. For randomised controlled trials (RCTs) and pseudo-RCTs, critical appraisal evaluated randomisation, blinding, allocation concealment, withdrawals, comparability and equivalent treatment of participants, outcome measurement and statistical analysis14. Consistent with JBI appraisal, RCTs and pseudo-RCTs were ranked as high quality or lower15. For descriptive studies and case series, process for randomisation, sample inclusion, outcome measurement, management of confounders, participant withdrawal and data analysis were evaluated14. These studies received a
ranking of low or very low quality15. For interpretive and critical research, congruity of philosophies, methodology, research methods and analysis was evaluated, as well as reflexivity14. Qualitative research was ranked as high quality or lower15. Textual and opinion papers were evaluated based on source and logic of opinion and arguments, focus, referencing and support from peers14 and ranked as low or very low quality15.
Data extraction used standardised JBI tools. Quantitative results were not appropriate for meta-analysis as they generally addressed different topics, had heterogeneous methods, or were meta-analyses. These results are reported in a narrative format. Qualitative studies and opinion papers were analysed to identify themes, concepts and meanings within the research14, with identification of primary findings that were grouped in categories based on similarity in meaning. The categories were meta-aggregated in syntheses.
IDENTIFIED RESEARCHThe Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram16 is presented in Figure 1. The searches initially identified over 2,000 potential studies that was reduced to 57 papers that met inclusion criteria and were critically appraised. As indicated in Figure 1, most studies were excluded in the first review of the flagged references due to having insufficient focus on the topic of this review.
Of the 57 included papers, 14 were quantitative research papers17-30, six were SRs31-36, three were qualitative research papers10,11,37 and 34 papers were non-research articles7-9,38-68. The quantitative research consisted of six RCTs18,21,23,25,26,29 (level 1.c evidence) that were of low or moderate quality15. There was one very low quality before/after study22 (level 2.d evidence), five observational studies17,19,20,28,30 (level 2 and 3 evidence), one very low quality cohort study24 (level 3.c evidence) and a very low quality cross-sectional study27 (level 4.b evidence). The SRs31-36 (level 1 evidence) ranged in quality from low to very high and the qualitative research10,11,37 (level 3 evidence) was of moderate to high quality. The majority of findings in this review arose from textual papers providing low and very low quality evidence. Table 1 presents summaries of the research papers.
Quantitative results from the literature
Cleansing solutions and technique
SRs and studies exploring irrigation fluids received the most attention in quantitative research. As the individual studies18,19,21,23,26,29 (Table 1) were included in identified SRs, only SR results are reported below; however, none of the individual RCTs established significant differences in infection rates between wounds cleansed with sterile solutions versus tap water18,19,21,23,26,29.
A high quality SR36 compared sterile saline (n=326) to tap water (n=257) for cleansing lacerations, acute and chronic wounds. Pooled results from two RCTs showed no significant
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 210
difference in wound infection rates, with tap water slightly less likely to result in infection (odds ratio [OR] 0.79, 95% confidence interval [CI] 0.36 to 1.72, p=0.55)36.
A moderate quality Cochrane SR33 compared cleansing methods for lacerations, open fractures, chronic and surgical wounds. Infection rate in all wound types (3 RCTs) was not significantly different between tap water cleansing and no cleansing (relative risk [RR] 1.06, 95% CI 0.07 to 16.50, p=not significant [ns]). There was no difference in infection rates in all acute sutured wounds (3 RCTs) between tap water versus sterile saline irrigation (RR 0.66, 95% CI 0.42 to 1.04, p=ns). Cost-effective analyses favoured tap water33. This Cochrane review reached the same conclusions as earlier systematic reviews by the same research team34,35.
A low quality SR compared tap water to sterile saline. Significantly more wounds cleansed with sterile saline became clinically infected (saline 7.1% versus tap water 4.3%, RR 0.62, 95% CI 0.39 to 1.01, p=0.05). There was no significant difference in wounds with positive cultures (saline 3.1% versus tap water 4.4%, RR 1.53, 95% CI 0.79 to 2.99, p=0.21)31.
A low quality SR compared bathing to no bathing for post-surgical foot wounds. Normal hygiene groups showered at 1–5 days postoperative (n=1,639). Patients abstaining from foot hygiene waited until sutures/staples removal (n=511). There were no significant differences in surgical site infection rates in any study32.
Although confounding factors are noted (for example, administration of saline at cooler temperatures than water) when controlled for these factors the outcomes did not change. Findings from the high-level evidence31,33-36 indicated no increase in wound infection rates associated with cleansing wounds in tap water.
Reuse of wound dressing products
A moderate quality observational study investigated rate of contamination of opened hydrogel products. The products were opened after handwashing, using clean gloves and away from direct patient care. After 28 days, one package from 60 random samples returned a positive bacterial culture. The sample collection technique may not reflect clinical practice17. A very low quality observational study reported contamination rates for opened dressings and reusable equipment stored in different containers in patients’ homes. After 14 days, 75% of samples (n=21) were contaminated30. Another low quality observational study investigated contamination rates for randomly selected multi-use saline flasks stored in hospital settings. Approximately half of the samples were found to be contaminated20.
Wound dressing practice
In a low quality RCT, leaving surgical wounds uncovered after surgery (n=235) was compared to wound dressings applied in the operating theatre (n=216). Patients were reviewed after seven days for clinical signs of infection and no significant difference in infection rates was found (exposed wounds 1.7% versus covered wounds 1.4%, p=ns)25.
Figure 1: PRISMA review flowFigure 1: PRISMA review flow
Original references flagged in searches as potentially meeting inclusion criteria (n> 2,000)
Excluded: (n=86) Published prior to 2000 (n=33) No unique information, summarises studies already included (n=19) Not focused on aseptic technique (n=12) Letters, abstracts, duplicate reports (n=12)Low quality, including no methods or no results reported (n=5) Libraries unable to obtain (n=3) Not wound care related (n=3)
Excluded as not sufficiently related to topic, letters to editor, duplicate reports and conference abstracts (n=37)
Full review against inclusion criteria and critically appraised (n=143)
Review of title/abstracts against inclusion criteria (n=180)
Included studies (n=57): Systematic reviews (n=6) Quantitative research (n=14) Qualitative studies (n=3) Non-research papers (n=34)
Excluded: duplicate references (majority of studies), not sufficiently related to topic (n>1,820)
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016211
A very low quality cohort study compared sterile (n=1,070 admissions) and clean (n=963 admissions) dressing procedures for surgical wounds. The outcome measure was positive wound culture established by wound swab. There was no significant difference in surgical site infection rates (0.84% versus 0.83%, p=ns) and the clean procedure was faster (10 minutes versus 13 minutes)24.
Aseptic technique education and behaviours
A very low quality before/after study investigated an education program delivered to medical students. The course was based on principles associated with handwashing and dressing procedures. After 10 weeks, there was a significant decline (p<0.001) in the ratio of students who were able to achieve a pass mark in the assessment, indicating the education had no prolonged influence on practice. Poor role modelling and lack of resources were identified as contributing to poor outcomes22. A very low quality observational study reported clinical practice amongst nurses in community settings. Practice was established through direct observation and validated in interviews with participants. As many as 40% of nurses did not engage in handwashing before a procedure28.
Qualitative results from the literature
Three hundred and eighty-six findings were extracted from qualitative studies and non-research articles. Using the JBI ratings15, 60 of the findings were rated as unequivocal, 218 were rated as credible and 20 findings were rated as unsupported, generally where an assertion was made without any supporting reference. These findings were grouped in 65 categories and aggregated into 23 syntheses (Figure 2).
Current evidence base
Synthesis 1: Research on wound cleansing and aseptic technique is insufficient and that which is available is poorly translated into practice.
There is a lack of research on aseptic techniques9,65. Inconsistencies in terminology and practice guidance, and ongoing change to theory interpretation has a negative impact on compliance7-9. The need for more research on aseptic technique, including translation to different clinical settings was highlighted38,44,48.
Handwashing practices
Six categories aggregated into two syntheses represented textual findings on handwashing.
Synthesis 2: Liquid alcohol rub, antimicrobial hand wash or soap and water can be used for washing hands. When hands are visibly soiled, use soap and water.
Articles referred to three handwashing solutions: alcohol-based rubs, antiseptic/antimicrobial hand washes and soaps/detergents. Alcohol rub has broad spectrum activity51 and is quick to apply without the need for water8,40,45,50,51,55,57,59. A small risk of fire from alcohol exposed to a heat source before complete evaporation45 and potential for dry hands are
reported. Some texts suggest alcohol-based hand rubs are not appropriate when hands are visibly soiled40,55. Antiseptic or antimicrobial hand wash with water is suggested for cleaning visibly dirty hands40,45,51,55 although it may be more expensive or cause irritation51. Antimicrobial-impregnated towels are an alternative for visibly clean hands, but not a replacement for soap and water40,45,55. Opinion articles agreed that soap and water is appropriate for visibly soiled hands40,49,51,55,64.
Synthesis 3: Handwashing should occur before and after patient contact, regardless of the use of gloves, and consist of vigorous rubbing for at least 15 to 30 seconds.
Hands should be washed before/after patient contact, or after contact with body fluids, to prevent cross-contamination7,40,55,56,64. Use of gloves does not preclude the need to wash hands40,55-57,59 because hands may become contaminated when removing gloves56. Handwashing should be a vigorous process covering all hand surfaces using soap and water or an alcohol rub40,55,59. Most papers suggested that handwashing should take at least 15 seconds40,55; however, one suggested at least 30 seconds59.
Gloves and personal protective equipment
Three syntheses related to the use and selection of gloves, and one related to other personal protective equipment.
Synthesis 4: Gloves are required to prevent contamination and cross-infection; however, they do not replace routine handwashing.
Textual findings highlighted that the primary purpose of gloves is to prevent contamination, between the patient and the nurse, or cross-infection between different anatomical sites on the same patient40,44,51,55,59. It was suggested that gloves are worn when there is a risk of coming into contact with bodily fluids or non-intact skin40,55; when removing old wound dressings45; and for invasive activities51. Use of gloves does not preclude handwashing45,57, regardless of the implementation of double-gloving45. Findings suggested gloves be removed immediately following care40,55.
Synthesis 5: Selection of gloves is guided by the procedure to be performed, risk of contamination, latex allergies and cost.
Synthesis 6: Sterile gloves are required for surgical aseptic non-touch technique, surgery and invasive aseptic procedures and clean gloves are for non-sterile procedures/standard aseptic non-touch technique.
Level of expected direct contact with susceptible sites44,53,57 should guide glove selection. Latex allergy influences glove choice44,50,59, and some texts identified the increased cost of sterile gloves as a factor in selection59,62. There was agreement that sterile gloves are required for sterile procedures44,48,51,57,61. Within the literature ‘sterile procedures’ referred to invasive activities44,51 surgical procedures44, aseptic technique44,
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 212
aseptic non-touch technique (ANTT) requiring direct contact with key parts61, and delivering sterile pharmaceuticals44. Clean, non-sterile gloves were suggested for removing old wound dressings48, performing clean procedures48 and performing procedures that do not require direct contact with the key parts61.
Synthesis 7: Wearing appropriately selected personal protective equipment helps to reduce the risk of cross-infection from exposure to body fluids or airborne contamination.
Personal protective equipment is designed to reduce the risk of contamination for both the patient and clinician57,64. When protective equipment is used, the clinician is protected from body fluid exposure (for example, blood splashes)51,57 and the patient is protected from the clinician as a source of infection risk59. Textual findings focused on using plastic aprons51,59 with selection of equipment based on the level of risk of body fluid exposure64.
Wound management environment
Two syntheses addressed the general and specific environment in which wound management is conducted.
Synthesis 8: Actions should be taken to reduce airborne and other infection risks in the home and hospital to ensure wound care is conducted in a clean environment.
The requirement for a clean environment, free from airborne and other infection risks was described51,61,64. The risk posed by carpets, soft furnishings and pets was reported64. Strategies to reduce environmental risk included reporting infection risk in the home to authorities64, ensuring there are cleaning routines that incorporate the ventilation and water supplies64; reducing airborne infection by closing windows, reducing foot traffic and turning off fans64; leaving the wound exposed for the shortest time64; and disposing of waste promptly and appropriately64.
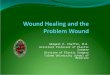
Synthesis 9: A wound management field can be established on a clean surface in a space at low risk of environmental contaminants. Once established, introduction of contaminated external objects should be avoided.
The importance of establishing a sterile local field on a clean surface8,57,64 was discussed. Strategies for establishing a sterile field in a clean environment included using a visually clean dressing trolley57 or cleaning a hard surface with a broad spectrum disinfectant64. In the community, a plastic apron or lid could be used8,64. Considering the wound, an extension of the wound management field was suggested7, as was ensuring the wound management field remains sterile57. Findings were consistent that objects external to the wound and field should not contaminate the wound management field7,57,61. Clinicians could use either a critical aseptic field into which only sterile equipment is introduced (for example, for an invasive or extensive procedure) or a general aseptic field in which key parts are individually protected within the field (for example, for a simple wound procedure)61.
Cleansing solutions and technique
Eighteen categories were aggregated into six syntheses related to wound cleansing.
Synthesis 10: An ideal wound cleanser should adequately clean the wound, not cause cell damage or sensitivity and have a long shelf life.
The principle of doing no harm and preventing infection were highlighted as guiding the choice of wound cleanser9. Consideration to the toxicity of a cleanser and its potential to cause sensitivity was highlighted42,63. Using an expired product should be avoided57 by selecting a wound cleanser with a long shelf life42,63. The ability to effectively remove organic material and reduce bioburden are other considerations42,63.
Synthesis 11: An assessment should be conducted by the interdisciplinary team to determine if a wound bed should be cleansed, and if so, the cleansing process to use.
Not all wound beds require cleansing as a wound may heal without disruption if there are no visual contaminants or signs of infection39,58. The wound management team could work together to determine the best approach for individual patients9,39,58.
Synthesis 12: Normal saline, potable tap water, sterile water and low concentration antimicrobial solutions are safe and effective wound cleansers. Antiseptics are not a good choice for wound cleansing.
Sterile saline is an isotonic solution that has no impact on tissue repair processes42,46; therefore it is a safe and traditional option62, particularly in hospital environments46 or for vulnerable wounds9. Tap water, sterile water and normal saline were all reported as safe; however, none of these solutions reduces bioburden in the wound42,46,56,57,67. Antimicrobial solutions reduce bioburden63,67, although concentrations should be selected carefully in light of potential cell toxicity63,67. Use of skin cleaners and antiseptics in wound cleansing is warned against39,42,58,63. Cell toxicity42,58,63, potential carcinogenicity41, insufficient contact time with the wound to effectively reduce bacteria levels39 and association with antibiotic-resistant bacteria39 were concerns.
Synthesis 13: Apply a wound cleanser at a lukewarm temperature with consideration to the potential for cross-infection and using low pressure to irrigate the wound bed.
Irrigation at a low pressure (4 to 15 pounds per square inch) using a syringe or faucet tubing is suggested for promoting debris removal without disrupting granulating tissue42,56,62,65. Applying fluid at lukewarm temperature avoids vasoconstriction that lowers tissue healing capacity9,45,46,54,62,66. The potential for cross-infection between patients, or contaminated water from dirty body areas flowing over a wound are considerations when washing in a shower9,54,58. Directing fluid flow appropriately when irrigating54 was noted as another strategy to prevent cross-infection.
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016213
Synthesis 14: Good quality tap water is a cost-effective option for cleansing dirty wounds, chronic wounds and wounds with closed or sutured edges, although it may cause pain.
Benefits and disadvantages of tap water were discussed39,42,46,54,56,58,62,66. Water was noted as acceptable for sutured39, sacral/perineal56, open traumatic56, and chronic56 wounds, and wounds with sealed edges39. Ensuring high quality water is important54,56,62,66, although commentators noted that in cities with monitored and drinkable tap water it is sufficiently safe for wounds54,56,62,66. Texts suggested using running tap water for at least 30 seconds62 or soaking wounds in a bucket58. Higher, constant pressure62, large fluid volumes62, patient satisfaction66 and reduced time66 are advantages of water. Lack of additional equipment (for example, syringes) contributes to the cost-effectiveness of water46,54,62,66. However, there is potential that water may cause pain due to increasing osmotic pressure46.
Synthesis 15: Precautions can be taken to reduce the risk of potential contamination of water sources.
Another disadvantage is the potential for contaminated tap water9,41. One commentator suggested a risk of acquiring virulent pathogens or biofilm from hospital water41. This risk may be higher for immunocompromised patients41. However, precautions can be taken41,42,56. Water filters41, running taps for a few minutes before using the water42 and evaluating the water storage and delivery before use9 were suggested.
Selecting wound care technique and equipment
Four syntheses addressed selection of wound care techniques and equipment.
Synthesis 16: Selection of sterile/surgical ANTT or clean/standard ANTT is determined by the level of risk posed to the patient by his or her health status, the environment, factors associated with the wound and the type of wound management procedure being performed.
The infection risk from the surrounding environment is one consideration in selecting a wound management technique7,37,44,57,60,61,68. Findings illustrated that both the health care setting7,37,44,68 and the storage of equipment68 influences the ability to maintain a sterile or aseptic environment. The complexity of the procedure is a contributing factor, for example extensive debridement, wound packing and necessity to touch key parts were considered more invasive and requiring greater precautions44,51,57,60,61,68. Patient-related factors (for example, immune status) may also contribute to the risk of infection from a dressing procedure7,44,57,60,68. The chronicity, depth and location of the wound also contribute to selection of a technique7,44,50,56,57,68. Rigorous asepsis was considered to be inappropriate for chronic wounds50,56,57,68.
Synthesis 17: Simple wound management procedures on low-risk patients can be performed with non-sterile but clean equipment, solutions and gloves. More complex procedures or procedures in higher risk patients require surgical aseptic
non-touch technique, using sterile gloves, solutions and equipment.
Textual findings referred to clean technique/standard ANTT and aseptic technique/surgical technique/surgical ANTT. The first technique is appropriate for routine dressing changes without surgical conservative debridement and simple procedures lasting less than 20 minutes37,61,68. This technique was reported to involve a clean surface, non-sterile gloves and clean equipment and irrigation fluids (for example, tap water)37,61,68. The surgical ANTT requires sterile gloves and equipment and a sterile irrigation fluid, with a strict aseptic field37,56,57,61,68. The findings suggested this procedure was appropriate for patients at high infection risk, wounds requiring surgical conservative debridement, complex/invasive procedures with many key parts or procedures lasting longer than 20 minutes56,57,61,68. One commentator suggested that this should be standard practice56.
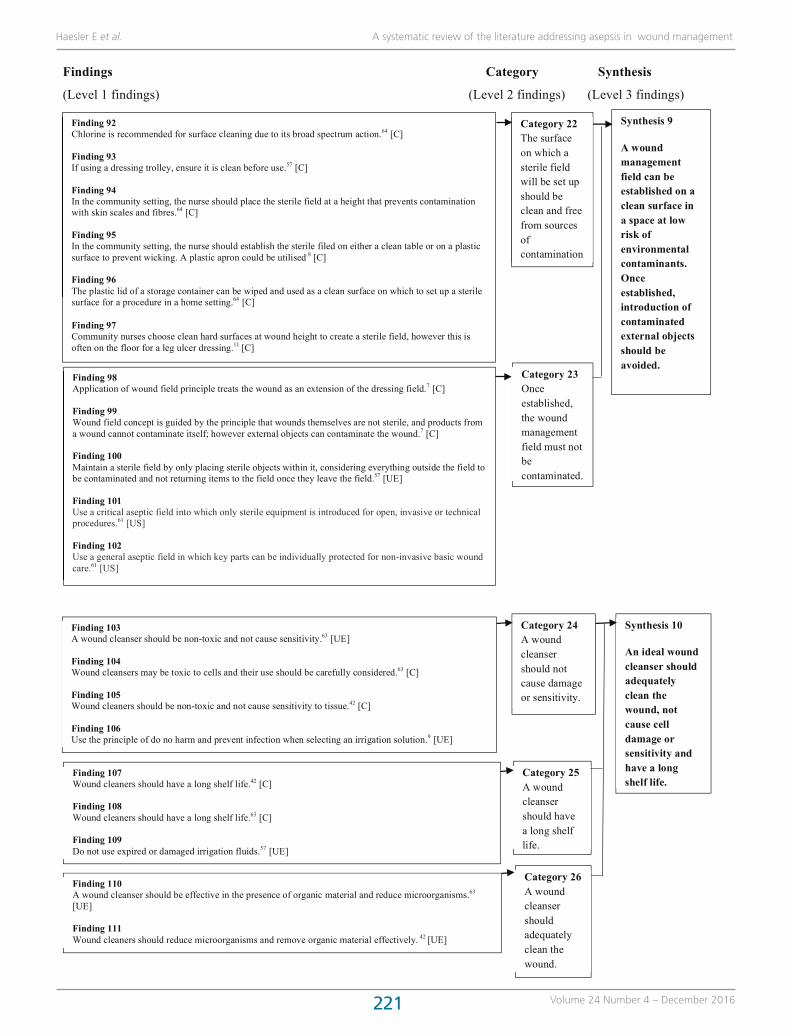
Synthesis 18: Wound management equipment should be single use or cleaned with alcohol preparations. Using cleansers and wound dressings in smaller packages reduces waste and contamination risk.
Ensuring products are cleaned appropriately via sterilisation, disinfection or decontamination is important57,61,64. Using alcohol preparations or wipes and vigorously rubbing equipment to remove visual soiling cleans reusable products61,64, although single-use products may be easier, especially in community settings64. Wastage of excess products was noted as a concern, especially from dressing packs with pre-selected materials that are not always appropriate for the procedure8,11. Selecting smaller packages to reduce waste or risk of contamination from reusing products was suggested45,65.
Synthesis 19: When performing surgical ANTT the wound management field must remain free of non-sterile items, including equipment, cleansing fluids and gloved hands that have touched a non-sterile object.
Commentary highlighted the importance of all sterile equipment being free from potentially contaminated objects, including water that had touched surrounding skin during washing or forceps that had touched the wound bed7,8,43,51,68. One text referred to a dirty hand or forceps/a clean hand or forceps7. The difficulty clinicians have in manoeuvring forceps was raised7,56, and using a gloved hand for parts of a procedure was proposed as an optional wound management method7,8,56, if the potentially contaminated hand could be maintained away from the wound management field7,68.
Managing patients with known infection
Synthesis 20: Extra infection control precautions should be taken for people with known infection.
One opinion article addressed infection control for patients with known methicillin-resistant Staphylococcus aureus (MRSA)49. Findings indicated that clinicians should take
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 214
additional precautions by thoroughly disinfecting surfaces, putting down plastic sheeting and using disposable equipment when possible49. Reusable equipment could be cleaned immediately49. Double-bagging waste products before disposal may reduce cross-infection49. Diligence is required in handwashing and the use of personal protective equipment49.
Product storage
Synthesis 21: Wound management products should be stored in dry, clean environments to reduce risk of contamination and cleansers should be dated on opening and discarded if visually contaminated or according to organisation policy.
Storing dressing products in a clean, dry space was suggested56,64. Wound cleansers should be dated and refrigerated on opening, although there is no set time frame after which they should be disposed45. One commentator mentioned discarding fluids if there is visual contamination, or to follow the organisation policy45. Risks posed by storing gloves in a manner that attracts mould or contamination were noted50,62.
Structural support
Two syntheses summarised eight categories related to structural support for aseptic technique and infection control.
Synthesis 22: Staff education that incorporates skills practice, simulation learning, theoretical knowledge update and procedures for different clinical settings is essential in promoting best practice in aseptic technique and infection control.
Importance of education was highlighted8,11,38,39,44,49-51,57,59,64. Some references suggested that clinicians develop ritualistic practice and may not fully understand theoretical concepts8,11,39. Qualitative studies indicated that community nurses experience frustration and have fatalistic attitudes11 that may influence the way in which they perform wound care10. Ongoing reinforcement of knowledge and skills through regular education using simulation learning53,57, visual feedback (for example, dye in handwashing exercises)59, hands-on practice with feedback64 and didactic lectures53 is suggested.
Synthesis 23: Best practice in aseptic technique and infection control procedures is promoted through development of facility policies, regular risk surveillance, annual auditing of staff practice, engaging with staff and patients and provision of acceptable hand hygiene products.
Regular risk surveillance7,50,59,64 promoting a culture of clinicians identifying risks50, and root cause analysis64 were highlighted as promoting quality improvement. Engaging with staff and patients by working with a wound champion to promote best practice38,64, empowering patients to ask clinicians about hand hygiene59 and ensuring adequate staffing levels may promote best practice51. Commentators
proposed incorporating annual handwashing audits into quality improvement programs8,38,40,55,59. The importance of local policies and procedures was raised8,48,61, especially for topics for which there is insufficient evidence to make recommendations48. Finally, provision of products that are acceptable to clinicians (for example, low allergen) may promote handwashing40,55.
DISCUSSIONThere was general agreement between the quantitative and qualitative/textual findings in this review. Use of potable tap water for irrigation received the most attention, and findings from SRs, RCTs and non-research articles were in agreement that for many wound types, cleansing with good-quality, lukewarm tap water does not increase risk of wound infection18,20,21,23-26,29,32-36,39,42,46,54,56,58,62,66. This evidence should be considered when selecting appropriate and cost-effective wound management techniques.
Limited evidence was available on other topics of interest. No significant evidence was identified regarding strategies for managing opened wound dressing packages and minimal commentary on the advantages and risks of this practice was identified. One moderate quality study17 suggested reusing hydrogel products may be safe if the product was dispensed in controlled conditions. A very low quality study suggested contamination of opened wound dressings is an issue in community settings30 and commentators suggested using smaller packages to reduce waste45,65. There was also limited evidence on methods of performing aseptic technique, with technique details often derived from unreferenced opinion sources61. There is a strong need for well-designed studies exploring these issues.
There was a paucity of evidence on environmental factors in conducting wound care identified in the available literature. There was agreement that the environment in which wound care is conducted should be clean51,61,64, with guidance generally focused on strategies to address the potential risk from airborne contamination51,61,64. Practical solutions for maintaining asepsis in home care settings were provided8,51,61,64; however, the evidence supporting these practices was at best minimal.
This review is not without limitations. Foremost, the literature search was limited to journal articles. Reports12 and guidelines13,69 also inform this topic; however, these resources are developed from the existing body of evidence and are not specific to wound management. The search terms used for this review focused specifically on asepsis in wound management. It is probable that evidence on some included topics is available in the broader literature. Except for evidence related to irrigation, the evidence was primarily from non-research texts of low and very low quality and this should be considered when evaluating the adoption of the suggestions into practice. It should be noted that theory and translation in this field has changed substantially over time. The reviewers attempted to identify a cut-off date in order
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016215
to exclude outdated concepts; however, given that much of the findings were opinion, some ideas may be anachronous.
CONCLUSIONSThe findings of this systematic review highlighted the lack of high-level evidence in many clinical areas associated with aseptic wound management practice. There is a need for further research in this field to establish with certainty the procedures that are necessary to prevent and control wound infection. Until such research exists, guidance based on the
current evidence base, evidence derived from other clinical procedures (for example, intravenous therapy), broader guidelines12,13,69 and expert opinion is required to assist facilities in developing local policies and procedures.
ACKNOWLEDGEMENTSSue Atkins and Liz Howse undertook second review of some papers included in this systematic review.
Wounds Australia contributed to the funding of the systematic review.
1
Figure 2: Thematic analysis of qualitative research and textual findings
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Synthesis 1
Research on wound cleansing and aseptic technique is insufficient and that which is available is poorly translated into practice
Finding 1 Inadequate advice on translating evidence into practice has led to variety in ways clinicians incorporate wound cleansing into aseptic technique.8 [C] Finding 2 There is inconsistency in irrigation technique between trials, particularly with respect to volume and pressure.9 [UE] Finding 3 Research conducting on irrigating acute wounds may cannot be extrapolated to diabetic foot ulcers, especially those with exposed tendon and bone.9 [C] Finding 4 Changes in wound care theory and practice can cause confusion for students and practising health professionals.7 [UE] Finding 5 Debate over use of clean versus aseptic technique have a negative impact on compliance with standardised technique.8 [C]
Category 1 Inconsistencies and changes in interpretation of evidence and theory related to wound cleansing into clinical practice has a negative impact on compliance.
Finding 6 Previous evidence on optimal pressure for removing bacteria while preventing contamination and disruption to wound healing is based on small studies and may not be reliable.65 [C] Finding 7 Studies investigating cleansing have inadequate sample sizes and have methodological limitation (e.g. do not ensure cleansers are equivalent temperature). 9 [C]
Finding 8 There is insufficient evidence to provide comprehensive recommendations for appropriate cleansing methods for traumatic wounds.65 [C]
Finding 9 More research is needed on how nurses currently perform wound care and the effectiveness of different wound care strategies.48 [UE] Finding 10 More research on the effectiveness and implications of different dressing technique is required.38 [C] Finding 11 Further research and evidence is required on influence of clean vs sterile gloves in aseptic techniques.48 [C]
Category 3 More research is required on aspects of performing aseptic technique.
Category 2 There is insufficient good quality existing evidence on wound cleansing.
[UE] unequivocal [C] credible [US] unsupported
1
Figure 2: Thematic analysis of qualitative research and textual findings
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Synthesis 1
Research on wound cleansing and aseptic technique is insufficient and that which is available is poorly translated into practice
Finding 1 Inadequate advice on translating evidence into practice has led to variety in ways clinicians incorporate wound cleansing into aseptic technique.8 [C] Finding 2 There is inconsistency in irrigation technique between trials, particularly with respect to volume and pressure.9 [UE] Finding 3 Research conducting on irrigating acute wounds may cannot be extrapolated to diabetic foot ulcers, especially those with exposed tendon and bone.9 [C] Finding 4 Changes in wound care theory and practice can cause confusion for students and practising health professionals.7 [UE] Finding 5 Debate over use of clean versus aseptic technique have a negative impact on compliance with standardised technique.8 [C]
Category 1 Inconsistencies and changes in interpretation of evidence and theory related to wound cleansing into clinical practice has a negative impact on compliance.
Finding 6 Previous evidence on optimal pressure for removing bacteria while preventing contamination and disruption to wound healing is based on small studies and may not be reliable.65 [C] Finding 7 Studies investigating cleansing have inadequate sample sizes and have methodological limitation (e.g. do not ensure cleansers are equivalent temperature). 9 [C]
Finding 8 There is insufficient evidence to provide comprehensive recommendations for appropriate cleansing methods for traumatic wounds.65 [C]
Finding 9 More research is needed on how nurses currently perform wound care and the effectiveness of different wound care strategies.48 [UE] Finding 10 More research on the effectiveness and implications of different dressing technique is required.38 [C] Finding 11 Further research and evidence is required on influence of clean vs sterile gloves in aseptic techniques.48 [C]
Category 3 More research is required on aspects of performing aseptic technique.
Category 2 There is insufficient good quality existing evidence on wound cleansing.
[UE] unequivocal [C] credible [US] unsupported
Figure 2: Thematic analysis of qualitative research and textual findings
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 216 2
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Category 5 Antimicrobial hand wash can be used to wash hands that are visibly soiled.
Synthesis 2
Liquid alcohol rub, antimicrobial hand wash or soap and water can be used for washing hands. When hands are visibly soiled, use soap and water.
Finding 12 Alcohol rub cannot remove spores, does not have persistent antibacterial activity, is flammable, does not remove soiling and can cause dry hands if used frequently.51 [C] Finding 13 When hands are not visibly soiled they can be cleaned with an alcohol-based hand rub.40,55 [C] Finding 14 Alcohol rub has broad spectrum activity that is simple, has fast action, is cost effective and contains emollient.51 [C] Finding 15 When using alcohol-based hand rubs, rub hands together after application until all alcohol has evaporated to reduce the small risk of fire.45 [C] Finding 16 Alcohol rub is faster to use than soap and water.59 [C] Finding 17 Alcohol based hand gels can be used as often as required without the need for soap and water washes in between applications.45 [C] Finding 18 Use an alcohol based hand rub.57 [C] Finding 19 Liquid aqueous alcohol rub can be used for hand washing instead of soap and water.50 [C] Finding 20 In the community setting, alcohol gels can be used for effective hand hygiene.8 [C]
Finding 26 Visibly dirty hands or those contaminated with protein material should be washed with soap and water.40,55 [UE] Finding 27 Wash visibly soiled hands with soap and water rather than alcohol rub.49 [UE] Finding 28 Hand hygiene can be achieved through washing with either soap and water or using alcohol decontaminant.64 [UE] Finding 29 Plain detergent, warm water and paper towels remove visible soiling and reduce skin irritation.51 [UE]
Category 4 Liquid alcohol rub can be used for washing hands, ensuring the all alcohol evaporates after application.
Category 6 Regular soap and water can be used to wash visibly soiled hands.
Finding 21Antiseptic hand wash, warm water and paper towel remove visible soiling, and have residual activity against microbes for approximately 6 hours.51 [C] Finding 22Antiseptic hand wash, warm water and paper towel is expensive, require nearby sink and waste bin, is time consuming and may irritate the skin.51 [C] Finding 23When hands are visibly soiled they can be cleaned with antimicrobial soap and water.40,55 [C] Finding 24Antimicrobial impregnated towels are not an acceptable replacement for alcohol based hand rubs or antibacterial soap. 45 [C] Finding 25Antimicrobial impregnated wipes are an alternative to non-antimicrobial soap and water but are not a replacement for alcohol hand rub or antimicrobial soap and water.40,55 [C]
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016217 3
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Category 8 Hands should be washed before and after wearing gloves.
Finding 30 Preventing contamination of the wound from dirty hands by implementing rigorous handwashing is the most effective way to prevent wound infection.7 [UE] Finding 31 Hands should be washed before direct contact with patients, after contact with patients and after contact with body fluids, including wound dressings.40,55 [C] Finding 32 Hands should be washed when moving from a contaminated part of the patient to a non-contaminated part of the patient during care.40,55 [C] Finding 33 Handwashing frequency should be determined based on patient and clinician factors.56 [C] Finding 34 Hands should be washed before and after touching the patient, before and after aseptic procedures, after body fluid exposure and after touching patient surroundings.64 [UE]
Finding 39 When using soap and water, hands should be rubbed together vigorously covering all surfaces for at least 15 seconds.40,55 [C] Finding 40 When using alcohol-based hand rub hands should be rubbed together, covering all surfaces until the hands are dry.40,55 [C] Finding 41 Hand disinfectants should be used for at least 30 seconds.59 [UE]
Category 7 Hands should be washed before and after patient care to prevent contamination.
Category 9 Hands should be rubbed vigorously for 15 to 30 seconds, covering all hand surfaces.
Finding 35 Wash hands before and after using sterile gloves.57 [C] Finding 36 Handwashing should be conducted before and after procedures, even if gloves are worn.59 [UE] Finding 37 Hands should be washed after wearing gloves because hands could become contaminated under the gloves or when the gloves are removed.56 [C] Finding 38 Hands should be washed after removing gloves.40,55 [UE]
Synthesis 3
Hand washing should occur before and after patient contact, regardless of the use of gloves, and consist of vigorous rubbing for at least 15 to 30 seconds.
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 218 4
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Category 11 Gloves do not replace hand washing.
Synthesis 4
Gloves are required to prevent contamination and cross infection; however, they do not replace routine handwashing.
Finding 42 Gloves should be worn when contact with blood or non-intact skin could occur.40,55 [UE] Finding 43 Gloves should be changed when moving from a contaminated patient site to a non-contaminated patient site.40,55 [C] Finding 44 Gloves should be removed when patient care is completed.40,55 [UE] Finding 45 Gloves are required for all procedures to protect nurses and patients from infection.59 [C] Finding 46 Aim of wearing gloves is to reduce cross infection, reduce contamination of hands or to protect the hands from chemicals.48 [UE] Finding 47 Gloves must be worn when removing an old dressing to prevent risk of cross-contamination.45 [C] Finding 48 Sterile gloves are required for invasive activities to protect the patient and health professional.51 [C]
Category 10 Gloves prevent contamination and cross infection.
Finding 49 After removing gloves, wash hands with either antiseptic hand wash or antiseptic rub.45 [C] Finding 50 Double gloving is not an acceptable replacement for washing hands (with either soap and water or an antiseptic rub) and donning new gloves.45 [C] Finding 51 Gloves are not a substitute for hand hygiene.57 [C]
Category 14 Cost is a consideration in selecting gloves.
Finding 56 Selection of gloves should be based on any allergies of nurse and patient.48 [C] Finding 57 Selection of gloves should be considered carefully due to latex allergy risks.59 [C] Finding 58 Before using latex gloves, assess the risk of latex allergy of the nurse and the patient.50 [UE]
Synthesis 5
Selection of gloves is guided by the procedure to be performed, risk of contamination, latex allergies and cost.
Finding 52 If forceps are used sterile gloves are not required for aseptic non touch technique.53 [C]
Finding 53 Selection of gloves should be based on their purpose. 48 [C] Finding 54 Selection of clean versus sterile gloves should be determined by level of expected contact with the wound.57 [C]
Finding 55 Selection of gloves should be guided by a risk assessment that includes assessment of contact with susceptible sites or devices, type of potential contamination and whether it is a sterile or a non-sterile task.48 [C]
Category 12 The type of procedure, level of contact and risk of contamination influence the choice of glove types.
Finding 59 Selection of gloves should be considered carefully due cost factors.59 [C] Finding 60 Sterile gloves are costly and may lead to requiring an assistant.62 [C]
Category 13 Latex allergy is a consideration in selecting gloves.
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016219 5
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Finding 70 When performing sterile procedure, clean gloves are used for removing the old dressing.48 [C] Finding 71 Clean gloves may be contaminated from other staff taking gloves from the box; however, evidence shows this risk does not influence wound infection rates.62 [C] Finding 72 When performing clean procedure, two pairs of clean gloves are required, one for removing the old dressing and one for applying a new dressing.48 [C] Finding 73 Clean, non-sterile gloves may be an acceptable alternative to sterile gloves.56 [C] Finding 74 Use clean non-sterile gloves if there is no requirement to touch key parts in an aseptic non-touch technique.61 [US]
Finding 61 Sterile gloves should be worn for surgical wound dressings and surgical procedures. 48 [C] Finding 62 Sterile gloves should be worn for procedures requiring aseptic technique.48 [C] Finding 63 Sterile gloves should be worn for invasive procedures and insertion of invasive devices, especially in immune compromised patients.48 [C] Finding 64 Sterile gloves should be worn for administering sterile pharmaceutical preparations.48 [C] Finding 65 Sterile gloves are required for invasive activities to protect the patient and health professional.51 [C] Finding 66 Sterile gloves are required for invasive activities to protect the patient and health professional.51 [UE] Finding 67 When performing sterile procedure, sterile gloves are used to apply the new dressing.48 [C] Finding 68 Do not touch non-sterile items after donning sterile gloves.57 [UE] Finding 69 Use sterile gloves for aseptic non-touch techniques if there is a need to touch key parts.61 [US]
Category 15 Sterile gloves are required for surgery, aseptic procedures, invasive procedures, procedures in which the wound will be touched and for inserting invasive devices or sterile pharmaceuticals.
Synthesis 6
Sterile gloves are required for surgical aseptic non-touch technique, surgery and invasive aseptic procedures and clean gloves are for non-sterile procedures/ standard aseptic non-touch technique.
Category 16 Clean gloves are worn as an alternative to sterile gloves for removing old dressings and for aseptic non-touch technique (ANTT) where there will be no requirement to touch the wound or key parts.
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 220 6
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Category 18 Selection of personal protective equipment should be guided by the level of risk of exposure to body fluids and airborne infection.
Synthesis 7
Wearing appropriately selected personal protective equipment helps to reduce the risk of cross infection from exposure to body fluids or airborne
Finding 75 Personal protective equipment is designed to prevent transmission from patient to healthcare professional.64 [UE] Finding 76 Use personal protective equipment when there is a risk of contamination to the caregiver, including contact with body fluids.51 [UE] Finding 77 Personal protective equipment should be used to prevent cross contamination and/or exposure to body fluids.57 [UE] Finding 78 Uniforms and jewellery are source of potential contamination.59 [C]
Category 17 Personal protective equipment is used to reduce the risk of cross infection.
Finding 79 Disposable plastic apron should be worn when undertaking tasks that risk contaminating the wearer’s clothing (e.g. splash back from irrigation).51 [C] Finding 80 Plastic aprons should be used to reduce cross infection and changed between patients.59 [C] Finding 81 Selection of personal protective equipment is determined by the level of risk, including exposure to body fluids and airborne infections.64 [UE]
Category 20 The home can be a source of contamination.
Synthesis 8
Actions should be taken to reduce airborne and other infection risks in the home and hospital to ensure wound care is conducted in a clean environment.
Finding 82 Cleanliness of the care environment influences actual and perceived risk of infection and should be maintained in all care environments.64 [C] Finding 83 Do not undertake aseptic procedures at times when environmental risk is higher, such as during housekeeping.51 [C] Finding 84 The environment in which aseptic non-touch technique is performed should be clean and dust free.51 [C] Finding 85 Infection sources include the health professional and the immediate environment.61 [US]
Category 19 Environment in which wound care is attended must be clean.
Finding 86 Carpets and soft furnishings may be a source of infection. 64 [UE] Finding 87 Consider the implications for cleanliness of pets in the home. 64 [UE]
Category 21 Effort should be made to reduce infection sources (including airborne infection sources) in the area in which wound care is performed.
Finding 88 If a home environment poses significant infection risk, assistance should be provided to reduce the risk and when high the risk should be reported to local and environmental agencies.64 [C] Finding 89 Cleaning schedules and standards and the ventilation and water supplies should be monitored regularly.64 [C] Finding 90 Reduce airborne infection risk by closing windows, turning off fans, completing housework before undertaking wound care, restricting foot traffic around wound care, exposing wound for the shortest time possible, dress clean wounds before infected wounds, dispose of old dressings in sealed waste bags.64 [C] Finding 91 The environment can be cleaned through disinfection or decontamination.64 [UE]
Haesler E et al. A systematic review of the literature addressing asepsis in wound management
Volume 24 Number 4 – December 2016221
7
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Finding 92 Chlorine is recommended for surface cleaning due to its broad spectrum action.64 [C] Finding 93 If using a dressing trolley, ensure it is clean before use.57 [C] Finding 94 In the community setting, the nurse should place the sterile field at a height that prevents contamination with skin scales and fibres.64 [C] Finding 95 In the community setting, the nurse should establish the sterile filed on either a clean table or on a plastic surface to prevent wicking. A plastic apron could be utilised.8 [C] Finding 96 The plastic lid of a storage container can be wiped and used as a clean surface on which to set up a sterile surface for a procedure in a home setting.64 [C] Finding 97 Community nurses choose clean hard surfaces at wound height to create a sterile field, however this is often on the floor for a leg ulcer dressing.11 [C]
Finding 98 Application of wound field principle treats the wound as an extension of the dressing field.7 [C] Finding 99 Wound field concept is guided by the principle that wounds themselves are not sterile, and products from a wound cannot contaminate itself; however external objects can contaminate the wound.7 [C] Finding 100 Maintain a sterile field by only placing sterile objects within it, considering everything outside the field to be contaminated and not returning items to the field once they leave the field.57 [UE] Finding 101 Use a critical aseptic field into which only sterile equipment is introduced for open, invasive or technical procedures.61 [US] Finding 102 Use a general aseptic field in which key parts can be individually protected for non-invasive basic wound care.61 [US]
Category 23 Once established, the wound management field must not be contaminated.
Synthesis 9
A wound management field can be established on a clean surface in a space at low risk of environmental contaminants. Once established, introduction of contaminated external objects should be avoided.
Category 22 The surface on which a sterile field will be set up should be clean and free from sources of contamination
Finding 110 A wound cleanser should be effective in the presence of organic material and reduce microorganisms.63 [UE] Finding 111 Wound cleaners should reduce microorganisms and remove organic material effectively. 42 [UE]
Category 26 A wound cleanser should adequately clean the wound.
Category 25 A wound cleanser should have a long shelf life.
Synthesis 10
An ideal wound cleanser should adequately clean the wound, not cause cell damage or sensitivity and have a long shelf life.
Finding 103 A wound cleanser should be non-toxic and not cause sensitivity.63 [UE] Finding 104 Wound cleansers may be toxic to cells and their use should be carefully considered.63 [C] Finding 105 Wound cleaners should be non-toxic and not cause sensitivity to tissue.42 [C] Finding 106 Use the principle of do no harm and prevent infection when selecting an irrigation solution.9 [UE]
Category 24 A wound cleanser should not cause damage or sensitivity.
Finding 107 Wound cleaners should have a long shelf life.42 [C] Finding 108 Wound cleaners should have a long shelf life.63 [C] Finding 109 Do not use expired or damaged irrigation fluids.57 [UE]
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 222
Haesler E et al. A systematic review of the literature addressing asepsis in wound management
8
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Finding 112 Only cleanse wounds that are visibly contaminated with debris, excess exudate, necrotic tissue or slough, because these encourage infection.39 [C] Finding 113 Only remove bacteria from a wound through cleansing in the presence of clinical signs of infection.39
[US] Finding 114 When no contaminants are present, a wound may heal better without cleansing.58 [US]
Category 27 Wound beds only need cleansing in the presence of visible contamination or signs of infection.
Finding 115 The interdisciplinary care team should work together to determine the best wound cleansing options for specific individuals.58 [C] Finding 116 Decisions about cleansing strategy for patients with DFU should be made by the multidisciplinary collaborative team.9 [C] Finding 117 Assess whether a wound needs cleansing.39 [C]
Synthesis 11
An assessment should be conducted by the interdisciplinary team to determine if a wound bed should be cleansed, and if so, the cleansing process to use.
Category 28 The interdisciplinary team should assess if and how a wound should be cleansed.
Finding 118 Normal saline is the only completely safe wound cleanser as it is isotonic and does not draw fluid from the wound.42 [C] Finding 119 As an isotonic solution, saline does not impact osmotic pressure or impede normal healing as it has no impact on blood flow, granulation tissue, collagen formation or DNA synthesis. 46 [C] Finding 120 Sterile saline should be the preferred irrigation fluid in hospital settings. 46 [C] Finding 121 The choice of saline for wound irrigation is based on tradition rather than evidence.62 [C] Finding 122 Use sterile saline solution for complex and vulnerable wounds.9 [C]
Category 29 Normal saline is a safe and traditional wound cleansing solution.
Synthesis 12
Normal saline, potable tap water, sterile water and low concentration antimicrobial solutions are safe and effective wound cleansers. Antiseptics are not a good choice for wound cleansing.
Finding 123 Use tap water or normal saline to cleanse wounds because antiseptics are ineffective and can delay healing.56 [C] Finding 124 Appropriate irrigation fluids include normal saline and sterile water.57 [UE] Finding 125 Water may be the best option for irrigation when using dressing products with which saline is contraindicated. 46 [C] Finding 126 Tap water is an acceptable alternative to saline.42 [C] Finding 127 Water and saline are ineffective cleansers for reducing the wound bioburden or improving wound healing.67 [C]
Category 30 Tap water, sterile water or normal saline are acceptable options for wound cleansing, although they do not reduce bioburden.
Category 31 Antimicrobial solutions are effective cleansers that play a role in reducing bioburden, although they are toxic in higher concentrations.
Finding 128 All antimicrobials are effective in reducing wound contamination.67 [C] Finding 129 Polyhexamethylene biguanide (PHMB), povidone-iodine, and ionised silver are wound cleaners that are effective for promoting wound healing.67 [C]
Finding 130 All antimicrobials are toxic to wounds (PHMB has lowest toxicity).67 [UE] Finding 131 Antimicrobials (e.g. Dakin’ solution and povidone-iodine) are toxic to cells and if used as a wound cleanser the concentration should be carefully considered.63 [C]
beds
bed

Volume 24 Number 4 – December 2016223
9
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Finding 132 Antiseptics should be used with caution for wound cleansing, particularly those deemed toxic or carcinogenic to tissues.42 [UE] Finding 133 Using antiseptics to cleanse wounds is controversial because they can negatively influence wound healing.63 [C] Finding 134 Skin cleansers are cytotoxic to cells and are not appropriate wound cleansers.63 [C] Finding 135 Antiseptics are not in contact with a wound surface sufficiently long to reduce bacteria.39 [C] Finding 136Antiseptics can damage healing wounds.39 [UE] Finding 137 Excessive use of antiseptics may be associated with antibiotic resistant bacteria.39 [C] Finding 138 Using antiseptics for wound cleansing can be detrimental to the wound healing process.58 [C]
Category 32Antiseptics and skin cleansers are toxic to wound healing and not appropriate for wound cleansing.
Finding 139 Low pressure irrigation using normal saline and a syringe is the preferred method for wound cleansing.42 [US] Finding 140 Irrigation is the preferred cleansing method.56 [C] Finding 141 When irrigating with tap water, use tubing attached to the faucet if the wound cannot be placed under the tap.62 [C] Finding 142 When cleansing or irrigating, suitable pressure to remove exudate, loose tissue and contaminants should be applied. However, pressure should not be high enough to disrupt granulation.65 [C]
Category 33 Low pressure irrigation removes debris without disrupting granulation.
Finding 143 When irrigating with tap water ensure it is lukewarm.62 [C] Finding 144 Rewarm refrigerated wound cleansing fluids before use.45 [UE] Finding 145 Cooler irrigation fluids may lead to impaired healing associated with local vasoconstriction.66 [UE] Finding 146 Because wound healing optimally occurs at 33°C, irrigation fluids should be warmed to between 37°C and 42°C before use.46 [UE] Finding 147 Consider refrigerating wound cleansers after opening to reduce bacterial growth.45 [C] Finding 148 Cleansing with cool fluids can increase risk of infection as the body’s defence mechanisms are lower due to vasoconstriction.9 [C] Finding 149 Fluid temperature should be considered when selecting a cleansing method.54 [C]
Synthesis 13
Apply a wound cleanser at a lukewarm temperature with consideration to the potential for cross infection and using low pressure to irrigate the wound bed.
Finding 150 Cross infection risk should be considered when deciding if cleansing a wound in a shower is appropriate.58 [C] Finding 151 The practicalities of cleansing techniques, including the difficulty in managing fluid flow direction should be considered when selecting a cleansing method.54 [C]
Finding 152 Consider cross infection risk when determining if a person with a diabetic foot ulcer can cleanse a wound in a shower (particularly in a multi-dwelling residence).9 [UE]
Category 35 There is a risk of cross infection when cleansing a wound.
Category 34 A wound cleanser should be lukewarm on application.
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 22410
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Category 37 The quality of water used for wound cleansing is important.
Category 39 Tap water may cause pain or damage cells due to its hypotonicity.
Category 38 It is cost effective to use tap water for wound cleansing.
Finding 153 Soap and water is acceptable for cleansing sutured wounds.39 [C] Finding 154 Bathing and showering can be undertaken once wound edges are sealed.39 [C] Finding155 Water should only be used occasionally.42 [US] Finding 156 Tap water has the advantage of providing a greater volume of fluid, at a constant high pressure when provided from city water mains.62 [C] Finding 157 Soaking the leg in a bucket of water is an option for cleansing legs with venous ulcers.58 [C] Finding 158 Tap water is sufficient for cleansing sacral, perianal wounds, open traumatic wounds and leg ulcers.56 [C] Finding 159 Soap and water are sufficient for removing transient flora in wounds.56 [C] Finding 160 When irrigating with tap water, place the wound under running water for 30 seconds.62 [C]
Finding 165 Tap water is cheaper than saline and eliminates the need for additional equipment including syringes.62 [C] Finding 166 Using tap water for wound cleansing is likely to have a large financial benefit.54 [C] Finding 167 Patient satisfaction, time and cost effectiveness should all be considered when selecting a wound cleanser.66 [UE] Finding 168 Water may be more cost-effective than saline.46 [C]
Category 36 Running tap water or water in a bucket is sufficient for cleansing dirty wounds, chronic wounds and wounds with closed or sutured edges.
Finding 161 Quality of drinking water should be considered when determining where to use it for wound cleansing. [UE]
Finding 162 Tap water should be from a clean, monitored supply.56 [C]
Finding 163 It is safe to use clean uncontaminated tap water to cleanse wounds.54 [C]
Finding 164 In major cities tap water is chlorinated therefore the risk from pathogens is minimal.62 [US]
Synthesis 14
Good quality tap water is a cost effective option for cleansing dirty wounds, chronic wounds and wounds with closed or sutured edges, although it may cause pain.
Finding 169 As a hypotonic solution, water can increase osmotic pressure within wounds and may be detrimental to cells during healing due to potential of excessive moisture absorption and exudate production.46 [C] Finding 170 Irrigating wounds with water can cause pain.46 [C] Finding 171 Irrigating wounds with water can cause loss of intracellular fluid and substances that promote wound healing.46 [C] Finding 172 Water may cause wound pain because it is hypotonic and therefore causes cells within the tissue to swell and rupture.42 [US]
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016225 11
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Finding 173 The risk of potential infection from tap water, particularly in immunocompromised patients and in the hospital environment should be considered when determining how to cleanse a wound.41 [UE] Finding 174 Biofilm in pipes, faucets and sinks are a potential source of contamination of running tap water.41 [C] Finding 175 Exposure to tap water during bathing (either from direct contact or inhalation) is a potential source of infection in hospitals.41 [C] Finding 176 Pseudomonas Aeruginosa, Acanthamoeba, Mycobacteria and Leptospira are common water-related pathogens that be transmitted via contact with water.41 [UE] Finding 177 More virulent bacteria may enter water sources in hospital environments.41 [C] Finding 178 When determining the infection risk of tap water, consider how the water was stored and delivered (consider the variation in water purity in different geographic locations and clinical settings).9 [UE] Finding 179 Hospitals do not always have high quality water.41 [C]
Category 40 Tap water may be a source of contamination in homes and hospitals.
Synthesis 15
Precautions can be taken to reduce the risk of potential contamination of water sources.
Category 41 Filters, autoclaving and running the faucet to remove bacteria can reduce the risk of contamination from water supply.
Finding 180 Tap mounted water filters reduce the number of microorganisms in tap water. 41[C] Finding 181 Holy water should be autoclaved due to risk of pathogens.56 [C] Finding 182 A tap should be run properly for a few minutes before the water is used for wound cleansing, to reduce risk of bacterial contamination.42 [US]
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 226
12
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Category 43 Selection of the technique for performing a wound dressing should be guided by the complexity or invasiveness of the procedure being performed.
Synthesis 16
Selection of sterile /surgical ANTT or clean/standard ANTT is determined by the level of risk posed to the patient by his or her health status, the environment, factors associated with the wound and the type of wound management procedure being performed.
Finding 183 The use and storage of dressing supplies and solutions influences the type of dressing technique selected. If materials are not stored in a way to ensure sterility, conditions for sterile and no touch techniques cannot be met.68 [UE] Finding 184 In selecting a dressing technique consider the clinical setting (e.g. surrounding environment, health professional skills).68 [UE] Finding 185 Aseptic non touch technique framework is based on assessing the risk the patient faces of infection from the health professional and environment.60 [C] Finding 186 Decision regarding technique is guided by the environment.57 [C] Finding 187 In deciding between clean and aseptic technique consider the healthcare setting.48 [C] Finding 188 Assess risks of contamination from the local environment.60 [C] Finding 189 Concern about potential infection is a barrier to uptake of clean technique in community settings.37
[C] Finding 190 Not all care environments require the strict asepsis that was developed for sterile operating rooms.7 [C]
Finding 198 In selecting a dressing technique consider patient factors (e.g. immune status, acuity).68 [C] Finding 199 In deciding between clean and aseptic technique consider the patient’s immune status.48 [C] Finding 200 Consider the patient’s context when selecting appropriate dressing technique.7 [C] Finding 201 Historically the selection of technique has been based on perceived patient risk of infection.60 [C] Finding 202 Patient-related factors to consider when determining technique include immune status; age; use of steroids patient lifestyle; concurrent skin conditions; nutritional and status.57 [C]
Finding 191 Decision regarding technique is guided by complexity of the procedure.57 [C] Finding 192 In selecting a dressing technique consider the invasive level of the procedure. 68 [UE] Finding 193 Selection of dressing technique should be guided by the intervention required to the wound.68 [C] Finding 194 In deciding between clean and aseptic technique consider the level of invasion of procedure (e.g. extensive debridement or packing).48 [C] Finding 195 Determine the level of risk of contamination with consideration to level of contact with the patient, when selecting a hand hygiene methods.51 [C] Finding 196 In deciding what technique to use, assess the complexity of the procedure and necessity to touch key parts.60 [US] Finding 197 Aseptic non touch technique (ANTT) framework is based on assessing the risk the patient faces of infection from the procedure.60 [C]
Category 42 Selection of technique for performing a wound dressing should be guided by the risk to the patient of infection from the surrounding environment.
Category 44 Selection of the technique for performing a wound dressing should be guided by patient factors that influence infection risk.
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016227
13
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Finding 203 In deciding between clean and aseptic technique consider the type of wound (e.g. acute vs chronic) and its location and depth.48 [C] Finding 204 In selecting a dressing technique consider wound factors (e.g. acuter versus chronic, depth, location).68 [C] Finding 205 Consider the wound history when selecting appropriate dressing technique.7 [C] Finding 206 Chronic wounds cannot become contaminated from “clean” products because they are already colonised with microbes.50 [US] Finding 207 Clean technique may be more appropriate than rigorous asepsis in caring for chronic wounds.57 [C] Finding 208 Clean wound care technique using non-sterile gloves and tap water could be used for some wound types.56 [C] Finding 209 Patient factors to consider when determining technique type of wound; depth, location and size of wound.57 [C]
Category 45 Selection of the technique for performing a wound dressing should be guided by the type and condition of the wound.
Category 47 Sterile/ surgical ANTT is appropriate for individuals at infection risk due to compromised immunity, and/or when the procedure is invasive, complex or breaches the skin (e.g. sharp debridement) or is of longer duration. It requires sterile gloves, sterile equipment and sterile cleansing solutions.
Finding 210 Use clean technique (handwashing, clean gloves, solutions, equipment maintained as clean) for dressing changes with mechanical, chemical or enzymatic debridement.68 [C] Finding 211 Use clean technique (handwashing, clean gloves, solutions and equipment maintained as clean) for routine dressing changes without debridement.68 [C] Finding 212 Use standard aseptic non-touch technique, critical micro-field and non-sterile gloves with a non-touch technique for a simple wound dressing that is less than 20 minutes in duration.61 [US] Finding 213 Clean technique allows irrigation or bathing with saline or tap water and use of a clean surface.37 [C] Finding 214 Use clean technique (handwashing, clean gloves, solutions and equipment maintained as clean) for irrigating wounds.68 [C]
Synthesis 17
Simple wound management procedures on low risk patients can be performed with non-sterile but clean equipment, solutions and gloves. More complex procedures or procedures in higher risk patients require surgical aseptic non-touch technique, using sterile gloves, solutions and equipment.
Category 46 Clean technique/standard ANTT is appropriate for irrigating and wound dressings without debridement. It requires clean gloves and equipment and cleansing solutions maintained as clean.
Finding 215 Use sterile technique (handwashing, sterile gloves, sterile solutions and equipment) for routine dressing changes with sharp conservative debridement.68 [C] Finding 216 Aseptic wound care using sterile equipment and wound cleansers prevents transmission of bacteria and is the standard recommended practice.56 [US] Finding 217 Surgical aseptic technique or aseptic non-touch technique is required when undertaking an invasive procedure when the patient’s defences are compromised.57 [C] Finding 218 Surgical aseptic technique or aseptic non-touch technique is required when undertaking an invasive procedure that breaches the skin.57 [C] Finding 219 Use surgical aseptic non-touch technique with an aseptic field, sterile gloves and barrier precautions for attending a complex or large dressing with key parts that require asepsis or procedures longer than 20 minutes.61 [US] Finding 220 Aseptic technique requires a sterile dressing pack and sterile cleansing solution.37 [C] Finding 221 Sterile technique is the most appropriate technique for patients at high infection risk.68 [C]
Haesler E et al. A systematic review of the literature addressing asepsis in wound management
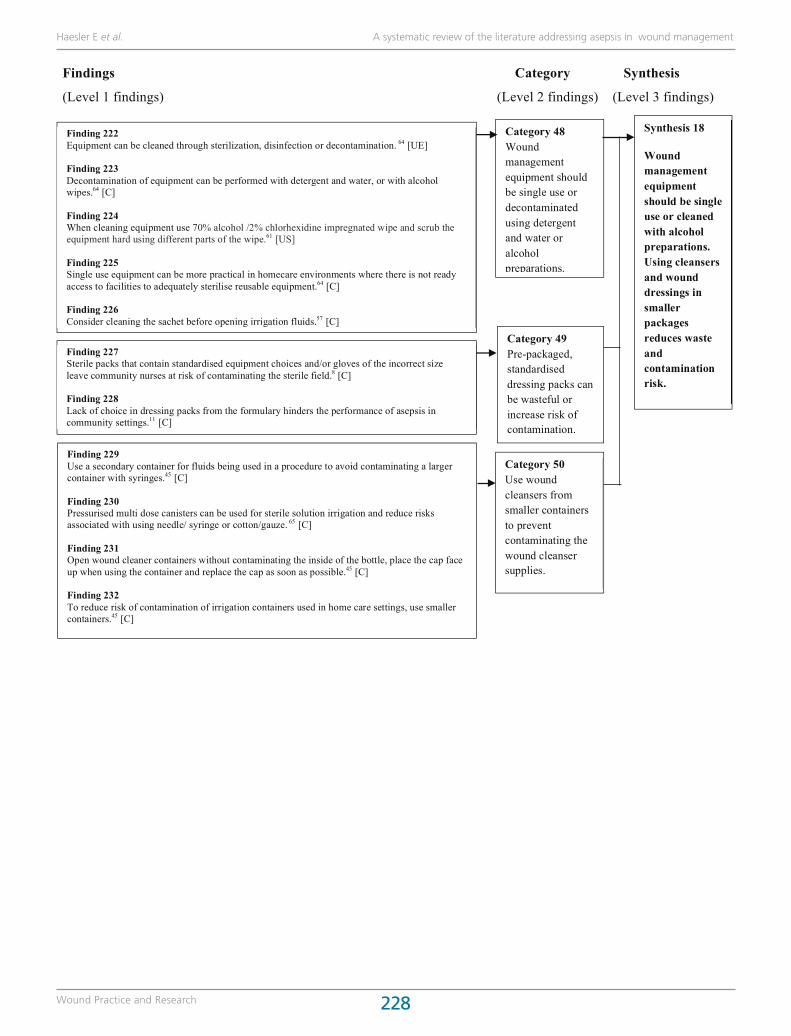
Wound Practice and Research 228 14
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Finding 229 Use a secondary container for fluids being used in a procedure to avoid contaminating a larger container with syringes.45 [C] Finding 230 Pressurised multi dose canisters can be used for sterile solution irrigation and reduce risks associated with using needle/ syringe or cotton/gauze. 65 [C] Finding 231 Open wound cleaner containers without contaminating the inside of the bottle, place the cap face up when using the container and replace the cap as soon as possible.45 [C] Finding 232 To reduce risk of contamination of irrigation containers used in home care settings, use smaller containers.45 [C]
Synthesis 18
Wound management equipment should be single use or cleaned with alcohol preparations. Using cleansers and wound dressings in smaller packages reduces waste and contamination risk.
Category 48 Wound management equipment should be single use or decontaminated using detergent and water or alcohol preparations.
Category 50 Use wound cleansers from smaller containers to prevent contaminating the wound cleanser supplies.
Category 49 Pre-packaged, standardised dressing packs can be wasteful or increase risk of contamination.
Finding 222 Equipment can be cleaned through sterilization, disinfection or decontamination. 64 [UE] Finding 223 Decontamination of equipment can be performed with detergent and water, or with alcohol wipes.64 [C] Finding 224 When cleaning equipment use 70% alcohol /2% chlorhexidine impregnated wipe and scrub the equipment hard using different parts of the wipe.61 [US] Finding 225 Single use equipment can be more practical in homecare environments where there is not ready access to facilities to adequately sterilise reusable equipment.64 [C] Finding 226 Consider cleaning the sachet before opening irrigation fluids.57 [C]
Finding 227 Sterile packs that contain standardised equipment choices and/or gloves of the incorrect size leave community nurses at risk of contaminating the sterile field.8 [C] Finding 228 Lack of choice in dressing packs from the formulary hinders the performance of asepsis in community settings.11 [C]
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016229 15
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Finding 233 In aseptic non touch technique used equipment must not re-enter the sterile field.51 [C]
Finding 234 When implementing sterile technique, sterile objects must not touch non-sterile objects.68 [UE] Finding 235 An aseptic technique requires all objects and fluid that come on touch with the wound to be sterile.7 [UE] Finding 236 To perform aseptic technique the health professional must: understand when an object is or is not sterile; maintain the dressing field separate from the wound; remove contaminated or non-sterile items from the field; ensure non-sterile items do not cross into to the sterile field and correct infractions if the sterile field becomes contaminated.7 [UE]
Finding 237 The concept of clean and dirty (hands and/or forceps) is incorporated into aseptic techniques.7 [UE] Finding 238 To maintain aseptic technique the process of cleansing with tap water and washing the surrounding skin (e.g. VLU leg) should be separate from applying a dressing.8 [C] Finding 239 Equipment that only touches the wound or the sterile field cannot be a source of contamination to the wound.43 [C]
Category 52 Because using forceps can be difficult, some clinicians use gloved hands in the wound dressing procedure.
Finding 240 Gloves have replaced the use of sterile forceps.56 [C] Finding 241 Use a dressing aid to remove the old wound dressing and use gloves and a clinical sheet to dry the leg, before commencing aseptic technique.8 [C] Finding 242 Forceps are difficult to manoeuvre and health professionals often become confused or are unable to prevent contamination of the clean forceps by the dirty forceps when applying aseptic non-touch technique.7 [UE]
Synthesis 19
When performing sterile/surgical ANTT the wound management field must remain free of non-sterile items, including equipment, cleansing fluids and gloved hands that have touched a non-sterile object.
Category 51 In sterile/surgical aseptic non-touch techniques the wound management field must remain free of non-sterile items, including equipment and cleansing fluids.
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 230 16
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Finding 251 Dressing packs should be stored in a clean, dry place and not used if they are damaged or soiled.56 [C] Finding 252 Support the strategies patients develop for storing equipment in a way that reduces contamination.64 [US]
Category 57 Gloves should be stored in a manner that reduces contamination.
Finding 253 There is no set timeframe after which an opened irrigation solution needs to be disposed.45 [C] Finding 254 If using larger irrigation fluid containers reduce the risk of contamination by dating on opening, discarding according to organisation policy and destroying any fluid containers that visually appear contaminated.45 [C]
Synthesis 21
Wound management products should be stored in dry, clean environments to reduce risk of contamination and cleansers should be dated on opening and discarded if visually contaminated or according to organisation policy.
Category 55 Wound products and equipment should be stored in a clean dry place that reduces risk of contamination.
Category 56 Wound cleaners should be dated on opening and destroyed when they are visually contaminated.
Finding 255 Gloves should be used and stored in a way that reduces risk of damage.50 [C] Finding 256 Gloves from damp boxes are at risk of contamination from mould.62 [US]
Finding 243 In a home with an MRSA infected wound, disinfect surfaces with bleach and water or an appropriate detergent.49 [C]
Finding 244 When caring for a wound infected with MRSA, clean reusable equipment with an intermediate disinfectant before returning it the bag.49 [C]
Finding 245 Dispose of MRSA-infected waste at the patient’s home, using double-bagging and labelling as hazardous waste if there is significant wound drainage.49 [C]
Finding 246 When caring for a wound infected with MRSA, use disposable equipment where possible to prevent MRSA spread.49 [C]
Finding 247 To prevent spread of MRSA in the community place a plastic sheet underneath the equipment bag when caring for a patient with MRSA.49 [C]
Category 53 Strategies to prevent contamination of equipment should be taken if a patient has MRSA.
Synthesis 20
Extra infection control precautions should be taken for patients with known infection.
Finding 248 In a home with an MRSA infected wound, the health professional should avoid using the patient’s soap or towels.49 [C]
Finding 249 Use personal protective equipment when caring for a wound infected with MRSA 49 [C]
Finding 250 When caring for an MRSA infected wound, hand washing and gloves are important in preventing the spread of MRSA in the community. 49 [UE]
Category 54 Pay extra attention to personal hygiene to prevent cross infection when a patient has MRSA.
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016231 17
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Finding 257 Ongoing education is required to improve asepsis skills.48 [C] Finding 258 Regular infection control training should include hand hygiene, asepsis, decontamination and cleaning, waste and laundry disposal, sharps management and use of personal protective equipment.64 [C] Finding 259 Education is an effective strategy in promoting best hand hygiene practice.64 [C] Finding 260 All health professionals involved in wound care should be offered training, regardless of discipline.38 [C] Finding 261 Nurses often have superficial and incomplete knowledge of principles underpinning wound care and this leads to ritualistic practice.39 [C] Finding 262 Education is an important factor in reducing hospital acquired infection.51 [UE] Finding 263 Good base knowledge and ongoing education are important to ensure health professionals have perform good handwashing technique.50 [UE] Finding 264 Provide education to the patient and caregivers on preventing spread of MRSA.49 [UE] Finding 265 Regular education contributes to improving infection control behaviour and compliance in hand hygiene.59 [C] Finding 266 Clinical staff require education and training in aseptic technique.8 [UE] Finding 267 Community nurses display confusion regarding clean technique and the use of tap water, often leading to sterile field contamination due to failure to separate wound washing from aseptic procedure.11 [C] Finding 268 Community nurses receive no guidance in how to adapt the principles of aseptic technique to the home setting and patient preferences.11 [C] Finding 269 Aseptic technique principles are ingrained in initial nurse training and community nurses maintain knowledge of important principles.11 [C] Finding 270 Appropriate education, training and skill assessment is required for all health professionals undertaking aseptic technique.57 [UE]
Synthesis 22
Staff education that incorporates skills practice, simulation learning, theoretical knowledge update and procedures for different clinical settings is essential in promoting best practice in aseptic technique and infection control.
Finding 271 District nurses are aware that performing aseptic technique in community settings is a challenge.11
[C] Finding 272 Community nurses perceive they have a lack of control over cleanliness and therefore risk of infection.10 [C] Finding 273 Community nurses use the term aseptic technique vaguely as they perceive asepsis as impossible in the home environment. 10 [C] Finding 274 Some community nurses view infection as unavoidable.10 [C]
Category 58 Staff education, including education on application in different clinical settings, is an essential component in ensuring best practice in aseptic technique and infection control.
Category 59 Nurses in the community experience frustration and fatalism when negotiating aseptic procedures.
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 232 18
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Finding 275 Students should first learn clean and aseptic wound care in simulation.57 [C] Finding 276 Observing clinical practice to provide feedback is an effective strategy in promoting best hand hygiene practice.64 [C] Finding 277 Students require a combination of didactic theory and opportunities for practical simulation to learn aseptic non touch technique.53 [C] Finding 278 Visual education strategies such as coloured dye and talcum powder activities helps health professionals visualise the spread of infection.59 [C]
Category 60 Skills practice and simulation learning can be used for infection control training and education.
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016233
19
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Synthesis 23
Best practice in aseptic technique and infection control procedures is promoted through development of facility policies, regular risk surveillance, annual auditing of staff practice, engaging with staff and patients and provision of acceptable hand hygiene products.
Finding 283 Engaging wound champions are a strategic strategy to promote infection control and appropriate dressing practices.38 [C] Finding 284 Quality practice can be achieved using linkage programs through which infection champions disseminate key messages.64 [C]
Finding 285 Partnership and understanding between the individual, informal carers and health professionals is essential to ensure effective infection prevention and control.64 [C]
Finding 286 Patients could be empowered to promote hand hygiene by asking health professionals about their practice. 59 [C] Finding 287 Adequate staffing is an important factor in reducing hospital acquired infection.51 [C]
Finding 279 Health professionals have a responsibility to identify infection risks and intervene to reduce that risk.50 [UE] Finding 280 Assessments of infection risk should be conducted in health facilities.59 [C] Finding 281 Continuous quality improvement through regular auditing, risk assessment and education is essential in maintaining appropriate wound care practices.7 [C] Finding 282 Infection surveillance and quality improvement using root cause analysis is essential for continuous quality improvement.64 [C]
Category 62 Engaging with staff members and patients promotes best practice in aseptic technique and infection control procedures.
Category 63 Annual auditing clinical practice of staff contributes to continuous improvement in aseptic technique and infection control procedures.
Finding 293 Standardising the technique used in a facility is one way to prevent and control hospital acquired infection.8 [C] Finding 294 There is insufficient evidence to make recommendations on approach to wound care therefore facilities should develop their own policies regarding wound care.48 [C] Finding 295 Health professionals should continue current practice consistent with their facility policies.48 [C] Finding 296 Standardising aseptic care reduces infection.61 [C]
Finding 288 Annual assessment of dressing technique should be a required organisational policy.38 [C]
Finding 289 Ongoing practice audits contribute to improving infection control behaviour.59 [C] Finding 290 Auditing of practice increases compliance with the standardised aseptic technique.8 [C] Finding 291 Facilities should periodically monitor hand hygiene. 40,55 [C] Finding 292 Annual auditing of aseptic non touch technique practises should be conducted a part of continuous quality improvement.38 [C]
Category 61 Regular risk surveillance within a health service promotes continuous improvement in aseptic technique and infection control procedures.
Category 64 Standardised policies and procedures increase compliance with best practice in aseptic technique and infection control procedures.
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 234
20
Findings Category Synthesis
(Level 1 findings) (Level 2 findings) (Level 3 findings)
Category 65 Providing low irritant products increases compliance with hand washing.
Finding 297 Plain detergent, warm water and paper towels reduce skin irritation and increase acceptability of handwashing.51 [C] Finding 298 Providing efficacious hand hygiene products with low irritancy and favourable aesthetics increases compliance with hand washing. 40,55 [C]
Haesler E et al. A systematic review of the literature addressing asepsis in wound management
Volume 24 Number 4 – December 2016235
1
Tabl
e 1:
Sum
mar
y of
rese
arch
pap
ers
Ref
T
ype
of
Stud
y Sa
mpl
e In
terv
entio
n(s)
O
utco
me
Mea
sure
s &
Len
gth
of F
ollo
w-u
p R
esul
ts
Cle
ansi
ng so
lutio
ns
Bansal,
2002
RC
T co
mpa
ring
irriga
tion with
no
rmal saline to
irriga
tion with
tap water fo
r man
agem
ent o
f laceratio
ns in
ch
ildren
Paed
iatric patients recruited in US em
erge
ncy
room
(n=4
5)
Inclusion crite
ria:
• ch
ildren ag
ed 1 to
18 ye
ars
• presen
ted with
in 8 hou
rs of injury
• simple laceratio
n (no muscle, bon
e or jo
int
invo
lvem
ent)
Exclusion crite
ria:
• la
ceratio
n from
dog
bite
•
hand
laceratio
n •
curren
tly ta
king
antibiotic
s Ch
aracteristics:
• ag
e rang
e 2 to 15
• sharp an
d blun
t injury laceratio
ns
• 64
% of laceration ≤ 3 cm
and
7% >6cm
• 64
% lo
cated on
leg, 22%
located on
arm
, 11
% lo
cated on
foot, 4
% lo
cated on
han
d
• All pa
rticipan
ts had
a w
ound
swab
co
nduc
ted pre an
d po
st irriga
tion
• All laceratio
ns w
ere sutured, had
an
tibiotic
cream
and
dressing ap
plied
• Pa
tients were rand
omised
to receive
: o
Group
1: irrigation of th
e laceratio
n with
normal saline at a pressure of
25 to
40 psi (n=2
4) or
o Group
2: irrigation of th
e laceratio
n with
tap water at a
pressure of 25 to
40 psi (n
=21)
Participan
ts re-‐attend
ed ER in 48 ho
urs
to assess for co
mplications
• Wou
nd culture perform
ed
post irriga
tion
• Infection rate at 4
8 ho
urs
using the follo
wing crite
ria to
defin
e a laceratio
n as in
fected
: o
cellulitis or erythe
ma of th
e wou
nd m
argin of m
ore than
4 mm w
ith te
nderne
ss,
o purulen
t disch
arge
from
the
wou
nd,
o ascen
ding
lymph
angitis
, o
deh
iscenc
e of th
e wou
nd
with
wou
nd sep
aration of
>2mm
Positive
post irriga
tion
wou
nd culture
(thresho
ld: a
ny growth)
No sign
ificant differen
ce betwee
n grou
ps in
po
st-‐irriga
tion wou
nd cultures: normal
salin
e 29
% versus tap water 51%
, p=0
.20
Infected
laceration
at 48
hou
rs
No sign
ificant differen
ce in
infected
laceratio
ns at 4
8 ho
urs: normal saline 8%
ve
rsus ta
p water 10%
, p=n
s
JBI lev
el of
eviden
ce:
1.c
JBI q
uality:
Mod
erate
Fernan
dez,
Giffiths
2001
and
Fe
rnan
dez,
Griffiths
2004
System
atic
review
of
controlle
d clinical
trials exp
loring
effic
acy of
clea
nsing
solutio
ns and
tech
niqu
es
In 200
1 review
, 9
RCTs in
clud
ed
In 200
4, 14 RC
Ts
includ
ed
The includ
ed trials w
ere co
nduc
ted in adu
lts
and ch
ildren in Australia, S
wed
en, T
anzania
and UK
Inclusion crite
ria:
• Adu
lts or ch
ildren with
wou
nds (e
xcluding
bu
rns)
Cha
racteristic
s:
• 4 stud
ies includ
ed peo
ple with
laceratio
ns
• 1 trial e
ach for trau
matic w
ound
s, ope
n fractures or ulcers
• 7 trials post-‐op
surgical w
ound
s
• Co
mpa
risons of d
ifferen
t clean
sing
solutio
ns
• Co
mpa
rison of sho
wering ve
rsus non
show
ering
• Infection rates
• Wou
nd deh
iscenc
e •
Wou
nd hea
ling
• Co
st
Tap water versus no
rmal saline
• Infection in
acu
te w
ound
s (1 RCT
):
favo
urs tap water odd
s ratio
(OR) 0.52
(95%
con
fiden
ce in
terval [C
I] 0.28
to
0.96
), p=
0.04
• Infection in chron
ic w
ound
s (1 RCT
): no
sign
ificant differen
ce; O
R 0.14
(95%
CI
0.01
to 2.94), p
=0.21
• Infection in children with
laceratio
ns (2
RC
TS): no sign
ificant differen
ce, O
R 1.07
(95%
CI 0
.42 to 2.75), p
=0.89
• Infection in all type
s wou
nds (4 RCT
s):
favo
urs tap water, O
R 0.60
(95
% CI 0
.37
to 0.99), p
=0.05
• Co
st ana
lysis: normal saline $1
.43 vs ta
p water $1.16
/dressing (currenc
y no
t repo
rted
) Sh
owering/ba
thing ve
rsus no show
ering
• Infection in post-‐op
erative wou
nds (5
RCTs): no sign
ificant differen
ce, O
R 0.80
(95%
CI 0
.29 to 2.23), p
=0.67
• Wou
nd hea
ling in post-‐op
erative wou
nds
(3 RCT
s): n
o sign
ificant differen
ce, O
R 1.21
(95
% CI 0
.29 to 5.10), p
=0.80
JBI lev
el of
eviden
ce:
1.a
JBI q
uality:
Mod
erate
Tab
le 1
: S
umm
ary
of r
esea
rch
pap
ers
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 236
2
Ref
T
ype
of
Stud
y Sa
mpl
e In
terv
entio
n(s)
O
utco
me
Mea
sure
s &
Len
gth
of F
ollo
w-u
p R
esul
ts
• Wou
nd deh
iscenc
e in post-‐op
erative
wou
nds (1 RCT
): no sign
ificant differen
ce,
OR 1.14
(95
% CI 0
.10 to 12.69
), p=
0.91
1%
pov
idon
e-‐iodine
versus no
rmal saline
• Infection rate in
laceratio
ns/ po
stop
wou
nds in small trials (2 RCT
S): favou
rs
povido
ne-‐io
dine
, OR 0.15
(95%
CI 0
.05 to
0.43
) p<0
.05
• Infection rate in
laceratio
ns and
postop
wou
nds in la
rge trials (1
RCT
): no
sign
ificant differen
ce, O
R 0.62
(95%
CI
0.25
to 1.53) p=0
.29
• Wou
nd hea
ling in post-‐op
erative wou
nds
(1 RCT
): fa
vours no
rmal saline, OR 4.46
(95%
CI 1
.45 to 13.68
) p<0
.05
1% pov
idon
e-‐iodine
versus no
clean
sing
Infection in con
taminated
trau
matic w
ound
s (1 RCT
): no sign
ificant differen
ce, O
R 1.00
(95%
CI 0
.05 to 19.3), p
=1.00
Fernan
dez
and Giffiths
2012
System
atic
review
of R
CTs
and qu
asi-‐R
CTs
exploring effic
acy
of w
ater fo
r clea
nsing
11 RCT
s includ
ed
Trials w
ere prim
arily con
ducted
in emerge
ncy
room
s (10/11
) Pa
rticipan
t cha
racteristic
s:
• Age
ran
ge 2 to
95 ye
ars
• Wou
nd ty
pes: 5 trials – la
ceratio
ns, 1
trial
– op
en fractures; 1 trial -‐ chron
ic w
ound
s;
4 trials – surgical w
ound
s
• 3 trials com
pared tap water to
no
clea
nsing
• 8 trials com
pared tap water to
other
clea
nsing solutio
n
• Wou
nd in
fection
• Wou
nd deh
iscenc
e •
Wou
nd hea
ling
• Co
st
Tap water versus no
clean
sing
•
Wou
nd in
fection (3 RCT
s): n
o sign
ificant
differen
ce, relative risk (R
R) 1.06, 95%
CI
0.07
to 16.50
•
Wou
nd deh
iscenc
e (2 RCT
s ): no
sign
ificant differen
ce, R
R 1.26
, 95%
CI
0.18
to 8.66
Tap water versus salin
e •
Wou
nd in
fection in acu
te w
ound
s that
were sutured (3 RCT
s): n
o sign
ificant
differen
ce, R
R 0.66
, 95%
CI 0
.42 to 1.04,
p=0.16
•
Wou
nd in
fection in chron
ic w
ound
s that
were no
t sutured
(1 RCT
): no sign
ificant
differen
ce, R
R 0.16
, CI 0
.01 to 2.96,
p=0.22
•
Wou
nd hea
ling in chron
ic w
ound
s that
were no
t sutured
1 RCT
): no sign
ificant
differen
ce, R
R 0.57
, CI 0
.30 to 1.07, p=n
s •
Cost ana
lysis (2 RCT
s): b
oth foun
d redu
ction in costs assoc
iated with
tap
water
Distille
d water vs co
oled
boiled water
Wou
nd in
fection in ope
n fractures (1 RCT
):
no signific
ant d
ifferen
ce, R
R 1.69
, 95%
CI
0.68
to 4.2, p
=ns
Distille
d water versus isoton
ic saline
JBI lev
el of
eviden
ce:
1.a
JBI q
uality:
Mod
erate
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016237
3
Ref
T
ype
of
Stud
y Sa
mpl
e In
terv
entio
n(s)
O
utco
me
Mea
sure
s &
Len
gth
of F
ollo
w-u
p R
esul
ts
Wou
nd in
fection in ope
n fractures (1 RCT
):
no signific
ant d
ifferen
ce, R
R 0.49
, 95%
CI
0.19
to 1.26, p=n
s Co
oled
boiled water versus isoton
ic saline
Wou
nd in
fection in ope
n fractures (1 RCT
):
no signific
ant d
ifferen
ce, R
R 0.83
, 95%
CI
0.37
to 1.87, p=n
s Distille
d or coo
led, boiled water versus
norm
al saline
Wou
nd in
fection in ope
n fractures (1 RCT
):
no signific
ant d
ifferen
ce, R
R 0.65
, 95%
CI
0.31
to 1.37, p=n
s Lakshm
i et
al 201
1 RC
T co
mpa
ring
tap water and
sterile
saline for
clea
nsing ch
ronic
wou
nds
Participan
ts recruite
d in outpa
tients an
d surgical w
ards in
India (n=8
2 recruited, n=6
1 co
mpleted
) Inclusion crite
ria:
• Ch
ronic wou
nd of ≥
3 w
eeks
• Up to date tetanu
s im
mun
isation
Exclusion crite
ria:
• Se
riou
s med
ical disorde
r • Malnu
trition
(BMI <
15 or >3
6)
• Im
mun
o-‐co
mprom
ised
• pressure ulcer
• diab
etic fo
ot ulcers with
• osteom
yelitis
Patie
nt cha
racteristic
s:
• mea
n ag
e 46
yea
rs
• co
mpa
rable bioc
hemical param
eters
except ta
p water group
had
signific
antly
high
er to
tal p
rotein (p
=0.02)
• most w
ound
s were VL
Us
• mea
n ulcer du
ratio
n ap
prox
. 49 da
ys (n
ot
differen
t betwee
n grou
ps)
• Sa
line grou
p ha
d sign
ificantly la
rger m
ean
wou
nd le
ngth at b
aseline (4cm
vs 2.94
cm,
p<0.05
)
• Pa
rticipan
ts w
ere rand
omised
to
receive:
o Saline grou
p: w
ound
irriga
tion with
sterile
saline de
livered
in a 50m
l syring
e an
d ne
edle at p
ressure of
8ppi (n
=39 co
mmen
ced, n=3
0 co
mpleted
and
rep
orted) or
o Tap
water: drinka
ble qu
ality
tap
water delivered
to w
ound
via PVC
pipe
and
irriga
ted 10
mins after
runn
ing the tap for 5 mins to clear
potential con
tamination (n
=43
commen
ced, n=3
1 co
mpleted
and
repo
rted
) •
All wou
nds trea
ted with
pov
idon
e-‐iodine
impreg
nated ga
uze an
d seco
ndary sterile
gau
ze pad
.
• Infection rate m
easured with
cu
lture ta
ken at 0 w
eeks and
co
mpletion of fo
llow up (5-‐6
wee
ks)
• Ra
te of h
ealin
g mea
sured as
percen
t decrease in w
ound
area
at 2
wee
kly intervals an
d mea
sured with
ruler and
tracings
Wou
nd hea
ling rate
• No sign
ificant differen
ce in
wou
nd
healing rate betwee
n grou
ps at w
eek 2,
wee
k 4 or w
eek 5-‐6.
• En
d trial result: normal saline 45
.34%
(m
ean size: 8
.42±
6.57
) versus tap water
40.58 % (m
ean size of 5
.36±
7.89
), p=
ns
Post irriga
tion
culture
• No sign
ificant differen
ce betwee
n grou
ps
Salin
e grou
p 64
.51%
versus tap water
grou
p 58
.06%
, p=0
.40
• Pa
rticipan
ts w
ith a pre-‐irriga
tion ne
gativ
e cu
lture and
a post-‐irriga
tion po
sitiv
e cu
lture did not differ (saline 13
.3% versus
tap water 9.6%)
JBI lev
el of
eviden
ce:
1.c
JBI q
uality:
Low
Valen
te,
2003
RC
T co
mpa
ring
tap water and
sterile
saline for
clea
nsing simple
laceratio
ns in
ch
ildren
presen
ting to an
emerge
ncy
depa
rtmen
t (ED
)
Conv
enienc
e sample of children with
laceratio
ns presenting at an ED
(586
eligible,
530 rand
omised
, 490
com
pleted
follo
w up,
equivalent lo
ss to
follo
w up be
twee
n grou
ps)
Inclusion crite
ria:
• Age
d 1 to 7 yea
rs
• Simple wou
nds of < 8 hou
rs duration
• Wou
nd lo
cated on
face, scalp, trunk
or
extrem
ity
• All pa
rticipan
ts receive
d an
aesthe
sia
as app
ropriate
• After irriga
tion wou
nd w
ere repa
ired
with
staples, sutures or skin glue
• Pa
rticipan
ts w
ere rand
omised
to
receive:
o M
inim
um 100
ml saline solutio
n irriga
tion using a 30
-‐60m
L syring
e (271
ran
domised
, 251
com
pleted
follo
w up)
• Dev
elop
men
t of w
ound
infection assessed
at 4
8 to 72
hours in person by
blin
ded
clinicians using
clin
ical signs
and symptom
s.
• Fo
r pa
tients un
able to
return,
a ph
one interview w
ith paren
t was con
ducted
to determine
infection (ED rev
iew: 1
65
salin
e irriga
tion grou
p ve
rsus
Dev
elop
men
t of in
fection
• No sign
ificant differen
ces be
twee
n grou
ps, saline grou
p 2.8%
(95%
CI 1
.1 to
5.7%
) versus tap water group
2.9% (9
5%
CI 1.2 to
5.9%)
• Ba
sed on
wou
nd lo
catio
n, fo
ot w
ound
s were 4.4 tim
es m
ore likely to be infected
if irriga
ted with
tap water (relative risk
4.4, 95%
CI 0
.6 to
33.1, p=n
ot rep
orted)
Volum
e of fluid used
JBI lev
el of
eviden
ce:
1.c
JBI q
uality:
Mod
erate
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 238
4
Ref
T
ype
of
Stud
y Sa
mpl
e In
terv
entio
n(s)
O
utco
me
Mea
sure
s &
Len
gth
of F
ollo
w-u
p R
esul
ts
• Re
quiring sutures, staples or skin glue
Exclusion crite
ria:
• Im
mun
ocom
prom
ised
• Co
mplicated
laceratio
ns (e
.g. joints;
tend
on ,cartilag
e, fa
scia or muscle
invo
lvem
ent; visco
us cavity
, gen
itourinary,
eyelids, m
outh, fractures, foreign
bod
ies)
• Cu
rren
t or prop
hylactic use of a
ntibiotic
s Pa
rticipan
t cha
racteristic
s:
• No sign
ificant differen
ce in
age
, gen
der,
ethn
icity
, wou
nd duration, w
ound
mecha
nism
, typ
e of ana
esthesia or type
of
wou
nd closure.
• Ta
p water group
had
more ha
nd
laceratio
ns (9
.2% versus 21
.3%)
o Minim
um of 1
0 seco
nds (a4p
prox
. 1.5 mL) ta
p water irriga
tion, w
ith ta
p run for 30
secon
ds before
commen
cing
irriga
tion an
d wou
nd
placed
directly
und
er fa
ucet or whe
n no
t possible, tu
bing
from
fauc
et w
as
used
to irriga
te w
ound
ove
r a ba
sin
(259
ran
domised
, 239
com
pleted
follo
w up (151
in ED and
88 by
ph
one)
152 in ta
p water group
; pho
ne
review
86 in saline irriga
tion
grou
p ve
rsus 88 in ta
p water
grou
p)
More flu
id w
as used in th
e tap water group
7,14
0mL (in
terqua
rtile
ran
ge [IQR] 3,570
to
14,280
) com
pared with
the salin
e grou
p 30
0mL 25
% to
75%
(IQR 18
0 to 400
)
Bee, 200
9 System
atic
review
includ
ing
4 RC
Ts
compa
ring
tap
water to
saline
for wou
nd
clea
nsing
4 RC
Ts in
clud
ed
(all includ
ed in
othe
r SR
s an
d this rev
iew)
Trials w
ere prim
arily con
ducted
in emerge
ncy
room
s in Australia, U
S an
d Sw
eden
Stud
y inclusion:
• Limite
d to RCT
s an
d qu
asi-‐R
CTs
• 4 RC
Ts com
paring
use of tap
water w
ith
use of sterile saline were iden
tified for
inclusion
• No exclusion crite
ria ba
sed on
partic
ipan
t ch
aracteristics
Participan
t cha
racteristic
s:
• To
tal 1
228 pa
rticipan
ts across 4 stud
ies
(636
trea
ted with
saline, 592
trea
ted with
tap water)
• Wou
nds varied
betwee
n stud
ies bu
t co
vered acute, chron
ic and
soft tissue
wou
nds, sim
ple wou
nds an
d trau
matic
laceratio
ns
• Ta
p water clean
sing
versus
sterile
salin
e clea
nsing
• Po
sitiv
e wou
nd culture
• Wou
nd in
fection iden
tified via
objective or sub
jective
outcom
e mea
sures
Positive
wou
nd culture (2
RCT
s, n = 662
) • No sign
ificant heterog
eneity
• Non
-‐signific
ant favou
ring
of S
aline (3.1%
versus 4.4%, relative risk [R
R] 1.53, 95%
CI 0.79 to 2.99, p=0
.21)
Infected
wou
nd (4 RC
Ts, n
=122
8)
• No sign
ificant heterog
eneity
• Sign
ificant fa
vouring of ta
p water (4
.3%
versus 7.1%, R
R 0.62
, 95%
CI 0
.39 to 1.01,
p=0.05
)
JBI lev
el of
eviden
ce:
1.a
JBI q
uality:
Low
Day
ton,
2013
System
atic
review
includ
ing
9 stud
ies that
compa
red
bathing to not
bathing po
st
surgical fo
ot
wou
nds
(9 case series or
prospe
ctive
observationa
l stud
ies)
Locatio
n no
t rep
orted.
Stud
y inclusion:
• Limite
d to case series and
prospectiv
e ob
servationa
l studies
• Stud
ies co
mpa
red no
rmal hygiene
to
abstaining
from
bathing
follo
wing surgery
on fo
ot or an
kle
• Se
arch
includ
ed resea
rch focu
sed on
differen
t soa
p prod
ucts but results not
presen
ted
Participan
t cha
racteristic
s:
Not rep
orted
• Normal hygiene
versus ab
staining
from
washing
follo
wing surgery
• Th
e no
rmal hygiene
group
s rang
ed
from
immed
iate permission
to w
ash to
waitin
g up
to 5 days, alth
ough
most
stud
ies ha
d a tim
e pe
riod
of w
ashing
with
in 1-‐2 days (n=1
639 pa
rticipan
ts)
• Th
e co
ntrol group
s ge
nerally abstained
from
washing
until after
stap
les/sutures were remov
ed (n
=511
pa
rticipan
ts)
• Stud
ies ap
peared
to use ta
p water but
no spe
cific
details w
ere prov
ided
• Su
rgical site
infection – the
metho
d of assessing
was not
repo
rted
Surgical site infection
There was no sign
ificant differen
ce in
infection rates be
twee
n washing
the
surgical site
in ta
p water w
ith ban
dage
remov
ed to
abstaining from
hygiene
in any
of th
e 9 includ
ed studies
JBI lev
el of
eviden
ce:
1.b
JBI q
uality:
Low
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016239
5
Ref
T
ype
of
Stud
y Sa
mpl
e In
terv
entio
n(s)
O
utco
me
Mea
sure
s &
Len
gth
of F
ollo
w-u
p R
esul
ts
Quieros,
2014
System
atic
review
co
mpa
ring
sterile
salin
e with
tap
water fo
r redu
cing
wou
nd
infection an
d prom
oting
healing
3 RC
Ts in
clud
ed
The stud
ies were RC
Ts con
ducted
in US an
d Australia.
Participan
ts w
ere ad
ults w
ith la
ceratio
ns,
acute or chron
ic w
ound
s presen
ting in an
emerge
ncy de
partmen
t in tw
o stud
ies.
Inclusion crite
ria:
Both studies only includ
ed w
ound
s with
out
sign
ificant com
plication (e.g. n
ot fu
ll thickn
ess, not in
volving joints, n
ot req
uiring
surgical deb
ride
men
t)
Exclusion crite
ria:
• In both stud
ies pa
tients with
signific
ant
comorbiditie
s (e.g. d
iabe
tes,
immun
osup
pressed) w
ere exclud
ed
• Pa
tients taking
antibiotic
s were exclud
ed
• Sterile
saline wou
nd irriga
tion (n=3
26)
versus
• Ta
p water irriga
tion (n=3
57)
In one
study
, fluids were at roo
m
tempe
rature
In both stud
ies, fluid was delivered
with
force using syring
e
• Wou
nd in
fection (the
trials
used
differen
t criteria to
defin
e infection)
Wou
nd in
fection rate (2
RCT
s, n=6
83)
Tap water w
as m
ore effective than
saline in
prev
entin
g wou
nd in
fection, how
ever th
e result was not signific
ant (OR 0.79
, 95%
CI
0.36
to 1.72, p=0
.55)
JBI lev
el of
eviden
ce:
1.a
JBI q
uality:
High qu
ality
Griffiths ,
2001
RC
T co
mpa
ring
tap water to
no
rmal saline for
irriga
ting wou
nds
Participan
ts w
ere recruited from
two
commun
ity hea
lth cen
tres in
Australia (n
=43
patie
nts with
60 wou
nds rand
omised
, n=3
5 pa
tients with
49 wou
nds co
mpleted
follo
w
up)
Inclusion crite
ria:
• Acu
te or ch
ronic no
n-‐sutured wou
nd of
Grade
II (p
artia
l thickne
ss skin loss dow
n to
epidermis and
/or de
rmis) o
r Grade
III (full
thickn
ess skin lo
ss dow
n to but not
includ
ing fascia)
Exclusion crite
ria:
• Im
mun
osup
pressed
• Existin
g infected
wou
nd
• Skin graft, skin graft d
onor site
s, w
ound
s with
sinus, u
nbroke
n skin w
ound
s, fu
ll thickn
ess wou
nds extend
ing into m
uscle,
bone
or supp
ortin
g structures
• Use of a
ntibiotic
s Pa
rticipan
t cha
racteristic
s:
• Mea
n ag
e 78
.9 yea
rs (S
D 12.63
) • Mea
n wou
nd duration 81
.70 (ran
ge 3 to
36
5) days in ta
p water group
and
21.6.15
(ran
ge 14 to 209
8) days in saline grou
p • Mea
n wou
nd size 50
3.04
mm2 (ran
ge 9 to
21
23) in tap water group
and
323
.38m
m2
(ran
ge 14 to 169
5) in
saline grou
p • More laceratio
n in saline grou
p (16 ve
rsus
8)
• All wou
nds received
irriga
tion via
syring
e an
d cann
ula with
fluid at
wou
nd te
mpe
rature
• All wou
nds ha
d exud
ate remov
ed w
ith
gauze prior to clean
sing
•
Participan
ts w
ere rand
omised
to
receive either:
o Clean
sing
with
tap water dispe
nsed
from
the he
alth cen
tre fauc
et w
ithin
the prev
ious 24 ho
urs an
d stored
in
an empty, clean
ed saline bo
ttle
(n=2
3 wou
nds)
o N
ormal saline stored
in th
e same
type
bottle
that had
its seal
remov
ed w
ithin th
e prev
ious 24
hours (n=2
6 wou
nds)
• Wou
nds were dressed with
ap
prop
riate dressing
s an
d pa
tients
kept dressing dry
• Assessm
ent o
f wou
nd at
baselin
e an
d 6 wee
ks by
research
er and
by co
mmun
ity
nurse at each dressing
cha
nge
using a stan
dardised
tool
• Assessm
ent o
f hea
ling do
ne
with
a w
ound
grid an
d a
cotton
bud
to m
easure dep
th
• Wou
nd classified
as he
aling
whe
n ep
ithelial tissue presen
t •
Wou
nd in
fection was
determ
ined
using
Cuttin
g’s
crite
ria an
d pu
rulent exu
date
was con
side
red to in
dicate
infection
Wou
nd in
fection rate at 6 wee
ks
• Ove
rall incide
nce 6.1%
(all in saline
grou
p)
• No sign
ificant differen
ce in
infection rate
betw
een grou
ps (p
>0.05)
Wou
nd hea
ling at 6 w
eeks
No sign
ificant differen
ce in
com
plete
healing be
twee
n he
aling in ta
p water group
ve
rsus saline grou
p (34.7%
versus 61
.5%,
p>0.05
) Amou
nt of irrigation flu
id used
No sign
ificant differen
ce betwee
n vo
lume of
water used co
mpa
red to saline (p>0
.05)
JBI lev
el of
eviden
ce:
1.c
JBI q
uality:
Mod
erate
quality
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 240
6
Ref
T
ype
of
Stud
y Sa
mpl
e In
terv
entio
n(s)
O
utco
me
Mea
sure
s &
Len
gth
of F
ollo
w-u
p R
esul
ts
• More ve
nous ulcers an
d pressure in
juries
in ta
p water group
(11 ve
rsus 7)
Fello
ws,
2006
An ob
servationa
l stud
y exploring
contam
ination
rate of h
ome-‐
mad
e salin
e solutio
n
Samples w
ere prep
ared
in a hom
e he
alth
agen
cy and
tested
by a registered
hospital
labo
ratory
• Sa
mples w
ere mad
e of saline using a
1-‐ga
llon (3
.78 litres) bottle
of d
istilled
water w
ith 8 te
aspo
ons of ta
ble salt to
mak
e isoton
ic saline
• Storag
e: 2 bottle
s were stored
in th
e refrigerator at 9°C an
d 5 bo
ttles were
stored
at roo
m te
mpe
rature (2
6°C)
• Sa
mples w
ere cu
ltured wee
kly
for 4 wee
ks at a
hospital
labo
ratory
Culture results room
tem
perature
• At 1
wee
k the salin
e at roo
m
tempe
rature 50%
con
tained
600
0 cfu/mL ba
cillu
s species
• At 2
wee
ks 50%
sam
ples con
tained
50
%>5
0,00
0 cfu/mL Pseudo
mon
as
pickettii and
50%
con
tained
>25
,000
cfu/mL ba
cillu
s species
Culture results refrigerator
• No grow
th until 4 wee
ks
• At 4
wee
ks 1 sam
ple co
ntaine
d 60
0 cfu/mL Pseu
domon
as spe
cies
JBI lev
el of
eviden
ce:
3.e
JBI q
uality:
Low qua
lity
Moscati,
2007
RC
T exploring
infection rate in
wou
nd irriga
ted
with
sterile saline
versus ta
p water
Participan
ts w
ere a no
n-‐co
nsecutive sample
of peo
ple attend
ing em
erge
ncy de
partmen
ts
(ED) in three ho
spita
ls in
US (n=7
11
rand
omised
, n=6
34 com
pleted
follo
w-‐up an
d an
alysed
) Inclusion crite
ria:
• Age
d ≥ 18
yea
rs
• Unc
omplicated
skin laceratio
n requ
iring
sutures or staple repa
ir
Exclusion crite
ria:
• Pu
ncture w
ound
s, self-‐inflicted
wou
nds
• Wou
nd ≥ 8 hou
rs old on presen
tatio
n •
Wou
nd in
volving tend
on, joint or bo
ne
• Wou
nd w
ith gross con
tamination requ
iring
scrubb
ing or deb
ride
men
t •
Periph
eral vascu
lar disease,
immun
ocom
prom
ised
, cortic
osteroids
• Preg
nanc
y •
Taking
antibiotic
s Pa
rticipan
t cha
racteristic
s:
• App
roximately 27
% w
ound
s on
hea
d/ne
ck,
66% on up
per extrem
ity, 7
% on lower
extrem
ity
• Prim
arily sha
rp fo
rce injuries
• Mea
n wou
nd le
ngth 2.8 to
3cm
(ran
ge 0.5
to 15)
• All pa
rticipan
ts receive
d an
aesthe
sia
prior to irriga
tion an
d closure of
wou
nd w
ith sutures or stap
les
follo
wing irriga
tion
• No pa
rticipan
ts receive
d an
tibiotic
s •
Participan
ts w
ere rand
omised
to
receive:
o Tap
water irriga
tion directly und
er
fauc
et (e
xtremities) o
r using a clea
n tube
. Partic
ipan
ts atten
ded ow
n irriga
tion an
d were instructed
to
irriga
te und
er ta
p water fo
r a
minim
um of 2
minutes (n
=300
) o
Irriga
tion by
clin
ician with
sterile
salin
e via 35
mL syring
e an
d splash
shield (n
=334
)
• Wou
nd in
fection assessed
at
follo
w-‐up be
twee
n 5 an
d 14
da
ys la
ter assessed
in ED by
blinde
d he
alth professiona
ls
or, for patients no
t returning
to ED, a
ssessed ov
er th
e ph
one by
blin
ded calle
rs
• Co
st of interve
ntion,
estim
ated
based
on co
st of
supp
lies at one
of the
cen
tres
Wou
nd in
fection rate
• Sterile
saline 3.3%
versus tap water 4.0%
• Differen
ce in
wou
nd in
fection rate w
as
0.7%
(95%
CI –
2.25
% to
3.64%
, p=n
ot
sign
ificant)
• Re
lativ
e risk fo
r infection in ta
p water
grou
p was 1.21 (95%
CI 0
.5 to
2.7)
Irriga
tion
costs
Includ
ing co
sts for eq
uipm
ent, w
ater and
ad
ditio
nal u
se of a
ntibiotic
s associated
with
high
er in
fection rate, costs of tap
water w
as
estim
ated
at $
US 0.91
/patient versus $U
S 9.11
for sterile
saline
JBI lev
el of
eviden
ce:
1.c
JBI q
uality:
Mod
erate
quality
Reu
se o
f wou
nd d
ress
ing
prod
ucts
(inc
ludi
ng r
eusi
ng ir
riga
tion
fluid
s)
Ara
s and
Su
ssm
an,
2000
Observatio
nal
stud
y exploring
the
contam
ination of
Samples of three
produ
cts:
• Hyd
roge
l in a plastic
pack with
long
nozzle
with
sna
p tip
(Instrasite
) •
Amorph
ous ge
l in a plastic
tube
with
screw
• Tw
enty packs of e
ach ite
m w
ere
open
ed after han
d washing
and
using
clea
n disposab
le la
tex glov
es and
away
from
the pa
tient
• Amou
nt of b
acterial growth
compa
red to a con
trol growth
environm
ent
• No co
ntam
ination in any
packs on da
y 1
• On da
y 14
, on pa
ck of intrasite gel th
at
had be
en used on
day 1 and
7 had
JBI lev
el of
eviden
ce:
2.c
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016241
7
Ref
T
ype
of
Stud
y Sa
mpl
e In
terv
entio
n(s)
O
utco
me
Mea
sure
s &
Len
gth
of F
ollo
w-u
p R
esul
ts
hydrog
els after
open
ing
on cap
(Solug
el)
• Hyroa
ctive ge
l with
metal tu
b an
d plastic
screw on cap (Duo
derm
hyd
roactiv
e ge
l)
• Sm
all sam
ple placed
on a tong
ue
depressor for ap
plication
• Pa
ckag
e recapp
ed and
put in
to origina
l pa
ckag
ing
• Proc
edure repe
ated
on da
ys 1, 7
, 14,
21 (n
ote, procedu
re w
as in
fron
t of
patie
nt on da
y 21
) •
On da
y 7,14
,21 an
d 28
a sterile syringe
was used to w
ithdraw
a 1ml sam
ple
from
the pa
ckag
ing of 5 of the
20
packs for testing for co
ntam
ination
grow
th
• On da
y 21
no samples had
growth
• On da
y 28
no samples had
growth
JBI q
uality:
Mod
erate
quality
Zw
anzi
ger
and
Rop
er,
2002
Observatio
nal
stud
y exploring
contam
ination of
reusab
le
prod
ucts stored
in patient hom
es
Conv
enienc
e sample of 17 ho
me sites with
in
one ho
mecare ag
ency in
the US
Samples:
47 w
ound
care prod
ucts w
ere selected
for
inclusion in th
e stud
y.
• Su
pplie
s were used
in th
e ho
me
setting by
nurses, careg
ivers an
d pa
tients.
• Su
pplie
s were either:
o ope
ned, unu
sed ite
ms (e.g. g
auze
squa
res, irriga
tion solutio
n) (n
=12)
or
o re
usab
le item
s such
as scissors,
plastic
wou
nd m
easure guide
s that
were clea
ned with
alcoh
ol betwee
n uses. (n=
35)
• Eq
uipm
ent w
as stored in th
e ho
me in
a variety of differen
t con
tainers
• Sw
abs were take
n from
the
prod
ucts in
the ho
me on
day 7
(n=2
6) and
day 14 (n=2
1)
• Sw
abs were take
n from
3
control p
rodu
cts (uno
pene
d ga
uze) stored at th
e ho
me
agen
cy office.
• Sterile
equ
ipmen
t, procedu
re
and storag
e used
to attain
samples fo
r testing.
• Cu
lture swab
s were take
n from
all prod
ucts.
Control sam
ples
No ba
cterial colon
y grow
th fo
und in con
trol.
Samples from
hom
e sites
Day 7
• 5 type
s of organ
isms iden
tified in cultures
Day 14
• 7 type
s of organ
isms iden
tified
• 75
% of sam
ples w
ere co
ntam
inated
•
The long
er th
e sample was stored in th
e ho
me, th
e more co
ntam
inan
ts fo
und
• More virulent bacterial strains w
ere
located on
reu
sable prod
ucts (e
.g.
scissors)
JBI lev
el of
eviden
ce:
3.e
JBI q
uality:
Very low
quality
Gou
veia
, 20
07
Observatio
nal
stud
y inve
stigating
leve
l of
contam
ination on
reused
saline
flasks
Conv
enienc
e sample of ran
domly selected
salin
e bo
ttles in 22 he
alth care centres in
Spain (n=4
4)
• Sa
line fla
sks were rand
omly selected
from
the em
erge
ncy room
(ER) and
an
outpatient clin
ic at 2
2 centres
• Sa
line solutio
n fla
sks were mixed
, the
top was disinfected
with
sod
ium
hypo
chlorite and
5 m
l sam
ples
remov
ed w
ith a syringe
and
nee
dle.
• Sw
abs were also ta
ken from
the salin
e fla
sk tran
sfers
• Sam
ples w
ere seed
ed on sterile
aga
r plates
• Leve
l of c
ontamination (colon
y form
ing un
its [C
FU]/ml)
• 54
.5% of saline solutio
n fla
sks were
contam
inated
(CFU
/ml ran
ged from
1 to
23
0)
• 50
% sam
ples con
taminated
in saline
solutio
ns, 3
7.5%
con
taminated
on
tran
sfer and
12.5%
con
taminated
at b
oth
sources
• ER
flasks w
ere sign
ificantly m
ore likely to
be con
taminated
com
pared to outpa
tient
flasks (p=0
.01)
• Co
ntam
ination is like
ly due
to th
e use of
the salin
e fla
sks for multip
le patients
JBI lev
el of
eviden
ce:
3.e
JBI q
uality:
low qua
lity
Wou
nd d
ress
ing
prac
tice
Lawson,
2003
Co
hort study
co
mpa
ring
sterile
versus clean
dressing
proc
edure for
open
surgical
wou
nds
Participan
ts w
ere ga
strointestinal, traum
a,
tran
splant, g
eneral surge
ry and
urology adu
lt pa
tients
Inclusion crite
ria:
• op
en surgical w
ound
hea
ling via seco
ndary
intention
• Dressing ch
ange
s three tim
es daily w
ith
• In th
e first 3 m
onth period nu
rses
were attend
ing op
en surgical w
ound
s using sterile
tech
niqu
e (not described
bu
t procedu
re req
uired sterile
glove
s,
scissors or bo
wls) (1,07
0 ad
mission
s,
unkn
own ho
w m
any ha
d op
en surgical
wou
nd)
• Wou
nd swab
for cu
ltures –
unclea
r ho
w it w
as
determ
ined
if a w
ound
sho
uld
be swab
bed
• Su
rgical site
infection rate iden
tified via
wou
nd culture th
roug
h infection co
ntrol
tracking
was not signific
antly
differen
t (0.84%
versus 0.83
%, p
=ns)
• Su
rgical sup
ply bu
dget w
as $38
0 less in
on
e un
it of th
ree mon
ths
• Time to atten
d dressing
s de
crea
sed from
JBI lev
el of
eviden
ce:
3.c
JBI q
uality:
Very low
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 242
8
Ref
T
ype
of
Stud
y Sa
mpl
e In
terv
entio
n(s)
O
utco
me
Mea
sure
s &
Len
gth
of F
ollo
w-u
p R
esul
ts
norm
al saline
Exclusion crite
ria:
• Non
e stated
Pa
rticipan
t cha
racteristic
s:
• Non
e supp
lied
• In th
e seco
nd 3 m
onths nu
rses
received
edu
catio
n in atten
ding
clean
dressing
s an
d used
this te
chniqu
e for
open
surgical w
ound
s (not described
bu
t procedu
re did not req
uire sterile
glov
es, scissors or bow
ls) (96
3 ad
mission
s, unk
nown ho
w m
any ha
d op
en surgical w
ound
)
approx
imately 13
mins to app
roximately
10 m
ins
Mer
cei,
2004
RC
T co
mpa
ring
dressing
versus
no dressing
follo
wing surgery
Consecutive sample of children un
dergoing
surgery ov
er a 4 yea
r pe
riod
in a hospital in
Jordan
(n=4
51)
Inclusion crite
ria:
Clea
n surgical w
ound
Exclusion crite
ria:
Central ven
ous catheter in
sertion
Participan
t cha
racteristic
s:
• 11
.3% abd
ominal w
ound
s, 80%
groin
wou
nds, 6.4% hea
d an
d ne
ck w
ound
s,
2.2%
thoracic w
ound
s No furthe
r de
mog
raph
ics repo
rted
Participan
ts w
ere rand
omized
by birth
date to
: • Wou
nd dressing follo
wing surgery
(n=2
16)
• Wou
nd le
ft exp
osed
follo
wing surgery
(n=2
35)
• Pa
rticipan
ts w
ith exp
osed
wou
nds
were pe
rmitted
to sho
wer, d
oes no
t repo
rt if th
ose with
dressings also
show
ered
.
• Fo
llow-‐up was con
ducted
in
the ou
tpatient dep
artm
ent 1
wee
k after discha
rge from
ho
spita
l but w
ithin 30 da
ys of
surgery
• Fo
r pa
tients no
t presenting to
outpatients, fo
llow-‐up was via
teleph
one co
nsultatio
n • Definition
of a
wou
nd
infection was not rep
orted
Wou
nd in
fection rate
There was no sign
ificant differen
ce in
infection rate betwee
n wou
nd le
ft exp
osed
an
d wou
nds co
vered (1.7% versus 1.4%
. p=
ns)
JBI lev
el of
eviden
ce:
1.c
JBI q
uality:
Low
Selim
200
1 Action research
qu
alita
tive stud
y aimed
at
prom
oting
effective clinical
practic
e with
respect to
clea
nsing wou
nds
in th
e co
mmun
ity
Three co
mmun
ity nursing
reg
ions in
Australia
Commen
ced with
7 partic
ipan
ts but
decrea
sed to 3-‐4 m
embe
rs after in
itial
mee
tings.
Participan
ts w
ere co
mmun
ity hea
lth nurses
enga
ged in th
e research
and
qua
lity
improv
emen
t process.
• Pa
rticipatory actio
n research
includ
ing
literature review
, foc
us group
s,
survey
s an
d attempted
RCT
. • Data is rep
orted as a com
men
tary of
the actio
n research
process and
includ
es som
e qu
antitative repo
rting
of surve
y results
and
som
e qu
alita
tive/op
inion ev
iden
ce on
ratio
nale fo
r ch
anging
practice an
d effectiven
ess of edu
catio
n.
• N/A
Major find
ings
• Aseptic te
chniqu
e requ
ires a sterile
dressing
pack an
d sterile
clean
sing
solutio
n.[C]
• Clea
n tech
niqu
e allows irriga
tion or
bathing with
saline or ta
p water and
pe
rforming using a clea
n surface for
dressing
equ
ipmen
t.[C]
• Pa
tients with
VLU
s may fe
el m
ore
comfortab
le w
hen the who
le le
g is
washe
d with
warm ta
p water rathe
r than
co
nfining clea
nsing to th
e wou
nd bed
. [C]
• Co
ncern ab
out p
oten
tial infectio
n is a
barrier to uptak
e of clean
tech
niqu
e in
commun
ity settin
gs. [C]
• Influ
encing
sustained
cha
nge in dressing
tech
niqu
e practic
e requ
ires lo
ng te
rm
strategies. [UE]
•
JBI lev
el of
eviden
ce:
3 (mea
ning
fuln
ess)
JBI q
uality:
High qu
ality
Poole an
d Co
ughlan
, 20
02
Cross-‐sectiona
l survey
on ch
ange
in practice for
asep
tic te
chniqu
e
Conv
enienc
e sample of 2 gen
eral practices in
UK (total pop
ulation served
, n=2
3,15
0)
Inclusion crite
ria:
• Prescribed
for district nurses, practice
nurses and
at lea
st one
nursing
hom
e with
> 60
bed
s • Able to provide
data from
com
puter
• Ed
ucation session de
livered
to nurses
in th
e sample practic
es on a ch
ange
d proc
edure for asep
tic te
chniqu
e that
requ
ires use of a
sterile plastic field
and sterile
glove
s in place of a
dressing
pack.
• Nurses were give
n 3 mon
ths to
• Su
rvey
collected
data for the 3
mon
th prior to
practice
chan
ge and
3 m
onth after
practic
e ch
ange
. •
Data includ
ed:
o N
umbe
r dressing
packs used
• Dollars spe
nt on dressing
Num
ber of dressing pa
cks used
Re
duced in both practic
es fo
llowing ch
ange
of procedu
re
(practice on
e from
240
to 10 dressing
packs,
practic
e 2 from
405
to 130
dressing pa
cks)
Mon
ey spe
nt on dressing
packs
Redu
ced in both practic
es fo
llowing ch
ange
JBI lev
el of
eviden
ce:
4.b
JBI q
uality:
Very low
quality
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016243
9
Ref
T
ype
of
Stud
y Sa
mpl
e In
terv
entio
n(s)
O
utco
me
Mea
sure
s &
Len
gth
of F
ollo
w-u
p R
esul
ts
system
Pa
rticipan
t cha
racteristic
s:
No de
scription of partic
ipan
ts or wou
nds
invo
lved
in th
is study
implem
ent n
ew practice
packs
of procedu
re
• (practice on
e from
154
to 23 UK po
unds,
practic
e 2 from
261
to 130
UK po
unds)
Edu
catio
n in
ase
ptic
tech
niqu
e
Jackson
2012
Be
fore/after
stud
y inve
stigating
effectiven
ess of
asep
tic te
chniqu
e ed
ucation an
d factors
influ
encing
kn
owledg
e
Med
ical stude
nts in ne med
ical sch
ool in UK
were invited to partic
ipate (pha
se 1 to
tal 1
12
stud
ents, p
hase 2 to
tal 7
2 stud
ents)
Inclusion an
d ex
clusion crite
ria no
t rep
orted
Participan
t cha
racteristic
s:
Year 3 and
Yea
r 5 med
ical stude
nts
• Ph
ase on
e: Yea
r 3 med
ical stude
nt
participan
ts w
ere traine
d an
d assessed
in aseptic non
touc
h tech
niqu
e in
wee
k 1 of clin
ical placemen
t. A
sub
-‐sample were reassessed
and
interviewed
in w
eek 7-‐10
. (n=
112,
assessed
in w
eek 1 an
d n =4
6 un
derw
ent rea
ssessm
ent in wee
k 10
) • Ph
ase tw
o: Yea
rs 3 and
5 stude
nts
participated
in a w
ritten
que
stionn
aire
on aseptic te
chniqu
e du
ring
fina
l exam
s (n=7
2). F
ocus group
was held
with
4 stude
nts an
d interviews with
3
nurse ed
ucators/man
ager
• Co
nten
t of e
ducatio
n prog
ram w
as not
detaile
d in dep
th but w
as based
on 4
key principles:
o a
lways wash ha
nds effectively
o to
uch no
n-‐ke
y pa
rts with
con
fiden
ce
o ta
ke app
ropriate in
fective
precau
tions
o nev
er con
taminate ke
y pa
rts
• Observatio
n of clin
ical
proc
edure using a no
n-‐valid
ated
tool w
ith 11 ite
ms.
Stud
ents given
a pass or fa
il grad
e (unc
ertain how
this
score was determined
) • Que
stionn
aire in
pha
se 2 had
63
item
s with
stron
g internal
consistenc
y of α=0
.76
• Metho
ds fo
r interviewing no
t de
scribe
d in detail.
Phase on
e results – tw
o co
horts
• Th
ere was a signific
ant d
ecrease in pass
rate from
wee
k 1 to w
eek 10
(coh
ort 1
: 95
% vs 9%
, p<0
.001
; coh
ort 2
: 96%
vs
33%, p
<0.001
) • Most c
ommon
error le
ading to fa
ilure
was fa
ilure to
use clean
surface
• 46
% of p
artic
ipan
ts stated in in
terview
that a con
tributing factor to
failu
re w
as
not u
sing
aseptic non
touc
h tech
niqu
e in
daily practice
Phase tw
o qu
estion
naire an
d interviews
• 9.7%
had
not receive
d form
al aseptic non
touc
h tech
niqu
e training
• Stud
ents exh
ibite
d do
ubt a
bout th
e valid
ity of a
septic non
touc
h tech
niqu
e • Stud
ents exp
ressed
difficulty in
remem
bering
steps of a
septic non
touc
h tech
niqu
e • Po
or role mod
ellin
g was id
entified as a
contribu
ting factor to
failu
re to
perform
asep
tic non
touc
h tech
niqu
e co
rrectly
• Lack of resou
rces w
as id
entified as a
contribu
ting factor to
failu
re to
perform
asep
tic non
touc
h tech
niqu
e co
rrectly
JBI lev
el of
eviden
ce:
2.d
JBI q
uality:
Very low
quality
Ribu
, 200
3 Observatio
nal
stud
y exploring
the ways in
which
nurses
attend
leg ulcers
in com
mun
ity
care
Participan
ts w
ere recruited in a m
unicipality
in Norway.
Inclusion crite
ria (patients, n=3
2):
• Adu
lts ≥ 21 ye
ars
• Living
at h
ome an
d receiving ho
me care
• ≥ on
e leg or fo
ot ulcer
Inclusion crite
ria (nurses, n=3
1):
• Re
gistered
nurse in
com
mun
ity care
• Trea
ted foot/leg
ulcer during stud
y
Participan
t cha
racteristic
s:
• Pa
tient m
ean ag
e 79
±0.47 ye
ars
• Ulcer duration rang
ed 6 w
eeks to
20 yrs
• Nurses ha
d mea
n practic
al exp
erienc
e rang
ing 3 mon
ths to 32 yrs
Nurse m
ean ag
e rang
e 23
to 54
• Stud
ent n
urses (n=3
0) volun
teered
to
be observe
r da
ta collectors, w
orking
in
pairs
• Observe
rs receive
d training
in th
e ob
servation tool (n
=35 wou
nd care
even
ts observe
d)
• Se
mi-‐struc
tured ob
servationa
l instrumen
t dev
elop
ed to
aud
it actual practice ag
ainst
reco
mmen
ded practic
e • Data includ
ed han
dwashing
an
d asep
tic te
chniqu
e, as well
as care practic
e for ulcers
• Data was collected
by 2 raters
in pairs w
ho observe
d the
same proc
edure then
co
mpleted
the da
ta collection
tool in
depe
nden
tly (o
verall,
89% observatio
ns w
ere in
agreem
ent, 83%
han
d washing
ob
servations w
ere in
Wou
nd clean
sing
•
63% used no
rmal saline to clean
se ulcer
• 20
% clean
sed with
tap water
Han
d washing
•
43% w
ashe
d ha
nds be
fore and
after
proc
edures
• 60
% w
ashe
d ha
nds be
fore procedu
re
• 60
% w
ashe
d ha
nds after proc
edure
App
roximately 10
% of n
urses with
poo
r ha
nd hygiene
exp
lained
it as a result of th
e un
hygien
ic nature of th
e pa
tient hom
e
JBI lev
el of
eviden
ce:
3.e
JBI q
uality:
Very low
quality
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 244
10
Ref
T
ype
of
Stud
y Sa
mpl
e In
terv
entio
n(s)
O
utco
me
Mea
sure
s &
Len
gth
of F
ollo
w-u
p R
esul
ts
agreem
ent)
• Data was qua
lified with
interviews after the proc
edure
Staf
f att
itude
s and
beh
avio
urs
Unsworth
and Co
llins
2011
Qua
litative stud
y exploring ho
w
nurses neg
otiate
performing
asep
tic te
chniqu
e in com
mun
ity
settings
Nurse practition
ers in com
mun
ity settin
gs
(n=1
0)
Inclusion crite
ria:
• nu
rse practitione
r qu
alificatio
n • minim
um of 2
yea
rs’ e
xperienc
e • pe
rforms asep
tic te
chniqu
e in com
mun
ity
setting
Participan
t cha
racteristic
s:
• med
ian ag
e 44
.8 yrs (ran
ge 33-‐58
) • Initial training
in asepsis con
ducted
mea
n 26
yrs prior (ran
ge 12 to 34 yrs)
• All pa
rticipan
ts w
ere interviewed
rega
rding ho
w th
ey ada
pt th
eir clinical
care and
neg
otiate th
e ho
me setting
to m
aintain asep
sis
• Re
search
ers ob
served
each nu
rse
attend
ing proc
edures req
uiring
aseptic
tech
niqu
e for three differen
t patients
• Re
search
ers used
an au
ditin
g tool
based on
the stan
dardised
procedu
re
man
ual to do
cumen
t ways nu
rses
prob
lem solve
d pe
rforming asep
tic
tech
niqu
e
• N/A
Major find
ings
• District n
urses are aw
are that perform
ing
asep
tic te
chniqu
e in com
mun
ity settin
gs
is a cha
lleng
e.[C]
• Aseptic te
chniqu
e principles are in
graine
d in in
itial nurse training
and
com
mun
ity
nurses m
aintain kn
owledg
e of im
portan
t principles.[C
] • Co
mmun
ity nurses receive no
guida
nce in
how to
ada
pt th
e principles of a
septic
tech
niqu
e to th
e ho
me setting an
d pa
tient preferenc
es. [C]
• Lack of c
hoice in dressing pa
cks from
the
form
ulary hind
ers the pe
rforman
ce of
asep
sis in com
mun
ity settin
gs. [C]
• Co
mmun
ity nurses ch
oose clean
hard
surfaces at w
ound
heigh
t to crea
te a
sterile
field, how
ever th
is is often
on the
floor fo
r a leg ulcer dressing
. [C]
• Co
mmun
ity nurses display co
nfusion
rega
rding clea
n tech
niqu
e an
d the use of
tap water, o
ften
lead
ing to sterile field
contam
ination du
e to fa
ilure to
sep
arate
wou
nd w
ashing
from
aseptic
proc
edure.[C]
JBI lev
el of
eviden
ce:
3 (mea
ning
fulness)
JBI q
uality:
Mod
erate qu
ality
Hallett 200
0 Qua
litative
research
exploring
fatalistic
attitud
es to
asep
tic te
chniqu
e
Commun
ity hea
lth nurses in th
e UK (n=7
) Inclusion crite
ria:
Not rep
orted
Participan
t cha
racteristic
s:
Nurses were from
a ran
ge of d
ifferen
t expe
rien
ce le
vels
• Pa
rticipan
ts w
ere selected
to eng
age
in sem
i-‐struc
tured interviews with
4
research
ers
• Fa
talistic
philosoph
ical perspectiv
e,
phen
omen
olog
ical m
etho
dology,
semi-‐struc
tured interviews an
d interpretativ
e da
ta ana
lysis using a
pred
etermined
stanc
e of fa
talism
• N/A
Major find
ings
• Co
mmun
ity nurses pe
rceive
they
have a
lack of c
ontrol ove
r clea
nliness an
d therefore risk of infectio
n. [C
] • Co
mmun
ity nurses use the term
aseptic
tech
niqu
e vagu
ely as th
ey perceive
asep
sis as im
possible in
the ho
me
environm
ent. [C
] • Asepsis is viewed
as bo
th a process th
at
includ
es spe
cific
beh
aviours an
d practic
es
(e.g. sterile field an
d glov
es) a
nd a
phen
omen
on (b
eing
con
taminan
t free).
[C]
• So
me co
mmun
ity nurses view
infection
as una
voidab
le. [C]
JBI lev
el of
eviden
ce:
3 (mea
ning
fulness)
JBI q
uality:
Mod
erate qu
ality
11
Ref
T
ype
of
Stud
y Sa
mpl
e In
terv
entio
n(s)
O
utco
me
Mea
sure
s &
Len
gth
of F
ollo
w-u
p R
esul
ts
• Aseptic te
chniqu
e is a te
rm used to
describe
a rou
tinized
practice that
includ
es id
entifying
a dirty han
d an
d a
clea
n ha
nd. [C]
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Volume 24 Number 4 – December 2016245
REFERENCES1. Ngo QD, Vickery K, Deva AK. The effect of topical negative
pressure on wound biofilms using an in vitro wound model. Wound Repair Regen 2012;20(1):83–90.
2. James GA, Swogger E, Wolcott R et al. Biofilms in chronic wounds. Wound Repair Regen 2008;16(1):37–44.
3. Sandy-Hodgetts K, Carville K, Leslie G. Determining risk factors for surgical wound dehiscence: a literature review. Int Wound J 2015;12:265–75.
4. Leaper D, Ousey K. Evidence update on prevention of surgical site infection. Curr Opin Infect Dis 2015;28(2):158–63.
5. Roodsari GS, Zahedi F, Zehtabchi S. The risk of wound infection after simple hand laceration. World J Emerg Med 2015: DOI 10.5847/wjem.j.1920–8642.2015.01.008.
6. Sarwat T, Rashid M, Rastogi V, Chander Y. A comparative study of antibiogram of Pseudomonas aeruginosa in hospital- and community-acquired infections. Int J Curr Microbiol App Sci 2015;1:286–91.
7. Gillespie BM, Fenwick C. Comparison of the two leading approaches to attending wound care dressings. Wound Practice & Research 2009;17(2):84.
8. Unsworth J. District nurses’ and aseptic technique: where did it all go wrong? Br J Community Nurs 2011;16(1):29–34.
9. Watret L, McClean A. Cleansing diabetic foot wounds: tap water or saline? Diabetic Foot Journal 2009;12(3):5p.
10. Hallett CE. Infection control in wound care: a study of fatalism in community nursing. J Clin Nurs 2000;9(1):103–109.
11. Unsworth J, Collins J. Performing an aseptic technique in a community setting: fact or fiction? Prim Health Care Res Dev 2011;12(1):42–51.
12. Australian Commission on Safety and Quality in Health Care (ACSQHC), Standard 3: Preventing and Controlling Healthcare Associated Infection. Safety and Quality Improvement Guide. Sydney: ACSQHC: 2012.
13. National Health and Medical Research Council. Australian Guidelines for the Prevention and Control of Infection in Healthcare. Commonwealth of Australia, 2010.
14. Joanna Briggs Institute. Reviewers’ Manual 2014. Adelaide: Joanna Briggs Institute, 2014.
15. Joanna Briggs Institute, Reviewers’ Manual 2014: Summary of Findings Tables for Joanna Briggs Systematic Reviews. Adelaide: Joanna Briggs Institute, 2014.
16. Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 2009;6(6):e1000097.
17. Aras PS, Sussman G. The clinical contamination of amorphous hydrogels. Primary Intention 2000;8(4):137–40.
18. Bansal BC, Wiebe RA, Perkins SD, Abramo TJ. Tap water for irrigation of lacerations. Am J Emerg Med 2002;20(5):469–472.
19. Fellows J, Crestodina L. Home-prepared saline: a safe, cost-effective alternative for wound cleansing in home care. J Wound Ostomy Continence Nurs 2006;33(6):606–609.
20. Gouveia JCF, Miguéns CIM, Nogueira CLS, Alves MIP. Is it safe to use saline solutions to clean wounds? EWMA J 2007;7(2):7–12.
21. Griffiths RD, Fernandez RS, Ussia CA. Is tap water a safe alternative to normal saline for wound irrigation in the community setting? J Wound Care 2001;10(10):407–411.
22. Jackson D, Wall D, Bedward J. The sociocultural contribution to learning: why did my students fail to learn Aseptic Non-
Touch Technique? Multidimensional factors involved in medical students’ failure to learn this skill. Med Teach 2012;34(12):e800–12.
23. Lakshmi R, Andrews R, Chumber S. A study to compare the effectiveness of normal saline vs tapwater in irrigation of chronic wounds. Int J Nurs Educ 2011;3(1):19–21.
24. Lawson C, Juliano L, Ratliff CR. Does sterile or nonsterile technique make a difference in wounds healing by secondary intention? Ostomy Wound Manage 2003;49(4):56.
25. Merei JM. Pediatric clean surgical wounds: is dressing necessary? J Pediatr Surg 2004;39(12):1871–3.
26. Moscati RM, Mayrose J, Reardon RF, Janicke DM, Jehle DV. A multicenter comparison of tap water versus sterile saline for wound irrigation. Acad Emerg Med 2007;14(5):404–409.
27. Poole M, Coughlan A. Use of sterile dressing packs: challenging tradition. Nurs Times 2002;98(25):59–60.
28. Ribu E, Haram R, Rustøen T. Observations of nurses’ treatment of leg and foot ulcers in community health care. J Wound Ostomy Continence Nurs 2003;30(6):342–350.
29. Valente JH, Forti RJ, Freundlich MS, Zandieh SO, Crain EF. Wound irrigation in children: saline solution or tap water? Ann Emerg Med 2003;41(5):609–16.
30. Zwanziger PJ, Roper S. Bacterial counts and types found on wound care supplies used in the home setting. J Wound Ostomy Continence Nurs 2002;29(2):83–87.
31. Bee TS, Maniya S, Fang ZR et al. Wound bed preparation — cleansing techniques and solutions: a systematic review. Singapore Nursing Journal 2009;36(1):16.
32. Dayton P, Feilmeier M, Sedberry S. Does postoperative showering or bathing of a surgical site increase the incidence of infection? A systematic review of the literature. Foot Ankle Surg 2013;52(5):612–614.
33. Fernandez R, Griffiths R. Water for wound cleansing. Cochrane Database Syst Rev 2012(2).
34. Fernandez R, Griffiths R, Ussia C. Effectiveness of solutions, techniques and pressure in wound cleansing. JBI Reports 2004;2(7):231–270.
35. Fernandez RS, Griffiths RD, Ussia C. Wound cleansing: which solution, what technique? Primary Intention 2001;9(2):51.
36. Queirós P, Santos E, Apóstolo J, Cardoso D, Cunha M, Rodrigues M. The effectiveness of cleansing solutions for wound treatment: a systematic review. JBI Database of Systematic Reviews & Implementation Report 2014;12(10):121–151.
37. Selim P, Bashford C, Grossman C. Evidence-based practice: tap water cleansing of leg ulcers in the community. J Clin Nurs 2001;10(3):372–379.
38. Aziz AM. Variations in aseptic technique and implications for infection control. Br J Nurs 2009;18(1):26–31.
39. Blunt J. Wound cleansing: ritualistic or research-based practice? Nurs Stand 2001;16(1):33–36.
40. Boyce JM, Pittet D, Healthcare Infection Control Practices Advisory Committee. Society for Healthcare Epidemiology of America. Association for Professionals in Infection Control. Infectious Diseases Society of America. Hand Hygiene Task Force. Guideline for hand hygiene in health-care settings: recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Infect Control Hosp Epidemiol 2002;23(12 Suppl):S3–40.
41. Clark AP, John LD. Legal and ethical. Nosocomial infections and bath water: any cause for concern? Clin Nurse Spec 2006;20(3):119–123.
Haesler E et al. A systematic review of the literature addressing asepsis in wound management

Wound Practice and Research 246
Wound Practice and Research
THANK YOU
On behalf of the Editorial Board, Joint Editors Allison Cowin and Michael Woodward sincerely thank all reviewers who contributed to the 22 manuscripts that were published this year in Volume 24.
Thank you to Donna Angel, Judith Barker, Keryln Carville, Kerrie Coleman, Ann Marie Dunk, Kathleen Finlayson, Laurence Foley, Nikki Frescos, Anne Gardner, Chris Jackson, Chloe Jansz, Donald MacLellan, Kerry May, William McGuiness, Sue McLennan, Katy Melrose, Charne Miller, Julie Miller, Stuart Mills, Pam Morey, Geraldine Moses, Rachael Murray, Jenny Prentice, Tabatha Rando, Jan Rice, Dianne Smith, Terry Swanson, Sue Templeton and Lyn Thomas.
Special thanks to those who reviewed multiple manuscripts.
The voluntary contribution that each reviewer makes contributes greatly to the high standards that Wound Practice and Research strives to achieve.
42. Cunliffe PJ, Fawcett TN. Wound cleansing: the evidence for the techniques and solutions used. Prof Nurse 2002;18(2):95–99.
43. Ellis T. CPD: understanding the act of contamination in wound dressing procedure ... including commentary by Dreimanis D and Rice J. Collegian 2004;11(3):39–42.
44. Flores A. Sterile versus non-sterile glove use and aseptic technique. Nurs Stand 2008;23(6):35–39.
45. Friedman MM. Infection control update for home care and hospice organizations. Home Healthc Nurse 2003;21(11):753–760.
46. Gannon R. Wound cleansing: sterile water or saline? Nurs Times 2007;103(9):44–46.
47. Gilmour D. Is aseptic technique always necessary? Journal of Community Nursing 2000;14(4):32.
48. Gray M, Doughty DB. Clean versus sterile technique when changing wound dressings. J Wound Ostomy Continence Nurs 2001;28(3):125–128.
49. Grossman S, Mager DD. Managing the threat of methicillin-resistant Staphylococcus aureus in home care. Home Healthc Nurse 2008;26(6):356–366.
50. Hampton S. Nurses’ inappropriate use of gloves in caring for patients. Br J Nurs 2003;12(17):1024.
51. Hart S. Using an aseptic technique to reduce the risk of infection. Nurs Stand 2007;21(47):43–8.
52. Karch AM, Karch FE. ‘Clean’ vs ‘sterile’: are sanitary napkins and diapers acceptable as wound dressings? Am J Nurs 2001;101(4):25–25.
53. Lewis G. ANTT clinical competencies for nursing students ... aseptic non touch technique (ANTT). Australian Nursing Journal 2009;17(4):39–41.
54. O’Neill D. Can tap water be used to irrigate wounds in A&E? Nurs Times 2002;98(14):56.
55. World Health Organisation. WHO Guidelines on Hand Hygiene in Health Care: First Global Patient Safety Challenge Clean Care Is Safer Care. Switzerland: WHO, 2009.
56. Parker L. Applying the principles of infection control to wound care. Br J Nurs 2000;9(7):394–404.
57. Pegram A, Bloomfield J. Wound care: principles of aseptic technique. Mental Health Practice 2010;14(2):14–18.
58. Platt C. Wound cleansing: is tap water best? Primary Health Care 2005;15(5):27–30.
59. Preston RM. Aseptic technique: evidence-based approach for patient safety. Br J Nurs 2005;14:540–46.
60. Rowley S, Clare S. ANTT: a standard approach to aseptic technique. Nurs Times 2011;107(36):12–14.
61. Rowley S, Clare S, Macqueen S, Molyneux R. ANTT v2: an updated practice framework for aseptic technique. Br J Nurs 2010;19(Supp 1):S5–11.
62. Schremmer RD. New concepts in wound management. Clin Pediatr Emerg Med 2004;5(4):239–245.
63. Spear M. Wound care management. Wound cleansing: solutions and techniques. Plast Surg Nurs 2011;31(1):29–31.
64. Swanson J, Jeanes A. Infection control in the community: a pragmatic approach. Br J Community Nurs 2011;16(6):282–288.
65. Towler J. Cleansing traumatic wounds with swabs, water or saline. J Wound Care 2001;10(6):231–234.
66. Whaley S. Tap water or normal saline for cleansing traumatic wounds? Br J Community Nurs 2004;9(11):471–476.
67. Wilkins RG, Unverdorben M. Wound cleaning and wound healing: a concise review. Adv Skin Wound Care 2013;26(4):160–163.
68. WOCN Wound Committee. Clean vs. sterile dressing techniques for management of chronic wounds: a fact sheet. J Wound Ostomy Continence Nurs 2012;39(2S):S30–s34.
69. Rowley S, Clare S. ANTT Core Clinical Guidelines 2016, Association for Safe Aseptic Practice: http://antt.org/ANTT_Site/about.html.
Haesler E et al. A systematic review of the literature addressing asepsis in wound management