Embed Size (px)
Citation preview

Page 1 of 22
The Newcastle upon Tyne Hospitals NHS Foundation Trust
Hand Hygiene Policy Effective: December 2011 Review December 2012
Summary
1. Hands must be decontaminated in accordance with the 5 moments for hand
hygiene. 2. Hand Hygiene may be performed using alcohol based hand gel, liquid soap or
an antiseptic solution. The choice of solution is dependant upon the activity performed.
3. All staff must be compliant with Bare Below the Elbow (BBE); all wrist watches
and jewellery (particularly stoned rings) must be removed before clinical contact. 4. Cuts and abrasions must be covered with waterproof dressings. 5. Effective handwashing technique involves three stages: preparation,
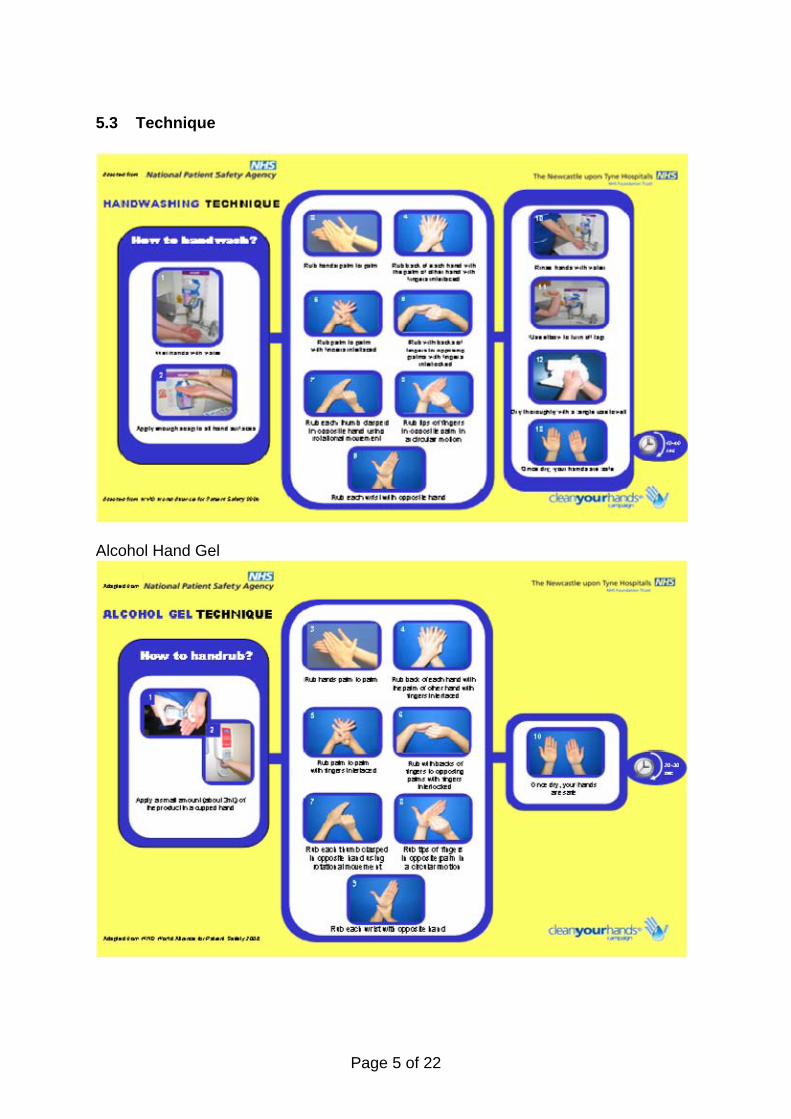
washing/rinsing, and drying (this should take 40-60 seconds). Preparation requires wetting hands under tepid running water before applying liquid soap or an antimicrobial preparation. The handwash solution must come into contact with all surfaces of the hand. The hands must be rubbed together vigorously for a minimum of 20-30 seconds paying particular attention to the tips of the fingers, the thumbs, wrists and areas between the fingers. Hands should be rinsed thoroughly prior to drying with paper towels.
6. When decontaminating hands using an alcohol based hand gel, hands should be
free of dirt and organic material. The handrub solution must come into contact with all surfaces of the hand. The hands must be rubbed together vigorously for a minimum of 20–30 seconds, paying particular attention to the tips of the fingers, the thumbs, wrists and the areas between the fingers, and until the solution has evaporated and the hands are left dry.
7. Apply a compatible hand cream regularly to protect skin from the drying effects
of hand decontamination. If a particular soap, antiseptic solution or alcohol based hand gel causes skin irritation, complete an incident form and seek occupational health advice.
1. Introduction
The most simple and effective way to prevent Healthcare Acquired Infections (HCAIs) is by undertaking effective hand hygiene. Hand hygiene must be performed at the right time using the correct technique. The hands of health-care workers are the most common vehicle for the transmission of micro-organisms from one patient to another, from one body site to another within the same patient, and from a contaminated environment to patients.
Page 2 of 22
Normal skin flora are referred to as resident micro-organisms. These can be responsible for cross infection if a staff member fails to decontaminate their hands. Transient micro-organisms exist on the skin surface and can be viral or bacterial. They are termed “transient”, as they are transferable through direct contact with equipment, the environment or individuals. These, unlike resident micro organisms, are more easily removed by hand decontamination therefore reducing the risk of transmission. Effective hand washing with liquid soap removes transient micro-organisms and renders hands socially clean and this is sufficient for general contact. The use of an antiseptic solution will remove transient micro-organisms and reduce resident flora prior to an aseptic procedure. Alcohol based hand gels require less time to use, offers a practical and acceptable alternative when handwashing and hand drying facilities are inadequate or not available. This is not the only time we advocate the use of alcohol gel. However, alcohol is not effective at removing dirt, organic material or spore forming organisms such as Clostridium difficile. It is essential that there is a risk assessment made on the handwashing agent to be used prior to undertaking an episode of care.
2. Purpose This policy is intended to ensure that all members of clinical and non clinical staff including students, agency workers and contractors working within the Newcastle upon Tyne Hospitals NHS Foundation Trust (NuTH) adhere to and practice good hand hygiene. All members of staff must also comply with ‘Your 5 moments for hand hygiene’. This is necessary to ensure a safe environment for patients, carers, public and staff in the interests of preventing and controlling the spread of infection. The key principles and aims of the policy are: • Achieve and sustain a minimum 98% compliance with hand hygiene audit
(opportunity, technique and bare below the elbow). • Prevent Healthcare Acquired Infection. • Ensure all staff receive hand hygiene training as part of Trust Induction and
Mandatory Infection Prevention and Control training. 3. Training • Breeze Infection Prevention and Control Level 1 (e-learning) is mandatory for
all Trust staff, on induction and annually thereafter as outlined in the Mandatory Training Policy. This programme contains hand hygiene training which all Trust staff must access, complete and pass. The training is recorded through the e learning completion software and reported to the Trust Education Board, Trust Board and Executive.
• Additional hand hygiene training can be delivered by the Infection Prevention
and Control (IPC) team or an IPC link person who has been trained to deliver the session

Page 3 of 22
4. Facilities All clinical areas should have • appropriate number and type of hand washing facilities • clear unobstructed access to all hand wash basins designated for handwashing
only, which are free of inappropriate items and fitted with elbow or wrist operated mixer taps/sensor taps
• wall mounted liquid soap and/or antiseptic solution available at every sink • paper towels available at every sink • alcohol based hand gel at the point of patient care and designated ward
entrances
The IPC team must be consulted, before any new construction or refurbishment work is planned, to advise on sink/tap type, number and location of hand washing facilities. To facilitate effective hand hygiene in the community healthcare workers should be provided with appropriate hand hygiene solutions and paper hand towels. 5. Hand Decontamination 5.1 Preparation
All staff must comply with the Trust Dress and Appearance Policy to ensure compliance with Bare Below the Elbow. Nails must be kept short. Artificial nails and the wearing of nail polish may increase the microbial load on hands and must not be worn. Similarly higher bacterial counts have been reported when stoned rings are worn. Stoned rings and wristwatches must not be worn in clinical areas/patients environment in the community. Wedding bands must be manipulated during hand washing
5.2 Hand Washing Agents
There are three types of agent that can be used to remove micro-organisms from hands: soap, antiseptic solution and alcohol based hand gel Soap Will mechanically remove transient micro-organisms but has little effect on resident micro-organisms. However, hand washing with soap is usually all that is necessary to prevent cross infection during social contact. It can be used before all routine tasks within the clinical area/patients in the community and after every patient contact. The IPC team recommend the use of liquid soap in containers which supply a measured dose. Antiseptic Solutions Will remove transient and reduce resident skin micro-organisms. Chlorhexidine based preparations have been found to be more effective than iodine-based solutions as they have a residual effect which influences the survival times of many organisms on hand surfaces.
Page 4 of 22
Antimicrobial agents should be used in situations when there is a need to reduce resident microbial flora, e.g. in operating theatres or similar departments, when dealing with patients in isolation, during outbreaks of infection and before performing an invasive procedure. In the community environment for example, patients homes, where antiseptic solutions may not be available staff must decontaminate their hands with soap and water followed by alcohol hand gel prior to undertaking an invasive procedure.
Alcohol-Based Hand Gels
Can be applied quickly and offers a practical and acceptable alternative when handwashing and hand drying facilities are inadequate or not available. However they are not effective in removing soiling or spores and should only be used if hands are visibly clean. Alcohol based hand gel must not be used with patients identified/suspected as Clostridium difficile positive.
All containers must be discarded when empty. Under no circumstances
should they be refilled or solutions decanted.
Page 5 of 22
5.3 Technique
Alcohol Hand Gel

Page 6 of 22
6. Hand Drying Agents In clinical areas wall mounted paper towels must be used to dry hands. A high absorbency paper towel will remove some of the transient organisms that remain after hand washing. In the community environment drying hands with disposable paper towels is preferable to using cotton towels. The use of hot air dryers should not be used in clinical areas as these spread airborne bacteria by re-circulating the surrounding environmental air. 7. Hand Care Frequent hand hygiene may cause skin problems for some health care workers. Hands must be wet prior to application of liquid soap or antiseptic solution. The use of an appropriate hand cream which is compatible with hand hygiene agents may help overcome some of these adverse effects. Compatible hand creams are provided in measured-dose pump dispensers. Health care workers must complete a Datix Incident Form and consult the Occupational Health Department if they experience any skin problems. 8. Hand Hygiene Opportunity Each hand hygiene opportunity corresponds to precise moments in patient care based on the 5 Moments for Hand Hygiene. All health-care workers must integrate hand hygiene in to all activities across NuTH. The Dental Hospital is an exception and the 5 Moments for Hand Hygiene have been amended; hand hygiene must be performed prior to and after contact with the patient and the working zone, this includes: the chair, light, equipment, stool, and table/bracket. Due to the low risk activity in the clean zone, i.e. notes writing, hand hygiene may not be necessary and will not be audited. An individual risk assessment as to whether hand hygiene in the clean zone is required must be undertaken by the individual health care worker.

Page 7 of 22
There are 5 indications for hand hygiene:

Page 8 of 22
9. Patients/Visitors Hand Hygiene All patients/visitors must be encouraged to attain good standards of hand hygiene to prevent transmission of infection. Staff must ensure that patients/visitors are offered the correct product and the opportunity to clean hands at the appropriate time Infection Prevention and Control information is available via the Trust Intranet and Internet, additionally; every clinical area has a dedicated Infection Prevention and Control information board for visitors and patients. Patients’ information leaflets are produced via the Patient & Public Involvement Committee and are available across the organisation. 10. Hand Hygiene Audit Process for Acute and Community Setting Acute Setting The compliance of hand hygiene opportunity/technique and Bare Below the Elbow (BBE) will be audited within the framework of the Clinical Assurance Tool (CAT)( see Appendix 1) on a monthly basis. Audits are to be completed by each clinical area using a system of peer review unless an exemption has been previously agreed by the IPCN team. Those areas that are self assessing must negotiate within their Directorate that peer review is achieved once per year, notifying the IPCN when this has been achieved. Hand Hygiene audit results will be included in the CAT Scorecard, which is reported to Trust Board, IPCC and Directorate Management Teams on a monthly basis. Community Setting The compliance of Hand Hygiene opportunity /technique and BBE will be audited within the framework of the Essential Steps Audit Tool (Appendix 4). Audits will take place on a quarterly basis. All clinical staff will be assessed annually 11. Performance Management – Escalation for Acute and Community Settings Achievement of 98% compliance, or above, is required by all staff groups for opportunity and all stages of hand decontamination processes (hand washing and/or alcohol gel application). All staff with direct patient contact or contact with patients’ surroundings must be BBE.
Failure to achieve 98% compliance will be monitored against the following escalation process.
11.1 Acute Setting
Immediate Action: Real time feedback will be provided directly to staff observed during
the audit period by the auditor. If any non-compliance is identified, the auditor must inform the Nurse-in-Charge/Manager and then email the Matron and IPCN for information. Nurse-in-Charge/Manager to take remedial action as necessary documenting what actions have been taken.

Page 9 of 22
Month 1: Where there is failure to achieve 98% compliance the Matron will investigate further documenting what actions have been taken if needed, identifying if any training requirements are required and liaising with Infection Prevention and Control Nurse(IPCN) and link personnel as necessary.
Month 2: Where there is failure to achieve 98% compliance for two
consecutive months, it is the responsibility of the Matron to initiate and complete an Action Plan (Appendix 2). As part of the Action Plan additional hand hygiene opportunity and technique audits (Appendix 3) will be undertaken for four consecutive weeks by a staff member nominated by the Matron. With this information the Matron will then be able to identify, target and address any education and training issues. The Matron will liaise with IPCN and IPC link personnel within their department for support if necessary. The completed Action Plans are to be submitted to the site Head of Nursing and the IPCN team.
Month 3: The Matron will continue with the Action Plan until 98% compliance
has been achieved. Month 4: Where there is failure to achieve 98% compliance for four
consecutive months Matron IPC will review with the Directorate Management Team.
Month 5: Where there is failure to achieve 98% compliance for five
consecutive months Head of Nursing review, with Matron Infection Prevention and Control and Directorate Management Team. The outcome of the review will be presented to the Director of Infection Prevention and Control, Medical Director and Nursing and Patient Services Director via IPCC. When the investigation has identified a system failure, support and guidance will be given to the Directorate. Where reckless behaviour/misconduct is identified, the Trust policy will be invoked.
11.2 Community Setting
Immediate Action: Real time feedback will be provided directly to staff observed during the audit period by the auditor. If any non-compliance is identified with an individual, the auditor must inform the Clinical/Cluster Lead. The auditor will document non-compliance and feedback on the audit forms which are returned to the Community IPCT and the Clinical Cluster Lead. The Clinical/Cluster Lead is to take remedial action where necessary, documenting the actions taken.
Quarter 1 Where there is failure to achieve 98% compliance the
Clinical/Cluster Lead will be informed by the Community IPCT The Clinical/Cluster Lead will then be able to identify, target and address any education and training issues. The IPCT and the Link Personnel for that area will offer support and advice if required.

Page 10 of 22
Quarter 2 Where there is failure to achieve 98% compliance for two
consecutive quarters the Clinical/Cluster Lead will investigate further and initiate and complete an Action Plan (Appendix 2) documenting what actions have been taken. As part of the Action Plan those members of staff identified as non-compliant from quarter 1 must be re-audited and forms submitted to the Community IPCT within the agreed 4 week period. This audit can be undertaken by the relevant link practitioner or a staff member nominated by the Clinical/Cluster Lead. The action plan will be managed by the Clinical/Cluster Lead liaising with the IPCT and IPC Link personnel as necessary.
The completed action plans are to be submitted to the Service
Manager and the IPCT for information. Failure to submit the re-audit data within the agreed time period will result in automatic reporting to Service Manager/Head of Nursing
Quarter 3 Where there is failure of a member of staff to achieve 98%
compliance for three consecutive quarters a review will be undertaken with the Matron IPC, Service Manager/Head of Nursing. The outcome of the review will be presented to the Director of Infection Prevention and Control, Medical Director and Nursing and Patient Services Director via IPCC. Where the investigation has identified a system failure, support and guidance will be given to the Directorate. Where reckless behaviour/misconduct is identified, the Trust policy will be invoked.
Failure to submit Essential Steps Audit Tool Where clinical teams fail to submit the Essential Steps Audit tool, the IPC team will inform the respective Clinical/Cluster Lead whose responsibility it will be to investigate further and unsure submission. Teams will be given a 1 week timescale from the original return date in which to complete and return the completed audit forms to the IPC team.
Where there is further failure in submission the relevant Service Manager will be informed.
Teams which fail to submit their forms will be highlighted in the quarterly report which goes to the Infection Prevention and Control Committee (IPCC)
Where there is continued failure to submit, a review will be undertaken with the Matron IPC, Service Manager / Head of Nursing. The outcome of the review will be presented back via IPCC. Where the investigation has identified a system failure, support and guidance will be given to the Directorate by the IPCNs. Where reckless behaviour/misconduct is identified, the Trust policy will be invoked.

Page 11 of 22
12. Monitoring Compliance in the acute setting with hand hygiene opportunity/technique and BBE will be monitored against the Hand Hygiene policy via the CAT framework. Results will be monitored/managed by Matron and IPCN, to ensuring audits are submitted on a monthly basis and non-compliance is reviewed and actioned. Wards/Departments that fail to achieve 98% compliance for two consecutive months will be reported to IPCC via Hand Hygiene Exception Reports on a monthly basis. Compliance for Community Services will be monitored against the Hand Hygiene policy via the Essential Steps Audit tool. Results will be monitored by the Clinical/Cluster Leads and IPCN to ensure audits are submitted on a quarterly basis and non compliance is reviewed and actioned. The IPCN Team will monitor areas in the acute setting that self assess, ensuring peer review occurs on an annual basis. A cross-section of directorates within the Acute and Community Setting will be independently validated on compliance with hand hygiene opportunity/technique and BBE on a annual basis by the IPC team. The validation results will be presented to the IPCC for review, on a quarterly basis. Staff knowledge of this policy is audited via IPC e-learning on an annual basis. References 1. Epic 2: National Evidence-Based Guidelines for Preventing Healthcare-
Associated Infections in NHS Hospitals in England. Journal of Hospital Infection (2007) 65 (Supplement) S1 – S64
2. National Patient Safety Alert (2004), Alcohol based Hand Gels (Up-dated 2008) 3. Code of Practice for the Prevention and Control of Health Care Associated
Infections (Health Act 2006, revised 2008) Department of Health. 2006 4. World Alliance for Patient Safety. WHO Guidelines on Hand Hygiene in
Healthcare. First Global Patient Safety Challenge. Clean Care is Safer Care. World Health Organisation (2009)
Related Policies
1. The Newcastle upon Tyne Hospitals NHS Foundation Trust Visitors Policy.
(2007) 2. The Newcastle upon Tyne Hospitals NHS Foundation Trust Dress, Appearance
and Uniform Policy (October 2010)
Policy Authors: Lesley Wilson Senior IPCN Sheila Postlewaite Senior Senior IPCN Louise Hall Matron IPC

Page 12 of 22
Appendix 1 Hand Hygiene CAT Audit – Opportunity and Technique The Newcastle upon Tyne Hospitals To be completed for 3 members of staff NHS Foundation Trust Site/Ward____________________ Date of Audit______________ Name of Auditor__________________________________
OPPORTUNITY Before patient contact
Before aseptic task
After body fluid exposure risk
After patient contact
After contact with patient surroundings
Staff 1 – Record Designation No. of Opportunities Observed Compliant Soap Compliant Alcohol Compliant Antiseptic Not Compliant Staff 2 – Record Designation No. of Opportunities Observed Compliant Soap Compliant Alcohol Compliant Antiseptic Not Compliant Staff 3 – Record designation No. of Opportunities Observed Compliant Soap Compliant Alcohol Compliant Antiseptic Not Compliant
TECHNIQUE (All stages of hand hygiene must be completed to be compliant) Palm to palm with fingers
interlaced Back of each hand with fingers
interlaced Back of fingers with fingers interlocked Thumbs Tips of fingers Wrists
Compliant Staff
1 How many techniques observed?___ How many are complete?_________
Staff 2
How many techniques observed?___ How many are complete?_________
Staff 3
How many techniques observed?____ How many are complete?__________
Bare Below Elbow (BBE) Staff
1 YES/NO Staff
2 YES/NO Staff
3 YES/NO
NHS

Page 13 of 22
Staff reporting skin complaints Staff 1
YES/NO Staff 2
YES/NO Staff 3
YES/NO
(please circle as appropriate) (February 2011) Hand Hygiene CAT Audit – Opportunity and Technique (Dental) The Newcastle upon Tyne Hospitals To be completed for 3 members of staff NHS Foundation Trust Site/Ward____________________ Date of Audit______________ Name of Auditor__________________________________
OPPORTUNITY Before contact with the patient/working zone
Before aseptic task
After body fluid exposure risk
After contact with patient/working zone
Staff 1 – Record Designation No. of Opportunities Observed Compliant Soap Compliant Alcohol Compliant Antiseptic Not Compliant Staff 2 – Record Designation No. of Opportunities Observed Compliant Soap Compliant Alcohol Compliant Antiseptic Not Compliant Staff 3 – Record Designation No. of Opportunities Observed Compliant Soap Compliant Alcohol Compliant Antiseptic Not Compliant
TECHNIQUE (All stages of hand hygiene must be completed to be compliant) Palm to palm with fingers
interlaced Back of each hand with fingers
interlaced Back of fingers with fingers interlocked Thumbs Tips of fingers Wrists
Compliant Staff
1 How many techniques observed?___ How many are complete?_________
Staff 2
How many techniques observed?___ How many are complete?_________
Staff 3
How many techniques observed?____ How many are complete?__________
Bare Below Elbow (BBE) Staff YES/NO Staff YES/NO Staff YES/NO
NHS

Page 14 of 22
1 2 3
Staff reporting skin complaints
Staff 1
YES/NO Staff 2
YES/NO Staff 3
YES/NO
(please circle as appropriate) (February 2011)

Page 15 of 22
Appendix 2
Action Plan Objective Action Target
Completion Date Person responsible
Comments

Page 16 of 22
Appendix 3
HAND HYGIENE AUDIT Name: Date: Directorate: Ward: Site: HAND WASHING TECHNIQUE T
otal observed
Palms Back of each hand
Finger webs
Thumbs Tips of fingers
Wrists Bare Below Elbow
Total observed
Doctor
Doctor
Nurse/HCA Nurse/HCA Domestic Domestic Physio/OTs Physio/OTs Porters Porters Students (Medical) Students (Medical) Student (Nursing) Student (Nursing) Radiographers Radiographers Other Other ALCOHOL GEL TECHNIQUE T
otal observed
Palms Back of each hand
Finger webs
Thumbs Tips of fingers
Wrists Bare Below Elbow
Total observed
Doctor
Doctor
Nurse/HCA Nurse/HCA Domestic Domestic Physio/OTs Physio/OTs Porters Porters Students (Medical) Students (Medical) Student (Nursing) Student (Nursing) Radiographers Radiographers Other Other To audit clinical areas only

Page 17 of 22
The Newcastle upon Tyne Hospitals NHS
NHS Foundation Trust
Opportunity Audit Name/Designation of Auditor Signature Date & time Base Ward/Site Ward/Site audited No. of persons observed
Before patient contact
Before aseptic task
After body fluid exposure risk
After patient contact
After contact with patient surroundings
Doctor (Total number observed = ) Potential Opportunities Compliant Soap Compliant Alcohol Compliant Antiseptic Not compliant Unknown Nurse/HCA (Total number observed = ) Potential Opportunities Compliant Soap Compliant Alcohol Compliant Antiseptic Not compliant Unknown Domestic (Total number observed = ) Potential Opportunities Compliant Soap Compliant Alcohol Compliant Antiseptic Not compliant Unknown Physio/OTs (Total number observed = ) Potential Opportunities Compliant Soap Compliant Alcohol

Page 18 of 22
Compliant Antiseptic Not compliant Unknown

Page 19 of 22
Porters (Total number observed = ) Potential Opportunities Compliant Soap Compliant Alcohol Compliant Antiseptic Not compliant Unknown Student (Medical) (Total number observed = )
Potential Opportunities Compliant Soap Compliant Alcohol Compliant Antiseptic Not compliant Unknown Student (Nursing) (Total number observed = )
Potential Opportunities Compliant Soap Compliant Alcohol Compliant Antiseptic Not compliant Unknown Other (Total number observed = ) Potential Opportunities Compliant Soap Compliant Alcohol Compliant Antiseptic Not compliant Unknown
Patients observed No. of soap dispensers: No. of alcohol dispensers/No. of staff with tottles No. antiseptic dispensers

Appendix 4 ADAPTED ESSENTIAL STEPS OBSERVATIONAL AUDIT TOOL Preventing the spread of infection Auditor Auditor Auditor Auditor Service and Locality: Staff Name/Role: OBSERVED ACTIVITY Observation 1 Observation 2 Observation 3 Observation 4 DATE OF OBSERVATION HAND HYGIENE Yes No N/A Yes No N/A Yes No N/A Yes No N/A 1. Fingernails are clean, short and free from varnish or artificial nails.
2. Jewellery including wrist watches/wrist jewellery is not worn (Plain wedding ring/band acceptable .If NO, please specify). 3. Staff member is bare below the elbows. 4. Staff perform hand hygiene as per the World Health Organisation Five Moments:
• Before patient contact • Before a clean/aseptic procedure • After body fluid exposure risk • After patient contact • After contact with patient surroundings
5. Routine Hand Wash Procedure – observed. a) Hands are wet first, and then liquid soap is applied. b) Palm to palm with fingers interlaced/Back of each hand with fingers interlaced/Back of fingers with fingers interlocked/Thumbs/Tips of fingers/Wrists
c) Hands are rinsed free of soap. d) All areas of the hands are dried thoroughly using paper towels. 6. Staff are observed using foot operated waste bins correctly. 7. Hand Sanitiser Procedure – observed.
a) Hands that are visibly soiled/contaminated ARE washed with liquid soap and water first. b) Solution is in contact with all surfaces of the hands for at least 15-30 seconds using the correct technique until evaporated as per hand hygiene policy. Hand Hygiene Total Additional comments:

Page 21 of 22
ADAPTED ESSENTIAL STEPS OBSERVATIONAL TOOL Preventing the spread of Infection OBSERVED ACTIVITY
Observation 1 Observation 2 Observation 3 Observation 4 DATE OF OBSERVATION
PERSONAL PROTECTIVE EQUIPMENT (PPE) Yes No N/A Yes No N/A Yes No N/A Yes No N/A
a) Appropriate use of sterile/non sterile golves and disposable aprons. b) Appropriate usage of other PPE e.g. eye/face protection Personal Protective Equipment (PPE) Total SHARPS
Yes No N/A Yes No N/A Yes No N/A Yes No N/A a) Box taken to point of use, and person using sharp is responsible for disposal. b) Boxes correctly signed and dated upon assembly/disposal. c) Stored in a secure environment at all times. Sharps Total ASEPTIC TECHNIQUE
Yes No N/A Yes No N/A Yes No N/A Yes No N/A a) Hand hygiene performed in accordance with WHO 5 moments. b) Correct PPE worn appropriately c) Appropriate risk assessment of sterile equipment required for procedure d) Appropriate preparation of area (home - utilise sterile field within dressing pack)
(clinic - dressings trolley cleaned with detergent and/or disinfectant ) e) Avoid contamination of sterile field, equipment and vulnerable site f) Asepsis maintained throughout procedure as per Aseptic Technique Policy Aseptic Technique Total Additional comments: (e.g. identified actions required to meet/maintain standards)
Completion provides supporting evidence for KSF dimensions C3, Health, Safety and Security and C5, Quality

Page 22 of 22
Audit Compliant Non-compliant
% Compliance
Hand Hygiene 0 0 0.00% Personal Protective Equipment 0 0 0.00% Sharps 0 0 0.00% Aseptic Technique 0 0 0.00% Total 0 0 0.00%

For advice on answering the above questions please contact Frances Blackburn, Head of Nursing, Freeman/Walkergate, or, Christine Holland, Senior HR Manager. On completion this form must be forwarded electronically to Steven Stoker, Clinical Effectiveness Manager, (Ext. 24963) [email protected] together with the procedural document. If you have identified a potential discriminatory impact of this procedural document, please ensure that you arrange for a full consultation, with relevant stakeholders, to complete a Full Impact Assessment (Form B) and to develop an Action Plan to avoid/reduce this impact; both Form B and the Action Plan should also be sent electronically to Steven Stoker within six weeks of the completion of this form. IMPACT ASSESSMENT FORM A October 2010
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST IMPACT ASSESSMENT – SCREENING FORM A
This form must be completed and attached to any procedural document when submitted to the appropriate committee for consideration and approval. Policy Title: Hand Hygiene Policy Policy Author: Lesley Wilson,Sheila Postlewaite and Louise Hall Yes/No? You must provide evidence to support your response: 1. Does the policy/guidance affect one group less or more favourably than another on
the basis of the following: (* denotes protected characteristics under the Equality Act 2010)
NO
• Race * NO • Ethnic origins (including gypsies and travellers) NO • Nationality NO • Gender * NO • Culture NO • Religion or belief * NO • Sexual orientation including lesbian, gay and bisexual people * NO • Age * NO • Disability – learning difficulties, physical disability, sensory impairment and
mental health problems * NO
• Gender reassignment * NO • Marriage and civil partnership * NO 2. Is there any evidence that some groups are affected differently? NO 3. If you have identified potential discrimination which can include associative
discrimination i.e. direct discrimination against someone because they associate with another person who possesses a protected characteristic, are any exceptions valid, legal and/or justifiable?
NO
4(a). Is the impact of the policy/guidance likely to be negative? (If “yes”, please answer sections 4(b) to 4(d)). NO
4(b). If so can the impact be avoided? 4(c). What alternatives are there to achieving the policy/guidance without the impact? 4(d) Can we reduce the impact by taking different action? Comments:
Action Plan due (or Not Applicable):
Name and Designation of Person responsible for completion of this form: Lesley Wilson Senior Infection Control Nurse Date: 29/12/11 Names & Designations of those involved in the impact assessment screening process: Sheila Postelwaite Senior Infection Control Nurse andLouise Hall Matron Infection Control (If any reader of this procedural document identifies a potential discriminatory impact that has not been identified on this form, please refer to the Policy Author identified above, together with any suggestions for the actions required to avoid/reduce this impact.)













![Hand hygiene [autosaved]](https://img.pdfslide.net/doc/110x75/554b598ab4c905793d8b4d70/hand-hygiene-autosaved.jpg)








