Embed Size (px)
Citation preview
![Page 1: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/1.jpg)
Handbook of Clinical Neurology, Vol. 92 (3rd series)Stroke, Part IM. Fisher, Editor# 2009 Elsevier B.V. All rights reserved
Chapter 4
Cerebral blood flow and the ischemic penumbra
KONSTANTIN-A. HOSSMANN1* AND RICHARD J. TRAYSTMAN2
1Max-Planck-Institute for Neurological Research, Cologne, Germany2University of Colorado at Denver and Health Sciences Center, Aurora, CO, USA
4.1. Normal values of cerebral blood flow
In middle-aged healthy humans, mean resting blood
flow is between 0.45 and 0.60 ml/g/min (Sokoloff
et al., 1957; Cohen et al., 1967; Slosman et al., 2001).
Partial volume-corrected blood flow of cortical gray
matter structures is 0.60–1.00 ml/g/min while white
matter blood flow is around 0.20 ml/g/min or lower
(Law et al., 2000; Meltzer et al., 2000). These values
for gray and white matter correspond to a mean transit
time of the circulating blood of about 3.0 and 6.0 sec-
onds respectively. In young children, blood flow is
twice as high as in adults (Kennedy and Sokoloff,
1957), probably resulting from an elevated brain meta-
bolism in the young, whereas there is a small decline
in blood flow with age that may be dependent upon
density of neurons per unit of tissue volume (Brody,
1955). Similarly, cerebral blood flow in laboratory ani-
mals varies with neuronal density and is highest in
small rodents, such as gerbils, rats, and mice, and lower
in other species, but this depends upon age and anesthe-
sia (Table 4.1).
Anesthesia, hypothermia, and metabolic inhibitors
reduce blood flow to a variable degree depending on
the kind and extent of intervention. Using barbiturates
as an anesthetic agent, the dose-dependent reduction in
blood flow correlates with the amplitude of sponta-
neous electroencephalogram (EEG) activity and results
in a decline in blood flow by about 50%, at which time
EEG becomes isoelectric (Michenfelder and Milde,
1975). However, reduction in blood flow with barbitu-
rates is not uniform throughout brain, with reduced
blood flow being greatest in brain areas with the
highest resting blood flow in the unanesthetized
state (Landau et al., 1955). Since brain blood flow,
*Correspondence to: K.-A. Hossmann, Max-Planck-Institut fur N
Germany. E-mail: [email protected]
metabolism, and function are closely coupled, it would
appear that, in the awake state, about one-half of the
resting blood flow is required to support the basic
metabolic needs of the brain whereas the other half is
required to fuel the spontaneous electrical activity of
the neuropil.
4.2. Blood flow changes after focal vascularocclusion
Extent and density of ischemia following focal vascu-
lar occlusion depend on many factors, notably anato-
mical site of vascular obstruction, local blood
perfusion pressure, blood viscosity and degree of
microvascular involvement, collateral blood supply,
and segmental resistance of conductance vessels
within the ischemic territory. The brain artery most
frequently affected under both clinical and experimen-
tal conditions is the middle cerebral artery, which sup-
plies roughly 60% of the ipsilateral hemisphere
(Fig. 4.1). The proximal branches of this artery, the
lenticulostriate arteries, supply the basal ganglia and
are end arteries, whereas more distal branches, which
support the circulation of cerebral cortex, make collat-
eral connections with the leptomeningeal network of
Heubner’s anastomoses (see below). Proximal
occlusion of the middle cerebral artery therefore con-
sistently produces infarction in basal ganglia and a
variable degree of ischemia in the cerebral cortex,
depending on the efficacy of the collateral blood
supply. After distal occlusion of the middle cerebral
artery, the basal ganglia are spared and cortical ische-
mia depends on the status of the collateral system.
The less frequent occlusions of the anterior and
posterior cerebral arteries produce mainly cortical
eurologische Forschung, Gleuelerstrasse 50, D-5093 Koln,
![Page 2: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/2.jpg)
Table 4.1
Cerebral blood flow values in laboratory animals
Species Blood flow (ml/g/min) Anesthesia Reference
Mouse 0.20 Isoflurane Foley et al., 2005
Rat Newborn (3–5 days) 0.36 Isoflurane Fumagalli et al., 2004
Newborn (7 days) 0.40 Isoflurane Vannucci et al., 2001
Adult 1.16 Awake Horinaka et al., 1997
Adult—cortex 1.19 Awake Sakurada et al., 1978
White matter 0.32 Awake Sakurada et al., 1978
Gerbil 0.81 Halothane Mies et al., 1990
0.54 Pentobarbital Turcani and Tureani, 2001
Rabbit Adult 0.40 Pentobarbital Littleton-Kearney et al.,
2000
0.56 Halothane/propofol Cenic et al., 2000
1.21 Awake Csete and Papp, 2000
Cat Adult cortex 1.30 Awake Sakurada et al., 1978
White matter 0.23 Awake Sakurada et al., 1978
0.44 Pentobarbital/halothane Rebel et al., 2003
1.00 Halothane Miyabe et al., 1996
0.30 Pentobarbital Schuier and Hossmann,
1980
Dog Newborn (2–7 days) 0.30 Halothane/nitrous oxide Mujsce et al., 1989
Adult—total brain 0.48 Awake Gross et al., 1980
White matter 0.19 Awake Gross et al., 1980
Adult—total 0.36 Pentobarbital McPherson et al., 1988
White matter 0.20 Pentobarbital McPherson et al., 1988
Sheep Preterm (93 day) 0.13 Awake Gleason et al., 2002
Near term (132 day) 0.20 Awake Gleason et al., 2002
Newborn lambs 1.00 Awake Jones and Traystman, 1984
Newborn lambs 0.60 Pentobarbital Miyabe et al., 1989
Adult 0.65 Awake Jones and Traystman, 1984
Pig Piglet (1–2 weeks) 0.48 Pentobarbital Ichord et al., 2001
Adult (4–6 weeks) 0.54 Pentobarbital Voelckel et al., 2002
Mini-pig 0.49 Isoflurane Andersen et al., 2005
Mini-pig (5–6 months) 0.55 Pentobarbital Delp et al., 2001
Monkey Young Rhesus (6 years) 0.55 Awake Noda et al., 2002
Old Rhesus (21 years) 0.43 Awake Noda et al., 2002
Adult monkey 0.26 Isoflurane Joshi et al., 2003
Adolescent baboon:
Total brain 0.75 Awake Meyer et al., 1980
White matter 0.35 Awake Meyer et al., 1980
Adolescent baboon 0.29 Etomidate/fentanyl Schumann-Bard et al., 2005
Adult baboon 0.55 Ketamine/nitrous oxide Kaufman et al., 2003
68 K.-A. HOSSMANN AND R.J. TRAYSTMAN
ischemia with a gradient of flow values, which
declines from the peripheral to more central parts of
the corresponding vascular territories.
Reversal of vascular occlusion initiates a triphasic
blood flow response, the dynamics of which depend
mainly on the duration of ischemia and the initial
reperfusion pressure. After ischemia times up to about
30 min, at normal blood pressure, tissue is reperfused
at increased blood flow rate (post-ischemic hyperemia
or luxury reperfusion), followed, after an interval that
roughly corresponds to the duration of the preceding
ischemia, by a reduction of blood flow below normal
(post-ischemic hypoperfusion). Finally, blood flow
increases again and stabilizes at or close to control
values. Post-ischemic hyperemia has been attributed
to release of vasoactive metabolites from injured brain
in combination with the post-ischemic loss of cerebro-
vascular regulation (Sundt and Waltz, 1971). The
![Page 3: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/3.jpg)
Fig. 4.1. Autoradiographic measurements of cerebral blood flow in different experimental models of focal ischemia.
CCA, common carotid artery; MCA, middle cerebral artery. (Courtesy of G. Mies.)
CEREBRAL BLOOD FLOW AND THE ISCHEMIC PENUMBRA 69
hyperemic response may also be due, in part, to neuro-
genic vasodilator mechanisms (Macfarlane et al.,
1991). Post-ischemic cerebral metabolic depression,
along with microvascular obstruction may account
for post-ischemic hypoperfusion (Iadecola, 1998).
After long durations of ischemia, post-ischemic hyper-
emia is gradually offset by post-ischemic recirculation
disturbances (no-reflow phenomenon). If a severe
degree of focal ischemia persists for more than 2 h,
hemodynamic and functional restitution are severely
impaired and the resulting tissue injury approaches
that of permanent ischemia.
4.2.1. No-reflow phenomenon
The no-reflow phenomenon has been attributed to
several mechanisms: increased blood viscosity, increa-
sed coagulation, microvascular occlusion, increased
intracranial pressure, endothelial swelling, and post-
ischemic hypotension (Hossmann, 1997). It was ori-
ginally described by Ames et al. (1968) following
global cerebrocirculatory arrest. Small circumscribed
foci of no-reflow appeared after 7.5 min of ischemia
and affected the larger part of the brain volume when
ischemia was prolonged to 15 min. The concept of
the no-reflow phenomenon was extended by Crowell
and Olsson (1972) to transient focal ischemia. These
authors noted impaired microcirculatory filling after
temporary occlusion of the middle cerebral artery in
monkeys and concluded that these disturbances con-
tributed to the irreversibility of the lesion. No-reflow
was also described by Ito et al (1980) following caro-
tid artery occlusion in gerbils, which could, however,
be reversed by induced hypertension. It should be
noted that at normal blood pressure such disturbances
were observed only after several hours of ischemia,
i.e. after ischemia sufficient to cause irreversible
neuronal damage even in the absence of recirculation
disturbances. After focal ischemia of 1 h, which is tol-
erated without primary injury, blood flow returned to
normal within 5 min (Levy et al., 1979). It can, there-
fore, be disputed if no-reflow after transient focal
ischemia at normal blood pressure is of pathogenic
significance for infarct development or merely an
accompaniment to irreversible tissue injury.
4.3. Collateral circulation
The brain is well protected against focal interruption
of its blood supply by a number of extra- and intracra-
nial collateral systems (Fig. 4.2) (Hossmann, 1993).
The principal anastomoses connecting the main sup-
plying territories are located (1) between the two com-
mon carotid arteries; (2) between the external carotid
artery and the vertebral artery; (3) between the exter-
nal carotid artery and the intracranial circulation
through anastomoses with the ophthalmic artery; (4)
through the intracranial system of the circle of Willis
at the base of the brain; (5) across the leptomeningeal
anastomoses of Heubner; (6) through the arterial ring
anastomoses of Schmidt; and (7) through the capillary
anastomoses of Pfeifer.
The rich anastomotic connections between the caro-
tid and vertebral arteries provide a powerful collateral
system that is able to compensate for occlusion of up
to three of these arteries. The intracerebral collateral
circulation is much less efficient and depends almost
entirely on Heubner’s network of pial anastomoses on
the surface of the brain. The arterial ring anastomoses
of Schmidt are of importance for maintenance of some
collateral flow during thromboangiitis obliterans, and
the capillary anastomoses of Pfeifer for maintenance
of collateral flow following microembolization, but
neither of these systems is able to compensate for
ischemic blockade of a major intracerebral artery. It is
also important to note that the medial penetrating
arteries supplying the basal ganglia and brainstem are
not connected to other vascular territories and behave
functionally like end-arteries.
Owing to the pial arterial network, occlusion of a
major intracerebral artery usually results in infarction
of the central part and not of the total supplying terri-
![Page 4: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/4.jpg)
ACAs
MCAsInternalcarotid art.
Internalcarotid art.
Internalcarotid art.
Basilary art.(A)
(B)
PCA PCA
MCA
MCA
ACA
ACA
PCA
PCA
Fig. 4.2. Collateral circulation of the brain. (A) The circle of Willis provides low resistance connections between the origins of
the anterior (ACA), middle (MCA) and posterior cerebral arteries (PCA). Reduction of blood supply by extracranial vascular
obstruction lowers blood perfusion pressure mostly in the peripheral branches of the brain arteries, leading to focal ischemia in
the border zones between the supplying territories (‘last meadow’ phenomenon). (B) Heubner’s leptomeningeal anastomoses
connect the peripheral branches of the brain arteries and provide collateral blood flow to the peripheral parts of the adjacent
vascular territories. Reduction of blood supply by intracranial occlusion of a brain artery lowers perfusion pressure mostly
in the proximal branches, leading to focal ischemia in the center of the vascular territory. (Modified from Zulch, 1985.)
70 K.-A. HOSSMANN AND R.J. TRAYSTMAN
tory. The actual size of the infarct is quite variable and
depends mainly on the number and vascular tone of
the leptomeningeal collateral channels, blood viscos-
ity, and blood perfusion pressure, which in turn is a
function of systemic blood pressure and intracranial
pressure. Computer simulations by Hudetz et al
(1982) revealed that middle cerebral artery occlusion
results in an infarct that covers about 50% of the terri-
tory of the middle cerebral artery when pial artery dia-
meter is 80 mm whereas dilation of pial arteries to
170 mm was able to completely prevent ischemia even
in the particularly endangered lenticulostriate areas.
This is the reason that young rats with a high capacity
for leptomeningeal vasodilation do not develop
infarcts after middle cerebral artery occlusion (Coyle,
1982), whereas in adult hypertensive rats, in which
the lumen of leptomenigeal vessels has narrowed,
infarcts may cover the whole supplying territory of
this artery (Coyle and Jokelainen, 1983).
The topography of ischemic lesions follows a differ-
ent pattern if cerebral blood flow is globally reduced,
e.g., by severe systemic hypotension or by multifocal
narrowing of the extracerebral supplying arteries in
advanced stages of atherosclerosis. Under these condi-
tions, blood flow is compromised initially in the periph-
ery and not in the center of the arterial territories
because the global reduction in blood perfusion pressure
results in the critical impairment of flow first in those
areas that are most distant from the arterial inflow. Since
these regions represent the borderlines between the sup-
plying territories of themain cerebral arteries, the result-
ing lesions have been termed ‘borderzone’ or watershed
infarcts. The hemodynamic situation leading to this type
of circulation failure has also been referred to as the ‘law
of the last meadow’ (Gesetz der letzten Wiese), in ana-
logy with the pattern of irrigation failure in agriculture
(Opitz and Schneider, 1950). The localization of such
infarcts on the brain surface is along the boundaries
between the territories of the anterior and middle and
the middle and posterior cerebral arteries, respectively,
and in basal ganglia in the terminal area of the lenticu-
lostriate arteries.
![Page 5: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/5.jpg)
D
The dynamics of collateral blood supply after acute
vascular occlusion have been studied by vital micro-
scopy and angiography. At normotension, the collat-
eral leptomeningeal circulation functions within 30
seconds (Meyer and Denny-Brown, 1957). Within a
few minutes, a further dilation of the collaterals occurs
due to accumulation of metabolic waste products.
After collateral flow has been established, the
occluded middle cerebral artery is retrogradely filled
from both the anterior and posterior cerebral arteries.
Finally, within a few weeks after vascular occlusion,
collaterals may undergo arteriogenesis, i.e. the active
remodeling of preformed vessels, leading to enlarge-
ment of the circle of Willis (Busch et al., 2003) and
appearance of serpentine leptomeningeal vessels with
distinctly larger lumen than the pre-existing anasto-
moses (Coyle, 1982). As the vascular conductance
increases to the fourth power of the vessel diameter
(see below), collateral blood supply increases accord-
ingly. This explains why, once collateral circulation
has been established, it is not likely to fail secondarily
(Sundt and Waltz, 1971).
4.4. Hemorheology and microcirculation
According to the equation of Hagen and Poiseuille,
Newtonian flow through tubes equals
Q ¼ DPr4
�8l;
where Q is the flow rate, DP is the pressure gradient, ris the tube radius, l is the length of the tube, and � is
the viscosity of the fluid. This equation is frequently
given to describe blood flow through the vascular sys-
tem; however, it provides only a rough approximation
of the actual situation. Blood is not a Newtonian fluid
and blood viscosity changes as a function of hemato-
crit, erythrocyte deformability, flow velocity (or shear
rate), and the diameter of the blood vessels.
In the macrocirculation, i.e. in vessels larger than
100 mm, blood viscosity is mainly a function of
hematocrit and shear rate: it increases in a non-linear
way with decreasing shear rate (Schmid-Schonbein,
1981) and increasing hematocrit (Grotta et al.,
1982). The influence of hematocrit on viscosity is
most pronounced at a low shear rate, representative
of low flow. This is partly because of erythrocyte
aggregation, which increases with low and decreases
with high shear rate. With laminar flow, aggregates
form mainly in the central low-shear-rate part of the
vessels but they disaggregate again when they move
into the high-shear region along the vessel wall.
Aggregation is also influenced by alterations of coa-
gulation parameters and by surface characteristics of
CEREBRAL BLOOD FLOW AN
erythrocytes that, in turn, depend on membrane struc-
ture, electrostatic forces, the presence of macromole-
cules such as fibrinogen, serum osmolality, and
blood pH. All these factors change during ischemia
and have a tendency to facilitate erythrocyte aggre-
gation (Wood and Kee, 1985). Platelet aggregation,
in contrast to erythrocyte aggregation, is irreversible.
Aggregates formed in the center of the axial stream
do not disaggregate when moving to the outer lamina
but rather are exposed to additional mechanical
injury by the higher peripheral shear, causing a
further increase of their adhesiveness and aggrega-
tion (Wood and Kee, 1985).
In the microcirculation, the influence of hemorheol-
ogy and blood flow is even more complex. The cere-
bral microcirculation, by definition, is the vascular
bed distal to the penetration of arterioles 30–70 mmin diameter into brain parenchyma. At this dimension,
blood viscosity substantially changes with blood vessel
diameter. As was first described by Fahreus and
Lindqvist (1931), apparent blood viscosity initially
falls as vessel diameter decreases (Fahreus and Lindq-
vist effect) but, when vessel diameter is reduced to less
than 5–7 mm, viscosity again increases (inversion phe-
nomenon; Dintenfass, 1967). The critical radius below
which inversion occurs increases with increasing
hematocrit, increasing erythrocyte stiffness, increasing
erythrocyte or platelet aggregation, and decreasing
flow rate (Gaethgens et al., 1978). Accumulation of
polymorphonuclear leukocytes has been reported in
areas of low or heterogeneous blood flow (Hallenbeck
et al., 1986), resembling in pattern that noted for plate-
let accumulation (Obrenovitch and Hallenbeck, 1985).
Since these processes increase blood viscosity at the
microcirculatory level, blood flow is further reduced
and a vicious circle is initiated that enforces the pri-
mary ischemic impact.
Other studies, however, suggest that microcircula-
tory disturbances are a secondary phenomenon, with
the primary lesion being neuronal damage. In fact,
Little et al. (1975) noted only mild microvascular
obstruction following middle cerebral artery occlu-
sion for up to 3 h, whereas severe changes were pre-
sent after 6 h of ischemia. Detailed neuropathological
studies revealed that morphological alterations con-
sistently precede microcirculatory obstruction, indi-
cating that the observed disturbances were not the
critical factor for the evolution of the ischemic
infarction.
4.5. Regulation of cerebral blood flow
Because of the rigid nature of the skull and incompres-
sibility of the brain, it had long been thought that
THE ISCHEMIC PENUMBRA 71
![Page 6: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/6.jpg)
ND
expansion of the cranial contents was severely limited
and that active changes in cerebral vessel caliber were
unlikely (Monro, 1783). This concept was later con-
firmed (Kellie, 1824) and became known as the
Monro–Kellie doctrine. It was not until 1890 that
Roy and Sherrington (1890) elucidated the two most
important concepts concerning the regulation of the
cerebral circulation: (1) that the brain has an intrinsic
mechanism to control its blood supply in accordance
with cerebral activity and (2) that chemical byproducts
of cerebral metabolism can lead to alterations in the
caliber of cerebral blood vessels.
4.5.1. CO2 reactivity
In intact brain, cerebral blood flow is tightly coupled
to the metabolic requirements of tissue (metabolic reg-
ulation) but remains constant in the presence of altera-
tions in blood pressure (autoregulation). Metabolic
regulation is reflected by the CO2 reactivity of cere-
bral vessels, which can be tested by the application
of carbonic anhydrase inhibitors or CO2 ventilation.
The effect of CO2 on the cerebral vasculature is pro-
nounced, easily demonstrated, and easily reproduced.
Cerebral vascular vasodilation and vasoconstriction
to increased and decreased CO2 are findings in mam-
mals at all ages. Under physiological conditions, blood
flow approximately doubles when CO2 is raised by
30 mmHg (Harper and Glass, 1965) and is reduced
by approximately 35% when CO2 is reduced to
25 mmHg (Reivich, 1964). The major factor account-
ing for the cerebrovascular response to CO2 is the
[H] of extracellular fluid but this mechanism could
work in conjunction with other influences such as
prostanoids or nitric oxide metabolism.
4.5.2. O2 reactivity
The effect of O2 on the cerebral circulation is also a
pronounced, easily demonstrated and reproducible
phenomenon. The brain has a high rate of aerobic
metabolism and thus depends on a continuous supply
of O2. Cerebral vasodilation and increased cerebral
blood flow are observed in response to oxygen chal-
lenges, including hypoxic hypoxia, carbon monoxide
hypoxia, and anemia hypoxia, and it is probably the
reduction in arterial O2 content rather than the O2 ten-
sion that is responsible for the increase of blood flow
(Traystman et al., 1978). A threshold for hypoxic
vasodilation exists at PO2 around 50 mmHg, below
which blood flow increases markedly (McDowall,
1966). Hyperoxia with 100% O2 breathing results in
mild cerebral vasoconstriction (Lambertsen et al.,
1953). Although it is clear that hypoxia produces cere-
72 K.-A. HOSSMANN A
bral vasodilation and a marked increase in cerebral
blood flow, the precise mechanism involved is unclear.
Hypotheses to explain this mechanism include direct
effects of O2, chemical or metabolic factors, and neu-
rogenic factors.
4.5.3. Autoregulation
The cerebral vasculature exhibits a remarkable capa-
city for autoregulation of cerebral blood flow; that is,
the relative constancy of cerebral blood flow over a
wide range of cerebral perfusion pressures (80–
150 mmHg) (Harper, 1966). This constancy in blood
flow is due to the active vasoconstrictions and vasodi-
lations occurring in response to increases and
decreases in pressure, respectively. The range of auto-
regulation may be shifted to the right with hyperten-
sion (Strandgaard et al., 1973) and to the left with
hypercarbia (Harper and Glass, 1965). Several the-
ories, which include myogenic, metabolic, and neuro-
genic influences, have been proposed to account for
the mechanism of autoregulation. The myogenic the-
ory proposes that changes in vessel diameter are
mediated by a direct effect of variations of blood pres-
sure on the myogenic tone of vessel walls. The meta-
bolic theory argues that some metabolic factor such
as CO2 or adenosine is the regulating factor. The neu-
rogenic notion proposes that autoregulation is
mediated by the adventitial nerves located on cerebral
vessels, but these may be secondary and not of great
significance.
4.5.4. Disturbances of flow regulation
During focal cerebral ischemia, tissue acidosis devel-
ops, leading to vasorelaxation and a severe disturbance
of the regulation of blood flow to autoregulation and
CO2 (Fig. 4.3). In the center of the ischemic territory,
CO2 reactivity is abolished or even reversed, i.e.
blood flow may decrease with increasing arterial
Pco2 (Symon, 1970; Waltz, 1970). This paradoxical
‘steal’ effect was attributed to the increase of blood
flow in non-ischemic adjacent brain areas that did
not lose CO2 reactivity (Hoedt-Rasmussen et al.,
1967) but this mechanism is disputed (Gogolak et al.,
1985), as described in more detail below.
Autoregulation is also disturbed following stroke
(Waltz, 1968; Symon et al., 1976), but the alterations
in blood flow are more severe with decreasing than
with increasing blood pressure. This is explained
by the fact that within the ischemic territory, local
cerebral perfusion pressure is below the lower limit
of autoregulation. A decrease in systemic blood pres-
sure cannot be compensated by further reduction of
R.J. TRAYSTMAN
![Page 7: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/7.jpg)
λ + 1
0x
λ + 1
0x
λ + 1
0x
λ + 1
0x
17
16
15
14
13
12
11
10
19
18
17
16
15
14
13
12
19
18
17
16
15
14
13
12
17
16
15
14
13
12
11
10
60 90 120Arterial blood pressure Arterial blood pressure
CO2 reactivity
Regulation of blood flow
Autoregulation
Control
Control
MCA occlusion
MCA occlusion
150 180 mmHg 60 90 120 150 180 mmHg
0 20 40
Arterial pCO2
60 80 Torr 0 20 40
Arterial pCO2
60 80 Torr
Fig. 4.3. Regulation of blood flow in the territory of the middle cerebral artery of cat. Autoregulation was tested by pharma-
cological alterations of systemic blood pressure, and CO2 reactivity by ventilation with 6% CO2. After middle cerebral artery
occlusion both autoregulation and CO2 reactivity are abolished. l, unit of thermoclearance for measurement of blood flow.
(Data from Shima et al., 1983.)
CEREBRAL BLOOD FLOW AND THE ISCHEMIC PENUMBRA 73
vascular resistance; an increase in blood pressure,
however, may shift local perfusion pressure into the
autoregulatory range and cause vasoconstriction. This
is of particular importance for collateral vessels, which
originate in the non-ischemic tissue and therefore pre-
serve their vascular reactivity (Shima et al., 1983). An
alternative explanation for the preserved blood flow
response to increased blood pressure is ‘false autore-
gulation’ (Miller et al., 1975). In the presence of
edema, an increase in blood pressure is associated with
an increase in local tissue pressure, thus precluding a
substantial improvement of actual tissue perfusion
pressure. Failure of cerebral autoregulation can be
demonstrated in such instances by dehydrating the
brain in order to reduce brain edema.
After transient ischemia, vasorelaxation persists
for some time, which explains the phenomenon of
post-ischemic hyperemia or luxury perfusion. During
luxury perfusion, oxygen supply exceeds the oxygen
requirements of the tissue, leading to the appearance
of red venous blood. With the cessation of tissue
acidosis, vascular tone returns and blood flow declines
to or below normal. Subsequently, autoregulation, but
not CO2 reactivity, may recover, resulting in uncou-
pling of metabolic regulation. This may be one of
the reasons why primary post-ischemic recovery may
be followed by delayed post-ischemic hypoxia and
secondary metabolic failure (Hata et al., 2000b).
4.6. Segmental vascular response
Two types of brain vessel must be distinguished: the
superficial or conducting vessels and the nutrient
or penetrating vessels (Gillian, 1971). Conducting ves-
sels comprise the extracerebral segment of the vascular
bed and include the carotid and basilar arteries, the
![Page 8: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/8.jpg)
ND
anterior, middle and posterior cerebral arteries, and the
network of interlacing branches of these arteries on the
surface of the brain (Heubner’s leptomeningeal anasto-
moses). Penetrating vessels and the associated capillary
network comprise the intracerebral segment of the brain
circulation. By recording the blood pressure difference
between the carotid and pial arteries on one hand, and
between the pial arteries and cerebrovenous outflow on
the other, segmental vascular resistances of the extracer-
ebral conducting and intracerebral nutrient vessels can be
calculated according to Ohm’s law (Shapiro et al., 1971;
Shima et al., 1983). In laboratory animals, about 50% of
total cerebral vascular resistance is accounted for by
extracerebral supplying vessels and 50% by intracerebral
nutrient vessels (Fig. 4.4) (Shapiro et al., 1971; Shima
et al., 1983). Both segments contribute equally to the
autoregulatory adjustment of vascular resistance; how-
ever, CO2 reactivity is controlled by the intracerebral
segment alone (Shima et al., 1983). This is in agreement
with the concept that CO2 reactivity reflects the behavior
of intracerebral (nutrient) vessels to alterations of
parenchymal metabolic activity, whereas autoregulation
74 K.-A. HOSSMANN A
Cortical blood flow
Arb
itrar
y un
its
161514131211109
100
80
60
40
20
0
% c
ontr
ol
0 20 40 60 80
mm HgPial artery pressure
EEG activity
0 20 40 60 80mm HgPial artery pressure
Fig. 4.4. Relationship between pial artery blood pressure measu
blood flow, segmental vascular resistance, the intensity of the enc
cular resistance is differentiated into an upstream segment, comp
segment that includes the intracerebral nutritional vessels. Pial a
middle cerebral artery. (Data from Date et al., 1984.)
is a myogenic response of the whole vascular system to
alterations of intraluminal pressure.
During middle cerebral artery constriction, resis-
tance of extracerebral supplying vessels rises and pial
arterial pressure falls (Date et al., 1984). Initially, this
decrease in pressure is compensated by an autoregulatory
dilation of the intracerebral vascular segment. As soon as
pial arteriolar pressure decreases to below 30 mmHg,
blood flow begins to fall and electrophysiological distur-
bances evolve (Fig. 4.4). At this level, the intracerebral
vascular segment is not yet fully dilated and vascular
resistance continues to decrease with further reduction
in blood flow (Date et al., 1984). This observation
demonstrates that acidosis, which develops during cere-
bral ischemia, causes a more pronounced vasodilation
than that induced by autoregulation alone.
After complete middle cerebral artery occlusion,
pial arterial pressure may be as low as 10–15 mmHg
(Shima et al., 1983; Date et al., 1984), and the back
pressure in the stump of the occluded artery is
less than 25% of the systemic pressure (Tulleken and
Abraham, 1975). If vascular occlusion is reversed, pial
R.J. TRAYSTMAN
Vascular resistance
Supplying arteries
Δm V
0−1−2−3−4−5−6−7
Arb
itrar
y un
its
12
10
8
6
4
2
0
Cortical steady potential
0 20 40 60 80
mm HgPial artery pressure
0 20 40 60 80mm HgPial artery pressure
red in the territory of cat middle cerebral artery and cortical
ephalogram and the cortical steady potential. Segmental vas-
rising the extracerebral supplying vessels, and a downstream
rtery pressure was lowered by transorbital constriction of the
![Page 9: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/9.jpg)
D
arterial pressure increases and frequently even rises
above control level. The slope of this increase deter-
mines the quality of reperfusion and explains why
reversal of mechanical vascular occlusion results in
faster and more homogenous reperfusion and meta-
bolic recovery than thrombolytic recanalization, in
which reperfusion is more slowly restored (Hossmann,
1998).
4.7. Anastomotic steal phenomenon
The interconnection of ischemic and non-ischemic
vascular territories by anastomotic channels may
divert blood from one brain region to another, depend-
ing on the magnitude and direction of the blood pres-
sure gradient across the anastomotic connections. The
associated change of regional blood flow is called
‘steal’ if it results in a decrease in flow and ‘inverse
steal’ if it results in an improvement in flow. Inverse
steal has also been referred to as the Robin Hood syn-
drome (Lassen and Palvolgyi, 1968) by analogy with
the legendary hero who stole from the rich and gave
to the poor. Steals may be symptomatic or asympto-
matic, depending on the magnitude of the flow
changes. It has been suggested that the term ‘steal syn-
drome’ should only be used in the presence of neurolo-
gical symptoms, whereas in the absence of such
symptoms the terms ‘steal phenomenon’ or ‘steal
effect’ would be more appropriate (Von Vollmar,
1971).
Steals are not limited to a particular vascular terri-
tory and may affect both the extra- and intracerebral
circulation (for review see Toole and McGraw, 1975).
Examples of extracerebral steals are the subclavian,
occipital-vertebral and ophthalmic steal syndromes.
Intracerebral steals occur across collateral pathways
of brain, notably the circle of Willis and Heubner’s net-
work of pial anastomoses (see section 4.3, above). The
pathophysiological importance of steal phenomena for
the evolution of brain infarction has been vividly dis-
puted and still remains controversial. Evidence in favor
of intracerebral steal was provided in patients and ani-
mal experiments following ventilation with carbon
dioxide or anesthesia with halothane (Symon, 1968;
Waltz, 1970). The effect was explained by vasodilation
in non-ischemic brain regions, causing a decrease in
local cerebral perfusion pressure and, hence, a reduc-
tion of collateral blood supply to the ischemic territory.
Conversely, an inverse steal was noted during hyperven-
tilation, barbiturate treatment, and occlusion of the exter-
nal carotid artery (Lassen and Palvolgyi, 1968; Abraham
et al., 1971; Branston et al., 1979). The improvement
was related to vasoconstriction in intact brain regions
or—indirectly—to a decrease in intracranial pressure
CEREBRAL BLOOD FLOW AN
causing improvement in cerebral blood perfusion pres-
sure. These findings, however, are at variance with other
observations that did not reveal alterations of blood flow
during either hypo- or hypercapnia (Meyer et al., 1972;
Harrington and DiChiro, 1973; Hanson et al., 1975).
Kogure et al. (1969) and Yamamoto et al. (1971) even
described improvement of blood flow and reduction in
size of the ischemic territory during ventilation with car-
bon dioxide. Steal—if it exists at all—seems to depend
on the individual hemodynamic situation and may lead
to unintended effects when flow in non-ischemic terri-
tories is manipulated. Most authors, therefore, do not
recommend such manipulations for the treatment of
stroke.
4.8. The penumbra concept of ischemia
The intact mammalian brain covers its energy needs
almost exclusively by oxidation of glucose. Opitz
and Schneider (1950) were the first to draw attention
to the fact that an impairment of energy production
induced by a reduction in oxygen supply affects the
energy-consuming processes in a sequential way: first
the functional activity of the brain is impaired, fol-
lowed, at a more severe degree of hypoxia, by the sup-
pression of the metabolic activity required to maintain
its structural integrity. The concept of two different
thresholds of hypoxia for the preservation of func-
tional and structural integrity was later refined by
Symon et al. (1977), who used a model of focal ische-
mia to establish the respective rates of blood flow.
These studies revealed that the EEG and evoked
potentials are disturbed at substantially higher flow
rates than the potassium gradient across the plasma
membranes (Fig. 4.5). Since the preservation of this
gradient is a sign of cell viability, Symon and his col-
leagues postulated that neurons located in the flow
range between ‘electrical’ and ‘membrane’ failure are
functionally silent but structurally intact. In focal
ischemia, this flow range corresponds to a crescent-
shaped region intercalated between the necrotic tissue
and the normal brain; it has been termed ‘penumbra’
by analogy with the partly illuminated area around
the complete shadow of the moon at full eclipse
(Astrup et al., 1981).
The penumbra concept of focal ischemia has been
partly revised over the years (Back, 1998; Sharp
et al., 2000; Touzani et al., 2001) but it remains of cru-
cial importance for the understanding of stroke patho-
physiology because it is the conceptual basis not only
for the progressive evolution of ischemic injury but
also for therapeutic reversal of the acute neurological
symptomatology arising from stroke (for reviews see
Hossmann, 1994; Heiss, 2000; Ginsberg, 2003; Fisher,
THE ISCHEMIC PENUMBRA 75
![Page 10: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/10.jpg)
60
70
50
40SEPEEG
Peri-infarctdepolarizations
Penumbra concept of cerebral ischemia
Penumbra
Infarct core
30
20
10
0%
Cerebral blood flow
Proteinsynthesis
hsp72expression
Glucoseutilization
Lactacidosis
ATPdepletion
Anoxicdepolarization
PE
NU
M
BRA
Fig. 4.5. Thresholds of metabolic and electrophysiological disturbances during graded reduction of cortical blood flow. The
infarct core is the region in which blood flow decreases below the threshold of energy failure, and the penumbra is the region
of reduced blood flow in which energy state is preserved. EEG, electroencephalogram; SEP, somatically evoked potentials.
(Modified from Symon et al., 1977 and Hossmann, 1994.)
76 K.-A. HOSSMANN AND R.J. TRAYSTMAN
2004; Guadagno et al., 2004). Hakim (1987) defined
penumbra as ‘fundamentally reversible’ ischemic injury
but stressed that this reversibility is time-limited. Mem-
ezawa et al. (1992) described penumbra as the differ-
ence between the ischemic infarct developing after 1 h
and 24 h of vascular occlusion. Other characterizations
include the mismatch between magnetic resonance
(MR) perfusion and diffusion imaging (Schlaug et al.,
1999), the mismatch between suppressed protein and
energy metabolism (Mies et al., 1991), the expression
of stress proteins (Kokubo et al., 2003), the preservation
of oxygen extraction or receptor binding (Heiss, 2000),
intermediate staining with neutral red as an indicator
of beginning acidosis (Selman et al., 1987), or the loss
of calmodulin staining (DeGraba et al., 1993) as an indi-
cator of increased intracellular calcium uptake.
The common denominator of these and other defi-
nitions of the ischemic penumbra is the differentiation
between viable and non-viable tissue. Since viability
of brain tissue requires maintenance of energy-
dependent metabolic processes, we propose to define
penumbra as a region of reduced blood flow in which
energy metabolism is preserved (Hossmann, 1994).
4.9. Viability thresholds of ischemia
During the initial few hours of vascular occlusion, dif-
ferent brain functions break down at widely varying
flow levels (for references see Table 4.2). Progressing
from the periphery to the core of the infarct, the most
sensitive parameter is protein synthesis, which is
inhibited by 50% at about 0.55 ml/g/min and comple-
tely suppressed below 0.35 ml/g/min. These values
are clearly above the disturbances of glucose utiliza-
tion and energy metabolism, which begin to evolve
at distinctly lower flow values. Glucose utilization
transiently increases at a flow rate below 0.35 ml/g/
min before it sharply declines below 0.25 ml/g/min.
This range corresponds to the beginning of acidosis
and the beginning of accumulation of lactate. At flow
rates below 0.26 ml/g/min tissue acidosis becomes
very pronounced and phosphocreatine (PCr) and ade-
nosine triphosphate (ATP) begin to decline.
Anoxic depolarization occurs at even lower flow
values. The sodium/potassium ratio of brain tissue
increases at flow values below 0.10–0.15 ml/g/min
and extracellular ion changes occur between 0.06 and
0.15 ml/g/min. At the same threshold extracellular cal-
cium declines because of the opening of calcium chan-
nels. The metabolic and ionic disturbances in the
periphery of focal ischemia thus proceed in the follow-
ing order (Fig. 4.5): initially protein synthesis is inhib-
ited (at a threshold of about 0.55 ml/g/min), followed
by a stimulation of anaerobic glycolysis (below
0.35 ml/g/min), a breakdown of energy state (at about
0.20 ml/g/min), and anoxic depolarization of the cell
membranes (below 0.15 ml/g/min).
As far as functional disturbances are concerned,
the first change is the suppression of EEG activity,
which occurs below 0.25 ml/g/min. Evoked potentials
![Page 11: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/11.jpg)
Table 4.2
Viability thresholds of ischemia
Threshold(ml/g/min
or % of control) Species Anesthesia Reference
Electrical activity
EEG 0.18–0.23 Gerbil Pentobarbital Naritomi et al., 1988
0.20 Macaca Awake Morawetz et al., 1979
0.15–0.20 Human Awake Sharbrough et al., 1973
Evoked potentials 0.15 Baboon a-chloralose Astrup et al., 1977
0.15 Macaca Awake Morawetz et al., 1979
0.20–0.25 Cat Halothane Shimada et al., 1990
Unit activity 0.06–0.22* Cat Nitrous oxide Heiss and Rosner, 1983
Ion and water homoiostasis
Extracellular Kþ 0.06 Baboon a-chloralose Astrup et al., 1977
0.06 Macaca Awake Morawetz et al., 1979
0.15 Rat Halothane Harris and Symon, 1984
Extracellular Ca2þ 0.06–0.09 Baboon a-chloralose Harris et al., 1981
0.15 Rat Halothane Harris and Symon, 1984
Na/K content 0.10–0.15 Cat Pentobarbital Hossmann and Schuier,
1980
Water content 0.10–0.15 Cat Pentobarbital Hossmann and Schuier,
1980
Extracellular space
Impedance 0.25–0.32 Cat Halothane Matsuoka and Hossmann,
1982
DWI 0.41 Rat Halothane Kohno et al., 1995
0.15–0.20 Gerbil Halothane Busza et al., 1992
Spreading depression
Increase duration 40% Rat Halothane Mies, 1997
Neurotransmitter release
Glutamate 0.20 Cat Halothane Shimada et al., 1989
0.20–0.30* Cat Halothane Matsumoto et al., 1993
48% Rat Halothane Takagi et al., 1993
Glycine 0.10–0.30 Cat Halothane Matsumoto et al., 1993
GABA 0.20–0.30 Cat Halothane Matsumoto et al., 1993
Adenosine 0.25 Cat Halothane Matsumoto et al., 1993
Metabolism
Protein synthesis < 0.80 Rat Halothane Jacewicz et al., 1986
0.55{ Rat Halothane Mies et al., 1991
0.49 Rat Halothane Kohno et al., 1994
> 0.40 Gerbil Halothane Xie et al., 1989
mRNA synthesis 0.25–0.30 Rat Halothane Kamiya et al., 2005
Glucose utilization
– Increase 0.35 Gerbil Halothane Paschen et al., 1992
0.20 Rat Halothane Yamamoto et al., 1988
– Decrease 0.25 Gerbil Halothane Paschen et al., 1992
Glucose 0.19–0.23* Rat Halothane Kohno et al., 1995
0.35 Gerbil Halothane Paschen et al., 1992
Lactate 0.30 Baboon a-chloralose Obrenovitch et al., 1988
Acidosis 0.25–0.30 Gerbil Halothane Allen et al., 1993
0.21–0.27 Gerbil Pentobarbital Naritomi et al., 1988
0.40–0.47* Rat Halothane Kohno et al., 1995
0.49 Rat Halothane Yamamoto et al., 1988
0.20–0.30 Baboon a-chloralose Obrenovitch et al., 1988
Phosphocreatine 0.20–0.25 Gerbil Halothane Allen et al., 1993
(Continued)
CEREBRAL BLOOD FLOW AND THE ISCHEMIC PENUMBRA 77
![Page 12: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/12.jpg)
Table 4.2
(Continued)
0.18–0.23 Gerbil Pentobarbital Naritomi et al., 1988
0.20 Baboon a-chloralose Obrenovitch et al., 1988
ATP 0.12–0.14 Gerbil Pentobarbital Naritomi et al., 1988
0.20 Gerbil Halothane Paschen et al., 1992
0.13–0.19* Rat Halothane Kohno et al., 1995
0.19–0.32* Rat Halothane Mies et al., 1991
Inosine, hypoxanthine 0.25 Cat Halothane Matsumoto et al., 1992
Neurological disorder
Hemiparalysis 0.23 Macaca Awake Jones et al., 1981
0.15 Macaca Awake Morawetz et al., 1979
Morphological changes
Neuronal loss < 0.80 Cat Pentobarbital Mies et al., 1983
Infarction
– Permanent ischemia 0.24 Rat Halothane Tamura et al., 1981
0.30 Rat Isoflurane Shen et al., 2003
0.17–0.18 Macaca Awake Jones et al., 1981
0.08 Human Awake Marchal et al., 1999
– Transient ischemia
1 hour < 20% Dog Thiopental Mizoi et al., 1987
2–3 h 0.10–0.12 Macaca Awake Jones et al., 1981
0.12 Macaca Awake Morawetz et al., 1979
3–4 h 0.21–0.25 Rat Halothane Kaplan et al., 1991
DWI: diffusion weighted magnetic resonance imaging.
*Increase of threshold with time.
{No increase with time.
78 K.-A. HOSSMANN AND R.J. TRAYSTMAN
disappear between 0.15 and 0.25 ml/g/min and sponta-
neous unit activity at a mean value of 0.18 ml/100 g/
min. Neurological studies suggest that reversible hemi-
paralysis appears at about 0.23 ml/g/min, followed by
irreversible paralysis below 0.17–0.18 ml/g/min. All
these values are distinctly below the threshold of the
suppression of protein synthesis and even below that
of the beginning activation of anaerobic glycolysis but
they fall into the range of the beginning energy crisis.
This is also true for the release of neurotransmitters
into the extracellular compartment, as measured by
interstitial dialysis techniques. According to these
investigations, both inhibitory and excitatory neuro-
transmitters are released at about 0.20 ml/g/min, with
a possibly slightly higher threshold for glycine, adeno-
sine, and gamma-aminobutyric acid (GABA) than for
glutamate. The release of neurotransmitters is probably
unspecific because other intracellular metabolites are
co-released.
A direct consequence of the metabolic disturbances
associated with focal ischemia is the rise of cell osmol-
ality, which causes an osmotically driven shift of water
from the extra- into the intracellular compartment. The
resulting decline in the fluid volume of the extracellular
compartment can be detected bymeasurements of electri-
cal impedance or by diffusion-weighted imaging (DWI),
both of which are sensitive to cell volume changes. Some
2 h after vascular occlusion the threshold of the begin-
ning rise of electrical impedance is about 0.30 ml/g/min
and that of the rise of signal intensity in DWI is
0.41 ml/g/min. These thresholds are distinctly higher
than the threshold of brain edema—defined as the volu-
metric increase of water content—which is close to
0.10 ml/g/min and corresponds to that of anoxic depolar-
ization. This difference is probably the reason for the fact
that T2-weighted magnetic resonance imaging (MRI),
which detects alterations of tissue water content, is less
sensitive to mild ischemic changes than DWI.
In contrast to the biochemical and functional
changes, which appear shortly after vascular occlu-
sion, histological lesions require some time before
they become visible. The threshold of histological
changes, therefore, depends on both the density and
the duration of flow reduction. Under conditions of
permanent ischemia, the threshold of pan-necrosis is
between 0.17 and 0.24 ml/g/min. When ischemia is
![Page 13: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/13.jpg)
D
reversed within 1–2 h, the tissue is able to survive a
reduction of flow to 0.12 ml/g/min. At flow values
below 0.80 ml/g/min, i.e. far above the threshold of
pan-necrosis, selective neuronal loss may occur. Inter-
estingly, this loss is not threshold-dependent: the flow
rate correlates linearly with the number of surviving
neurons, which suggests a coupled decrease in parallel
with the reduced metabolic requirements of the tissue.
This interpretation is in line with the hypothesis that
the peri-infarct brain tissue suffers pathological
changes that are not directly related to the reduction
of blood flow (see below).
Most of these thresholds have been determined at a
single time point a few hours following the vascular
occlusion. However, studies dealing with the
dynamics of infarct development clearly indicate that
the thresholds may change with time. In rats, the
threshold of ATP depletion increases from 0.13 ml/
g/min after 30 min to 0.19 ml/g/min after 2 h of vas-
cular occlusion and further to 0.23 and 0.32 ml/g/
min after 6 and 12 h respectively. Similarly, the
threshold of glutamate release rises from 0.20 ml/g/
min after 1 h to 0.30 ml/g/min after 6–15 h of ische-
mia. The threshold of the irreversible suppression of
spontaneous neuronal unit activity rises from 0.05 to
0.12 ml/g/min during the initial 2 h of vascular occlu-
sion, and that of the signal intensity in DWI—which
reflects alterations in the intra/extracellular water
compartmentation—from 0.41 to 0.47 ml/g/min
between 30 min and 2 h vascular occlusion. In con-
trast to these gradually progressing threshold values,
the threshold for the suppression of protein synthesis
remains remarkably stable at about 0.55 ml/g/min
during the initial 12 h of ischemia.
4.10. Imaging of the penumbra
Precise visualization of penumbra is of equal impor-
tance for the experimental elucidation of penumbral
pathophysiology as for clinical prognosis and treat-
ment decisions, such as thrombolytic treatment of
stroke (Kidwell et al., 2003). The penumbra can be
imaged either by quantitative mapping of hemody-
namic or metabolic alterations that conform to the
threshold definitions of penumbra (direct mapping) or
by delineating the mismatch between alterations that
affect only the core and others that affect both the core
and the penumbra (mismatch imaging). The reliability
of penumbral imaging depends not only on the defini-
tion of the penumbra but also on the rigor with which
the various penumbral markers have been validated
against independent methods. Other uncertainties of
penumbral imaging arise from the presence of multiple
penumbras for different molecular pathways (Sharp
CEREBRAL BLOOD FLOW AN
et al., 2000), the absence or presence of post-ischemic
recirculation (Jansen et al., 1999), and the time-
dependent dynamics of penumbral viability (Hata
et al., 2000b). Finally, the differentiation between
penumbra and ‘benign’ oligemia that is not at risk of
infarction (Kidwell et al., 2003) is a problem of con-
siderable importance, particularly with regard to treat-
ment decisions. The selection of the appropriate
approach for penumbral imaging, therefore, requires
solid knowledge of the pathophysiological background
on which this approach is based.
4.10.1. Direct penumbral imaging
4.10.1.1. Cerebral blood flow
According to the threshold concept of cerebral ische-
mia, the penumbra can be delineated on quantitative
flow maps by drawing isocontour lines of flow values
that correspond to established thresholds of core and
penumbra (hemodynamic penumbra). Depending on
the definition of penumbra and the time of measure-
ment, flow values of 12–18 ml/100 g/min have been
reported to demarcate the penumbra from the core
region, and of 22–33 ml/100 g/min for the demarcation
between the penumbra and the surrounding intact tis-
sue (Heiss, 2000; Baron, 2001). The most reliable
method for experimental flow mapping is 131I- or14C-iodoantipyrin autoradiography, which provides
highly resolved flow data from cryostat sections of
brain (Fig. 4.1) (Sakurada et al., 1978). Non-invasive
quantitative flow measurements include, among
others, the 15O-H2O intravenous bolus method for
positron emission tomography (PET) scanning (Hers-
covitch et al., 1983), stable xenon computed tomogra-
phy (CT) (Meyer et al., 1981), MR perfusion imaging
using bolus tracking (Ostergaard et al., 1998) or arter-
ial spin labeling (Williams et al., 1992), and perfusion
CT with iodinated contrast material as an intravascular
tracer (Wintermark et al., 2001). Operationally defined
thresholds have also been derived from semi-
quantitative MR bolus track imaging with time-to-
peak values of 4–6 s for the transition between core
and penumbra (Grandin et al., 2002; Sobesky et al.,
2004). Similarly, prolongation of mean transit time or
time-to-peak of the impulse response (Tmax) by more
than 6 s demarcates tissue that progresses to infarction
(Parsons et al., 2001; Rohl et al., 2001). These num-
bers represent statistical values that vary in different
species and that change with duration of ischemia,
temperature, drugs, and the tissue compartment under
investigation. Precise demarcation of penumbra on
flow images, therefore, requires experimental or clini-
cal conditions in which the effects of these variables
are known and well controlled.
THE ISCHEMIC PENUMBRA 79
![Page 14: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/14.jpg)
ND
4.10.1.2. Cerebral blood volume
The reduction of blood supply to brain evokes an autore-
gulatory dilation of resistance vessels that is reflected by
an increase in cerebral blood volume. However, as soon
as blood flow ceases, vessel tone exceeds intraluminal
pressure and cerebral blood volume declines. Penumbra
has, therefore, been associated with an increase of cere-
bral blood volume, as mapped by single-photon emission
CT (SPECT;Watanabe et al., 1999), perfusion CT (Win-
termark et al., 2001) or contrast-enhanced MRI (Oster-
gaard et al., 1998). Operationally, a blood volume
above 2.5 ml/100 g predicts tissue at risk (Wintermark
et al., 2002; Cheung et al., 2003) but the rather crude rela-
tionship between autoregulation and ischemic viability
thresholds precludes accurate delineation of penumbra
based on cerebral blood volume images.
80 K.-A. HOSSMANN A
4.10.1.3. Cerebral metabolic rate of oxygen
and oxygen extraction fraction
The quantitative mapping of cerebral metabolic rate of
oxygen (CMRO2) and oxygen extraction fraction by
PET is widely considered to be the gold standard of
penumbral imaging (Fig. 4.6) (Baron, 1999; Heiss,
Cerebral blood flow
12 hours
Flumazenil distribution Flumazenil
12 hou
12 hours 13 hou
Oxygen extract
Fig. 4.6. Transaxial positron-emission tomography mapping of c
zation, early flumazenil distribution, steady state flumazenil bind
acute onset of stroke. The contour delineating the MR-visible in
extraction fraction and reduced flumazenil binding. (Courtesy of
2000). Changes in oxygen extraction fraction can also
be visualized by near-infrared spectroscopy (Kurth
et al., 2002), MRI using multiecho gradient-echo/
spin-echo sequences (An and Lin, 2002), or the para-
magnetic blood-oxygen-level-dependent (BOLD)
effect (Turner et al., 1991; Crespigny et al., 1992).
As long as oxygen metabolism is preserved, a decline
in blood flow is associated with an increase in blood
oxygen extraction fraction. The increase in oxygen
extraction fraction is, therefore, thought to depict the
still viable penumbra, whereas cessation of CMRO2
is equivalent to cessation of metabolic activity in the
infarct core.
Correlation of oxygen extraction fraction maps with
final infarct size confirms the overall validity of this
approach (Heiss, 2003) but, from a conceptual point
of view, precise delineation of the core and penumbra
cannot be expected. In fact, oxygen extraction fraction
increases not only in the penumbra but also in areas of
‘benign’ oligemia, and CMRO2 ceases before energy
metabolism breaks down (see section 4.9, above).
The apparent borders of both core and penumbra are
therefore shifted outwards towards less severely
injured parts of the ischemic territory. In treatment
R.J. TRAYSTMAN
binding MR imaging
rs 14 days
rs 14 days
ion fraction Glucose utilisation
erebral blood flow, oxygen extraction fraction, glucose utili-
ing, and magnetic resonance (MR) imaging in a patient with
farct co-localizes precisely with the areas of reduced oxygen
W.-D. Heiss.)
![Page 15: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/15.jpg)
D
studies this shift could lead to an overestimate of the
therapeutic effect because undamaged tissue that has
been misinterpreted as penumbra survives even with-
out any therapeutic intervention. However, as other
non-invasive mapping techniques present similar pro-
blems, oxygen extraction fraction and CMRO2 are
widely recommended as methods of choice for penum-
bral imaging.
4.10.1.4. Glucose utilization
With decreasing flow values and beginning tissue
hypoxia, glucose utilization transiently increases to
support anaerobic energy production before it preci-
pitously declines when blood glucose supply ceases
(Paschen et al., 1983; Yao et al., 1995). Glucose uti-
lization can be imaged invasively on histological
brain sections using the 14C-deoxyglucose method.
On such images the ischemic core is detected by
absence of and the penumbra by increase in glucose
utilization. With 18F-2-fluoro-2-deoxy-d-glucose
(FDG) as tracer, glucose metabolism can also be
imaged non-invasively by PET, albeit at lower reso-
lution. It has to be considered, however, that during
ischemia the lumped constant of the operational
equation—on which the calculation of glucose meta-
bolism is based—changes (Greenberg et al., 1992),
and that a steady-state condition for up to 45 min is
required for accurate measurement. Another problem
is the increase of glucose utilization during the pas-
sage of peri-infarct depolarization waves. As these
waves are not confined to the penumbra, they must
be excluded to avoid misinterpretation.
CEREBRAL BLOOD FLOW AN
Blood flow
penumbra
penumbrahsp72 mRNA Protein
core
*
Tiss
Fig. 4.7. Imaging of infarct core and penumbra after middle cere
bolism (ATP) and protein synthesis are outlined and projected on
radiogram of hsp72 (below). Note correspondence of the biochem
of hsp72 upregulation. The area of ‘benign oligemia’ (*) does no
(Data from Mies et al., 1991 and Hata et al., 1998.)
4.10.1.5. Selective gene expression
With increasing use of high-throughput gene profiling
procedures for assessment of differential gene expres-
sion, a steadily increasing number of genes have been
associated with the evolution of penumbral injury
(Lipton, 1999; Read et al., 2001; Carmichael, 2003).
Pictorial evaluations of gene expression can be carried
out on histological sections at both the transcriptional
and translational level, using cDNA in situ hybridiza-
tion or immunohistochemistry respectively. Thus far,
the gene most closely associated with penumbra is
the cytosolic stress gene hsp-70, which is sharply upre-
gulated shortly after onset of ischemia and which is
thought to function as an endogenous protective
mechanism that facilitates renaturation of unfolded
proteins (Kinouchi et al., 1993). In fact, hsp-70 mRNA
expression co-localizes precisely with the mismatch
area between preserved energy and suppressed protein
synthesis that characterizes the biochemically defined
penumbra (Fig. 4.7) (Hata et al., 1998).
The low level of molecular oxygen in the penumbra
also results in upregulation of hypoxia-inducible factor
(HIF)-1 but this response expands more peripherally
into regions with ‘benign’ oligemia (Bergeron et al.,
1999). Genes indirectly linked to ischemia include the
immediate-early genes c-fos, c-jun and junB, whichare activated by peri-infarct depolarization waves (Kies-
sling and Gass, 1994). In accordance with the spread of
these waves, upregulation is not restricted to the penum-
bra but occurs throughout the ipsilateral hemisphere
(Hata et al., 1998). Finally, peri-infarct induction of a
large number of genes has been reported in association
THE ISCHEMIC PENUMBRA 81
synthesis
ue pH ATP
ATP
bral artery occlusion in rat. Areas of disturbed energy meta-
images of blood flow (above) and in situ hybridization auto-
ically characterized penumbra with hypoperfusion and area
t exhibit biochemical changes and is not at risk of infarction.
![Page 16: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/16.jpg)
ND
with edema formation, inflammation, functional distur-
bances, and plasticity, albeit with poor spatial corre-
spondence to the penumbra and at greatly varying
delays after onset of stroke (Lu et al., 2004; MacManus
et al., 2004; Rickhag et al., 2006). They are, therefore, of
limited interest for penumbral mapping.
82 K.-A. HOSSMANN A
4.10.1.6. Tissue water properties
Ischemic injury is intimately associated with disturbed
water homeostasis, some properties of which can be
imaged for direct detection of penumbra. The most
important parameter is the apparent diffusion coeffi-
cient (ADC) of tissue water, which can be measured
by MRI and reflects the viscosity and tortuosity of
intra- and extracellular fluid spaces. At declining flow
values, stimulation of anaerobic glycolysis increases
intracellular osmolality and an osmotically driven
uptake of water, followed—at the threshold of anoxic
depolarization—by a massive shift of electrolytes and
water from the extra- into the intracellular compart-
ment. The resulting decline of ADC has been corre-
lated with blood flow and the associated biochemical
and structural changes of the tissue (Kohno et al.,
1995; Liu et al., 2003; Shen et al., 2004). Hoehn-Berlage
et al., (1995) reported in the rat middle cerebral
artery occlusion model that a decline of ADC to
90% of control correlates with the beginning of
acidosis and a further reduction to 77% with the
breakdown of energy metabolism. The ADC range
between these two values thus delineates the bio-
chemically defined penumbra. Other experimental
observations confirmed that a ‘mild’ decline from
850 to 800 mm2/s corresponds to penumbra whereas
a ‘large’ decline to 650 mm2/s (Miyabe et al., 1996)
or below 550 mm2/s (Kidwell et al., 2003) carries a
high likelihood of irreversible injury. With ongoing
ischemia time the cerebral blood flow threshold for
the ‘large’ reduction increases from 15 to 24 ml/
100 g/min (Kidwell et al., 2003). This is consistent
with the time-dependent increase in the threshold of
energy metabolism (Mies et al., 1991) and reflects
the gradual expansion of the infarct core into the
penumbra (see section 4.9, above).
An inherent problem of ADC mapping is the possi-
ble confusion of alterations caused by ischemia with
peri-infarct spreading depolarizations (Gyngell et al.,
1994). Unless such depolarizations are excluded by
appropriate electrophysiological monitoring, a reliable
differentiation between penumbra and intact tissue is
not possible. Finally, the possibility of a ‘pseudonor-
malization’ of ADC changes must be considered
(Warach et al., 1995). This phenomenon is caused by
accumulation of extracellular water due to vasogenic
brain edema and becomes of pathophysiological
relevance at about 1 week after stroke. However,
at this time, brain infarction is clearly detectable on
T2-weighted MRI, which allows the differentiation
from normal tissue.
Other tissuewater properties that have been associated
with ischemic brain injury and can be detected by MRI
are the increase in proton density and prolongation of
T1 and T2 relaxation times (Baird and Warach, 1998).
As these parameters reflect mainly the infarct core, they
can be used for mismatch imaging (see below) but are
of lesser interest for direct penumbral mapping.
4.10.1.7. Hypoxia marker
A clever approach for direct mapping of the ischemic
penumbra is the use of tracers that are trapped in
viable hypoxic but not in normoxic or necrotic tissue
(Chapman et al., 1983; Rasey et al., 1987). The best
characterized tracer of this kind is 18F-nitromidazol
(F-MISO) (Read et al., 1998; Saita et al., 2004). In
viable tissue F-MISO undergoes enzyme-mediated sin-
gle electron reduction of the nitro group to a free radical
anion. If tissue oxygen content is in the normal range,
the free radical anion is rapidly re-oxidized and cleared
from the tissue but under hypoxic conditions—as in
penumbra—re-oxidation is impaired and the compound
undergoes further reduction to reactive products that
bind to proteins and accumulate intracellularly. As the
first step of this process requires functional nitro-
reductase activity, it is blocked in the non-viable infarct
core. Nitroimidazoles are, therefore, true penumbral
markers that can be used for construction of ‘penum-
bragrams’ that map the spatial extension of penumbra
relative to the final infarct volume (Markus et al., 2004).
Hypoxia-dependent cell binding has also been shown
for iodoazomycin arabinoside (Lythgoe et al., 1997). In
rats with permanent middle cerebral artery occlusion
correlation with blood flow and DWI revealed
enhanced uptake of iodoazomycin arabinoside in
regions of reduced diffusion and perfusion (cerebral
blood flow threshold 34 � 7%) but not in the necrotic
infarct core or in oligemic tissue without disturbances
of water diffusion (Lythgoe et al., 1999). This is different
from the viability marker flumazenil, which binds to
viable tissue irrespective of diffusion properties and
which therefore does not allow differentiation between
penumbra and surrounding intact tissue (see below).
4.10.2. Mismatch imaging
The generation of mismatch maps is an extension of the
threshold concept of brain ischemia, which states that
the flow threshold for penumbral disturbances is higher
than that causing loss of tissue viability in the infarct core.
R.J. TRAYSTMAN
![Page 17: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/17.jpg)
D
The mismatch of images reflecting these disturbances
corresponds to the peri-infarct penumbra. An important
methodological requirement for the generation of such
maps is the acquisition of two different images from the
same brain slice, performed either simultaneously or at
short interval. Various invasive and non-invasive meth-
ods have been proposed for this purpose.
4.10.2.1. ATP mismatches
Under animal experimental conditions the most obvious
biochemical marker of core injury is breakdown of
energy metabolism. Spatially highly resolved images of
tissue energy state are obtained by bioluminescencemap-
ping of the ATP content of cryostat sections prepared
from in situ frozen brains (Kogure and Alonso, 1978).
These images can be matched with maps of alterations
that evolve at higher flow thresholds and include both
core and penumbra (Fig. 4.7). Examples of these are auto-
radiographic images of reduced protein synthesis (Xie
et al., 1989), images of tissue acidosis obtained by fluoro-
scopic (Csiba et al., 1983), autoradiographic (Kobatake
et al., 1984), or histochemical approaches (Van der Veer
et al., 1985), fluoroscopic images of increased nicotina-
mide adenine dinucleotide (NADH) content (Welsh
et al., 1991) and bioluminescence images of increased
lactate (Paschen, 1985). As thresholds of these alterations
differ slightly, the corresponding mismatch maps
also vary, in accordance with the concept of multiple
penumbras (Sharp et al., 2000). Mismatch maps also
change with ongoing time after stroke onset because the
flow threshold for the breakdown of energy metabolism
gradually increases, reflecting expansion of the infarct
core into the peri-infarct penumbra (Mies et al., 1991).
This phenomenon has been best documented by imaging
CEREBRAL BLOOD FLOW AN
ATP bioluminescence
Penumbra
1 hour 3 hours
Protein synthesis
core
Fig. 4.8. Time-dependent expansion of infarct core into penum
Simultaneous imaging of tissue content of ATP and protein synth
ischemia time. (Data from Hata et al., 2000a.)
ATP and cerebral protein synthesis after increasing dura-
tions of experimental middle cerebral artery occlusion
which reveals the gradual disappearance of ATP/cerebral
protein synthesis mismatch within 6–12 h (Hata et al.,
2000a) (Fig. 4.8).
As an alternative to ATP mapping, core tissue can
also be detected by vital stains such as triphenyltetra-
zolium chloride (Hatfield et al., 1991), high-contrast
silver infarct staining (Vogel et al., 1999), or histochem-
ical stainings of the total tissue content of calcium
(Araki et al., 1990) and potassium (Mies et al., 1984),
which change inversely after anoxic depolarization.
However, these alterations require some time for evolu-
tion and are not suited for acute mismatch mapping.
4.10.2.2. Diffusion/perfusion mismatch
A widely accepted although not rigorously validated
signature of irreversible brain injury is the increase in
signal intensity in DWI. The combination of such images
with blood perfusion-weightedMR images (PWI) has led
to the DWI/PWI mismatch concept, which states that the
penumbra is the area of reduced blood flow in which
alterations of water diffusion are absent (Fig. 4.9) (Soren-
sen et al., 1996; Neumann-Haefelin et al., 1999). This
assumption is not undisputed, however (Kidwell et al.,
2003). The apparent diffusion coefficient of tissue water
begins to change before energy metabolism fails, indi-
cating that DWI-detectable areas include parts of
the penumbra (Kohno et al., 1995). The PWI-detectable
area of reduced blood flow, in turn, is not based on
quantitative thresholds and varies with the MR method
used. Hypoperfusion, therefore, includes an undefined
volume of ‘benign’ oligemia in which blood flow is
reduced but still adequate to support metabolic needs of
THE ISCHEMIC PENUMBRA 83
6 hours 1 day 3 days
bra after permanent occlusion of the middle cerebral artery.
esis. Note gradual disappearance of penumbra with ongoing
![Page 18: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/18.jpg)
Core
MCA occlusionControl
ADC
PWI
Penumbra
Core
Fig. 4.9. Magnetic resonance (MR) diffusion-perfusion mismatch for the demarcation of infarct core and penumbra after occlusion
of middle cerebral artery in rat. The mismatch area is highlighted by projecting the outline of the area of disturbed diffusion (as
detected on quantitative ADC maps) on the perfusion-weighted MR image (PWI) (courtesy of L. Olah and M. Hoehn).
84 K.-A. HOSSMANN AND R.J. TRAYSTMAN
the tissue (Parsons et al., 2001). Compared to quantitative
biochemical and hemodynamic maps of the penumbra,
DWI/PWI mismatch is, therefore, only an approximation
of the real situation, with a marked tendency for overesti-
mation of the size of the penumbra (Grandin et al., 2002;
Sobesky et al., 2004). The inclusion of ‘benign’ oligemic
tissue is reflected by the long persistence after stroke onset
of PWI/DWImismatch, which in 44% of stroke patients is
still detected at 18–24 h (Darby et al., 1999). This is much
longer than the experimentally determined survival time of
penumbra and, if misinterpreted as an indication for late
reperfusion therapy, could provoke hemorrhagic and other
complications. However, preliminary data from ongoing
stroke trials designed to confirm clinical utility of the
MR mismatch hypothesis indicate that the demarcation
of penumbra may not be critical because reperfusion ame-
liorates tissue fate irrespective of mismatch (Butcher et al.,
2005; Hacke et al., 2005).
4.10.2.3. Loss of receptor binding
Areliable non-invasive signature of tissue viability is bind-
ing of SPECT- and PET-detectable radioligands, 123I-
iomazenil or 11C-flumazenil, to the benzodiazepine site
of the neuronal GABA receptor (Sette et al., 1993; Al-
Tikriti et al., 1994). In focal ischemia early loss of recep-
tor binding predicts irreversible infarction with high
probability, under both experimental and clinical condi-
tions (Sette et al., 1993; Watanabe et al., 2000; Heiss
et al., 2004). The mismatch between absence of fluma-
zenil binding and areas of either reduced blood flow or
increased oxygen extraction fraction thus provides a
pathophysiologically well supported estimate of
ischemic penumbra (Fig. 4.6). In fact, comparison of
this approach with DWI/PWI mismatch maps revealed
a similar predictive power but a lower incidence of
false-positive results (Heiss et al., 2004), which is read-
ily explained by the more precise detection of the infarct
core using flumazenil (see above). However, as demar-
cation of brain regions with normal and reduced fluma-
zenil binding takes some time, flumazenil imaging is not
suited for fast treatment decisions, as required for the
early initiation of thrombolysis in acute stroke.
4.10.2.4. Other imaging modalities
In principle, any neuroimaging method with different
thresholds for core and penumbra can be combined to pro-
duce penumbral mismatch maps. Examples of such
combinations are MR spectroscopic imaging of N-acety-laspartate (which declines in core due to the loss of irre-
versibly injured neurons) and lactate (which increases
both in core and penumbra) (Barker et al., 1994), or ima-
ging of blood volume (which increases in penumbra due
to autoregulatory vasodilation) in combination with CT
scans or other anatomical images of the structurally
injured infarct core (Grandin et al., 2001; Lee et al., 2002).
An indicator of functional impairment that charac-
terizes the penumbra is the activation of voltage- and
receptor-operated calcium channels. These channels can
be detected in vivo by binding to nimodipine (Hakim
and Hogan, 1991) or dizocilpine (Di and Bullock,
1996). It has not been clearly established, however, if
increased binding co-localizes only with the penumbra
or also with the core of the evolving infarct.
4.10.3. Penumbral imaging during reperfusion
According to the concept of flow-dependent viability
thresholds, penumbral tissue escapes lasting damage
when blood flow is restored to normal levels before
structural changes have evolved (Symon et al., 1977).
![Page 19: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/19.jpg)
D
In fact, prevention of brain infarction after restitution
of blood flow is an important argument for the opera-
tional definition of penumbra (Schlaug et al., 1999;
Shih et al., 2003; Butcher et al., 2005). However, as
the dynamics of post-ischemic reperfusion greatly
vary, tissue may remain at risk of infarction despite
successful recanalization. Obviously, hemodynamic
or flow-related penumbral markers are not suited for
detection of such areas but metabolic or tissue signa-
tures of penumbra, such as the mismatch between
ATP and cerebral protein synthesis, increased glucose
utilization, upregulation of stress genes, or reduced
ADC levels, provide valuable information on the per-
sistence or reversal of penumbral injury (Fig. 4.10)
(Hata et al., 2000b; Izaki et al., 2001; Kokubo et al.,
2003). Penumbral imaging is also of great interest for
predicting delayed ischemic injury. Depending on
ischemic duration and severity, reperfusion may
reverse part of the core injury, as reflected by restora-
tion of energy metabolism or reversal of ‘large’ ADC
reduction (Hata et al., 2000b; Fiehler et al., 2002) but
despite adequate blood circulation these regions
remain at risk of secondary infarction. During the
interval between primary metabolic recovery and sec-
ondary cell death these regions exhibit ATP/cerebral
protein synthesis mismatch, mild ADC decline and
hsp-70 upregulation, by analogy with the ‘true’
ischemic penumbra (Hata et al., 2000b; Olah et al.,
2000; Kokubo et al., 2002). This points to similar
injury mechanisms and suggests that neuroprotective
interventions may be equally effective during reperfu-
sion as during ischemia.
CEREBRAL BLOOD FLOW AN
penumbra
core
release1 hour1 hour
Ischemia
ATP bioluminescence
Protein synthesis
Fig. 4.10. Reversal of focal ischemia after mechanical occlusion
tissue ATP content and protein synthesis. Note rapid restoration
not of protein synthesis. A few hours after restoration of blood flo
protein synthesis did not recover. (Data from Hata et al., 2000b.
4.10.4. Practical recommendations for penumbral
imaging
Important criteria for selection of the most appropriate
approach for penumbral imaging are the choice
between invasive or non-invasive methods on the one
hand and between direct and mismatch imaging on
the other. For animal experimental purposes, in which
brain tissue can be dissected at the end of experiment,
ATP/cerebral protein synthesis or ATP/pH mismatch
imaging provides spatially highly resolved penumbra
maps that are sharply demarcated from both the
ischemic core and the surrounding intact tissue,
including areas of ‘benign’ oligemia in which adequate
oxygen delivery is maintained (Mies et al., 1991; Hos-
smann, 1994). ATP/cerebral protein synthesis or ATP/
pH mismatch maps can be generated without prior
knowledge of the particular viability thresholds, as
required for quantitative blood flow or ADC maps,
and they identify tissue at risk both during ischemia
and reperfusion. Obviously, this approach is restricted
to animal experiments but if with improving sensitivity
of MR spectroscopy non-invasive phosphorus imaging
should become feasible, ATP mismatch maps could be
acquired in patients and would serve as reliable stan-
dards for validation of other penumbral imaging mod-
alities.
Under clinical conditions and for animal experiments
that require repeated measurements, the two methods of
choice are DWI/PWI mismatch imaging using MR
technology (Abe et al., 2003; Warach, 2003) and ima-
ging of blood flow, oxygen consumption, oxygen
THE ISCHEMIC PENUMBRA 85
3 hours 6 hours 3 days
Reperfusion
of the middle cerebral artery for 1 h. Simultaneous imaging of
of energy metabolism after release of vascular occlusion but
w, energy metabolism secondarily fails in the areas in which
)
![Page 20: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/20.jpg)
ND R.J. TRAYSTMAN
extraction fraction, and flumazenil binding using PET
(Baron, 1999; Heiss, 2000). PET studies are quantita-
tive and therefore considered by many to be the gold
standard for penumbral imaging but they require expen-
sive instrumentation, prior knowledge of individual via-
bility thresholds (for quantitative cerebral blood flow
and CMRO2 maps), and the manifestation of structural
injury (for flumazenil maps) to allow precise demarca-
tion from the core and the surrounding intact tissue.
DWI/PWI mismatch imaging, in contrast, is readily per-
formed with most clinical MR scanners, does not
require prior knowledge of individual viability thresh-
olds, does not have to await structural manifestation of
injury, and provides excellent spatial resolution even
in small-animal brains. However, uncertainties about
the demarcation between penumbra and core on the
one hand and between penumbra and ‘benign’ oligemia
on the other preclude precise spatial allocations. Direct
comparisons of PET and MRI data in the same subject
demonstrated that the predictive power for the evolution
of brain infarction is similar for both methods (Heiss
et al., 2004) but, as MRI provides a less precise alloca-
tion of penumbra, PET is the preferred method for basic
pathophysiological studies. Neither, however, matches
the spatial resolution and pathophysiological unambigu-
ousness of invasive metabolic imaging techniques such
as ATP/cerebral protein synthesis mismatch mapping.
Validation of new penumbral mapping proced-
ures should, therefore, be based on this or similar
approaches.
References
Abe O, Aoki S, Shirouzu I, et al. (2003). MR imaging of
ischemic penumbra. Eur J Radiol 46: 67–78.
Abraham J, Shetty G, Chandy J (1971). Preliminary observa-
tion on the hemodynamics of the internal carotid artery
following bilateral external carotid ligation in the monkey.
J Neurosurg 35: 192–196.
Allen KL, Busza AL, Proctor E, et al. (1993). Controllable
graded cerebral ischaemia in the gerbil—studies of cerebral
blood flow and energy metabolism by hydrogen clearance
and P-31 NMR spectroscopy. NMR Biomed 6: 181–186.
Al-Tikriti MS, Dey HM, Zoghbi SS, et al. (1994). Dual-isotope
autoradiographic measurement of regional blood flow and
benzodiazepine receptor availability following unilateralmid-
dle cerebral artery occlusion. Eur J Nucl Med 21: 196–202.
Ames A, Wright RL, Kowada M, et al. (1968). Cerebral
ischemia II. The no-reflow phenomenon. Am J Pathol
52: 437–453.
Andersen F, Watanabe H, Bjarkam C, et al. (2005). Pig brain
stereotaxic standard space: mapping of cerebral blood
flow normative values and effect of MPTP-lesioning.
Brain Res Bull 66: 17–29.
An HY, Lin WL (2002). Cerebral oxygen extraction fraction
and cerebral venous blood volume measurements using
86 K.-A. HOSSMANN A
MRI: effects of magnetic field variation. Magn Reson
Med 47: 958–966.
Araki T, Inoue T, Kato H, et al. (1990). Neuronal damage
and calcium accumulation following transient cerebral
ischemia in the rat. Mol Chem Neuropathol 12: 203–213.
Astrup J, Symon L, Branston NM, et al. (1977). Cortical
evoked potential and extracellular Kþ and Hþ at critical
levels of brain ischemia. Stroke 8: 51–57.
Astrup J, Symon L, Siesjo BK (1981). Thresholds in cerebral
ischemia—the ischemic penumbra. Stroke 12: 723–725.
Back T (1998). Pathophysiology of the ischemic penum-
bra—revision of a concept. Cell Mol Neurobiol 18:
621–638.
Baird AE, Warach S (1998). Magnetic resonance imaging of
acute stroke. J Cereb Blood Flow Metab 18: 583–609.
Barker PB, Gillard JH, Zijl PCMV, et al. (1994). Acute
stroke: evaluation with serial proton MR spectroscopic
imaging. Radiology 192: 723–732.
Baron JC (1999). Mapping the ischaemic penumbra with
PET: implications for acute stroke treatment. Cerebrovasc
Dis 9: 193–201.
Baron JC (2001). Perfusion thresholds in human cerebral
ischemia: Historical perspective and therapeutic implica-
tions. Cerebrovasc Dis 11: 2–8.
Bergeron M, Yu AY, Solway KE, et al. (1999). Induction of
hypoxia-inducible factor-1 (HIF-1) and its target genes
following focal ischaemia in rat brain. Eur J Neurosci
11: 4159–4170.
Branston NM, Hope DT, Symon L (1979). Barbiturates in
focal ischemia of primate cortex: effects on blood flow
distribution, evoked potential and extracellular potassium.
Stroke 10: 647–653.
Brody H (1955). Organization of the cerebral cortex III.
A study of aging in the human cerebral cortex. J Comp
Neurol 102: 511–516.
Busch HJ, Buschmann IR, Mies G, et al. (2003). Arteriogen-
esis in hypoperfused rat brain. J Cereb Blood Flow Metab
23: 621–628.
Busza AL, Allen KL, King MD, et al. (1992). Can diffusion-
weighted magnetic-resonance-imaging detect critical cere-
bral blood-flow thresholds and energy failure during
cerebral-ischemia? Eur J Neurosci 1992: 242.
Butcher KS, Parsons M, MacGregor L, et al. (2005). Refining
the perfusion-diffusion mismatch hypothesis. Stroke 36:
1153–1159.
Carmichael ST (2003). Gene expression changes after focal
stroke, traumatic brain and spinal cord injuries. Curr Opin
Neurol 16: 699–704.
Cenic A, Craen RA, Howard-Lech VL, et al. (2000). Cerebral
blood volume and blood flow at varying arterial carbon
dioxide tension levels in rabbits during propofol anesthe-
sia. Anesth Analg 90: 1376–1383.
Chapman JD, Baer K, Lee J (1983). Characteristics of the
metabolism-induced binding of misonidazole to hypoxic
mammalian cells. Cancer Res 43: 1523–1528.
Cheung RTF, Cheng PW, Lui WM, et al. (2003). Visualiza-
tion of ischaemic penumbra using a computed tomography
perfusion method. Cerebrovasc Dis 15: 182–187.
![Page 21: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/21.jpg)
CEREBRAL BLOOD FLOW AND THE ISCHEMIC PENUMBRA 87
Cohen PJ, Alexander SC, Smith TC, et al. (1967). Effects of
hypoxia and normocarbia on cerebral blood flow and meta-
bolism in conscious man. J Appl Physiol 23: 183–189.
Coyle P (1982). Middle cerebral artery occlusion in the
young rat. Stroke 13: 855–859.
Coyle P, Jokelainen PT (1983). Differential outcome to mid-
dle cerebral artery occlusion in spontaneously hyperten-
sive stroke-prone rats (SHRSP) and Wistar Kyoto
(WKY) rats. Stroke 14: 605–611.
Crespigny AJD, Wendland MF, Derugin N, et al.
(1992). Real-time observation of transient focal ischemia
and hyperemia in cat brain. Magn Reson Med 27:
391–397.
Crowell RM, Olsson Y (1972). Impaired microvascular fill-
ing after focal cerebral ischemia in monkeys. J Neurosurg
36: 303–309.
Csete K, Papp JG (2000). Effects of moxonidine on corticocer-
ebral blood flow under normal and ischemic conditions in
conscious rabbits. J Cardiovasc Pharmacol 35: 417–421.
Csiba L, Paschen W, Hossmann K-A (1983). A topographic
quantitative method for measuring brain tissue pH under
physiological and pathophysiological conditions. Brain
Res 289: 334–337.
Darby DG, Barber PA, Gerraty RP, et al. (1999). Pathophy-
siological topography of acute ischemia by combined
diffusion-weighted and perfusion MRI. Stroke 30:
2043–2052.
Date H, Hossmann K-A, Shima T (1984). Effect of middle
cerebral artery compression on pial artery pressure, blood
flow, and electrophysiological function of cerebral cortex
of cat. J Cereb Blood Flow Metab 4: 593–598.
DeGraba TJ, Ostrow PT, Grotta JC (1993). Threshold of cal-
cium disturbances after focal cerebral ischemia in rats—
Implications of the window of therapeutic opportunity.
Stroke 24: 1212–1217.
Delp MD, Armstrong RB, Godfrey DA, et al. (2001). Exer-
cise increases blood flow to locomotor, vestibular, cardior-
espiratory and visual regions of the brain in miniature
swine. J Physiol 533: 849–859.
Dintenfass L (1967). Inversion of the Fahreus-Lindqvist phe-
nomenon in blood flow through capillaries of diminishing
radius. Nature 215: 1099–1100.
Di X, Bullock R (1996). Effect of the novel high-affinity
glycine-site N-methyl-D-aspartate antagonist ACEA-1021
on I-125-MK-801 binding after subdural hematoma in
the rat—an in vivo autoradiographic study. J Neurosurg
85: 655–661.
Fahreus R, Lindqvist T (1931). The viscosity of blood in nar-
row capillary tubes. Am J Physiol 96: 562–568.
Fiehler J, Foth M, Kucinski T, et al. (2002). Severe ADC
decreases do not predict irreversible tissue damage in
humans. Stroke 33: 79–86.
Fisher M (2004). The ischemic penumbra: Identification, evo-
lution and treatment concepts. Cerebrovasc Dis 17: 1–6.
Foley LM, Hitchens TK, Kochanek PM, et al. (2005). Murine
orthostatic response during prolonged vertical studies:
effect on cerebral blood flow measured by arterial spin-
labeled MRI. Magn Reson Med 54: 798–806.
Fumagalli M, Mosca F, Moos Knudsen G, et al. (2004). A
newborn rat model for the study of cerebral hemodynamics
by near-infrared spectroscopy and laser-Doppler flowmetry
in the immature brain. Biol Neonate 85: 112–120.
Gaethgens P, Albrecht KH, Kreutz F (1978). Fahreus effect
and cell screening during tube flow of human blood I.
Effect of variation of flow rate. Biorheology 15: 147–154.
Gillian LA (1971). General principles of the arterial blood
vessel patterns to the brain. American Neurological Asso-
ciation 82: 65–68.
Ginsberg MD (2003). Adventures in the pathophysiology of
brain ischemia: penumbra, gene expression, neuroprotection.
The 2002 Thomas Willis Lecture. Stroke 34: 214–223.
Gleason CA, Robinson R, Harris AP, et al. (2002). Cerebro-
vascular effects of intravenous dopamine infusions in fetal
sheep. J Appl Physiol 92: 717–724.
Gogolak I, Gotoh F, Tomita M, et al. (1985). No intracereb-
ral steal phenomenon in the ischemic brain following
papaverine administration. Stroke 16: 114–117.
Grandin CB, Duprez TP, Smith AM, et al. (2001). Usefulness
of magnetic resonance-derived quantitative measurements
of cerebral blood flow and volume in prediction of infarct
growth in hyperacute stroke. Stroke 32: 1147–1153.
Grandin CB, Duprez TP, Oppenheim C, et al. (2002). Which
MR-derived perfusion parameters are the best predictors
of infarct growth in hyperacute stroke? Comparative study
between relative and quantitative measurements. Radiol-
ogy 223: 361–370.
Greenberg JH, Hamar J, Welsh FA, et al. (1992). Effect of
ischemia and reperfusion on lambda of the lumped con-
stant of the [14C]deoxyglucose technique. J Cereb Blood
Flow Metab 12: 70–77.
Gross PM, Marcus ML, Heistad DD (1980). Regional distri-
bution of cerebral blood flow during exercise in dogs.
J Appl Physiol 48: 213–217.
Grotta J, Ackerman R, Correia J, et al. (1982). Whole blood
viscosity parameters and cerebral blood flow. Stroke 13:
296–301.
Guadagno JV, Donnan GA, Markus R, et al. (2004). Imaging
the ischaemic penumbra. Curr Opin Neurol 17: 61–67.
Gyngell ML, Back T, Hoehn-Berlage M, et al. (1994). Tran-
sient cell depolarization after permanent middle cerebral
artery occlusion: an observation by diffusion-weighted
MRI and localized 1H-MRS. Magn Reson Med 31:
337–341.
Hacke W, Albers G, Al-Rawi Y, et al. (2005). The Desmote-
plase in Acute Ischemic Stroke Trial (DIAS)—A phase II
MRI-based 9-hour window acute stroke thrombolysis trial
with intravenous desmoteplase. Stroke 36: 66–73.
Hakim AM (1987). The cerebral ischemic penumbra. Can J
Neurol Sci 14: 557–559.
Hakim AM, Hogan MJ (1991). In vivo binding of nimodi-
pine in the brain: I. The effect of focal cerebral ischemia.
J Cereb Blood Flow Metab 11: 762–770.
Hallenbeck JM, Dutka AJ, Tanashima T, et al. (1986). Poly-
morphonuclear leukocyte accumulation in brain regions
with low blood flow during the early postischemic period.
Stroke 17: 246–253.
![Page 22: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/22.jpg)
88 K.-A. HOSSMANN AND R.J. TRAYSTMAN
Hanson EJ, Anderson RE, Sundt TM (1975). Influence of
cerebral vasoconstricting and vasodilating agents on blood
flow in regions of focal ischemia. Stroke 6: 642–648.
Harper AM (1966). Autoregulation of cerebral blood flow:
influence of the arterial blood pressure on the blood flow
through the cerebral cortex. J Neurol Neurosurg Psychia-
try 29: 398–403.
Harper AM, Glass HI (1965). Effect of alterations in the
arterial carbon dioxide tension on the blood flow through
the cerebral cortex at normal and low arterial pressures.
J Neurol Neurosurg Psychiatry 28: 449–452.
Harrington T, DiChiro G (1973). Effect of hypocarbia and
hypercarbia in experimental brain infarction. A microan-
giographic study in the monkey. Neurology 23: 294–299.
Harris RJ, Symon L (1984). Extracellular pH, potassium, and
calcium activities in progressive ischaemia of rat cortex.
J Cereb Blood Flow Metab 4: 178–186.
Harris RJ, Symon L, Branston NM, et al. (1981). Changes
in extracellular calcium activity in cerebral ischaemia.
J Cereb Blood Flow Metab 1: 203–209.
Hata R, Mies G, Wiessner C, et al. (1998). Differential
expression of c-fos and hsp72 mRNA in focal cerebral
ischemia of mice. Neuroreport 9: 27–32.
Hata R, Maeda K, Hermann D, et al. (2000a). Dynamics of
regional brain metabolism and gene expression after mid-
dle cerebral artery occlusion in mice. J Cereb Blood Flow
Metab 20: 306–315.
Hata R, Maeda K, Hermann D, et al. (2000b). Evolution of
brain infarction after transient focal cerebral ischemia in
mice. J Cereb Blood Flow Metab 20: 937–946.
Hatfield RH, Mendelow AD, Perry RH, et al. (1991). Triphe-
nyltetrazolium chloride (TTC) as a marker for ischaemic
changes in rat brain following permanent middle cerebral
artery occlusion. Neuropathol Appl Neurobiol 17: 61–67.
Heiss W-D (2000). Ischemic penumbra: evidence from func-
tional imaging in man. J Cereb Blood Flow Metab 20:
1276–1293.
Heiss W-D (2003). Best measure of ischemic penumbra:
positron emission tomography. Stroke 34: 2534–2535.
Heiss W-D, Rosner G (1983). Functional recovery of cortical
neurons as related to degree and duration of ischemia. Ann
Neurol 14: 294–301.
HeissW-D, Sobesky J, Smekal UV, et al. (2004). Probability of
cortical infarction predicted by flumazenil binding and
diffusion-weighted imaging signal intensity—a comparative
positron emission tomography/magnetic resonance imaging
study in early ischemic stroke. Stroke 35: 1892–1898.
Herscovitch P, Markham J, Raichle ME (1983). Brain blood
flow measured with intravenous H215O. I. Theory and
error analysis. J Nucl Med 24: 782–789.
Hoedt-Rasmussen K, Skinhoj O, Paulson J, et al. (1967).
Regional cerebral blood flow in acute apoplexy. The ‘luxury
perfusion syndrome’ of brain tissue. Arch Neurol 17:
271–281.
Hoehn-Berlage M, Norris DG, Kohno K, et al. (1995). Evolu-
tion of regional changes in apparent diffusion coefficient
during focal ischemia of rat brain: the relationship of
quantitative diffusion NMR imaging to reduction in cere-
bral blood flow and metabolic disturbances. J Cereb Blood
Flow Metab 15: 1002–1011.
Horinaka N, Artz N, Jehle J, et al. (1997). Examination of
potential mechanisms in the enhancement of cerebral
blood flow by hypoglycemia and pharmacological
doses of deoxyglucose. J Cereb Blood Flow Metab
17: 54–63.
Hossmann K-A (1993). Collateral circulation of the brain.
In: W Schaper, J Schaper (Eds.), Collateral Circulation:
Heart, Brain, Kidney, Limbs, Kluwer Academic Publish-
ers, Boston, MA, pp. 291–315.
Hossmann K-A (1994). Viability thresholds and the penum-
bra of focal ischemia. Ann Neurol 36: 557–565.
Hossmann K-A (1997). Reperfusion of the brain after global
ischemia—hemodynamic disturbances. Shock 8: 95–101.
Hossmann K-A (1998). Experimental models for the investi-
gation of brain ischemia. Cardiovasc Res 39: 106–120.
Hossmann K-A, Schuier FJ (1980). Experimental brain
infarcts in cats I. Pathophysiological observations. Stroke
11: 583–592.
Hudetz AG, Halsey JH, Horton CR, et al. (1982). Mathemati-
cal simulation of cerebral blood flow in focal ischemia.
Stroke 13: 693–700.
Iadecola C (1998). Cerebral circulatory dysregulation in
ischemia. In: M Ginsberg, J Bogousslavsky (Eds.), Cere-
brovascular Diseases; Pathophysiology, Diagnosis and
Management, Vol. 1. Blackwell Scientific, Oxford, pp.
319–357.
Ichord RN, Johnston MV, Traystman RJ (2001). MK801
decreases glutamate release and oxidative metabolism dur-
ing hypoglycemic coma in piglets. Brain Res Dev Brain
Res 128: 139–148.
Ito U, Ohno K, Yamaguchi T, et al. (1980). Transient
appearance of ‘no-reflow’ phenomenon in Mongolian ger-
bils. Stroke 11: 517–521.
Izaki K, Kinouchi H, Watanabe K, et al. (2001). Induction of
mitochondrial heat shock protein 60 and 10 mRNAs fol-
lowing transient focal cerebral ischemia in the rat. Mol
Brain Res 88: 14–25.
Jacewicz M, Kiessling M, Pulsinelli WA (1986). Selective
gene expression in focal cerebral ischemia. J Cereb Blood
Flow Metab 6: 263–272.
Jansen O, Schellinger P, Fiebach J, et al. (1999). Early reca-
nalisation in acute ischaemic stroke saves tissue at risk
defined by MRI. Lancet 353: 2036–2037.
Jones MD Jr, Traystman RJ (1984). Cerebral oxygenation of
the fetus, newborn, and adult. Semin Perinatol 8: 205–216.
Jones TH, Morawetz RB, Crowell RM, et al. (1981). Thresh-
olds of focal cerebral ischemia in awake monkeys. J Neu-
rosurg 54: 773–782.
Joshi S, Hartl R, Sun LS, et al. (2003). Despite in vitro increase
in cyclic guanosine monophosphate concentrations, intracar-
otid nitroprusside fails to augment cerebral blood flow of
healthy baboons. Anesthesiology 98: 412–419.
Kamiya T, Jacewicz M, Nowak TS, et al. (2005). Cerebral
blood flow thresholds for mRNA synthesis after focal
ischemia and the effect of MK-801. Stroke 36:
2463–2467.
![Page 23: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/23.jpg)
CEREBRAL BLOOD FLOW AND THE ISCHEMIC PENUMBRA 89
Kaplan B, Brint S, Tanabe J, et al. (1991). Temporal thresh-
olds for neocortical infarction in rats subjected to reversi-
ble focal cerebral ischemia. Stroke 22: 1032–1039.
Kaufman JA, Phillips-Conroy JE, Black KJ, et al. (2003).
Asymmetric regional cerebral blood flow in sedated baboons
measured by positron emission tomography (PET). Am
J Phys Anthropol 121: 369–377.
Kellie G (1824). An account with some reflections on the
pathology of the brain. Edin Med Chir Soc Trans 1:
123–169.
Kennedy C, Sokoloff L (1957). An adaptation of the nitrous
oxide method to the study of the cerebral circulation in
children: Normal values for cerebral blood flow and cere-
bral metabolic rate in childhood. J Clin Invest 36:
1130–1137.
Kidwell CS, Alger JR, Saver JL (2003). Beyond mismatch:
Evolving paradigms in imaging the ischemic penumbra
with multimodal magnetic resonance imaging. Stroke 34:
2729–2735.
Kiessling M, Gass P (1994). Stimulus-transcription coupling
in focal cerebral ischemia. Brain Pathol 4: 77–83.
Kinouchi H, Sharp FR, Koistinaho J, et al. (1993). Induction
of heat shock hsp70 messenger RNA and HSP70-kda pro-
tein in neurons in the penumbra following focal cerebral
ischemia in the rat. Brain Res 619: 334–338.
Kobatake K, Sako K, Izawa M, Yamamoto Y, Hakim A
(1984). Autoradiographic determination of brain pH fol-
lowing middle cerebral artery occlusion in the rat. Stroke
15: 540–547.
Kogure K, Alonso OF (1978). A pictorial representation of
endogenous brain ATP by a bioluminescent method. Brain
Res 154: 273–284.
Kogure K, Fujishima M, Scheinberg P, et al. (1969). Effects
of changes in carbon dioxide pressure and arterial pressure
on blood flow in ischemic regions of the brain in dogs.
Circ Res 24: 557–565.
Kohno K, Mies G, Djuricic B, et al. (1994). NBQX reduces
threshold of protein synthesis inhibition in focal ischaemia
in rats. Neuroreport 5: 2342–2344.
Kohno K, Hoehn-Berlage M, Mies G, et al. (1995). Relation-
ship between diffusion-weighted MR images, cerebral
blood flow, and energy state in experimental brain infarc-
tion. Magn Reson Imaging 13: 73–80.
Kokubo Y, Matson GB, Liu JL, et al. (2002). Correlation
between changes in apparent diffusion coefficient and
induction of heat shock protein, cell-specific injury marker
expression, and protein synthesis reduction on diffusion-
weighted magnetic resonance images after temporary
focal cerebral ischemia in rats. J Neurosurg 96:
1084–1093.
Kokubo Y, Liu JL, Rajdev S, et al. (2003). Differential cere-
bral protein synthesis and heat shock protein 70 expression
in the core and penumbra of rat brain after transient focal
ischemia. Neurosurgery 53: 186–190.
Kurth CD, Levy WJ, McCann J (2002). Near-infrared spec-
troscopy cerebral oxygen saturation thresholds for
hypoxia–ischemia in piglets. J Cereb Blood Flow Metab
22: 335–341.
Lambertsen CJ, Dough RH, Cooper DY, et al. (1953). Oxy-
gen toxicity: effects in man of oxygen inhalation at 1 and
3.5 atmospheres upon blood gas transport, cerebral circu-
lation and cerebral metabolism. J Appl Physiol 5:
471–486.
Landau WM, Freygang WH Jr, Roland LP, et al. (1955). The
local circulation of the living brain; values in the una-
nesthetized and anesthetized cat. Trans Am Neurol Assoc
80: 125–129.
Lassen NA, Palvolgyi R (1968). Cerebral steal during hyper-
capnia and the inverse reaction during hypocapnia
observed by the 133 Xenon technique in man. Scand J
Clin Lab Invest Suppl 102: XIII D.
Law I, Iida H, Holm S, et al. (2000). Quantitation of regional
cerebral blood flow corrected for partial volume effect
using O-15 water and PET. II. Normal values and gray
matter blood flow response to visual activation. J Cereb
Blood Flow Metab 20: 1252–1263.
Lee SK, Kim DI, Jeong EK, et al. (2002). Temporal changes
in reversible cerebral ischemia on perfusion- and
diffusion-weighted magnetic resonance imaging: the value
of relative cerebral blood volume maps. Neuroradiology
44: 103–108.
Levy DE, Uitert RLV, Pike CL (1979). Delayed postis-
chemic hypoperfusion: a potentially damaging conse-
quence of stroke. Neurology 29: 1245–1252.
Lipton P (1999). Ischemic cell death in brain neurons. Phy-
siol Rev 79: 1431–1568.
Little JR, Kerr FWL, Sundt TM (1975). Microcirculatory
obstruction in focal cerebral ischemia. Relationship to
neuronal alterations. Mayo Clin Proc 50: 264–270.
Littleton-Kearney MT, Agnew DM, Traystman RJ, et al.
(2000). Effects of estrogen on cerebral blood flow and
pial microvasculature in rabbits. Am J Physiol Heart Circ
Physiol 279: H1208–H1214.
Liu Y, Karonen JO, Vanninen RL, et al. (2003). Detecting
the subregion proceeding to infarction in hypoperfused
cerebral tissue: a study with diffusion and perfusion
weighted MRI. Neuroradiology 45: 345–351.
Lu XCM, Williams AJ, Yao C, et al. (2004). Microarray ana-
lysis of acute and delayed gene expression profile in rats
after focal ischemic brain injury and reperfusion. J Neu-
rosci Res 77: 843–857.
Lythgoe MF, Williams SR, Wiebe LI, et al. (1997). Autora-
diographic imaging of cerebral ischaemia using a combi-
nation of blood flow and hypoxic markers in an animal
model. Eur J Nucl Med 24: 16–20.
Lythgoe MF, Williams SR, Busza AL, et al. (1999). The
relationship between magnetic resonance diffusion ima-
ging and autoradiographic markers of cerebral blood flow
and hypoxia in an animal stroke model. Magn Reson Med
41: 706–714.
McDowall DG (1966). Interrelationships between blood oxy-
gen tensions and cerebral blood flow. Int Anesthesiol Clin
4: 205–219.
Macfarlane R, Moskowitz MA, Tasdemiroglu E, et al.
(1991). Postischemic cerebral blood flow and neuroeffec-
tor mechanisms. Blood Vessels 28: 46–51.
![Page 24: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/24.jpg)
90 K.-A. HOSSMANN AND R.J. TRAYSTMAN
MacManus JP, Graber T, Luebbert C, et al. (2004). Transla-
tion-state analysis of gene expression in mouse brain after
focal ischemia. J Cereb Blood Flow Metab 24: 657–667.
McPherson RW, Koehler RC, Traystman RJ (1988). Effect
of jugular venous pressure on cerebral autoregulation in
dogs. Am J Physiol 255: H1516–H1524.
Marchal G, Benali K, Iglesias S, et al. (1999). Voxel-based
mapping of irreversible ischaemic damage with PET in
acute stroke. Brain 122: 2387–2400.
Markus R, Donnan G, Kazui S, et al. (2004). Penumbral
topography in human stroke: methodology and validation
of the ‘Penumbragram’. Neuroimage 21: 1252–1259.
Matsumoto K, Graf R, Rosner G, et al. (1992). Flow thresh-
olds for extracellular purine catabolite elevation in cat
focal ischemia. Brain Res 579: 309–314.
MatsumotoK,Graf R, RosnerG, et al. (1993). Elevation of neu-
roactive substances in the cortex of cats during prolonged
focal ischemia. J Cereb Blood Flow Metab 13: 586–594.
Matsuoka Y, Hossmann K-A (1982). Cortical impedance and
extracellular volume changes following middle cerebral
artery occlusion in cats. J Cereb Blood Flow Metab 2:
466–474.
Meltzer CC, Cantwell MN, Greer PJ, et al. (2000). Does cer-
ebral blood flow decline in healthy aging? A PET study
with partial-volume correction. J Nucl Med 41:
1842–1848.
Memezawa H, Smith M-L, Siesjo BK (1992). Penumbral tis-
sues salvaged by reperfusion following middle cerebral
artery occlusion in rats. Stroke 23: 552–559.
Meyer JS, Denny-Brown D (1957). The cerebral collateral
circulation. 1. Factors influencing collateral blood flow.
Neurology 7: 447–458.
Meyer JS, Fukuuchi Y, Shimazu K, et al. (1972). Abnormal
hemispheric blood flow and metabolism in cerebrovascu-
lar disease. II. Therapeutic trials with 5 per cent CO2 inha-
lation, hyperventilation and intravenous infusion of
THAM and mannitol. Stroke 3: 157–167.
Meyer JS, Hayman LA, Yamamoto M, et al. (1980). Local
cerebral blood flow measured by CT after stable xenon
inhalation. AJR Am J Roentgenol 135: 239–251.
Meyer JS, Hayman LA, Amano T, et al. (1981). Mapping
local blood flow of human brain by CT scanning during
stable xenon inhalation. Stroke 12: 426–436.
Michenfelder JD, Milde JH (1975). Influence of anesthetics
on metabolic, functional and pathological responses to
regional cerebral ischemia. Stroke 6: 405–410.
Mies G (1997). Blood flow dependent duration of cortical
depolarizations in the periphery of focal ischemia of rat
brain. Neurosci Lett 221: 165–168.
Mies G, Auer LM, Ebhardt G, et al. (1983). Flow and neuro-
nal density in tissue surrounding chronic infarction. Stroke
14: 22–27.
Mies G, Kloiber O, Drewes L, et al. (1984). Cerebral blood
flow and regional potassium distribution during focal
ischemia of gerbil brain. Ann Neurol 16: 232–237.
Mies G, Paschen W, Hossmann K-A (1990). Cerebral blood
flow, glucose utilization, regional glucose, and ATP con-
tent during the maturation period of delayed ischemic
injury in gerbil brain. J Cereb Blood Flow Metab 10:
638–645.
Mies G, Ishimaru S, Xie Y, et al. (1991). Ischemic thresholds
of cerebral protein synthesis and energy state following
middle cerebral artery occlusion in rat. J Cereb Blood
Flow Metab 11: 753–761.
Miller JD, Garibi J, North JB, et al. (1975). Effects of
increased arterial pressure on blood flow in the damaged
brain. J Neurol Neurosurg Psychiatry 38: 657–665.
Miyabe M, Jones MD Jr, Koehler RC, et al. (1989). Chemo-
denervation does not alter cerebrovascular response to
hypoxic hypoxia. Am J Physiol 257: H1413–H1418.
Miyabe M, Mori S, Van Zijl PCM, et al. (1996). Correlation
of the average water diffusion constant with cerebral
blood flow and ischemic damage after transient middle
cerebral artery occlusion in cats. J Cereb Blood Flow
Metab 16: 881–891.
Mizoi K, Suzuki J, Abiko H, et al. (1987). Experimental
study on the reversibility of cerebral ischemia. Residual
blood flow and duration of ischemia. Acta Neurochir
(Wien) 88: 126–134.
Monro A (1783). Observations on the Structure and Function
of the Nervous System Creech, Edinburgh.
Morawetz RB, Crowell RH, DeGirolami U, et al. (1979).
Regional cerebral blood flow thresholds during cerebral
ischemia. Fed Proc 38: 2493–2494.
Mujsce DJ, Christensen MA, Vannucci RC (1989). Regional
cerebral blood flow and glucose utilization during hypo-
glycemia in newborn dogs. Am J Physiol 256:
H1659–H1666.
Naritomi H, Sasaki M, Kanashiro M, et al. (1988). Flow
thresholds for cerebral energy disturbance and Naþ pump
failure as studied by in vivo 31P and 23Na nuclear mag-
netic resonance spectroscopy. J Cereb Blood Flow Metab
8: 16–23.
Neumann-Haefelin T, Wittsack HJ, Wenserski F, et al.
(1999). Diffusion- and perfusion-weighted MRI. The
DWI/PWI mismatch region in acute stroke. Stroke 30:
1591–1597.
Noda A, Ohba H, Kakiuchi T, et al. (2002). Age-related
changes in cerebral blood flow and glucose metabolism
in conscious rhesus monkeys. Brain Res 936: 76–81.
Obrenovitch TP, Hallenbeck JM (1985). Platelet accumula-
tion in regions of low blood flow during the post-ischemic
period. Stroke 16: 224–234.
Obrenovitch TP, Garofalo O, Harris RJ, et al. (1988). Brain
tissue concentrations of ATP, phosphocreatine, lactate,
and tissue pH in relation to reduced cerebral blood flow
following experimental acute middle cerebral artery occlu-
sion. J Cereb Blood Flow Metab 8: 866–874.
Olah L, Wecker S, Hoehn M (2000). Secondary deterioration
of apparent diffusion coefficient after 1-hour transient
focal cerebral ischemia in rats. J Cereb Blood Flow Metab
20: 1474–1482.
Opitz E, Schneider M (1950). Uber die Sauerstoffversorgung
des Gehirns und den Mechanismus der Mangelwirkungen.
Ergeb Physiol 46: 126–260.
Ostergaard L, Smith DF, Vestergaard-Poulsen P, et al.
(1998). Absolute cerebral blood flow and blood volume
measured by magnetic resonance imaging bolus tracking:
comparison with positron emission tomography values. J
Cereb Blood Flow Metab 18: 425–432.
![Page 25: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/25.jpg)
CEREBRAL BLOOD FLOW AND THE ISCHEMIC PENUMBRA 91
Parsons MW, Yang Q, Barber PA, et al. (2001). Perfusion
magnetic resonance imaging maps in hyperacute
stroke—Relative cerebral blood flow most accurately
identifies tissue destined to infarct. Stroke 32: 1581–1587.
Paschen W (1985). Regional quantitative determination of
lactate in brain sections. A bioluminescent approach. J
Cereb Blood Flow Metab 5: 609–612.
Paschen W, Djuricic BM, Bosma H-J, et al. (1983). Biochem-
ical changes during graded brain ischemia in gerbils. 2.
Regional evaluation of cerebral blood flow and brain
metabolites. J Neurol Sci 58: 37–44.
Paschen W, Mies G, Hossmann K-A (1992). Threshold rela-
tionship between cerebral blood flow, glucose utilization,
and energy metabolites during development of stroke in
gerbils. Exp Neurol 117: 325–333.
Rasey JS, Grunbaum Z, Magee S, et al. (1987). Characteriza-
tion of radiolabeled fluoromisonidazole as a probe for
hypoxic cells. Radiat Res 111: 292–304.
Read SJ, Hirano T, Abbott DF, et al. (1998). Identifying
hypoxic tissue after acute ischemic stroke using PET and
F-18-fluoromisonidazole. Neurology 51: 1617–1621.
Read SJ, Parsons AA, Harrison DC, et al. (2001). Stroke
genomics: Approaches to identify, validate, and under-
stand ischemic stroke gene expression. J Cereb Blood
Flow Metab 21: 755–778.
Rebel A, Ulatowski JA, Kwansa H, et al. (2003). Cerebrovas-
cular response to decreased hematocrit: effect of cell-free
hemoglobin, plasma viscosity, and CO2. Am J Physiol
Heart Circ Physiol 285: H1600–H1608.
Reivich M (1964). Arterial PCO2 and cerebral hemody-
namics. Am J Physiol 206: 25–35.
Rickhag M, Wieloch T, Gido G, et al. (2006). Comprehensive
regional and temporal gene expression profiling of the rat
brain during the first 24 h after experimental stroke identi-
fies dynamic ischemia-induced gene expression patterns,
and reveals a biphasic activation of genes in surviving tis-
sue. J Neurochem 96: 14–29.
Rohl L, Ostergaard L, Simonsen CZ, et al. (2001). Viability
thresholds of ischemic penumbra of hyperacute stroke
defined by perfusion-weighted MRI and apparent diffu-
sion coefficient. Stroke 32: 1140–1146.
Roy CS, Sherrington CS (1890). On the regulation of the
blood supply of the brain. J Physiol 11: 85–108.
Saita K, Chen M, Spratt NJ, et al. (2004). Imaging the
ischemic penumbra with F-18-fluoromisonidazole in a rat
model of ischemic stroke. Stroke 35: 975–980.
Sakurada O, Kennedy C, Jehle J, et al. (1978). Measurement
of local cerebral blood flow with iodo(14C)antipyrine. Am
J Physiol 234: H59–H66.
Schlaug G, Benfield A, Baird AE, et al. (1999). The
ischemic penumbra—operationally defined by diffusion
and perfusion MRI. Neurology 53: 1528–1537.
Schmid-Schonbein H (1981). Factors promoting and pre-
venting the fluidity of blood. In: R Effros, H Schmid-
Schonbein, J Ditzel (Eds.), Microcirculation, Academic
Press, New York, pp. 249–266.
Schuier FJ, Hossmann K-A (1980). Experimental brain infarcts
in cats II. Ischemic brain edema. Stroke 11: 593–601.
Schumann-Bard P, Touzani O, Young AR, et al. (2005). Cer-
ebrovascular effects of sodium nitroprusside in the anaes-
thetized baboon: a positron emission tomographic study.
J Cereb Blood Flow Metab 25: 535–544.
Selman WR, VanderVeer C, Whittingham TS, et al. (1987).
Visually defined zones of focal ischemia in the rat brain.
Neurosurgery 21: 825–830.
Sette G, Baron JC, Young AR, et al. (1993). Invivo mapping
of brain benzodiazepine receptor changes by positron
emission tomography after focal ischemia in the anesthe-
tized baboon. Stroke 24: 2046–2057.
Shapiro HM, Stromberg DD, Lee DR, et al. (1971). Dynamic
pressures in the pial arterial microcirculation. Am J Phy-
siol 221: 279–283.
Sharbrough FW, Messick JM, Sundt TM (1973). Correlation
of continuous electroencephalograms with cerebral blood
flow measurements during carotid endarterectomy. Stroke
4: 674–683.
Sharp FR, Lu AG, Tang Y, et al. (2000). Multiple molecular
penumbras after focal cerebral ischemia. J Cereb Blood
Flow Metab 20: 1011–1032.
Shen Q, Meng TJ, Sotak CH, et al. (2003). Pixel-by-pixel
spatiotemporal progression of focal ischemia derived
using quantitative perfusion and diffusion imaging. J
Cereb Blood Flow Metab 23: 1479–1488.
Shen Q, Ren HX, Fisher M, et al. (2004). Dynamic tracking of
acute ischemic tissue fates using improved unsupervised
ISODATA analysis of high-resolution quantitative perfusion
and diffusion data. J Cereb Blood Flow Metab 24: 887–897.
Shih LC, Saver JL, Alger JR, et al. (2003). Perfusion-weighted
magnetic resonance imaging thresholds identifying core,
irreversibly infarcted tissue. Stroke 34: 1425–1430.
Shima T, Hossmann K-A, Date H (1983). Pial arterial pres-
sure in cats following middle cerebral artery occlusion 1.
Relationship to blood flow, regulation of blood flow and
electrophysiological function. Stroke 14: 713–719.
Shimada N, Graf R, Rosner G, et al. (1989). Ischemic flow
threshold for extracellular glutamate increase in cat cortex.
J Cereb Blood Flow Metab 9: 603–606.
Shimada N, Graf R, Rosner G, et al. (1990). Differences in
ischemia-induced accumulation of amino acids in the cat
cortex. Stroke 21: 1445–1451.
Slosman DO, Chicherio C, Ludwig C, et al. (2001). 133Xe
SPECT cerebral blood flow study in a healthy population:
determination of T-scores. J Nucl Med 42: 864–870.
Sobesky J, Zaro Weber O, Lehnhardt FG, et al.
(2004). Which time-to-peak threshold best identifies
penumbral flow? A comparison of perfusion-weighted
magnetic resonance imaging and positron emission tomo-
graphy in acute ischemic stroke. Stroke 35: 2843–2847.
Sokoloff L, Perlins S, Kornetsky C, et al. (1957). The effects
of D-lysergic acid diethylamide on cerebral circulation and
overall metabolism. Ann N Y Acad Sci 66: 468–477.
Sorensen AG, Buonanno FS, Gonzalez RG, et al. (1996).
Hyperacute stroke: evaluation with combined multisection
diffusion-weighted and hemodynamically weighted echo-
planar MR imaging. Radiology 199: 391–401.
Strandgaard S, Olesen J, Skinhoj E, et al. (1973). Autoregula-
tion of brain circulation in severe arterial hypertension. Br
Med J 1: 507–510.
Sundt TM, Waltz AG (1971). Cerebral ischemia and reactive
hyperemia. Studies of cortical blood flow and microcircula-
![Page 26: [Handbook of Clinical Neurology] Stroke Volume 92 || Chapter 4 Cerebral blood flow and the ischemic penumbra](https://reader030.pdfslide.net/reader030/viewer/2022020300/575096001a28abbf6bc6bfbc/html5/thumbnails/26.jpg)
92 K.-A. HOSSMANN AND R.J. TRAYSTMAN
tion before, during, and after temporary occlusion of middle
cerebral artery of squirrel monkeys. Circ Res 28: 426–433.
Symon L (1968). Experimental evidence for ‘intracerebral
steal’ following CO2 inhalation. Scand J Clin Lab Invest
102: 13A.
Symon L (1970). Regional vascular reactivity in the middle
cerebral arterial distribution. An experimental study in
baboons. J Neurosurg 33: 532–541.
Symon L, Branston NM, Strong AJ (1976). Autoregulation
in acute focal ischemia. An experimental study. Stroke 7:
547–554.
Symon L, Branston NM, Strong AJ, et al. (1977). The con-
cepts of thresholds of ischaemia in relation to brain struc-
ture and function. J Clin Pathol 30: 149–154.
Takagi K, Ginsberg MD, Globus MY, et al. (1993). Changes
in amino acid neurotransmitters and cerebral blood
flow in the ischemic penumbral region following middle
cerebral artery occlusion in the rat: correlation with
histopathology. J Cereb Blood Flow Metab 13: 575–585.
Tamura A, Graham DI, McCulloch J, et al. (1981). Focal
cerebral ischaemia in the rat: 2. Regional cerebral blood
flow determined by (14C)iodoantipyrine autoradiography
following middle cerebral artery occlusion. J Cereb Blood
Flow Metab 1: 61–69.
Toole JF, McGraw CP (1975). The steal syndromes. Annu
Rev Med 26: 321–329.
Touzani O, Roussel S, MacKenzie ET (2001). The ischaemic
penumbra. Curr Opin Neurol 14: 83–88.
Traystman RJ, Fitzgerald RS, Loscutoff SC (1978). Cerebral
circulatory responses to arterial hypoxia in normal and
chemodenervated dogs. Circ Res 42: 649–657.
Tulleken CAF, Abraham J (1975). The influence of changes
in arterial CO2 and blood pressure on the collateral circu-
lation and the regional perfusion pressure in monkeys with
occlusion of the middle cerebral artery. Acta Neurochir
(Wien) 32: 161–173.
Turcani P, Tureani M (2001). Effect of propentofylline on
cerebral blood flow in a gerbil focal cerebral ischemia. J
Neurol Sci 183: 57–60.
Turner R, LeBihan D, Moonen CT, et al. (1991). Echo-pla-
nar time course MRI of cat brain oxygenation changes.
Magn Reson Med 22: 159–166.
Van der Veer CA, LaManna JC, Whittingham JC, et al.
(1985). Metabolic studies of focal ischemic zones in brain
defined by neutral red. Fed Proc 44: 1355.
Vannucci RC, Towfighi J, Brucklacher RM, et al. (2001). Effect
of extreme hypercapnia on hypoxic–ischemic brain damage
in the immature rat. Pediatr Res 49: 799–803.
Voelckel WG, Lurie KG, Sweeney M, et al. (2002). Effects of
active compression-decompression cardiopulmonary resus-
citation with the inspiratory threshold valve in a young por-
cine model of cardiac arrest. Pediatr Res 51: 523–527.
Vogel J, Mobius C, Kuschinsky W (1999). Early delineation
of ischemic tissue in rat brain cryosections by high-
contrast staining. Stroke 30: 1134–1140.
Von Vollmar J (1971). Steal syndrome. Munch Med
Wochenschr 113: 501–506.
Waltz AG (1968). Effect of blood pressure on blood flow in
ischemic and in nonischemic cerebral cortex. The phe-
nomena of autoregulation and luxury perfusion. Neurol-
ogy 18: 613–621.
Waltz AG (1970). Effect of PaCO2 on blood flow and micro-
vasculature of ischemic and nonischemic cerebral cortex.
Stroke 1: 27–37.
Warach S (2003). Measurement of the ischemic penumbra
with MRI: it’s about time. Stroke 34: 2533–2534.
Warach S, Gaa J, Siewert B, et al. (1995). Acute human stroke
studied by whole brain echo planar diffusion-weighted
magnetic resonance imaging. Ann Neurol 37: 231–241.
Watanabe Y, Takagi H, Aoki S, et al. (1999). Prediction of
cerebral infarct sizes by cerebral blood flow SPECT per-
formed in the early acute stage. Ann Nucl Med 13:
205–210.
Watanabe Y, Nakano T, Yutani K, et al. (2000). Detection of
viable cortical neurons using benzodiazepine receptor
imaging after reversible focal ischaemia in rats: compari-
son with regional cerebral blood flow. Eur J Nucl Med
27: 308–313.
Welsh FA, Marcy VR, Sims RE (1991). NADH fluorescence
and regional energy metabolites during focal ischemia and
reperfusion of rat brain. J Cereb Blood Flow Metab 11:
459–465.
Williams DS, Detre JA, Leigh JS, et al. (1992). Magnetic
resonance imaging of perfusion using spin inversion of
arterial water. Proc Natl Acad Sci U S A 89: 212–216.
Wintermark M, Thiran JP, Maeder P, et al. (2001). Simulta-
neous measurement of regional cerebral blood flow by
perfusion CT and stable xenon CT: a validation study.
AJNR Am J Neuroradiol 22: 905–914.
Wintermark M, Reichhart M, Thiran JP, et al. (2002). Prog-
nostic accuracy of cerebral blood flow measurement by
perfusion computed tomography, at the time of emergency
room admission, in acute stroke patients. Ann Neurol 51:
417–432.
Wood JH, Kee DB (1985). Hemorheology of the cerebral
circulation in stroke. Stroke 16: 765–772.
Xie Y, Mies G, Hossmann K-A (1989). Ischemic threshold
of brain protein synthesis after unilateral carotid artery
occlusion in gerbils. Stroke 20: 620–626.
Yamamoto YL, Phillips KM, Hodge CP, et al. (1971). Micro-
regional blood flow changes in experimental cerebral
ischemia. Effects of arterial carbon dioxide studied by
fluorescein angiography and xenon133 clearance. J Neuro-
surg 35: 155–166.
Yamamoto YL, Nakai H, Diksic M, et al. (1988). Regional
cerebral blood flow threshold for metabolic changes in
cerebral ischemia in rat studies by triple-tracer autoradio-
graphy. Can J Neurol Sci 15: 243–244.
Yao H, Ginsberg MD, Eveleth DD, et al. (1995). Local cere-
bral glucose utilization and cytoskeletal proteolysis as
indices of evolving focal ischemic injury in core and
penumbra. J Cereb Blood Flow Metab 15: 398–408.
Zulch K-J (1985). The Cerebral Infarct. Pathology, Pathogen-
esis, and Computed Tomography. Springer-Verlag, Berlin.



![Realistic Soft Shadows by Penumbra-Wedges Blending · Penumbra-wedges X + Specular & diffuse Visibility buffer Modulated spec+diff Ambient Final image. Penumbra-wedges [3/4] Penumbra-wedges](https://img.pdfslide.net/doc/110x75/5f543a4c0135c76e2b226697/realistic-soft-shadows-by-penumbra-wedges-penumbra-wedges-x-specular-diffuse.jpg)


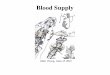
![Machine learning-based segmentation of ischemic penumbra ... · and salvageable ischemic penumbra (IP) is essential for a patient to be eligible for therapy [2–4]. In the DAWN and](https://img.pdfslide.net/doc/110x75/60b6cccfac40f5674337bc9a/machine-learning-based-segmentation-of-ischemic-penumbra-and-salvageable-ischemic.jpg)




















