Embed Size (px)
Citation preview

HANDOUT 1
(INTRODUCTION)
T-CELL INFILTRATES

CUTANOEUS LYMPHOID INFILTRATESCOMMONLY ASKED QUESTIONS
1. Is it benign or malignant?• Distinguishing benign from
neoplastic lymphoid infiltrates
in the skin
2. What sort of lymphoma is this?• Problems with existing
classifications• Recognizing (very) rare entities
Modern lymphoma classifications define entities on basis of ALL available information•Morphology•Immunophenotype•Genetic features•Clinical features
Two systems applicable to skin
CLASSIFICATION OF CUTANEOUS LYMPHOMA
WHO CLASSIFICATIONSite of origin recognised as important in determining characteristics of a lymphoma, but little clinical detail given for B-cell lymphomas arising primarily in the skin EORTC CLASSIFICATIONOnly includes cutaneous lymphomas. Provides detailed clinical information, including best treatment, but not widely accepted outside Europe
CONSIDERABLE OVERLAP BUT TERMINOLOGY AND DEFINITIONAL CRITERIA USED FOR SOME
ENTITIES NOT DIRECTLY COMPARABLE
WHICH CLASSIFICATION?
A pragmatic approach
•Use terminology and criteria consistent with WHO classification
•Include EORTC equivalent in conclusion and/or additional
information to highlight lymphoma subtypes which are biologically
distinct when arising primarily in skin
BOTH!
CASE 1 ADDITIONAL FINDINGS
•Phenotype of majority of cells in both biopsies CD3+/CD4+/CD8-
•Same clonal TCR re-arrangement in both biopsies
DIAGNOSIS
FOLLICULAR MYCOSIS FUNGOIDESMF-associated follicular mucinosis
(EORTC)Pilotropic mycosis fungoidesFolliculocentric mycosis fungoides
CLINICOPATHOLOGICALLY DISTINCT VARIANT OF MYCOSIS FUNGOIDES
CLINICAL FEATURES
•Predilection for head and neck
•Patches, plaques or grouped papules
•Alopecia, pruritis, bacterial infection common
•Rare presentations includenodules/tumourscysts/comedoneserythroderma
PATHOLOGY (1)
•Perivascular/perifollicular or diffuse dermal
infiltrate
•Lack of epidermotropism
•Medium to large T-cells with cerebriform
nuclei
•Infiltration of hair follicle epitheliumUsually (not always) with follicular mucinosisOften relatively few infiltrating lymphocytes
•Infiltration of sweat duct epithelium rarely
PATHOLOGY (2)
•Reactive cellsSmall lymphocytes, histiocytes, eosinophils, plasma cells
•Disease progression associated withMore diffuse dermal infiltrateDestruction/loss of hair folliclesIncreasing numbers of blasts
•ImmunophenotypeCD3+/CD4+/CD8-CD30+ blasts variable

TREATMENT/OUTCOME
Compared to classic MF•Respond less well to skin targeted therapy
(Total skin electron beam in favour of
PUVA)•Fewer achieve complete remission
regardless of treatment•Much poorer survival than plaque/patch
stage MF•Similar survival to tumour stage MF•5-year DSS = 68%; 10-year DSS = 26%

DIFFERENTIAL DIAGNOSIS
1. Non-epidermotropic CTCL• Look hard for follicular damage
2. Idiopathic follicular mucinosis/Alopecia mucinosa
3. Pseudolymphomatous folliculitis
2. IDIOPATHIC FOLLICULAR MUCINOSIS
Younger adults, adolescentsSolitary/localised lesions on head & neckNo progression to overt CTCL
NO pathological features which permit D/Dx from follicular mucinosis due to CTCL
•histology•immunophenotype•PCR (~50% monoclonal TCR re-arrangement)
A localised variant of follicular MF with excellent prognosis?
3. PSEUSOLYMPHOMATOUS FOLLICULITIS• Solitary or localised dome shaped lesions on face
• Dense dermal infiltrate; variable proportion of T & B cells
• Perifollicular distribution
Enlargement & distortion of hair follicles (activation)
Lymphocytic infiltration of epithelium
• Aggregates of histiocytes adjacent to follicles (S-100/CD1a positive)
• PCR polyclonal
• Spontaneous regression may occur following incisional biopsy
FURTHER READING
Cerroni et al. Arch Dermatol 2002; 138: 182
Van Doorn et al. Arch Dermatol 2002; 138: 191
Eichii et al. Am J Surg Pathol 1999; 23: 1313
CASE 2: ADDITIONAL FINDINGS
•No history of prior or concurrent MF
•Localised to skin on staging

DIAGNOSISCD30-POSITIVE CUTANEOUS LARGE T-CELL LYMPHOMA
(EORTC)
NOTE:Strict application of WHO classification would result in this case being classified as, ‘peripheral T-cell lymphoma, unspecified’ because cells do not have an anaplastic morphology.
This would result in overtreatment: should really be included in category of‘PRIMARY CUTANEOUS ANAPLASTIC LYMPHOMA’
CLINICAL
•Disease of adults; rare in children (cf systemic ALCL)
•Nodules or tumours +/- ulceration
•80% solitary or localised
•20% multicentric
•Partial/complete spontaneous regression in some

PATHOLOGYDiffuse non-epidermotropic infiltrate of large T-cells
80% anaplastic morphology•Round, oval, irregular nuclei•Prominent nucleoli•Abundant cytoplasm•R-S-like cells
20% large T-cells•Pleomorphic•Immunoblastic
N.B. ANAPLASTIC or LARGE CELL HAS NO EFFECT ON OUTCOME
IMMUNOPHENOTYPE/GENETICS
•CD4/CD30 positive (>75% cells)
•Loss of pan-T-cell antigens (CD2/3/5/7) common but ‘null-cell’ phenotype rare
•Cytotoxic granule associated proteins usually positive (>70% cases)
•TIA-1•Granzyme B•perforin
•EMA & ALK negative
•NO t(2;5)
TREATMENT/OUTCOME•Most cases treatable by XRT or low dose methotrexate (if multicentric)
•5-year survival ~90%
DIFFERENTIAL DIAGNOSIS1. Systemic ALCL involving skin
2. Transformed MF
3. Lymphomatoid papulosis
4. Benign lesions with CD30-positive cells
SYSTEMIC ANAPLASTIC LARGE CELL LYMPHOMA
•Similar morphology
•Bimodal age distribution; affects children
•Almost always disseminated at presentation
•Different phenotype•ALK+•EMA+•t(2;5) present

TRANSFORMED MYCOSIS FUNGOIDES
•Biopsy proven history of MF
•Infiltrate >25% large T-cells (>x4 small lymphocyte)
•In 1/3 cases majority of cells CD30+
•Usually correlates with tumour-stage lesions
•Very poor outcome: 5-year survival ~20%
•CLINICOPATHOLOGICAL CORRELATION/REVIEW

LYMPHOMATOID PAPULOSIS
•Crops of papular, papulonecrotic, nodular skin lesions
•Grouped but may be in different stages of development
•Spontaneous regression of individual lesion; 3-6 weeks
•Chronic but benign course; months-years
•5 year survival ~100%
•No treatment required or low dose methotrexate, PUVA or XRT for large, numerous or scarring lesions
PATHOLOGY: TWO TYPES OF LESION
TYPE A•Wedge shaped dermal infiltrate: non-epidermotropic•Large atypical CD30+ T-cells•Histiocytes, small lymphocytes, granulocytes
TYPE B•Simulates plaque-stage MF•Perivascular or band-like epidermotropic infiltrate•Small lymphocytes with cerebriform nuclei
IMMUNOPHENOYPE/GENETICS•Large T-cells: same as for CD30+ LTCL•TCR often clonally rearranged; type B>type A•t(2;5) not found
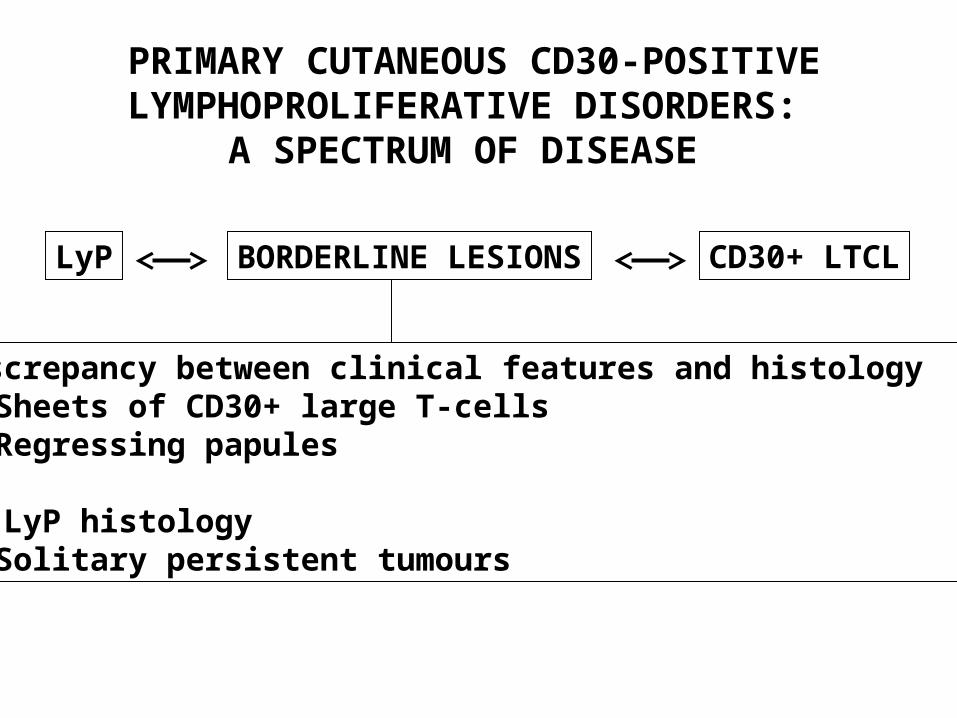
PRIMARY CUTANEOUS CD30-POSITIVE LYMPHOPROLIFERATIVE
DISORDERS: A SPECTRUM OF DISEASE
LyP BORDERLINE LESIONS CD30+ LTCL
Discrepancy between clinical features and histology1. Sheets of CD30+ large T-cells
Regressing papules
2. LyP histologySolitary persistent tumours
BENIGN LESIONS WITH CD30+ CELLS
•Drug reaction (carbamazepine)
•Viral infection (molluscum, herpes simplex)
•Arthropod bite reactions (scabies)
•CLINICOPATHOLOGICAL CORRELATION
CD30+ CUTANEOUS INFILTRATES:THREE STEPS TO DIAGNOSIS
Step 1: exclude benign conditions
Step 2: is the lesion primary or secondary?•Hx of prior or concurrent MF(If localised to skin manage as tumour stage MF; N.B. ~3% of MF have concurrent LyP so make sure lesions don’t spontaneously regress)
•ALK/EMA positivity: ALCL; needs systemic CTX
Step 3: LyP or CD30+ LTCL?•In view of ‘borderline cases’ give lesions chance to regress
FURTHER READING
Bekkenk et al. Blood 2000; 95: 3653
Beylot-Barry et al. Blood 1998; 91: 4668
Wood et al. Blood 1996; 8: 1765
Whittaker et al. J Invest Dermatol 1991; 96: 786
Nathan & Belsito. J Am Acad Dermatol 1998; 38: 806
McCalmont & LeBoit. Am J Dermatopathol 2000; 22: 188

CASE 3: ADDITIONAL FINDINGS
•Confined to skin on staging
•Monoclonal TCR-gamma gene re-arrangement
DIAGNOSIS
PERIPHERAL T-CELL LYMPHOMA, UNSPECIFIED (WHO)
OR
PRIMARY CUTANEOUS CD30- LARGE T-CELL LYMPHOMA(EORTC)
PTL, UNSPECIFIED PRESENTING IN SKIN•Heterogeneous group of diseases•Poor prognosis: 5-year survival ~20%
•Diffuse, nodular or band-like infiltrate•Variably sized T-lymphocytes
+/- epidermotropism+/- angiocentricity
•Admixture of reactive cellsHistiocytes > eosinophils, plasma cellsB-cells; up to 5-10% of infiltrate
•CD3+/CD4+/CD8- > CD3+/CD4-/CD8+•TIA-1 +/- (CD8+ cases)•CD56 rarely positive•CD30 negative

SUBCLASSIFICATION
Prognosis appears to be influenced by cell size
Overall 5-year survival• Large cells confined to skin 12%• Large cells + lymph node involvement 12%• Small/medium cells confined to skin 45%
(only localised CD4+ cases do well)
EORTC recommend sub-division on basis of cell size1. CD30- large T-cell lymphoma
>30% large cells
2. Small/medium sized CD30- pleomorphic T-cell lymphoma
DIFFERENTIAL DIAGNOSIS
1. CD30+ large T-cell lymphoma• > or < 75% cells express CD30
2. Tumour stage MF• Clinicopathological correlation
3. Follicular MF• +/- infiltration of hair follicles
4. Subcutaneous panniculitis-like T-cell lymphoma
5. Cutaneous T-cell pseudolymphoma
FURTHER READING
Bekkenk et al. Blood 2003; 102: 2213
Beljaard et al. J Pathol 1994; 172: 53
Grange et al. Blood 1999; 3637
CASE 4: ADDITIONAL FINDINGS
Immunophenotype•CD3+•CD8+•CD4-•CD56-
PCR•Monoclonal TCR gene re-arangement
DIAGNOSIS
SUBCUTANEOUS PANNICULITIS-LIKE T-CELL LYMPHOMA(EORTC, WHO)
Synonymscytophagic histiocytic panniculitis
CLINICAL
Multiple skin nodules•+/- ulceration•Often tender•Trunk, extremities
Systemic symptoms due to haemophagocytic syndrome in some
•Pancytopaenia•Fever•Hepatospelonmegaly

PATHOLOGY
Preferential involvement of subcutis•Resembles panniculitis with lobular & septal involvement•Dermis only occasionally involved (CD56+, )
Variably sized neoplastic lymphocytesRimming of fat cellsTumour cell necrosis, histiocytes, erythrophagocytosis
IMMUNOPHENOTYPE
Lymphoma of cytotoxic T-cells•CD3+, CD8+, CD4-•TIA-1, granzyme , perforin (cytotoxic molecules)•CD16, CD30, CD56 (except for cases), CD57 negative•EBV negative
PROGNOSIS
•Aggressive but usually good response to CTX
•CD56+ cases seem to do badly

DIFFERENTIAL DIAGNOSIS
1. CD30- CTCL/peripheral T-cell lymphoma unspecified• Distribution of infiltrate; dermis vs subcutis• Rimming of fat cells, karryhorexis• Most CD30- CTCL are also CD8-
2. Nasal NK/T cell lymphoma• Usually involves other extranodal sites• Prominent angiocentricity• Overruns rather than rims fat cells• CD2/CD56+, CD3-, CD3+ (cytoplasmic)• EBV+• TCR usually germline
FURTHER READING
Salhany et al. Am J Surg Pathol 1998; 22: 881
Chan et al. Mod Pathol 1996; 9: 109
Gonzalez et al. Am J Surg Pathol 1991; 15: 17
Santucci et al. Cancer 2003; 97: 610
CASE 5: ADDITIONAL FINDINGS
•Polyclonal TCR re-arrangement
•Patient found to be on ACE inhibitor
DIAGNOSIS
CUTANEOUS T-CELL PSEUDOLYMPHOMA(drug induced)
Synonyms:lymphomatoid drug reactionT-cutaneous lymphoid hyperplasia
CUTANEOUS T-CELL PSEUDOLYMPHOMA
Definition1. Lymphoid infiltrate highly suggestive of CTCL
2. Clinical features NOT consistent with CTCL• Identification of causative agent• Uncommon presentation or course
CUTANEOUS T-CELL PSEUDOLYMPHOMA: SUBTYPES
1. Well defined clinicopathological entities• Drug induced
Anticonvulsants; phenytoin, carbamazepine
ACE inhibitors Miscellaneous; atenolol, allopurinol,
mexilitine, cyclosporine, antihistamines, griseofulvin
• Insect bite reactions• Lymphomatoid contact dermatitis• Actinic reticuloid;
chronic photosensitive dermatitis Scaly erythema of exposed skin
2. Idiopathic
HISTOLOGY: TWO PATTERNS
1. Band-like infiltrate (MF-like)• Subepidermal infiltrate• Atypical medium sized cerebriform cells
+/- blasts• histiocytes• Few/no eosinophils, plasma cells
Seen in all types of CTCPL except insect bite reactions
2. Nodular pattern
•Many small round T-cells
•Scattered T-blasts & medium/large cerebriform cells
•Histiocytes usually numerous +/- plasma cells, eosinophils
Seen in
•Drug induced CTCPL
•Persistent arthropod bite reactions
•Idiopathic CTCPL
MF-LIKE CTCPL vs MYCOSIS FUNGOIDES
Features which strongly suggest MF
1. Pautrier’s microabscesses
2. Medium/large cerebriform cells in epidermis
3. Linear epidermotropism
4. Disproportionate epidermotropism
5. ‘Haloed’ lymphocytes in epidermis
ACTINIC RETICULOID vs MYCOSIS FUNGOIDES
•CD8+ T-cells, MF usually CD4+
•Multinucleate giant cellsfibroblastshistiocytes
•Vertically orientated collagen in papillary dermis
NODULAR PATTERN vs CTCL
•Solitary lesions favour pseudolymphoma
•Admixture of CD4+ & CD8+ T-cellsCD4+ usually > CD8+
•Numerous small round T-cells
•Numerous B-cells (up to 10%)
•Numerous histiocytes
USEFUL ADDITIONAL FINDINGSABERRANT PHENOTYPE1.Loss of pan-T-cell antigens
CD2, CD3, CD5, CD7BUT also lost in some benign conditions
(esp CD7)
2. Ratio of CD4:CD8vast excessdual expressionno expression
MONOCLONAL TCR RE-ARRANGEMENTBUT monoclonality found in typically
benign lesionse.g. lichen planus, pityriasis lichenoides,
LSAthus monoclonal but benign infiltrates
may arise in the skin
FURTHER READING
Rijlaarsdam et al. Cancer 1992; 69: 717
Rijlaarsdam & Willemze. Sem Diagn Pathol 1991; 8: 102
Van Vloten & Willemze. J Eur Acad Dermatol Venereol 2003; 17: 3
Holm et al. J Cutan Pathol 2002; 29: 447