Embed Size (px)
Citation preview

HARM REDUCTION IN ASIA
Adeeba Kamarulzaman
University of Malaya, Kuala Lumpur

*Mathers et al., 2008. The global epidemiology of injecting drug use and HIV among people who inject drugs: a systematic review.
The Lancet: IN PRESS
No estimate of HIV prevalence
0% ‐
<7.5%
7.5% ‐
<15%
15% and greater
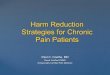
Prevalence of HIV among IDUs: 2007
• DU identified in 148 countries
• 15.9 million PWID
• Accounts for 30% of all new infections outside Sub-Saharan Africa
• Up to 3.3 million PWID living with HIV IDU
Reference Group to the United Nations on HIV and Injecting Drug Use Lancet 2008

Estimated number of people who inject drugs in selected Asian Countries
China 541,184Indonesia 219,130Malaysia 205,000India 164,820Thailand 160,528Vietnam 135,305Pakistan 130,460Myanmar 75,000Bangladesh 30,000Nepal 22,050Cambodia 1,750Lao PDR Not knownTotal 1,685,227

HIV prevalence among people who inject drugs
UNRTF 2008

HIV prevalence in incarcerated settings
• Vietnam - 28.4% of the estimated 88,000 prisoners
• Indonesia - 20.0% of 100,000 prisoners• China and Malaysia - 4.0 % • Vietnam - 40 – 50% among residents in
drug rehabilitation centres

Progress of Harm Reduction in Asia

Harm Reduction in Philippines• Has three identified sites with people who inject drugs
• Harm reduction programme supported by the Global Fund and ADB – implemented mainly by NGOs – Needles and syringes continue to be distributed discreetly in
identified sites, with support from GF Rounds 3 and 5 AIDS Project
– NGOs refer IDUs to treatment hubs for treatment, care and support
• Outreach work and outreach post supported by ADB in one site
• Government drafting the national guidelines on HR

•National Strategic Plan for drug use and HIV/AIDS, 2008 2010
•NSP operational since 2004
•Outreach programmes
•Govt authorisation to commence MMT through Ministry of Health
Cambodia


10
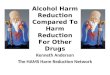
China• First NSP in Yunnan province and Guangxi Zhuang AR
in 1999;
• Since 2001, the State Council has officially advocated needle social marketing;
• National policy guidelines on NSP in 2002;
• Almost 800 NSP in 17 Provinces by September 2008• 50,000 accessing NSP
• 515 MMT clinics by end of 2007 in 22 Provinces• 100,000 on MMT
• Wu, Sullivan et al. (2007) Evolution of China's response to HIV/AIDS, The Lancet. 369:679‐690• Mesquita, F et al. (2008, submitted) Accelerating Harm Reduction
interventions to confront the HIV epidemic in the Western
Pacific and Asia: the role of WHO (WPRO), Harm Reduction Journal.• WHO Report, Towards Universal Access, Geneva, 2 of June 2008.

11
Methadone Maintenance Clinic inKunming - China

12
Malaysia
• National response since 2005 after evaluation of the
non achievement of the Millennium Goals.
• Mainly a Public Health Based approach, combined with
NGOs for NSP
• Comprehensive approach - NSP, MMT and CST
• Currently 74 MMT clinics, started in prisons in 2008
• 6 NSP covering 3600 IDUs by the end of 2007.
• National Government supports the response
• Mesquita, F et al. (2008, submitted) Accelerating Harm Reduction
interventions to confront the HIV epidemic in the Western
Pacific and Asia: the role of WHO (WPRO), Harm Reduction Journal.

• 22 000 on opiate substitution treatment
• 11 NSP sites ‐
> 1.3 M needles and syringes distributed as of
June 2008
• Pre‐release prison methadone project


Indonesia• Strong political commitment
• Costed National Action Plans
• ST: – 7 methadone clinics (4 in Hospital, 2 in Puskesmas, 1
in prison)– Around 1700 on MMT and Buprenorphine
• NSP:
– 130 NSP sites
• ARV: Required for IDU – limited access/availability

Vietnam
• Public Health Based approach
• 42 Provinces in Vietnam conducting HR activities• 60,000 IDU accessing NSP with a total of 11
million syringes distributed• In April 2008 Vietnam announced its first MMT
clinic– Currently ~ 500 on MMT
• ARV for IDUs has good coverage, thanks to PEPFAR

Deputy First Minister of Vietnam Addressing the National HR Conf.

India• Political commitment:
– No established policy on Harm Reduction.
• Enabling environment:
– Drug use remains a criminal offence.
– Methadone classified as narcotic and not used.
– The legality of NSP under the NDPS Act is
unclear.

India• OST: Buprenorphine.
– NGO interventions in Delhi, Chennai, Kolkata and Mumbai
– 4,000 on Buorenorphine
• NSP: – 122 government supported NGO targeted intervention
sites which include NSP .
• ARV:
– Affordability generally limited.

Thailand• Political commitment:
– No concrete political commitment to HR strategies - law enforcement
approach dominates.
• Enabling environment: – A National Strategy for collaboration between public health and law
enforcement required.
• Policy environment: – Incarceration for drug possession. No effort to address legal/policy
issues.

Thailand
• ST: Methadone only free in Bangkok – very hard to access in other provinces. No methadone in prison settings.
• NSP: Small scale (needle distribution almost totally underground)2 official NSP - less than 500 clinets

Factors that Hamper Progress of Harm Reduction in Asia
• Legislative and policy barriers to harm reduction
• High level of stigma and discrimination
• Overlap between SW and injecting drug use
• Limited government capacity and infrastructure
to develop, scale up and monitor harm,
reduction programmes

Factors that Hamper Progress of Harm Reduction in Asia
• Disproportionately low allocation of national
AIDS budget for HIV prevention and harm
reduction among IDU
• Absence, or limited availability of research,
surveillance and M&E data for planning,
implementation and scaling‐up

What Role for TREAT Asia
• Advocacy– Policy– Access to OST, ARV, HCV therapy
• Capacity Building– Healthcare workers– Community
• Operational Research– Integration of prevention and treatment
– Integrating ARV/OST/TB/HCV

What Role for TREAT Asia
• Clinical Research• Coinfections
–
HIV/HCV/Tuberculosis
– Hepatotoxicity– Drug‐drug interaction
• HAART‐TB treatment
• HAART‐OST• HAART‐HCV treatment

Acknowledgements
• Anna Bergenstrom
–
UN Regional Task Force on HIV & IDU
• Fabio Mesquita
–
WPRO
• David Jacka
–
WHO, Vietnam