-
Report Prepared by: HCA of MA Project Committee
Based on survey work by: Massachusetts EHealth Collaborative
(MAeHC)
HOME CARE ALLIANCE OF
MASSACHUSETTS REPORT ON
HEALTH INFORMATION EXCHANGE
(HIE)ADOPTION SUPPORT PROJECT 2016
-
2
Background
Member agencies of the Home Care Alliance in many cases have
worked with various technology vendors
to implement internal electronic health records (EHRs), but are
challenged in terms of connectivity with
referral sources and physician practices.
A 2014 report from the Massachusetts eHealth Institute (MeHI),
the designated state agency for
promoting Health IT innovation, technology and competitiveness
to improve the safety, quality and
efficiency of health care, found that 74 percent of home health
agencies have adopted electronic health
records and only 28 percent of healthcare entities use health
information exchange (HIE) for transitions
of care. Despite being relatively advanced with the use of
mobile technology and home tele-monitoring
systems, among other tools, the MeHI report identified home
health agencies as being among the least
likely of all provider types to participate in health
information exchange, with current participation
estimated at 17 percent.
This report starts with this question: Given the promise and
availability of the HIE in Massachusetts, why
arent more than 17% of home health providers participating in
this important technology? Perhaps the
most important factor is that home health, along with behavioral
health and long term care providers did
not receive financial incentives under the HITECH Act and
American Recovery & Reinvestment Act (ARRA)
that hospitals and eligible medical professionals have used to
offset costs related to achieving meaningful
use of health IT, such as HIE adoption. In addition, the
anticipation that new care and payment models,
such as ACOs, might support the cost of health IT/HIE adoption
among non-incentivized providers, such
as home health, has not yet been realized.
Despite the low participation by home health in HIE, and a lack
of government sponsored funding thus
far, connectivity has been identified as an essential strategy
for sustainability and success for home care
going forward. For example, electronic connections between home
health agencies and physicians are
becoming increasingly critical to support multiple care
processes including continuous updates and sign-
off on care plans, alerts/status updates, medication ordering
and oversight, and chronic care
management.
While the industry continues to lobby for IT funding for long
term care in future phases of meaningful
use, Home Care Alliance of Massachusetts (HCA of MA) has taken
steps to better position home health
agencies to demonstrate their value proposition as connected
partners. To do this, HCA of MA contracted
with the Massachusetts eHealth Collaborative (MAeHC) to survey
members agencies in order
to develop strategies for expanding home health participation in
health information exchange (HIE).
The Massachusetts eHealth Collaborative (MAeHC) is a national
leader in health information technology
implementation, delivery strategy, and best practices for
meaningful adoption of electronic health
records, including Health Information Exchange (HIE)
projects.
This report presents an overview of the survey process and
findings as well as general recommendations
to the membership regarding HIE adoption. Members who
participated in the survey were provided with
individualized strategies for accessing and utilizing the Mass
HiWay. Agencies who did not participate in
the survey may find this report a useful tool to complete an
assessment of their agencys state of readiness
for HIE adoption.
-
3
I. Understanding this Report The purpose of this report is to
present key findings from the HCA of MA landscape survey and
provide
recommended next steps for participation in HIE. The data was
collected from a 40 question electronic
survey which was sent to all certified home health agencies
across the Commonwealth. (See Appendix
A). Questions were divided into 6 categories: 1) Leadership
& Organizational Alignment, 2) Alternative
Payment Models, 3) Infrastructure, 4) EHR/HIE capabilities, 5)
Use of Electronic tools, 6) IT Staffing
Agencys survey answers were analyzed and a level of readiness
for HIE/HIT adoption was
assigned for each of the 5 categories of questions. The
following was used to benchmark each
responding agencys readiness.
Category Level 1 Level 2 Level 3 Level 4
1) Leadership & Organization Alignment
No defined clinical and business needs for IT and leadership is
inactive
Clinical and business needs for IT are loosely defined and
leadership primarily is involved at key decisions
Clinical and business needs align with IT and are clear but not
widely shared across leadership
Clinical and business needs for IT alignment are clear and
shared across an active leadership
2) Alternative Payments
Funding sources not identified to cover investment
Funding to cover investment is possible through grants
Funding identified to cover investment through HIT focused
metrics within state level grants
Funding identified to cover HIT investment through value-based
initiatives (i.e. ACO, preferred provider)
3) Infrastructure No internet access for clinical staff
Dial-up and/or no broadband access
Broadband available to staff but no remote access and/or mobile
devices not deployed
Secure wireless network and deployment of mobile devices to
clinical staff
4) EHR/HIE No electronic documentation system
Have some type of electronic documentation system
Use EHR and do exchange some information with other orgs
Use EHR and exchange information with other orgs over an HIE
and/or send or receive alerts
5) Use of electronic tools
Do not use any electronic tools regularly
Use an electronic order entry or reporting system
Use multiple electronic tools for clinical, reporting or
administrative functions
Regularly use electronic tools (such as e-referrals), reporting
tools (such as for OASIS, and mobile tools (devices, monitors)
6) IT Staffing No IT resources, staff not trained to use HIT
IT resources engaged as needed (not dedicated), staff has some
training in HIT
Dedicated IT resources engaged Staff trained in basic use of
HIT
Dedicated, full-service IT resources engaged Staff highly
trained in use of HIT
-
4
A. Summary of General Survey Findings
1. Despite the lack of direct incentives available to other
health care providers, home care agencies
in Massachusetts have a high level of adoption of basic EHR
technology, and their use of this
technology for core EHR functions appears to be high as well.
(See Charts A and B below.)
2. Achievement of interoperability is uniformly low, and where
it exists, it is very fragmented.
Patchwork of types and methods of exchange exist which vary by
vendor, agency factors, and
local environmental factors. For example: although 45% are
connected to the Mass HIway, none
of the surveyed agencies use it for routine interoperability
needs.
3. Leadership and organization alignment with advanced payment
model goals appears to be a
key factor in adoption of EHR/HIE technology. At this point, not
all agencies have equal access
to advanced payment model opportunities, however, some type of
models are available to
virtually all agencies (e.g., bundled payments, etc)
4. Progress in EHR/HIE maturity is highly dependent on local
factors. A major driver is the
technology capability and requirements of key trading partners,
such as hospitals and physician
practices. Agencys query/retrieve and view capabilities are
highly dependent on actions and
motivations of these partners. As a result, each agencys roadmap
will need be adapted to these
local factors
5. Some core EHR/HIE technology functions should be adopted by
all home care agencies. This
would include the ability to send/receive Clinical Care
Documents (CCDs) through Direct
messaging capability via the Mass HIway or connected networks.
Additionally, having basic
send/receive capability will be important to all care
transitions
6. Choice of vendor may influence HIE capacity. 14 different
technology vendors were identified
in the survey, only 6 vendors have versions that are ONC
certified: Allscripts, Cerner, Epic, GE,
Healthwyse and McKesson.
-
5
The vendors that the responding agencies used were as
follows:
Vendor # Agencies
Healthwyse 7
Allscripts 4
Axxess 3
McKesson 2
Cerner 2
Homecare Homebase 2
Additional (only 1 agency per vendor) 8
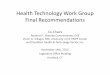
Chart A. Use of Electronic Communication by Responding
Agencies
-
6
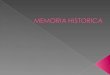
Chart B Type of Clinical Information Received Electronicaly
A. Summary of Key Findings by Category
1. LEADERSHIP & ORGANIZATIONAL ALIGNMENT
Key Findings: Leadership and staff buy-in on the transformation
of health care delivery models from fee-for-service to an outcomes/
value-based model is vital for bridging the transition of these two
models. An emphasis on quality care delivery, in a highly-reliable
model through integrated and interoperable systems across the
continuum is integral to this success. Leadership and
organizational alignment with advanced payment model is a key
factor in adoption of
EHR/HIE technology
Recommendations:
Leadership should identify patient outcomes of care and utilize
dashboards and benchmarks to facilitate staff understanding of the
shift from a fee for service model to an outcomes based model. Some
tools for informing staff on the value-based and alternative
payment models can be found at:
https://innovation.cms.gov/index.html
Leadership should identify the participation of trading partners
(hospitals, physician practices, post-acute partners) in
alternative payment models and seek alignment. Consider creating
care pathways with hospitals or providers participating in a
bundled-payment for a disease
-
7
which your organization offers stellar home care (i.e. CHF
bundle at hospital and tele monitoring in the home).
Leadership should determine if there are preferred provider
and/or integrated delivery networks within the agencys catchment
area and speak with point of contact to inquire about the
participation requirements, goals, quality metrics, and
benchmarking possibilities. Business plans and clear marketing
tools to portray clinical offerings are vital for care managers to
have access to when referral patients, ensure these are regularly
circulated and to the correct contacts.
Finally, leadership should monitor transformation funding
opportunities by subscribing to
pertinent mailing lists and regularly visiting leading funding
sources, such as Robert Wood
Johnson Foundation and the Department of Health and Human
Services grant website. State
funding opportunities for system redesign with technology as
integral for enabling care
innovation can be found through both the Health Policy
Commission and Massachusetts
eHealth Institute. Regularly exploring areas of potential grant
funding is necessary for many
agencies to invest in HIT.
2. INFRASTRUCTURE
Key findings:
All agencies have access to broadband internet.
Reliable, high speed internet is a prerequisite for a range of
technologies that can provide more cost-
effective and higher-quality care, such as telemedicine and
remote patient monitoring. This is especially
important for the providers who wish to participate in
alternative payment and care delivery reforms like
medical homes, bundled payments, and Accountable Care
Organizations, which are particularly likely to
depend on telemedicine and better communication capabilities to
succeed.
Recommendations:
Agencies with slow and/or unreliable internet connection should
consider speaking to your
service provider about increasing bandwidth. The Federal
Communications Commissions (FCC)
Connect2HealthFCC initiative provides a list of potential
federal funding sources for
telecommunication and broadband services. For more
information,visit:
https://www.fcc.gov/general/funding-broadband-enabled-health-care
Many organizations have a dedicated internet connection for
their electronic medical record.
Consider weighing the cost of setting up an additional
connection with the cost of wasted staff
time and frustration.
3. EHR & HEALTH INFORMATION EXCHANGE
Key findings:
Most agencies are documenting information electronically, but
many cannot electronically exchange data
with trading partners. There are EHR/HIE technology functions
that should be adopted by all home care
-
8
agencies, including ability to send and receive Continuity of
Care Documents through Direct messaging
capability via an HIE.
Recommendations:
All home health agencies should adopt Office of the National
Coordinator (ONC) certified
Electronic Health Records as soon as possible. Of those not
currently using an HER at the time of
the survey, 100% reported that they intend to in the near
future.
All home health agencies should take steps to connect to the
Mass HiWay. Only thirteen agencies
indicated that they were participating in the Mass HiWay.
(Details about connecting to the Mass
HiWay are provided in Appendix B.) The Mass HiWay relies upon
participants commercial
internet connectivity and does not utilize any private networks
or dedicated circuits.
4. USE OF ELECTRONIC TOOLS
Key Findings
Most agencies report using smart phones and or tablets for Point
of Care documentation. Almost all
agencies utilize an electronic order system and roughly 73% of
respondents regularly use electronic tools
for referrals and OASIS reporting.
Recommendations
Full adoption of a paperless, electronic- based system. Trading
partners want a single method
of sharing information. Faxing and mailing documents will be
obsolete in the near future
Provide all staff with electronic devices to communicate across
the continuum.
Implement telehealth programs for chronic disease management.
Most systems provide
alerts to agencies as well reports, which can be electronically
sent to physicians. MassHealth
may soon be reimbursing agencies for telehealth monitoring.
Utilize encrypted smartphones to send pictures along with
clinical information to physicians
for ongoing patient management and updating of orders.
5. IT STAFFING
Key Findings:
EHR vendors recognize the importance of attending to client
workflow and process changes, but most
agencies do not have the dedicated staff resources to make it a
cost-effective part of their
implementations. Most EHR vendors offer self-service tools such
as online videos and user groups.
-
9
Suggested Actions:
Low cost and/or free part-time workforce development programs
are available at a number of
Massachusetts institutions. Bristol Community College offers an
online program designed to
prepare a workforce of seasoned professionals with the requisite
knowledge able to assist and
support HIT adoption.
http://mehi.masstech.org/programs/workforce-development/bristol-
community-college-hitech-program.
Additional workforce development related programs are listed
here:
http://mehi.masstech.org/programs/workforce-development
II. Conclusions and Possible Next Steps:
The HCA Member Survey was undertaken in order: 1) to assess an
agencys readiness to use the Mass
HiWay, and 2) to provide individualized road maps for
participating agencies to connect to, and begin
sharing information via the Mass HiWay
Electronic connectivity to healthcare partners has been
identified as an essential strategy for sustainability
and success for home care going forward. Results from the Home
Care Alliance of Massachusetts HIE
Adoption Survey suggest that the industry may be ready, but that
many member agencies are not well
connected electronically to their referrers, physicians,
hospitals and other trading partners along the
healthcare continuum. Without the financial support of the
Federal Government, and other stakeholders,
home health agencies have been forced to rely on their own
financial resources to both adopt and
implement electronic health records. Many of the home health
EHRs do not communicate well with each
other and this has negatively impacted an agencys ability to
utilize communication across the continuum
through the use of a health information exchange.
Agencies who did participated in the survey received readiness
roadmaps. Other agencies as well as policy
makers should find this report useful as a means of assessing
their agencys and the industrys state of
readiness to begin utilizing the Mass HiWay to connect to their
trading partners across the continuum.
Possible Next Steps for HCA of MA:
Continue efforts to educate all member agencies on the
importance of electronic connectivity
Work with MAeHC and MeHi to assist all non-participating
agencies to access and utilize the Mass
HiWay
Engage funding sources to support home care agencies to adopt
electronic technologies
-
10
Appendix A
The MAeHC survey document.
Appendix B
Information on the Statewide Health Information Exchange (The
Mass HIway)
1. Overview
The Mass HIway is a state-wide Health Information Exchange (HIE)
that is open to all interested
providers, hospitals, and other organizations within the
healthcare community. Mass HIway offers two
services to support exchange of health information:
Direct Messaging: Secure point-to-point transport of electronic
patient health information among
healthcare organizations and authorized government agencies for
purposes of patient treatment,
payment, or operations.
Query and Retrieve: Relationship Listing Service (RLS) for
authorized healthcare organizations to locate
other healthcare organizations that hold records for a
particular patient. Medical Record Request (MRR)
service for initiating a query for a patients records.
The HIway is not a repository of health information, it is a
tool for sending secure health information
from one organization to another. Similar to package delivery,
the HIway reads only the address on the
message, it does not open the message content.
There are three regional presentations available for download
which provide a geographically focused
update on HIway active use:
Mass HIway Overview: Whats happening in My Community?
Southeast Region Presentation
Western Central Massachusetts Presentation
Northeast Region Presentation
2. Current HIway Participants and Provider Directory
Over 600 organizations are participating in the HIway, the full
list of participants is available here. If you
don't see your trading partner on this list, let the HIway team
know by emailing [email protected]
or calling 1-855-MA-HIway (624-4929) and pressing option 1.
-
11
The Participant list includes organizations that have signed a
Participation Agreement with the Mass
HIway and are either implementing or actively transacting. Use
this list to identify any organizations in
your referral circles are on the Mass HIway, then reach out to
them to discuss a potential use case for
the Mass HIway with your organization.
Some EHR vendors use a Health Information Service Provider
(HISP), providing a connection to the
HIway on behalf of their users. If your vendor allows you to
choose which HISP to connect to, you can
connect directly to the Mass HIway HISP. If your vendor requires
that you use their designated HISP,
you will have to connect to the Mass HIway through their HISP,
as long as their HISP is connected to the
Mass HIway.
If you are a member of a HISP that is connected to the Mass
HIway, contact your vendor representative
to discuss the steps to get connected to the Mass HIway network.
The following HISPs are connected
with the Mass HIway:
Aprima
Athenahealth
CareConnect (NetSmart)
Cerner
DataMotion
eLinc
eClinicalWorks
EMR Direct
Inpriva
MaxMD
MedAllies
Medicity
MyHealthProvider (Mercy Hospital)
NextGen Share
NHHIO
RelayHealth
SES
Surescripts
UpDox
Wellport (by Lumira)
3. Provider Directory Service
The Mass HIway Provider Directory (PD) is a look up tool to
locate a known contact at another
participating organization (i.e. locating Dr. X at facility Y).
In order to use the Mass HIway, all Participants
must provide contact addresses where departments or individual
staff can send and receive secure
communications.
-
12
Getting data in: Mass HIway provides the domain name and the
Participant provides the organization
information, individual addresses for their authorized users,
and the minimal data set required to power
the Directory.
For first time uploads into the Provider Directory, Participants
must supply this information using the
below documents. Once the initial upload is completed,
Participants must use the HIway Directory
Provider Upload file to submit new additions, changes, or
deletions.
4. Public Health Reporting
The Mass HIway enables the electronic submission of reporting
for public health registries to improve
public health research, intervention, and program development.
This allows for easier compliance with
applicable state laws and can also help providers earn
incentives in Stage 2 of Meaningful Use. For more
information on Meaningful Use and Public Health objectives and
steps to submit, click here.
The following state registries and applications are connected to
the Mass HIway:
1. Syndromic Surveillance (SS): State data submitted to the CDCs
BioSense program to identify excess morbidity and mortality.
2. Immunizations (MIIS): Supports compliance with state law
M.G.Lc.111, s.24M for submission of immunization data to the
Massachusetts Department of Public Health (MDPH). Click here for
official MIIS Regulations and here for the MIIS Compliance Schedule
(March 2015)
3. Electronic Lab Reporting (ELR) Supports electronic submission
of laboratory results to the MDPH Bureau of Infectious Disease to
meet regulation 105 CMR 300.170.
4. Cancer Registry (MCR): Provides an electronic means to
comprehensively identify and report cancer cases to the
Massachusetts Cancer Registry for further reporting to the CDC as
required by Massachusetts law.
5. Specialized Registry (MAVEN): Web based disease surveillance
and case management system. 6. Children's Behavioral Health
Initiative (CBHI) 7. Opioid Treatment Program (OTP) 8. Childhood
Lead Prevention Program (CLPP) 9. Intake Enrollment and Assessment
Transfer Service (IEATS): Supports electronic information
submission of provider data to evaluate client outcomes and
assure program effectiveness for opioid treatment services.
10. e-Referral: Supports health information exchange from
healthcare provider organizations to affiliated community-based
organizations.
5. Registry Interface Connections by Vendor *as of December
2015
MIIS: Allscripts, athenahealth, Cerner, eClinicalWorks, GE
Qvera, Netsmart, SMART, Surescripts
Opioid Treatment Program: Netsmart, SMART
eReferral: eClinicalWorks
Syndromic Surveillance: Cerner
6. Mass HIway Connection Options
-
13
There are several options to connect to Mass HIway: LAND,
Webmail, Direct, SOAP Web Services.
Determining which method is best will depend upon technical
capabilities of your system, the volume of
data you intend to transmit, and your use case. The below
information can help you decide the best
solution.
LAND
LAND allows for a high-volume connection to the Mass HIway with
multiple options for how messages are sent to the gateway and then
onto the HIway. This connection involves a physical piece of
hardware that is installed at the participating site and can then
be integrated into the participants infrastructure.
Benefits:
Supports high-volume and automatic/scripted message and data
dropping
Multiple options for integrating message transmission into a
Participants infrastructure (HTTP POST, Directory drop, and more)
to create minimal impact for non-technical users
Participant is not responsible for appliance maintenance or
installation
Considerations:
LAND appliance is a black box and cannot be accessed by
participant staff
Some configuration of the IT environment is required for
messages to reach the LAND, so Participant IT support is required
until connectivity is established
Installation and/or physical replacement of the box requires
Mass HIway staff to visit the site
Recommended for:
Participants who need to regularly send data or are expecting to
transmit a lot of messages but who do not have a dedicated IT staff
to manage their infrastructure
Larger sized Participants with an implemented EHR that is not
compatible with the Direct solution
Webmail
Webmail provides for communication on the Mass HIway through a
web browser, such as Internet Explorer or Firefox. Users log into a
website to receive and send messages manually. The user interface
looks very much like modern online mail sites (such as Gmail or
Yahoo) and has many of the same capabilities. Attachment files can
be sent through webmail and the communications are secure.
Benefits:
No hardware or software installs at the participant site; no IT
staff required
Non-technical interface for users; access through web
browser
Communication functions just like e-mail but is secure through
The Mass HIway
Considerations:
Configuring automatic uploads of clinical information requires
expert resources
Users manually check for received messages on an e-mail system
that is not integrated with their EHR
Recommended for:
-
14
Participants without a need to regularly send large volumes of
data but who would like to be able to send or receive clinical and
patient information securely on an ad-hoc basis
Direct Direct XDR and/or SMTP/SMIME is the most robust
connection option and allows for seamless integration into a
Participants system with the proper configuration. The direct
connection can interface directly with the participants EHR or SMTP
message sending service. The connection provides the largest
opportunity for the participant to integrate their HIway
connection, but requires the IT staff and infrastructure to manage
the connection.
Benefits:
Interfaces directly with EHR or other message sending software
given correct protocols on the Participant side
Can receive data files and/or messages directly from the
Participant's systems and transmit them automatically with proper
setup
Can be configured to deliver messages directly to the
Participants internal mail system to create a seamless experience
for end users
Considerations:
Established IT infrastructure must be present at the participant
site to implement the connection and install the secure
certificate(s)
Experienced IT staff is required to implement and integrate the
connection for use
Not all EHRs are compatible with the connection
Recommended for:
Participants who anticipate sending a lot of data or messages on
the Mass HIway and have a compatible EHR and/or a dedicated IT team
who can configure existing system to interface with the
connection
SOAP Web Services
SOAP is the alternative method of transport to and from the
Massachusetts Immunization Information System (MIIS). This method
uses a CDC standardized WSDL with local specifications. For more
details, on this transport method, visit the MIIS Resource Center
at https://www.contactmiis.info/crcnews.asp.
The MIIS is a secure web-based immunization registry and vaccine
management system for the Commonwealth of Massachusetts. Healthcare
providers can report immunizations to the MIIS directly through the
web interface or via electronic data exchange from their sites EHR
system and through the Mass HIway. HL7 messages are processed in
real time and acknowledgements are sent to the initiating system as
soon as the message processing is complete.
Benefits:
Executing a Mass HIway Participation Agreement (PA) is not a
requirement, which can speed up process of submitting data to MIIS
as it may take time to process at your organization. Instead, you
work only with the MIIS team, which will provide a username and
password- based connection to MIIS via SOAP.
-
15
Considerations:
SOAP Web Services are for data transmission to MIIS only.
Participants that connect to MIIS via SOAP will need an alternate
connection to the Mass HIway to send and receive data to other Mass
HIway Participants and all other public health registries.
Should you wish to migrate to a certificate-based Mass HIway
connection in the future to transact with other Mass HIway
Participants, your organization will need to complete a Mass HIway
PA first, then go through the steps of onboarding.
Mass HIway does not charge for any set up and related service
fees for any connection option, including SOAP Web Services, if the
Mass HIway is being used solely to send and receive data to and
from the MDPH.
Recommended for:
Organizations that are not already connected to the Mass HIway
and need to quickly transmit data to MIIS.
Organizations not ready operationally to manage a more technical
Mass HIway implementation.
Organizations not ready or able to execute a Mass HIway PA in
order to implement a certificate-based connection to the Mass
HIway.
Fees
7. HIway Rates/Fees
Mass HIway services are flexible to the services participants
access and to the ways in which these
services are deployed. Mass HIway pricing is designed around
this flexibility:
Participants may access Direct Messaging as a standalone
offering or combine with Query & Retrieve Services. As Query
& Retrieve is dependent upon a Participant's connectivity for
Direct Messaging, Query & Retrieve is not available as a
standalone service.
Participants may connect to the services directly through their
electronic health record if available, or through a Local Access
Network Device (LAND) appliance or via Webmail. Click here for more
information about each connection method.
Participants may access the services through a single node
(connection) or through multiple nodes.
Prices have two components: One time set up fee and annual
services delivery fee. The annual HIE
services delivery fee is based on the Participant's connection
type(s) and number of connections.
HIE services fees are fixed regardless of message volume,
message size, number of users or number of
underlying organizations. For example, a legal entity with
multiple sub-organizations (e.g. Integrated
Delivery Network) may purchase a single node and take
responsibility for all onward message handling.
Webmail fees are fixed per mailbox and subject to storage and
message size restrictions as noted in the
HIway Policies and Procedures.
-
16
A participant may pay fees on behalf of other organizations
(e.g. a small hospital that wants to buy Webmail accounts for
affiliated ambulatory practices).
Mass HIway encourages Technical Integrators to assist
Participants to connect to the Mass HIway. In general, the
Technical Integrator will not be charged a fee. However, a
Technical Integrator may pay fees on behalf of the Participants it
connects to the Mass HIway. If the Technical Integrator pays the
fee on behalf of the Participant, it will be considered a "Tier 1-
Multi Entity HIE" type. This rate allows a Technical Integrator to
connect as many Participants as they like. If Participant wishes to
act as a Technical Integrator on behalf of trading partners or
other related entities, and the Participant plans to pay on behalf
of the additional parties, the Participant would be charged the
"Multi Entity HIE" fee and will not be charged separately as a
Participant.
Mass HIway does not charge for HISP connections nor does it
charge organizations to connect to the Mass HIway via a HISP.
Mass HIway program costs are covered through a combination of
funds from the Centers for Medicare
& Medicaid Services (CMS), the state government, and
Participant fees. Mass HIway is highly subsidized
by CMS, and Participant fees and state funds allow Mass HIway to
meet the match requirement to
access these subsidies. The HIway rate card is below:
-
17
Tier Category Definition
Tier 1
Large hospitals/Health Systems: Large hospitals include teaching
hospitals and/or large health care delivery systems. Includes:
Baystate, Beth Israel Deaconess, Boston Medical Center, Cambridge
Health Alliance, Childrens Hospital of Boston, Dana-Farber Cancer
Institute, Lahey Clinic, MEEI, Mount Auburn Hospital, Partners,
Saint Vincent Hospital, Steward, Tufts Medical Center, UMass
Memorial. Small hospitals include all others. The list of Large
hospitals will be reviewed and may be updated annually.
Health Plans: Health insurance carriers.
Multi Entity HIE: Health Information Exchange (HIE) networks
that include more than one authorized legal entity (e.g., NEHEN,
SafeHealth, Wellport).
Commercial Imaging and Lab Centers: Standalone imaging and lab
centers as defined by Massachusetts state licensing and not
included in larger health systems.
Tier 2
Small Hospitals: Hospital or Healthcare systems not included in
list of Large hospitals/Health Systems above.
Large Ambulatory practices (50+): Practices with 50 or more
licensed providers (MD/DO/NP/PA) in a single legal entity
regardless of number of sites, and not otherwise included in larger
systems (i.e. not employed or owned by a hospital or health
system). Category does not include federally qualified health
centers (FQHCs) or FQHC look-alikes.
Large Long Term Care entities: Nursing homes or nursing home
systems with 500+ licensed beds (e.g., Kindred, Genesis, Golden
Living Center, Wingate, Life Care Centers, Epoch Senior Healthcare,
Radius Healthcare, Beaumont).
Ambulatory surgical centers: As defined by Massachusetts state
licensing.
Ambulance and Emergency Response: Standalone emergency medical
service providers as defined by Massachusetts state licensing and
not included in larger systems.
Business Associate Affiliates: Business associates of
participant covered entities.
Tier 3 Small Long Term Care entities: Nursing homes or nursing
home systems with
-
18
APPENDIX C
Project Team Members:
Micky Tripathy, Ph.D., MPP, President and CEO MAeHC
Jessica Hatch, MS, CNL, RN, Business Analyst
Jennifer Monahan, Business Analyst
Pat Kelleher, Executive Director, Home Care Alliance of
Massachusetts
Jeanne Ryan, MA, OTR, MBA, HIT, Home Care and Hospice
Consultant
Steering Committee Members (will receive by 2/15/16)
Tim Burgers Associate Director Home Care Alliance
Peg Doherty Vice-President Home Health VNA
Jim Ellsworth IT Systems Administrator Porchlight VNA
Judy Flynn Vice-President, Quality Partners Healthcare at
Home
Russ Duboc Chief Financial Officer Community VNA
Wendy Cofran Chief Information Officer Natick VNA
Judy Dionne Hospice Director Baystate VNA & Hospice
Ricardo Muchitti Chief IT Officer Metro West Home Care
Kate Mercier Quality Director Brockton, VNA
Additional References
1) MeHI Provider and Consumer Health IT, Research Study
(2014)
http://mehi.masstech.org/education/resources-tools/ehealth-reports/Survey2014-KeyFindings
2) Massachusetts Health Information Highway, (2015)
http://www.mass.gov/eohhs/gov/commissions-and-initiatives/masshiway/
3) Health Information Technology for Economic and Clinical
Health Act-HITECH (2009)
http://searchhealthit.techtarget.com/definition/HITECH-Act
4) Home Care Alliance of Massachusetts Strategic Plan
(2015-2017)
file:///C:/Users/Owner/AppData/Local/Microsoft/Windows/INetCache/IE/PD5N3M4Y/HCAM-2015-
2015-Strategic-Pla.pdf
-
19