Embed Size (px)
Citation preview

HCCA’s Resident ComplianceTraining
Debbie Troklus, CHC, Assistant VP for Compliance University of Louisville
Georgette Gustin, CPC, CCS-P, CHC, Director, PricewaterhouseCoopers

2
Agenda
Introduction & Background
Resident Teaching Section
Break
Resident Teaching Section
Lunch
Office of Inspector General Work Plan
Teaching Physician Regulations
Break
Case Studies and Questions/Answers

3
Introduction and BackgroundResident Education Program
To provide HCCA members and the industry with a comprehensive, inexpensive product that can be used to provide education to residents on a variety of compliance related topics
To provide tips/suggestions for implementing a system-wide resident education curriculum

4
Evolution & Development
HCCA conducted a member survey seeking input on what organizations are doing to educate and train residents on compliance topicsRespondents comments varied significantly
Organized training programs in mature state• Frequency, topics, in-person and/or web or video
based• Some are moving to specialty rotation training
Programs in infancy stages • Provide one-time orientation to compliance topics
each JulySome organizations are still developing their programs and have not implemented any training

5
Evolution & Development (cont.)
Identified and organized volunteers in July/August 2003Conducted brainstorming conference calls to develop a training program outline
Volunteers included representatives from a variety of backgrounds:
• Clinical, Legal, Regulatory, Compliance and Coding
Outline was prepared and section chairs appointedSection chairs coordinated development of contents and submitted “drafts”Draft sections were collated into master “prototype”

6
Evolution and Development (cont.)
Draft prototype binder/manual was reviewed by various content professionalsRevisions, formatting and final touches were madeMarketing materials developedProduction began and guide published June 2004Workshops scheduled (October, November, December 2004)

7
Research and Numbers
400 Major Teaching Hospitals and Health Systems126 Accredited U.S. granting Medical Schools and 16 Canadian23 AOA approved
Source: http://www.aamc.org

8
Research and Numbers (cont.)
Accreditation of Graduate Medical Education (ACGME)Private professional organizationResponsible for accreditation of over 7,800 residency education programsAccredits residency programs in 110 specialty and subspecialty areas of medicine
Residency Review Committees (RRC)Comprised 27 specialtiesAssists with developing & refining accreditation standards
Year Ending June 2004 144 Newly accredited programs
• 59 Specialties – Largest Group - Developmental Behavioral Pediatrics
» 19 Programs– Second Largest – Vascular Neurology
Year Ending June 30, 20058,202 programs, 104,754 filled positions
Source: http://www.acgme.org

9
Course Curriculum
Structured by sectionIntroduction to ComplianceFraud & AbuseBasic Coding & Reimbursement TerminologyBasic CPT coding and conventionsEvaluation and Management Coding and DocumentationDiagnostic coding concepts and Medical NecessityAcademic Medical Centers & Teaching HospitalsHIPAA/ConfidentialityAccreditation of Residency ProgramsAppendix A: Websites of InterestAppendix B: Sample Coding Tools/Pocket Cards

Section 1: Introduction to Compliance

11
Section 1: Introduction to Compliance
EthicsConflicts of InterestJoint Commission on Accreditation of Healthcare Organizations (JCAHO)

12
Section I:Introduction to Compliance: Ethics
What does this mean to the Resident?Clinical Ethics Definition
• Practical discipline that provides a structured approach to assist physicians in identifying, analyzing, and resolving ethical issues in clinical medicine
Ethical Responsibilities• Patient Choice• Patient/physician relationship
Regulatory Responsibility• Professional Ethics• Fiduciary Duties• Federal and State Regulations

13
Section I:Introduction to Compliance: Ethics Case Study
Resident authorizes a medical student to obtain and document the history and condition of a patient without supervision. The resident then tells the student to write a progress note and leave it unsigned.
What are the ethical concerns?

14
Section I:Introduction to Compliance: Conflicts of Interest
When does a conflict exist?When a Resident or other Employee’s personal interests or activities may influence his or her judgment in the performance of his or her job duties
Joint Commission on Accreditation of Healthcare Organization Standards (JCAHO) requires hospitals to be aware of potential conflicts

15
Section I:Introduction to Compliance: Conflict Situations
Accepting gifts from vendorsUsing your employer’s facilities for financial gainParticipating in activities that violate or might reasonably be perceived to violate any of the principles governing research may create a conflict of interest

16
Section I:Introduction to Compliance: Conflict Case Study
You have been chosen to decide which type of new scanner to purchase for your clinic. After speaking with several manufacturers, the rep for scanner “X” offers to fly you, the physician making the assessment, to a training seminar at a distant resort area for two days with all expenses paid.
Are there conflicts?

17
Section I:Introduction to Compliance: JCAHO
Independent not-for-profit organization which sets standards by which healthcare quality is measured in American and around the world.Requirement for hospitals to participate in MedicareStandards applied to all patient care giversProvision of care, treatment and services
Assessing patient needsPlanning care, treatment, and servicesProviding the care, treatment, and services the patients needsCoordinating care, treatment, and services

18
Section I: Introduction to ComplianceCMS Quality Initiative
The Doctors' Office Quality (DOQ) project is designed to developand test a comprehensive, integrated approach to measuring the quality of care for chronic disease and preventive services in the doctors' offices. The goals of the DOQ project are to:
to provide information for informed decision makingsupport and stimulate the adoption of quality improvement strategies by practitioners in doctors' offices
CMS is working closely with key stakeholders such as nationally recognized physicians associations, consumer advocacy groups, philanthropic foundations, purchasers, and quality accreditationor quality assessment organizations to develop and test the Doctors' Office Quality (DOQ) measurement set. This includes and is not limited to the American Medical Association (AMA), National Committee on Quality Assurance (NCQA), National Quality Forum (NQF), Robert Wood Johnson Foundation (RWJ) and others.

19
Section I: Introduction to ComplianceCMS Quality Initiative (cont.)
The DOQ measurement set has three components
Clinical performance measurement setPhysicians practice connections toolPatient’s experience of care survey
Source: http://www.cms.hhs.gov/quality/pfqi.asp

20
CMS Physician Focus Quality Measures

21
Physician Office Information Technology
Electronic Health Record (EHR) project, CMS is working with the Veterans Health Affairs (VHA) to transfer health information technology to the private sector. CMS is funding and collaborating with VHA and other key federal agencies on the development of a VistA-Office EHR version of the VHA's hospital VistA system for use in clinics and physician offices. An overriding goal of VistA-Office EHR is to stimulate the broader adoption and effective use of EHRs by making a robust, flexible EHR product available in the public domain.
Source: http://www.cms.hhs.gov/quality/pfqi.asp

22
Physician Office Information Technology (cont.)
This government collaboration is pursuing the goals listed aboveby:
Support for disease management in areas such as hypertension, coronary artery disease, and diabetes. This will include reporting clinical data to a CMS-sponsored clinical data warehouse for quality improvement purposes Enhance the registration process to meet the needs of the general population Enhance the functionality for Obstetrics/Gynecology (OB/GYN) and Pediatrics care Interface with practice management and billing systems Improve installation procedures
VistA-Office EHR is expected to be available July 2005 to support the Quality Improvement Organization activities aimed at improving quality in physician offices.
Source: http://www.cms.hhs.gov/quality/pfqi.asp

Section 2: Fraud & Abuse

24
Section 2:Fraud & Abuse
Federal Sentencing GuidelinesSeven Elements
Stark I and IIAnti-KickbackPharmaFalse Claims ActCivil Monetary Penalties

25
Section 2:Fraud & Abuse – Federal False Claims Act (FCA)
Applies to “any person” who “knowingly presents or causes to be presented”A “false or fraudulent claim for payment”To the “United States Government”“Knowingly” includes acting in “reckless disregard of truth or falsity of the information”“No proof of specific intent to defraud is required”

26
Section 2: Fraud & AbuseFederal Sentencing Guidelines and the Seven Elements
Created in 1984 by Congress to develop a federal sentencing structure that would diminish disparate treatment of criminal offendersSeven elements are the minimum standards for an effective compliance programAmendment revisions are due to become effective November 1, 2004
Corporate responsibilityEthicsMandatory Training

27
Section 2: Fraud & AbuseStark Law
Self-referral provision enacted in 1989Stark I – became effective January 1, 1992
Prohibits a physician from referring patients to a clinical laboratory in which the physician or a member of his or her immediate family has a financial relationship
Stark II – became effective January 1, 1995Expands the referral prohibitions to include not only clinical laboratory but also Designated Health Services (DHS)
• Prohibited Conduct• Designated Health Services• Financial Relationships• Exceptions• Penalties

28
Section 2: Fraud & AbuseStark Law
DHS includes:Clinical Laboratory ServicesPhysical Therapy, occupation therapy, and speech-language pathology servicesParenteral and enteral nutrients, equipments, and suppliesProsthetics, orthotics, and prosthetic devices and suppliesRadiology and certain other imaging servicesDurable medical equipments and suppliesOutpatient prescription drugsHome health servicesInpatient and outpatient hospital servicesRadiation therapy services and supplies

29
Section 2: Fraud & Abuse: Anti-kickback
Knowing and willful offer, payment, solicitation, or receipt of remuneration to induce (or in return for) the referral of Federal health care program business
OIG may seek up to $25,000 and imprisonment up to 5 years for each act (offer, payment, solicitation or receipt of remuneration), an assessment of up to three times the amount of the improper remuneration (without regard for whether a portion of the remuneration was for lawful purposes), and exclusion

30
Section 2: Fraud & Abuse: PhRMA
JAMA – January 19, 2000 – Vol. 283, No 3
Physician interactions with pharmaceutical representatives were generally endorsed, began in medical school, and continued at a rate of about 4 times per month
Meetings with pharmaceutical representatives were associated with requests by physicians for adding the drugs to the hospital formulary and changes in prescribing practice

31
Section 2: Fraud & Abuse: PhRMA (cont.)
JAMA Conclusion:
The present extent of physician industry interactions appear to affect prescribing and professional behavior and should be further addressed at the level of policy and education.

32
Section 2: Fraud & Abuse:PhRMA (cont.)
TAP Settlement
October 3, 2001Largest settlement to dateIn excess of $875 millionLupron issue

Section 3: Basic Coding and Reimbursement Terminology

34
Section 3: Basic Coding & Reimbursement Terminology
Resident’s need to become aware of the coding and reimbursement acronyms, abbreviations and standard terms that reflect the complexity of medicine
CPT DefinitionsHCPCS DefinitionsICD-9-CM DefinitionsReimbursement Terminology
• General, Hospital and PhysicianIntroduction to PayersMiscellaneous acronyms

35
Section 3: Basic Coding & Reimbursement Terminology (cont.)
Part B covers physician services, Durable Medical Equipment, outpatient hospital services, x-rays, lab tests, home health, ambulance, etc.Services provided in the clinic and hospital setting (office visits, admissions, daily care, surgical procedures, etc.)
Coding Classifications• Current Procedural
Terminology – CPT codes• ICD-9-CM Diagnosis Codes• HCPCS Level II Codes
Reported on CMS 1500 form

Section 4: CPT & Coding Conventions

37
Section 4: CPT & Coding Conventions
Define the various coding systemsCPT Coding Conventions
• Format and terminology• Modifiers
HCPCSICD-9-CM
National Correct Coding Initiative (NCCI)Medicare Fee Schedule
Relative Value Units (RVU)Geographic Practice Cost Indices (GPCI)

38
Section 4:CPT Coding Conventions
CPT® - is the American Medical Association’s Current Procedural Terminology, Fourth Edition (first level of HCPCS codes)
Published and updated annually by the AMA - proprietaryTransforms medical services and procedures into 5 digit numeric codesCommunicates “what” service was providedDivided into 6 major sectionsOver 8,200+ CPT codesContains 2-digit numeric modifiers

39
Section 4: CPT Coding Conventions HCPCS Level II Coding
HCPCS Level II - is the acronym for Healthcare Financing Administration Common Procedure Coding
National codes published annually by CMS and are public domainCodes consist of an alphanumeric code – a letter from A through V followed by four digits
• J1160, injection digoxin, up to 0.5 mg
Grouped by the type of supply or service they represent
• Home Health, Rehabilitation• Injections-Chemotherapeutic Drugs• Orthotics/Prosthetics• Durable Medical Equipment
Used by Medicare and private payers

40
Section 4: CPT Coding ConventionsHCPCS Codes

41
Section 4: CPT & Coding Conventions National Correct Coding Initiative (NCCI) Edits
Updated quarterlyVersion 10.3 (effective October 1, 2003)Over 800 new edits/code pairsCurrently there are 239,000 editsOriginally in 1996 total of 83,000 editsAverage Medicare saving per code pair edit is ~ $55.00Available on CMS website

42
Section 4: CPT & Coding Conventions National Correct Coding Policy

43
Section 4: CPT & Coding Conventions (CMS Medlearn Matters) www.cms.hhs.gov

44
Medicare Physician Fee Schedule DatabaseFederal RegisterRelative Value Units (RVUs)
Work, Practice Expense, Malpractice Conversion FactorGPCIs (Geographic Practice Cost Indices)
Professional, Technical and Total ComponentFacility vs. Non-facility SettingStatus Indicators
Section 4: CPT Coding Conventions Resource Based Value System (RBRVS)

45
Section 4: CPT Coding Conventions Resource Based Value System (RBRVS)
Relative Value Unit (RVU)Work, Practice Expense, Malpractice
Geographical Practice Cost Indices (GPCI)A GPCI reflects the relative costs of practice expenses, malpractice insurance, and physician work in an area compared to the national average for each component. Medicare payment will vary dependent upon the GPCI of a particular geographic region.
Conversion Factor (CF)Fee utilized to multiply the total RVU assigned to each CPT code to determine the fee assigned to the code.
Payment [(RVU work x GPCI work) + (RVU practice expense x GPCI practice expense) + (RVU malpractice x GPCI malpractice)] x Conversion Factor.

46
Section 4: CPT Coding Conventions Resource Based Value System (RBRVS)
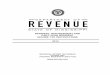
2004 National Physician Fee Schedule Relative Value File CPT codes and descriptions only are copyright 2003 American M edical Association. All Rights Reserved. Applicable FARS/DFARS Apply. Dental codes (D codes) are copyright 2002 American Dental Association. All Rights Reserved.REVISED 1/14/2004
FULLY FULLYIMPLEMENTED IMPLEMENTED
STATUS NON-FACILITY FACILITY GLOB PRE INTRA POST MULT BILAT ASST CO- TEAMHCPCS MOD DESCRIPTION CODE TOTAL TOTAL DAYS OP OP OP PROC SURG SURG SURG SURG11100 Biopsy, skin lesion A 2.12 1.23 000 0.00 0.00 0.00 2 0 1 0 019101 Biopsy of breast, open A 8.11 5.10 010 0.10 0.80 0.10 2 1 1 0 044320 Colostomy A 26.86 26.86 090 0.09 0.81 0.10 2 0 2 1 046260 Hemorrhoidectomy A 10.44 10.44 090 0.09 0.81 0.10 2 0 1 0 047605 Removal of gallbladder A 22.73 22.73 090 0.09 0.81 0.10 2 0 2 1 048152 Pancreatectomy A 66.94 66.94 090 0.09 0.81 0.10 2 0 2 1 050240 Partial removal of kidney A 34.11 34.11 090 0.08 0.83 0.09 2 0 2 1 052000 Cystoscopy A 5.53 2.91 000 0.00 0.00 0.00 2 0 1 0 068100 Biopsy of eyelid lining A 6.43 2.03 000 0.00 0.00 0.00 2 0 1 0 093975 26 Vascular study A 2.53 2.53 XXX 0.00 0.00 0.00 0 0 0 0 099203 Office/outpatient visit, new A 2.57 1.92 XXX 0.00 0.00 0.00 0 0 0 0 099213 Office/outpatient visit, est A 1.41 0.95 XXX 0.00 0.00 0.00 0 0 0 0 099223 Initial hospital care A 4.15 4.15 XXX 0.00 0.00 0.00 0 0 0 0 099233 Subsequent hospital care A 2.09 2.09 XXX 0.00 0.00 0.00 0 0 0 0 099238 Hospital discharge day A 1.87 1.87 XXX 0.00 0.00 0.00 0 0 0 0 099243 Office consultation A 3.23 2.47 XXX 0.00 0.00 0.00 0 0 0 0 099253 Initial inpatient consult A 2.61 2.61 XXX 0.00 0.00 0.00 0 0 0 0 0
Medicare Physician Fee Schedule 2004
Source: CMS Website (www.cms.hhs.gov)CPT ® Copyright American Medical Association

Section 5: Evaluation and Management Services

48
Section 5:Evaluation and Management (E/M) Services
American Medical Association (AMA) and the Centers for Medicare and Medicaid Services (CMS) developed Documentation Guidelines for E/M servicesFirst introduced early November 1994 with implementation January 1, 1995 with six month grace periodSpecialty specific single organ system (ten in total) and general multi-system exam introduced in 1997Both of sets of guidelines are acceptable Payers are to use those that are found to be most advantageous to the provider

49
Section 5:Evaluation and Management Services (cont.)
Commonly referred to as E/M or E&M services or visit codesCategorized by place of service (Hospital, Office, ER, SNF)Various “levels” of intensity for each category (1-5 in most cases, with “5” being the most intensive)Definitions for new and established patientsAll begin with “99” and are 5 digits Documentation requirements for various types and “levels” of service Requires history, physical examination and/or medical decision makingDescribes the “Who, Where, What, and Why”

50
Section 5:Evaluation and Management Services (cont.)
These services are reported with Current Procedural Terminology (CPT) codes 99201 -99499
Select the code which best:Describes the location and type of service provided; andExtent of the history, physical examination and medical decision making provided to the patient.
Medical record documentation should always support the category and level of service reported for billing
CPT codes & descriptions copyright AMA. Refer to CPT for complete definition.

51
Section 5:Evaluation and Management Services (cont.)
Office/Other OutpatientHospital ObservationHospital InpatientConsultationsEmergency DepartmentCritical CareNeonatal Intensive CareNursing Facility
Domiciliary, Rest Home or Custodial CareHomeCase ManagementPreventive MedicineNewborn CareSpecial Services
Each E/M service category has special instructions for use
CPT codes & descriptions copyright AMA. Refer to CPT for complete definition.

52
Section 5:Evaluation and Management Services (cont.)
New PatientEstablished PatientInitial CareSubsequent CareConsultations
Inpatient or OutpatientInitialFollow-upConfirmatory
Comprehensive Assessment (e.g., nursing home)Discharge ServicesAge-based (e.g., preventive medicine)Time-based (e.g., critical care, care plan oversight)
E/M Categories
CPT codes & descriptions copyright AMA. Refer to CPT for complete definition.

53
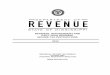
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
99241 99242 99243 99244 99245
Medicare Dr. A Dr. B Dr. C Dr. D
Section 5: Evaluation and Management Services Medicare E/M Bell Curve Sample Analysis

54Source: CMS Website (www.cms.hhs.gov)CPT ® Copyright American Medical Association

55Source: CMS Website (www.cms.hhs.gov)CPT ® Copyright American Medical Association

56Source: CMS Website (www.cms.hhs.gov)CPT ® Copyright American Medical Association

57Source: CMS Website (www.cms.hhs.gov)CPT ® Copyright American Medical Association

Section 6: Diagnosis Coding & Medical Necessity

59
Section 6: Diagnostic Coding Concepts & Medical Necessity
ICD-9-CM Coding ConventionsCoding for SpecificityAbbreviationsRule-out diagnosesV & E Codes
Facility CodingICD-10ResourcesMedical NecessityLimited Coverage
Local Medical Review PoliciesMedical Necessity and Level of E/M ServiceE/M Services Coded Based on TimeCertificates of Medical Necessity

60
Section 6: Diagnostic Coding Concepts & Medical Necessity / ICD-9-CM Coding Conventions
ICD-9-CM is the International Classification of Diseases, Ninth Revision, Clinical Modification
Updated annually in October by CMS and public domainContains 3, 4 and 5 digit codesContains diagnosis and procedure codesArranged by diseases, injuries, and causes of death according to established criteria 3 Volumes
• Volume 1 contains the Tabular List of Diseases and Injuries
• Volume 2 contains the Alphabetic Index of Diseases and Injuries
• Volume 3 includes the Tabular List and Alphabetic Index to Procedures – (used for facility billing)
Only Volumes 1 and 2 are used for physician professional servicesCommunicates “why” the service was provided

61
Section 6: Diagnostic Coding Concepts & Medical Necessity
42 CFR 482.24 (c) Providers must maintain records that contain sufficient documentation to justify diagnoses, admissions, treatments performed and continued care
Section 1862(a)(1)(A) of the Act states that no payment shall be made for any services which “..are not reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member.”
Documentation should always be date and patient specific

62
Section 6: Case Study - Class Discussion
Patient sees the physician in the clinic and is treated for an upper respiratory infection.
What type of information would the physician need to be provide in order to process the claim for payment?

Section 7: Human Subject Research

64
Section 7:Human Subject Research
Clinical Trial A controlled study involving human subjects, designed to evaluate prospectively the safety and effectiveness of new drugs, devices, or behavioral interventions and to identify any adverse events caused by these investigational agents
Human SubjectAn individual who voluntarily allows his physiologic or behavioral characteristics and responses to be the object of study in a research project
Extremely complex and highly regulated

Section 8: HIPAA & Confidentiality

66
Section 8: HIPAA & Confidentiality
HIPAA was passed in 1996Administration Section of Title II contains the HIPAA regulationsHIPAA affects most providers in every aspect of their daily practice
Privacy, Security and Transaction Code SetsThere are penalties for non-compliance
Civil – up to $100 for each violation with $25,000 annual limitCriminal – up to $50,000 and one year in jail: up to $250,000 fine and 10 years in jail for selling patient information

67
Section 8: Case Study – Class Discussion
Susie is responsible for checking patients in when they arrive at the clinic, as well as scheduling patients who call for appointmentsIt is a busy day at the office and one of the other receptionists is out ill Susie has patients lined up to check-in at the front desk and the phone is constantly ringingSusie answers the phone and puts the patient on hold, while she attempts to transfer the call to the nurse

68
Section 8: Case Study – Class Discussion (cont.)
In the meantime, her neighbor is the next person at the window waiting to check-inShe calls her out by name and makes the statement, “It is about time you get in here to take care of that mass on your leg”, “while you’re at it, tell Dr. Smith about the headaches and night sweats that you’ve been having too”Unknowingly, the patient who was “hold” was not on “hold” and overheard the entire conversation

69
Section 8: Case Study – Class Discussion (cont.)
Jim arrives home early from work before his wife.He receives a phone call from the Dentist office asking for his wife, Judy.He informs them that she is not home and inquires what the matter is about and if he can take a message.The receptionist informs Jim that she is not able to discuss the matter due to HIPAA and that his wife will need to call the office to discuss.

Section 9: Accreditation of Residency Program

71
Section 9: Accreditation of Residency Programs
Education program requires Residents to obtain competency in the following areas:
Patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health
Medical knowledge needs to be established through evolving biomedical, clinical and cognate sciences and their application of this knowledge to patient care

72
Section 9: Accreditation of Residency Programs (cont.)
Practice based learning and improvement which improves patient care through investigation and evaluation of their own patient care appraisal and assimilation of scientific evidence
Interpersonal and communication skills are taught so that they result in effective information exchange and collaboration with patient, their families, and other health professionals

73
Section 9: Accreditation of Residency Programs (cont.)
Professionalism, as manifested through a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population
Systems-based practice, as mentioned by actions that demonstrate an awareness of, and representative to the larger context and system and healthcare, and the ability to effectively call on system resources to provide care that is optimal in value

74
Section: 9Accreditation of Residency Programs (cont.)
Supervision of ResidentsAll patient care must be supervised by quality facultyFaculty schedules must be structured to provide residents with continuous supervision and consultation
Duty HoursClinical and Academic Activities related to the Residency ProgramLimited to 80 hours per week (averaged over a 4 week period), inclusive of all in house activities
MoonlightingActivities within the Scope of Program may not bill for services

75
Section: 9Accreditation of Residency Programs / Duty Hours
In July 2003, ACGME instituted a comprehensive approach that includes:
(1) standards for resident hours and institutional oversight(2) promoting compliance; and (3) Increasing knowledge on the effect of the standards and on
innovative ways to conduct education and patient care under limited resident hours.
ACGME considers duty hour limits an important element of its comprehensive approach to promote high-quality education and safe patient care.
Source: Accreditation Council for Graduate Medical Education, Report of the Work Group on Resident Duty Hours and the Learning Environment, June 11, 2002;
(http://www.acgme.org, accessed July 16, 2004).

76
Section: 9Accreditation of Residency Programs / Duty Hours (cont.)
The duty hour standards include:An 80-hour weekly limit, averaged over four weeks;An adequate rest period, which should consist of 10 hours of rest between duty periods;A 24-hour limit on continuous duty, and up to six added hours for continuity of care and education;One day in seven free from patient care and educational obligations, averaged over four weeks;In-house call no more than once every three nights, averaged over four weeks; andThe option for programs in some specialties to request an increase of up to 8 hours in the weekly hours, if this benefits resident education, with approval by their sponsoring institution and theResidency Review Committee (RRC) in the given specialty.
Source: Accreditation Council for Graduate Medical Education, Report of the Work Group on Resident Duty Hours and the Learning Environment, June 11, 2002;
(http://www.acgme.org, accessed July 16, 2004).

Overview of Appendices

78
Appendices
Internet ResourcesE/M Audit Worksheets
Incident-to Billing Psychiatry and Human BehaviorConsultationObservation CareSubsequent Care
E/M Coding ToolsGeneral Multi-system examCardiovascular examE/M Code Builder
E/M Progress Notes/Documentation TemplatesInfectious Disease, Psychiatry, OB/GYN, Podiatry, etc.

Office of Inspector GeneralFY 2005 Work Plan Overview

80
OIG FY 2005 Work Plan Physician Initiatives
Billing Service Companies
Review the relationships among billing companies and the physicians and other Medicare providers who use their services.
Identify the various types of arrangements physicians and other Medicare providers have with billing services and determine the impact these arrangements in the physician’s billings.

81
OIG FY 2005 Work Plan Physician Initiatives (cont.)
Medicare Payments to VA Physicians
Assess validity of Medicare reimbursement for services billed by physicians who receive remuneration from the Department of Veterans Affairs (VA) for the time the physicians reported as being on duty at a VA hospital.
Physicians employed by the VA may not bill Medicare for services rendered at other hospital’s during the times they were on duty at a VA hospital.

82
OIG FY 2005 Work Plan Physician Initiatives (cont.)
Care Plan Oversight
Evaluate the efficacy of controls over Medicare payments for care plan oversight (CPO) claims submitted by physicians.
Assess whether these services were provided in accordance with Medicare regulations.

83
OIG FY 2005 Work Plan Physician Initiatives (cont.)
Ordering Physicians Excluded from Medicare
Quantify the extent of services, if any, ordered by physicians excluded from Federal health care programs and the amount paid by Medicare Part B.
Under Federal regulation, physicians who are excluded from Federal health care programs generally are precluded from ordering or performing services for Medicare beneficiaries.

84
OIG FY 2005 Work Plan Physician Initiatives (cont.)
Physician Services at Skilled Nursing FacilitiesExamine Medicare Part A and Part B claims with overlapping services for skilled nursing facility patients and determine whether duplicate payments were made to either the physicians or nursing homes for the same patient services.Physicians may bill Medicare only for the professional component of a service on behalf of skilled nursing facility patients.The technical component of physicians’ services is covered under the patient’s Medicare Part B stay in the skilled nursing facilities and should not be billed separately by the nursing home.Under an exception to this rule, nursing homes may receive Part B payments for both the professional and technical components of physicians’ services if both parties have an agreement under which only the nursing home may bill and receive these Part B payments.

85
OIG FY 2005 Work Plan Physician Initiatives (cont.)
Physician Pathology Services
Focus on pathology services performed in physicians’ offices.
Pathology services include the examination of cells or tissue samples by a physician who prepares a report of his findings.
Medicare pays over $1 billion annually to physicians for pathology services.
Identify and review the relationships between physicians who furnish pathology services in their offices and outside pathology companies.

86
OIG FY 2005 Work Plan Physician Initiatives (cont.)
Cardiography and Echocardiography Services
Review Medicare payments for cardiography and echocardiography services to determine whether physicians billed appropriately for the professional and technical components of the service.
These services include both professional and technical components.
When the physician performs the interpretation separately, the modifier -26 should be used to bill Medicare for professional services.

87
OIG FY 2005 Work Plan Physician Initiatives (cont.)
Physical and Occupational Therapy Services
Review Medicare claims for therapy services provided by physical and occupational therapists to determine whether the services were reasonable and medically necessary, adequately documented, and certified by physician certification statements.
Physical and occupational therapies are medically prescribed treatments concerned with improving or restoring functions, preventing further disability, and relieving symptoms.

88
OIG FY 2005 Work Plan Physician Initiatives (cont.)
Part B Mental Health Services
Determine whether Medicare Part B mental health services provided in physicians’ offices were medically necessary and billed in accordance with Medicare requirements.
Payments for mental health services provided in the physicians’ office setting accounted for approximately 55% of the $1.3 billion in Medicare payments for Part B mental health services in 2002.
Medicare allowed $185 million for inappropriate mental health services in the outpatient setting.
OIG will determine the financial impact of claims that do not meet Medicare requirements.

89
OIG FY 2005 Work Plan Physician Initiatives (cont.)
Coding of Evaluation and Management Services
Examine patterns of physician coding of evaluation and management services and determine whether these services were coded accurately.
In 2003, Medicare allowed over $29 billion for evaluation and management services.
Prior work found a significant portion of certain categories of these services is billed with incorrect codes resulting in large overpayments.
Assess the adequacy of controls to identify physicians with aberrant coding patterns.

90
OIG FY 2005 Work Plan Physician Initiatives (cont.)
Use of Modifier -25
Determine whether providers used modifier -25 appropriately.Providers should not bill evaluation and management codes on the same day as a procedure or other service unless the evaluation and management service is significant, separately identifiable service from such procedure or other service.In 2001, Medicare allowed over $23 billion for evaluation and management services. Of that, approximately $1.7 billion was for evaluation and management services billed with modifier -25.Determine if these claims were billed and reimbursed appropriately.

91
OIG FY 2005 Work Plan Physician Initiatives (cont.)
Use of Modifiers with National Correct Coding Initiative Edits
Determine whether claims were paid appropriately when modifiers were used to bypass the NCCI edits.One of CMS’s tools for detecting and correcting improper billing, is designed to provide Medicare Part B carriers with code pair edits for use in reviewing claims.A provider may include a modifier to allow payment for both services within the code pair under certain circumstances.In 2001, Medicare paid $565 million to providers who included the modifier with code pairs within the NCCI edits. Determine whether modifiers were used appropriately.

92
OIG FY 2005 Work Plan Physician Initiatives (cont.)
“Long Distance” Physician Claims
Review Medicare claims for face-to-face physician encounters where the practice setting and the beneficiary’s location were separated by a significant distance.
While all beneficiaries may seek professional services for specialized consultation during leisure travel, those with ongoing illnesses requiring skilled nursing care would be unlikely to travel long distances from home.
Examine the claims to confirm that services were provided and accurately reported.
If warranted, we will recommend enhancements to existing program integrity controls.

93
OIG FY 2005 Work Plan Physician Initiatives (cont.)
Provider-Based Entities
Determine the extent to which health care entities that have been designated as “provider based” are in compliance with requirements for receiving this designation.
In prior work, found that hospital ownership of physician practices is widespread and that fiscal intermediaries are frequently unaware whether these hospitals are being treated as provider based or freestanding.
Medicare and it beneficiaries may be paying excessive amounts for services inappropriately billed as provider based.
Determine the impact on Medicare reimbursements of entities billing as provider based instead of freestanding.

94
OIG FY 2005 Work Plan Other Initiatives
Medical Necessity of Durable Medical Equipment
Determine the appropriateness of Medicare payments for certain items of DME, such as power wheelchairs and therapeutic footwear.
Assess whether the suppliers’ documentation supports the claims, whether the item was medically necessary, and whether the beneficiary actually received the item.

How to Train Residents

96
How To Train Residents
For years physicians have been told:“You must attend this session—it is mandatory.” “You will learn how to code and document your services in accordance with the guidelines and regulations.”
Do physicians really learn and/or change behaviors when they are taught in this type of environment and under these types of circumstances?
How can an organization modify the approach it has taken in the past to design educational programs that will be effective and well attended?

97
Convincing Physicians of the Value of Compliance
“Physicians view compliance as a tedious, arbitrary and unrealistic
compendium of stupid rules, made up by mindless bureaucrats who
have never practiced medicine --designed
to waste my time, threaten andpunish the
innocent, and undermine my profession.”
- Mark Pfeifer, MD, U of Louisville School of Medicine, 4/98

98
Educational Approaches
Traditional approachGroup IndividualShadowing
Modified and streamlinedWeb-basedNewsletters
FrequencyMonthly/Department MeetingsAnnual

99
Educational Approaches (cont.)
Shift to “tie” into other initiativesResearchQualityCost ManagementHospital services
Using data and quality indicatorsProfilesBenchmarkingQuality Outcomes

100
AAMC Survey Results (December 2003)
Question #12: What approaches have you found to be the most effective in attaining increased proficiency in documentation and coding?
Using their own notes when educating seems to help as well as providing them documentation guides that they can carry around with them or post in the dictation roomRounding with physicians while seeing inpatientsShadowing them for a day or half-day an explaining to them real-time with patients that they just saw how to appropriately document for the services they just deliveredOngoing, frequent department monitoringTraining and more training, peer pressureIndividual interaction Tools such as laminated cards, exam templates, etcProblem-based educational sessions
Number of Respondents: 32Source: AAMC E/M Survey on Audits – 12/2003

101
AAMC Survey Results (December 2003) – cont.
Question #12:Continuous training, Support from peer physician leadersRegular communication via e-mail, newsletters, or group sessionsSmall sessions, specialty-specific, individual audit resultsBy reporting deficiencies and providing actual case examples to the physicians and requiring a corrective action planPersonalization, specialization, templates and being positive (while doing what you must do)Group sessions, (grand rounds, department faculty meetings, sub-specialty group meetings, faculty presenting to faculty one-on oneInteractive sessions
Number of Respondents: 32Source: AAMC E/M Survey on Audits – 12/2003

102
Critical Success Factors
#1—Gaining internal sponsorship#2—Understanding the objectives of the education project#3—Creating a master template#4—Relating to the adult learner#5—Applying critical training techniques#6—Planning#7—Conducting a dress rehearsal

103
Critical Success Factor #1
Gaining internal sponsorship from physicians/residents and other health care professionals:
Identify physician/resident “champions” who will work with you to:
• formulate the compliance message• communicate with the organization’s
physicians/residents and other health care providers
• emphasize the program’s importance• encourage or require participation• respond to questions, issues, or problems

104
Select champions who are:• respected by colleagues• viewed as leaders• supportive of the organization’s compliance
missionUse champions’ time wisely:
• seek their input on compliance message/materials• enlist their support in encouraging attendance• request their presence and participation at all
sessions
Critical Success Factor #1 (cont.)

105
Critical Success Factor #2
Understanding the objectives of the education project:What is the message?Why is it important?Who should hear it?How will the audience benefit (what’s in it for them)?How should the sessions be structured?What will the organization achieve?
Group education versus individualized training:Classroom (didactic) One-on-one sessionsShadowing physicians
“Seek first to understand before you can be understood”Stephen Covey

106
Survey the target audience(s) to identify:• their challenges and issues—“buy-in”• preferred meeting days and times—attendance• options for session types and material—session
formatEnsure the message meets organizational needs:
• physician “champion” review• leadership approval
Communicate benefits when advertising sessions
Critical Success Factor #2 (cont.)

107
Critical Success Factor #3
Identify the message and objectivesCreating a master template for the session materials will:
Ensure a consistent message is delivered across all sessions and specialtiesAllow you to customize applicable portions of the material without creating a whole new presentationSave an enormous amount of time and effort

108
Critical Success Factor #3 (cont.)
Use tools to help relay conceptsDeliver messages in small sound bites:
Incorporate the “Sevens Rule”:• no more than seven lines or seven words per
conceptBe cognizant of using abbreviations, acronyms, and/or mnemonicsUse analogies, anecdotes, and/or props

109
Prepare an outline for the master templateDevelop a draft document:
• thoroughly check references and research cited to support key points
• ensure the document follows the outline• review contents with physician/resident
champions and organization leadershipIncorporate issues identified during your survey of the target audience
Critical Success Factor #3 (cont.)

110
Critical Success Factor #4
Relating to the adult learner:Engage participants in the learning processTailor the message to the audienceCreate opportunities for audience participationReinforce retention by:
• telling them what you are going to tell them• telling them• telling them what you told them

111
Critical Success Factor #5
Applying critical training techniques:Learning styles:
• auditory:– role-play– review cases
• visual:– show them– use graphs, overheads, pictures, illustrations,
etc.• kinetic:
– get them moving– hands-on experience

112
Identify ways to encourage audience participation:
• question/answer sessions• case example workbooks• group or team discussions/exercises
Incorporate case examples to illustrate key points:• specialty-specific documentation (e.g., progress
notes, operative reports)• samples of actual vs. benchmark code
distribution• recent chart review findings
Critical Success Factor #5 (cont.)

113
Critical Success Factor #6
Planning all aspects of the education project is key to its success:
Devote time to Critical Success Factors #1–#5Identify key participants in mission-critical areas and define their roles in preparing and delivering the sessionsDevelop realistic project timelines:
• begin with the end in mind (Stephen Covey)• monitor progress
If possible, obtain continuing education units to include in duty hours

114
Allowing sufficient time to develop a high-quality program
Identifying the trainers:• internal or external?• qualifications, including public speaking and
training capabilitiesUsing appropriate technology:
• program management and scheduling software• presentation media
Critical Success Factor #6 (cont.)

115
Critical Success Factor #7
Conducting a dress rehearsal:Ensures trainers thoroughly understand all materials and case examplesAllows you to identify possible issues with materialsEnables trainers to practice using equipment, handouts and other documentationIdentifies potential logistical issues

116
Have trainers:• present each session type to physician/resident
champions, compliance officers, and others• practice responding to possible questions and
issuesEvaluate and revise session contents, flow, and/or materials, as necessaryProvide feedback to trainers:
• body language, voice, eye contact, responsiveness to questions, etc.
Critical Success Factor #7 (cont.)

117
Best Practices
Determine educational learning objectivesDefine the structure of the sessions (didactic, individual, etc.)Engage physician/resident champions throughout the process:
Beginning—identify compliance messageMiddle—review materials, get the word outEnd—participate in sessions, respond “peer to peer”
Advertise the sessionsScheduling:
Minimize impact on patient careUtilize regularly scheduled meeting times when possibleDon’t overbook the trainer

118
Best Practices (cont.)
Logistics:Book appropriate meeting spaces with proper set-up for type of session and number of attendeesEnsure necessary equipment is scheduled and in working order (e.g., laptop, projector)Provide refreshments
Documentation:Sign-in sheetsEvaluationsContinuing education credits

119
Best Practices (cont.)
Limit session contents to material that can be covered in one to two hours, including questionsUse specialty-specific case examples to:
Tailor each sessionEngage the audience
Have a physician/resident champion and a compliance office representative at each sessionInclude coder and biller representatives as well as management from each clinical areaSummarize frequently asked questions in an “FAQ” document and post on the organization’s intranet

120
Using an Outside Vendor
Consider outsourcing the education program if:There is not enough staff to maintain the compliance schedule as well as develop and deliver the sessionsThe program is very large, complex, or sensitive in natureThe organization does not have compliance educators on staff or the staff don’t have training experience or established credibility
Evaluate vendors’ qualifications:Specialty-specific experienceNumbers and types of sessions deliveredEvaluations from previous clients

121
Best Practice Tips Resident Education
Gain internal supportIdentify and involve key stakeholdersDefine learning objectives Allow adequate time for up-front planningPrepare meaningful materials Provide reference toolsConduct post-education reviews
“I am always ready to learn although I do not always like to be taught”
—Winston Churchill

122
Case Study # 1
You have just been appointed to take over as the Compliance Officer for your organization which has 250 faculty physicians and 85 residents.The organization is comprised of 2 hospitals, various physician clinics, a reference laboratory and a skilled nursing facility.You are in the process of analyzing previous compliance activities and data that had been prepared by your predecessor.In doing so, you identify that all Residents receive an Introduction to Compliance training session during their initial orientation each July. It appears that there was no subsequent education throughout the year. How would you propose to train the Residents throughout the next year and on what topics?

123
Case Study # 2
AMC with 450 faculty and 400 residents 16 clinical departmentsResidents staff the AMC’s 13 primary care clinics Residents do rotations at six local hospitals throughout the community including the VA and the State’s Mental Health FacilityResidents do rotations at many physician offices and emergency rooms throughout the community
Given the information below please design an education program utilizing the HCCA tool as we have discussed.

Teaching Physician Regulations

125
Teaching Physician Regulations
BackgroundProblems with IL-372 Intermediary Letter (1969)
Subject to InterpretationNo consistent enforcement throughout CMS regions or from state to stateNo standard audit plan from carrier to carrierRelied upon a single physician as the attending
July 1996, CMS issued standard Teaching Physician Guidelines, Section 15016November 22, 2002, CMS issued Transmittal 1780 which clarifies the documentation guidelines for E/M services

126
Teaching Physician Regulations: Definitions
Teaching HospitalHospital engaged in an approved GME residency program in medicine, osteopathy, dentistry, or podiatry
Teaching SettingAny provider, hospital-based provider, or nonprovidersetting in which Medicare payment for the services of residents is made by the FI under the direct GME payment methodology or freestanding SNF or HHA in which payments are made on a reasonable cost basis
Teaching PhysicianA Physician (other than a resident) who involves residents in the care of his or her patients
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

127
Teaching Physician Regulations: Definitions
Resident
An individual who participates in an approved GME program or a physician who is not in an approved GME program who is authorized to practice in a hospital setting. The term includes interns and fellows in GME programs recognized as approved for purposes of direct GME payments made by the FI. Receiving a staff or faculty appointment or participating in a fellowship does not by itself alter the status of “resident”, Additionally, the status remains unaffected regardless of whether a hospital includes the physician in its full time equivalency count of residents
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

128
Teaching Physician Regulations: Definitions
Medical Student
A student is NEVER considered to be an intern or resident. Medicare does not pay for any service furnished by a student
Medical Students must be personally supervised by a teaching physician/resident/fellow
Only the Review of Systems, and Past, Medical/Family, and Social History may be referred to by the Teaching Physician
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

129
Required for the “KEY PORTION” of the service or procedureDefined differently depending on the “type” of service or procedure:
• Evaluation and Management (E/M) Services (time based codes)
• Surgery (minor, single, overlapping)• Complex or High Risk Procedures• Radiologic or Other Diagnostics• Anesthesia• Endoscopy• Psychiatry
Teaching Physician Regulations: Presence and Participation
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

130
Teaching Physician (TP) must “personally” document PARTICIPATION and INVOLVEMENT in patient care
Physically present means the TP is located in the same room (or partitioned or curtained area if the room is subdivided to accommodate several patients) as the patient and/or performs a face-to-face service
The Teaching Physician (TP) is required to personally document at least the following:
Documentation that supports the TP performed the service or was physically present during the critical or key portions of the service when performed by a resident; andParticipated in the management of the patient
Teaching Physician Regulations: Presence and Participation
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

131
The documentation required of the TP is critical to substantiate that his/her personal services were provided
Resident documentation of the presence and participation of the TP is not sufficient to establish the TP’s presence and participation
The combined entries into the medical record by the TP and resident must support the medical necessity of the service.
Teaching Physician Regulations: Presence and Participation
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

132
“I performed a history and physical exam of the patient and discussed the management with Dr Resident. I reviewed Dr. Resident’s note and agree with the documented findings and care.”
“I saw the patient with Dr. Resident and agree with the his/her findings and plan.”
“I saw and evaluated the patient. Agree with Dr. Resident’s note but lower extremities are weaker now 3/5 order MRI of spine.”
Teaching Physician Regulations:Minimally Accepted Documentation
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

133
Co-signature only of resident’s note by the TP
“Seen and agree”
“Agree with resident’s plan”
“Agree with above”
“Rounded, Reviewed, Agree”
“Discussed with resident. Agree.”
“Patient seen and evaluated”
Teaching Physician Regulations:Examples That Do Not Establish Presence
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

134
Teaching Physician Regulations:Documentation
Defined as notes recorded in the patient’s medical records by a resident and/or TP or others as outlined in specific situations regarding the service furnishedDocumentation may be dictated and typed, hand-written or computer-generated, and typed or hand-writtenMust be dated and include a legible signature or identity Must identify at a minimum the service furnished, the participation of the TP in providing the service, and whether the TP was physically present
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

135
Teaching Physician Regulations:Scenario # 1
TP personally performs all of the elements of the E/M service without the resident
In the absence of a note by the resident the TP must document as he or she would document an E/M service in a non-teaching setting
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

136
Teaching Physician Regulations:Scenario # 2
The resident performs the elements required for an E/M service in the presence of, or jointly with, the TP and the resident documents the service
In this case, the TP must document that he or she was present during the performance of the critical or keyportion(s) of the service and that he or she was directly involved in the management of the patient
TP’s note should reference the resident’s note
The composite of the TP’s entry and the resident’s entry together must support the medical necessity and the level of the service billed by the TP
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

137
Teaching Physician Regulations:Scenario # 3
The resident performs some or all of the required elements of the service in the absence of the TP and documents his/her service.
The TP independently performs the critical or key portion(s) of the service with or without the resident present and, as appropriate, discusses the case with the resident.
In this instance, the TP must document that he or she personally saw the patient, personally performed critical or key portions of the service, and participated in the management of the patient.
TP’s note should reference the resident’s note.
The composite of the TP’s entry and the resident’s entry together must support the medical necessity of the billed service and the level of the service billed by the TP.
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

138
Teaching Physician Regulations:Medical Student Documentation
The only documentation made by medical students that may be used by the TP is their documentation of the ROS and PFSH
The TP may not refer to a medical student’s documentation of physical exam findings or medical decision-making in the TP’s personal note
Any contribution and participation of a student to the performance of a billable service (other than the review of systems and/or past family/social history which are not separately billable, but are taken as part of an E/M service) must be performed in the physical presence of a TP or physical presence of a resident in a service meeting the requirements for TP billing.
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

139
Teaching Physician Regulations:Primary Care Exception Rule
The Teaching Physician’s physical presence requirement may be waived for certain residency programs that qualify for the primary care exception rule:
Family PracticeGeneral Internal MedicineGeriatric MedicinePediatrics Obstetrics and GynecologyPsychiatry (may qualify in special situations)
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

140
Teaching Physician Regulations:Primary Care Exception Rule
Applies only to the following outpatient lower and mid-level E/M services:
99201 - 99203 New Office/Outpatient visits 99211 - 99213 Established Office/Outpatient visits
The exception rule does not apply to inpatient E/M services, procedures or any other servicesTP may not supervise more than four residents at any give time and must direct care from such a proximity to constitute immediate availability
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

141
Teaching Physician Regulations:Minor Procedures
General Rules
Minor procedures are not defined within CPTMedicare characterizes minor procedures as those taking only a few minutes to complete (5 minutes or less) and involve relatively little decision-making once the need for the procedure is determined
TP must be present for the entire procedure in order to bill for the service
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

142
Teaching Physician Regulations: Minor Procedures
Documentation requirementsMay be provided by resident, nurse, or personally by the TPIf the resident provides the documentation, an attestation should be written
Examples of attestations“Procedure performed with (by) Dr. TP.”
“Dr. TP was present during the entire procedure.”
“Dr. TP observed me perform this procedure.”
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

143
Teaching Physician Regulations:Surgical (Including Endoscopic Operations)
TP surgeon is responsible for the preoperative, operative and post-operative care of the patient
TP’s presence is not required during the opening and closing of the procedure
TP surgeon determines which post-operative visits are considered to be key or critical and require his/her presence
During the non-critical or non-key portions of the surgery, if the is TP is not physically present, he/she must be immediately available to return to the procedure (cannot be performing another procedure)
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

144
Teaching Physician Regulations:Surgical (Single)
Single Surgery
If the TP is present during the entire period between opening and closing of surgical field, then his/her presence may be demonstrated:
• By notes made by resident or nurse, with a countersignature of TP
or• Personally by the TP
There is no required documentation that TP must note in record
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

145
Teaching Physician Regulations:Surgical (Overlapping)
Overlapping CasesThe TP must be present during the key portions of both procedures
Key portions must not occur at the same time
The TP must personally document:• What the “key portions” were• His/her presence during the “key portions” • His/her immediate availability for the rest of the
procedure
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

146
Teaching Physician Regulations: Surgical (Overlapping)
Two overlapping surgeries are acceptable for billing, as long as presence, participation and documentation guidelines are met
Two concurrent surgeries are not acceptable for billing (e.g., closing one surgery while in the “key portion” of another surgery)
Three concurrent surgeries constitutes supervision; these procedures are never billable
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

147
Teaching Physician Regulations: Endoscopies
Requirements:Presence is required by the TP during entire viewing portion including insertion and removal of the scopeViewing starts at the time of insertion of the endoscope and ends at the time of the removal of the endoscopeViewing of the entire procedure through a monitor in another room does not meet the TP presence requirementDocumentation of procedure should state that the TP was present for the entire period or performed the procedure
• Documentation may be made by residents or nurses with countersignature by TP, or
• The statement may be made personally by the TP
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

148
Teaching Physician Regulations:High Risk and Complex Procedures
For high risk or complex procedures, the TP must:
Be present for all critical and key portions of a single procedure or two “overlapping” procedures
Determine what the critical and key portions of the high risk or complex procedure
Be immediately available for all non-critical portions
Not observe via a monitor in another location - this is not acceptable for billing purposes
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

149
Teaching Physician Regulations: High Risk and Complex Procedures (cont.)
Examples of High Risk/Complex Procedures:Interventional radiology and cardiology services Cardiac catheterizationCardiovascular stress testsTransesophageal echocardiographyHyperbaric Oxygen Therapy (TP must be present for entire service)ArthrogramsMyelogramsEP Studies
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

150
Teaching Physician Regulations:Maternity Care
Ob/Gyn-specific Teaching Physician rules state:
TP physical presence requirements for both vaginal and Cesarean deliveries is to be consistent with those of other surgeries
If the TP was only involved in the delivery, only bill the “delivery only” code
In order to bill for global care, the TP must be present for the minimum number of visits indicated in the code description
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

151
Teaching Physician Regulations:Anesthesia
Single procedureTP must document in the medical records that he/she was present during all critical (or key) portions of the procedureTP’s physical presence during only the pre-opertaiveor postoperative visits with the patient is no sufficient to receive Medicare payment,
Concurrent proceduresTP is involved in more than one case with more than one resident or with a resident and a non-physician anesthetist, this is consider medical direction
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

152
Teaching Physician Regulations:Psychiatry
Presence of the TP during the service may be met by concurrent observation of the service through the use of one-way mirror or video equipmentAudio-only equipment does not satisfy the physical presence requirementTime-based services such as psychotherapy the TP must be present for the period of time for which the claim is made
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

153
Teaching Physician Regulations:Interpretation Diagnostic Radiology/Other Tests
The interpretation must be performed or reviewed with a TP
If the TP’s signature is the only signature present on the interpretation, Medicare assumes he/she is indicating that he/she personally performed the interpretation
If a resident prepares and signs the interpretation, the TP must indicate that he/she has personally reviewed the image and the residents interpretation and either agrees with it or edits the findings
Medicare will not pay for an interpretation performed by a resident that contains only a TP countersignature
Source: CMS, Medicare Carrier Manual Transmittal 1780, November 22, 2002

154
Teaching Physician Regulations:Case Study # 1
Resident sees the patient at 8:15 a.m. and performs and documents an expanded history, problem focused exam and low complexity medical decision making
TP documents “Patient seen and examined, agree with Resident’s plan of care”

155
Teaching Physician Regulations:Case Study # 2
Patient presents to the clinic with knee pain
Resident examines the patient and determines that the patient is in need of a joint injection
Resident administers 40 mg of Kenalog into the right knee
TP discusses the case with the resident and agrees with plan of care
Resident completes the encounter form and checks off an established patient level three and the joint injection code
TP reviews and signs the form

156
Teaching Physician Regulations:Case Study # 3
Operative Report includes the following information:
Date/Patient’s Name/DemographicsName of Procedure (hip replacement) / Pre-operative Diagnosis (degenerative joint disease)Surgeon: Teaching Physician NameAssistant Surgeon: Resident NameSummary of procedure and outcomeProcedure dictated by Resident with statement indicating TP was present for the key critical portionsTyped TP signature block that is blankTranscriptionist initials and date present

157
Teaching Physician Regulations:Case Study # 4
Family Practice Residency Clinic12 Residents and 8 Teaching Physicians who staff the clinic Monday through Saturday3 Nurse Practitioners and 1 Physician Assistant Approximately, 100-120 patients are seen each dayWhat type of staffing arrangements are necessary in order to support the clinic operating under the Primary Care Exception rules?

158
Questions and Answers
Visit: hcca-info.org

159
Enthusiasm Goes a Long Way …
“What goes on in the mind is what determines the outcome. When an individual really gets enthusiasm, you
can see it in the flash of the eyes, in the alert and vibrant personality.
You can see it in the verve of the whole being. Enthusiasm makes the difference in one’s attitude
toward other people, toward one’s job, toward the world. It makes the big difference in the zest and delight of human existence.”
—Dr. Norman Vincent Peale

160
References
DiResta, Diana. Knockout Presentations, How to Deliver Your Message with Power, Punch and Pizzazz.Dunaway, Tray, M. “Health care language translation errors.” Compliance Today,Health Care Compliance Association, December 2002.Gustin, Georgette. “Tips to Presenting Technical Information to a Nontechnical Audience.” Journal of Health Care Compliance, October 2001.Hart, Kathy, Paul Magalian. “Audit, Individualized Training Dramatically Increase Physician Compliance.” Journal of Health Care Compliance, March-April 2001.http:www.oig.gov.hhshttp:www.presentersuniversity.comJeary, Tony. Inspire Any Audience.Knapp, Daniel. “Eight Time-Proven Presentation Tips.” Program Manager, Jan/Feb 99.Moffatt, Lauren. “Seven Steps for Using Scarce Resources to Deliver Education Sessions.” Journal of Health Care Compliance, July-August 2002.Medicare Carriers ManualOffice of Inspector General FY 2005 Work PlanHCCA Residents Guide to ComplianceCMS WebsiteACGME Website