Embed Size (px)
Citation preview

HCV Drug Resistance:
Regulatory Perspective
Patrick Harrington, PhD
Senior Clinical Virology Reviewer
Division of Antiviral Products, FDA/CDER
2016 HIV and Hepatitis Clinical Pharmacology Workshop
Washington, D.C.
Disclosures: none
1

Disclaimer
The views expressed in these slides are those of the
presenter and do not necessarily represent official
policy of the Food and Drug Administration.
2

Presentation Outline
• Review of basic HCV antiviral drug resistance
concepts
• Impact of HCV polymorphisms on treatment
efficacy in DAA clinical trials, and considerations
for pre-treatment resistance testing
• Perspective on re-treatment for DAA-
experienced patients
3

HCV Drug Resistance Basic Concepts and Definitions (1)
Baseline polymorphism
Major natural genetic variant that is present in the viral population of a
minority of infected individuals.
“Major” means detectable by Sanger population sequencing or at a
comparable sensitivity level by Next Generation Sequencing (generally at
least 10-15% of sequence reads).
Not to be confused with a low abundance minority variant present in viral
quasispecies.
Treatment-emergent substitution
Amino acid change that emerged or became enriched in the viral
population with treatment.
4

HCV Drug Resistance Basic Concepts and Definitions (2)
Resistance-associated polymorphism or substitution
Amino acid variant that is associated with treatment failure with a DAA or
regimen, or associated with phenotypic resistance to a DAA.
The presence of a resistance-associated polymorphism or substitution in a
viral population does not necessarily mean a drug is ineffective.
Drug resistance barrier
Describes the potential for drug resistance selection.
Generally reflects the number and type of viral genetic changes that confer
resistance to a clinically relevant concentration of the drug.
5

Drug Resistant Virus Often Pre-Exists(Example from Rong, Perelson et al., 2010)
• HCV: 1012 virions produced each day in an individual.
• Replication error rate: 10-5 to 10-4 per nucleotide (i.e., 0.1 to 1 change per
genome per round of replication).
• Do the math→ all possible single and combinations of double
nucleotide mutant viruses preexist in the quasispecies before
treatment, and additional mutations arise early during therapy.
• Many early generation HCV DAAs have a low barrier to resistance:
impacted by single amino acid changes in the target protein.
• Drug resistant virus preexists and is rapidly selected by monotherapy.
• Combinations of drugs with non-overlapping resistance mechanisms
prevent drug resistance selection because they collectively have a higher
resistance barrier than the individual drugs.
6

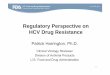
Monotherapy with a Low Resistance Barrier
Drug Selects for Resistance
Schiffer et al., Nat Med 2011
Dvory-Sobol et al., AAC 2012
HCV RNA decline during monotherapy “unmasks” and enriches drug resistant virus
Green=low dose, Pink=mid dose,
Purple=high dose
7

Examples of Early Low Resistance
Barrier IFN-Free DAA Regimens
8Zeuzem et al., Hepatology (2012) 55, 3: 749-58
GS-9256 + Tegobuvir(PI + Non-Nuc)
GS-9256 + Tegobuvir + RBV(PI + Non-Nuc + RBV)
Lok et al., NEJM 2012; 366:216-224

Highly Effective (>90% SVR Rates) IFN-
Free Regimens(HCV Treatment Guidelines Spring 2016)
9
DAA Combination DAA Class(es)Genotype
Coverage
Sofosbuvir + RBV NS5B Nuc. Analogue Polymerase Inhibitor 2
Ledipasvir/Sofosbuvir ± RBV NS5A Inhibitor/
NS5B Nuc. Analogue Polymerase Inhibitor
1, 4, 5, 6
Ombitasvir/Paritaprevir/
ritonavir ± Dasabuvir ± RBV
NS5A Inhibitor/NS3 PI/
NS5B Non-Nuc. Polymerase Inhibitor
1, 4
Daclatasvir + Sofosbuvir ±
RBV
NS5A Inhibitor/
NS5B Nuc. Analogue Polymerase Inhibitor
1, 2, 3
Simeprevir + Sofosbuvir ±
RBV
NS3 PI/
NS5B Nuc. Analogue Polymerase Inhibitor
1
Elbasvir/Grazoprevir ± RBV NS5A Inhibitor/NS3 PI 1, 4

Impact of HCV Polymorphisms on
Efficacy of DAA-based Regimens
10

Impact of HCV Polymorphisms on
Efficacy of DAA-based Regimens
• Many IFN-free DAA combinations can be impacted by the presence
of polymorphisms in drug target genes.
• The clinical impact of HCV polymorphisms is influenced by other
factors that also impact treatment efficacy, such as patient disease
characteristics (e.g., cirrhosis), the activity and resistance barrier for
other drugs in the regimen, and treatment duration.
• The presence of a DAA resistance-associated polymorphism does
not preclude the use of the DAA.
• Optimized/intensified DAA regimens (e.g., additional DAAs, ribavirin,
and/or longer treatment duration) can overcome the presence of
polymorphism(s) in drug target genes.
11

12
To screen or not to screen for
polymorphisms...Favoring Screening Screening Not Necessary
Clear impact on efficacy No clear impact on efficacy
Significantly impacts U.S. populationVery low (<<5%) overall virologic failure
rates in population
Assay commercially available No commercially available assay
Reasonable alternative treatment options
available (including waiting)
Alternative treatment options
not available
Resistance consequences of failure Minimal resistance consequences of failure
Limited or no re-treatment options Reasonable re-treatment options available
Clinical consequences of failure Minimal clinical consequences of failure
Factors Generally Not Considered
Cost
Complicating the treatment algorithm

Resistance testing is relatively simple
Response-Guided Therapy
13
Cirrhosis Determination in Trials (e.g.)
Resistance Test
Test: NS5A
Substitution Detected: Y93H
Afdhal N, Reddy KR, Nelson DR, et al. N Engl J Med 2014;370:1483-93.
VA boceprevir treatment algorithm

14
To screen or not to screen for
polymorphisms...Favoring Screening Screening Not Necessary
Clear impact on efficacy No clear impact on efficacy
Significantly impacts U.S. populationVery low (<<5%) overall virologic failure
rates in population
Assay commercially available No commercially available assay
Reasonable alternative treatment options
available (including waiting)
Alternative treatment options
not available
Resistance consequences of failure Minimal resistance consequences of failure
Limited or no re-treatment options Reasonable re-treatment options available
Clinical consequences of failure Minimal clinical consequences of failure
Factors Generally Not Considered
Cost
Complicating the treatment algorithm

Key factors that contributed to label recommending screening for Q80K:
• GT1a Q80K polymorphism substantially reduces efficacy of SMV + P/R
• High prevalence of Q80K in U.S. (48% of GT1a)
• Resistance consequences of failure: Emergence of R155K (or others)
• Boceprevir and telaprevir not impacted and represented alternative treatments
15
Simeprevir + P/R: GT1a NS3 Q80K
D.Deming, FDA Clinical Virology review of simeprevir

• Q80K associated with reduced efficacy in non-cirrhotic GT1a patients for 8-week duration
but not with 12-week duration
Longer treatment duration reduces impact of Q80K
• Q80K associated with reduced efficacy in cirrhotic GT1a patients treated for 12 weeks
Disease status influences clinical impact of Q80K16
Simeprevir + Sofosbuvir: GT1a Q80K
Sarrazin C., 2016. J Hepatol.

• Relapse rates -2% to +20% in those with baseline PMs versus those without
• Greatest efficacy impact associated with use of “less intense regimens”, presence of
multiple key NS5A polymorphisms, and/or presence of polymorphisms that reduce LDV
activity by >100-fold (Zeuzem et al., AASLD 2015).
• Impact of PMs minimized with regimens recommended in labeling: 12 weeks for most
patients, 24 weeks for cirrhotic tx-exp.; 8-weeks considered if low BL HCV RNA
L.Naeger, FDA Clinical Virology review of ledipasvir/sofosbuvir
LDV/SOF: NS5A PMs and Relapse Rates
17
Trial (GT1) Regimen No NS5A PM With NS5A PM
ION-3
(tx-naïve)
LDV/SOF 8W 4.8% (8/167) 6.3% (3/48)
LDV/SOF 12W 1.9% (3/158) 0% (0/56)
LDV/SOF + RBV 8W 3% (5/167) 8.2% (4/49)
ION-2
(tx-exp.)
LDV/SOF 12W 2.3% (2/86) 22% (5/23)
LDV/SOF 24W 0% (0/90) 0% (0/19)
LDV/SOF + RBV 12W 3.4% (3/89) 4.5% (1/22)
LDV/SOF + RBV 24W 0% (0/91) 0% (0/19)

OBV/PTV/r + DSV (GT1a)
• Low estimated impact (~0-8%) of NS3 Q80K or NS5A polymorphisms in Phase 2b/3 trials
• Label-recommended regimens maximize efficacy for all subjects regardless of baseline
polymorphisms: 2-3% VF rate overall for GT1a
Recent retrospective analyses showed NS5A polymorphisms and NS3 Q80K did not
impact efficacy of label-recommended regimens (Sulkowski et al., CROI 2016)
P.Harrington, FDA Clin. Virology review of OBV/PTV/r+DSV
18

Daclatasvir + Sofosbuvir (GT3)
• Clear impact of Y93H polymorphism
• Low or no NS5A inhibitor resistance consequence of failure
– No other major NS5A resistance-associated substitutions emerged in failures
who already had the Y93H polymorphism
– Y93H alone confers >3,000-fold reduction in DCV activity
• At the time, assay for screening was not commercially available and
alternative treatment options were not ideal.
P.Harrington, FDA Clin. Virology review of daclatasvir
19

Elbasvir/Grazoprevir
20
Impact of NS5A Resistance-Associated Amino Acid Polymorphisms on Efficacy
of EBR/GZR ± RBV for HCV GT1a Infected Subjects
• Clear impact of NS5A polymorphisms (present in ~10-12% of GT1a subjects),
although impact variable by NS5A position
• Nearly all virologic failures with these NS5A polymorphisms gained additional
treatment-emergent, resistance-associated substitution(s) in NS3 and/or NS5A
• No signal of virologic failure among subjects w/ or w/o NS5A polymorphisms
treated with EBR/GZR + RBV for 16 weeks (small #s w/ polymorphisms, but
challenging group)
T. Komatsu, FDA Clin. Virology review of elbasvir/grazoprevir

21
EBR/GZR for HCV GT1a:
NS5A PolymorphismsFavoring Screening Screening Not Necessary
Clear impact on efficacy No clear impact on efficacy
Significantly impacts U.S. populationVery low (<<5%) overall virologic failure
rates in population
Assay commercially available No commercially available assay
Reasonable alternative treatment options
available (including waiting)
Alternative treatment options
not available
Resistance consequences of failure Minimal resistance consequences of failure
Limited or no re-treatment options Reasonable re-treatment options available
Clinical consequences of failure Minimal clinical consequences of failure
Factors Generally Not Considered
Cost
Complicating the treatment algorithm

EBR/GZR Label
22
• First example where pre-treatment screening for resistance-associated
polymorphisms is recommended to guide optimal use of an IFN-free regimen
• AASLD/IDSA treatment guidelines consistent with prescribing information

Daclatasvir/Sofosbuvir ± RBV GT1aImpact of NS5A Polymorphisms
• Signal that NS5A polymorphisms (same 4 NS5A positions as EBR/GZR) may impact
treatment efficacy in HCV GT1a infected subjects with cirrhosis, although very few subjects
• Additional tx-emergent NS5A and/or NS5B substitutions in 3 of 4 virologic failures
• Evidence from other trials/populations that DCV-based regimens impacted by NS5A PMs
• Evidence from other trials that disease status can influence the impact of BL PMs
• Not a well-supported alternative to EBR/GZR-12W for GT1a compensated cirrhotic patients
with NS5A polymorphisms
23
P. Harrington Clin. Virology review of daclatasvir
Population
SVR12 with
Polymorphism(s)
SVR12 without
Polymorphism(s)
Subjects with Child-Pugh A/B Cirrhosis1 2/6 (33%) 38/39 (97%)
Subjects without Cirrhosis 9/9 (100%) 72/72 (100%)
Subjects Post-Transplant 2/2 (100%) 28/29 (97%)
1No subjects with Child-Pugh C cirrhosis had NS5A resistance polymorphisms

Daclatasvir Label (GT1)
24
• Not consistent with AASLD/IDSA guidelines for HCV GT1a infected patients with compensated cirrhosis, which recommend a longer DCV/SOF ± RBV duration of 24 weeks irrespective of NS5A polymorphisms (“Alternative regimen”)

Clinical Relevance of BL Phenotype (?)• Baseline phenotypic resistance may be associated with
reduced clinical efficacy, but lack of a baseline phenotype
does not preclude clinical relevance.
• Two NS5A examples illustrate relationship between
baseline phenotype, clinical impact, and treatment-
emergent substitutions
– Elbasvir/Grazoprevir 12W: GT1a L31M
• SVR rate: 38% (5/13)
• 0.5-fold impact in stable replicon assay, 10-fold in transient assay
• “High fold-change” according to AASLD/IDSA tx guidelines
– Daclatasvir/Sofosbuvir 12W: GT3a Y93H
• SVR rate: 54% (7/13)
• 3,733-fold impact on activity 25

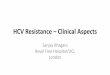
Phenotypic Impact of Clinically
Relevant NS5A Polymorphisms
0,001
0,01
0,1
1
10
100
GT1a EC50 GT1a EC50(Serum-Adj)
GT1a-L31M EC50(Serum-Adj)
Elb
as
vir
Co
nc
en
tra
tio
n (
nM
)
26
EBR/GZR treatment failure in GT1a
subjects with NS5A PMs associated with
additional emergent NS5A substitutions
DCV/SOF treatment failure in GT3 subjects
with Y93H generally not associated with
additional emergent NS5A substitutions
0,001
0,01
0,1
1
10
100
1000
GT1a EC50 GT3a EC50 GT3a-Y93HEC50
Da
cla
tas
vir
Co
nc
en
tra
tio
n (
nM
)EBR Plasma
C24
DCV Plasma
C24

How can a polymorphism without a clinically
relevant phenotype still be clinically relevant?
Wild-type Predominant L31M Predominant
No Resistance PM
L31M (Sensitive)
NS5A Resistant(L31M + Other Subst)
NS5A Resistant +NS3 PI Resistant
27
Absolu
te Q
uantity
of H
CV
Popula
tion (
log)
What leads to failure
No NS3+NS5A resistant virus
present

Re-Treatment Following
DAA Failure
28

29
Re-Treatment Following DAA Failure
Combination DAA Treatment Outcome
Must Address These Challenges:
1. Baseline characteristics that reduced efficacy of 1st line DAA regimen, such as:
Poor IFN/immune status and IL28B unfavorable genotype
HCV GT 1a or GT3
High HCV RNA levels
Natural drug resistance polymorphisms
Advanced disease
Poor drug PK
Poor adherence or tolerability
2. AND…
Treatment-emergent DAA resistance
(possibly across multiple classes)
Any further disease progression or
other comorbidities

Effective Strategies for
DAA Re-treatment• More potent, non-cross-resistant regimen (e.g.,
Sofosbuvir + NS5A inhibitor ± RBV in P/R + PI Failures)
• Intensified regimen (e.g., add RBV or additional DAA,
longer duration)
• Combinations of novel DAAs with activity against DAA-
resistant viruses: promising efficacy results emerging in
DAA failure populations (including NS5A failures)
30

Remaining Questions
• Impact of resistance-associated polymorphisms/
substitutions and need for resistance testing in DAA
combination regimen failures
• Optimal re-treatment for HCV GT3 infected patients who
failed an NS5A inhibitor
• Scope of GT4 and GT6 subtype diversity and impact on
DAA efficacy
• Optimal treatment for patients with advanced cirrhosis +/-
resistance-associated polymorphisms/substitutions
31

Thanks to the following FDA/DAVP
HCV DAA review team members...
Clinical Virology Reviewers
Damon Deming, PhD
Eric Donaldson, PhD
Takashi Komatsu, PhD
Lalji Mishra, PhD
Lisa Naeger, PhD
Jules O’Rear, PhD, Team Leader
Clinical Reviewers
Sarita Boyd, PharmD
Wendy Carter, DO
Sarah Connelly, MD
Russ Fleischer, PA-C,MPH, Acting TL
Poonam Mishra, MD, Dep. Dir. Safety
Adam Sherwat, MD, Team Leader
Kim Struble, PharmD, Team Leader
32
Debbie Birnkrant, MD, Division Director
Jeffrey Murray, MD, MPH, Deputy Division Director




















![Hepatitis C virus: Virology, diagnosis and treatment · VIROLOGY HCV life cycle[21-23] HCV is a small enveloped RNA virus belonging to the family Flaviviridae and genus hepacivirus](https://img.pdfslide.net/doc/110x75/5f0ab3cd7e708231d42ceb92/hepatitis-c-virus-virology-diagnosis-and-treatment-virology-hcv-life-cycle21-23.jpg)


![CCO HCV Resistance Slides[1]](https://img.pdfslide.net/doc/110x75/544b3b46b1af9f1a508b4a13/cco-hcv-resistance-slides1.jpg)