Embed Size (px)
Citation preview

HCV in People who Inject Drugs (PWID)
Christian B. Ramers, MD, MPH, AAHIVS Assistant Medical Director – Research/Special Populations
Family Health Centers of San Diego

Disclosures
Speakers Bureau: Clinical Care Options (HIV), Janssen Therapeutics (HIV), ViiV (HIV), Gilead Sciences (HIV, HCV), AbbVie (HCV), Bristol-Myers Squibb (HCV)
Scientific Advisor: Gilead Sciences (HIV, HCV), Janssen Therapeutics (HCV), Bristol-Myers Squibb (HCV)
Grant/Contracted Support: California Dept of Public Health, UNM Project ECHO, CDC/HRSA, Pacific AETC, HealthHIV, California HIV Research Program (CHRP), Gilead Sciences
Employer: Family Health Centers of San Diego

Learning Objectives
At the end of this lecture, you will be able to:
• Describe the epidemiology of HCV in PWID
• Identify unique challenges in treating PWID
• Describe clinical trials including PWID
• Review Guidance on mgmt of HCV in PWID

– Injected once?
– Injects regularly?
– Injects occasionally?
– Last injected 35 years ago?
– On stable OST and no longer injects?
What do we mean by PWID?
Larney S, et al. Int J Drug Policy 2015;26:9507; Grebely J, Dore GJ. Antiviral Res 2014;104:62–72.
• NSP: needle/syringe programme;
• OST: opioid substitution therapy;
• PWID: people who inject drugs
Lifetime PWID
OST
NSP
Active PWID

Epidemiology

•3-4 million new infections/yr
•150-180 million infections worldwide
Estimated HCV Prevalence: Global
> 10% 2.5%-10%
1%-2.50%
Prevalence of infection
NA
World Health Organization 2008 (http://www.who.int/ith/es/index.html), Razavi et al AASLD 2013

Estimated HCV Prevalence in PWID Worldwide (millions)
Grebely J, Dore GJ. Antiviral Res 2014;104:62–72.
No evidence of injecting drug use
No eligible report (74 countries)
<40% (16 countries)
40–<60% (24 countries)
60–<80% (25 countries)
≥80% (12 countries) Global estimate: 10.0 million PWID (range 6.0–15.2)
Global prevalence: 67.0% of PWID
W Europe: 0.73 E Europe: 2.35
E/SE Asia: 2.64 South Asia: 0.35
S America: 1.02
N America: 1.67
Australia New Zealand: 0.10
Sub-Saharan Africa:† 0.80
Middle East N Africa: 0.06
Central America: 0.15
Prevalence of HCV in PWID
..

Estimated chronic HCV Prevalence: US
• NHANES1: 2.7-3.2 million
• Adjusted for homeless, institutionalized, prisoners, military2: 5-7 million
Denniston MM et al Ann Intern Med. 2014; 160:293-300, Chak E, et al. Liver Int. 2011;31:1090-1101,
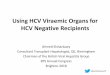
• Declining Prevalence of HCV Ab (1.3%) AND HCV RNA (1.0%)

NHANES Survey: United States, 1988-1994 and 1999-2002
Prevalence of HCV Antibody, by Year of Birth
Armstrong GL, et al. Ann Intern Med. 2006;144:705-14.
Year of Birth
HC
V P
reva
len
ce
(%)
1910
1988–1994
1999–2002
7.0
6.0
5.0
4.0
3.0
2.0
1.0
0
1920 1930 1940 1950 1960 1970 1980 1990
1945-1965

Hepatitis C Incidence in United States, 1982-2010
CDC MMWR 2010
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010
Nu
mb
er
of
Cases
Estimated New Infections

How is IDU contributing to HCV Epidemiology?
• Estimated 60% of prevalent HCV in US in current or former IDU’s1, 2
• Estimated 29,718 new infections in 2013
– 80% of incident HCV in PWID
• 3.8 Million have injected heroin at least once
– 425,000 have injected in the last year
• 289,000 actively injecting
• 64% of PWIDs are infected with HCV
1. Litwin AH, et al. Clin Infect Dis. 2005;40:S339-S345. 2. Grebely J, et al. Clin Infect Dis. 2013;57:1014-1020 3. CDC. MMWR. 2012;61:1-43 4. SAMHSA. National Survey on Drug Use and Health Report. September 4, 2014. 4. CDC. MMWR. 2015:64:1-7.

Increasing Incidence of HCV in Young PWID
MMWR. May 6, 2011:60; 17:537-541.

HCV testing at FHCSD – 12 month Results
Ramers C et al CROI abstract #661– Seattle, WA, Feb 24-27, 2015

Suryaprasad AG et al CID 2014, CDC, MMWR 2011, CDC MMWR 2015

Indiana HIV Outbreak - 2015
Brooks J – CROI 2016 – Boston, MA

Management Challenges in PWID

Very few PWID treated in IFN era
597
418
86 56
26 5
0
100
200
300
400
500
600
HCV antibody+ve
Aware oftreatment
Discussed withprovider
Agreed to starttreatment
Initiatedtreatment
Sustainedvirologicalresponse
Mehta SH, et al. J Community Health 2008;33:126–33.
n=237
Num
ber
of P
WID
<10% of PWID with HCV antibody positive were cured

PWID who receive HCV treatment ETHOS: 5 OST clinics, 2 CHCs, 1 aboriginal center in New South Wales, Australia, 2009–2012
Alavi M, et al. Clin Infect Dis 2013;57:S62–9.
387
236
191
84
0
100
200
300
400
500
600
Assessed by nurse Referred tospecialist
Attendedspecialist
appointment
Startedinterferon-based
treatment
Num
ber
of patie
nts
61% 49%
22%
100%

Reasons for Non-Engagement
Bamvita JM, et al. Hepat Res Treat 2014;2014:631481; ; Salvalaggio G, et al. SAGE Open 2013; doi:10.1177/2158244013509252. Harris, M. Hepatitis C testing & treatment for PWID: Barriers and Facilitators.
Alcohol consumption
Homeless or living in temporary accommodation
(shelters, prison)
Poorly educated (secondary education or less)
Poor quality of life
Limited access to healthcare
Use of multiple substances
“I am treated as a criminal and this makes it hard to take care of my health”
“There are no friendly healthcare services near where I live”
“I cannot get opioid substitution therapy/syringes because it is illegal”
“I would like to give up drugs, but I cannot get help”
“Healthcare workers do not trust me, as if I just want drugs”
“Without clean needles and syringes, I have to share”

Pt-reported Barriers in OST & NSPs
Feller S, et al. AASLD 2013; Oral #274.
Fear of judgement by doctor
0
20
40
60
80
100
No insurance
Can’t afford to pay
Can’t afford
transportation
Treatment will make me sick
Fear of liver
biopsy
Feel fine without
treatment
Patients
(%
)
Self-reported barriers to care among HCV-positive PWID (n=117)*

Reasons for non-referral/non-treatment in a testing/linkage program in Denver
0 10 20 30 40 50 60
Muething L, et al. ID Week 2015, Poster #1029.
•
• Individuals born 1945–1965 were screened for HCV and HCV evaluation, and treatment courses were followed prospectively from January 2013–March 2015. PWID: people who inject drugs
Reaso
ns n
ot
refe
rred
t
o H
CV
care
Reaso
ns n
ot
treate
d f
or
HC
V
Mental illness
Referral declined
Lost to follow-up
Medical disease
Not documented
Substance abuse
Mental illness
Substance abuse
Medical disease
Work on-going
Lost to follow-up
Not advanced liver disease
11
14
14
29
46
55
4
4
8
9
23
28
Number of HCV-infected individuals
• Most common reasons: substance abuse and co-morbid medical disease.

Clinical Trials of HCV treatment in PWID

Retrospective analysis: ION-1, -2, -3: patients on stable OST
• No differences between OST and non-OST participants:
– Overall SVR12 (94% vs. 97%, p=0.29)
– Adherence to LDV/SOF ≥80% (94% vs. 96%, p=0.33)
– Proportion with AEs (89% vs. 80%, p=0.07)
• No cases of HCV reinfection were observed up to SVR24
Jacobson I, et al. AASLD 2014; Poster #1945.
8 weeks 12 weeks 24 weeks 8 weeks 12 weeks 24 weeks
LDV/SOF+RBV LDV/SOF
SV
R 1
2 (
%)
0
10
20
30
40
50
60
70
80
90
100
Patients not receiving OST Patients receiving OST
94 100 97 94 99 91
93 100
97 91 99 100
196/ 209
6/6 492/ 508
29/31 311/ 315
10/11 195/ 210
6/6 308/ 317
10/11 320/ 323
5/5
. IFN: interferon; LDV: ledipasvir; OST: opioid substitution therapy;
SOF: sofosbuvir; RBV: ribavirin; PWID: people who inject drugs

High SVR12 for pts on OST with OMV/PTV/RTV + DSV + RBV
Lalezari J, et al. J Hepatol 2015;63:364–9.
97 97 97
0
20
40
60
80
100
37/38 37/38 37/38
EOT SVR4 SVR12
Virolo
gic
al r
esponse (
%)
Phase 2, open-label, single arm study of OMV/PTV/RTV + DSV for 12 weeks in GT 1 adult patients on stable OST with methadone or buprenorphine (N=38)

Grazoprevir/Elbasvir x 12 weeks in pts on OST (C-EDGE CO-STAR)
92 94 93 92
20
0
20
40
60
80
100
All GT GT 1a GT 1b GT 4 GT 6
Dore G, et al. AASLD 2015 Oral #49.
SVR
12
(%
)
Phase 3, randomised, double-blind study in PWID on OST with GT 1, 4 or 6 (n=201)
17 patients did not achieve an SVR
– 7 cases of relapse
– 5 cases of re-infections
– 5 patients were lost to follow-up or discontinued due to events unrelated to treatment failure
184/201 144/154 28/30 11/12 1/5

ELB/GRZ x 12 weeks in pts on OST – C-EDGE CO-STAR: Adherence
100 99 97
0
20
40
60
80
100
Dore G, et al. AASLD 2015 Oral #49.
>80% (>67 doses)
>90% (>76 doses)
>95% (>79 doses)
Adhere
nce (
%)
Phase 3, randomised, double-blind study in PWID on OST with GT 1, 4 or 6
Number of missed doses
Number (%) patients
0 153 (76.9)
1 23 (11.6)
2 8 (4.0)
3 8 (4.0)
4 1 (0.5)
≥5 6 (3.0)
Adherence Missed doses
99% (199/201) patients completed 12 weeks of treatment with grazoprevir/elbasvir
Majority of patients (97%) missed 3 doses or fewer
Around 60% patients tested positive for illicit drug use during the study
199/199 197/199 192/199

High SVR12 for PWID in Community setting
Norton BL et al CROI 2016
121 consecutive patients from urban FQHC in the Bronx
HCV Care Coordinator responsible for scheduling, reminder calls, prior authorizations
Outcomes compared between People who use drugs (Opiate substitution therapy or positive Urine tox screens)

HCV Re-infection rates in PWID

Pooled estimate of HCV reinfection risk for PWIDs1:
2.4 (95% CI 0.9–6.1) per 100 person-years
• Reinfection rates among PWIDs may be higher:
• In communities with high HCV prevalence2
• For young PWIDs3-5
• For active injection drug users3-5
Reinfection Rates Are Low Among PWID (‘ever’ injectors)
Reinfection Rates Among Persons Who Ever Injected Drugs Per 100 Person-Years2
Australia 4.70
Germany 3.94
Netherlands 0.76
USA 2.63
Norway 0.80
Canada 3.20
1. Aspinall EJ, et al. Clin Infect Dis. 2013;57(suppl 2):s80-s89. 2. Grady BP, et al. Clin Infect Dis. 2013;57(suppl 2):s105-s110. 3. Aitken CK, et al. Hepatology. 2008;48:1746-1752. 4. Micallef JM, et al. J Viral Hepat. 2007;14:413-418. 5. Page K, et al. J Infect Dis. 2009;200:1216-1226

Risk of HCV re-infection in low and high risk groups and HIV/HCV co-infection
Hill A, et al. CROI 2015, Abstract #654.
Meta-analysis of 66 studies in 11,071 patients
Low risk 43 studies; N=9,419
FU=4.1±2.1 years
High risk (PWID/prisoners) 16 studies; N=819
FU=2.9±1.6 years
HIV/HCV co-infected 7 studies; N=833
FU=3.1±1.2 years
0
2
4
6
8
10
Low risk High risk HIV/HCV co-infected
Rec
urr
ence
rat
e/
10
0 p
atie
nt
year
s
0.23 (95%CI 0.18–0.28)
2.80 (95%CI 2.06–3.71)
4.78 (95%CI 3.97–5.71)

Practical Considerations

HCV Can Be Managed in PWIDs Across the Spectrum
Former Injectors
Opioid Agonist Therapy
Active Injectors
HCV treatment outcomes
improved among those treated for
opioid addiction compared to
untreated individuals2
• Occasional drug use does not
impact adherence, treatment
completion, or treatment efficacy1
• Frequent drug use (daily/
every other day) does1
Successful HCV outcomes are more
likely to be achieved if PWIDs are
stabilized for addiction and then
undergo HCV therapy3
1. Robaeys G, et al. Clin Infect Dis. 2013;57(suppl 2):s129-s137.
2. Dimova RB, et al. Clin Infect Dis. 2013;56:806-816.
3. Zeremski M, et al. World J Gastroenterol. 2013;19:7846-7851.

Risk of HCV Transmission and Progression in PWIDs
Grebely J, et al. Clin Infect Dis. 2013;57:1014-1020. .
• Lower risk of
advanced liver disease1
• Higher risk of HCV transmission
due to the propensity of young/new
PWIDs to share needles and
syringes
• Moderate risk of advanced liver
disease1
• Moderate risk of
HCV transmission1
• Higher risk of
advanced liver disease1
• Lower risk of
HCV transmission1
15 25 35 45 55 65
Years of age
Individual Level1 Risk of liver-related morbidity
and mortality
Population Level1 Risk of HCV transmission
Highest prevalence of PWIDs2

Summary
• PWIDs are disproportionately affected by HCV
– 60% of prevalent and 80% incident infections in US
• Ample evidence of increasing HCV incidence among young people using opiates
• Growing body of clinical trials and ‘real world’ studies showing comparable SVR rates
• Professional societies recommend comprehensive approach involving Opiate Substitution therapy, case management, HCV treatment

Questions?

Extra Slides: Drug-drug interactions

Potential for drug interactions between OST and DAAs
Drug interaction charts. Available at: www.hep-druginteractions.org
DCV LDV/SOF OMV/PTV/ RTV + DSV
SMV SOF
Buprenorphine
Methadone
No clinically significant interaction expected
Potential interaction – may require close monitoring, alteration of drug dosage or timing of administration

Potential for drug interactions between antidepressants, antipsychotics and DAAs
Adapted from EASL. J Hepatol 2015;63:199–236.
DCV LDV/SOF OMV/PTV/ RTV + DSV
SMV SOF
Antidepressants
Amitriptyline
Sertraline
Trazodone
Venlafaxine
Antipsychotics
Aripiprazole
Chlorpromazine
Clozapine
Flupentixol
Haloperidol
Olanzapine
Quetiapine
Risperidone
No clinically significant interaction expected Potential interaction Do not co-administer

Extra Slides: Published Guidelines

2015 INHSU recommendations on management of HCV among PWID
Grebely J, et al. Int J Drug Policy 2015;26:1028–38.
Prevention • Access to OST and sterile injecting equipment as part of widespread
harm reduction programmes
Screening • Annual screening via anti-HCV with RNA confirmation of positive tests • Non-invasive liver fibrosis assessment should be offered to enhance screening
Assessment • Pre-assessment should include HCV education and evaluation of social situation • Models of integrated HCV care to increase linkage between addiction and HCV services
to support successful pre-assessment
Treatment • SOF, LDV/SOF, OMV/PTV/RTV + DSV ± RBV, DCV or SMV are suitable regimens depending
on local availability and patients’ disease characteristics
Management • Individualised and delivered in a multidisciplinary team • Access to harm reduction programmes
Prisoners • Screening and assessment should be offered • Treatment is feasible and should be offered

EASL Recommendations 2015
• PWID should be routinely tested for HCV antibodies and, if negative, every 6–12 months (B1)
• Provided with clean drug injecting equipment and access to OST as part of widespread comprehensive harm reduction programmes, including in prisons (B1)
• Pre-therapeutic assessment should include evaluation of housing, education, cultural issues, social functioning and support, finances, nutrition, and drug and alcohol use. PWID should be linked into social support services and peer support if available (A1)
• A history of IDU and recent drug use at treatment initiation are not associated with reduced SVR and decisions to treat must be made on a case-by-case basis (B1)
• The anti-HCV regimens that can be used in PWID are the same as in non-PWID. No dose adjustment for methadone or buprenorphine is required but monitoring for opioid toxicity or withdrawal should be undertaken. More data are needed for daclatasvir (B1)
EASL. J Hepatol 2015;63:199–236.

AASLD/IDSA Guidelines 2015
• PWID should receive treatment because of the elevated risk of HCV transmission (IIa, Level C)
• Annual HCV testing is recommended for PWID and for HIV seropositive MSM (Class IIA, Level C)
• Adherence and efficacy rates are comparable to those of patients who do not inject drugs
• The rate of reinfection in PWID who are treated is lower (2.4/100 py) than that of incident HCV in this population (6.1-27.2/100 py)
AASLD/IDSA HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C. Available at: www.hcvguidelines.org/full-report-view (accessed August 2015).













![Elizabeth Sherman, PharmD, AAHIVPhivaidsinstitute.med.miami.edu/documents/...HIV-HCV...• SVR rates similar to HCV monoinfected [1,2] • In HCV/HIV coinfection, treat HCV as though](https://img.pdfslide.net/doc/110x75/5fbc30e57653e03e261e9924/elizabeth-sherman-pharmd-aa-a-svr-rates-similar-to-hcv-monoinfected-12.jpg)













