Embed Size (px)
Citation preview

HCV infection
Experiences from Europe Massimo Puoti
AO Ospedale Niguarda Ca’ Granda Milano, Italy
Disclosures
• Member of advisory boards &/or speaker in own events &/or investigator in RCT &/or research grants &/or teacher during courses for employees for
– Janssen, Vertex, MSD, Roche, ViiV, GSK, Abbott, Abbvie, Novartis, BMS, Gilead Sciences, Boehringer Ingelheim, Astellas, Astra Zeneca.

HCV infection Experiences from Europe
• European guidelines
• Taking treatment from trials to the real world
– CUPIC study
– Preliminary data from real life experience
– Experiences in special populations
HCV infection Experiences from Europe
• European guidelines
• Taking treatment from trials to the real world
– CUPIC study
– Preliminary data from real life experience
– Experiences in special populations

Treatment options for naïve genotype 1 patients
TRIPLE THERAPY CONSIDER DUAL THERAPY IN
Primary treatment option in CT/TT or F3–F4
France: ≤F2 with CC and LI RVR+ if CC + ≤F2 with LI RVR–, add PI
Italy: ≤F2 with CC
Primary treatment option No advanced fibrosis with CC,
VL <600-800K IU/mL and LI RVR+
Primary treatment option in F2 with CT/TT or F3-F4
F0–F1 or F2 with CC regardless of RVR
Primary treatment option*
Peg-IFN 2a/RBV if CC, mild fibrosis, VL<600K IU/mL, <40 years, absence of metabolic
syndrome, IP10 <150pg/mL If LI RVR–, add PI or watchful waiting
Primary treatment option ≤F2 with VL <400K IU/mL and RVR+
Primary treatment option <F4 with VL<400-800K IU/mL
and LI RVR+
*TVR recommended over BOC in Sweden
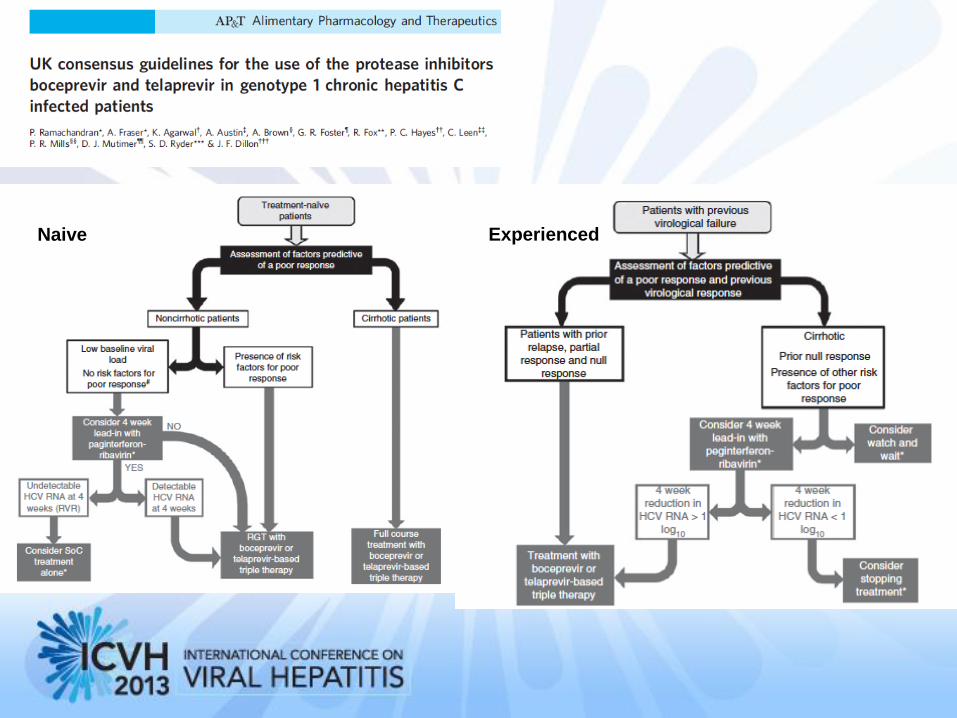
Naive Experienced


European guidelines
• Why the Tower of Babel ?
– Lack of EASL guidelines
– Lack of data in patients with the highest potential cost effectiveness
– Guidelines influence reimbursment policies by European NHS clinical governance of health budget restrictions

HCV infection Experiences from Europe
• European guidelines
• Taking treatment from trials to the real world
– CUPIC study
– Preliminary data from real life experience
– Experiences in special populations

Delays between approval and availability/reimbursement
*Telaprevir and Boceprevir were available but not reimbursed until UK NICE approval obtained 16 March 2012
• National reimbursement does not mean product availability due to regional access
policies
2011 2012
Approval Reimbursement
France
Sweden
Germany
UK*
Austria
Finland
Denmark
Switzerland
Norway
Scotland Spain
UK*
Netherlands
Luxembourg
Israel Belgium
Ireland
Italy
Russia
May Sept
2011
15 months
TVR
BOC
Jan Dec Dec

Taking treatment from clinical trials to the real world
1. Hézode C, et al. Hepatology 2012;56(Suppl.):217A 2. Forestier N, et al. Hepatology 2012;56(Suppl.)1038A
3. Werner C et al, KSGG 2012, Poster 2.9 4. Berg T, et al. J Int AIDS Soc 2012;15 (Suppl. 4):18424
5. Colombo M, et al. Presented at AASLD 2012:LB15 6.Benito JM, et al. HIV and Liver Disease, September 6–8 2012 USA
CUPIC1
Compassionate Use
Telaprevir EAP in 16 European countries5
N=609
CUPIC1
Compassionate Use of Protease Inhibitors in viral hepatitis C Cirrhosis N=497
German cohorts PAN cohort N=7692 Tubingen cohort N=1093 German non-interventional study N=1004
Spanish/Italian HIV cohort6
N=70

Clinical trials
Treating patients with DAAs in the real world
1. Hézode C, et al. Hepatology 2012;56(Suppl.):217A; 2. Colombo M, et al. Presented at AASLD 2012. LB15; 3. Berg T, et al. J Int AIDS Soc 2012;15 (Suppl. 4):18424; 4. Jacobson I, et al. New Eng J Med 2011;364:2405–16; 5. Zeuzem S, et al. New Eng J Med 2011;364:2417–28
6. Poordad F, et al. New Eng J Med 2011;364:1195–206; 7. Bacon BR, et al. New Eng J Med 2011;164:1207–17
CUPIC1
German cohort3
F0 F1 F2 F3 F4 Liver
cancer
EAP2
Real world
REALIZE5
ADVANCE4
SPRINT-26
RESPOND27 73% 12% 7%
86% 6% 5%
22% 29% 22% 26%
36% 42% 15% 6%
11% 89% other
55% 44%
100%

HCV infection Experiences from Europe
• European guidelines
• Taking treatment from trials to the real world
– CUPIC study
– Preliminary data from real life experience
– Experiences in special populations
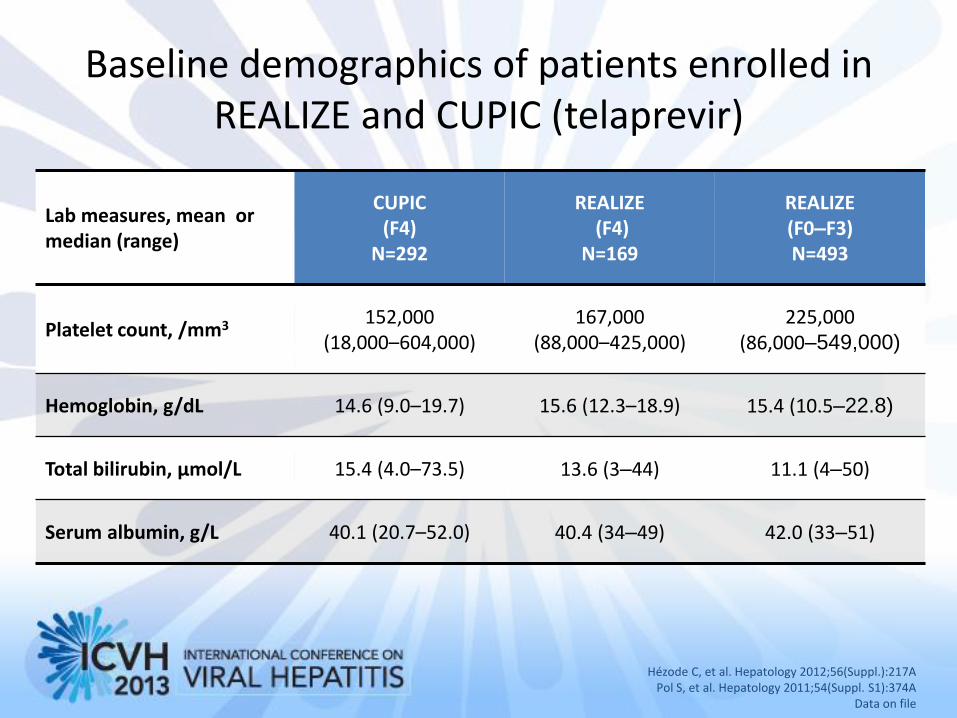
Baseline demographics of patients enrolled in REALIZE and CUPIC (telaprevir)
Hézode C, et al. Hepatology 2012;56(Suppl.):217A Pol S, et al. Hepatology 2011;54(Suppl. S1):374A
Data on file
Lab measures, mean or median (range)
CUPIC (F4)
N=292
REALIZE (F4)
N=169
REALIZE (F0–F3) N=493
Platelet count, /mm3 152,000 (18,000–604,000)
167,000 (88,000–425,000)
225,000 (86,000–549,000)
Hemoglobin, g/dL 14.6 (9.0–19.7) 15.6 (12.3–18.9) 15.4 (10.5–22.8)
Total bilirubin, μmol/L 15.4 (4.0–73.5) 13.6 (3–44) 11.1 (4–50)
Serum albumin, g/L 40.1 (20.7–52.0) 40.4 (34–49) 42.0 (33–51)
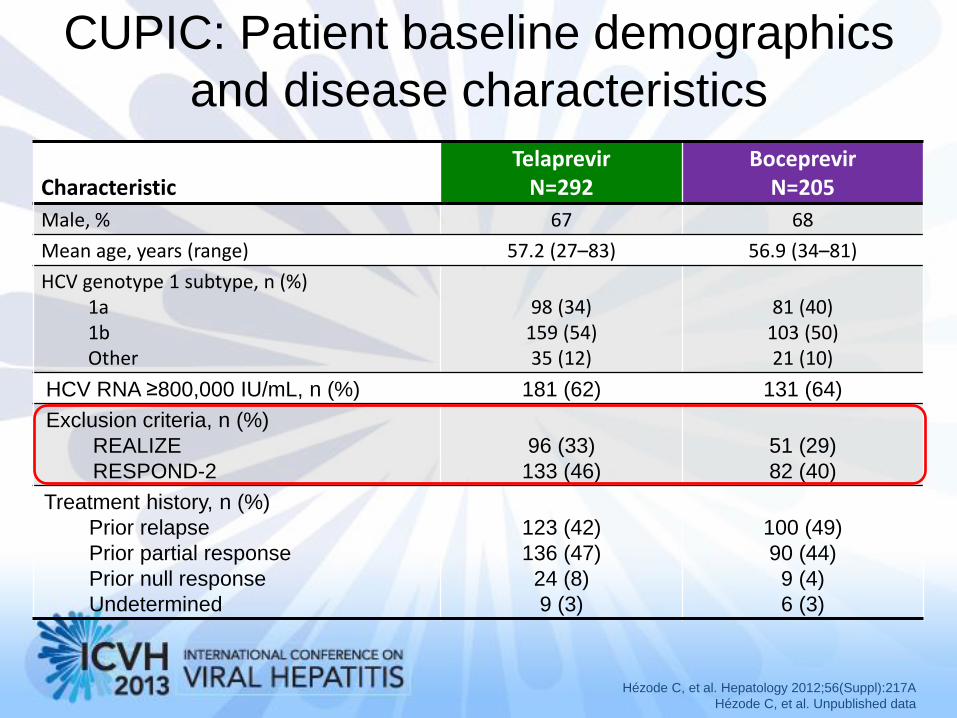
CUPIC: Patient baseline demographics
and disease characteristics
Characteristic Telaprevir
N=292 Boceprevir
N=205
Male, % 67 68
Mean age, years (range) 57.2 (27–83) 56.9 (34–81)
HCV genotype 1 subtype, n (%) 1a 1b Other
98 (34)
159 (54) 35 (12)
81 (40)
103 (50) 21 (10)
HCV RNA ≥800,000 IU/mL, n (%) 181 (62) 131 (64)
Exclusion criteria, n (%)
REALIZE
RESPOND-2
96 (33)
133 (46)
51 (29)
82 (40)
Treatment history, n (%)
Prior relapse
Prior partial response
Prior null response
Undetermined
123 (42)
136 (47)
24 (8)
9 (3)
100 (49)
90 (44)
9 (4)
6 (3)
Hézode C, et al. Hepatology 2012;56(Suppl):217A
Hézode C, et al. Unpublished data

CUPIC: Patient baseline demographics and disease
characteristics
SD: standard deviation
Characteristic Telaprevir
N=292 Boceprevir
N=205
Hb level g/dL, mean (range) 14.6 (9.0–19.7) 14.8 (9.7–18.4)
Platelet count /mm3, mean (range) 152,000
(18,000–604,000) 146,000
(33,900–346,000)
Prothrombin time ratio, mean % (range) 86.3 (27–100) 87.3 (23–100)
Serum albumin g/L, mean (range) 40.1 (20.7–52.0) 40.4 (27.0–50.3)
Total bilirubin μmol/L, mean (range) 15.4 (4.0–73.5) 15.0 (4.0–78.0)
MELD score, mean (SD)
<10, n (%)
10 – <13, n (%)
≥13, n (%)
8.1 (2.8)
213 (81)
33 (13)
16 (6)
8.1 (3.0)
137 (83)
19 (11)
10 (6)
Child-Pugh score, n (%)
A
B
C
285 (98)
7 (2)
0
204 (99)
1 (1)
0
Upper gastrointestinal endoscopy done,
n (%)
Esophageal varices, n (%)
145 (49.7)
48 (33.1)
104 (50.7)
41 (39.4)
Hézode C, et al. Hepatology 2012;56(Suppl):217A; Hézode C, et al. Unpublished data
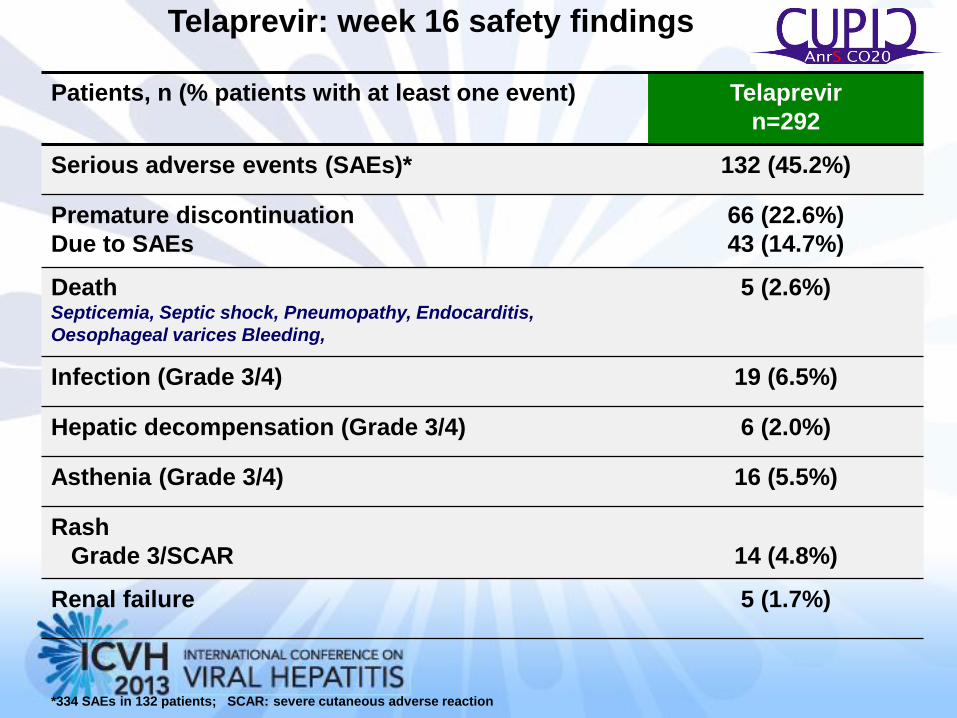
Patients, n (% patients with at least one event) Telaprevir
n=292
Serious adverse events (SAEs)* 132 (45.2%)
Premature discontinuation
Due to SAEs
66 (22.6%)
43 (14.7%)
Death Septicemia, Septic shock, Pneumopathy, Endocarditis,
Oesophageal varices Bleeding,
5 (2.6%)
Infection (Grade 3/4) 19 (6.5%)
Hepatic decompensation (Grade 3/4) 6 (2.0%)
Asthenia (Grade 3/4) 16 (5.5%)
Rash
Grade 3/SCAR
14 (4.8%)
Renal failure 5 (1.7%)
*334 SAEs in 132 patients; SCAR: severe cutaneous adverse reaction
Telaprevir: week 16 safety findings
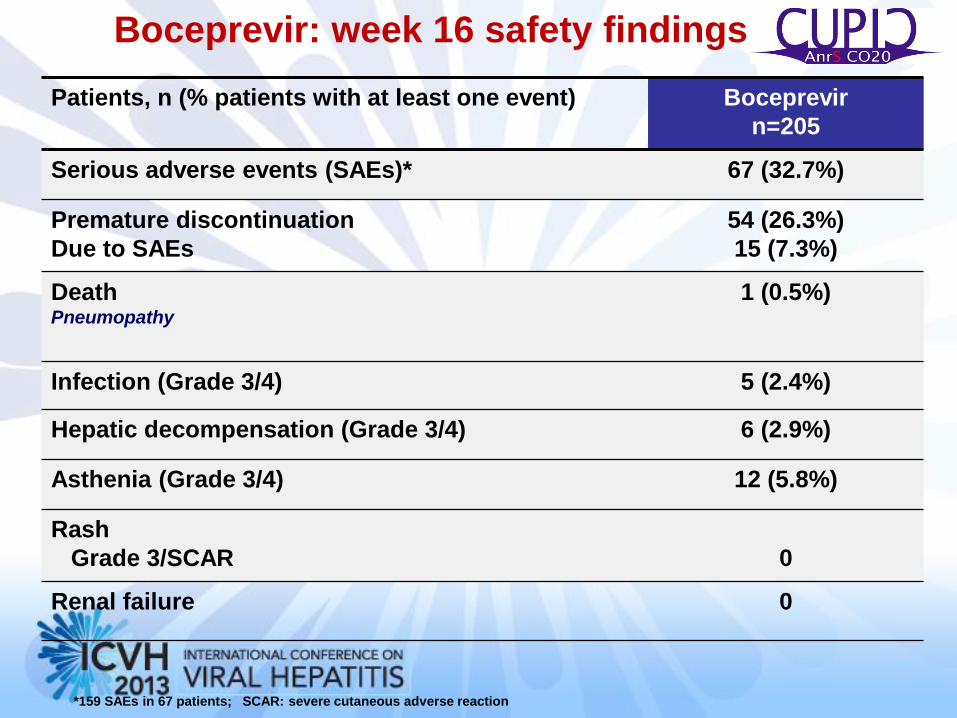
Patients, n (% patients with at least one event) Boceprevir
n=205
Serious adverse events (SAEs)* 67 (32.7%)
Premature discontinuation
Due to SAEs
54 (26.3%)
15 (7.3%)
Death Pneumopathy
1 (0.5%)
Infection (Grade 3/4) 5 (2.4%)
Hepatic decompensation (Grade 3/4) 6 (2.9%)
Asthenia (Grade 3/4) 12 (5.8%)
Rash
Grade 3/SCAR
0
Renal failure 0
*159 SAEs in 67 patients; SCAR: severe cutaneous adverse reaction
Boceprevir: week 16 safety findings
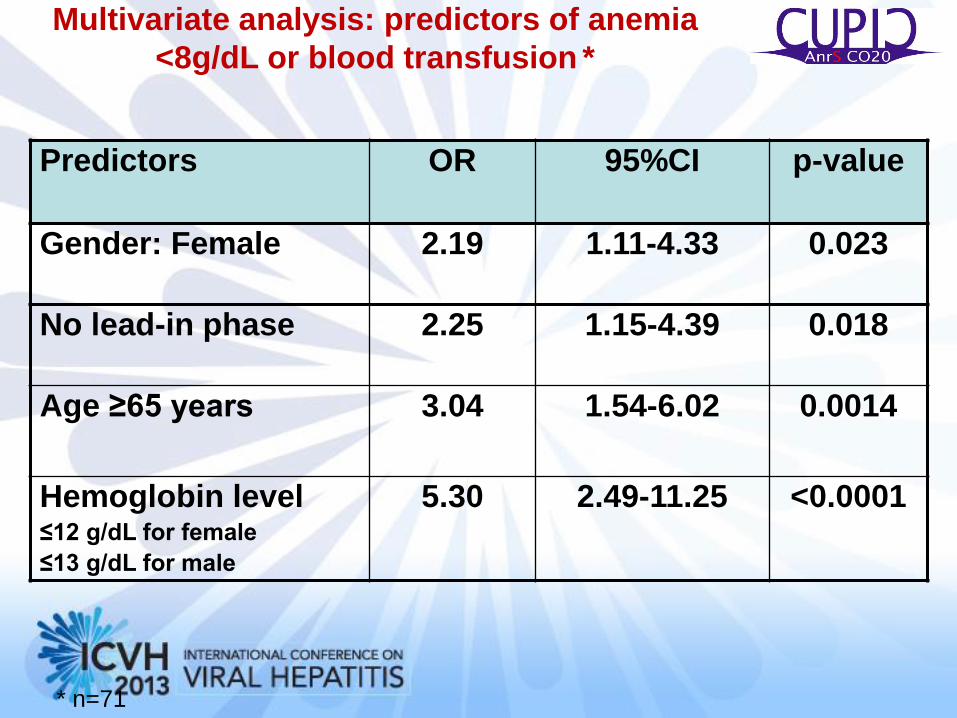
Multivariate analysis: predictors of anemia
<8g/dL or blood transfusion *
Predictors OR 95%CI p-value
Gender: Female 2.19 1.11-4.33 0.023
No lead-in phase 2.25 1.15-4.39 0.018
Age ≥65 years 3.04 1.54-6.02 0.0014
Hemoglobin level ≤12 g/dL for female
≤13 g/dL for male
5.30 2.49-11.25 <0.0001
* n=71
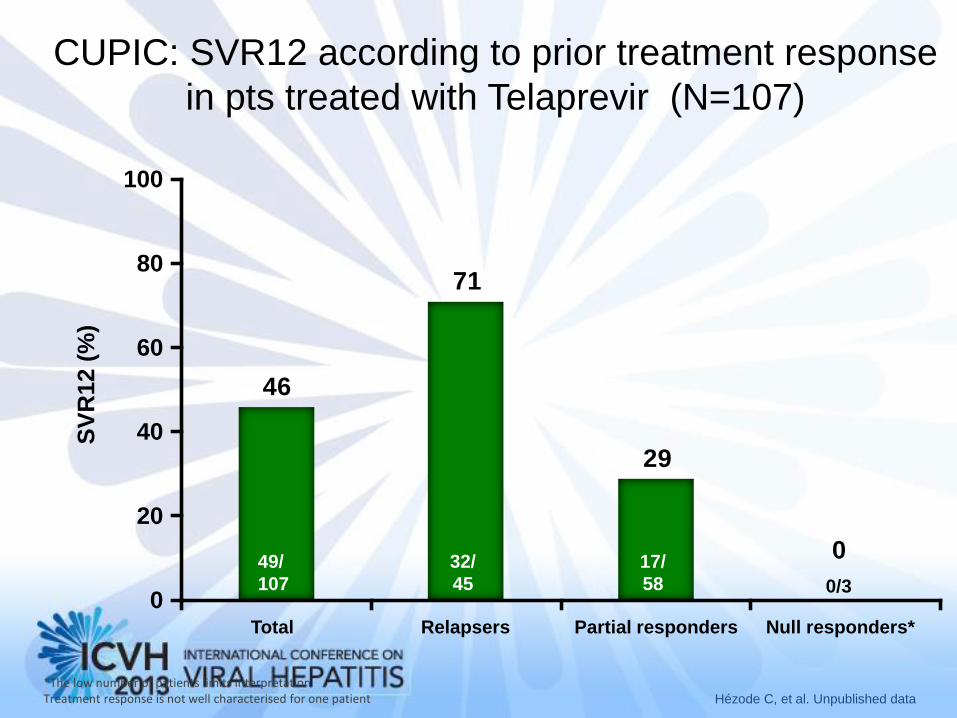
CUPIC: SVR12 according to prior treatment response
in pts treated with Telaprevir (N=107)
Hézode C, et al. Unpublished data
46
71
29
0
20
40
60
80
100
Total Relapsers Partial responders Null responders*
SV
R12
(%
)
49/
107
32/
45
17/
58 0/3
*The low number of patients limits interpretation Treatment response is not well characterised for one patient
0

CUPIC: SVR12 with Boceprevir according to prior
treatment response (N=112)
Hézode C, et al. Unpublished data
SV
R12 (
%)
20
0
40
60
80
100
Total Relapsers Partial responders Null responders*
44/
112 24/
46 20/
64 0/2
*The low number of patients limits interpretation

HCV infection Experiences from Europe
• European guidelines
• Taking treatment from trials to the real world
– CUPIC study
– Preliminary data from real life experience
– Experiences in special populations

Preliminary real life data with Telaprevir in Europe Study Pts N
Pts N n (%)F3/F4 % with HCVRNA <LLD at 4 weeks
% with HCVRNA <LLD at 12 weeks
SAE % withdrawala for SAE %
European EAP1
609
Naïve 124 Rel 171 PR 94 Null 176
F3 271 (44%) F4 335 (55%)
Naïve 59% Rel 63% Part 52% Null 41%
Naive85% Rel 85% Part 77% Null 68%
Deaths 3 (0.5%) F3: 0 F4: 3
Week 16 F3 12% F4 16%
German EAP2
93
93 Naïve 13 Rel 23 Part 21 Null 26
F3 49(53%) F4 46 (46%)
Naïve 62% Rel 74% Null 39%
Naïve 92% Rel 83% Null 63%
Anemia 22% Rash 2%
Rash 8,6% Anemia 2.2%
German Real Life Experience 3
100
Naïve 32 Exp 66
F4 11% Naïve 57% Exp 71%
Naïve 87% Exp 93%
8%
PAN cohort Germany4
574
Naïve 167 Rel 209 Part 59 Null 43
All 62,3% All 73,6% 6%
1. Colombo M, et al. AASLD 2012 Abstract LB–15
2. Wedemeyer H, et al. GASL 2012, 25–26 Jan 2013, Hannover, Germany
3. Berg T, et al. J Int AIDS Soc 2012;15(Suppl. 4):18424
4. Forestier N et al. Hepatology 2012;56(Suppl.)1038A
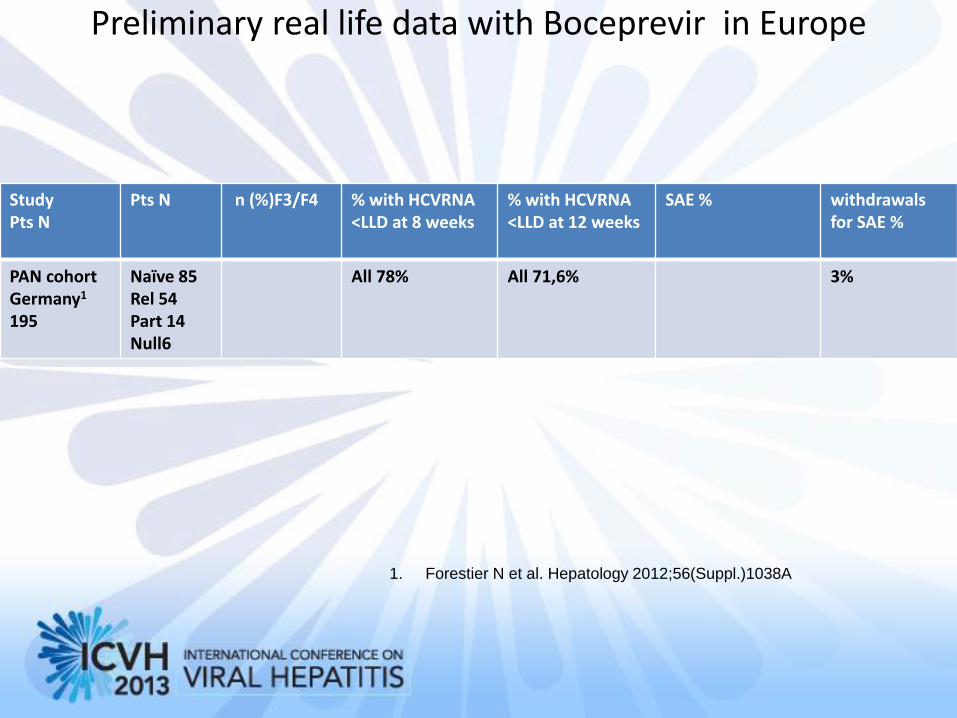
Preliminary real life data with Boceprevir in Europe
Study Pts N
Pts N n (%)F3/F4 % with HCVRNA <LLD at 8 weeks
% with HCVRNA <LLD at 12 weeks
SAE % withdrawals for SAE %
PAN cohort Germany1
195
Naïve 85 Rel 54 Part 14 Null6
All 78% All 71,6% 3%
1. Forestier N et al. Hepatology 2012;56(Suppl.)1038A

HCV infection Experiences from Europe
• European guidelines
• Taking treatment from trails to the real world
– CUPIC study
– Preliminary data from real life experience
– Experiences in special populations
Does HIV-coinfection Reduce Initial Safety or Efficacy of Boceprevir (BOC) or Telaprevir (TPV)-based triple
therapy in cirrhotic patients in the "real life"?
• 13 HIV/HCV; 15 HCV-monoinfected TPV (85% vs 33%)
• HCV negativization (62% vs 80%, p=0.4) RVR (54% vs 60%, p=0.7)
• early withdrawals due to toxicity (8% vs 20%, p=0.6
• In HCV-cirrhotic patients treated in the clinical setting, HIV-coinfection did not worsen safety or efficacy of BOC or TPV-based triple therapy during the first 12 weeks
Moreno A AASLD 2013 Abstract 1789

RVR: Telaprevir vs Boceprevir in HIV+ • 92 pts
• RVR was 95% for TLV and 68% for BOC (p=0.04).
• RVR HCV-1b (100% vs 75%, respectively) than HCV-1a (88% vs 50%, respectively).
• Serum HCV-RNA decay was more pronounced in patients on TLV than BOC (5.18 vs. 4.82 log IU/ml, p=0.02) with respect to baseline.
• Interestingly, serum HCV-RNA decline was on average of 1.58 log IU/ml during the lead-in phase and of 2.55 log IU/mL after adding BOC (from weeks 4 to 8).
• In the multivariate analysis, TLV use was significantly associated with the achievement of RVR.
• A linear regression analysis confirmed the association between TLV use and faster serum HCVRNA decay (R=0.89; β coefficient=0.70+0.07; p<0.0001) after adjustment for other variables
Rick F et al AASLD 2012 Abstract 1773
Special Populations - Cryoglobulinemia
• Rationale
– Improvement of mild- moderate MC after eradication of HCV infection
– Poor response in HCV G1
• Data ( Triboli E et al. Dig Liv Dis 2013; 45: S10)
• 24 HCVMC G1 treated with triple BOC + PEGIFN + RBV vs 11 no MC:
– similar safety but lower response;
– dramatic effect of Boc introduction on symptoms

HCV infection Experiences from Europe
Key messages • EASL guidelines are urgently needed
• Accurate selection of cirrhotic patients for Boceprevir and Telaprevir treatment:
– EAP and NPP inclusion criteria
– Strict surveillance of liver function and symptoms of infections
– Patients with more advanced disease should be treated by expert physicians in connection with a transplant centre
– Data from special populations from real life studies are urgently needed