Embed Size (px)
Citation preview

HCV response to treatment in IDUs (PWID) in the
Czech Republic
Vratislav RehakRemedis Clinic, Prague, Czech Republic 1
Institute of Public Health “Dr. Milan Jovanovic Batut”Belgrade, SerbiaMay 24, 2014
Czech Republic and drug use
Population of CR 10 000 000
„Problematic“ drug users (EMCDDA) 40 200of them
- injecting drug users 38 600
- opiate users 9 300
- metamphetamine users 30 900
Office of the Government (2012) - data from the year 2011
Czech Republic - HCV prevalence
In general population < 0.2 % In IDU‘s ≈ 30% Overall prevalence 0.3 %
Very low prevalence of HIV IDU‘s
Zabransky T, Mravcik V, Korcisova B, Rehak V. Hepatitis C Virus Infection among Injecting Drug Users in the Czech Republic - Prevalence and Associated Factors. European Addiction Research 2006; 12:151-160

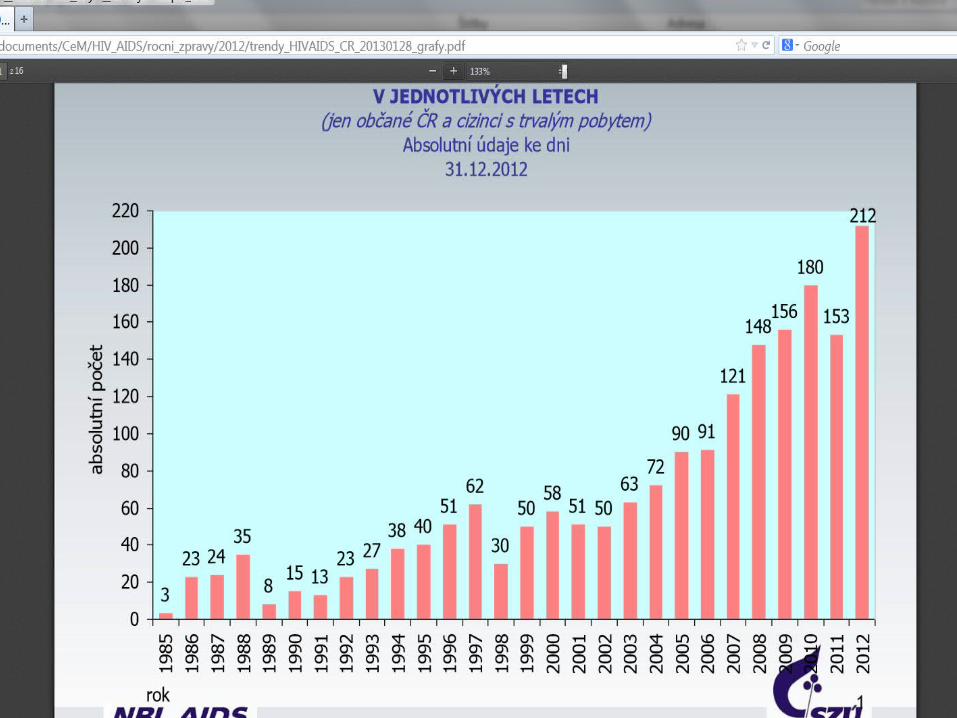
HIV/AIDS, Czech Republic
1985 – 31.12.2012
HIV + cumulatively 1887M 1554 (82,4 %) F 333 (17,6 %)
of them
developed AIDS 366of them
died 187
4
5
6

7
Hepatitis C – notified cases in the Czech Republic 1993 - 2012

Remedis – Program of Comprehensive Care
Goal: to concentrate all available „drug“ services in one place to promote effectiveness of interventions and patient compliance including adherence to antiviral treatment

On site available services
Medical careInternal medicine, gastroenterology, hepatology (incl. liver biopsy), surgery, gynecology, primary care, X-ray, …
Psychiatry, clinical psychology Easy to reach referrals BBD, STD, TB testing Counselling (psychosocial, harm reduction) Opiate substitution treatment Psychotherapy (group or individual) Social work Established collaboration with harm reduction
centers in Prague
10
Study design – inclusion criteria
Prospective recruitment 2003 – 2010 in single center – Remedis Prague, Czech Republic
Proven chronic hepatitis C based on standard serological and histological criteria with detectable HCV RNA
History of past or current IDU
Psychosocially stabilized and motivated patient (including those on OST)
Individualized assessment of eligibility and suitability for antiviral therapy in multidisciplinary setting
No other selection, restriction or limitation to Tx
All efficacy analyses were conducted on →Modified intent-to-treat population – included are all subjects who received at least 1st dose of medication
11
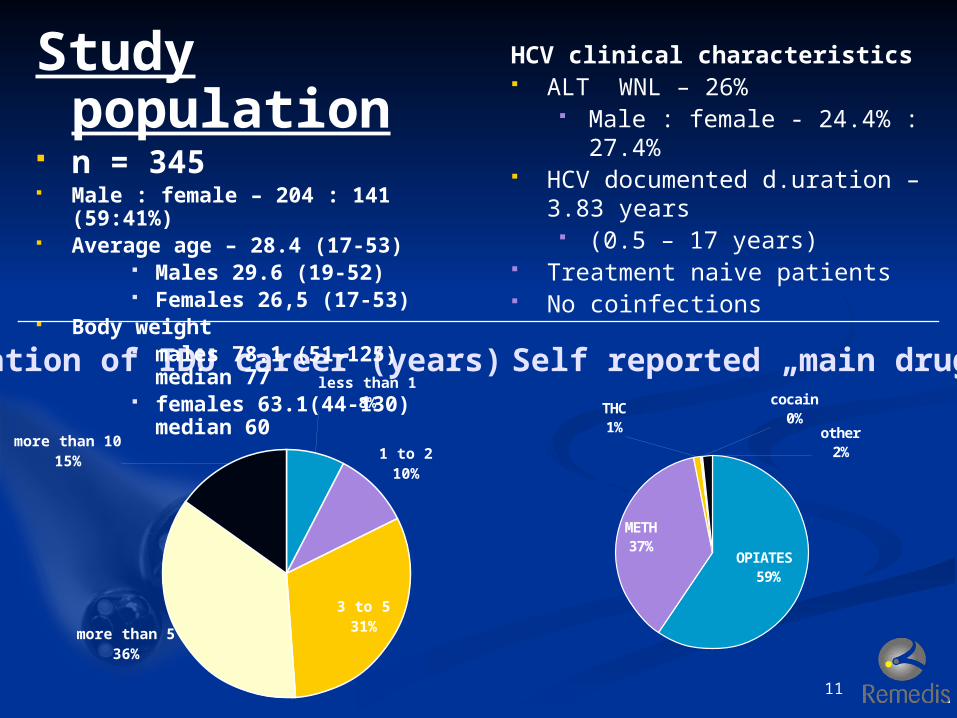
Duration of IDU career (years)less than 1
8%
1 to 210%
3 to 531%more than 5
36%
more than 1015%
OPIATES 59%
METH37%
THC1%
cocain0%
other2%
Self reported „main drug“
Study population
n = 345 Male : female – 204 : 141
(59:41%) Average age – 28.4 (17-53)
Males 29.6 (19-52) Females 26,5 (17-53)
Body weight males 78.1 (51-125)
median 77 females 63.1(44-130)
median 60
HCV clinical characteristics ALT WNL – 26%
Male : female - 24.4% : 27.4%
HCV documented d.uration – 3.83 years (0.5 – 17 years)
Treatment naive patients No coinfections

12
HCV genotypes – 1 vs. non-1
G 1 (4)70%
G 2/329%
UNK 1%
G 115%
G 1a14%
G 1a/1b1%
G 1b43%
G1b/4a1%
1b/3a0%
20%
2a/2c1%
30%
3a28%
40% UNK
1%
HCV subtypes
Stage 0 Stage 1 Stage 2 Stage 3 Stage 4 Stage 5 Stage 6 UNK0
20
40
60
80
100
120
140
Histological stage (modif. Ishak)
OST YES41%
(of them 6% for drug relaps)
OST NO59%
Opiate substitution treatment while on HCV therapy
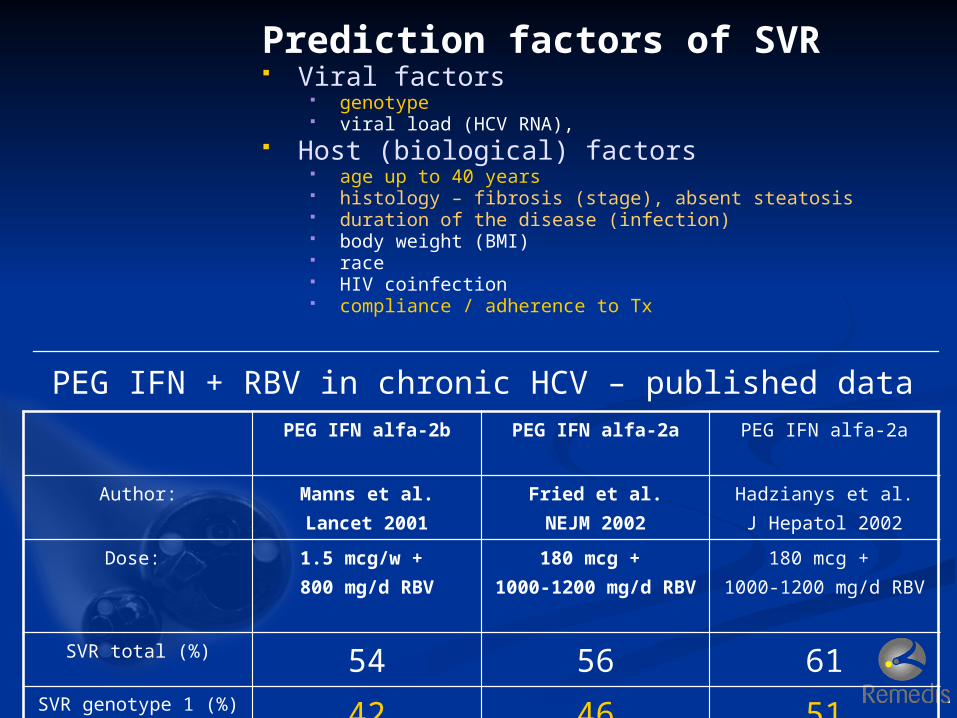
PEG IFN + RBV in chronic HCV – published dataPEG IFN alfa-2b PEG IFN alfa-2a PEG IFN alfa-2a
Author: Manns et al.Lancet 2001
Fried et al.NEJM 2002
Hadzianys et al.J Hepatol 2002
Dose: 1.5 mcg/w + 800 mg/d RBV
180 mcg + 1000-1200 mg/d
RBV
180 mcg + 1000-1200 mg/d RBV
SVR total (%) 54 56 61SVR genotype 1 (%) 42 46 51
Prediction factors of SVR Viral factors
genotype viral load (HCV RNA),
Host (biological) factors age up to 40 years histology – fibrosis (stage), absent steatosis duration of the disease (infection) body weight (BMI) race HIV coinfection compliance / adherence to Tx

14
Pre-treatment follow-up
Mean 14,2 months (0-72 months)
Prior dependency stabilization
Psychosocial stabilization
Other relevant interventions accomplished
Treatment regimen - standard
Pegylated interferon alfa weekly
+ Ribavirin 800-1200 mg/d weight based
Genotype 1 - 48 weeksGenotype 2,3 – 24 weeks
15
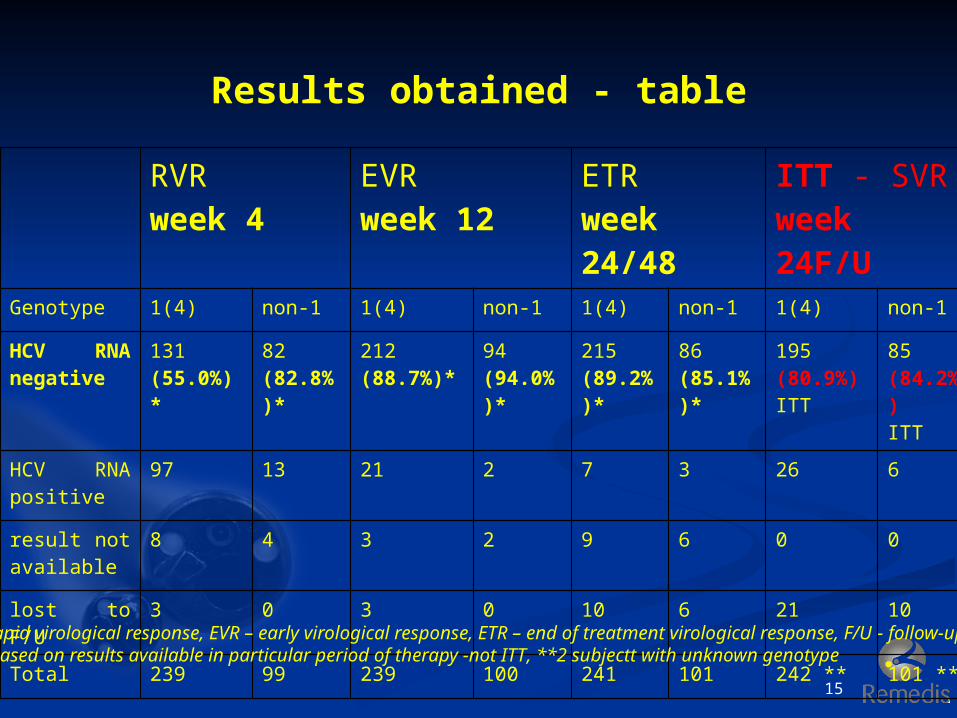
Results obtained - table
RVRweek 4
EVRweek 12
ETRweek 24/48
ITT - SVRweek 24F/U
Genotype 1(4) non-1 1(4) non-1 1(4) non-1 1(4) non-1
HCV RNA negative
131(55.0%)*
82(82.8%)*
212(88.7%)*
94(94.0%)*
215(89.2%)*
86(85.1%)*
195(80.9%)ITT
85(84.2%)ITT
HCV RNA positive
97 13 21 2 7 3 26 6
result not available
8 4 3 2 9 6 0 0
lost to F/U 3 0 3 0 10 6 21 10
Total 239 99 239 100 241 101 242 ** 101 **
RVR – rapid virological response, EVR – early virological response, ETR – end of treatment virological response, F/U - follow-up*data based on results available in particular period of therapy -not ITT, **2 subjectt with unknown genotype
16
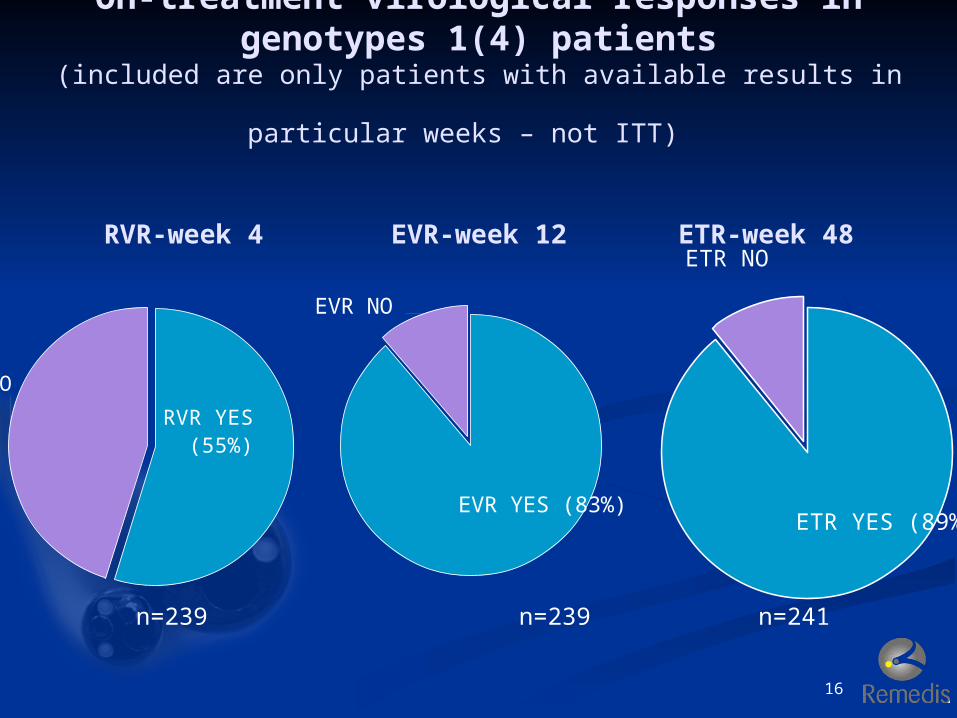
On-treatment virological responses in genotypes 1(4) patients
(included are only patients with available results in particular weeks
– not ITT)
RVR-week 4 EVR-week 12 ETR-week 48
RVR YES (55%)
RVR NO
EVR YES (83%)
EVR NO
ETR YES (89%)
ETR NO
n=239 n=239 n=241

17
Sustained virological response, genotypes 1(4) – week 24 of F/U
ITT population
SVR YES 195(80.9%)
SVR- NO 26(10.6%)
Lost to follow-up 21(8.5%)
n=128
18
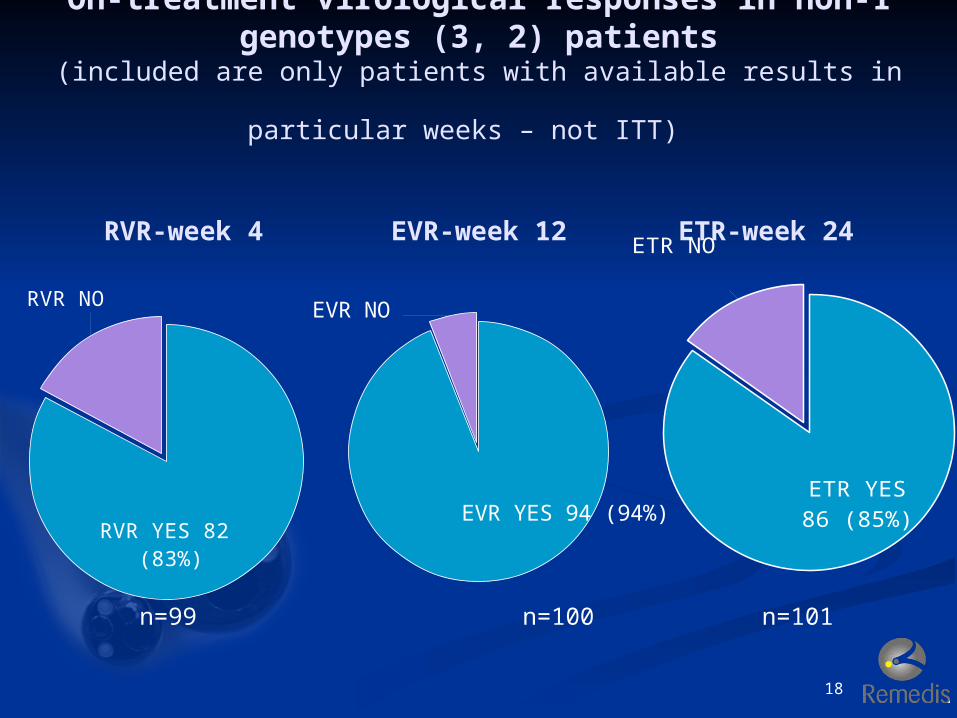
On-treatment virological responses in non-1 genotypes (3, 2) patients
(included are only patients with available results in particular weeks
– not ITT)
RVR-week 4 EVR-week 12 ETR-week 24
RVR YES 82 (83%)
RVR NO
EVR YES 94 (94%)
EVR NO
ETR YES86 (85%)
ETR NO
n=99 n=100 n=101

19
Sustained virological response, GENOTYPES non-1 (3, 2)
– week 24 of F/U
ITT population
SVR YES 85(84,2%)
SVR- NO 6 (5.9%)
Lost to follow-up 10 (9.9%)
20
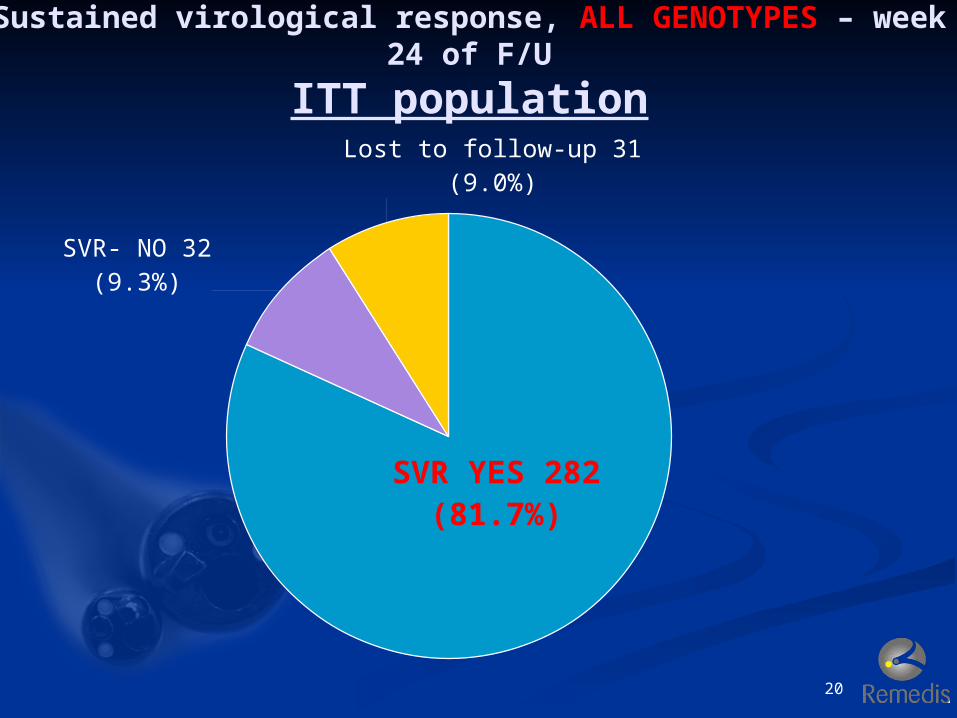
Sustained virological response, ALL GENOTYPES – week 24 of F/U
ITT population
SVR YES 282
(81.7%)
SVR- NO 32 (9.3%)
Lost to follow-up 31 (9.0%)
Adverse events observed
Mood disorders 45,3%
Thyroid disorders 18,3%
Ribavirin dose reduction due to anemia 13,3%
AE‘s were managed individually, not á la carte
Adverse events frequency was generally comparable or lower than published elsewhere
Reinfection rate(data not updated)
3 years standard F/U in 76% of patients
2 reinfection documented Frequency of 0.6% per person/year 1 reinfection after 5 years
Reasons for good treatment response
Low age and short duration of HCV infection
Early stages of HCV infection (low fibrosis)
Low body weight (BMI) Low somatic comorbidity Good adherence / compliance →
comprehensive care setting in Remedis HCV antiviral Tx is an integral part of
addiction treatment HCV antiviral therapy is considered as one
of the steps of an addicted patient recovery
24
Conclusions Chronic hepatitis C in certain settings can be
nearly fully treatable disease even with current standard of therapy
IDU‘s can be successfully treated with higher than average efficacy
HCV antiviral therapy should optimally be initiated and performed within a comprehensive service setting promoting good adherence
HCV antiviral therapy can be one of the most powerful preventative measure in low prevalence countries such as the Czech Republic
The cost-effectiveness of HCV antiviral treatment for injecting drug user populations
Natasha K. Martin1,2,*,†, Peter Vickerman1,2, Alec Miners2, Graham R. Foster3, Sharon J. Hutchinson4,5, David J. Goldberg4, Matthew Hickman1
DOI: 10.1002/hep.24656
Abstract
Background & Aims: Injecting drug use is the main risk of hepatitis C virus transmission in most developed countries. HCV
antiviral treatment (peginterferon-α+ribavirin) has been shown to be cost-effective for patients with no reinfection risk. We examined the cost-effectiveness of providing antiviral treatment for injectors (IDUs) as compared to treating ex/non-IDUs or no treatment.
Methods: A dynamic model of HCV transmission and disease progression was developed, incorporating: a fixed
number of antiviral treatments allocated at the mild HCV stage over 10 years, no retreatment after
treatment failure, potential reinfection, and three baseline IDU HCV prevalence scenarios (20%, 40%, and 60%). We performed a probabilistic cost-utility analysis estimating long-term costs and outcomes measured in Quality Adjusted Life Years (QALYs) and calculating the incremental cost-effectiveness ratio (ICER) comparing treating IDUs, ex/non-IDUs or no treatment.
Results: Antiviral treatment for IDUs is the most cost-effective option in the 20% and 40% baseline chronic
prevalence settings, with ICERs compared to no treatment of £521 and £2,539 per QALY saved, respectively. Treatment of ex/non-IDUs is dominated in these scenarios. At 60% baseline prevalence treating ex/non-IDUs is slightly more likely to be the more cost-effective option (with an ICER compared to no treatment of £6,803), and treating IDUs dominated due to high reinfection. A sensitivity analysis indicates these rankings hold even when IDU sustained viral response rates as compared to ex/non-IDUs are halved.
Conclusions: Despite the possibility of reinfection, the model suggests providing antiviral
treatment to IDUs is the most cost-effective policy option in chronic prevalence scenarios less than 60%. Further research on how HCV treatment for injectors can be scaled up, and its impact on prevalence is warranted. (HEPATOLOGY 2011.)
Seroprevalence study in prisons in the Czech Republic 2009-2012
Total inmates tested 971 Results – 2 HIV + (0,2%)
1 HIV+ , HCV+ 1 HIV + , HCV-
274 HCV + (28,12%)
28
Opportunity for prevention of HCV? Prisons! In many countries a considerable gap in testing is in
incarcerated populations. Prisons provide an excellent opportunity to diagnose and
treat the largest known reservoir of infected individuals and provides the single most effective HCV public health strategy.
Intake testing and councelling should be mandatory, treatment should be made available based on the patients will and local conditions.







