Embed Size (px)
Citation preview

HDF ? Haut volume ?
Guillaume JEAN NEPHROCARE Tassin-Charcot
Ste Foy-les-Lyon





Ok et al, Turkish Conflict of interest statement. E.O. and A.B. are the members of the scientific advisory board of Fresenius Medical Care, Turkey.

Mais très faible…


Pas de différence HD et HF pour le phosphore

Svara 2016, ASAIO 62(2)176
• Epuration phosphate HD low, high flux et HDF
• Pas de différence Hflux HD et HDF

Epuration des phosphates




28,3 8,5 (9 – 71) mg/L Médiane 27

Survie à 5 ans
NS


Davenport 2016 KI 89(1):193
• Avantage hauts volumes
• - maintenu si standardisation avec la surface corporelle ou l’eau totale ou sans standardisation.
• Plus d’avantage si standardisation sur le poids ou l’IMC
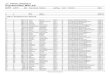
Description de la population
Pas de comparaison des 2 groupes !
This study was partly supported by grants from Fresenius Medical Care and Gambro

Critères secondaires
Critère Réduction
risque p
Mortalité CV -33% 0,06
AVC -61% 0,03
Mortalité infectieuse -55% 0,03
Taux hospitalisation toute cause -22% 0,001
Nb hypotensions intradialytiques -28% <0,001
Pas de différence : -IDM, infarctus mésentérique, AOMI, arythmie - mortalité liée au cancer, mort subite, cachexie
-Poids, albumine - Hb, fer, poso ASE
- phosphate, chelateurs - beta2microglobuline


Baisse de l’albumine après switch HD HDF


Rôle de l’autoSub

Rôle du volume de réinjection

Rôle du filtre

Baisse de l’albumine chez tous ? CONTRAST

HDF 1, 6 mois- HD; 6 mois - HDF2, 6 mois
Même débit sang et dialysat, même filtre, même TT, même dialysat

HDF 1 HD HDF 2
Albumine (g/l) 34,4 3 35,9 3** 34,1 4**
ß2-micro (mg/l) 26,1 5 28 6* 26,5 5*
Calcémie (mmol/l) 2,2 0,1 2,19 0,1 2,18 0,1
Phosphatémie (mmol/l) 1,58 0,2 1,59 0,3 1,61 0,2
PTH (pg/ml) 215 110 220 111 245 108
Kt/V (Daug-2) 1,67 0,2 1,71 0,25 1,74 0,25
nPCR (g/kg/j) 1 0,1 1,08 0,19 1,05 0,19
CRP (mg/l) 7,5 9 7 8 7,7 8
Hb (g/dl) 11,7 1 11,8 0,8 11,7 0,7
PAS/PAD (mmHg) 133/61 17/11 132/59 18/11 134/61 18/11
Poids sec (kg) 72,6 11 72 12 72,1 12
Prise de poids inter séance ( kg) 1,8 0,6 2 0,6 2 0,7
Calcium dialysat (mmol/l) 1,51 0,2 1,56 0,2 1,54 0,17
Chute de tension/crampes (% des séances perturbées)
15,7% 12% 20%
Traitements
Anti hypertenseurs (%) 37,3 37,3 37,3
ASE (U/semaine) 5000 4000 4660 3500 4900 3500
Alfacalcidol µg/semaine (%) 2,1 (37%) 2,2 (37) 2 (35)
Calcium (unité/j), % 1,9 2 (48%) 1,88 2,2 (50) 1,9 2,2 (48)
Mimpara mg/j (%) 52 (5,8%) 52 (5,8) 47 (7,8)
Sevelamer (unité /j), % 3,3 4 (31%) 3,4 4 (33) 4 4 (33)

25
30
35
40
45
50
Alb
um
ine
g/l
Alb1 Alb2 Alb3HDF 1 HDF 2 HD
**

R²=0.2 P= 0.001

10
15
20
25
30
35
40
45
Bé
ta 2
M m
g/l
Beta1 Beta 2 Beta 3HDF 1 HDF 2 HD
ß2
mic
ro
*
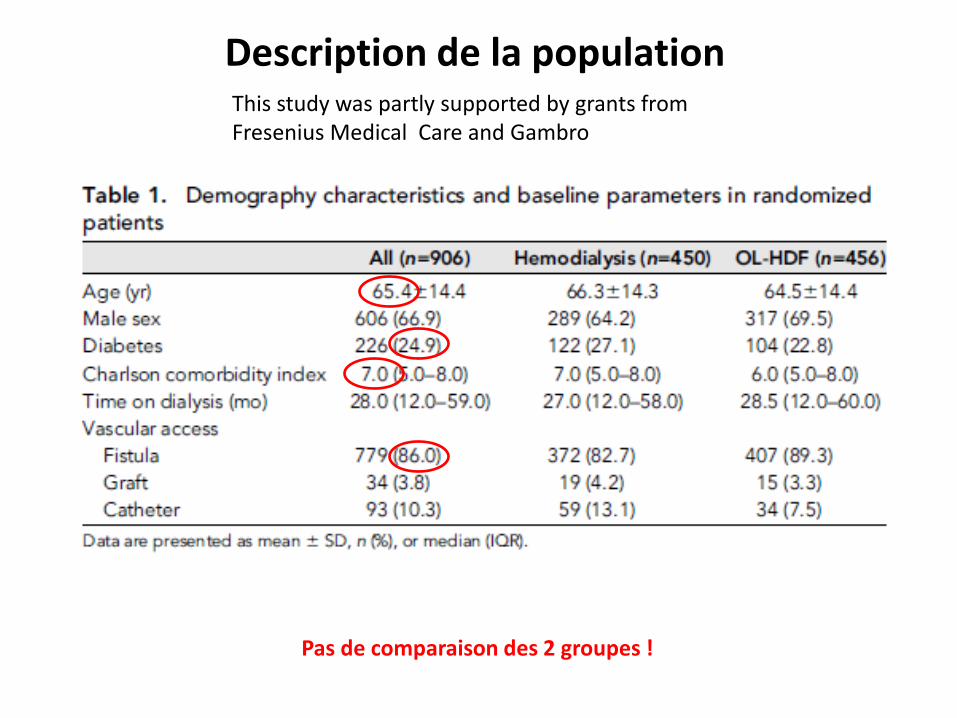
Volume convectif HDF (Tassin)
22 litres 4,7

Pression transmembranaire et perte d’albumine

Pas de différence de qualité de vie


Etude CONTRAST
HDF cannot be considered a cost-effective treatment for patients with end-stage renal disease at present. Apparently, minor additional costs of HDF are not counterbalanced by a relevant QALY gain

-0,1
0,0
0,1
0,2
0,3
Dialysate calcium mmol/l
Duréé<5
De
lta
io
niz
ed
ca
lciu
m m
mo
l/l
1,25 1,5 1,75
HDF
No
Yes
Calcium balance in HDF vs HD
*
**
ns
Online HDF “magnifies” the exchanges
iCa, PTH, DCC, Blood and dialysate flow rate were similar
Jean et al EDTA 2013 Istanbul

*
P= 0,045 0,6013, (0,3777 to 0,96578) Cox ajusté pour âge, ancienneté, diabète, cardiopathie, artérite, sexe, cancer, KT
Jean et al SN-SFD 2015 Lyon
≤ 5 H
> 5 heures
Survie 4,5 ans

HDF ?
• Rct's discutables++
• Stabilité hémodynamique: balance sodée, calcique, thermique, glucidique ?
• Pas de ≠ cliniquement significative d’ épuration urée, phosphore, ß2-m
• Risque d’hypoalbuminémie (si incapacité à compenser les pertes)