Head Trauma - safpa.org 2020/DAY 3 LE… · HEAD TRAUMA MAJ BRIAN SMEDICK, MPAS, APA-C, US ARMY...
52
HEAD TRAUMA MAJ BRIAN SMEDICK, MPAS, APA-C, US ARMY SURGICAL PA FELLOW; BROOKE ARMY MEDICAL CENTER
Head Trauma - safpa.org 2020/DAY 3 LE… · HEAD TRAUMA MAJ BRIAN SMEDICK, MPAS, APA-C, US ARMY SURGICAL PA FELLOW; BROOKE ARMY MEDICAL CENTER. Good afternoon, My name is MAJ Brian
HEAD TRAUMA MAJ BRIAN SMEDICK, MPAS, APA-C, US ARMY
SURGICAL PA FELLOW; BROOKE ARMY MEDICAL CENTER
Presenter
Presentation Notes
Good afternoon, My name is MAJ Brian Smedick. I’m an Army Physician Assistant currently in the Army-Baylor Surgical PA Fellowship at Brooke Army Medical Center. For this glorious block of instruction we will talk about Head Trauma, primarily focusing on the initial trauma assessment and management as well as care in the austere environment.
DISCLAIMER
• I speak Army…Sorry.
• My statements and views are based on peer reviewed journals, workshops, personal experience, and discussions with experts. If there is something more up-to-date that I have missed or left out, please don’t stone me in a public square.
• My experience with field medicine is primarily dismounted, aid bag medicine over 8 yrs as a PA with Airborne Infantry units and Special Operations teams.
• So if I say something that seems off base/Too ARMY please let me know during the questions portion and I will expand or elaborate for clarity sake.
Presenter
Presentation Notes
So here is my general disclaimer. I’m indoctrinated thanks to 15 years in the Army, so at this point I don’t even realize what comes out of my mouth unless it was issued to me. Everything in this presentation is evidence based and/or experience based. I know literature changes and best practices adapt so If something in this presentation appears out of date email me and I will provide you the exact references that went into these guidelines and will gladly accept any new resources to help improve my practice and instruction.
OBJECTIVES
• Provide an overview of head injury patterns, mechanisms of injury, and patient presentations
• Discuss management of head injuries according to current guidelines • ATLS
• Joint Trauma System
• Neurocritical Care Society
• Society of Critical Care Medicine
• Introduction to management of head injuries in the austere environment• PFC Clinical Practice Guidelines
Presenter
Presentation Notes
Every military PowerPoint must have objectives, I’m pretty sure there is a regulation on that. As such here is our focus today. We will discuss a variety of injury patterns and presentations for head trauma and provide an overview of current practice guidelines to identify and manage head injury patients in both CONUS and OCONUS environments
AGENDA
• Anatomical Overview
• Injuries and Evaluation
• Austere Environments
• Summary
• Good Resources
Presenter
Presentation Notes
Here is the blueprint for how I hope to achieve those objectives. We will start with a quick overview of key anatomy, followed by injury patterns and evaluation, then we dive into some austere considerations, and finally wrap it up by restating what I just told you and send you to lunch with a few good resources to help you in your practice.
ANATOMY
Presenter
Presentation Notes
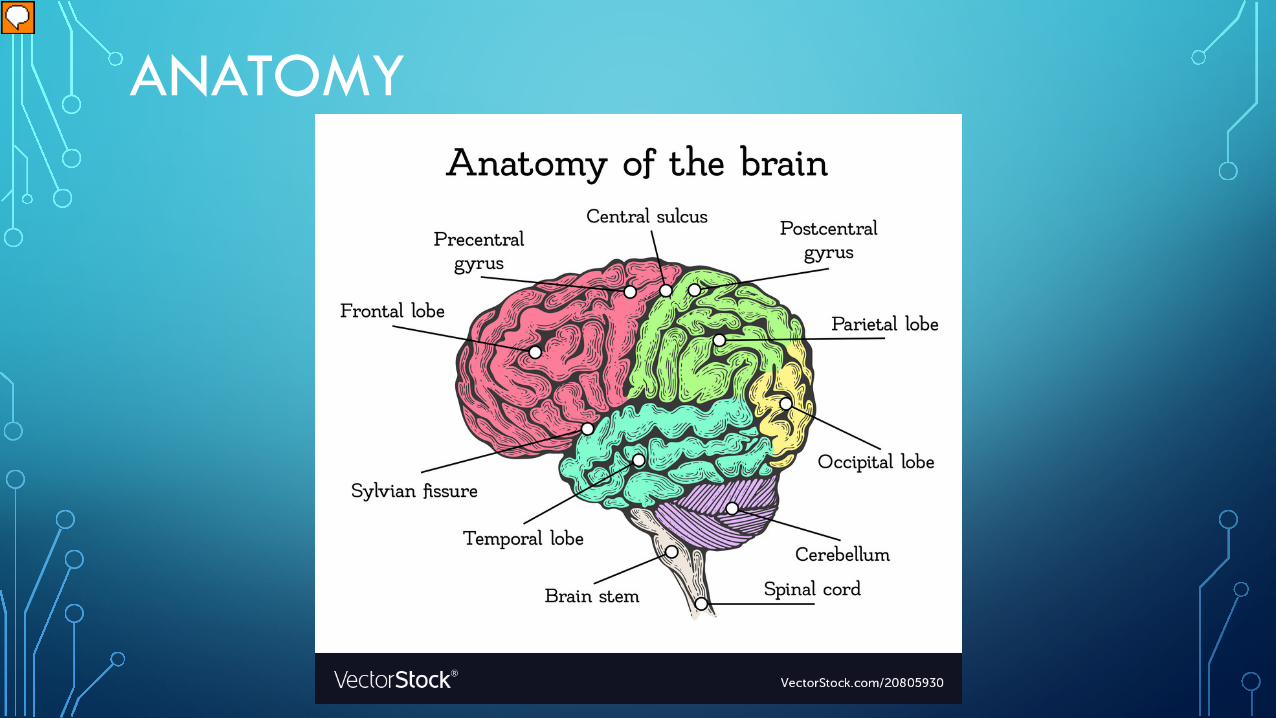
The human brain is primarily composed of the Cerebrum, the Cerebellum, and the Brain Stem. For purposes of this lecture, the Cerebrum's significant components are the lobes, identified as the frontal lobe, parietal lobe, temporal lobe, and occipital lobe. Each lobe has specific functions and responsibilities. The lobes provide touch, vision, hearing, speech, reasoning, emotions, learning, and fine motor control. The Cerebellum regulates coordination, posture, balance, and proprioception. Finally, the Brain Stem serves as the relay station for the Cerebrum and Cerebellum to the spinal cord. It coordinates involuntary activities such as breathing, heart rate, body temperature, sleep/wake cycles, digestion, coughing, vomiting, and swallowing. The brain stem may be a small area but it is high value real estate; even minor injury of the brainstem can cause serious neuro deficits.
ANATOMY
Presenter
Presentation Notes
Here we have a cross section of the cranial compartment, and all its many splendid layers. This slide should help all the visual learners in the room when we discuss intracranial hemorrhage. Pay attention to the Dura, and Arachnoid mater. While looking at these layers you can see how a hemorrhage above or below each layer would track, giving these injuries a predictable pattern on imaging.
INJURIES AND EVALUATION
WHY DO WE CARE?
• In the US: Approx. 2.5 million TBIs/yr.
• 283,000 hospitalizations (~11%)
• 52,000 do not survive (~2%)
• Worldwide: TBI is a leading cause od death in children and young adults
• Falls and motor vehicle collisions are the most common etiologies (civilian)
Neurocritical Care Society: enls.neurocriticalcare.org
Presenter
Presentation Notes
A considerable amount of traumas both civilian and military involve head injuries. The Neurocritical care society notes around 2.5 million brain injuries occur annually. Roughly 1/8th of those require hospitalization. and 1/5th of those hospitalized will not survive. While Motor vehicle collisions and falls account for most of the civilian head traumas, Operationally, head injury is due to blast exposure, penetrating trauma, and blunt force. OCONUS roughly 83% of non-survivable injuries are TBIs, compared to hemorrhage the next most common which comes in at 16%.
CASE
• 25yo M flips over his handlebars while cycling to work. He was not wearing a helmet. Bystanders report the patient was unresponsive at the scene for less then a minute then got up for a bit walking around, mildly confused, with limited recall of the event. EMS is called and the patient is taken to the hospital. He arrives at your trauma bay, responds incoherently, opens eyes when asked, and localizes to pain (E3V4M5). What is our initial concern?
PRIMARY AND SECONDARY BRAIN INJURY
• Primary: Occurs at the time of impact, or point of injury(POI), and may result in altered mental status and/or level of consciousness
• Secondary: The sequelae resulting from the primary injury. All TBI interventions are aimed at preventing Secondary injury.
Neurocritical Care Society: enls.neurocriticalcare.org
Presenter
Presentation Notes
The initial brain injury is not preventable. It happens at Point of Injury and progresses as the inflammatory response mounts. It is important to note that in penetrating ballistic trauma the initial projectile path may be apparent however the pressure wave caused when the projectile hits a viscous medium, like you would see in a ballistic gel demonstration, causes significant damage to surrounding structures leading to edema and vascular compromise which is difficult to appreciate on initial exam. It is important to note the cognitive symptoms like confusion and memory loss can occur without Loss of consciousness. Loss of consciousness usually indicates a cortical and subcortical injury and is a good indicator of severity. The brainstem is usually the last area to be injured except in penetrating trauma. As trauma providers we make our money identifying and managing secondary brain injury. These injuries progress over time as the Brain reacts to the trauma and failure to prevent and/or treat these issues worsens the patient’s prognosis considerably.
SECONDARY BRAIN INJURY
• Causes of secondary brain injury• Hypoxia
• Ischemia
• Hypotension
• Hematoma expansion
• Cerebral edema
• Intracranial Hypertension
• Seizure
• Fever
Neurocritical Care Society: enls.neurocriticalcare.org
• Tissue is the issue!
• Maximize cerebral perfusion
• Minimize oxygen consumption in the rest of the body
• Hemorrhage • Fever• Pain• Exertion• Seizure
Presenter
Presentation Notes
The key concept when dealing with with secondary brain injury is preventing further damage. This is accomplished by conserving oxygenation of brain tissues by maintaining blood pressure and oxygen saturation and preventing oxygen demand elsewhere in the body. Cerebral perfusion pressure is a great indicator of tissue oxygenation within the Brain however, unless you have the skills and equipment to place a bolt or perform a ventriculostomy and place a drain this number is irrelevant in the field and initial trauma assessment. Cerebral perfusion pressure is the difference between Mean Arterial Pressure and Intracranial Pressure, so without the ICP you cannot calculate it. So trying to maintain a MAP of >80-85 mmHg will give you a fighting chance. Treating causes of increased metabolic or oxygen demand such as the items listed on the right of the slide will also assist in the prevention of secondary brain injury and should always be monitored in the TBI patient.
CASE
• 25yo M flips over his handlebars while cycling to work. He was not wearing a helmet. Bystanders report the patient was unresponsive at the scene for less then a minute then got up for a bit walking around, mildly confused, with limited recall of the event. EMS is called and the patient is taken to the hospital. He arrives at your trauma bay, responds incoherently, opens eyes when asked, and localizes to pain (E3V4M5). What do we do next?
PRIMARY SURVEY
• ATLS• A: Airway
• B: Breathing
• C: Circulation
• D: Disability
• E: Exposure/Environment
• TCCC• M: Massive Hemorrhage
• A: Airway
• R: Respirations
• C: Circulation
• H: Hypothermia
Presenter
Presentation Notes
We care about LOC, GCS, and what the eyes are doing (pupils, EOMs, gaze) during the primary survey. This gives a great deal of information to the provider in reference to intracranial pressure, potential herniation, and general prognosis. Neither of these two surveys are 100% wrong nor right. It really is dependent on where you see your patient at. In a hospital use ATLS, in the field or OCONUS focus on TCCC due to the types of injuries you may encounter.
INITIAL EVALUATION
• Glasgow Coma Scale• Should be performed as part of your
primary survey (“D”)
• Motor score is best indicator of prognosis/severity
• Good thing to MEMORIZE
E
V
M
Presenter
Presentation Notes
The GCS score is mandatory in your initial assessment of a TBI patient. Keep in mind the score is 3-15, even this table has a GCS of 3. Some may think a score of three is the worst score possible, but a score of 3 is sometimes correctable, Think hypothermia, severe acidosis, sedation etc. I would argue that a patient with extensor posturing or a GCS of 4, is worse because it signifies supra tentorial injury which is an extensive injury and in most cases is not survivable. This is good to remember in mass casualty situations when performing triage.
DO YOU EVEN MACE?• Military Acute Concussion Evaluation
• Used as close to POI as possible• Can be repeated to assess
progression/recovery
• Issues• GCS score is best tool for assessment of
head injury and can be performed as serial exams
• Right after an explosion people tend to be confused and anxious leading to false positives
• Best used by medics12 hours after injury to assess for late onset symptoms (HA, Dizziness, Memory loss etc.)
Presenter
Presentation Notes
By a show of hands who has performed a MACE exam?............................Now how many of you like the MACE exam? I am sadly not one of the MACE exams most adoring fans. Typically this exam is administered to close to point of injury when your patients adrenaline is at max, they may have seen a friend injured, they may have distracting injuries, and on, and on. I have seen this test miss used repeatedly by medics and providers, and more concerning then miss use…..in lieu of a primary survey and GCS. If you chose to use this to screen patients leave it until your tertiary exam, somewhere in the first 20-30 minutes, and for mild to moderate TBI patients only. Again I do not want to convince you not to use this tool just because I hate it, if you know how to use it and see benefit then go for it.
SECONDARY SURVEY
• Main priority is to prevent secondary brain injury• Avoid fever, seizures, anxiety, pain, shivering etc.
• As complete a neurologic exam as possible; look for worsening defects and/or new symptoms.
• Key features for head injury:• Level of consciousness
• Cranial nerves
• Repeat GCS
Presenter
Presentation Notes
During your secondary trauma survey you will transition from the ”what will kill my patient now to what did I miss when treating those severe injuries. This is the perfect time to perform a quick neuro exam. Motor evaluation is critical during this part of the survey to identify neurologic deficit. Additionally assessing level of consciousness with a mini mental exam, and a cranial nerve assessment should help the provider better qualify the severity of the injury.
WHAT IS A “GOOD” NEUROEXAM?• Primarily Neurosurgeons and Neurocritical care providers will care about a few key
items• Motor Response
• Pupillary response and EOMs
• Check sensation and motor in all extremities (patient may move one side only and be GCS M6, but if you don’t assess the other extremities you may miss a deficit)
• Have a quick Cranial Nerve exam process. It is easy to evaluate and requires little to no tools.
• Can’t find an exam you Like?• The Navy’s Dive Manual has a good overall exam that can be completed in 10 mins or less
• The Prolonged Field Care CPG on TBI has another decent example
Presenter
Presentation Notes
But Brian what makes a good neuro exam? I am so glad you asked. Since you have an accurate GCS you should now focus on sensory, motor, in-depth ocular exams, and cranial nerves. In the interest of time I am not going to expand on the entire workup, but the Navy’s Dive Manual or the PFC guideline on TBI are great resources to use when developing a reliable exam you can easily and quickly replicate.
CONCERNING “EASY TO SEE” EXAM FINDINGS
Presenter
Presentation Notes
Some findings you may notice on the secondary survey are more apparent. In the top Left is a patient with facial ecchymosis and a fixed and dilated right pupil, its easy to suspect a brain injury in that patient. The lower left shows battle’s sign which suggests a basilar skull fracture and probably injury to the brain parenchyma. The photo on the left may show up in textbooks, though I can tell you without a pan optic or similar device you won't appreciate this finding. We have normal intraocular vasculature on the right and papilledema on the left. This is a late finding, but if you have the tools to get this view it may help drive further consult and care.
CASE
• 25yo M flips over his handlebars while cycling to work. He was not wearing a helmet. Bystanders report the patient was unresponsive at the scene for less then a minute then got up for a bit walking around, mildly confused, with limited recall of the event. EMS is called and the patient is taken to the hospital. He arrives at your trauma bay, responds incoherently, opens eyes when asked, and localizes to pain (E3V4M5). Is imaging indicated?
INDICATIONS FOR IMAGING• CT Head and Neck without Contrast
• “Stable patient” – do not delay operative intervention to obtain a CT• Especially in poly-traumas
• Most Head injury patients who are operative candidates will need a CT before the OR to show where the injury is and help with surgical planning
• A positive CT scan does not mandate surgery; it all about the exam findings
• CT Angiography• Not acutely indicated; Reserved for penetrating traumas and post
operative evaluation
• MRI Brain• Not Acutely indicate; Primarily used to evaluate acute ischemic events,
axonal injuries, or hypoxic brain injury severity
Presenter
Presentation Notes
When deciding when to image a head injury patient you need to remember that a scan should not prevent any life-saving interventions including a trip to the OR. Severe injuries are easy, if stable scan them if not get them to surgery. The milder ones require more finness. The Canadian CT Head Rule is a great tool for use in these patients. To summarize it states that a CT is required for minor head injury patients with any of the seven listed items. Important note…this rule does not apply to non trauma cases, GCS<13, AGE <16, patients on coumadin or those with bleeding disorders, or patients with open skull fractures.
WHAT ARE WE LOOKING FOR?
• “BLOOD CAN BE VERY BAD”• Blood
• Cysterns
• Bone
• Ventricles
• Brain
Presenter
Presentation Notes
If you don’t look at brain CT scans often here is a good mnemonic to focus your evaluation. Since this lecture is not on how to read a CT scan, we won't dive any deeper. If you have an opportunity to review normal head CTs do so, it makes finding the abnormal much easier.
INTRACRANIAL HEMORRHAGE
• Epidural Hematoma
• Subdural Hematoma
• Subarachnoid Hemorrhage
• Intraparenchymal Hemorrhage
• **Side Note**• Though not intracranial, Scalp Lacerations bleed profusely and should not be ignored.
Presenter
Presentation Notes
The main abnormality you will appreciate acutely is the intracranial hemorrhage. You may see one or some combination of these in the TBI patient. Like I mentioned in the anatomy section the appearance of blood on CT is dictated by the location within the cranium and meningeal layers. The last bullet up there is some free chicken, the scalp is profoundly vascular and bleeds profusely. Treat these with sutures, staples, or a good pressure dressing as soon as able.
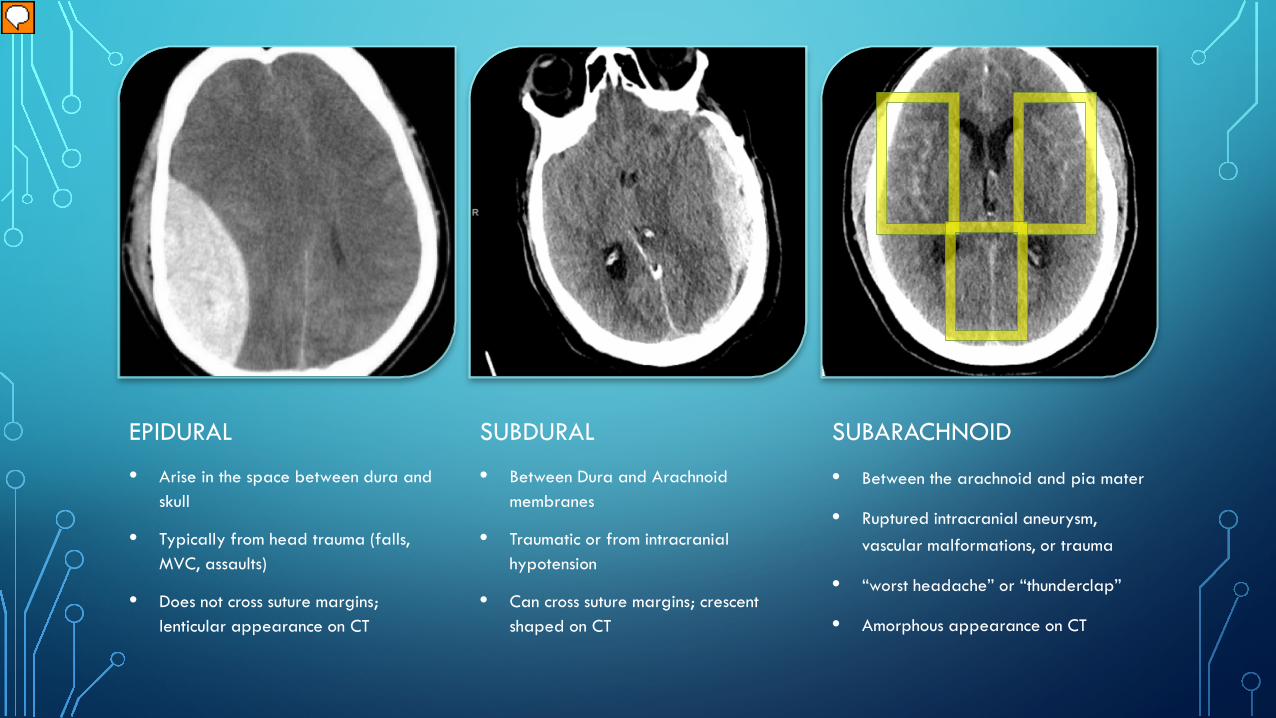
EPIDURAL
• Arise in the space between dura and skull
• Typically from head trauma (falls, MVC, assaults)
• Does not cross suture margins; lenticular appearance on CT
SUBDURAL
• Between Dura and Arachnoid membranes
• Traumatic or from intracranial hypotension
• Can cross suture margins; crescent shaped on CT
SUBARACHNOID
• Between the arachnoid and pia mater
• Ruptured intracranial aneurysm, vascular malformations, or trauma
• “worst headache” or “thunderclap”
• Amorphous appearance on CT
Presenter
Presentation Notes
Here are some common presentations of intracranial bleeds. The first two pictures are relatively easy to see thanks to the cranial anatomy and if you have a good radiologist probably a positive arrow sign. The Subarachnoid is a bit more subtle ****{click for box}*** but can be identified even by an Army PA.
CASE• Patient is stable and taken for a CT
head/neck.
• What does the CT show?
• What is a major worry in this patient?
Presenter
Presentation Notes
So back to our patient, we scanned him. What do we see on CT? what is a major concern after seeing this?
CASE
• You properly diagnose the patient with an SDH, you position the HOB at 30deg to help with ICP, get the patient a bed in the ICU and page Neurosurgery. While transitioning from the CT scanner the patient becomes unresponsive, E1V1M4. His left pupil is larger than his right with sluggish to no reaction to light. Vital signs: HR 60, BP 145/95, RR 30 and irregular. What is happening and what should you do next?
HERNIATION
Presenter
Presentation Notes
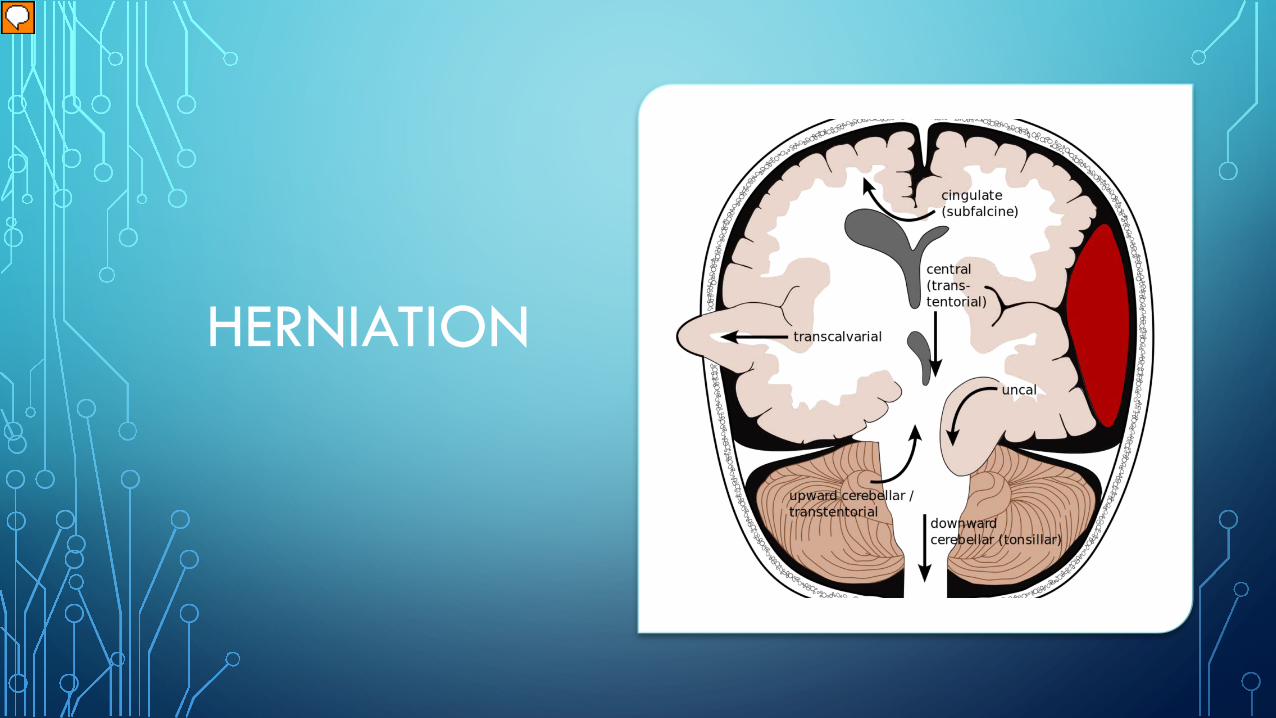
This patient is quickly decompensating and showing signs of herniation. This picture depicts ways the brain can herniate. Subfalcine or cingulate is regularly seen and usually is described as midline shift, it is usually corrected by decreased edema, craniotomy or craniectomy, or other intervention that reduces the mass effect or intracranial pressure. Uncal herniation is extremely dangerous as the brain is herniating through the foramen magnum and compressing the brain stem, disrupting the essential life processes the brain stem is responsible for.
Presenter
Presentation Notes
Ok let's look back at our CT scan. You can see the crescent shape that is seen with subdural hemorrhage. You can also appreciate the subfalcine herniation and midline shift in this scan.
INTRACRANIAL PRESSURE
• Monroe-Kellie Doctrine, 1783• The Skull is Non-distensible
• The Brain is Non-Compressible
• An increase in the volume of one component of the intracranial cavity will cause a decrease in the volume of the other components, an increase in pressure within the intracranial cavity, or a combination of the two.• “Non-compressible” components
• Brain (1300-1500ml, ~80%)
• CSF (75ml, ~10%)
• Cerebral Blood Volume (75ml, ~10%)
Presenter
Presentation Notes
Why does the brain herniate? In 1783 The Monroe-Kellie doctrine was first hypothesized, describing the pressure-volume relationship within the cranial compartment. When thinking of the Cranial compartment as a somewhat closed system with a rigid exterior and a non-compressible filling the primary buffers to abnormality are the CSF and to a lesser extent cerebral blood volume.
INTRACRANIAL PRESSURE
Presenter
Presentation Notes
Again for my visual learners this is a great depiction of the previous slide. Keep in mind that the Brain will try to compensate, but it can only do so much and when it reaches its limit intracranial pressure will increase and herniation becomes more likely.
HERNIATION
• Presentation• Sudden decline in mental status or decrease in GCS (usually 2 or more points)
• Non-reactive pupil
• Extensor Posturing
• Cushing’s response
• HTN
• Bradycardia
• Irregular Respirations
Presenter
Presentation Notes
I want to highlight some of the key symptoms and findings in a patient with imminent herniation. Sudden decline in mental status, pupillary changes, extensor posturing, and Cushing's response are all indicators. Cushing’s is typically a late finding and doesn’t always come as a triad. This is why serial neuro exams are so crucial while managing your patient.
CASE• GCS <8 Intubate!
• Vitals demonstrate Cushing’s response (typically a late finding)
• Elevate HOB to 30deg
• Check neck positioning and adjust C-Collar to help with venous return
• HTS bolus or mannitol if no HTS available
• Emergent NSGY consult, they need to see the patient and evaluate surgical options
Presenter
Presentation Notes
Because you are fantastic providers and had a decent lecture on head trauma you jump into action intubating the patient and providing noninvasive means to decrease ICP like elevating the head of the bed and adjusting C-collars, while your team prepares the hypertonic saline you ordered. This patient needs to see a neurosurgeon immediately, so you also get on the phone and call for a STAT consult.
INITIAL MANAGEMENT OF ICP
•HOB >30deg (venous return)
•C-Collar positioning (venous return)
•Hypertonic Saline (3%) bolus over 10mins• Ok through a peripheral line for short
duration
• Central Line is preferred.
•Mannitol 1g/kg IV or IO
• Non-selective, will cause systemic diuresis
Presenter
Presentation Notes
Increased intracranial pressure as we have highlighted is a major concern. It is important to initiate therapy immediately once symptoms are identified. In the trauma setting a head injury patient should always have the head of bed elevated and ensure the c-collar isn’t restricting jugular blood flow. If there is any focal neuro-deficit of cognitive impairment, consider use of hypertonic saline or mannitol. A lot of hospitals and providers may question use of hypertonic through a peripheral IV, however, literature and experience suggests that short duration use is appropriate in the acute setting of increased ICP. Mannitol, while effective should be reserved for transient responders to hypertonic saline given its systemic activity which can cause hypotension which of course is bad in the poly-trauma patient.
CASE
• Patient is now intubated, GCS 3T. He received a 250ml bolus of 3% HTS. NSGY has seen the patient and are preparing the OR for emergent Hemicraniectomy to decompress the cranium and evacuate the hematoma.
• If the patient hadn’t shown signs of herniation and went to the ICU how would it change their care?
Presenter
Presentation Notes
Read first part. This was an extreme case. And some of you may be thinking ”Brian, this doesn’t sound like a scenario that we would encounter OCONUS.” Well surprisingly this situation is based on a patient from my last unit who was injured while in Germany awaiting transportation into Africa. So keep in mind not all injuries in the deployed setting are combat related. Now for completeness sake, let's say there wasn’t a change after CT, and we are concerned about ICP. How do we monitor this patient?
ICP MONITORING
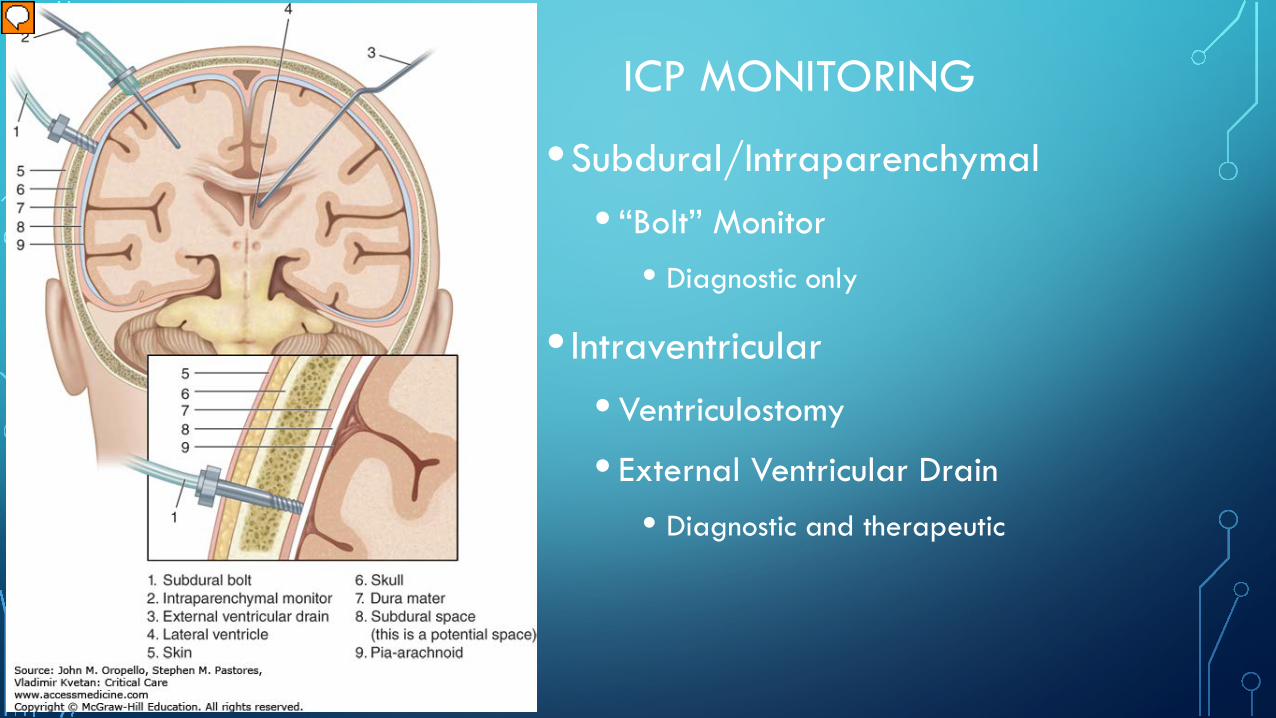
•Subdural/Intraparenchymal• “Bolt” Monitor
• Diagnostic only
• Intraventricular• Ventriculostomy
• External Ventricular Drain• Diagnostic and therapeutic
Presenter
Presentation Notes
If any of you have worked in ICUs you may have seen ICP monitors in place. These will be placed by Neurosurgery staff, or occasionally neurocritical care providers with appropriate training. Typically these will be a subdural or intraparenchymal bolt, or a ventriculostomy with an external ventricular drain. These monitors can be placed in the OR or at bed side.
KEY TAKE AWAYS
• Remember your Primary and Secondary surveys, don’t just assume the head injury is the only issue
• PREVENT SECONDARY BRAIN INJURIES
• Have a go to neuro exam and know the GCS scores
• Serial exams (Q1-2hrs) will help the provider identify progression
• Consult early! Brain is tissue and tissue is the issue; Protect it
Presenter
Presentation Notes
That was a long section and I promise the next section is much faster since we covered the key points already. But before we move on, if you had to remember anything from what we just discussed here is a great starting point.
AUSTERE MANAGEMENTNO SUPPLIES? NO EVAC? NO PROBLEM!
Presenter
Presentation Notes
Austere management, this is a section near and dear to my heart as I have spent the last four years working to educate and improve military medical provider’s skillsets to care for patients with limited equipment and capabilities in conjunction with the prolonged field care working group.
PROLONGED FIELD CARE
• Last decade (+)
• Linear medical protocols with robust evac systems and Role 3s
• The Medic/PA’s Job: POI-60mins
• Keep the red stuff inside: Tourniquets, Dressings
• Diagnose and manage the complications of polytrauma patients
• Nursing care
• Optimizing patient for transport to next echelon of care.
Presenter
Presentation Notes
Over the last, roughly, two decades our primary deployment theaters were well established with multiple role 1, role 2, and role 3 facilities coupled with readily available MEDEVAC assets. As forces have drawn down these assets have become scarce and some of our forces have shifted to new Areas of operation without significant medical support. Previously provider roles were clear, the medic/PA focused on TCCC and POI care, prep for transport, and load on EVAC. Surgeons focused on Damage control surgery and Resuscitation at role 2 facilities then evacuated to role 3’s for either definitive management and critical care efforts or to continue DCR/DCS until patient was stable enough to evacuate to Germany. Overall the goal was treating preventable death and evac to the next echelon of care.
UNCLASSIFIED
UNCLASSIFIED
• Memphis • Raleigh• Atlanta
• New Orleans
Tyranny of Distance
Iraq
Afghanistan
Presenter
Presentation Notes
One of the main issues with our current operational environment is the tyranny of distance. The Larger the Area of Operations the longer it takes to MEDEVAC a patient. On the left you can see Afghanistan and Iraq in relation to the United States. It is easy to appreciate why so many resources were required to facilitate battlefield care during OIF and OEF. Now focus your attention to the right. Africa is becoming a popular deployment destination primarily for Special operations Forces and Humanitarian mission sets. This photo encompasses the struggle medical providers will face in the coming conflicts. Little to no infrastructure in place and vast travel distances greatly impact the on-ground provider.
SO WHAT DOES THIS MEAN?
• Capabilities in our previously developed theaters are limited
• Role 1 providers have more responsibility to fill the gaps with drastically less equipment
• ICU in a Ruck concept
• Understanding injury/illness progression is essential to do the most good with the least amount of support and supplies.
Presenter
Presentation Notes
Again I like to provide context. The IRAQ and AFGHAN theaters have greatly reduced manpower and medical assets. And new theaters never had them to begin with. As the unit or on ground provider you may have to sit on patients for extended periods of time, meaning TCCC is not enough, you will have to employ some critical care skills to keep your patients alive long enough to make it to a Damage control resuscitation and surgery capability, keeping in mind this could be hours or even days. You would be surprised what you can do with a foundation in critical illness, a BP cuff and stethoscope, and good critical care nursing practices when in this situation. Ok SOAP BOX complete now back to head injuries!
HEMODYNAMIC CONTROL
• Goal Systolic BP: >110; keep MAP high so CPP is preserved.
• Best: active hemorrhage = transfuse Whole blood or blood products; target >110 SBP
• Better: administer 1L 0.9% NaCl (NS)
• Minimum: control external bleeds. Administer TXA, Avoid meds that will lower BP
JTS CPG: Traumatic Brain Injury Management in PFC 15AUG2017
Presenter
Presentation Notes
Goals for our patients in the austere setting are similar to the standards within CONUS hospitals. The major difference is you may not have the fancy tools to accurately measure most of them. Trust your training and your gut instinct and do the best with what you have. The highlight for hemodynamics, as with all trauma the best practice is to stop the source and replace what you lost…so give them blood. If you can’t give blood, avoid hypotonic solutions. TXA currently is indicated, though there is still some discussion amongst the Neruo specialties especially after the CRASH 3 trial. The CRASH Trials are a series of publications focused on medical interventions in traumas. CRASH 1 looked at corticosteroid use in head injuries. CRASH 2 evaluated TXA use in hemorrhage. CRASH 3 looked at TXA use in head injuries. The trial showed limited to no benefit for mild and severe TBIs but a significant improvement in morbidity when used in Moderate TBI. Since many of our traumas OCONUS are polytraumas it is best to use TXA given the current practices.
AIRWAY, OXYGENATION/VENTILATION
• GCS <8 Intubate
• Avoid hypoxia, hypo/hypercapnia
• Best:/Better Difinitive airway per provider (cric/ET) target SPO2 >95% and EtCO2 35-40mmHg.
• Minimum: NPA and Bag Valve Mask with supplemental O2 if available.
JTS CPG: Traumatic Brain Injury Management in PFC 15AUG2017
Presenter
Presentation Notes
Very similar focus with airway management. Again our goal is preventing the secondary brain injury, so hypoxia and hypercapnia is bad. You see we used SPO2 as a goal where in the hospital settings we use arterial blood gasses of PAO2 >80 which roughly equals an SPO2 of 95%. If you think the patient needs it take the airway by whatever means you feel most comfortable with or have the capability of performing. Worst case get your friends together and rotate through Bag-valve-mask shifts.
ICP MANAGEMENT• Expect in all GCS 8 or less and worsening neurologic exam.
• Best: Hypertonic Saline 250ml Bolus (over 10mins); repeat Q3 PRN . Mannitol if no 3% saline at 1g/kg IV or IO
• Better: stop possible causes; Pain, Anxiety.• Ketamine 20mg IV
• Fentanyl 25-50 ug IV
• Minimum: general measures• Elevate HOB
• Neck in midline position
• Properly position C-Collar
• **If Herniation is imminent consider hyperventilating the patient for no more than 20 mins to decrease ICP
JTS CPG: Traumatic Brain Injury Management in PFC 15AUG2017
Presenter
Presentation Notes
ICP management we already hit on, remember to use the non-invasive techniques in all head injuries, treat anything that could increase metabolic demand elsewhere in the body, and get hypertonic saline on board if able. In a pinch you can hyperventilate a patient. This decreases PaCO2 leading to vasoconstriction which reduces cerebral blood flow. This of course is not ideal for long periods of time so use only if necessary. If you are going to Hyperventilate the patient try to have an end tidal CO2 monitor and target an ETCO2, 32-35mmhg .
ICP: CAN WE MEASURE THIS OUTSIDE THE HOSPITAL?
• No “reliable” test for ICP measurement in the field
• Optic Nerve Sheath diameter • Can serve as an adjunct to the neuro exam
• Can identify if ICP is increasing or decreasing
• About 10-20 reps for most to become proficient
• Make this a new vital sign in all Head injury patients (Serial Exams)
JTS CPG: Traumatic Brain Injury Management in PFC 15AUG2017
Presenter
Presentation Notes
Can we measure ICP without the monitors we discussed. Not really. Currently there are no non-invasive modalities to measure ICP. There are some tricks to monitoring ICP in austere settings such as optic nerve sheath ultrasound.
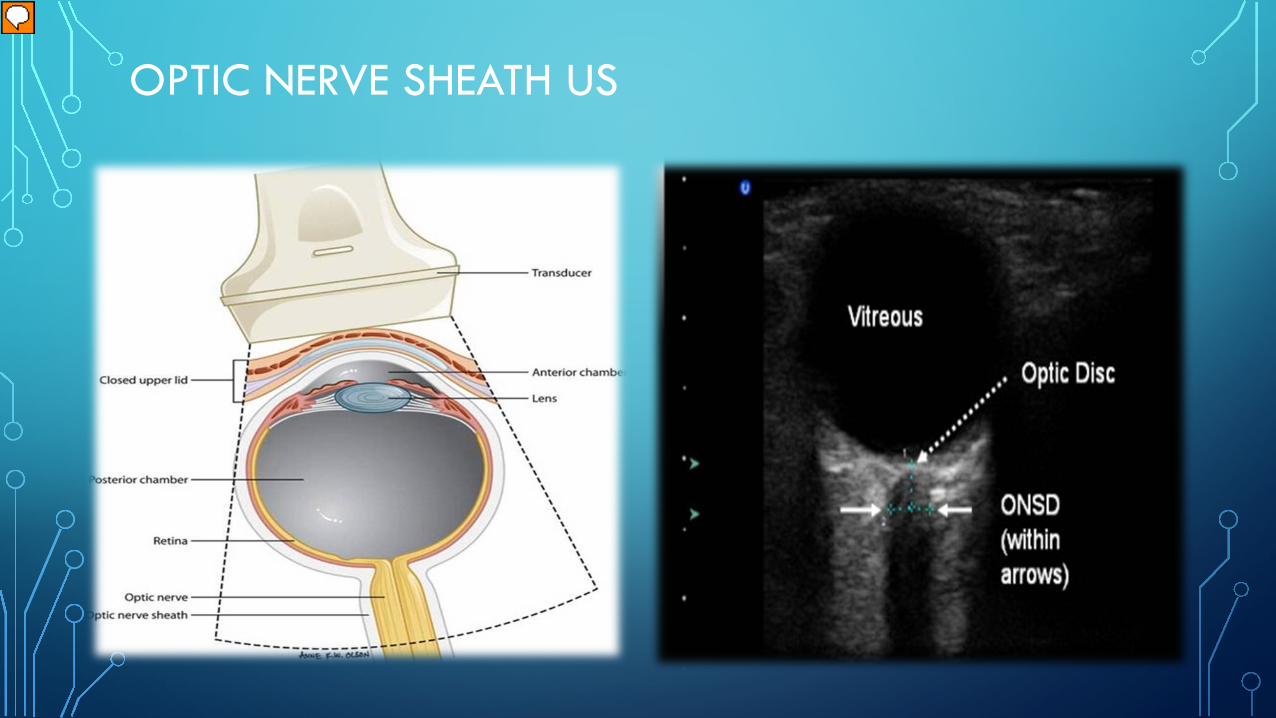
OPTIC NERVE SHEATH US
Presenter
Presentation Notes
Please keep in mind that the suggested use of this test is to trend optic nerve sheath diameter over time. There is no consensus as to what a normal nerve sheath should be, and current literature suggests it can range from 3.5mm to 6.5mm. Now if you have a head injury patient and get an initial measurement and an hour later it goes up you can attribute that to ICP elevation. Likewise if your treating a patient for elevated ICP and after therapy their diameter decreases you know the treatment is effective. Again it’s a tool not a absolute.
INFECTION CONTROL
• ABX are mandatory if penetrating or open injury.
• Best:
• Ceftriaxone 2g IV/IO Q8
• Metronidazole 500mg IV/IO Q8
• Better: Ancef 2g IV QD
• Minimum: Clean and Dress all wounds to prevent further introduction of potentially infectious materials
JTS CPG: Traumatic Brain Injury Management in PFC 15AUG2017
Presenter
Presentation Notes
Infection control is paramount in head injury especially penetrating trauma. Ceftriaxone and Metronidazole have great coverage for suspected pathogens and cross the blood brain barrier. If you don’t have those clean and protect any wounds and give what you can.
SEIZURE PROPHYLAXIS/MANAGEMENT
• Any witnessed seizure requires rapid response
• Best: Keppra 2g IV/IO; 500mg Q12
• Better: Phenytoin 1.5g for 1 hr then 100mg/day; or phenobarbital 1.5g for 1 hr then then 100mg/day
• Minimum: Midazolam 5mg q5 mins (Max 10-15mg) or alternate benzodiazepine if versed is not available. (lorazepam/diazepam)
JTS CPG: Traumatic Brain Injury Management in PFC 15AUG2017
Presenter
Presentation Notes
Seizures are another concern due to increased metabolic demand and impact in ICP. I doubt many of you pack your aid bags full Keppra, Phenytoin, or phenobarbital. Most of us will carry some form of benzo, typically midazolam and or valium. These will work to break the seizure but will not prevent them so use your judgment. As a side note if you have Keppra available a good practice is to initiate Keppra at 500mg q12 to prevent seizure development.
FEVER CONTROL
• Fever increases cerebral metabolism and can increase ICP. It also increases O2 demand elsewhere in the body
• Goal: 96F – 99.5F
• Best: Acetaminophen 650mg PO/PR Q4
• Better: Apply cold packs to axillary regions, posterior cervical region, and groin
• Minimum: remove unnecessary heat sources, place patient in a cool area
JTS CPG: Traumatic Brain Injury Management in PFC 15AUG2017
Presenter
Presentation Notes
The Brain on average is 1deg Celsius higher then the rest of body so fever is another item on the naughty list. Everyone in the room should know how to manage a fever so give them Tylenol and cool the patient until the fever subsides.
SODIUM MANAGEMENT
• Goal: Avoid Hyponatremia, target serum sodium between 145mmol/L and 160mmol/L
• Minimum: Avoid use of hypotonic solutions and restrict free water intake
JTS CPG: Traumatic Brain Injury Management in PFC 15AUG2017
Presenter
Presentation Notes
Osmotic gradients can be our greatest savior or worst nightmare. It may be difficult if not at a role 2 or higher to monitor Na levels, But if you can, aim for Na levels between 145 and 160. Avoid hypotonic solutions and restrict free water intake.
WHO YOU GONNA CALL?• Know when you have reached your
limits and where to get help
• ADvanced VIrtual Support for OpeRational forces (ADVISOR)
• DoD telemedicine network
• Use during training so you can better interact with the program while deployed
• Crucial in underdeveloped theaters
Presenter
Presentation Notes
Just like consults in the hospital setting you may need to phone a friend while deployed. Since TBI patients are generally complex, telemedicine could help you work through some of the potential critical care components of your patient’s care. The ADVISOR line is a great resource for any deployment.
WRAP THIS UP ALREADY…ITS LUNCH TIME.
• Head injuries are significant medical issues and should be closely monitored
• Memorize a basic neurologic exam and the GCS scores
• Prevent secondary brain injury; the key to all head injury patients
• If your resources are limited or you are intellectually maxed out use telemedicine to bridge the gaps
Presenter
Presentation Notes
Ok lets wrap up and get you to your break. Head injuries require a lot of time and resources, have a good go to neuro exam , remember interventions should aim to prevent secondary brain injury, and when resources are limited and your out there alone and unafraid , have a life line and use it.
GOOD REFERENCES
• Deployed Medicine App (JTS CPGs and best practices)
As promised here are some resources for your kit bag. Please don’t hesitate to reach out if you need more information or want other nice to have cheat sheets and references.
QUESTIONS?DISCLAIMER: “MAJ BRIAN SMEDICK HAS NO FINANCIAL INTERESTS TO DISCLOSE WITH REGARD TO THIS SUBJECT OR THE CONTENTS OF THE
PRESENTATION."
Presenter
Presentation Notes
And with that, thank you for your time, hopefully you all learned something new today, and enjoy your lunch. I will hang around if anyone has specific questions that they want to ask now or just shoot me an email.