Embed Size (px)
Citation preview

@ แพร 8 Feb 2012
HEADACHE: AN APPROACH
CHESDA UDOMMONGKOL MD PhD
Neurology-Phramongkutklao Hospital

@ แพร 8 Feb 2012
PAIN SENSITIVE : Dural Sinuses, scalp, arteries, falx cerebri INSENSITIVE: Most of the brain parenchyma, ependyma, pial veins (except dorsal raphe midbrain)
Anterior and middle cranial fossas : Trigeminal nerve Posterior cranial fossa : C1 C2 C3 cervical spinal nerves

@ แพร 8 Feb 2012
IHS Classification: ICHD-2
• Primary headache
- Symptom based
• Secondary headache
Etiology based
• Key to diagnosis is the “HISTORY”
(Wolff’s Headache)
HIS=International Headache Society

@ แพร 8 Feb 2012
1. Recurrent attacks
2. Symptoms free between the attacks
3. Clinical syndromes : IHS criteria
4. Physical examination: normal
5. No organic causes
Primary Headache

@ แพร 8 Feb 2012
Primary Headache
1. Migraine
2. Tension type
3. Cluster & other trigeminal autonomic cephalalgias
4. Other primary headaches
- Cough
- Exertional
- Headache associated with sexual activity
- Hypnic
- Primary thunderclap
- Hemicranial continua
- New daily-persistent headache

@ แพร 8 Feb 2012

Secondary headache
1. Progressive course
2. Symptoms persist
3. Pain selected to anatomical lesions
4. Physical examination usually abnormal

@ แพร 8 Feb 2012
• Vascular : ICH, SAH
• Meningitis
• Giant cell arteritis
• Sinusitis
• Systemic infection
• Idiopathic intracranial hypertension
• Spontaneous low CSF pressure
• Medication overuse
• Cervicogenic headache
• Others
Secondary headache

Acute
Sudden Chronic

@ แพร 8 Feb 2012
6.2.2 Headache attributed to SAH Diagnostic criteria:
A. Severe headache of sudden onset fulfilling criteria C & D
B. Neuroimaging (CT or MRI T2 or FLAIR) or CSF evidence
of non-traumatic subarachnoid hemorrhage with or
without other clinical signs
C. Headache develops simultaneously with hemorrhage
D. Headache resolves within 1 month
IHS

@ แพร 8 Feb 2012
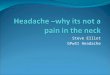
Acute SAH (5d) due to
a dissecting aneurysm
of the left VA
CT; T1-W; T2-W; &
G-echo T2*-W no SAH
A FLAIR showing SAH. J Chin Med Assoc 2005;68(3):131–7

@ แพร 8 Feb 2012
Subacute/chronic SAH
(10 d). CT; T1-W; Flair ;
T2-W; no SAH.
G-echo T2* W image
showing as low signal-
intensity areas in the
bilateral cortical sulci.
J Chin Med Assoc 2005;68(3):131–7

@ แพร 8 Feb 2012
T1 W contrast/ FLAIR contrast/FLAIR
Yoon et al. Radiology 2002;223:384-9
IVY sign

@ แพร 8 Feb 2012

@ แพร 8 Feb 2012 West J Med 1998; 168:203-212

@ แพร 8 Feb 2012
Migraine without aura A. At least 5 attacks lasting 4 - 72 hrs (untreated or unsuccessfully
treated), which has at least 2 of the 4 following characteristics:
1. Unilateral location
2. Pulsating quality
3. Moderate or severe intensity (inhibits or prohibits daily
activities)
4. Aggravated by walking stairs or similar routine physical
activity
B. During headache at least 1 of the 2 following symptoms occur:
1. Phonophobia and photophobia
2. Nausea and/or vomiting

Migraine with aura
A. At least 2 attacks fulfilling with at least 3 of the following:
1. One or more fully reversible aura symptoms indicating focal
cerebral cortical and/or brain stem functions
2. At least 1 aura symptom develops gradually over more than 4
min, or 2 or more symptoms occur in succession
3. No aura symptom lasts more than 60 min; if more than one aura
symptom is present, accepted duration is proportionally increased
4. Headache follows aura with free interval of at least 60 min
B. At least 1 of the following aura features establishes a diagnosis of migraine with typical aura:
1. Homonymous visual disturbance
2. Unilateral paresthesias and/or numbness
3. Unilateral weakness
4. Aphasia or unclassifiable speech difficulty

Migraine Aura ≠ TIA

@ แพร 8 Feb 2012
Migraine: a manifestation of neurological disorders
• Hemiplegic migraine (FHM)
• Alternating hemiplegia
• CADASIL (CARASIL)
• EA-2
• Paroxysmal torticollis
• Mitochondrial Disease

@ แพร 8 Feb 2012
หญง 28 ป ปวดศรษะดานซาย throbbing รนแรงมาก 2-3 สปดาห ตองนอน รพ. และ จ าเปนตองได opiate analgesic injection ชวงทปวด มองไมเหนภาพทางดานขวา รวมกบอาการชาปากดานขวา และชามอชาแขนดานขวา ตองนอนหลบตา ปวดมากนานกวา 1 ชม. มอาการมากกวา 1 ครงตอวน ไมออนแรง คลนไสไมอาเจยน
Am J Roentgenol. 2006;187:107-15
Moyamoya

@ แพร 8 Feb 2012
Tension-Type Headache
A. Headache lasting from 30 min to 7 days
B. At least 2 of the following criteria:
1. Pressing/tightening (non-pulsatile) quality
2. Mild or moderate intensity (may inhibit, but does not prohibit
activity
3. Bilateral location
4. No aggravation by walking, stairs or similar routine physical
activity
C . Both of the following:
1. No nausea or vomiting (anorexia may occur)
2. Photophobia and phonophobia are absent, or one but not both
are present

@ แพร 8 Feb 2012
Cephalagia 2004;4:1-160

@ แพร 8 Feb 2012 Cephalagia 2004;4:1-160

@ แพร 8 Feb 2012 HIS-Classification
Cluster headache
Cephalagia 2004;4:1-160

@ แพร 8 Feb 2012

@ แพร 8 Feb 2012

@ แพร 8 Feb 2012
INDOTEST
• Indomethacin-responsive headache syndromes:
PH, HC, jabs-and-jolts syndrome;
(icepick headache, hypnic headache, benign cough headache syndrome, benign exertional headache, coital headache, and thunderclap headache)
Trigeminal neuralgia (CPH-tic syndrome);
• The dose should be increased to at least 150 mg/d for 3-4 d.
• Beneficial effect is seen usually within 48 h.
• Maintenance dosage: 25-100 mg/d (range from 12.5-300 mg/d).

@ แพร 8 Feb 2012
• หญง 45 ป ปวดศรษะดานขวา นานกวา 1 ป ปวดนานประมาณ 10-15 วนาท รสกปวดแปลบ มอาการมากกวา 20 ครงตอวน รวมดวยกบอาการน าตาไหลดานทปวด บางครงมตาแดงรวมดวย
ประวตเพมเตม มอาการแบบนมากกวา 10 ปแตไมบอยเทาน
• SUNCT
• Treatment : Lamotrigine (case นได Carbamazepine)

@ แพร 8 Feb 2012

@ แพร 8 Feb 2012
Short-lasting Unilateral Neuralgiform headache attacks with cranial Autonomic symptoms (SUNA)
A. At least 20 attacks fulfilling criteria B–E
B. Attacks of unilateral orbital, supraorbital or temporal stabbing or pulsating pain lasting from 2 sec to 10 min
C. Pain is accompanied by one of:
1. conjunctival injection and/or lacrimation
2. nasal congestion and/or rhinorrhea
3. eyelid edema
D. Attacks occur with a frequency of ≥1 per day for more than half of the time
E. No refractory period follows attacks triggered from trigger areas
F. Not attributed to another disorder

@ แพร 8 Feb 2012
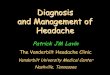
Aberrant loop of the PICA abutting CN V
J Neurol Neurosurg Psychiatry 2010;81:992

@ แพร 8 Feb 2012
Dissection of aberrant artery
J Neurol Neurosurg Psychiatry 2010;81:992
Worthy?

ผปวยชายไทย อาย 39 ป ปวดศรษะมากทงสองขาง ระหวางมเพศสมพนธชวงท orgasim เคยมอาการปวดประมาณ 4 ปมกเปนหลงมเพศสมพนธ แตเปนไมบอยโดยมกปวดตอมนทวศรษะทงสองขาง นานเปนชวโมง มอาการมากขนชวง 2-3 เดอนนจงมารพ.
ผปวยชายไทย อาย 48 ป ปวดศรษะมากทงสองขาง รนแรงเหมอนศรษะจะระเบด ขณะมเพศสมพนธ ไมเคยเปนแบบนมากอน ขณะมาถง รพ. ผปวยซมลง ถามตอบไดชา ตรวจพบ stiffness of neck
Case 1
Case 2

ผปวยชาย 32 ป ปวดศรษะมากทงสองขาง 1 วน หลงมอาการเกรงกระตกทงตวและหมดสต ปวดมนทบทงศรษะ ศรษะไมกระแทก เคยมอาการเกรงและกระตกแขนขวาเปนพกๆ มา 3 สปดาหและปวดศรษะทวๆเปนๆหายๆ มา 1 เดอน
MRI brain


@ แพร 8 Feb 2012
Headache attributed to spontaneous (or idiopathic) low CSF pressure
A. Diffuse and/or dull headache that worsens within 15 min after sitting or standing, with at least 1 of the following and fulfilling criterion
1. neck stiffness 2. tinnitus 3. hypacusia 4. photophobia 5. nausea
B. At least 1 of the following:
1. evidence of low CSF pressure on MRI (eg, pachymeningeal
enhancement)
2. evidence of CSF leakage on conventional myelography, CT
myelography or cisternography
3. CSF opening pressure <60mm H2O in sitting position
C. No history of dural puncture or other cause of CSF fistula
D. Headache resolves within 72 hours after epidural
blood patching
Cephalalgia 2004;24(S1):79-80

@ แพร 8 Feb 2012 Cephalagia 2004;4:1-160

@ แพร 8 Feb 2012
• ชาย 35 ปอายรแพทย Migraine, chest pain & thrombophebitis
: Morphine addict
• ชาย 40 ป เภสชกร ; chronic daily headache
: Cafergot dependent (overuse)
• หญง 42 ป ปวดศรษะรนแรงหยดงาน 1 สปดาห ตอมาดวย depression หลง LP เดมมปวดศรษะเรองรง
: Menstrual migraine
• พลทหาร 20 ป pain and arterial insufficiency in lower extremities หลง URI และรกษาปวดศรษะ
: Cafergot overdose
Complications of Headache