Embed Size (px)
Citation preview

Headache and Migraine Part 2
Headache and Migraine,
Part 21
I want to welcome you again to tonight's webinar which is Part Two of the Headache and Migraine course. My hope is that all of you have had the opportunity to experience Part One of this course, not only once but hopefully twice so that you can really lock in your learning. As always, I am going to assume that you have well-absorbed and are retaining informa�on for that first webinar and we're going to build on that material in tonight's session.
In terms of agendas, we're going to do a quick review of some of the key concepts from the first webinar and then we're going to talk for just a li�le bit about hormone-mediated headaches, or at least some of the most common categories of those. Cluster headaches which are thankfully fairly rare given how unbelievably debilita�ng that type of pain can be but I do want you to be aware of cluster headaches and what makes them unique. Then we will spend definitely the bulk of tonight's presenta�on on migraines. We're going to take quite a bit of a clinical deep dive into the biochemistry and physiology associated with migraines, at least our best understanding of them today.
Migraines, like many modern common inflammatory states are quite complex and cover a number of different body systems. We're going to talk about today's understanding of what causes migraines and I'm going to share with you some of the top natural remedies that you can consider recommending to your clients who struggle with migraines. Especially where they may be ge�ng relief from more than one category of symptom by using certain types of remedies or supplementa�on or dietary changes. We'll talk about some of the overlapping symptom dynamics that can exist in order to give you clues about which remedies will work best for your individual client.
I'm going to talk in par�cular a bit in-depth about the no�on of cellular energy produc�on as it relates to migraine. Now, I do want to say as a precursor that we have an en�re SAFM Clinical course on cellular energy produc�on. I'm certainly not going to try and repeat even a substan�al amount of that in tonight's program. But I am going to cover some summary points because it's a great example of the fact that we need good cellular energy produc�on in every cell of our body.
If we don't have good cellular energy produc�on in our hearts, then we might wrestle with different types of arrhythmia or simply with low cardiac output. If we have low cellular energy produc�on in our muscles, then we're not going to have as much strength or stamina. Low cellular energy produc�on in our GI tract, we may not produce as many diges�ve fluids or have adequate mo�lity. Similarly, if we lack adequate genera�on in certain neural structures in the brain, then indeed migraine can be one of the outcomes.
We're just going to do a quick summary on some of the key dynamics in cellular energy produc�on. And then I will wrap us up with a summary specific to migraines and then I'll also show you a quick case study from my own client files. As always, I encourage you to post your ques�ons as we move along or if you are listening to this course in recording. A gentle reminder that you are always more than welcome to post your follow-up ques�ons a�er the webinar on the Headache and Migraine course page.
Headache and Migraine,
Part 2
2
Now, we talked before about the functional medicine view at the bird's eye level of a headache and this view is
certainly common to an awful lot of modern chronic inflammatory multi‐system dynamics. Where a number of
the various types of choices that our clients and patients might make in their lifestyle have a huge impact on the
existence, the persistence, the frequency and the severity of their symptoms, certainly including migraines. It's
really the notion of how our choices affect our various biochemical systems or physiological systems individually
and then also in an interactive way that can play a huge role in our perceived state of wellness or illness.
Now, given what we've already covered, you can start to see some of the specific dynamics that are involved in
these various systems as it specifically relates to a headache. In particular, as it relates to a migraine. Certainly,
the most debilitating, relatively common type of headache. We've talked a little bit about all of these dynamics
certainly after thoroughly reviewing both of the webinars in this course. I think you will be in a position of having
a keen understanding and a good comprehensive insight into how these dynamics interact in the case of
migraine.
I want to start off with a brief recap of some of the particular dynamics that we talked about in regard to
headache. In the first webinar, we talked quite a bit about typical chronic daily tension headaches. Which are
certainly the most common type of headache. We talked a bit about the etiology of pain and how we perceive
pain in the brain; that nociceptors are tissues that can be affected by a number of different stimuli and register
as pain in the brain.
Now, we talked about a number of different common causes of headaches and some very typical and some
more esoteric. I've included the cartoon I shared with you last time. I like to show that to my clients as well as a
gentle reminder of the fact that more often than not, it is the more simple straightforward, obvious root causes
that can have the largest impact on greater wellness with our clients as opposed to the more esoteric or unusual
types of drivers. Keeping in mind that simple explanation such as being mildly dehydrated, being mildly deprived
of sleep, having too much stress, working at a job where there's too much repetitive motion or perhaps
improper posture, and then also having insufficient magnesium which is certainly common in most Western
cultures. These are all very straightforward dynamics that as you work with your clients to coach them on
implementing specific recommendations about lifestyle improvement, these can have huge impacts.
I'm amazed at how often addressing this small handful of dynamics gives my clients dramatic relief from
headaches. While we're diving into a deeper understanding of the physiology and also some of the more
esoteric reasons for headaches. Please always keep in mind that it pays to start with the simple and prioritize
implementing the simple and obvious first before diving into more esoteric dynamics.
All headaches are exacerbated by stress. We talked about how the exacerbating and sustaining effect that stress
has on pain pathways in the brain. That there are wide variety of different types of headaches. We talked about
how conventional treatment for headaches can have surprisingly dramatic negative side effects in the body even
for over‐the‐counter medication. In particular, I shared in our first webinar how often I see a fairly well
entrenched gastrointestinal dysfunction in clients who have been through a period of time maybe even for just
three or four months where they had some type of struggle with pain and were taking over‐the‐counter NSAID
medications on a daily or perhaps even twice daily basis.
Headache and Migraine,
Part 23
We even learned a li�le bit about rebound headaches and how excessive painkiller or NSAID an�-inflammatory drug use can actually completely on their own encourage or promote headaches. I think in terms of looking at something more clinical or nutrient related, it's very important for chronic headache to always be checking magnesium status. I think in the absence of kidney issues, drama�c kidney filtra�on issues or certainly any type of documented kidney disease, outside of that, I believe magnesium supplementa�on at moderate levels is really quite safe and certainly it is a need for an awful lot of our clients given the prevalence of insufficient magnesium.
Now, we talked about some natural alterna�ves to the non-steroidal an�-inflammatory drugs or NSAIDs that are so o�en taken in popping a pill to try and alleviate headache pain. I've summarized some of those for you here, and added a couple of addi�onal ones that really don't have too much research into them but definitely have the poten�al capability of reducing that par�cular type of inflamma�on.
Let's move on from this to talk a li�le bit specifically about hormonal headaches. Now, these generally are always going to be associated with women, specifically the experience of the menstrual cycle. Now, we have an en�re course in School AFM called Demys�fying Hormones that does very deep dives into hormones for both men and women. But talking about the roles of the various hormones and how imbalanced in the various hormones or rela�vely high or low levels can cause a huge variety of different types of dysfunc�on, not only in the gonads but systema�cally throughout the rest of the body.
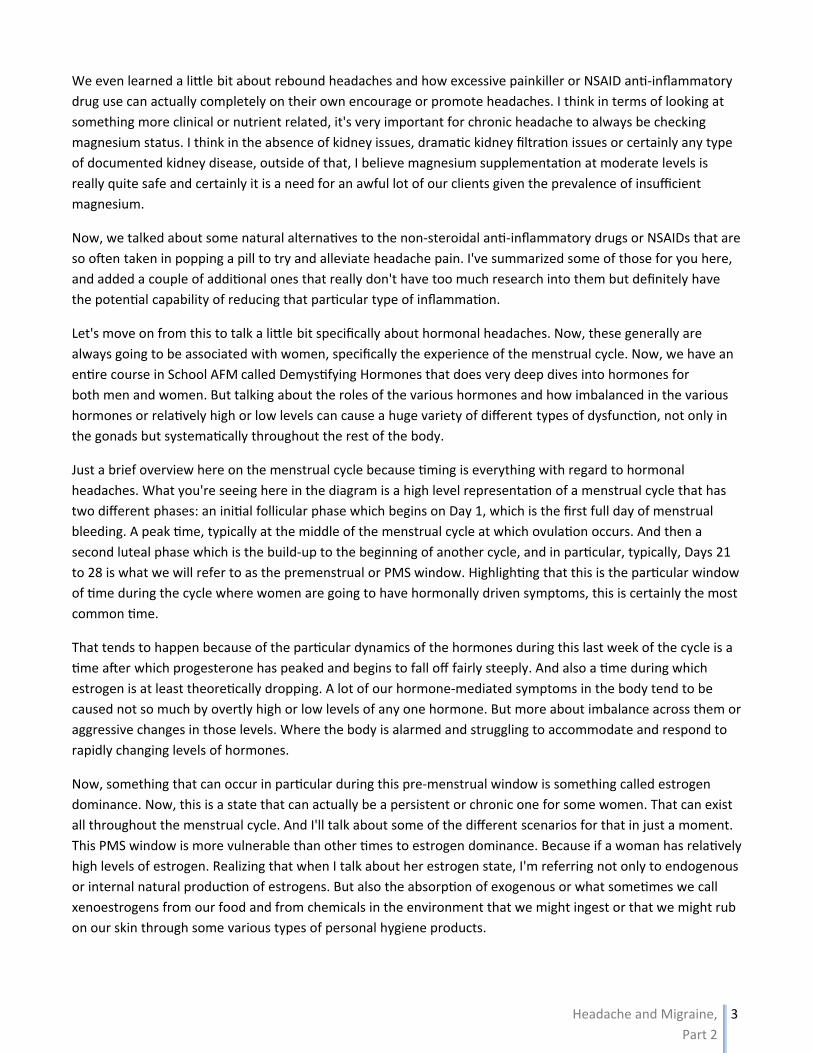
Just a brief overview here on the menstrual cycle because �ming is everything with regard to hormonal headaches. What you're seeing here in the diagram is a high level representa�on of a menstrual cycle that has two different phases: an ini�al follicular phase which begins on Day 1, which is the first full day of menstrual bleeding. A peak �me, typically at the middle of the menstrual cycle at which ovula�on occurs. And then a second luteal phase which is the build-up to the beginning of another cycle, and in par�cular, typically, Days 21 to 28 is what we will refer to as the premenstrual or PMS window. Highligh�ng that this is the par�cular window of �me during the cycle where women are going to have hormonally driven symptoms, this is certainly the most common �me.
That tends to happen because of the par�cular dynamics of the hormones during this last week of the cycle is a �me a�er which progesterone has peaked and begins to fall off fairly steeply. And also a �me during which estrogen is at least theore�cally dropping. A lot of our hormone-mediated symptoms in the body tend to be caused not so much by overtly high or low levels of any one hormone. But more about imbalance across them or aggressive changes in those levels. Where the body is alarmed and struggling to accommodate and respond to rapidly changing levels of hormones.
Now, something that can occur in par�cular during this pre-menstrual window is something called estrogen dominance. Now, this is a state that can actually be a persistent or chronic one for some women. That can exist all throughout the menstrual cycle. And I'll talk about some of the different scenarios for that in just a moment. This PMS window is more vulnerable than other �mes to estrogen dominance. Because if a woman has rela�vely high levels of estrogen. Realizing that when I talk about her estrogen state, I'm referring not only to endogenous or internal natural produc�on of estrogens. But also the absorp�on of exogenous or what some�mes we call xenoestrogens from our food and from chemicals in the environment that we might ingest or that we might rub on our skin through some various types of personal hygiene products.
Headache and Migraine,
Part 2
4
We can end up with an overall estrogen load that may be quite high. Or we can end up with an estrogen load
that is just relatively higher than our progesterone levels. Again, the Demystifying Hormone course covers this in
pretty significant detail but when we go through periods of our life where we are under a lot of stress, especially
during the perimenopausal or postmenopausal years. We can end up with low or suboptimal levels of
progesterone. What can happen during this PMS window is that there are actually lower levels of progesterone
where maybe it has a lower peak or it falls off more aggressively and there are relatively higher levels of
estrogen and these two lines actually end up crossing a bit or coming too close to each other. Then there's a
relative state of estrogen dominance. This is important because that type of hormone imbalance can cause
inflammatory symptoms in the body.
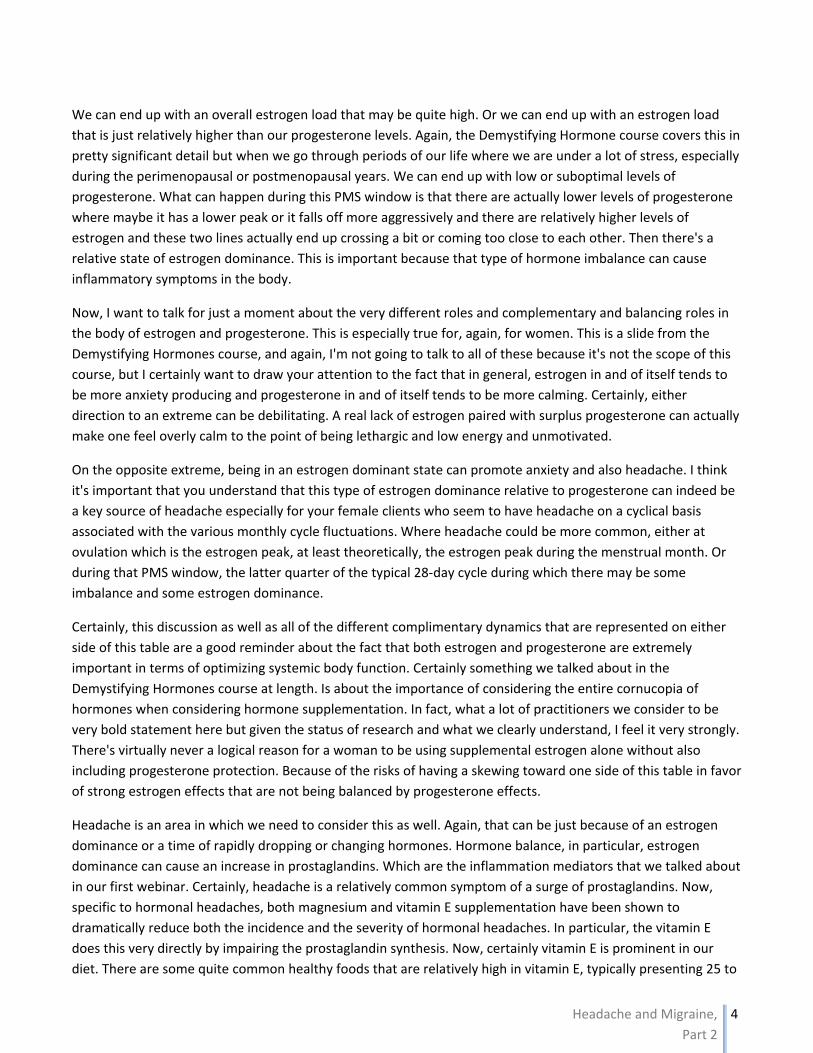
Now, I want to talk for just a moment about the very different roles and complementary and balancing roles in
the body of estrogen and progesterone. This is especially true for, again, for women. This is a slide from the
Demystifying Hormones course, and again, I'm not going to talk to all of these because it's not the scope of this
course, but I certainly want to draw your attention to the fact that in general, estrogen in and of itself tends to
be more anxiety producing and progesterone in and of itself tends to be more calming. Certainly, either
direction to an extreme can be debilitating. A real lack of estrogen paired with surplus progesterone can actually
make one feel overly calm to the point of being lethargic and low energy and unmotivated.
On the opposite extreme, being in an estrogen dominant state can promote anxiety and also headache. I think
it's important that you understand that this type of estrogen dominance relative to progesterone can indeed be
a key source of headache especially for your female clients who seem to have headache on a cyclical basis
associated with the various monthly cycle fluctuations. Where headache could be more common, either at
ovulation which is the estrogen peak, at least theoretically, the estrogen peak during the menstrual month. Or
during that PMS window, the latter quarter of the typical 28‐day cycle during which there may be some
imbalance and some estrogen dominance.
Certainly, this discussion as well as all of the different complimentary dynamics that are represented on either
side of this table are a good reminder about the fact that both estrogen and progesterone are extremely
important in terms of optimizing systemic body function. Certainly something we talked about in the
Demystifying Hormones course at length. Is about the importance of considering the entire cornucopia of
hormones when considering hormone supplementation. In fact, what a lot of practitioners we consider to be
very bold statement here but given the status of research and what we clearly understand, I feel it very strongly.
There's virtually never a logical reason for a woman to be using supplemental estrogen alone without also
including progesterone protection. Because of the risks of having a skewing toward one side of this table in favor
of strong estrogen effects that are not being balanced by progesterone effects.
Headache is an area in which we need to consider this as well. Again, that can be just because of an estrogen
dominance or a time of rapidly dropping or changing hormones. Hormone balance, in particular, estrogen
dominance can cause an increase in prostaglandins. Which are the inflammation mediators that we talked about
in our first webinar. Certainly, headache is a relatively common symptom of a surge of prostaglandins. Now,
specific to hormonal headaches, both magnesium and vitamin E supplementation have been shown to
dramatically reduce both the incidence and the severity of hormonal headaches. In particular, the vitamin E
does this very directly by impairing the prostaglandin synthesis. Now, certainly vitamin E is prominent in our
diet. There are some quite common healthy foods that are relatively high in vitamin E, typically presenting 25 to

Headache and Migraine,
Part 2
5
30 milligrams of vitamin E per serving, in particular things like sunflower seeds, almonds and spinach.
When the hormones are relatively common, I mean we might all have a perfect storm where we would have a
hormone‐mediated headache, at least women, a couple of times a year. If it is chronic or particularly
debilitating, I highly recommend using supplementation in order to alleviate that. Especially because as we
talked about before, the persistence of the pain in headache can lead to its exacerbation and also predisposes
one for a depression and other types of debilitating symptoms.
What you're seeing here is my current favorite supplement recommendation for vitamin E which is a product
called toco‐sorb made by a company called Harrow. I like this because it's one of the few supplements out there
that actually presents true full spectrum vitamin E. Now, as is common in many supplements which is why it's so
important to be savvy and to give your clients very specific recommendations on which brands or forms to use,
the vast majority of vitamin E that is included in supplements is a synthetic form and you can recognize that in
the naming convention because it will be usually DL and it's the L here that's the giveaway. DL‐alphatocopherol
is by far the most common type of vitamin E included in supplements and it's a synthetic form that has been
shown to not be as effective as the natural forms.
In particular, there are specific roles of all the tocopherols and the tocotrienols, including just one particular
form of vitamin E rather than all eight of them is going to be suboptimal. This particular supplement includes all
of them. One capsule daily would supply 400 milligrams collectively of vitamin E which is a good healthy dose
and quite sufficient based on what was used in the studies in order to have dramatic effects for headache
reduction.
Now, when we look at some of the different root causes of estrogen dominance and some of the symptoms.
Again, we cover this in‐depth in the dedicated course. But I want you to understand that estrogen dominance is
not necessarily an excess estrogen state. It can be. Certainly based on the huge variety of estrogenic molecules
that we can pickup in our external environment. And it's important to understand that in any type of hormonal
testing where one is looking at measuring the three typical human estrogens: estrone, estradiol, and estriol.
That levels of xenoestrogens or exogenous estrogens that we pick up from our environment are not going to be
reflected in those totals. What we're really going to see in that data is really what is produced internal to the
body or what might be taken in supplement form that is bio‐identical.
Unfortunately, there are many different types of estrogenic molecules and our clients who use the typical
national brands of personal hygiene products or who consume hormone‐laden conventionally raised animal
foods. Who eat pesticide‐sprayed, herbicide‐sprayed foods. These are individuals who are going to typically be
at greater risk for struggling with estrogen dominance. We know that caffeine can over‐sensitize estrogen
receptors which can exacerbate symptoms of estrogen dominance.
We also know that intake of mild or weakly estrogenic foods like flax seed or curcumin or rosemary or lavender.
These are things that can actually increase our circulating levels of weak estrogens and populate our estrogen
receptors with more weak estrogens. Which leaves less room for strong estrogens to fit into receptors. Although
it may seem illogical or backward from what you would expect, supplementing with weakly estrogenic foods can
actually help to improve an estrogen dominant situation by putting more weak estrogens into receptors that
could otherwise be housing and registering the effects of strong estrogens.
Headache and Migraine,
Part 2
6
Now, some people can struggle with a estrogen dominant state because of impaired ability to detoxify or
excrete estrogen. We use the different biochemical detoxification processes, in particular, sulfation, methylation
and glucuronidation in order to detoxify and excrete most steroid hormones, including estrogens. And also being
constipated or having overgrowths of certain bacteria in the gut can also impair our ability to excrete excess
estrogen through our GI tract when the body chooses to do so.
There are a number of different things that can get in the way of this. I think a very simple tip that can help with
that dynamic is simply increasing intake of cruciferous vegetables. Which contain a couple of different
phytonutrients, in particular, I3C or indole‐3‐carbinol. Which accelerates the body's ability to detoxify estrogen
down these pathways. B‐complex is something that people might need in order to up‐regulate methylation
especially if they have genetic impairment in methylation pathways. For many people, simply increasing the
intake of course cruciferous vegetables is sufficient. And in particular, broccoli and especially broccoli sprouts
are really quite high in these supportive compounds.
Now, people can also wrestle … Women can also in particular wrestle with insufficient progesterone. And I give
you some thoughts here on when that is more likely to be. Again, I'm not going to focus too much on this in this
particular course. But I want you to be aware of these dynamics and aware of hormone‐mediated headache and
aware of some of the types of drivers for the hormone imbalance for the hormone state that can cause it and
aware of some of the simple remedies that could give dramatic improvement.
Certainly, for women who are used to having debilitating headaches, especially migraines during the menstrual
period. That's a wonderful way to help create a wildly satisfied client or patient. As you likely already well know,
headache is one of the areas I focus on consistently in my own practice for addressing right away to try and
bring rapid relief to my clients as a way of galvanizing their passion for their work with me and their belief in
their body's ability to heal.
All right. We're going to move from hormonal headaches now to talk about cluster headaches. Now, if you ever
had a cluster headache or you know someone that does, you are definitely going to concur with the word I've
used here which is excruciatingly severe. There's all sorts of anecdotal information even including in clinical
studies where people talk about this being the worst pain they've ever experienced. Even people comparing it to
the pain of childbirth without painkillers or the pain of passing kidney stones or the pain of passing gallstones, a
gallbladder attack. Even in people who've experienced both, this is regarded as more severe and more
debilitating pain.
It's a bit unusual in that it tends to originate behind the eyes. And then the feeling that it is spreading further
back into the head and sometimes spreading to the sides of the head. Cluster headaches are a bit unusual in
that they tend to recur in a somewhat predictable pattern, maybe multiple in a given day, multiple in a given
week or month. But followed by very significant periods of time, often many months without any headaches at
all. They tend to follow, again, some sort of cycle. They may occur during the similar times of day when they are
active. And cycles may also respond to various seasonal changes.
These are a bit unusual and quite a bit different from migraines in that they tend to be relatively short in terms
of duration, unlike a migraine. These might last for just a few minutes up to maybe an hour or two. But they can
often be accompanied by other debilitation in the face, in particular, watery or bloodshot eyes. There may
actually be a bit of neuropathy of drooping eyelid in the eye area, and also a runny nose. There may be twitching
Headache and Migraine,
Part 27
in the face as well and the pain may radiate actually into the teeth.
Now, interes�ngly enough, while migraines are much more common in women. Cluster headaches are much more common in men, and especially rela�vely young adult men. As I said earlier, thankfully, this is a rela�vely rare type of headache, typically occurring in less than 3% of the chronic headache popula�on.
Now, cluster headaches. We fairly well understand what is happening with cluster headaches. And as you might expect if you've been a SAFM Course par�cipant for some �me and if I were to ask you what part of the brain might be likely being affected when there is cyclical or even seasonality dynamic in headaches. And that is involving fluctua�ons in the hypothalamus. Which is the part of the brain that plays a huge role in regula�ng overall endocrine func�on or hormonal func�on and coordina�on in the HPATG axis. It also plays a drama�c role in our sleep-wake rhythms, especially with regard to regula�on of the pineal gland and, therefore, our melatonin synthesis. It's also been demonstrated in research that there is usually, not always, but usually involves some type of hyperac�va�on, specifically of the trigeminal nerve. Which is prominent in the front part of the head and in the face.
Interes�ngly enough, I think current research is honing in on the combina�on of a lack of synchroniza�on between the typical diurnal curve of cor�sol and the typical diurnal curve of melatonin secre�on. I'm giving you, as always, a lot of different clinical references here if you want to do a deep dive into some of these topics if they interest you. These are, of course, two different pathways, right? The typical cor�sol secre�on. That would come from the adrenal glands s�mulated by the hypothalamus through the pituitary. Which gives us our primary stress hormone that mediates a lot of our typical waking pa�erns as far as ac�va�ng various gland and �ssue func�on.
The pineal gland in the brain, also being guided by the hypothalamus, secre�ng melatonin. Which is as you likely know, a cri�cal neurotransmi�er and hormone with regard to media�ng sleep. But also an extremely powerful an�oxidant in the body overall and certainly, in par�cular, in the brain. This type of lack of synchroniza�on, when it is paired with low levels of testosterone and melatonin in concert with high cor�sol. Now this may seem like a pre�y esoteric or unusual combina�on of things and perhaps that speaks to the rela�vely low occurrence of these headaches. But it really represents a de-synchroniza�on within really cri�cal cyclical hormonal cycles in the body on a daily basis.
What's very interes�ng is that typically NSAID medica�ons are not effec�ve for these types of headaches. And that's probably not a surprise to you. Conven�onal therapy in terms of triage would typically involve oxygen and sumatriptan. Which can decrease trigeminal nerve hyper reac�vity. Sumatriptan is a serotonin agonist. And then also glucocor�coids, typically prednisone, for acute pain just in terms of very aggressively reducing inflamma�on that is being caused by this par�cular physiological dynamic in the body.
Now, unlike a lot of other types of headache, a key symptom of people who are in a cluster headache is restlessness. And typically they demonstrate the fact that physical ac�vity helps to reduce the pain. Some level of pacing or rocking or even head banging, banging the head against the wall or hi�ng something with your fist. These can help to reduce, or take the edge of rather, the intensity of the pain. Now during periods of �me where someone who is prone to cluster headaches is actually experiencing ac�va�on. Lifestyle choices such as alcohol intake and smoking and napping can all be strong triggers for cluster headaches. Interes�ngly enough, research shows that these lifestyle choices during the dormant �mes of the year when a person is not experiencing these
Headache and Migraine,
Part 2
8
headaches, these choices can be chosen and will not trigger a headache.
Again, it speaks to the notion of a circadian pattern and also typically a seasonal pattern. Which certainly makes
sense given the shift in our circadian rhythm that happens in response to the changing daylight patterns
throughout a typical year.
I think really fascinating dynamics with regard to cluster headaches and certainly addressing this type of
hormone imbalance and insufficiency has been shown in clinical study to be the most promising pathways of
effectively addressing and alleviating cluster headaches so that they are less frequent and less severe.
Now I want to move on to migraine headaches. Which are certainly much more common. We talked about the
fact that tension type headaches are the most common. But as far as a more debilitating headache, migraines
are the next most common in particular for women. Migraines affect women more than twice as much as men.
Migraines are characterized by a throbbing type or a pulsing type of debilitating pain in the head often affecting
only one half of the head though it can be experienced on both sides. It may or may not be accompanied with
visual aura or visual disturbance such as blurry vision or double vision. It might be accompanied with extreme
nausea or vomiting as well as pretty acute light or noise sensitivity.
Migraine sufferers usually seek to be as still as possible and find that even the smallest of movement worsens
the headache. This is a good example of how migraines are very different from cluster headaches. Migraines
also differ in the fact that they tend to unfortunately last a fairly long time. Typical migraine can last anywhere
from 4 to 48 hours. Occasionally, a more extreme example might be as long as 72 hours. I would say in my
experience, just in my own client base, a typical migraine last about 24 hours.
We do understand that there are familial predispositions for migraines; they can run in families. We don't
necessarily understand the full set of genetic variants that can contribute to that, although I think more recent
research in the past 5 to 10 years in particular is really honing it in on differences with regard to serotonin
sensitivity. The behavior and the sensitivity of serotonin receptors, particularly in the brain. We talked a little bit
about the role of serotonin in our first webinar and certainly it is even much more dramatic in the etiology of
migraines in particular.
Now as we get into the discussion here on migraines, it's probably going to start to make a little bit more sense
why we also believe through study that the incidence of migraines has increased dramatically in the past several
decades. And in particular, studies have shown that during the decade at the end of the last century, the
incidence of migraines increased by more than 50%. Now when we think about the number of lifestyle choices
that we have that might dramatically increase inflammation or oxidative stress. And that twisted, terrible feed
forward cycle where inflammation increases oxidative stress and oxidative stress increases inflammation.
Especially given the prevalence of high stress, low nutrient, high toxin, high chemical lifestyle choices that we
can make. It's perhaps not a surprise that migraines have become more prevalent.
Let's talk a little bit about the pattern of a migraine because most migraines have very predictable phases.
Periods of increased stress or inflammation can create what is known as a typical higher vulnerability to a
migraine. Interestingly enough, a lot of migraines occur during the letdown phase after a period of acute stress.
Migraines are more likely to happen on the weekend. Some people are much more likely to experience them
during vacation. I've actually had a couple of clients experience this where they knew that after working on a
particularly intense work project or coming off of a particularly demanding period of work, when they were
Headache and Migraine,
Part 2
9
going on vacation and perhaps even working harder in preparation for that vacation. They would unfortunately
be setting themselves up for a migraine.
This diagram from a study in Lancet magazine, I think very well demonstrates the typical pattern. The amplitude
of the curve here really representing the level of discomfort or pain and a period of vulnerability leads into the
initiation of migraine attack that starts with what is called a proteome. This is when people can experience their
own unique early warning signs for a migraine. Interestingly enough, these early warning signs can be really far
ranging, and in some cases opposite for different individuals. But if you talk to people who experience chronic
migraines. They will, in my experience, very quickly tell you what those warning signs are. They just know.
"I'm going to have this feeling where I'm particularly vulnerable and I'm very moody and irritable, I know that
within about 24 hours or so my migraine is going to hit." On the other hand, some people will say they get into
this state where they are not only feeling very good but they feel like what they would consider to be a period of
euphoria that would belie the migraine to come in the following day or two.
Many people experience an aura phase. This is a period of time during which they will have neurological
disturbances. Now we associate aura specifically with vision. Where people can see various types of color or
hazy lights, maybe flashing lights, and again a disturbed sense of vision. Aura can also involve or instead involve
other senses like smell or taste. Imagined odors, for example, as well as disturbances in speaking. The aura
phase is usually a time during which there is a ramp up in discomfort, usually the initial twinges of a headache
that rolls over into the bulk period of the migraine itself. This can be anywhere to debilitating enough that
someone feels the need to just come home from work and relax all the way up to someone feeling that they
need to be in a completely dark, silent room completely undisturbed in order for the pain to even be tolerable.
You can imagine the debilitation of that. Especially if those migraines last up to two or three days.
Now the resolution phase that what one would call a postdrome often is characterized by lengthy deep sleep.
And perhaps this is not a surprise just based on our expected reaction to the stress of the headache itself. It's
also believed that the period of deep sleep is a time during which the brain chemistry is recalibrating itself. And
the deep sleep is necessary for the brain to recover neurologically from the migraine itself. It would certainly be
common for up to 24 hours post headache itself for people to report higher levels of fatigue or malaise and
occasional lower intensity return of the headache pain itself. Especially after a bout of coughing or a sudden
head turn or a sudden standing up. I've had a couple of clients refer to this as hangover or aftershock of a
migraine.
As you know, there are a number of different documents posted on the Headache Migraine page, as with all of
our courses, to give you more information. Some of these documents are made‐for‐you handouts that you can
readily use with your clients or copy and paste right into your own customized handouts to use with your clients.
But a number of them are posted in order to give you deeper or more detailed clinical information about some
of the topics covered in the course. The Lancet article here which dives in‐depth into the etiology of a migraine, I
actually pulled down as a PDF file and posted that in the course documents. If you really are passionate about
migraine and supporting clients and patients with migraine, I highly encourage you to review this in detail so you
can become more comfortable with and conversant in the various phases and the wide variety of types of
triggers of migraine.
Now let's talk a little bit about migraine physiology. As a geek myself, I find all of this very fascinating. But
certainly I've posted some additional documentation about it. But I want to summarize for you that we've spent

Headache and Migraine,
Part 2
10
a lot of research effort over the past few decades trying to really understand what actually causes a migraine.
We've had a lot of different theories about it and it's taken a while for us to really pull the various theories
together into a single unified theory that makes a lot of sense.
Certainly now, in the past 5 or 7 years, it is now I think widely agreed that migraines are neurovascular
headaches. Ultimately caused by excessive and unbalanced constriction and then dilation of blood vessels.
Which is triggered in part by hyper‐excited neural activity. Now it's going to be different for each unique person,
but for example, it can be the initial period of highly constrictive blood vessels which creates an aggressive
alarm, inflammatory response in the brain that then causes an aggressive dilation of blood vessels to counter
the ischemia in that part of the brain. If we look at the maybe typical etiology or pathophysiology of a migraine.
Certainly we know that stress and a number of different hormonal types of shifts can drive changes in the
neurotransmitters of the brain.
It is widely believed that there are issues with regard to stability in serotonin secretion and re‐uptake that can
be a big player here. Surges, large surges of serotonin can cause blood vessel constriction and then an imbalance
in serotonin and a relative dearth of serotonin after that can cause or contribute to dilation. Malfunctioning in
the balance of serotonin can be at play here. And this is one of the reasons why supplementation with 5‐HTP or
5‐hydroxytryptophan has been studied with regard to reducing the incidence and the frequency of serotonin. I
think in part because supplementation with 5‐HTP would help the body to have a more consistent steady state
availability of serotonin for keeping this type of vasoconstriction and vasodilation behavior more stable.
This is also a good example of how neurotransmitter balance has a very direct role on the cardiovascular system,
right? The neural activity also comes into play here. We know that some individuals, perhaps via genetics or
perhaps via inflammatory dynamics from lifestyle choices can have very sensitive trigeminal nerves. And when
inflamed our nerves are triggered to release neuropeptides. And there are a variety of them that are released,
but in particular something called CGRP which can trigger pretty dramatic vasodilation. Again, I've given you
some references with this. I don't want to get too geeky on you here because the super detailed level of
biochemistry is not of interest or relevance to a lot of us as practitioners. But if you are passionate about it and
want to learn more about it, I certainly want to have resources available for doing that.
Perhaps this is not a surprise, magnesium also rears its head here. Because we know that magnesium is critical
for keeping blood vessels appropriately responsive to hormones and neurotransmitters that are driving
constriction or dilation. Even just looking at this quick summary, you can see that issues with serotonin, issues
with inflammation, issues with stress, issues with magnesium can all be involved in a very specific way with
regard to migraine. Just like this can also be involved with pretty much any other type of headache.
Now, conventional migraine treatment typically involves a variety of different drugs. For prevention, the most
common choices are going to be beta blocker drugs. These are drugs that affect the cardiovascular system by
reducing blood vessel's sensitivity to rapid changes in vasodilation. In particular, making blood vessels less
sensitive to the effects of stress or inflammation coming from adrenaline: epinephrine and norepinephrine.
There are other drugs used as well. I wanted to just make you conversant on some of the other typical choices
here. But more targeted conventional therapy for ongoing migraine experiences is usually a combination of
NSAIDs plus a class of drug calls triptans and sumpatriptan, it would certainly be, I think, the most common
variety of drug on brand names typically Imitrex or Treximet. These are medications which mimics serotonin and
cause mild vasoconstriction during the phase when the headache has become active when prominent
Headache and Migraine,
Part 2
11
vasodilation is in effect. You see a photo here actually of a typical device used to administer Imitrex because it's
been shown to be most effective when injected under the skin for rapid absorption.
Like a lot of other medications as we've discussed for headaches. We know that frequent use of these drugs can
actually cause rebound headaches. It's not just the overuse of the NSAIDs or the analgesic medications but
overuse of the triptans can also be a problem. We talked about this in the first webinar, but I just want to give
you a little bit more data because I think it's important to help our clients understand that more is not better in
terms of the medication. I mean it can be wonderful to have the drugs available for managing the severe effects
of a headache that maybe our lifestyle choices have not been able to prevent. But the typically medications are
not a viable solution for chronic migraine, not only because of the debilitating side effects but because they end
worsening the very situation they've been prescribed in order to address.
I also think it's very interesting and I give you some references here for this in particularly that more recent
research. Literally in the past year or two, is starting to look at the use of monoclonal antibodies for CGRP to
actually very directly block the action of the peptide that causes the vasodilation, that causes the headache
itself. This, I think, is a great example of really trying to target pharmaceutical development to get at, at least,
the biochemical true root cause of the headaches so that it can be more effective at providing relief. So an
interesting dynamic.
A monoclonal antibody would be literally injecting an antibody that would cause the body to breakdown or
prevent the secretion of the substance itself. Monoclonal antibodies are relatively new pharmaceutical tool that
are also being heavily researched in the area of cancer. In order to help our immune system to be directed to
attacking something that isn't surplus in the body or causing an actual disease process. It's a great way to target
a substance in the body that is normal and expected and healthy when it's secreted in moderate amounts, but
when it's secreted aggressively, it causes a disease state. Essentially, helping us to use our own immune system
to our own advantage by keeping house in the body and keeping any natural substances from becoming surplus.
Now, I want to start to talk a little bit more in‐depth about some migraine specific dynamics in the body. Now,
we talked about the role of food allergy and food sensitivity in headache in our first webinar. Certainly, they can
play a role in a wide variety of different types of headaches. Specific to migraine, we need to consider the effects
of histamine. Histamine is a natural substance in the body. It is released in a wide variety of inflammatory
dynamics. Histamine, as one of its more fundamental actions, causes vasodilation in the body. A surge of
histamine either due to high ingestion of histamine from foods or high production of histamines as an allergic or
inflammatory response in the body can definitely trigger a migraine.
There are other substances like the dietary amines like what we talked about before like tyramine. Which can
cause the secretion of other vasodilating substances. What we want to keep in mind that aggressive vasodilation
is a huge driver in migraine. Again, especially when it's paired with that hyper‐reactivity in the neural system. It
is definitely more common for a combination of specific foods to be involved in triggering migraine. Perhaps a
combination of foods that contain a lot of histamine than cells, such as cheese, especially aged cheeses in
combination with histamine triggering foods like chocolate, for example.
Red wine … I give you a great listing down here at the bottom. There's an article or a clinical study, by the way,
specifically about red wine. Which interestingly enough, not only contains histamine but triggers the release of
more histamine and also has an impact on the serotonin system. It's not a surprise perhaps that red wine is one
of the foods most commonly implicated in triggering migraine. There can be other food additives triggers as
Headache and Migraine,
Part 2
12
well. Yellow Number 5, tartrazine; this actually shows up as a relatively common trigger for migraine.
I want to talk a little bit about the notion of histamine intolerance. If we have a high intake of histamine‐
containing foods but an inability to effectively breakdown that histamine in the GI tract, then we're going to be
absorbing a lot of that histamine. Lack of an enzyme called diamine oxidase can actually be involved in creating
histamine intolerance. For people who struggle with histamine intolerance, there are a variety of digestive aids
that can be taken at mealtime in order to breakdown histamine in foods.
Certainly, avoiding high histamine foods and I give you some references for that later on in the webinar. But
avoiding high histamine foods is an excellent strategy for people who believe that it's a trigger for their
migraines. We know clearly from clinical study that migraine sufferers across the board are more likely to have
higher histamine not only during their headaches but actually during times without headaches. Indicating that
histamine intolerance or histamine surplus is a fairly common predisposing factor for migraines. These are
supplements that can be taken just like any other digestive enzyme in order to help reduce histamine absorption
into the body.
I give you a little factoid there. Interestingly enough, women have lower levels of diamine oxidase than men.
And there are certainly many scientific bastions that would argue that that is one of the major reasons why
women are more likely to have migraine than men. Interestingly enough, migraines during pregnancy are quite
uncommon. We know that our levels of diamine oxidase in women skyrocket during pregnancy. Which I find …
Again, that's just a correlation. But I find it to be very interesting in terms of the body protecting itself from
various potential sources of inflammation during pregnancy.
Again, just a reminder as we're cruising along here that there is always a number of references at the bottom of
the pages here that are a mixture of clinical studies, references for further information, maybe references that
you might want to share with your client. In reviewing these courses, especially during your second viewing of a
course. Make sure that you follow through on these references. You can always use the PDF file of the slides for
the webinars to easily click on the links embedded in the PDF for following up online.
Now, we know that there are a number of vitamin and mineral co‐factors in producing diamine oxidase, but
interestingly enough, vitamin B6 is a critical co‐factor, an enzyme co‐factor for making diamine oxidase and this
has been studied. We know that vitamin B6 supplementation in the majority of migraine sufferers increases the
production of diamine oxidase. Now, generally, I am a big fan of supplementing with any B vitamin by using a full
spectrum complex. I gave you some examples of my favorite choices here on this page. But in particular for
migraine, I am a fan of using full spectrum, B complex supplements for migraine. Not only to boost B6 but also
to boost Vitamin 9 or folate and also Vitamin B12. Because while B6 in particular is needed to boost diamine
oxidase to help reduce histamine in the gut coming in from food, for example, or beverage. The other B vitamins
are necessary to promote a biochemical process called methylation in the body.
Intracellular histamine is broken down by an enzyme called HNMT that we have to be able to methylate in order
to produce. Indeed, it's been studied a few different times in good high quality studies that supplementing with
these methylation‐driving B vitamins reduces the incidence of migraine. Now, it's perhaps not a surprise given
this that individuals with high homocysteine. Which is a lab marker, HCY, that can be ordered in typically fairly
conventional lab work. We know that homocysteine is an amino acid that when it's built up can cause
inflammation internal to blood vessels. Which certainly could easily be related in migraine. It also independently
Headache and Migraine,
Part 213
increases the risk for cardiovascular disease as an aside.
Elevated levels of homocysteine are basically evidence of insufficient methyla�on within the body. There is a correla�on between migraine and homocysteine. You likely know from prior SAFM Clinical courses that certain individuals can have gene�c impairments in methyla�on. Which present a need for higher levels of folate, although different gene�c snips can actually be targeted to B12 or B6 as well. But certainly the most common ones that we talk about, that is the MTHFR snips, and that extended family of snips. Basically require an individual to have higher intake of folate in order to methylate efficiently.
Again, a number of clinical references here for you to follow-up on if you're interested. These are some of my favorite supplements for B-complex, in par�cular, for migraine. Each of them includes full spectrum B-complex including good methyl forms of vitamin B12 and folate, and also a mixture of B6 in the more typically pyridoxine form but also the pyridoxal 5-phosphate or P5P form. That's the ac�vated final form that can be immediately used. For those of you joining us for the semester program, we're going to talk more about these forms of nutrients in our Supplements course. In order to help you understand some of the different issues that people can have making use of nutrients. Because of an inability to converts supplements into the final form that the body needs in the biochemical processes.
It's beyond the scope of this class to really get into the detail and the workings of the methyla�on cycle. That is covered in several other SAFM Clinical courses. But I did include just a simple diagram here for you if you want to know more. The reference is down here below. Also a couple of them go into more detail explaining methyla�on.
Now, I want to start to talk about some of the proven remedies for migraine. The first one is an herb called feverfew. Also o�en known colloquially as wild chamomile. Which I want to point out is quite dis�nct from German chamomile which is the typically herb that would be included, for example, in most chamomile teas. This is arguably the most popular herbal remedy, especially for preven�on of migraines. It's been clearly shown in mul�ple studies that ongoing use of feverfew reduces both the frequency and the intensity of migraine a�acks.
In fact, a couple of the studies here include a very strong crossover result where not only does random double blind addi�on of feverfew in a popula�on reduce the incidence of migraine. But removing it from that same popula�on later on results in resurgence of migraines. Which is really quite conclusive in terms of the effects. Now, like all herbs, there are hundreds of different cons�tuents in feverfew. But it's wildly believed that two par�cular ones: chamozulene and parthenolide are the main ac�ve ingredients with regard to migraine. It's interes�ng.
There are a number of different avenues of belief about their modes of effect but one of the ones that I think is most interes�ng is that both of these phytonutrients have high molecular similarity to serotonin. Like anything else, supplemen�ng with them would inhibit or reduce any other type of endogenous serotonin surge in the body and can prevent their being quite as aggressive as a vasoconstric�ve surge. Which is that star�ng point of migraine that then causes that reac�ve vasodila�on in response.
It's also been shown directly that feverfew inhibits the secre�on of prostaglandins. And again, inhibits that release of serotonin from the platelets in the blood which is what can cause that vasoconstric�ve surge. These par�cular ingredients are much more prevalent in the leaves of this plant. Rather than the flowers or the root,

Headache and Migraine,
Part 214
and so the form of the supplement is important. I just gave you some notes here with regard to dosage that's been studied as being effec�ve. Generally speaking, a herbal supplement with li�le to no side effects, very well-tolerated.
Otherwise in the herbal arena, I think a couple of other ones that are worth men�oning: Bu�erbur has also been studied not quite as broadly as feverfew but in a couple of good quality studies it's been shown that migraine incidence and frequency are reduced by at least 40%. I wanted to men�on bu�erbur in par�cular because it's been studied in children. I'm sure most of you can relate to the fact that that's a wonderful discovery. Because so few herbal remedies have been studied specifically in children or adolescents. To the point of really being able to not only demonstrate efficacy but just safety. This is a remedy that can be used. But very importantly, and I really wanted to call this out separately, as is o�en the case, herbs can have suppor�ve ingredients but they can also have other cons�tuents that when consumed in high dose can be liver toxic. That is the case with bu�erbur.
There are a number of different brand names that offer par�cular formula�ons of bu�erbur, in par�cular the Petadolex formula�on. Which has been refined to remove the alkaloids in bu�erbur that are specifically toxic to the liver.
Another good example for that, a non sequitur, but another good example for that are related to our first webinar for this course is curcumin. Which is an extract from the herb turmeric. While consuming turmeric in really high doses can have a very nega�ve side effect in rapidly increasing the incidence of kidney stones. Because turmeric as a whole herb contains high levels of oxalates. And high oxalate consump�on can quickly and drama�cally predispose you for kidney stones. Curcumin as an extract of turmeric is one of the most potent an�-inflammatory ingredients in curcumin. But it does not have a high oxalate content. It's a good example of an extract from an herb just like Petadolex is from bu�erbur. That removes some of the nega�ve side effects or some of the more harmful ingredients when consumed in high levels.
I also wanted to men�on ginger because it's such an easy thing to add to someone's diet. And certainly, ginger can be taken in supplement form, but it's so delicious. It's an easy thing to just include in the diet. The equivalent of ginger that's included in the studies that has been shown clinically to be as effec�ve as sumatriptan for migraine preven�on. It's only about a quarter inch of fresh ginger root daily, which is not very much. Interes�ng, I wanted to include a study on looking at the combina�on of ginger and feverfew in a supplement that's called LipiGesic that I've shown you here. If someone is unable to tolerate, for example, ginger in dietary form. Then certainly there are supplement op�ons. Certainly, when we can, enjoy the benefits of an herb through dietary enjoyment rather than a supplement. I'm a big fan of that.
Okay, I'm going to shi� into cellular energy produc�on now, but I'm going to recommend that we just take a li�le bit of a break here at this point in the presenta�on. Give you a chance to just collect your thoughts. Hopefully get up and walk around and stretch a li�le bit. Maybe use the bathroom or refill your beverage and just get yourself re-energized for the second half of our presenta�on and I will be back with you in about five minutes.
All right, so welcome back from your break. Hopefully you feel a li�le rejuvenated. Ready to refocus. I plan to take our break right here because I'm going to shi� gears on you a li�le bit. I want to talk about the impact of cellular energy produc�on, specifically as it relates to migraine. Again, I'm going to try to not get pulled into doing too much of an in-depth explana�on here because as I described earlier, we have an en�re SAFM
Headache and Migraine,
Part 215
Clinical course focused on this. Which is a really founda�onal course. In fact, it's one of the two that are required clinical course choices in our semester program for being able to sit for the cer�fica�on exams for Applied Func�onal Medicine for Coaching cer�fica�on. Because I think it's such a cri�cal concept.
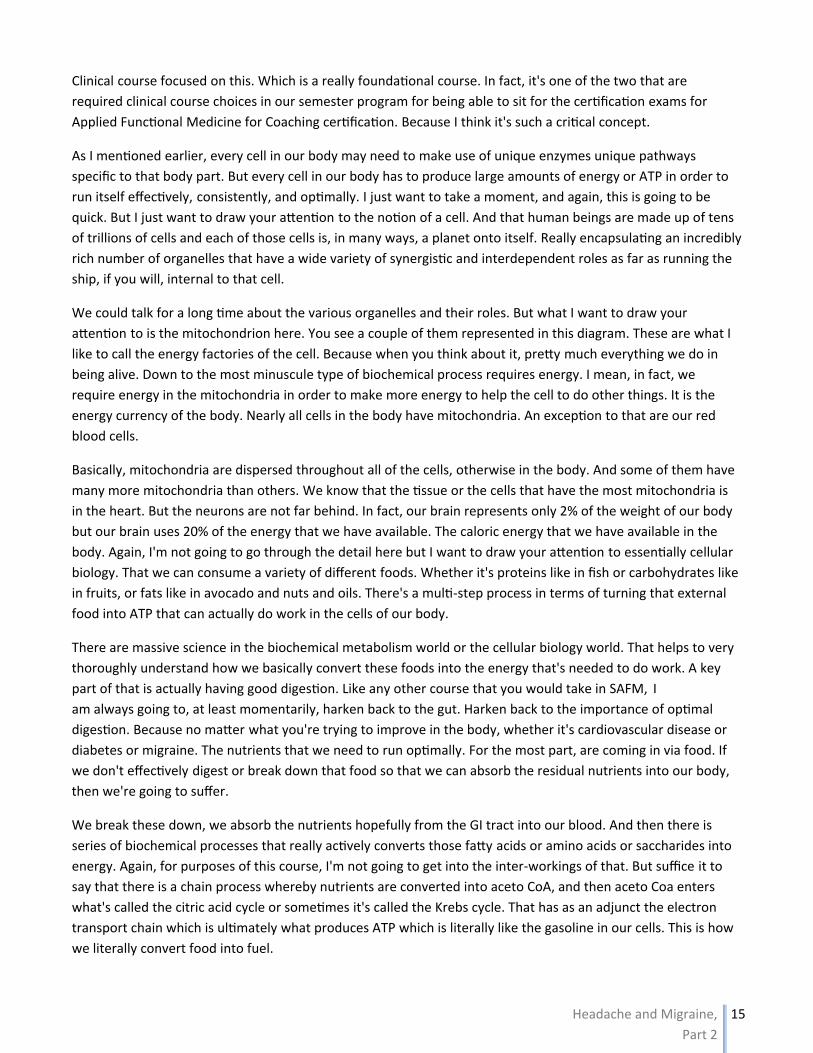
As I men�oned earlier, every cell in our body may need to make use of unique enzymes unique pathways specific to that body part. But every cell in our body has to produce large amounts of energy or ATP in order to run itself effec�vely, consistently, and op�mally. I just want to take a moment, and again, this is going to be quick. But I just want to draw your a�en�on to the no�on of a cell. And that human beings are made up of tens of trillions of cells and each of those cells is, in many ways, a planet onto itself. Really encapsula�ng an incredibly rich number of organelles that have a wide variety of synergis�c and interdependent roles as far as running the ship, if you will, internal to that cell.
We could talk for a long �me about the various organelles and their roles. But what I want to draw your a�en�on to is the mitochondrion here. You see a couple of them represented in this diagram. These are what I like to call the energy factories of the cell. Because when you think about it, pre�y much everything we do in being alive. Down to the most minuscule type of biochemical process requires energy. I mean, in fact, we require energy in the mitochondria in order to make more energy to help the cell to do other things. It is the energy currency of the body. Nearly all cells in the body have mitochondria. An excep�on to that are our red blood cells.
Basically, mitochondria are dispersed throughout all of the cells, otherwise in the body. And some of them have many more mitochondria than others. We know that the �ssue or the cells that have the most mitochondria is in the heart. But the neurons are not far behind. In fact, our brain represents only 2% of the weight of our body but our brain uses 20% of the energy that we have available. The caloric energy that we have available in the body. Again, I'm not going to go through the detail here but I want to draw your a�en�on to essen�ally cellular biology. That we can consume a variety of different foods. Whether it's proteins like in fish or carbohydrates like in fruits, or fats like in avocado and nuts and oils. There's a mul�-step process in terms of turning that external food into ATP that can actually do work in the cells of our body.
There are massive science in the biochemical metabolism world or the cellular biology world. That helps to very thoroughly understand how we basically convert these foods into the energy that's needed to do work. A key part of that is actually having good diges�on. Like any other course that you would take in SAFM, I am always going to, at least momentarily, harken back to the gut. Harken back to the importance of op�mal diges�on. Because no ma�er what you're trying to improve in the body, whether it's cardiovascular disease or diabetes or migraine. The nutrients that we need to run op�mally. For the most part, are coming in via food. If we don't effec�vely digest or break down that food so that we can absorb the residual nutrients into our body, then we're going to suffer.
We break these down, we absorb the nutrients hopefully from the GI tract into our blood. And then there is series of biochemical processes that really ac�vely converts those fa�y acids or amino acids or saccharides into energy. Again, for purposes of this course, I'm not going to get into the inter-workings of that. But suffice it to say that there is a chain process whereby nutrients are converted into aceto CoA, and then aceto Coa enters what's called the citric acid cycle or some�mes it's called the Krebs cycle. That has as an adjunct the electron transport chain which is ul�mately what produces ATP which is literally like the gasoline in our cells. This is how we literally convert food into fuel.
Headache and Migraine,
Part 2
16
Now, specifically as it relates to migraine. The cellular energy factories are just as critical for the functioning of
neurons as they are for the heart tissue. We know that low or inconsistent energy production within the
neurons can lead very specifically to hyper sensitization in the neural system and then also increased pain
sensitivity. Alongside the whole neurotransmitter piece that we were talking about earlier. This is a major
dynamic in migraine and it's been demonstrated that this type of lower inconsistent energy production is much
more common in migraine sufferers than it is in the average population.
Now, magnesium yet again rears its head in the sense of having a role here. Because we know that low
magnesium promotes insulin resistance and insulin sensitivity is necessary to get glucose as a fuel from the
outside of the cell to the inside of the cell. Where it can actually enter the mitochondria and be turned into fuel.
Once again, magnesium is playing a role in the etiology of headache down … I think we talked about maybe six
different pathways at this point.
What you're seeing here in the upper right‐hand corner is an actual micrograph of a mitochondrion. It's pretty
interesting. It looks a lot like a bacteria. If you've taken our Cellular Metabolism course. We talk about the
evolution of man as a creature and the basic engendering or bringing in of the mitochondria through the
evolution of the species over billions of years in order to sequester the function that used to be performed by a
bacteria internal to the organism. I'm not going to get into the biology of the mitochondrion. Just a simple
diagram here so you can see what it looks like if you're curious. Certainly, within all of the different folds here is
where the ATP production is taking place.
It also requires ample hydration and oxygen. In fact, people with pre‐existing asthma are more likely, at least
based on one I think very provocative study. More likely to have migraines and actually more likely to have them
worsen over time. I think an interesting reflection on our body's need for optimal respiration in terms of oxygen
availability for helping us to run our neurons and thinking clearly.
Now, I want to talk about some of the key nutrients that are necessary for optimal cellular energy production
that have been well‐studied specifically with regard to migraine. Vitamin B2 or riboflavin is a particularly
important co‐factor for multiple enzymes involved in cellular energy generation, especially in that latter stage of
the electron transport chain. At this point, it's actually multiple studies that have clearly demonstrated the
efficacy of high dose riboflavin in preventing migraine. If you were going to make one nutrient or one
supplement suggestion to your clients and patients who suffer from chronic migraine, this should be it, 400 to
500 milligrams a day, which is a very big dose.
In the vast majority of people, the only thing they're going to experience as a result of this dose is that their
urine is going to be very yellow. I think an important thing to consider about riboflavin is that this type of
therapy has been shown to take some time to be effective. And it's really critical that you set expectations with
your patients and clients so that they are not unrealistically expecting a supplement to yield results in just a few
days. In many ways, it's unfortunate that our culture toward health remedies has been highly biased by
medications. Which are designed to essentially numb us from our pain, and that typically take … They start to
have an effect after half an hour. People can readily expect and understandably expect that any type of
supplement that they take is going to have some sort of therapeutic benefit, if not within hours, certainly within
a few days.
It's important when things are much more longer acting that we clearly explain that to them upfront. In fact, in
the case study I'm going to show you, it was a good four months before dramatic effects were seen in terms of
Headache and Migraine,
Part 217
reduc�on of migraine. It's important to set expecta�ons. The only other cau�on around riboflavin use at this dose is that in a few rare cases, it can create photosensi�vity in terms of strong reac�on on the skin when someone is exposed to sunlight. Typically perhaps a rash or some other type of radia�on sensi�vity. Interes�ngly enough, in those cases significantly lower doses of riboflavin may be as effec�ve for migraines. Interes�ng dichotomy in some of the studies that looked at lower dose versus higher dose, and the higher dose certainly had a more consistent broad-based effect. But there are some people who showed the same type of effect at a much, much lower dose, about a fi�h or less than the higher dose that's been studied.
Again, showing you just some common brands of the high dose riboflavin. You're typically going to be pairing this along with a full spectrum B-complex, and so the typical dose of riboflavin and a B-complex which might be a 10 or 15 or maybe 20 milligrams is certainly going to be �ny in comparison to what is needed given the studies with regard to migraine. There's no issues with overlapping those two.
Now, I also want to talk about CoQ10. For those of you who have studied cellular energy produc�on before, you know that CoQ10 is absolutely cri�cal for mitochondrial energy produc�on on mul�ple levels. Once again, perhaps not surprisingly, it's been shown that those with migraines, chronic migraines sta�s�cally have lower CoQ10 levels, serum CoQ10 levels. It has been studied and shown that increasing CoQ10 through supplementa�on reduces migraine frequency and severity in those with reduced levels but also in those with normal levels. The dosing that I would recommend given study results would be 150 milligrams twice a day. I want you to be aware that a number of your clients who take certain prescrip�on drugs are going to be more likely to have insufficient CoQ10. Specifically those using sta�ns, typically to reduce cholesterol. Beta-blocker drugs, typically for hypertension but beta-blockers can be prescribed for a variety of issues. And then glyburide, which is one of mul�ple types of medica�ons used for Type 2 diabetes.
Now, CoQ10 is available in a few different forms. In the body it oscillates between the ubiquinone which is the oxidized form and then the reduced or ubiquinol form which is the reduced form is with the one that's ac�vated for, actually being used in these biochemical processes. Like a number of other nutrients, in a young healthy body conversion from the oxidized to the reduced form is readily accomplished. But that becomes impaired as we age, so where possible, I like to recommend that people purchase the ubiquinol form specifically, especially for those over the age of about 40.
Recognizing that it is more expensive and certainly for people who are suffering with migraine, I think it's most important that they take it. Period. It's important to realize that your typical CoQ10 supplement, which is going to be ubiquinone, it's not that it's going to be totally ineffec�ve in people who are older, it's just the risk that they will be less effec�ve. Where cost is not a huge barrier, I highly recommend ubiquinol, but certainly encourage people to take what they can afford and what they can get.
All right, so again, just showcasing some different varie�es of what is available in terms of supplements. Now, I want to spend a few moments talking about inflamma�on and oxida�ve stress. Now we talked about this in a number of other SAFM Clinical courses, so for many of you this is going to be a review. I think the easiest way to think about oxida�ve stress is essen�ally biological rust. We know that iron, for example, when it is oxidized, when it is exposed to oxygen in a unprotected or uncoated state, it's going to rust. That is evidence of ac�ve oxida�on or breakdown of the substance. Well, unfortunately, our �ssue is vulnerable all the �me, every day we're alive to the effects of oxida�ve stress.
If our burden of oxida�ve stress or pro-oxidant molecules outweighs or overloads our available supply of an�-
Headache and Migraine,
Part 2
18
oxidant capability. Then we're going to end up with a net positive load of oxidative stress. Which over time, if
un‐addressed is going to create damage. Essentially, I like the simplicity of Dr. Blaylock's description here. Very
reactive particles that can burn most things they touch through a process called oxidation. This is what free
radicals or reactive oxygen species are. Either directly or more typically through an indirect triggered process,
there are thousands of different types of antioxidants in the body to help counter this effect. Because it's
important to realize that oxidation or oxidative stress is not always negative. There are positive effects of
controlled mild oxidative stress. It's part of what allows us, for example, to fight an infection, is creating localized
oxidative stress in order to kill something that we don't want in the body.
In this modern day and age where a lot of the sources of oxidative stress can be quite potent and common. And
in our diet we struggle to bring on board as many antioxidants, we can end up with imbalance. Also realizing
that a number of different antioxidants and some of the most powerful like glutathione or superoxide
dismutase. These are endogenous antioxidants. Meaning these are not things that we typically consume. They
are things that are produced by the body given the availability of nutrients. Of course, you know I'm going to
take this right back to the gut.
In order to make glutathione, for example, we have to have really good digestion. We have to have good intake
of healthy proteins and minerals and B vitamins in order to make these substances that are going to protect us.
Free radicals or these reactive oxidative species can damage any tissue throughout the body. In fact, it's well‐
understood that a primary etiology of cancer is by DNA damage. Damage within the nucleus of our cells caused
by oxidative stress. Now, we have in our cells, especially in our DNA, internal repair processes that are designed
to correct for and counter the effects of oxidative stress. Unfortunately, like many things, those processes can
become impaired especially over time as we age.
If we have a typical Western highly processed nutrient‐poor diet. That's a bit of a double whammy and a double
negative in terms of impairing our body's ability to counter oxidative stress. It's important to realize that just
living creates oxidative stress, creates free radicals. Our basic metabolism generates free radicals. There are a
number of things that we might typically do or expose ourselves to that can generate a real surge of oxidative
stress. I included the picture here because I've had a couple of clients over time realize that one of the
contributors to their chronic headaches was over‐exercise, overly aggressive exercise. People can be addicted to
exercise just like they can be addicted to alcohol or carbohydrates or any other type of neuromodulating activity
simply in an effort to feel better.
Sustained elevated blood sugar we know causes oxidative stress internal to our arteries. High intake of highly
processed oils like typical bottled refined vegetable oils or damaging fats like trans‐fats. Toxins like heavy metals.
Highly processed or overcooked foods. There are a number of common lifestyle choices that can be generating
oxidative stress. And so these aren't specific to migraines. These are the kinds of things that I would encourage
you to always discuss and cover with your patients and clients in terms of helping them to understand that the
root causes of chronic inflammatory conditions might be things that they take for granted or even things that
they think of as healthy.
Now, the biochemical process that our cells use to create aceto CoA and to run the citric acid cycle and the
electron transport chain. This whole series of cascading biochemical conversions can be highly disrupted by a
build‐up of oxidative stress. Literally slowing the pace or the efficiency of the enzymes that run the cellular
energy production. This is the simple example of how a buildup of oxidative stress can end up causing
dysfunction in cells of tissue anywhere in the body. A great example of how our lifestyle choices very directly
Headache and Migraine,
Part 219
affect the func�oning of the body. In par�cular, we know toxins can play a huge role in genera�ng oxida�ve stress.
I just wanted to give you some really simple pearls about this in terms of helping you to realize the impact of toxins and the poten�al benefit of your clients making lifestyle choices such as a regular seasonal inflamma�on or inflamma�on cleanse or detoxifica�on type of regimen. CAC is citric acid cycle. I've give you a lot of references here. Again, this may or may not be of acute interest to you but I wanted to give you plenty of material if you wanted to pursue it. We have an en�re course in SAFM focused on heavy metal detoxifica�on and a number of other courses go in-depth into liver detoxifica�on and toxin clearance.
Here, I just want to highlight that exposure to these types of things and high levels of downstream oxida�ve stress coming from the biochemical cascade can absolutely create a lot of oxida�ve stress and be part of what contributes to migraine. Unlike the no�on of a one or two or three weeks detoxifica�on type of cleanse a couple �mes a year because it's an opportunity for people in a more isolated way to ramp up nutrients that the body needs in order to process and detoxify so that they can excrete certain chemical substances, especially heavy metals. Because in general, when we bring toxins on in the body, the majority of them are not water soluble so they're not simply excreted in our urine.
A lot of them are fat soluble. And they have to actually be converted in order to be excreted. The liver, of course, has a need for certain amino acids and minerals and vitamins in order to do that. As a prac��oner, I will share with you that running this type of detoxifica�on cleanse can be a very lucra�ve group program choice not only in and of itself but it's a great way to have poten�al clients get to know you and begin to see some strong posi�ve results and perhaps follow through on becoming an individual client or pa�ent of yours.
I want to propose an interes�ng ques�on that out of all the different dynamics we talked about for migraine: Is perhaps the ul�mate common root cause for all of the poten�al triggers for migraine just about oxida�ve stress? This is very hot and current in the medical and clinical research world regarding migraine. We already know for sure that a build-up of reac�ve oxygen species is usually involved in the development and certainly the progression of neuropathic pain. Interes�ngly enough, studies published in the past year, a year and a half, are beginning to really acknowledge that serum levels of an�oxidants are lower in people who suffer from migraines. Serum levels of oxidants are higher. Serum levels of glutathione are lower.
These are just obviously associa�ons but I think it presents a really compelling argument or case for the fact that underneath all of these different dynamics, perhaps it is the build up through mul�ple triggers of oxida�ve stress that spills over that ul�mately causes the neural dysfunc�on that is a key component of migraine. Certainly, at a minimum, we can absolutely assure that diet ma�ers. Because we can't make endogenous an�oxidants without having a diverse healthy diet and without having good gastrointes�nal diges�on and nutrient absorp�on. Interes�ng food for thought. And these references here are really fascina�ng. One of the course documents that I gave you is actually a really fascina�ng write up diving into every single one of these trigger categories and how it generates oxida�ve stress and how that might be directly involved in this common mode of ac�on. Really interes�ng read if migraine and headache are a strong interest of yours.
In summary, I've talked a lot of different dynamics. My recommenda�ons for your pa�ents and clients with migraines include, first of all, the subset of most common simple straigh�orward headache triggers or headache drivers that we discussed in our first webinar and then a series of migraine specific items. I think beyond the ini�al few, what I would most recommend taking a close look at is iden�fying and elimina�ng the dietary

Headache and Migraine,
Part 2
20
triggers for each individual person. But then otherwise, I think all of these are likely quite straightforward in light
of what we've talked about. I want to pull all of this together by reviewing with you just a quick case study.
I want to introduce you to Nellie. Nellie is a client of mine that I started … Actually I worked with Nellie a while
ago. I think she and I first started working together probably about 5 years ago and we worked together over in
a steady state fashion for about a year and a half, and then after that we continued to have intermittent
sessions every few months for another, almost two years. Nellie came to me with a few irritating kinds of
symptoms but her primary symptoms were persistent migraines. That she said she had had since her 20s. So
essentially persistent in her adult life. And she knew that those were exacerbated with poor quality sleep. Nellie
specifically was not having trouble falling sleep. She was having trouble staying asleep and would find herself
awakening multiple times during the night and struggling to go back to sleep rapidly. But would typically be
awake for 15, 20 minutes or more each time.
Nellie struggled with chronic sinus and nasal congestion. She had year round allergies. As she put it, a chronic
user of tissues. Tissue boxes all over her house. And tried not to use any histamine medications on a regular
basis because she felt very vulnerable to the wooziness as she put it, that she got the sedative effects of anti‐
histamines. She was wrestling with borderline and hypertension and was really resisting going on medications
but she had had that since about the age of 40, and she tended to struggle with moderate constipation. Typically
having four or five bowel movements during a week, but not really feeling like it was complete as it should be.
Given what we've discussed so far, I'll ask you to make use of the Questions tab on your GoToWebinar
dashboard, what interconnected do you see? What do you think is at play with Nellie's migraines? What might
you consider in helping her? Go ahead and type in and share your thoughts with me. Excellent. Hypertension,
constipation as it relates to magnesium insufficiency, questioning food sensitivities, questioning poor nutrient
absorption, questioning hormones. Excellent. Looks like all of you are ready to work with Nellie.
I don't think that this was a very confusing case. But it's important for you to understand that the connections
that you are making are the kinds of connections that Nellie had gone to, not one, not two, but as she shared,
five different conventional practitioners in an effort to try and get to the bottom of something to help her with
her migraines besides just drugs. The fact that you are bringing up topics such as low magnesium and low
serotonin and hormone imbalance and food sensitivity. These may seem straightforward to you in light of the
discussion we've had or in light of your functional medicine awareness now. But you need to understand that
Nellie is presenting with a typical kind of case that at least conventional non‐integrative medicine still struggles
to address in a way other than prescribing a standard of care medication.
You are all spot on. In fact, I like celebrating Nellie as a case because she is an example of someone who truly,
100% got rid of her migraines. At this point, the last time I met with her was about 18 months ago, but it's 18
months and counting from no migraines whatsoever. She went through essentially a, I would say a good four
months probably, three or four months, before she noticed a significant reduction in migraines. There was a
pretty dramatic improvement then around month 5 and then they started becoming intermittent where she
might have one a month or over time she might have one every few months. At this point, 18 months and
counting, she hasn't had any migraines.
I wanted to use this case and emphasize the timing. Because, again, I think setting expectations with your
patients and clients with regard to how quickly they can expect to experience major improvement and healing is
really critical. So that they don't give up on the journey before it's had enough time to have an effect. Indeed,
Headache and Migraine,
Part 2
21
we did a little follow‐up testing, not too much, but we did a little follow‐up testing and discovered that Nellie's
red blood cell magnesium was in the bottom 20% of the typical reference range and she started supplementing
with 300 milligrams of magnesium glycinate twice a day.
Now, I didn't capture it here. But after the first few weeks of that, just based on the fact that her bowel
movements improved and she started to feel better. For a period of time, she actually upped that to 500
milligrams twice a day which is a full thousand milligrams or a gram a day which is a lot of magnesium. She did
that for about six weeks or so. It might have been a full two months. It's a way of really getting a boost burst of
magnesium, and then she dropped back down to the 300 milligrams twice a day as a steady state supplement.
Which has actually been able to now keep her in the top 20% of the typical reference range.
I do recommend that she still get it checked when she goes in for her check‐ups every year or so. Just to make
sure that she's not suddenly finding herself substantially elevated outside of the reference range. I think a mild
elevation outside of reference range is fine. But we want to be cautious about having people getting it too high
because magnesium, like any other electrolyte, needs to be in balance with the others.
Nellie did a trial of supplementation with hydrochloric betaine with pepsin during her meals and found …
Actually, even though she had described it as a dramatic symptom ahead of time, she would say, "oh, I feel so
much better after my meals now. I feel lighter. I don't feel as heavy." We saw that Nellie's albumin was 3.7 and
with ongoing use of supplemental HCL, it's now up to 4.6. Interestingly enough, I've really come to the
conclusion that Nellie is perhaps just one of those people that simply is not producing enough HCL because of
age.
I did talk with Nellie about doing hormone testing. She didn't want to do that. She has a history of some
hormone mediated cancers in her family and just very afraid of hormones as a topic. It's certainly possible that
solutions to some of these things are in her hormones. But at least to date, she hasn't wanted to explore that.
But I definitely feel that a major reason why she has felt better is simply through better digestion. Making sure
that she's breaking down her dietary proteins to provide amino acids.
We also discovered through testing that Nellie is homozygous for the C677T variant of the MTHFR snip. Single
nucleotide polymorphism that impairs the body's ability to take up and make use of folate in methylation. That
was corroborated actually with a serum homocysteine level pretty soon after we started working together of
almost 30. Which is quite elevated. And over time, I will say it did take a while, I think it took a good nine months
of supplementation and lifestyle change, but homocysteine came down to a nice fairly optimal level of 8 which
not only I'm sure improved your body's ability to process histamine, but also decreased her risk for
cardiovascular disease.
Now, given her symptoms, of course we wanted to do some very migraine specific things. So we added
riboflavin and ubiquinol and quercetin. Actually quercetin twice daily was a real breakthrough for Nellie because
she started getting really dramatic relief from her congestion. But it was ultimately through the elimination of
dairy foods that she really … Well, as she put it, "I've decided now that I actually don't have year‐round allergies.
What I have is a permanent sensitivity to dairy and as long as I don't eat dairy, the only time I really suffer from
allergies is in the spring." Pretty huge lifestyle improvement for her with regard to simply reducing food, known
inflammatory foods for her. And improving her body's ability to process histamine.
Headache and Migraine,
Part 2
22
Now, I knew early on that likely a big driver for Nellie's migraines was intake of red wine. Which she and her
husband just both strong wine aficionados. She was consuming not excessive, but typically one glass of red wine
probably five nights a week. Admittedly, this was a painful change for her. But as I really worked on the
educational component … Please, please, please, never underestimate the criticality of education. Not just
telling your client what's going to make a difference, but teaching them. Just like I've done with you tonight.
Explaining the physiology to them, explaining what's involved, helping them to use the empowerment of
knowledge to motivate them to make lifestyle change. I do think the combination of eliminating the red wine
and the dairy was huge for her.
She switched to just enjoying an occasional vodka cocktail and she didn't love it as much. And so back down to
typically enjoying that once, maybe twice a week at most, and certainly cutting back on the alcohol was perhaps
therapeutic as well. A good example of just eliminating known high histamine foods. Supplementing with 5‐HTP
was a huge breakthrough. Most of you caught it right away. But people who have trouble staying asleep often
have trouble with sufficient serotonin in order to make a steady state supply of melatonin all night long. We
tried a couple of different frequencies in which she ended up settling in on, was using a 100 milligrams of 5‐HTP
around mid‐day.
She actually credited that with also perhaps making her less drawn toward alcohol around happy hour. Which I
think is also a wonderful pearl for all of you that one of the reasons why people would be drawn to drinking
alcohol every day, not just in terms of taking the edge off of the stressful lifestyle, but helping us to calm the
brain. Which is something that serotonin as an inhibitory neurotransmitter naturally does. She liked that timing
of taking the 5‐HTP at mid‐day and then she would take it again prior to bed. And really credited that perhaps in
combination with the reduction in red wine for helping her to sleep more soundly.
Certainly, another pearl for all of you is that as we age, we don't process alcohol as well. It is really common in
my client base for people to say, "Well, how come I used to be able to have a couple of beers and then go sleep
like a baby, and now I just have one beer and I fall asleep and I'm wide awake in two hours?" Unfortunately, this
is a very well‐documented effect of aging where we simply don't handle alcohol as well as we used to.
Then in terms of working on stress management and mindfulness practices. After some fits and starts, Nellie did
end up adopting a near daily meditation practice. She liked doing during the weekdays because she had other
spiritual and religious things that she enjoyed during the weekend. Certainly, I think this was also contributing to
her wonderful success by virtue of helping to reduce stress and creating a stronger mind‐body connection. A
pretty good subset of the migraine specific items that we talked about. Obviously applied for this unique person.
But she continues to sustain these lifestyle choices and the handful of supplements here to really great effect
and certainly there are no concerns about her continuing with those. She remains a very wildly satisfied client
who has sent me several different referrals. Because … I mean, I, too, would be over the moon excited about
having my migraines not just be improved but actually gone.
Like a lot of my clients, Nellie fell off the wagon about six months in to her improvement thinking that maybe
her migraine vulnerability was gone and cutting back on some of the supplements and got pretty rapid feedback
within about two weeks when she ended up experiencing a couple of migraines within a week. She actually to
her credit celebrated that as, "wow, I guess I really convinced myself now that the supplements are at work and
that they're having a large effect and that I really do need to continue to do them." I think it's human nature for
our patients and clients to, even when they're feeling great and they've experienced a lot of improvement, to go
Headache and Migraine,
Part 2
23
through a challenging time where they just want to be convinced that it's making a difference.
It's one of the reasons why I very often, nearly all the time, will recommend what I call a supplement holiday for
clients who are using supplements. Just taking a two‐week period at some point during the year where they
back away from all non‐critical supplements. And really trying to keep the list of what they stay on extremely
small, maybe one or two things at most. Stopping everything else, giving their body a rest from it. Certainly
giving their liver a rest from having to process so many things. And then methodically adding things back one at
a time. It's a wonderful opportunity to reinforce as you're adding them back why someone is using a certain
supplement and then also giving them a chance to re‐evaluate how it makes them feel as they add it back.
Hopefully, the case study is inspiring. I do not obviously think it is beyond possibility to provide this type of relief.
I've actually had several clients over the years who have experienced dramatic migraine relief. Nellie is only one
of two that have actually experienced complete eradication of their migraines. Certainly, the improvement, one
gentleman, Dave, who went from having migraines at least once a week to having them maybe once a month.
Well, for him, that's huge, huge lifestyle improvement in terms of being able to function normally and not have
his lifestyle so frequently interrupted with the debilitating migraine.
I encourage you to not be intimidated by migraines but to use what you've learned in this course as motivation
and inspiration to confidently and aggressively help your clients to counter migraine. As I mentioned earlier,
there are I think just over a dozen different documents posted for this particular course. I want to encourage
you to make sure that during the next week, you set aside time, a study slot in order to review all of the
documents for additional information and exploration, and then I just give you some additional resources here
that you can check out.
If you would like to read a book about migraine, I have explored several, and the one that I think is most helpful
and most well anchored in science is really this one here, What Your Doctor May Not Tell You About Migraines. I
should say that I do not think all of the books in this series are very well‐written at all, so I'm not promoting this
entire series of books, but this particular one written by Dr. Mauskop I think is very well‐written and does a good
job of highlighting and honing in on some of the concepts we talked about. It's really, really, I think, written so
it's accessible to a lay audience, so definitely something that you could also have your more savvy clients dive
into reading as well.
I hope you've enjoyed our course on Headache and Migraine. I hope this has given you a good strong
foundational understanding about the physiology and the pathophysiology of headache. A good understanding
of the variety of types of headache and a working knowledge of conventional therapies and their downsides.
And also built your toolbox and confidence in helping people to use lifestyle change and supplementation in
order to counter migraine. I think it's perhaps one of the best examples of the fact that though we perceive a
migraine or a headache as happening in the head, everything in the body is interconnected and all lifestyle
choices can have a systemic affect that can show up as symptoms or debilitation that maybe far distant from the
true root cause in the body.
I thank you very, very much for your time and your attention. As always, you'll be able to access this course
material by mid‐day tomorrow in terms of planning your second review of this course. As always, I will be
available to you for additional follow‐up Q&A on the course page. So I encourage you to feel free to post follow‐
up questions there. I will remain on the line here for a few more minutes just responding to the posted
questions on the Q&A tab, but otherwise I will go ahead and end our webinar and wish you all a good evening.

Headache and Migraine,
Part 2
24
Thank you so much.
The End